 Qianqian Wu1
Qianqian Wu1 Aiping Chi
Aiping Chi
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health , 19 December 2023
Sec. Public Mental Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1243213
Purposes: A meta-analysis was conducted to examine the differences in heart rate variability (HRV) between depressed patients and healthy individuals, with the purpose of providing a theoretical basis for the diagnosis of depression and the prevention of cardiovascular diseases.
Methods: To search China National Knowledge Infrastructure (CNKI), WanFang, VIP, PubMed, Web of Science, Science Direct, and Cochrane Library databases to collect case–control studies on HRV in depressed patients, the retrieval date is from the establishment of the database to December 2022. Effective Public Health Practice Project (EPHPP) scale was used to evaluate literature quality, and Stata14.0 software was used for meta-analysis.
Results: This study comprised of 43 papers, 22 written in Chinese and 21 in English, that included 2,359 subjects in the depression group and 3,547 in the healthy control group. Meta-analysis results showed that compared with the healthy control group, patients with depression had lower SDNN [Hedges’ g = −0.87, 95% CI (−1.14, −0.60), Z = −6.254, p < 0.01], RMSSD [Hedges’ g = −0.51, 95% CI (−0.69,-0.33), Z = −5.525, p < 0.01], PNN50 [Hedges’ g = −0.43, 95% CI (−0.59, −0.27), Z = −5.245, p < 0.01], LF [Hedges’ g = −0.34, 95% CI (−0.55, − 0.13), Z = −3.104, p < 0.01], and HF [Hedges’ g = −0.51, 95% CI (−0.69, −0.33), Z = −5.669 p < 0.01], and LF/HF [Hedges’ g = −0.05, 95% CI (−0.27, 0.18), Z = −0.410, p = 0.682] showed no significant difference.
Conclusion: This research revealed that HRV measures of depressed individuals were lower than those of the healthy population, except for LF/HF, suggesting that people with depression may be more at risk of cardiovascular diseases than the healthy population.
Depression is a mental health condition characterized by prolonged feelings of sadness and lack of interest in activities. People suffering from this disorder may have decreased appetite, be unresponsive, experience physical discomfort and even thoughts of suicide (1). With the world advancing, the rate of depression has been on the rise, with 11.7% of people in China estimated to be affected (2). By the year 2020, depression had become the second most widespread medical condition globally (3). Besides causing certain shared symptomatic responses, depression may also affect the autonomic performance of the heart (4).
Heart rate variability (HRV), which refers to the magnitude of the difference in fluctuations between adjacent R-R intervals, is a noninvasive monitoring tool that can be used to assess the balance of sympathetic and vagal tone and autonomic activity in the heart (5). The combination of the sympathetic and parasympathetic nervous systems is essential for the maintenance of the autonomic balance of the heart, and if this balance is disrupted, HRV can be used to measure the degree of pathology (6). The SDNN index is deemed the “gold standard” for predicting the gravity of cardiac diseases and mortality rates (7), and it is feasible to evaluate an individual’s well-being through prolonged testing of the SDNN index (8); RMSSD is indicative of alterations mediated by the vagus nerve; PNN50 is strongly associated with vagal nerve activity; The frequency domain index LF is thought to mirror the equilibrium between sympathetic and vagal nerves; HF is affected by respiratory regulation and may be indicative of parasympathetic activity and vagal function; Whether LF/HF is a reliable indicator of the balance between sympathetic and vagal nerves is still a matter of debate. Depression is a potential risk factor of cardiovascular disease, and the autonomous nervous system is believed to be connected to a wide range of physical and mental conditions.
Research has indicated that there is a significant link between HRV and cardiovascular disorders, such as coronary heart disease and heart failure. Furthermore, a decrease in HRV is usually a sign of damage to the autonomic nervous system (9). Compared to healthy individuals, those suffering from depression have a greater risk of developing cardiovascular diseases, and those with CVD are more likely to experience depression than those without, forming a two-way relationship between depression and CVD (10). Due to the fact that HRV contains a wealth of data concerning cardiovascular regulation, it can be utilized to effectively monitor the cardiovascular functioning of individuals suffering from depression. In this study, we conducted a meta-analysis of published controlled experiments on HRV in depressed patients and healthy subjects in order to gain a better understanding of the changes in HRV in depressed patients via a systematic analysis, which is anticipated to provide an objective foundation for the diagnosis and treatment of depressed patients and the prevention of cardiovascular diseases.
This systematic review was conducted according to the Preferred Reporting of Systematic Reviews and Meta Analyses (PRISMA) guidelines (11). In this paper, two researchers searched PubMed, Science Direct, Web Of Science, Cochrane, CNKI, WanFang, and VIP databases by computer, using a mixed search of subject terms and free words in English and Chinese, and the search terms were mainly (Depression or Depression or Depressive Symptoms or Depressive Symptom or Symptom, Depressive or Emotional Depression or Depression, Emotional) and (Heart Rate Variability or HRV or autonomic nervous system or cycle length variability or RR variability or heart period variability or vagal or ANS). To make the search more comprehensive, we also performed a manual search from published meta-analyses to literature reviews. The search was conducted from the date of database creation to December, 2022. Take PubMed as an example, its specific search strategy was ((“Depression”[Mesh]) OR (((((Depressive Symptoms [Title/Abstract]) OR (Depressive Symptom [Title/Abstract])) OR (Symptom, Depressive [Title/Abstract])) OR (Emotional Depression [Title/Abstract])) OR (Depression, Emotional [Title/Abstract]))) AND (((((((Heart Rate Variability [Title/Abstract]) OR (HRV [Title/Abstract])) OR (autonomic nervous system [Title/Abstract] OR cycle length variability [Title/Abstract])) OR (RR variability [Title/Abstract])) OR (heart period variability [Title/Abstract])) OR (vagal [Title/Abstract])) OR (ANS [Title/Abstract])).
Two pre-trained researchers independently conducted a literature screening process, adhering to the inclusion and exclusion criteria, and then combined the chosen literature. In the event of conflicting conclusions between the two researchers, the discrepancies were initially addressed through dialog, and if the disagreement persisted, a third-party specialist was consulted to make a final decision, ensuring agreement was reached prior to inclusion. According to PICOS, that is, the study population, intervention, comparison, outcome and study design were used for literature screening.
Inclusion criteria: (1) published journals, conference papers, and dissertations at home and abroad; (2) the experimental group was patients who met the assessment criteria of the depression scale or had been clinically diagnosed with depression, and the control group was the healthy general population; (3) the study type was a controlled trial; (4) the outcome indicators were SDNN, RMSSD, and PNN50 in the time domain, and LF, HF, and LF/HF in the frequency domain.
Exclusion criteria: (1) Exclusion of review articles, animal experiment articles, and articles where full text and outcome indicators were not available; (2) Exclusion of articles with depression co-morbidities such as diabetes, hypertension, heart disease, and other serious physical diseases; (3) Excluded patients who had taken antidepressants or medications that affected heart rate in the recent past.
Researchers conducted a thorough search of each database, applied the inclusion and exclusion criteria to the literature, and then summarized the findings. In the event of any discrepancies, these were discussed and resolved. If the problem still could not be solved, the third-party experts would make a ruling, and the inclusion could only be reached by consensus. The content of literature data extraction mainly includes: (1) general characteristics of literature (first author, publication year, country); (2) Characteristics of subjects (gender, age, sample size, diagnostic scale, etc.); (3) The mean and standard deviation of each outcome index.
This research has made Effective Public Health Practice Project (EPHPP) scale was biased risk assessment (12). The scale included evaluations of selection bias, study design, confounding factors, blinding, data collection, and inclusion and exclusion, each rated as weak, medium, and strong. According to the number of sub-items rated as weak, the overall evaluation is divided into three levels: strong (no weak items), medium (1 weak item), and weak (2 or more weak items). The retrieval, inclusion and quality evaluation of the literature are carried out by two authors, who discuss the results of the operation and make a decision. If no consensus can be reached through discussion, the results will be submitted to the third author for consultation before making a decision.
Data were statistically analyzed using Stata14.0 software, and effect sizes were calculated using mean and standard variance (Mean ± SD). The effect size employed was Hedges’ g, which is a modification of Cohen’s d to account for a small sample size. A Hedges’ g value of 0.2 ~ 0.5 indicates a low effect, 0.5 ~ 0.8 indicates moderate effect, and greater than 0.8 indicates significant effect. Although the people included in this study were patients with depression, there were many types of depression, which were not subdivided in this study, so we chose the random effects model. Q test was used to examine the heterogeneity among the included references. In Q test, when p < 0.01, the heterogeneity was considered significant (13). However, since Q value cannot judge the degree of heterogeneity among studies, I2 is further used to describe the proportion of variance between studies in the total variance. According to Cochrane systematic reviews, heterogeneity among studies can be ignored when I2 is less than 50%. If I2 is greater than 50%, heterogeneity between studies cannot be ignored (14). Subgroup analysis was used to explore the source of heterogeneity. Sensitivity analysis was carried out to check the stability of the results by using the one-by-one elimination method and model transformation. Publication bias was evaluated by Egger test and funnel plot. If there was publication bias, the effect value was corrected by non-parametric trim and fill procedure.
A total of 25,957 articles were retrieved through PubMed, Science Direct, Web Of Science, Cochrane, CNKI, WanFang, and VIP databases. Following the removal of duplicate published literature, 15,683 articles were obtained; upon preliminary reading of titles and abstracts, 1,295 articles were retained after the exclusion of reviews, policy research, results category, less relevant research and inaccessible articles. Moreover, through reading the full text to discard any unqualified literature, 43 references were included. The literature screening process is illustrated in Figure 1.
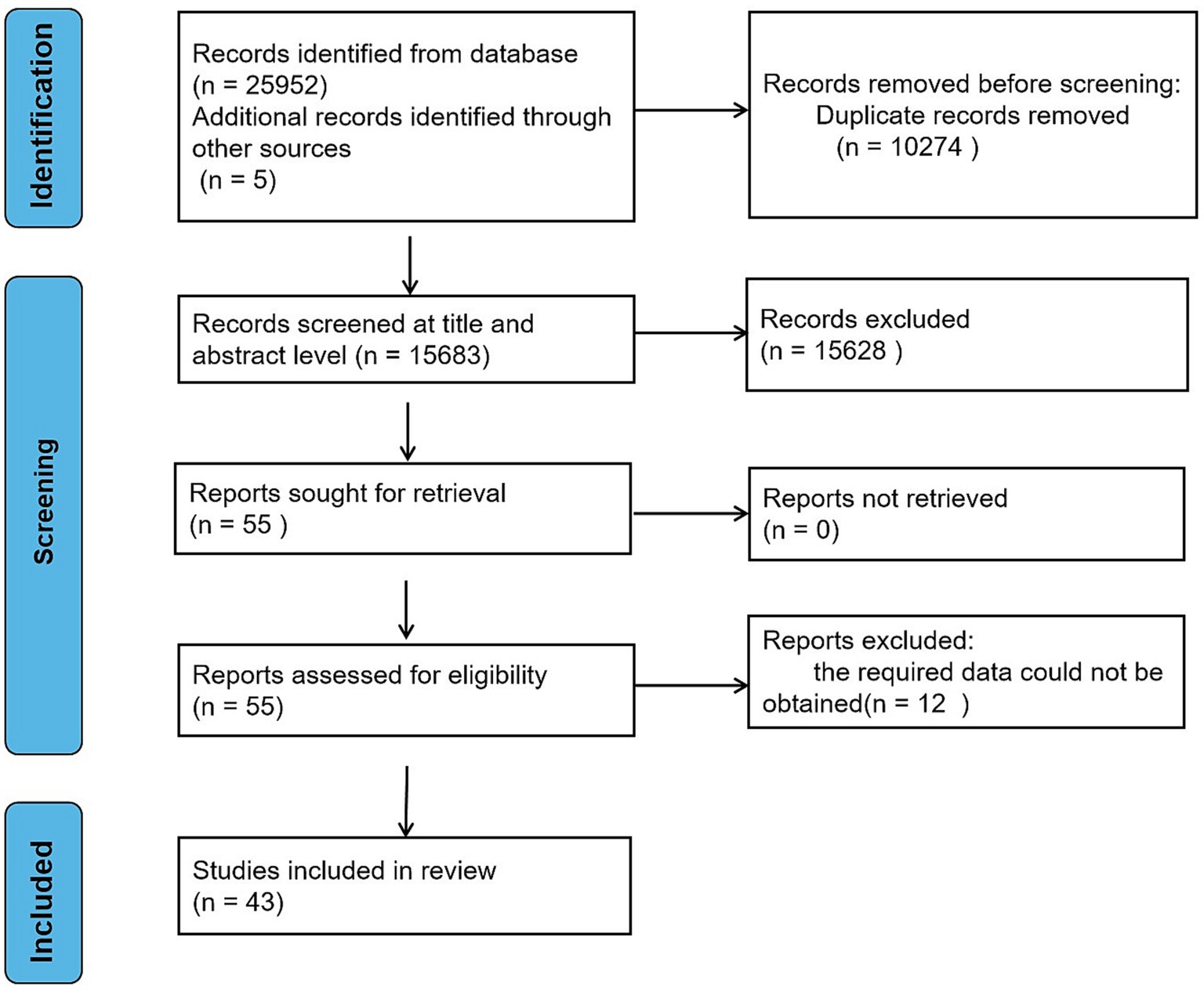
Figure 1. Flow chart of literature search.
The basic information of all included literature was shown in Table 1, a total of 43 papers were included, 22 (15–36) in Chinese and 21 (37–54) in English. However, 24 (15–36, 42, 51) of the studies involved Chinese people, and 19 (37–41, 43–50, 52–54) involved participants from countries other than China. Among them, 2,359 were in the depression group and 3,547 were in the healthy control group, and the years of publication were between 2000 and 2021. 26 (15–20, 22–37, 42, 44, 45, 47, 55) studies reported the outcome indicator SDNN. 28 (15–26, 28, 29, 31, 33–35, 38, 40–42, 44, 45, 47, 49, 50, 52, 55) studies reported the outcome indicator RMSSD. 13 (14, 15, 22, 25–27, 29, 31, 33–35, 42, 48, 50) studies reported the outcome indicator PNN50. The outcome indicator LF was reported in 27 (15, 17–23, 27, 29–32, 34, 35, 38, 39, 42, 43, 45, 48, 50, 51, 54, 56) studies. 31 (15, 17–23, 27, 29–32, 34, 38–43, 45–51, 54–56) studies reported the outcome indicator HF. 31 (15, 17–19, 21–24, 28–32, 34–36, 38–46, 48–57) studies reported the outcome indicator LF/HF. The overall quality of two (26, 33) of the articles was weak, and the overall quality of the others was moderate (15–27, 29–34, 36–57).
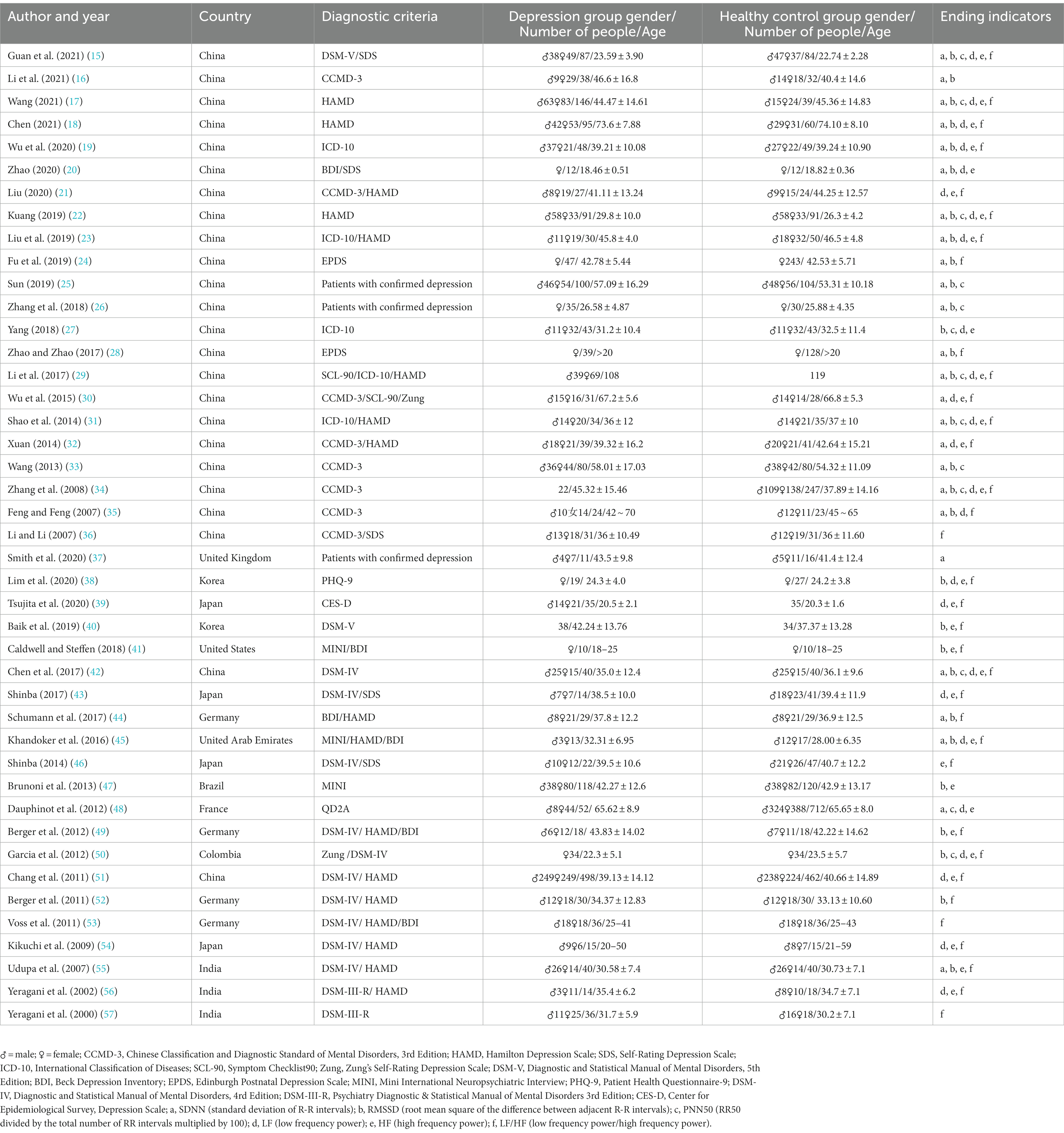
Table 1. Basic information of the included literature.
The results of the risk of bias assessment are shown in Table 2.
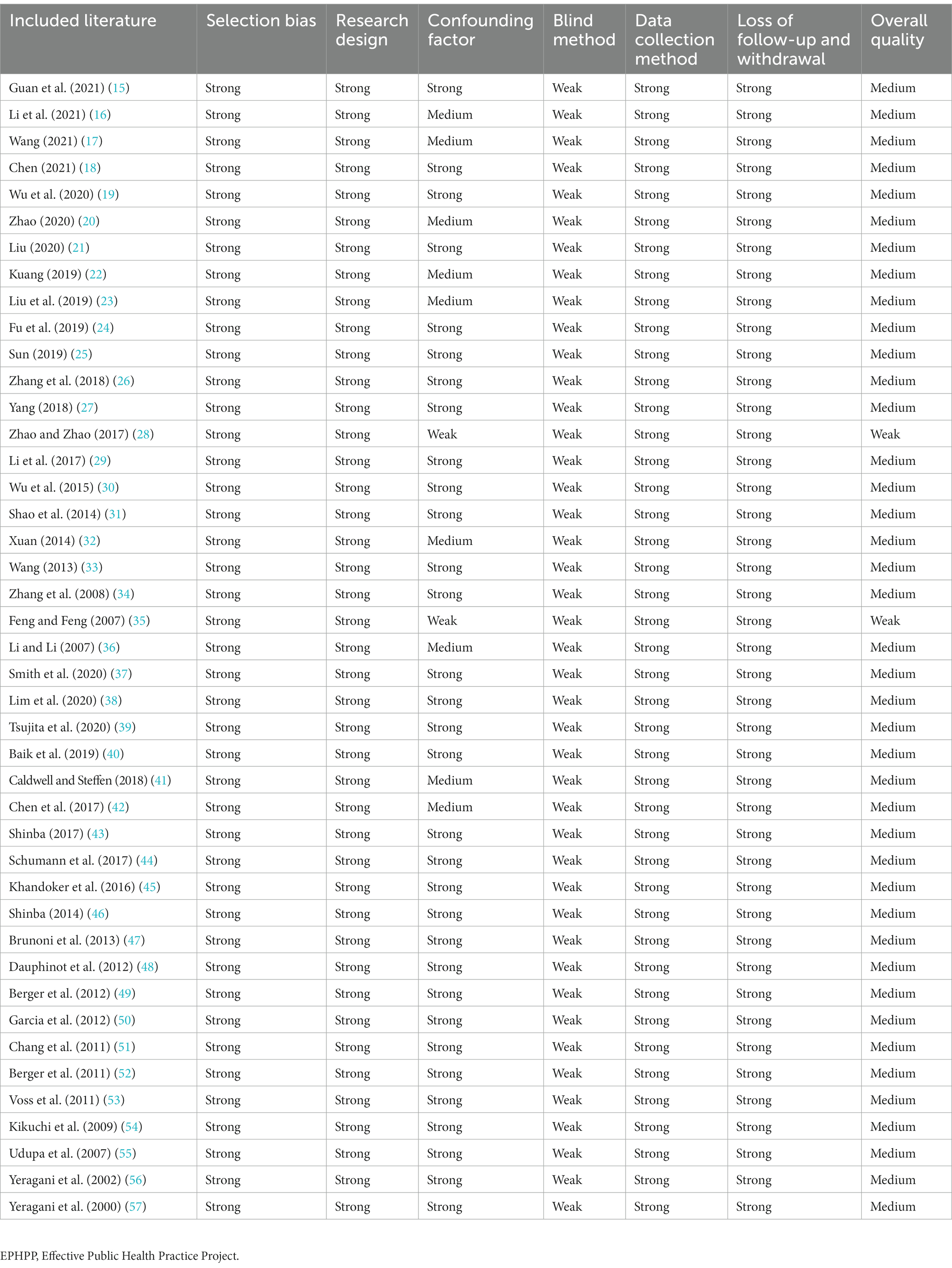
Table 2. Quality assessment of included studies according to the EPHPP.
The random effects model was used for meta-analysis of outcome index SDNN. Heterogeneity test results showed: Q25 = 270.84, p < 0.001, I2 = 90.8%, the heterogeneity between the studies was significant. Combined effect size: Hedges’ g = −0.87, 95% CI (−1.14, −0.60), Z = −6.254, p < 0.001. The effect size was large. The forest plot (Figure 2) showed that the horizontal line of the 95% CI for the indicator Hedges’ g was to the left of the null line for the depressed and healthy control groups, indicating that the SDNN was significantly lower in the depressed group compared to the healthy control group.
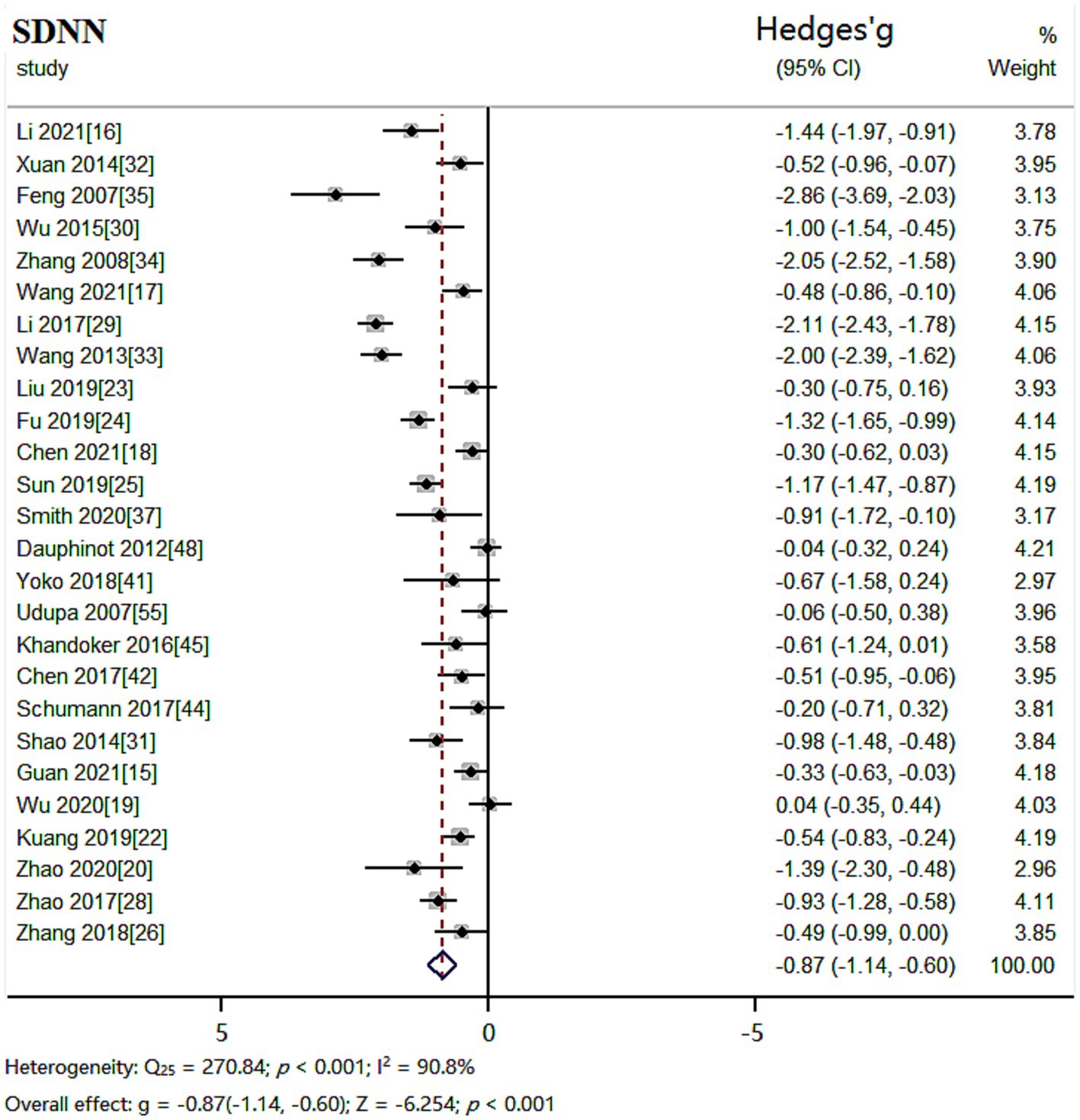
Figure 2. Meta-analysis forest plot of indicator SDNN.
The random effects model was used for meta-analysis of outcome index RMSSD. Heterogeneity test results showed: Q27 = 151.63, p < 0.001, I2 = 82.2%, the heterogeneity between the studies was significant. Combined effect size: Hedges’ g = −0.51, 95% CI (−0.69, −0.33), Z = −5.525, p < 0.001. The effect size was moderate. The forest plot showed (Figure 3) that the horizontal line of the 95% CI for the indicator Hedges’ g was to the left of the null line in the depressed and healthy control groups, indicating a significantly lower RMSSD in the depressed group compared to the healthy control group.
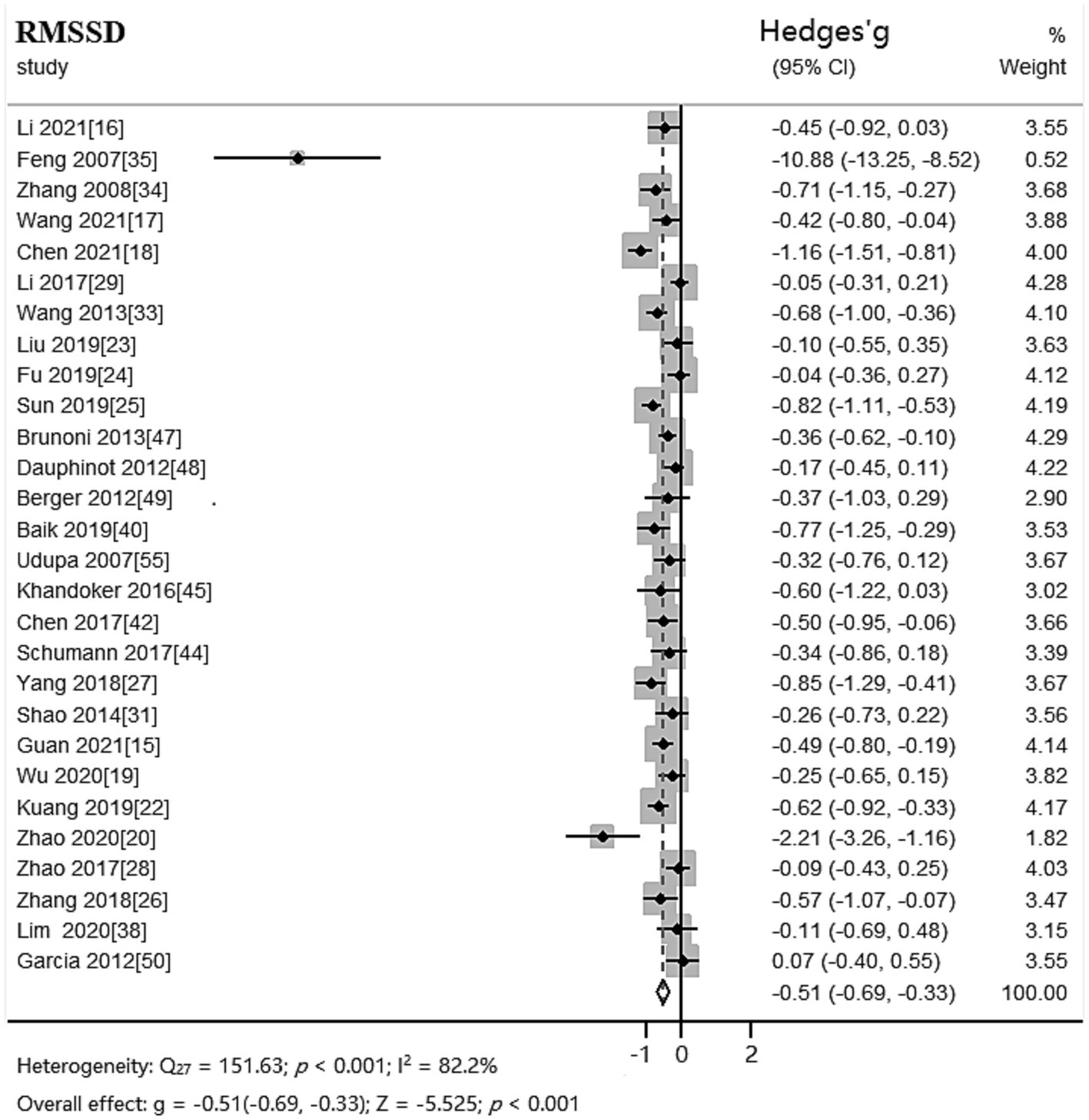
Figure 3. Meta-analysis forest plot of indicator RMSSD.
The random effects model was used for meta-analysis of outcome index PNN50. Heterogeneity test results showed: Q12 = 31.13, p = 0.002, I2 = 61.4%, the heterogeneity between the studies was significant. Combined effect size: Hedges’ g = −0.43, 95% CI (−0.59, −0.27), Z = −5.245, p < 0.001. The effect size was small. The forest plot showed (Figure 4) that the horizontal line of the 95% CI for the indicator Hedges’ g was to the left of the null line for the depressed and healthy control groups, indicating that the PNN50 was significantly lower in the depressed group compared to the healthy control group.
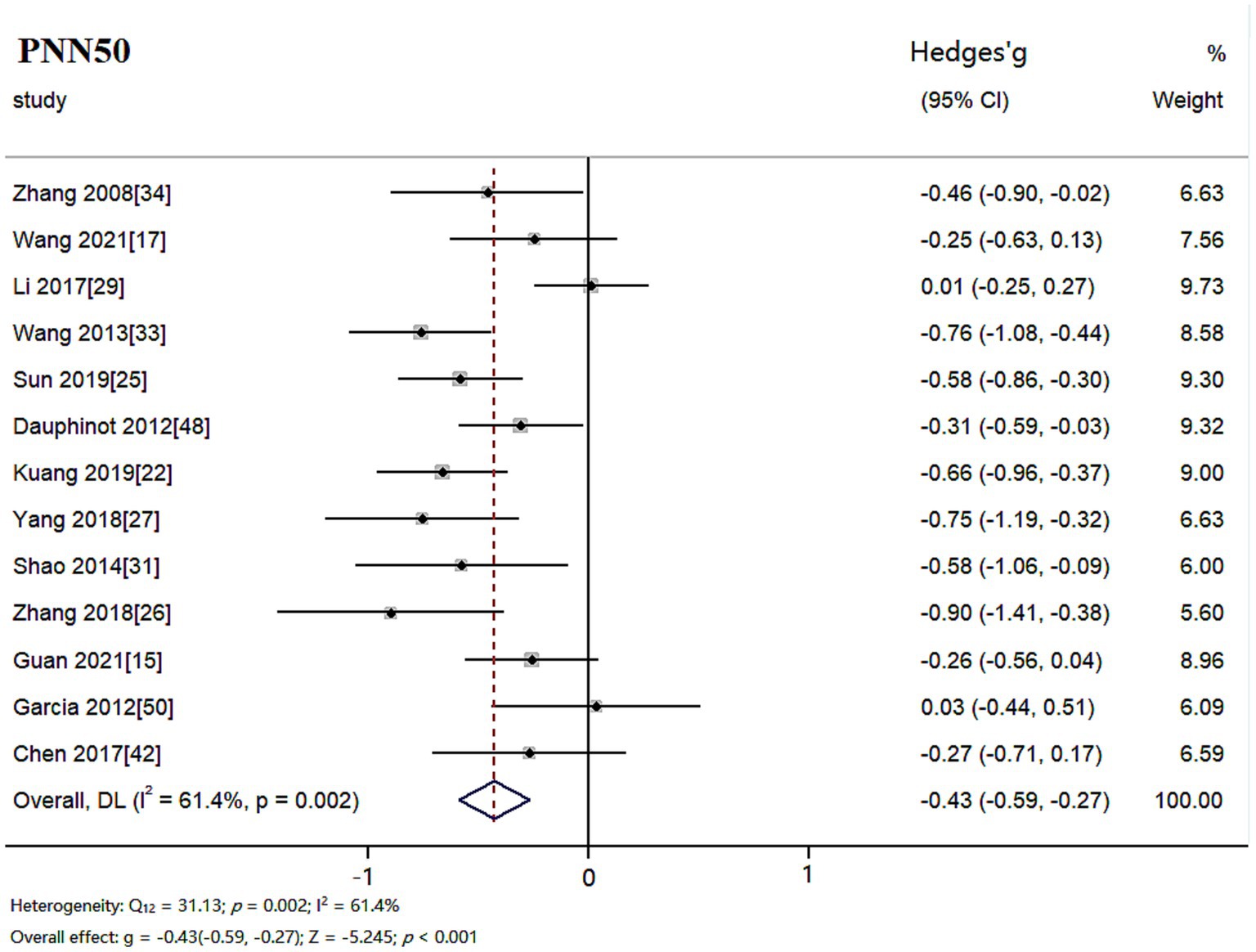
Figure 4. Meta-analysis forest plot of indicator PNN50.
The random effects model was used for meta-analysis of outcome index LF. Heterogeneity test results showed: Q26 = 181.54, p < 0.001 and I2 = 85.7%, the heterogeneity between the studies was significant. Combined effect size: Hedges’ g = −0.34, 95% CI (−0.55, −0.13), Z = −3.104, p = 0.002. The effect size was small. The forest plot showed (Figure 5) that the horizontal line of the 95% CI for the indicator Hedges’ g was to the left of the null line in the depressed and healthy control groups, indicating that LF was significantly lower in the depressed group compared to the healthy control group.
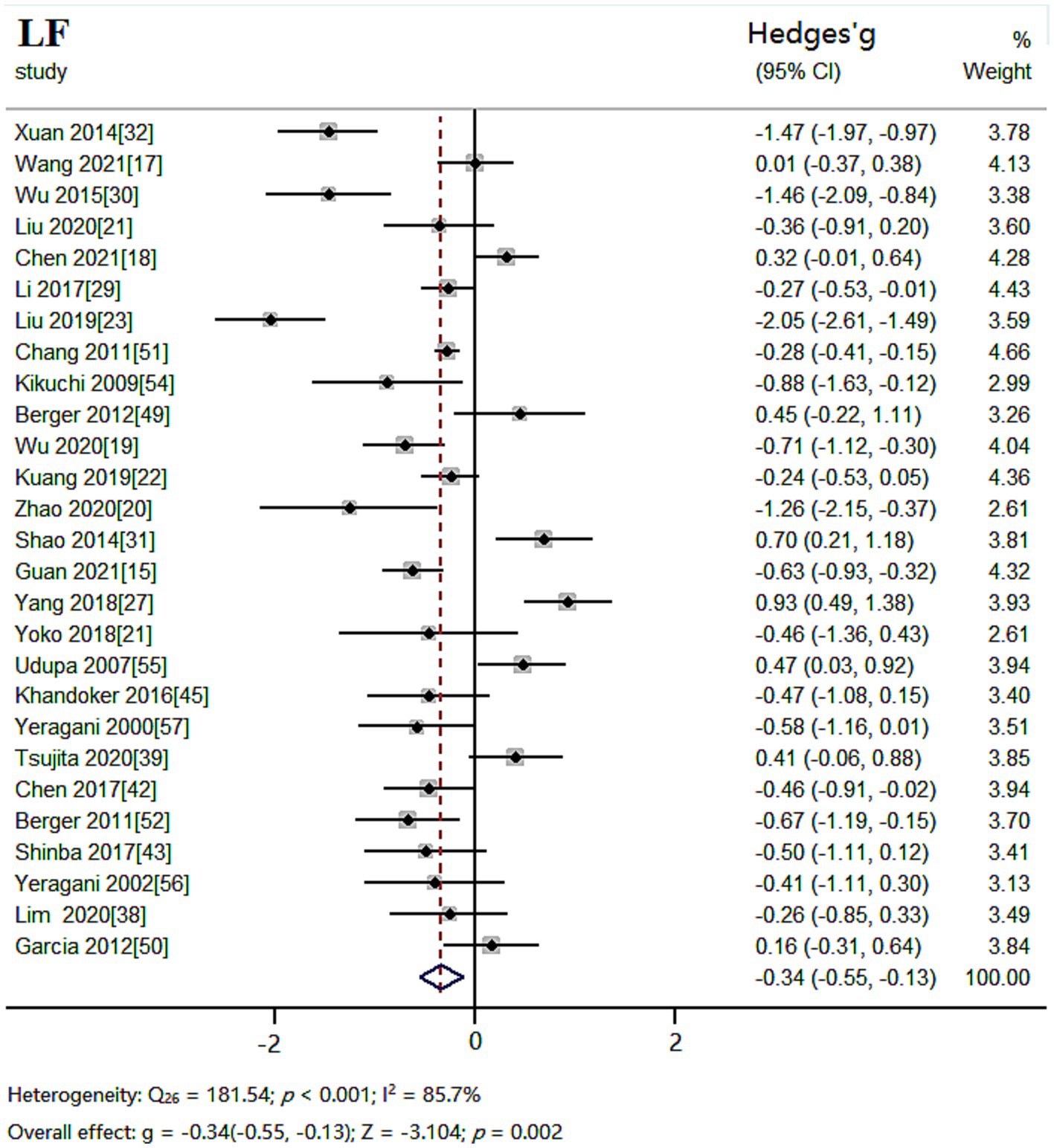
Figure 5. Meta-analysis forest plot of indicator LF.
The random effects model was used for meta-analysis of outcome index HF. Heterogeneity test results showed: Q30 = 170.96, p < 0.001, I2 = 82.5%, the heterogeneity between the studies was significant. Combined effect size: Hedges’ g = −0.51, 95% CI (−0.69, −0.33), Z = −5.669, p < 0.001. The effect size was moderate. The forest plot showed (Figure 6) that the horizontal line of the 95% CI for the indicator Hedges’ g was to the left of the null line in the depressed and healthy control groups, indicating that HF was significantly lower in the depressed group compared to the healthy control group.
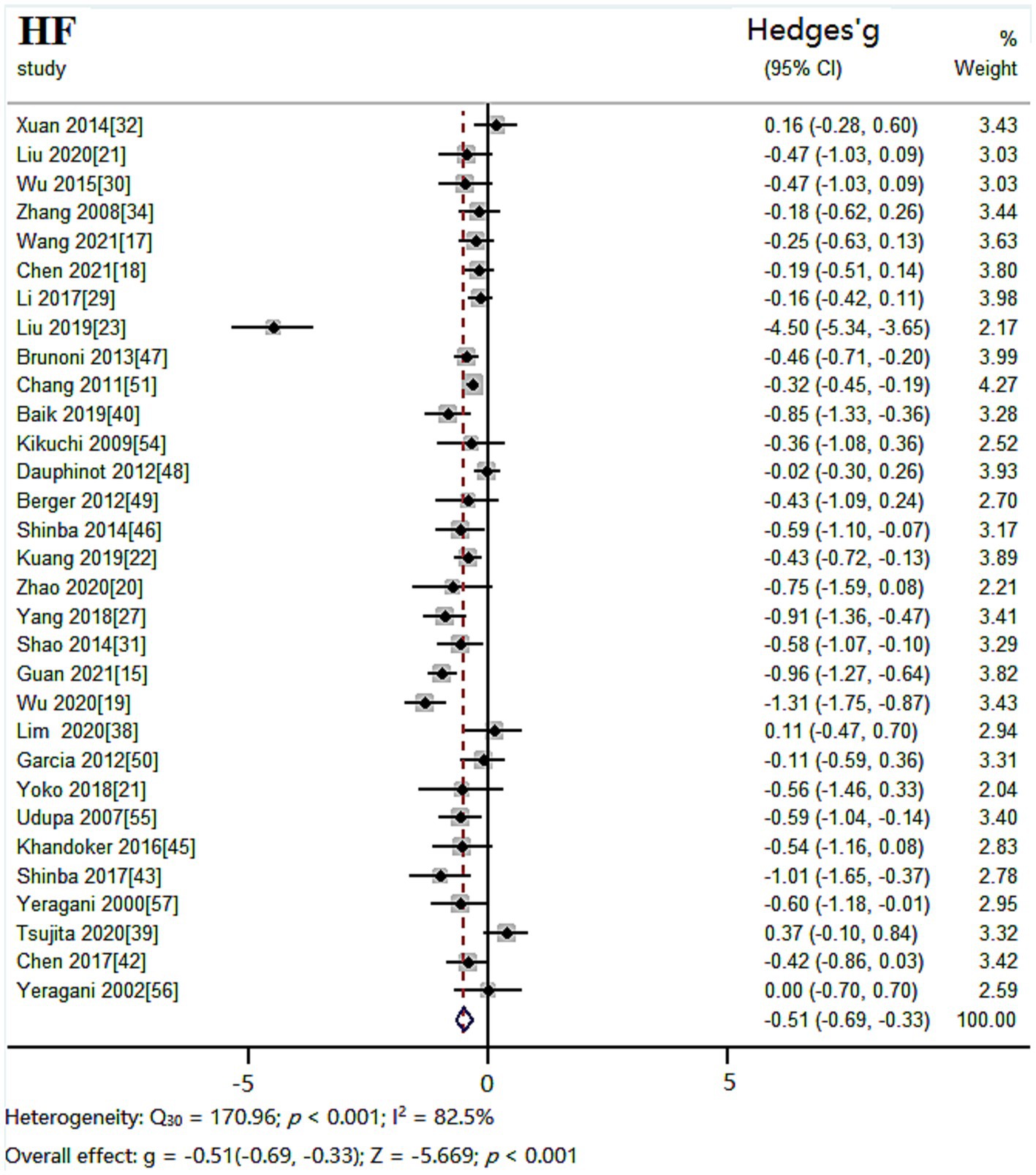
Figure 6. Meta-analysis forest plot of indicator HF.
The random effects model was used for meta-analysis of outcome index LF/HF. Heterogeneity test results showed: Q30 = 266.69, p < 0.001, I2 = 88.8%. Combined effect size: Hedges’ g = −0.05, 95% CI (−0.27,0.18), Z = −0.410, p = 0.682. The effect size was very small. The forest plot showed (Figure 7) that the 95% CI horizontal line for the indicator Hedges’ g between the depressed and healthy control groups was in the center of the null line, indicating that there was no significant difference between LF/HF in the depressed group compared to the healthy control group.
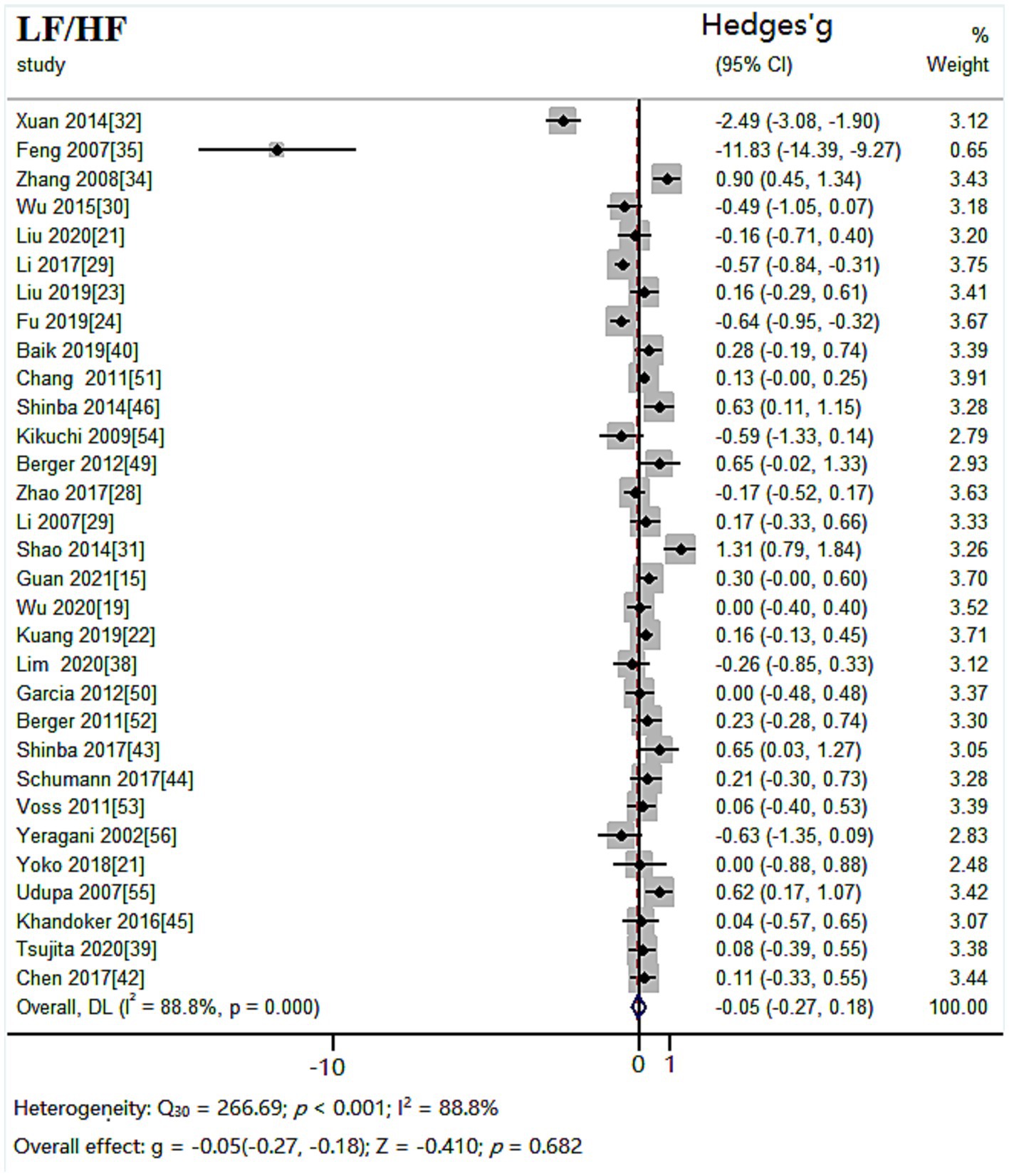
Figure 7. Meta-analysis forest plot of indicator LF/HF.
In order to explore the source of heterogeneity, a subgroup analysis was conducted on the six indicators according to age distribution and literature sources, and the results are displayed in Tables 3, 4.
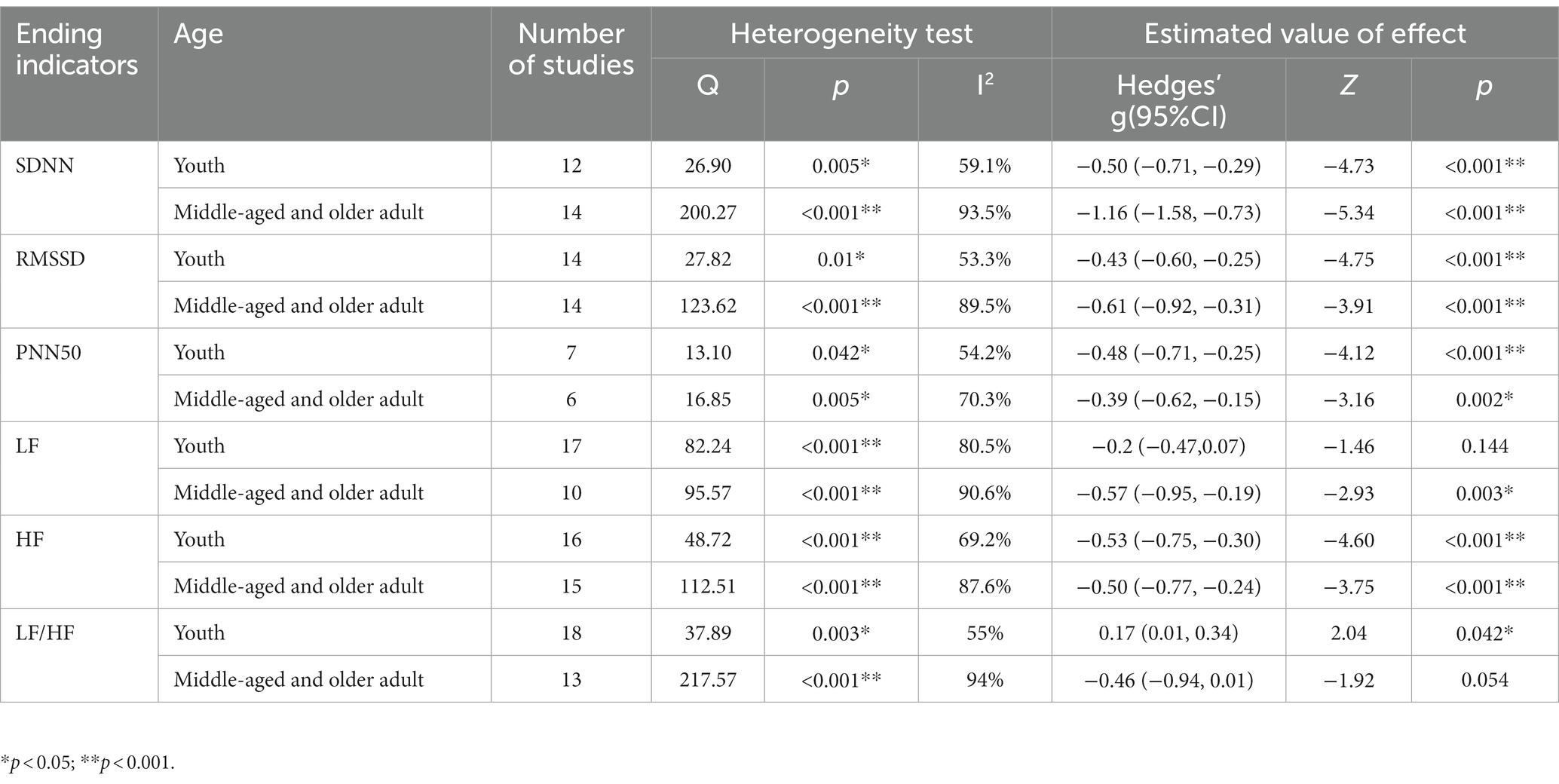
Table 3. Subgroup analysis of the 6 indicators by age distribution.
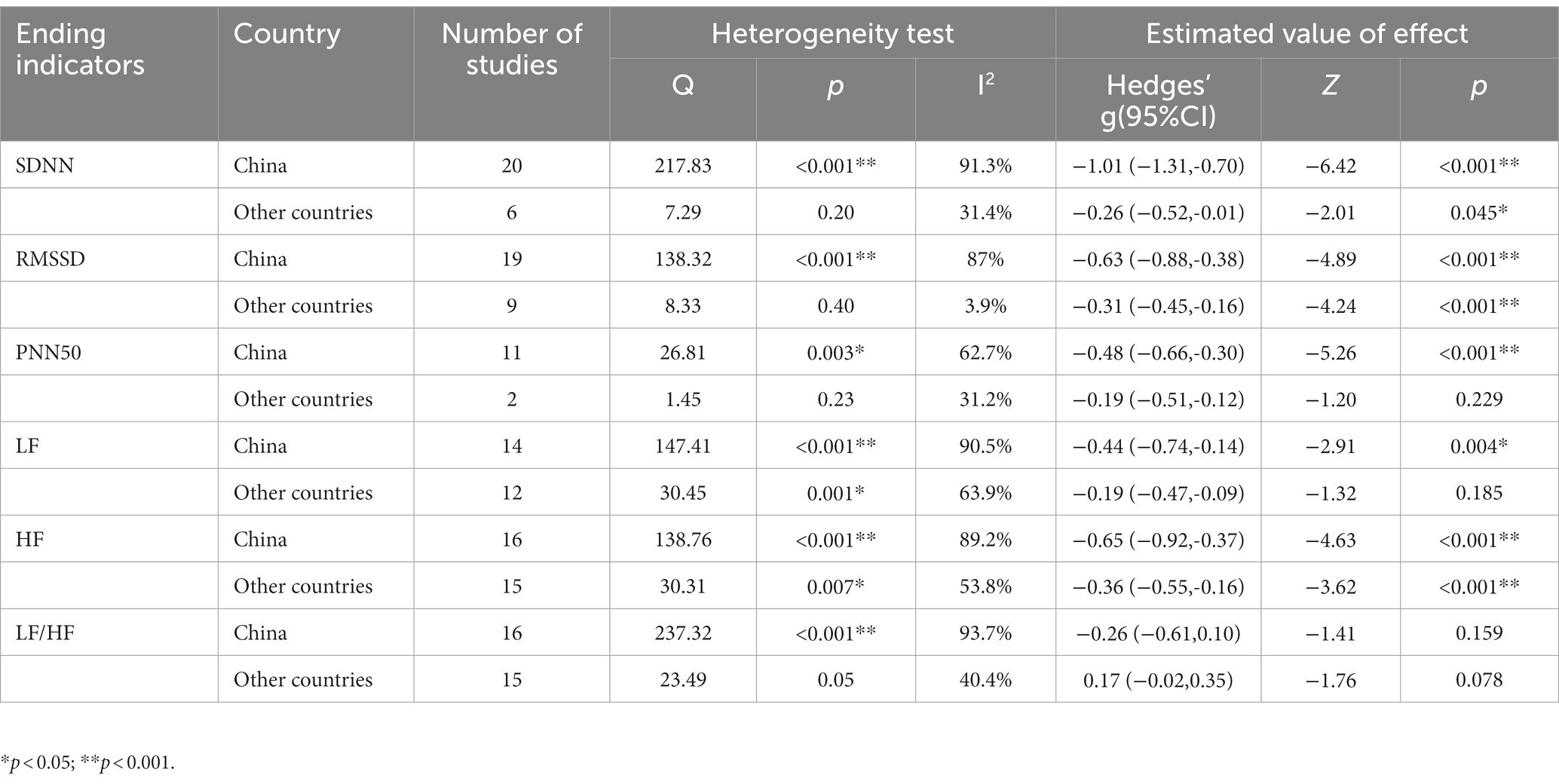
Table 4. Subgroup analysis of the 6 indicators by literature sources.
The included studies were eliminated one by one, and the effect size of the meta-analysis obtained after each elimination was compared to the total effect size to assess whether the results had significant changes. After using the one-by-one elimination method, it was found that after deleting Feng (35), Q = 76.84, p < 0.001, I2 = 66%, Hedges’ g = −0.45, 95%CI (−0.58, −0.32), although I2 has decreased, there was still heterogeneity in RMSSD indicators. The results showed that after removing the article by Li (29), the heterogeneity of PNN50 index decreased significantly: Q = 19.45, p = 0.053, I2 = 43.5%, and the merging result was stable: Hedges’ g = −0.48, 95% CI (−0.62, −0.34), p < 0.001. No alterations were noticed in other indices after the one-by-one elimination method was implemented. Moreover, two effect models were also employed to assess the dependability of the meta-analysis’ outcomes. Table 5 demonstrated that the six outcome indicators did not significantly vary when the effect model was altered, indicating that the results of the meta-analysis in this investigation were relatively consistent.
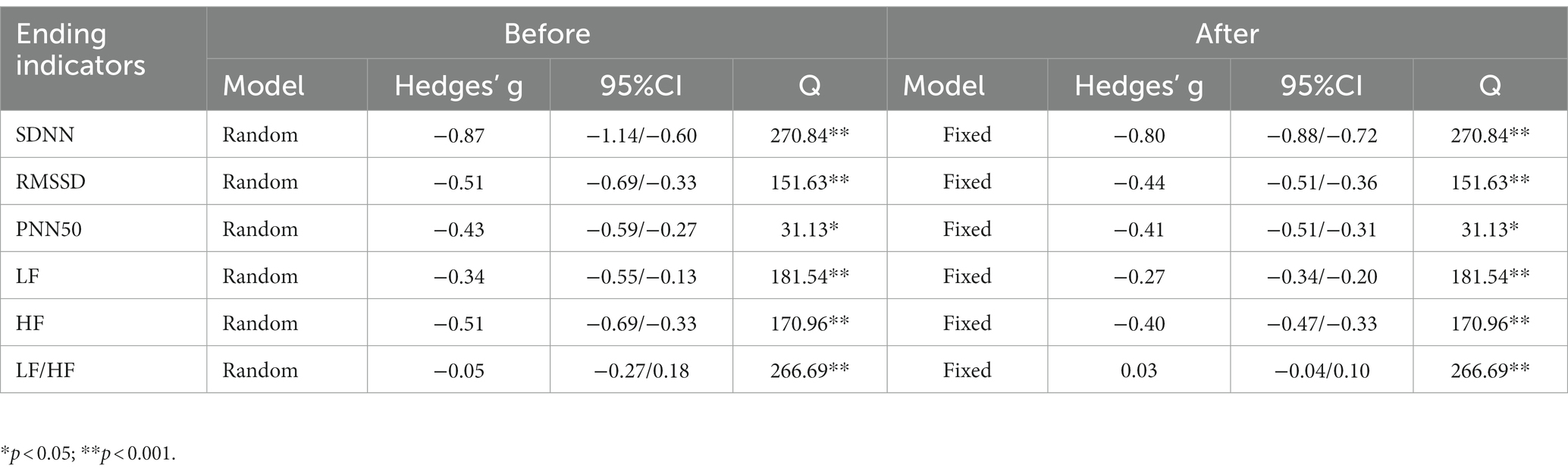
Table 5. Comparative analysis of two effect models.
The six outcome indicators used in this study, each of which included more than 10 papers, can be tested for publication bias by means of funnel plots (Figure 8). Since funnel plot method is a qualitative method to identify publication bias, we use the Egger’ s method. The results of Egger’ s method further showed that there was no publication bias for SDNN (p = 0.419), PNN50 (p = 0.416), LF (p = 0.511), HF (p = 0.108), and LF/HF (p = 0.263). While RMSSD (p = 0.009) had publication bias, eight research data were simulated by trim and fill procedure, Results were not significantly reversed before and after shear compensation analysis (Hedges’ g = −0.718, 95%CI: −0.907, 0.528, p < 0.001), suggesting that the meta-analysis results were stable.
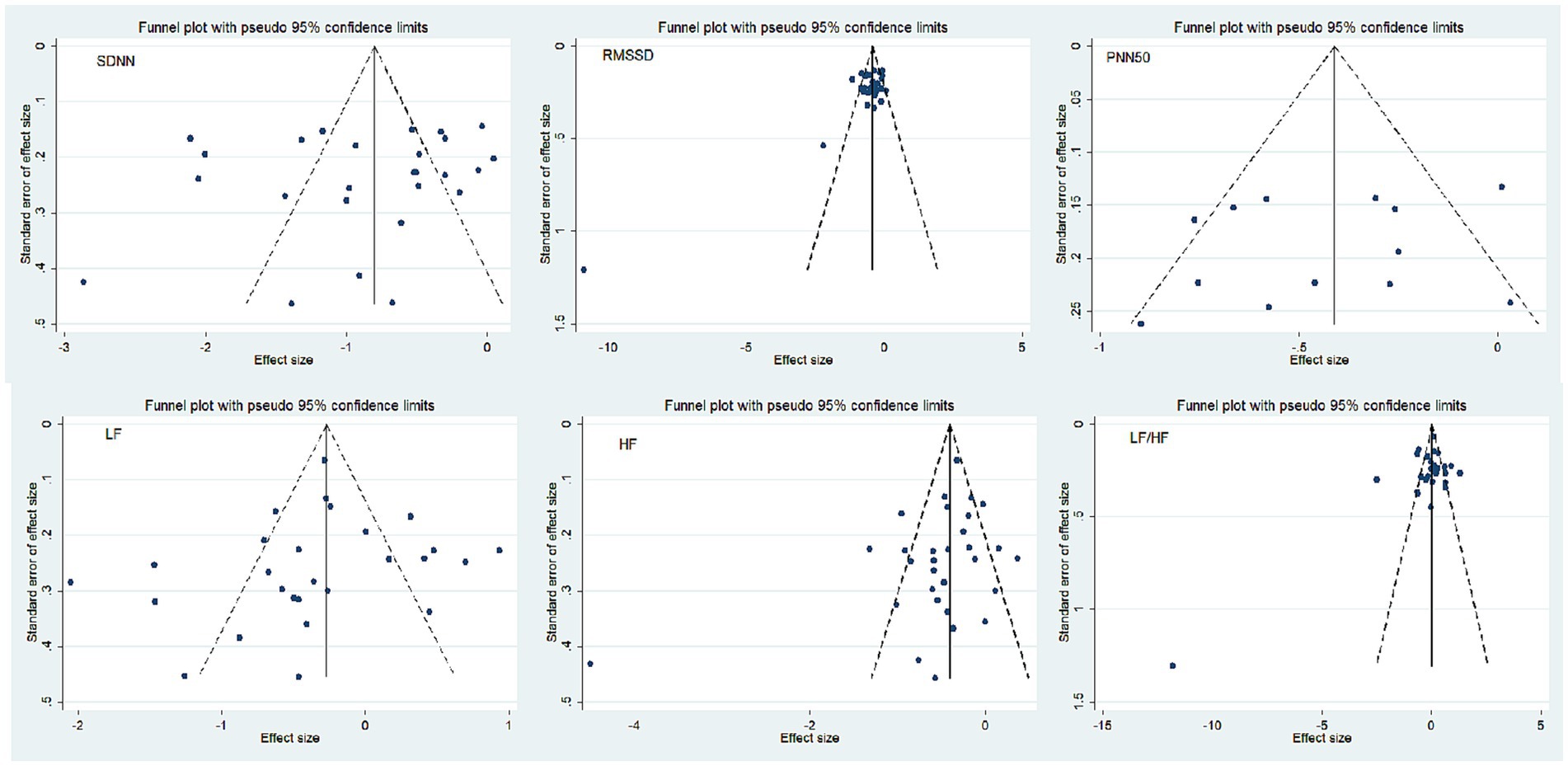
Figure 8. Funnel plot of publication bias.
The World Health Organization conducted a survey which showed that over 300 million people around the world are suffering from depression (58). Depression can have a significant influence on people’s quality of life and is frequently accompanied by other psychiatric conditions, particularly anxiety disorders (59), as well as somatic chronic diseases such as coronary heart disease and heart failure (60). Research revealed that patients with depression combined with coronary artery disease had increased plasma catecholamines, autonomic dysfunction, and a decline in multiple HRV markers in comparison to those with depression alone (61). A meta-analysis demonstrated that a lower HRV was associated with a higher incidence of cardiovascular disease and mortality (62). A cohort study conducted in the United States revealed that depressive symptoms are linked to the risk of heart failure events, with women being at a greater risk. This finding was further corroborated in 2014 when the American Heart Association issued a statement on depression as a risk factor for a poor prognosis in patients with acute coronary syndromes (63). Meta-analysis has indicated that an overactive hypothalamic–pituitary–adrenal axis is connected to the development of depression (64), and it can also influence the cardiovascular system of humans by modulating autonomic nerves (6). Detecting autonomic function in depressed individuals can help to protect against cardiovascular disease.
The findings of this study indicated that depressed patients displayed a significantly diminished SDNN, RMSSD, PNN50, LF, and HF in comparison to the healthy population. Additionally, Koch et al.’s (65) meta-analysis of HRV in patients with major depression revealed that depressed patients had notably diminished SDNN, RMSSD, LF, and HF indicators compared to the control group, which is in agreement with the current study’s results. The decrease in SDNN indexes indicates that depressed patients experience an increase in sympathetic nerve activity and a decrease in parasympathetic nerve activity, implying that they have disorders of the central nervous system’s energy supply due to external stress and heightened sensitivity to stimuli. RMSSD and PNN50 are primarily indicators of changes in vagal tone, and these can be influenced by age and gender (66). The analysis of bias revealed that there was publication bias in RMSSD, however, the results stayed nearly the same after the exclusion of the literature (35) that could have been the cause of the bias. After eliminating the study of Li (29), the heterogeneity of PNN50 index was significantly reduced, and the combined results were stable, still indicating abnormal parasympathetic activity in patients with depression. Wang et al. (67) conducted an analysis of HRV in patients with major depression and discovered that RMSSD, PNN50 and HF values were lower in the depressed group than in the control group. The imbalance in nerve activity in depressed patients, with a surge in sympathetic nerve activity and a decrease in parasympathetic nerve activity, could be the mechanism behind arrhythmia. According to Kemp et al. (68), there was no difference in LF between depressed and normal individuals. Additionally, Brown et al. (69) revealed a significant decrease in LF in older adult depressed patients when compared to healthy controls, yet no noteworthy alterations were seen in HF. For those with first-onset major depression, LF was likely to decrease and HF was likely to increase (30). The decrease in HRV predicts an imbalance in the body’s autonomic nervous system and can serve as a mediator of other psychological stress changes in depression (70), anxiety disorders (71), etc. Depression has been linked to cardiovascular disease in many cases, which is one of the most prevalent somatic comorbidities (72). According to Thayer (73), the autonomic nervous system and parasympathetic tone are connected to glucose regulation and inflammatory response, while a reduction in HRV is correlated with increased fasting glucose, nocturnal urinary cortisol, and augmented pro-inflammatory cytokines and acute phase proteins. He proposed that identifying neuroendocrine regulatory systems may aid in understanding the pathways in which psychosocial factors have an effect on health. The results of the current study did not demonstrate any significant disparity between the two groups in terms of LF/HF index. Catrambone chose subclinically depressed female patients as participants, and the LF/HF ratio was not different from that of the control group, which is in line with the findings of this study. However, other studies have reported that the LF/HF ratio (74) was higher in depressed patients than in healthy individuals (63), and the LF/HF index was significantly correlated with the Profile of Mood States (POMS) questionnaire (75).
The Q test results demonstrated a considerable degree of heterogeneity in the outcome indicators of this study, so we conducted subgroup analysis to determine the source of this heterogeneity. After conducting subgroup analysis according to age range, the LF/HF index of normal young people was found to be significantly higher than that of depressed young people, yet the heterogeneity in all indicators remained high, with no other notable changes. Ngampramuan’s study revealed that the LF/HF ratio of older adult patients with major depression was significantly higher than that of normal subjects, which differs from the results of the present study (76). Udupa (55) discovered that the LF/HF ratio was significantly higher in young people with major depression than in healthy subjects, which implies a decrease in parasympathetic activity and an increase in sympathetic activity, which is in agreement with the results of the subgroup analysis in this study. The LF/HF index has been employed for a considerable amount of time, yet other research has indicated that the LF/HF ratio may be more associated with respiratory parameters and mechanical factors, and not with alterations in cardiac autonomic nervous regulation (77). Proposals to utilize the new analytical method LF-HF for analysis (78) have been made by some academics, yet many studies presently continue to use the LF/HF index, so our research can only be evaluated based on existing studies. In the future, empirical studies and theoretical innovations should be conducted to further explore the LF/HF results, and the interpretation of these results should be done with caution. We conducted a subgroup analysis on the sources of the literature, and the results indicated that when the subjects in SDNN, RMSSD, PNN50 and LF/HF were not Chinese, the heterogeneity was not significant. This may be attributed to the differences in experimental design, environmental region, and domestic and foreign diagnostic criteria. Perhaps in the future it will be possible to directly compare the differences in heart rate variability among depressed patients in different countries or regions.
There are some shortcomings in this study. First, although we have tried our best to find the literature related to this study, there is still a possibility of missing the examination. Some grey literature was not included in this study, which may have a certain impact on the results of this study. Secondly, we only performed subgroup analysis for the age distribution range, but whether the type of depression, gender, and diagnostic criteria may have an effect on the results also deserves more detailed exploration in the future. Finally, most of the literature included in this study is based on clinical case–control data, which makes it difficult to achieve random grouping and blinded implementation, and more high-quality articles related to heart rate variability in depressed patients are expected to be published in the future.
In conclusion, the results of the meta-analysis of this study provide relevant evidence for the alteration of HRV in depressed patients. The utilization of the HRV test can be an effective way to assess cardiovascular health and autonomic function, which has significant implications for the prevention and surveillance of cardiovascular disease in individuals suffering from depression.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
QW and AC were responsible for the conception and writing of the study. QW, AC and TX were responsible for the design and revision of this study. XM and YC were responsible for the screening of the literature. All authors have read and agreed to the published version of the manuscript.
This research was supported by the Signature Achievement Project of Sports School in Shaanxi Normal University (No. 2022AA002).
Thanks to all participants for their help in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1243213/full#supplementary-material
1. Chakrabarti, S . Bipolar disorder in the international classification of diseases-eleventh version: a review of the changes, their basis, and usefulness. World J Psychiatry. (2022) 12:1335–55. doi: 10.5498/wjp.v12.i12.1335
2. Friedrich, MJ . Depression is the leading cause of disability around the world. JAMA. (2017) 317:1517. doi: 10.1001/jama.2017.3826
3. Phillips, MR , Zhang, J , Shi, Q , Song, Z , Ding, Z , Pang, S, et al. Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001–05: an epidemiological survey. Lancet. (2009) 373:2041–53. doi: 10.1016/S0140-6736(09)60660-7
4. Sgoifo, A , Carnevali, L , Pico Alfonso, MA , and Amore, M . Autonomic dysfunction and heart rate variability in depression. Stress. (2015) 18:343–52. doi: 10.3109/10253890.2015.1045868
5. Cygankiewicz, I , and Zareba, W . Heart rate variability. Handb Clin Neurol. (2013) 117:379–93. doi: 10.1016/B978-0-444-53491-0.00031-6
6. Zhu, J , Ji, L , and Liu, C . Heart rate variability monitoring for emotion and disorders of emotion. Physiol Meas. (2019) 40:064004. doi: 10.1088/1361-6579/ab1887
7. Shaffer, F , and Ginsberg, JP . An overview of heart rate variability metrics and norms. Front Public Health. (2017) 5:5. doi: 10.3389/fpubh.2017.00258
8. Tanwar, G , Chauhan, R , Singh, M , and Singh, D . Pre-emption of affliction severity using HRV measurements from a smart wearable; case-study on SARS-Cov-2 symptoms. Sensors (Basel). (2020) 20:7068. doi: 10.3390/s20247068
9. Mejía-Mejía, E , Budidha, K , Abay, TY , May, JM , and Kyriacou, PA . Heart rate variability (HRV) and pulse rate variability (PRV) for the assessment of autonomic responses. Front Physiol. (2020) 11:779. doi: 10.3389/fphys.2020.00779
10. Zhang, Y , Chen, Y , and Ma, L . Depression and cardiovascular disease in elderly: current understanding. J Clin Neurosci. (2018) 47:1–5. doi: 10.1016/j.jocn.2017.09.022
11. Liberati, A , Altman, DG , Tetzlaff, J , Mulrow, C , Gøtzsche, PC , Ioannidis, JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ (Clinical research ed). (2009) 339:b2700. doi: 10.1136/bmj.b2700
12. Armijo-Olivo, S , Stiles, CR , Hagen, NA , Biondo, PD , and Cummings, GG . Assessment of study quality for systematic reviews: a comparison of the Cochrane collaboration risk of Bias tool and the effective public health practice project quality assessment tool: methodological research. J Eval Clin Pract. (2012) 18:12–8. doi: 10.1111/j.1365-2753.2010.01516.x
13. Wu, J , Chen, Z , Zheng, K , Huang, W , Liu, F , Lin, J, et al. Benefits of Exergame training for female patients with fibromyalgia: a systematic review and Meta-analysis of randomized controlled trials. Arch Phys Med Rehabil. (2022) 103:1192–1200.e2. doi: 10.1016/j.apmr.2021.10.022
14. Wu, J , Sun, Y , Zhang, G , Zhou, Z , and Ren, Z . Virtual reality-assisted cognitive behavioral therapy for anxiety disorders: a systematic review and Meta-analysis. Front Psych. (2021) 12:575094. doi: 10.3389/fpsyt.2021.575094
15. Guan, QL , Wu, ZY , Peng, HJ , Huang, SJ , and Deng, SM . Correlation between mental health status and autonomic nervous function in young depression patients. Guangdong Med J. (2021) 42:691–5. doi: 10.13820/j.cnki.gdyx.20202347
16. Li, HY , Li, ZG , and Guan, PF . Analysis of electrocardiogram and heart rate variability in patients with moderate to severe depression. JMEP. (2021) 28:23–5. doi: 10.3969/j.issn.1672-0458.2021.01.005
17. Wang, JH . Research of depression state recognition based on heart rate variability. Jinan: Shandong University (2021).
18. Chen, DY . The state of anxiety and depression in elderly inpatients and its correlation with heart rate variability. Nanchong: North Sichuan Medical College (2021).
19. Wu, HL , Wang, S , Huang, WL , Zhang, YX , and Liu, ZP . Study of heart rate variability in schizophrenia, bipolar disorder, depression and generalized anxiety disorder. Jiangxi Med J. (2020) 55:517–519+627. doi: 10.3969/j.issn.1006-2238.2020.05.007
20. Zhao, SG . The effect and physiological mechanism of 18 weeks physical activity on depression in college students. Xi’an: Shaanxi Normal University (2020).
21. Liu, Y . A study on the influence of depression emotions on viscera qi activity based on HRV features. Nanchang: Jiangxi University of Chinese Medicine (2020).
22. Kuang, DN . Assisted diagnosis Technology of Depression Using Heart Rate Variability. Guangzhou: South China University of Technology (2019).
23. Liu, ZP , Wu, HL , and Hu, MR . Heart rate variability in patients with generalized anxiety disorder and depressive disorder. Chin Gen Prac. (2019) 22:4069–72. doi: 10.12114/j.issn.1007-9572.2019.00.597
24. Fu, ZX , Zhang, J , and Liu, BZ . Correlation analysis between postpartum depression and autonomic nervous function and personality characteristics of elderly menthymus. Maternal Child Health Care China. (2019) 34:4782–5. doi: 10.7620/zgfybj.j.issn.1001–4411.2019.20.60
25. Sun, YP . Analysis of clinical diagnostic value of holter electrocardiogram in patients with depression. Electron J Clin Med Literat. (2019) 6:134–6. doi: 10.16281/j.cnki.jocml.2019.76.104
26. Zhang, T , Zhang, Y , and Cai, TT . Change and clinical significance of heart rate variability in patients with postpartum depression. Maternal Child Health Care China. (2018) 33:1945–7. doi: 10.7620/zgfybj.j.issn.1001–4411.2018.09.07
27. Yang, H . Heart rate variability and endothelial function in depression. World Latest Medicine Information. (2018) 18:103–6. doi: 10.19613/j.cnki.1671-3141.2018.40.079
28. Zhao, HT , and Zhao, J . The correlation analysis of autonomic nerve function and postpartum depression. Chinese J Pract Nervous Dis. (2017) 20:86–88+91. doi: 10.3969/j.issn.1673-5110.2017.16.027
29. Li, P , Li, RX , Li, N , and Peng, Y . Heart rate variability in outpatient patients with depression of different genders. Modern Commun. (2017) 24:25–7.
30. Wu, B , Wang, T , and Li, XL . Changes and significance of heart rate variability in senile depression. Chin J Gerontol. (2015) 35:2021–2. doi: 10.3969/j.issn.1005-9202.2015.08.003
31. Shao, YF , Wu, AH , Xu, BY , and Lu, JJ . Correlation study of the level of hypersensitive C-reactive protein and the heart rate variability in patients with episode depressive disorder. China Med Herald. (2014) 11:34–7.
32. Xuan, JL . Clinical study of short route heart rate variability in 39 cases of depressive disorders. J Med Sci Yanbian Univ. (2014) 37:200–1. doi: 10.16068/j.1000-1824.2014.03.015
33. Wang, XY . Relationship between deceleration capacity of rate and heart rate variability in the patients with depression. J Clin Electrocardiol. (2013) 22:354–5.
34. Zhang, Q , Luan, T , Shen, J , Wu, AQ , Pan, NR , Mei, QY, et al. Characteristics of heart rate variability in anxiety or depressive diseases. Suzhou Univ J Med Sci. (2008) 5:804–6.
35. Feng, YS , and Feng, SH . The analysis of the depressive Patient’s heart rate variability. West China Med J. (2007) 4:806–7.
36. Li, XJ , and Li, DQ . Spectral decomposition of heart rate variability in patients with depressive disorders. Zhejiang Med J. (2007) 9:916–8.
37. Smith, LT , Levita, L , Amico, F , Fagan, J , Yek, JH , Brophy, J, et al. Using resting state heart rate variability and skin conductance response to detect depression in adults. Annu Int Conf IEEE Eng Med Biol Soc. (2020) 2020:5004–7. doi: 10.1109/EMBC44109.2020.9176304
38. Lim, JA , Yun, JY , Choi, Y , Choi, SH , Kwon, Y , Lee, HY, et al. Sex-specific differences in severity of depressive symptoms, heart rate variability, and neurocognitive profiles of depressed young adults: exploring characteristics for mild depression. Front Psych. (2020) 11:217. doi: 10.3389/fpsyt.2020.00217
39. Tsujita, N , Akamatsu, Y , Nishida, MM , Hayashi, T , and Moritani, T . Physical activity, nutritional status, and autonomic nervous system activity in healthy young adults with higher levels of depressive symptoms and matched controls without depressive symptoms: a cross-sectional study. Nutrients. (2020) 12:690. doi: 10.3390/nu12030690
40. Baik, SY , Kim, C , Kim, S , Yook, DW , Kim, HS , Chang, H, et al. The moderating effect of heart rate variability on the relationship between alpha asymmetry and depressive symptoms. Heliyon. (2019) 5:e01290. doi: 10.1016/j.heliyon.2019.e01290
41. Caldwell, YT , and Steffen, PR . Adding HRV biofeedback to psychotherapy increases heart rate variability and improves the treatment of major depressive disorder. Int J Psychophysiol. (2018) 131:96–101. doi: 10.1016/j.ijpsycho.2018.01.001
42. Chen, X , Yang, R , Kuang, D , Zhang, L , Lv, R , Huang, X, et al. Heart rate variability in patients with major depression disorder during a clinical autonomic test. Psychiatry Res. (2017) 256:207–11. doi: 10.1016/j.psychres.2017.06.041
43. Shinba, T . Major depressive disorder and generalized anxiety disorder show different autonomic dysregulations revealed by heart-rate variability analysis in first-onset drug-Naïve patients without comorbidity. Psychiatry Clin Neurosci. (2017) 71:135–45. doi: 10.1111/pcn.12494
44. Schumann, A , Andrack, C , and Bär, KJ . Differences of sympathetic and parasympathetic modulation in major depression. Prog Neuro-Psychopharmacol Biol Psychiatry. (2017) 79:324–31. doi: 10.1016/j.pnpbp.2017.07.009
45. Khandoker, AH , Luthra, V , Abouallaban, Y , Saha, S , Ahmed, KI , Mostafa, R, et al. Predicting depressed patients with suicidal ideation from ECG recordings. Med Biol Eng Comput. (2017) 55:793–805. doi: 10.1007/s11517-016-1557-y
46. Shinba, T . Altered autonomic activity and reactivity in depression revealed by heart-rate variability measurement during rest and task conditions. Psychiatry Clin Neurosci. (2014) 68:225–33. doi: 10.1111/pcn.12123
47. Brunoni, AR , Kemp, AH , Dantas, EM , Goulart, AC , Nunes, MA , Boggio, PS, et al. Heart rate variability is a trait marker of major depressive disorder: evidence from the sertraline vs. electric current therapy to treat depression clinical study. Int J Neuropsychopharmacol. (2013) 16:1937–49. doi: 10.1017/S1461145713000497
48. Dauphinot, V , Rouch, I , Kossovsky, MP , Pichot, V , Dorey, JM , Krolak-Salmon, P, et al. Depressive symptoms and autonomic nervous system dysfunction in an elderly population-based study: the PROOF study. J Affect Disord. (2012) 143:153–9. doi: 10.1016/j.jad.2012.05.045
49. Berger, S , Kliem, A , Yeragani, V , and Bär, KJ . Cardio-respiratory coupling in untreated patients with major depression. J Affect Disord. (2012) 139:166–71. doi: 10.1016/j.jad.2012.01.035
50. Garcia, RG , Zarruk, JG , Guzman, JC , Barrera, C , Pinzon, A , Trillos, E, et al. Sex differences in cardiac autonomic function of depressed young adults. Biol Psychol. (2012) 90:179–85. doi: 10.1016/j.biopsycho.2012.03.016
51. Chang, H-A , Chang, C-C , Chen, C-L , Kuo, TBJ , Lu, R-B , and Huang, S-Y . Major depression is associated with cardiac autonomic dysregulation. Acta Neuropsychiatr. (2012) 24:318–27. doi: 10.1111/j.1601-5215.2011.00647.x
52. Berger, S , Schulz, S , Kletta, C , Voss, A , and Bär, KJ . Autonomic modulation in healthy first-degree relatives of patients with major depressive disorder. Prog Neuro-Psychopharmacol Biol Psychiatry. (2011) 35:1723–8. doi: 10.1016/j.pnpbp.2011.05.018
53. Voss, A , Boettger, MK , Schulz, S , Gross, K , and Bär, KJ . Gender-dependent impact of major depression on autonomic cardiovascular modulation. Prog Neuro-Psychopharmacol Biol Psychiatry. (2011) 35:1131–8. doi: 10.1016/j.pnpbp.2011.03.015
54. Kikuchi, M , Hanaoka, A , Kidani, T , Remijn, GB , Minabe, Y , Munesue, T, et al. Heart rate variability in drug-Naïve patients with panic disorder and major depressive disorder. Prog Neuro-Psychopharmacol Biol Psychiatry. (2009) 33:1474–8. doi: 10.1016/j.pnpbp.2009.08.002
55. Udupa, K , Sathyaprabha, TN , Thirthalli, J , Kishore, KR , Lavekar, GS , Raju, TR, et al. Alteration of cardiac autonomic functions in patients with major depression: a study using heart rate variability measures. J Affect Disord. (2007) 100:137–41. doi: 10.1016/j.jad.2006.10.007
56. Yeragani, VK , Rao, KARK , Smitha, MR , Pohl, RB , Balon, R , and Srinivasan, K . Diminished Chaos of heart rate time series in patients with major depression. Biol Psychiatry. (2002) 51:733–44. doi: 10.1016/S0006-3223(01)01347-6
57. Yeragani, VK , Pohl, R , Jampala, VC , Balon, R , Ramesh, C , and Srinivasan, K . Increased QT variability in patients with panic disorder and depression. Psychiatry Res. (2000) 93:225–35. doi: 10.1016/S0165-1781(00)00119-0
58. World Health Organization . Depression and other common mental disorder: Global Health estimates. Geneva: World Health Organization (2017).
59. Watson, D . Differentiating the mood and anxiety disorders: a quadripartite model. Annu Rev Clin Psychol. (2009) 5:221–47. doi: 10.1146/annurev.clinpsy.032408.153510
60. Harshfield, EL , Pennells, L , Schwartz, JE , Willeit, P , Kaptoge, S , Bell, S, et al. Association between depressive symptoms and incident cardiovascular diseases. JAMA. (2020) 324:2396–405. doi: 10.1001/jama.2020.23068
61. Carney, RM , Freedland, KE , and Veith, RC . Depression, the autonomic nervous system, and coronary heart disease. Psychosom Med. (2005) 67:S29–33. doi: 10.1097/01.psy.0000162254.61556.d5
62. Fang, S-C , Wu, Y-L , and Tsai, P-S . Heart rate variability and risk of all-cause death and cardiovascular events in patients with cardiovascular disease: a meta-analysis of cohort studies. Biol Res Nurs. (2020) 22:45–56. doi: 10.1177/1099800419877442
63. Lichtman, JH , Froelicher, ES , Blumenthal, JA , Carney, RM , Doering, LV , Frasure-Smith, N, et al. Depression as a risk factor for poor prognosis among patients with acute coronary syndrome: systematic review and recommendations: a scientific statement from the American Heart Association. Circulation. (2014) 129:1350–69. doi: 10.1161/CIR.0000000000000019
64. Pariante, CM . Why are depressed patients inflamed? A reflection on 20 years of research on depression, glucocorticoid resistance and inflammation. Eur Neuropsychopharmacol. (2017) 27:554–9. doi: 10.1016/j.euroneuro.2017.04.001
65. Koch, C , Wilhelm, M , Salzmann, S , Rief, W , and Euteneuer, F . A Meta-analysis of heart rate variability in major depression. Psychol Med. (2019) 49:1948–57. doi: 10.1017/S0033291719001351
66. Togo, F , and Takahashi, M . Heart rate variability in occupational health ―a systematic review. Ind Health. (2009) 47:589–602. doi: 10.2486/indhealth.47.589
67. Wang, Y , Zhao, X , O'Neil, A , Turner, A , Liu, X , and Berk, M . Altered cardiac autonomic nervous function in depression. BMC Psychiatry. (2013) 13:187. doi: 10.1186/1471-244X-13-187
68. Kemp, AH , Quintana, DS , Gray, MA , Felmingham, KL , Brown, K , and Gatt, JM . Impact of depression and antidepressant treatment on heart rate variability: a review and Meta-analysis. Biol Psychiatry. (2010) 67:1067–74. doi: 10.1016/j.biopsych.2009.12.012
69. Brown, L , Karmakar, C , Gray, R , Jindal, R , Lim, T , and Bryant, C . Heart rate variability alterations in late life depression: a Meta-analysis. J Affect Disord. (2018) 235:456–66. doi: 10.1016/j.jad.2018.04.071
70. Kemp, AH , Koenig, J , and Thayer, JF . From psychological moments to mortality: a multidisciplinary synthesis on heart rate variability spanning the continuum of time. Neurosci Biobehav Rev. (2017) 83:547–67. doi: 10.1016/j.neubiorev.2017.09.006
71. Friedman, BH . An autonomic flexibility-Neurovisceral integration model of anxiety and cardiac vagal tone. Biol Psychol. (2007) 74:185–99. doi: 10.1016/j.biopsycho.2005.08.009
72. Penninx, BWJH . Depression and cardiovascular disease: epidemiological evidence on their linking mechanisms. Neurosci Biobehav Rev. (2017) 74:277–86. doi: 10.1016/j.neubiorev.2016.07.003
73. Thayer, JF , and Sternberg, E . Beyond heart rate variability: vagal regulation of allostatic systems. Ann N Y Acad Sci. (2006) 1088:361–72. doi: 10.1196/annals.1366.014
74. Catrambone, V , Messerotti Benvenuti, S , Gentili, C , and Valenza, G . Intensification of functional neural control on heartbeat dynamics in subclinical depression. Transl Psychiatry. (2021) 11:221. doi: 10.1038/s41398-021-01336-4
75. Minakuchi, E , Ohnishi, E , Ohnishi, J , Sakamoto, S , Hori, M , Motomura, M, et al. Evaluation of mental stress by physiological indices derived from finger plethysmography. J Physiol Anthropol. (2013) 32:17. doi: 10.1186/1880-6805-32-17
76. Ngampramuan, S , Tungtong, P , Mukda, S , Jariyavilas, A , and Sakulisariyaporn, C . Evaluation of autonomic nervous system, saliva cortisol levels, and cognitive function in major depressive disorder patients. Depress Res Treat. (2018) 2018:1–8. doi: 10.1155/2018/7343592
77. Billman, GE . The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front Physiol. (2013) 4:26. doi: 10.3389/fphys.2013.00026
Keywords: depression, heart rate variability, meta-analysis, case-control study, adult
Citation: Wu Q, Miao X, Cao Y, Chi A and Xiao T (2023) Heart rate variability status at rest in adult depressed patients: a systematic review and meta-analysis. Front. Public Health. 11:1243213. doi: 10.3389/fpubh.2023.1243213
Edited by:
Simone Messerotti Benvenuti, University of Padua, ItalyReviewed by:
Claudio Imperatori, European University of Rome, ItalyCopyright © 2023 Wu, Miao, Cao, Xiao and Chi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aiping Chi, Y2hpbXVAc25udS5lZHUuY24=; Tao Xiao, eGlhb3R0eUBzbm51LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.