
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 26 September 2023
Sec. Public Health Policy
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1248260
This article is part of the Research TopicEthical and Economic Aspects of Genetic Testing and Frameworks and Policies to Assess and Regulate itView all 6 articles
 Savino Sciascia1†
Savino Sciascia1† Dario Roccatello1†
Dario Roccatello1† Marco Salvatore2
Marco Salvatore2 Claudio Carta2Laura L. Cellai2Gianluca Ferrari2Aimè Lumaka3,4
Claudio Carta2Laura L. Cellai2Gianluca Ferrari2Aimè Lumaka3,4 Stephen Groft5
Stephen Groft5 Yasemin Alanay6Maleeha Azam7
Yasemin Alanay6Maleeha Azam7 Gareth Baynam8Helene Cederroth9Eva Maria Cutiongco-de la Paz10
Gareth Baynam8Helene Cederroth9Eva Maria Cutiongco-de la Paz10 Vajira Harshadeva Weerabaddana Dissanayake11
Vajira Harshadeva Weerabaddana Dissanayake11 Roberto Giugliani12
Roberto Giugliani12 Claudia Gonzaga-Jauregui13
Claudia Gonzaga-Jauregui13 Dineshani Hettiarachchi11
Dineshani Hettiarachchi11 Oleg Kvlividze14Guida Landoure15
Oleg Kvlividze14Guida Landoure15 Prince Makay3
Prince Makay3 Béla Melegh16
Béla Melegh16 Ugur Ozbek6
Ugur Ozbek6 Ratna Dua Puri17
Ratna Dua Puri17 Vanessa I. Romero18
Vanessa I. Romero18 Vinod Scaria19
Vinod Scaria19 Saumya S. Jamuar20,21
Saumya S. Jamuar20,21 Vorasuk Shotelersuk22
Vorasuk Shotelersuk22 William A. Gahl23
William A. Gahl23 Samuel A. Wiafe24
Samuel A. Wiafe24 Olaf Bodamer25
Olaf Bodamer25 Manuel Posada26
Manuel Posada26 Domenica Taruscio2*
Domenica Taruscio2*Background: Patients, families, the healthcare system, and society as a whole are all significantly impacted by rare diseases (RDs). According to various classifications, there are currently up to 9,000 different rare diseases that have been recognized, and new diseases are discovered every month. Although very few people are affected by each uncommon disease individually, millions of people are thought to be impacted globally when all these conditions are considered. Therefore, RDs represent an important public health concern. Although crucial for clinical care, early and correct diagnosis is still difficult to achieve in many nations, especially those with low and middle incomes. Consequently, a sizeable amount of the overall burden of RD is attributable to undiagnosed RD (URD). Existing barriers and policy aspects impacting the care of patients with RD and URD remain to be investigated.
Methods: To identify unmet needs and opportunities for patients with URD, the Developing Nations Working Group of the Undiagnosed Diseases Network International (DNWG-UDNI) conducted a survey among its members, who were from 20 different nations. The survey used a mix of multiple choice and dedicated open questions covering a variety of topics. To explore reported needs and analyze them in relation to national healthcare economical aspects, publicly available data on (a) World Bank ranking; (b) Current health expenditure per capita; (c) GDP per capita; (d) Domestic general government health expenditure (% of GDP); and (e) Life expectancy at birth, total (years) were incorporated in our study.
Results: This study provides an in-depth evaluation of the unmet needs for 20 countries: low-income (3), middle-income (10), and high-income (7). When analyzing reported unmet needs, almost all countries (N = 19) indicated that major barriers still exist when attempting to improve the care of patients with UR and/or URD; most countries report unmet needs related to the availability of specialized care and dedicated facilities. However, while the countries ranked as low income by the World Bank showed the highest prevalence of referred unmet needs across the different domains, no specific trend appeared when comparing the high, upper, and low-middle income nations. No overt trend was observed when separating countries by current health expenditure per capita, GDP per capita, domestic general government health expenditure (% of GDP) and life expectancy at birth, total (years). Conversely, both the GDP and domestic general government health expenditure for each country impacted the presence of ongoing research.
Conclusion: We found that policy characteristics varied greatly with the type of health system and country. No overall pattern in terms of referral for unmet needs when separating countries by main economic or health indicators were observed. Our findings highlight the importance of identifying actionable points (e.g., implemented orphan drug acts or registries where not available) in order to improve the care and diagnosis of RDs and URDs on a global scale.
An accurate diagnosis is the cornerstone of medicine; it is essential for informed care and promoting patient and family well-being. However, individuals and families living with a rare disease (RD) typically spend more than 5 years on a diagnostic odyssey of specialist visits and invasive testing that is lengthy, costly, and often futile. Graessner and colleagues estimated that up to 50% of patients with a rare disease remain undiagnosed even in advanced expert clinical settings where genome sequencing techniques are applied routinely (1). The main reason is that the current diagnostic paradigm based on single-center expertise is not well designed for rare diseases, especially for patients who remain undiagnosed after the initial set of investigations (clinical, instrumental, and laboratory). In this setting, collaboration among all parties (clinicians, researchers, and patient organizations) is essential to reduce the burden associated with a delayed diagnosis and improve the overall management of patients living with rare diseases.
Among ongoing national and international initiatives, the Undiagnosed Diseases Network International (UDNI) (2), by actively involving patients and patient organizations, aims to reduce or eliminate information gaps that contribute to delay diagnosis and promote the integration of research into clinical practice in a process of mutual education.
To map unmet needs and opportunities, a first pilot survey was launched in October 2020 among the UDNI Developing Nations Working Group (UDNI DN WG, hereafter WG) (3). The WG is composed of representatives from 20 countries, including developed as well as low- and middle-income countries (LMIC). In this work, we present the findings of a follow-up survey, aimed to better characterize the global scenario, focusing on existing barriers and policy aspects impacting the care of patients with rare and undiagnosed diseases.
Based on the results of the pilot survey (3), this study was developed within the WG to further investigate the main needs for diagnosing undiagnosed patients, aiming to better characterize existing barriers, explore policy aspects, and correlate those needs to national healthcare economics and advocacy organizations.
The survey was structured into three domains, each explored through a mix of multiple choice and dedicated open questions. The results were structured based upon descriptions provided by each country’s representative and summarized in tables and figures. Three domains were addressed.
Domain 1. Unmet needs.
Domain 2. Characteristics of healthcare organizations.
Domain 3. Regulatory aspects and policy.
The survey’s technical functionality and overall consistency were first tested among the co-chairs of the Working Group and members of their respective teams. The WG representatives from all 20 nations were then informed of the WG objectives and supported them. This approach has been previously detailed (3).
To explore reported needs and analyze them in relation to national healthcare economical aspects, publicly available data on the following indicators were retrieved and incorporated in our study: (a) World Bank ranking; (b) Current health expenditure per capita; (c) GDP per capita; (d) Domestic general government health expenditure (% of GDP); and (e) Life expectancy at birth, total (years). Categorization into quartiles for each indicator were used for our analyses. Data were retrieved as open source in the World Health Organization Global Health Expenditure database.
The Global Health Expenditure Database provides comparable data on health expenditure for more than 190 WHO Member States since 2000 with open access to the public. WHO works collaboratively with Member States to update the database annually, using available information such as health accounts data, government expenditure records, and official statistics. The database represents a unique data source to perform research on public health topics, such as health care functions, primary health care, spending by diseases, and conditions (apps.who.int./nha/database, Accessed August 21, 2023).
Undiagnosed Diseases Network International members of the 20 countries involved in this study (100%) provided their responses based on their own knowledge of the country’s situation on a comprehensive array of RD-related challenges. Each participant member was actively involved in RD at a high level in their own nation. Each respondent answered the questions based on his or her specific understanding of the country’s RD ecosystem and URD condition.
The main characteristics of the participant members, including the type of institution, the presence of an initiative dedicated to undiagnosed and rare diseases within the country’s health care system, the presence of a specific genetic program dedicated to undiagnosed and rare disease, and the type of coverage are described in Table 1. The UDNI countries and country representatives contributing to the UDNI Developing Nations Working Group have been previously described (3). In this study, we provide descriptors to explore the current scenario of rare diseases across different countries with a specific focus on policies in place.
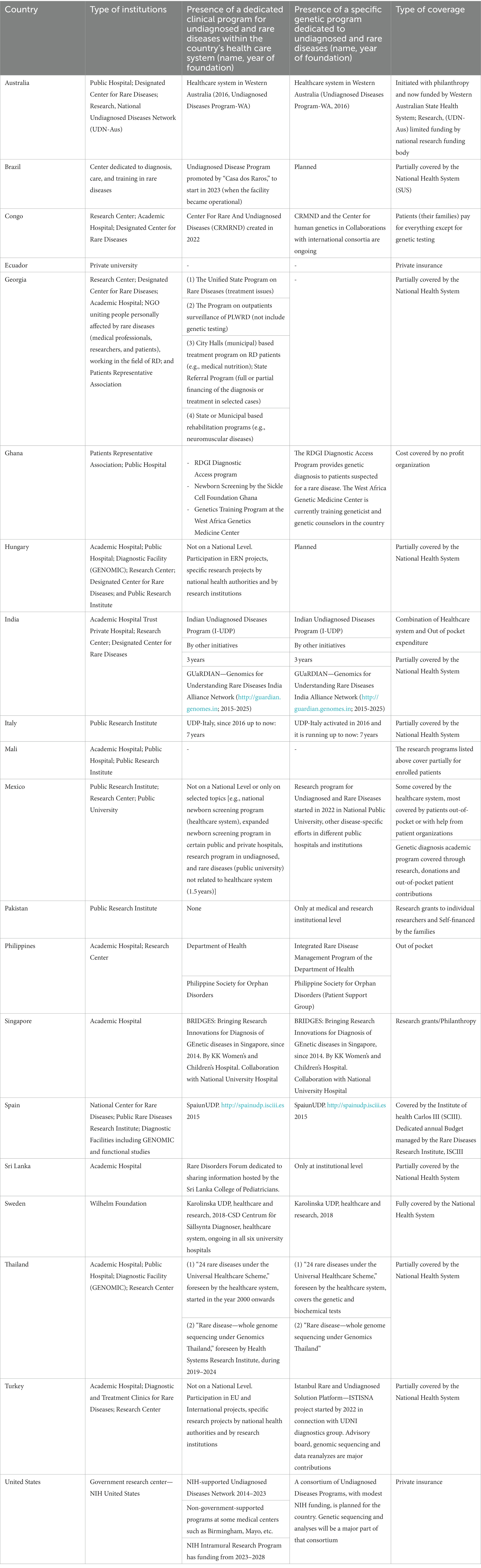
Table 1. Main characteristics of available infrastructures for undiagnosed and rare diseases.
We collected data on the existence of National Rare Disease Policy dedicated to undiagnosed and/or rare diseases, Orphan Drug Acts, National Registries dedicated to undiagnosed and/or rare diseases, and Patient Association programs (Table 2). To improve comparability, the definition of rare disease for each country is also provided. As expected, the organization of health care for RDs and the presence of programs and activities in place vary considerably across countries (Table 3).
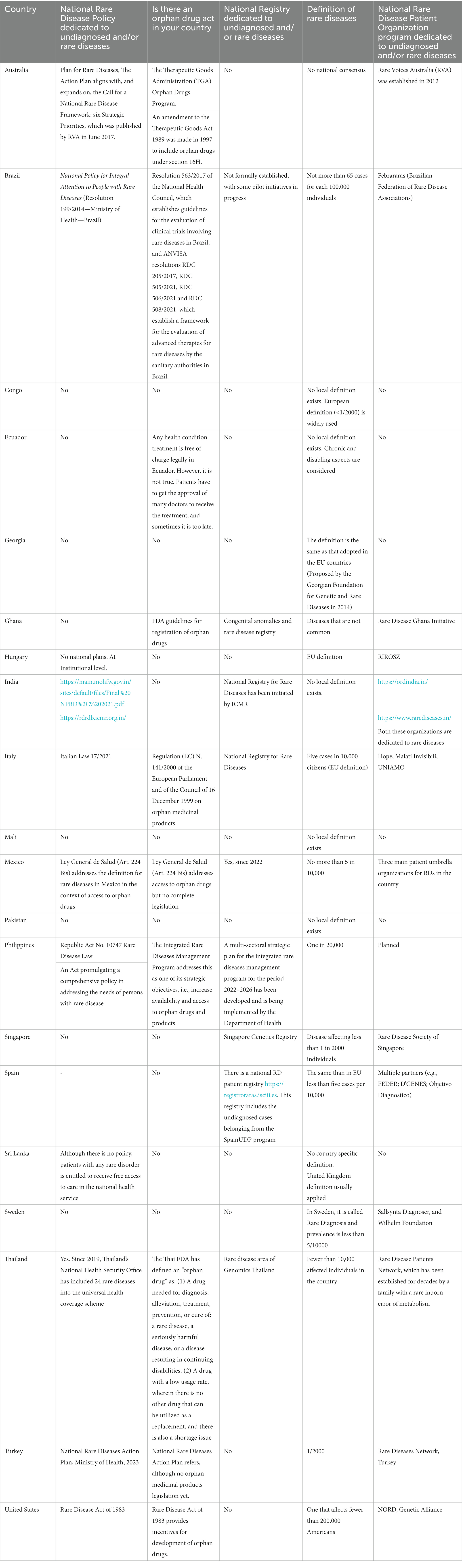
Table 2. Policy aspects related to rare disease.
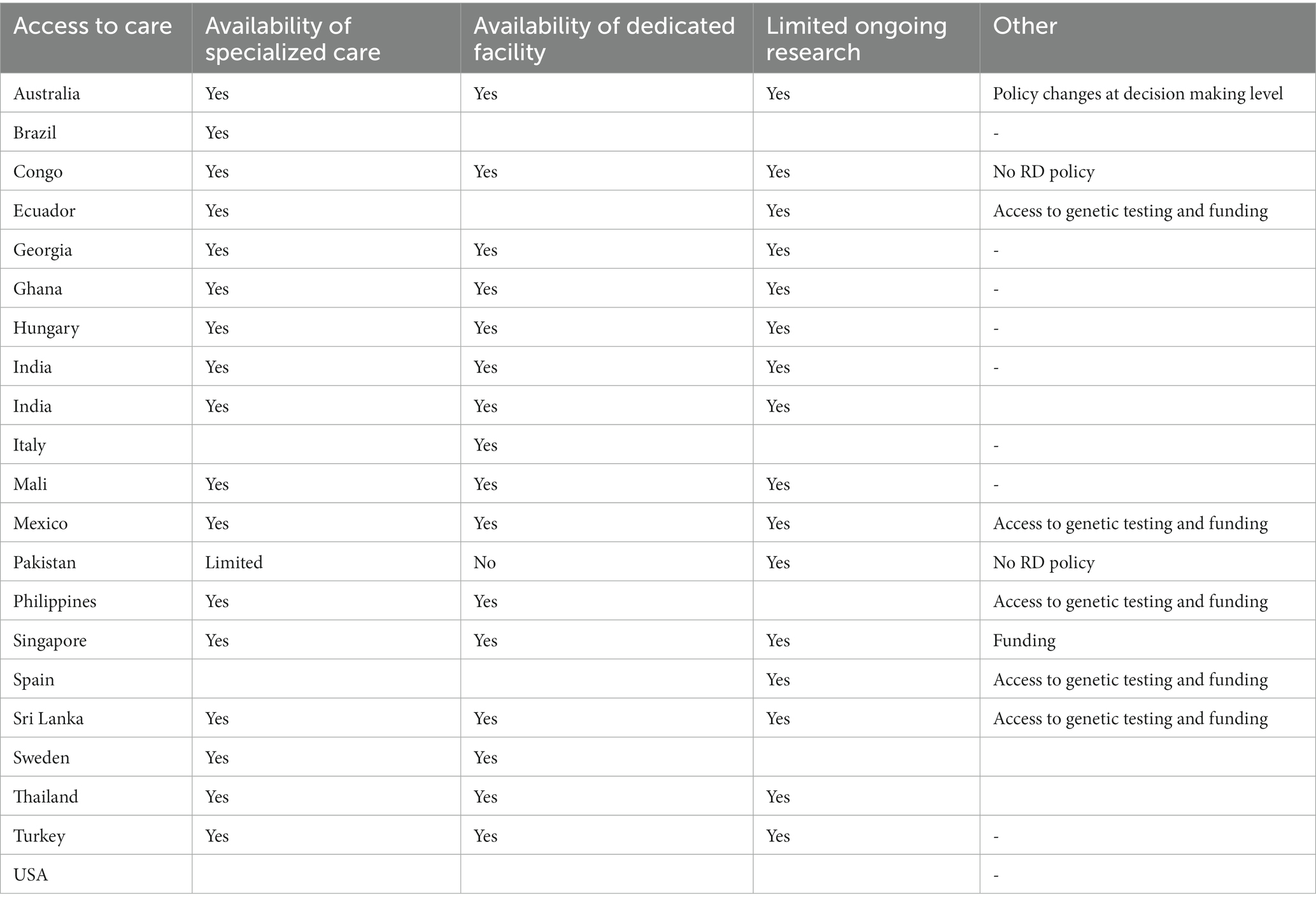
Table 3. Main reported needs for undiagnosed and rare diseases.
When analyzing reported unmet needs, almost all countries (N = 19) indicated that major barriers still exist when attempting to improve the care of patients with rare and/or undiagnosed diseases; most countries report unmet needs related to the availability of specialized care and dedicated facilities (Table 3). Figure 1 shows the unmet needs to tackle undiagnosed patients in different countries divided by World Bank classifications. While the countries ranked as low income by the World Bank showed the highest prevalence of referred unmet needs across the different domains, no specific trend appeared when comparing the high, upper, and low-middle income nations.
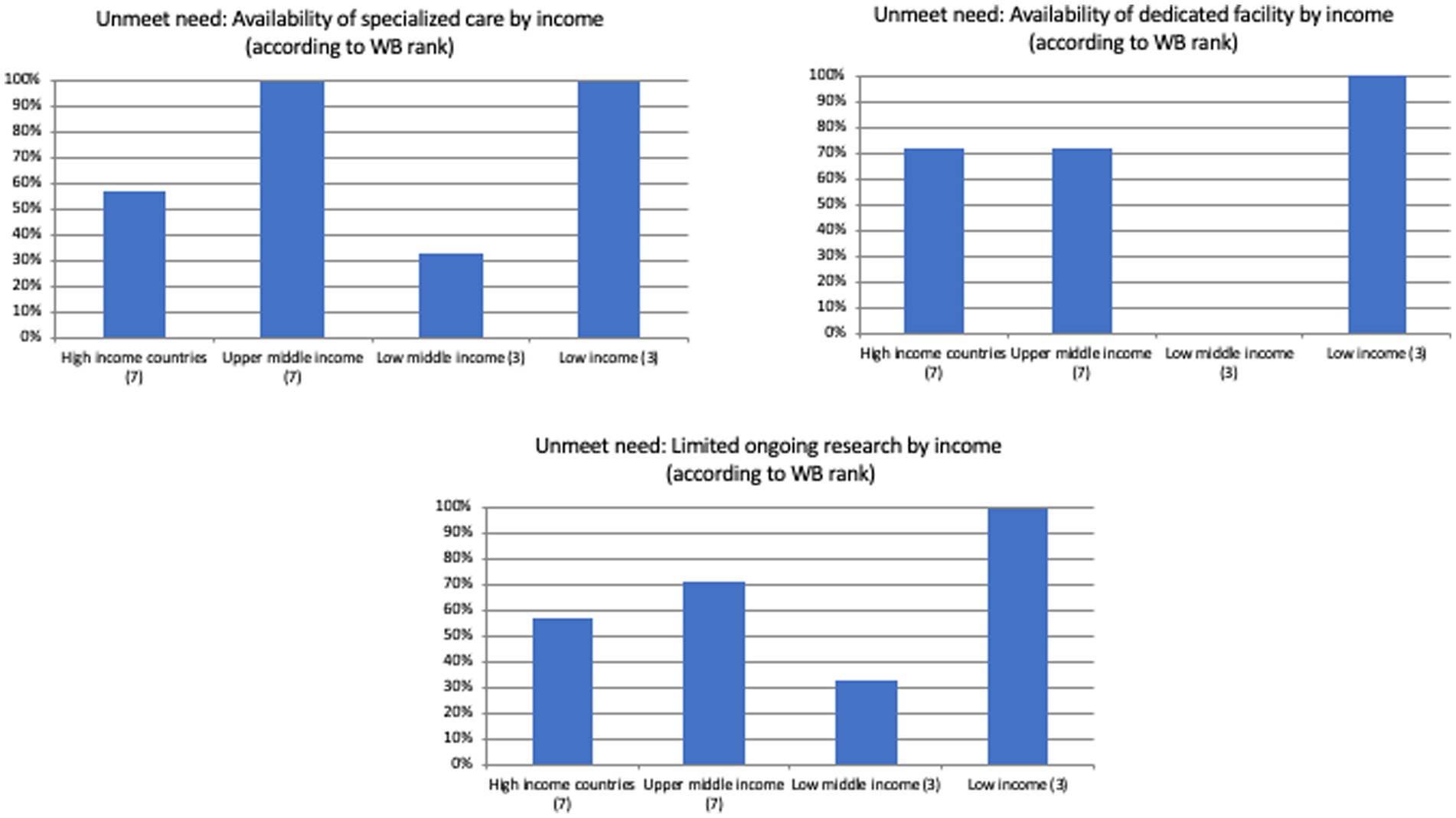
Figure 1. Unmet needs to tackle undiagnosed patients in different countries divided by the World Bank ranking.
Specifically, no overt trend was observed when separating countries by current health expenditure per capita, GDP per capita, domestic general government health expenditure (% of GDP), and life expectancy at birth, total (years; Figures 2–5). However, both the GDP and domestic general government health expenditure for each country impacted the presence of ongoing research in the field of rare and undiagnosed diseases.

Figure 2. Unmet needs to tackle undiagnosed patients in different countries divided by the current health expenditure per capita.
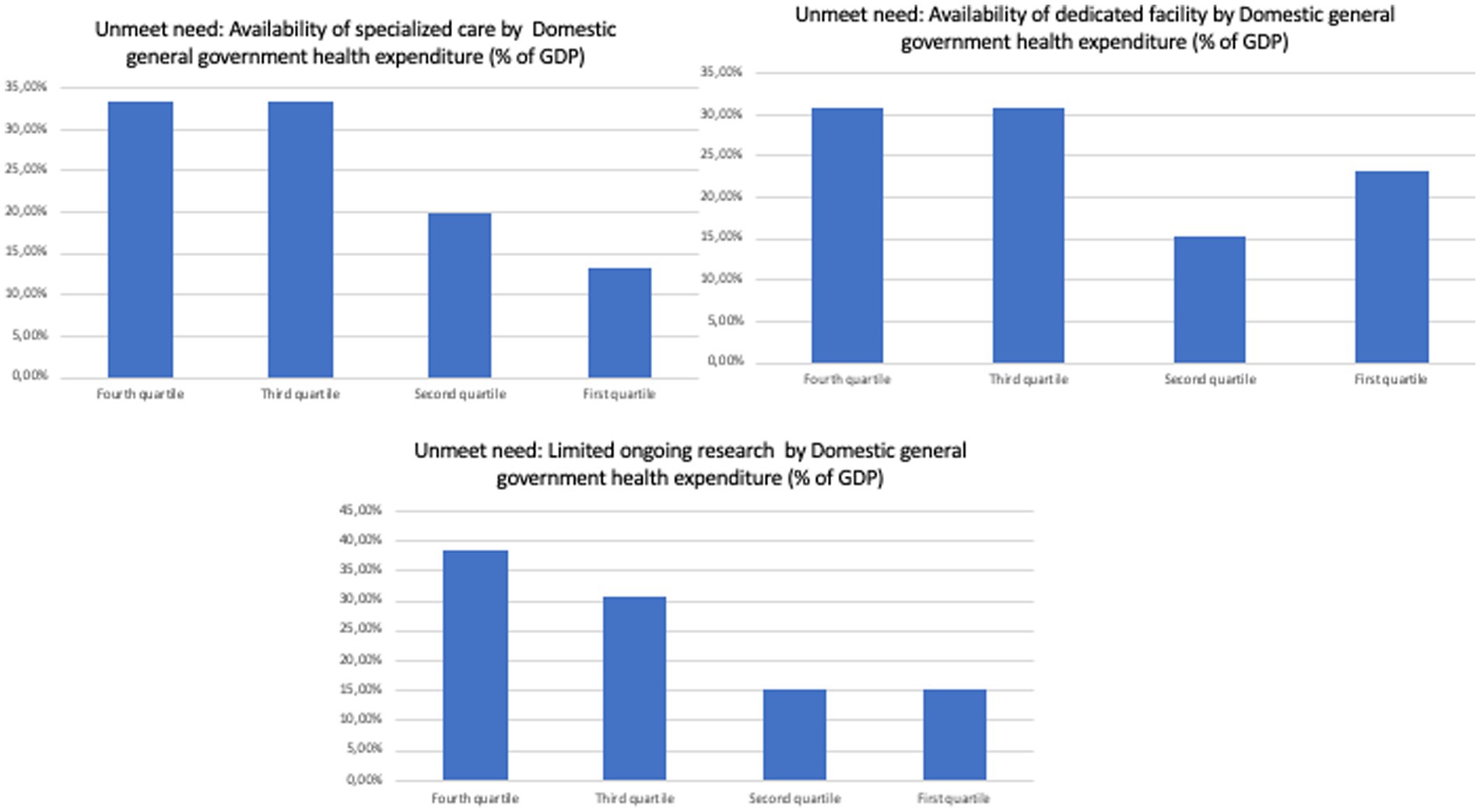
Figure 3. Unmet needs to tackle undiagnosed patients in different countries divided by domestic general government health expenditure (% of GPD).
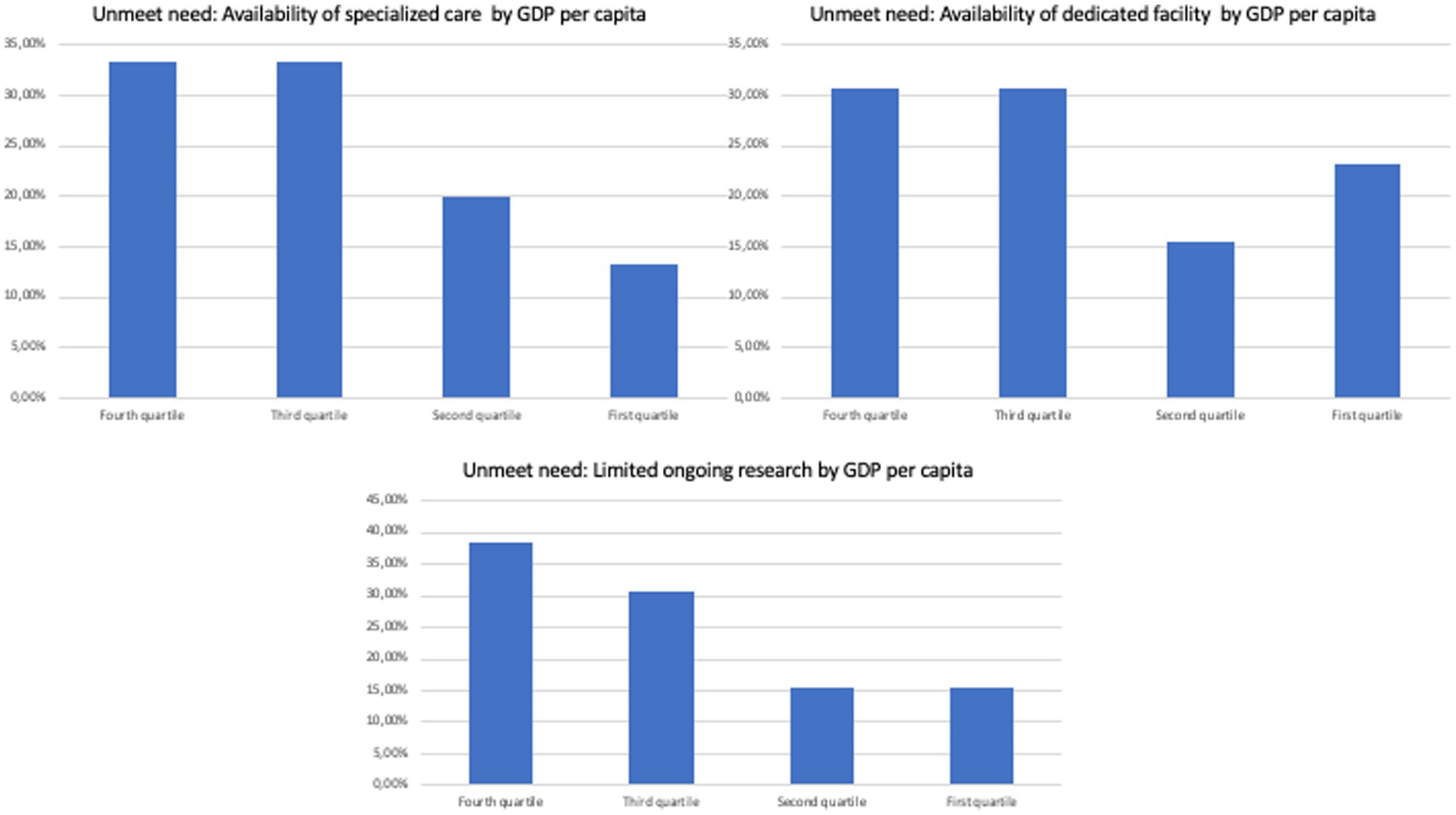
Figure 4. Unmet needs to tackle undiagnosed patients in different countries divided by GPD per capita.
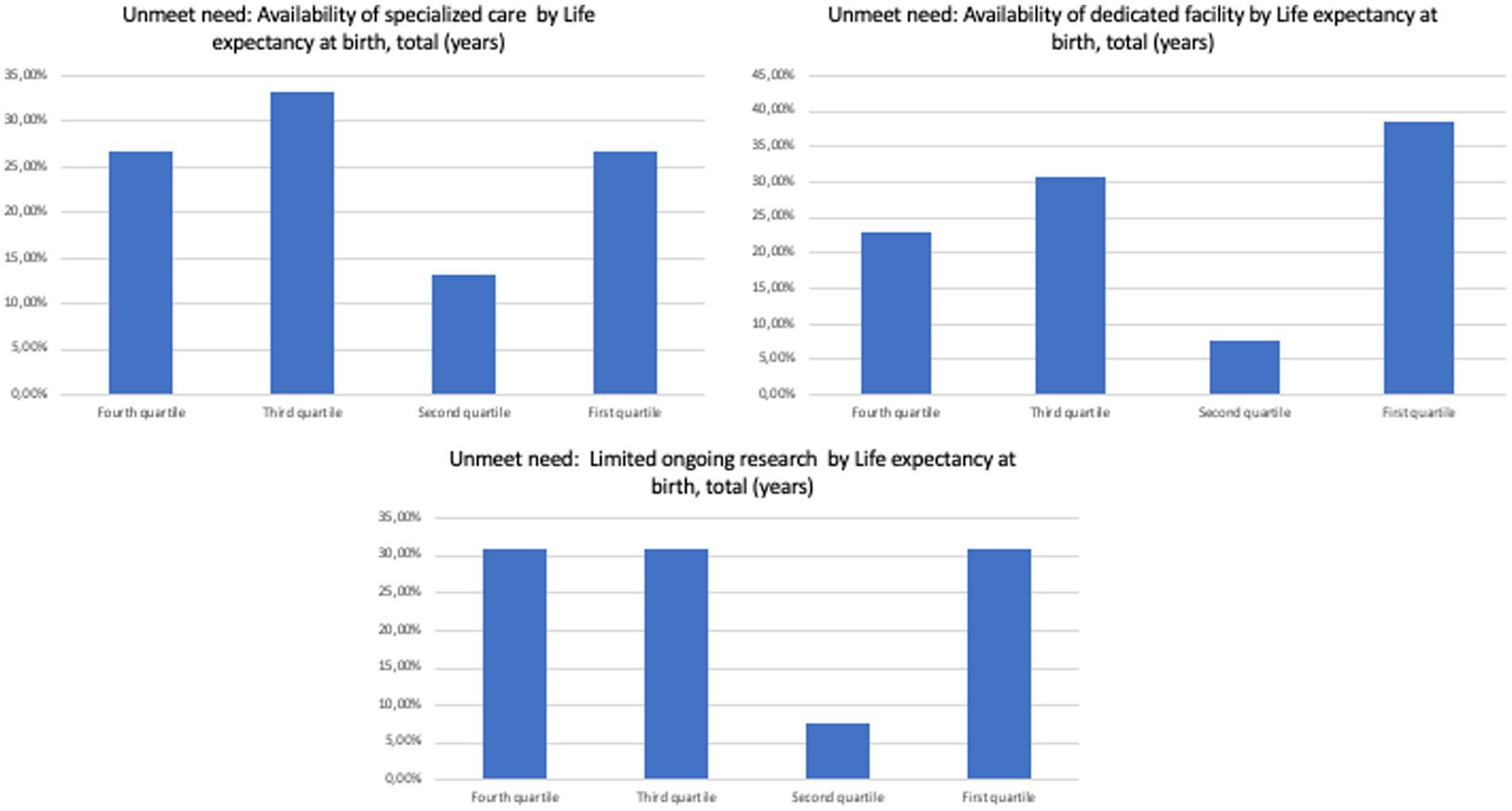
Figure 5. Unmet needs to tackle undiagnosed patients in different countries divided by life expectancy at birth.
This study provides an in-depth evaluation of the unmet needs for 20 countries: low-income (3), middle-income (4), and high-income (5). We found that policy characteristics varied greatly with the type of health system and country. Interestingly, we observed no overall pattern in terms of referral for unmet needs when separating countries by main economic or health indicators were observed. Our analysis is one of the first in its kind, especially when attempting to explore trends in national health care and economic indicators through the lens of URDs across different countries. While the possibility of comparisons with previous studies is limited, the lack of overt trends between the selected indicators and the main reported unmet needs requires further investigations. Indicators such as current health expenditure per capita, GDP per capita, and domestic general government health expenditure (% of GDP) have been associated to trends in health outcomes (e.g., Mortality-to-Incidence Ratio) in different settings, including oncologic and non-communicable diseases (5–8). Conversely, our analysis shows a general agreement in terms of actions needed to foster the care of patients with RD and URDs. This observation supports the concept that the global challenge for the future of rare and undiagnosed diseases includes the identification of actionable points (e.g., implemented orphan drug acts or registries where not available) and this perception is shared across the members of the UNDI participating in this survey.
On the other hand, our analysis suggested that more interest in research in the field in RDs and URDs is reported in countries with higher income. These trends are aligned with those observed in medical research beyond the field of RD, suggesting that higher GDP or government health expenditure might correlate with more medical research activity when evaluated through different outcome measures (e.g., number of published papers, R&D expenditure by sector) (4, 9–12).
Some limitations of our survey include the limited sample size and lack of the ability to perform inference analysis. Similarly, we note that participants in the survey were selected from among members of the UDNI. Further research effort is currently ongoing to expand these aspects.
It should also be considered that, as there are no universal epidemiological criteria for RDs (13), the concept of RD in the current political and legislative framework is closely linked to a definition that may vary across countries. When assessing the population burden of disease, point prevalence is probably the most appropriate indicator for RDs. However, for the purpose of our study, while we cannot exclude a degree of heterogeneity in the applied definitions of RDs in the countries participating in our survey as shown in Table 2, it seems unlikely that these differences might have significantly impacted our observations due to the macrolevel approach of our analysis.
Our analysis also highlighted the heterogeneity in terms of policy for RDs and URDs across countries. A National Rare Disease Policy dedicated to undiagnosed and/or rare diseases is in place in nine out of the 20 countries participating to our survey, an orphan drug act in nine out of 20 and only eight registries have been implemented at national level, albeit with very different characteristics. Conversely, at least half of the participating countries report the presence of one or more patients’ associations supporting people with RDs.
The diagnostic odyssey for rare and undiagnosed disease patients must be shortened, their management must be improved, the morbidity and early mortality of these patients must be decreased, and the socioeconomic potential and quality of life of these patients must all be improved by joint national and international initiatives.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
SS, DR, DT, MS, CC, and LC analyzed the data and were the major contributor in drafting the manuscript. GF, SG, YA, MA, GB, HC, EC, VD, RG, CG-J, DH, OK, GL, PM, BM, UO, RP, VR, VSc, SJ, VSh, WG, SW, OB, AL, and MP carefully revised draft, tables, and figures, and approved final manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Graessner, H, Zurek, B, Hoischen, A, and Beltran, S. Solving the unsolved rare diseases in Europe. Eur J Hum Genet. (2021) 29:1319–20. doi: 10.1038/s41431-021-00924-8
2. Taruscio, D, Groft, SC, Cederroth, H, Melegh, B, Lasko, P, Kosaki, K, et al. Undiagnosed diseases network international (UDNI): white paper for global actions to meet patient needs. Mol Genet Metab. (2015) 116:223–5. doi: 10.1016/j.ymgme.2015.11.003
3. Taruscio, D, Salvatore, M, Lumaka, A, Carta, C, Cellai, LL, Ferrari, G, et al. Undiagnosed diseases: needs and opportunities in 20 countries participating in the undiagnosed diseases network international. Front Public Health. (2023) 11:1079601. doi: 10.3389/fpubh.2023.1079601
4. Pegkas, P, Staikouras, C, and Tsamadias, C. Does research and development expenditure impact innovation? Evidence from the European Union countries. J Policy Model. (2019) 41:1005–25. doi: 10.1016/j.jpolmod.2019.07.001
5. Yang, TW, Wang, CC, Hung, WC, Liu, YH, Sung, WW, and Tsai, MC. Improvement in the mortality-to-incidence ratios for gastric Cancer in developed countries with high health expenditures. Front Public Health. (2021) 9:713895. doi: 10.3389/fpubh.2021.713895
6. Su, CC, Chen, BS, Chen, HH, Sung, WW, Wang, CC, and Tsai, MC. Improved trends in the mortality-to-incidence ratios for liver cancer in countries with high development index and health expenditures. Health. (2023) 11:159. doi: 10.3390/healthcare11020159
7. Dong, C, Fu, JT, Wu, HR, Chao, YC, Chen, YC, Sung, WW, et al. Mortality—to incidence ratio for nasopharyngeal carcinoma is associated with health expenditure. Health. (2022) 10:1615. doi: 10.3390/healthcare10091615
8. Gupta, N, Mocumbi, A, Arwal, SH, Jain, Y, Haileamlak, AM, Memirie, ST, et al. NCDI poverty network secretariat. Prioritizing health-sector interventions for noncommunicable diseases and injuries in low- and lower-middle income countries: national NCDI poverty commissions. Glob Health Sci Pract. (2021) 9:626–39. doi: 10.9745/GHSP-D-21-00035
9. Halpenny, D, Burke, J, McNeill, G, Snow, A, and Torreggiani, WC. Geographic origin of publications in radiological journals as a function of GDP and percentage of GDP spent on research. Acad Radiol. (2010) 17:768–71. doi: 10.1016/j.acra.2010.01.020
10. R&D expenditure (2023). Statistics explained—European Commission. Availabe at: https://ec.europa.eu/eurostat/statisticsexplained/index.php?title=R%26D_expenditure&oldid=551418#R.26D_expenditure_by_sector_of_performance (Accessed August 21, 2023).
11. Meo, SA, Al Masri, AA, Usmani, AM, Memon, AN, and Zaidi, SZ. Impact of GDP, spending on R&D, number of universities and scientific journals on research publications among Asian countries. PLoS One. (2013) 8:e66449. doi: 10.1371/journal.pone.0066449
12. Vinkler, P. Correlation between the structure of scientific research, scientometric indicators and GDP in EU and non-EU countries. Scientometrics. (2008) 74:237–54. doi: 10.1007/s11192-008-0215-z
Keywords: undiagnosed diseases, developing nations, rare diseases, survey, GPD
Citation: Sciascia S, Roccatello D, Salvatore M, Carta C, Cellai LL, Ferrari G, Lumaka A, Groft S, Alanay Y, Azam M, Baynam G, Cederroth H, Cutiongco-de la Paz EM, Dissanayake VHW, Giugliani R, Gonzaga-Jauregui C, Hettiarachchi D, Kvlividze O, Landoure G, Makay P, Melegh B, Ozbek U, Puri RD, Romero VI, Scaria V, Jamuar SS, Shotelersuk V, Gahl WA, Wiafe SA, Bodamer O, Posada M and Taruscio D (2023) Unmet needs in countries participating in the undiagnosed diseases network international: an international survey considering national health care and economic indicators. Front. Public Health. 11:1248260. doi: 10.3389/fpubh.2023.1248260
Edited by:
Eleonora Hristova-Atanasova, Medical University of Plovdiv, BulgariaReviewed by:
Kang Qi, Shanghai Health Development Research Center, ChinaCopyright © 2023 Sciascia, Roccatello, Salvatore, Carta, Cellai, Ferrari, Lumaka, Groft, Alanay, Azam, Baynam, Cederroth, Cutiongco-de la Paz, Dissanayake, Giugliani, Gonzaga-Jauregui, Hettiarachchi, Kvlividze, Landoure, Makay, Melegh, Ozbek, Puri, Romero, Scaria, Jamuar, Shotelersuk, Gahl, Wiafe, Bodamer, Posada and Taruscio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Domenica Taruscio, ZG9tZW5pY2EudGFydXNjaW9AaXNzLml0
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.