 Abu Bakkar Siddique1,2,3*†
Abu Bakkar Siddique1,2,3*† Sudipto Deb Nath4,5
Sudipto Deb Nath4,5 Mahfuza Mubarak1Amena Akter6
Mahfuza Mubarak1Amena Akter6 Sanjida Mehrin7
Sanjida Mehrin7 Mst Jemi Hkatun1Antara Parvine Liza8M. Ziaul Amin5
Mst Jemi Hkatun1Antara Parvine Liza8M. Ziaul Amin5- 1Department of Public Health and Informatics, Jahangirnagar University, Savar, Dhaka, Bangladesh
- 2Centre for Advanced Research Excellence in Public Health, Savar, Dhaka, Bangladesh
- 3International Centre for Research, Innovation, Training and Development (ICRITD), Dhaka, Bangladesh
- 4Army Medical College Jashore, Jashore, Bangladesh
- 5Department of Genetic Engineering and Biotechnology, Jashore University of Science and Technology, Jashore, Bangladesh
- 6Department of Agriculture, Bangabandhu Sheikh Mujibur Rahman Science and Technology University, Gopalganj, Dhaka, Bangladesh
- 7Department of Political Studies, Shahjalal University of Science and Technology, Sylhet, Bangladesh
- 8Shahjalal University of Science and Technology, Sylhet, Bangladesh
Background: Poor menstrual hygiene practices during menstruation increases the risk of reproductive tract infections, absenteeism, and negative impact on school performance. Despite being a global problem, there is a lack of knowledge and misconceptions about menstrual hygiene among women of all ages, especially in developing countries like Bangladesh. The study aims to assess the knowledge, attitudes, and practices toward menstrual hygiene among early reproductive-aged women in Bangladesh to help policymakers and planners take effective initiatives.
Methodology: A cross-sectional survey was conducted between July and December 2022 in Dhaka, Rajshahi, Chittagong, Sylhet, and Barisal regions of Bangladesh. A convenience sampling technique was utilized to recruit a total of 1,214 participants (100% female; mean age: 22.87 ± 2.64 years). A semi-structured questionnaire including informed consent, socio-demographic information, as well as questions regarding knowledge (6-item), attitudes (7-item), and practices (6-item) toward menstruation and menstrual hygiene practices, was used to conduct the survey. All analyses were performed using the STATA (Version 15.0) and Statistical Package for the Social Sciences (SPSS version 25.0).
Result: The mean scores of the knowledge, attitudes, and practices were 4.9 ± 1.51 (out of 6), 12.58 ± 1.58 (out of 14), and 8.80 ± 1.87 (out of 12), respectively. The higher scores of knowledge, attitudes, and practices were significantly associated with several socio-demographic and menstruation-related factors (education, family type, type of menstruation, duration of menstruation, etc.).
Conclusion: This study identified several key factors associated with improved knowledge, attitudes, and practices related to menstrual hygiene, including higher education levels, student status, younger age, non-alcohol consumption, and regular menstrual cycles. To enhance menstrual hygiene practices among women, it is crucial to implement targeted interventions that address knowledge disparities and tackle social and environmental influences.
1 Introduction
Menstruation, often known as a period, is regular vaginal bleeding brought on by the monthly release of blood and tissue from the uterine lining (1). The beginning of menstruation, or menarche (puberty), together with the mental, emotional, and social changes up until the end of reproductive age, or menopause (the cessation of menstruation), are the most significant physiological transitional processes in women. Menstrual hygiene (MH) is a hygienic practices that takes place during menstruation. Proper menstrual hygiene involves thoroughly washing the external genitalia, utilizing sanitary napkins, tampons, menstrual cups, and similar products (2), while also replacing the napkin every 3 to 4 h to prevent odor (3).
Indian investigations discovered a connection between MH practices and urogenital infection (4, 5). According to a study on adolescent women in Ethiopia, stress-related mental states, such as low confidence and self-esteem, as well as academic failure owing to absence, all enhance the chance of infection (6). Another study of adolescent women from Rwanda and Ethiopia discovered that poor MH was also associated with infertility, reproductive tract infections (RTI), anemia, vaginal discharge with odor, itching, and other conditions (7). A study in Bangladesh of 2,332 schoolgirls, aged 11 to 17, from 700 schools indicated that menstruation had a detrimental impact on 32% of the participants’ academic performance and that 41% of them missed an average of 2.8 days per cycle (8). In addition, many women lack access to basic sanitary facilities (9), which makes it challenging for them to manage their MH owing to lack of facilities and proper knowledge (10). Unsanitary activities during menstruation increase the risk of infection or gynecological disorders in women. The frequency of reproductive tract infections is three times higher in women who practices poor MH (1). Menstrual absorbents may include these viruses and bacteria, therefore improper disposal of them could result in the transmission of hepatitis and HIV (11). Although the majority of the research focuses on young girls in school and adolescence, MH is a global issue that affects women and girls of all ages. Not just young girls, but women of many ages struggle with inadequate MH. Women frequently lack access to necessities like sanitary products, potable water, and private restrooms. Major health problems like infections and the spread of diseases may come from this (10, 12). Bangladesh and other lower-income nations are therefore very concerned about MH-related knowledge and practices.
Factors contributing to educational institutions and workplace absences among women included their attitudes, limited knowledge, and misconceptions about menstruation, as well as family restrictions, and inadequate facilities at the workplace (6). In Bangladesh as well as many developing countries, MH management among reproductive aged women remains poorly discussed so far. A pilot study on rural and urban women in Bangladesh found that they had got a chance to submit any question, 45% of them wanted to know about menstruation and 35% of these questions were about experiences of menstrual bleeding (13). So, there is a huge knowledge gap regarding MH and a proper KAP study can address this knowledge gap. Achieving SDG’s goal of sustainable water and sanitation, good health, and gender equality can be accelerated by assessing MH safely. The effective and timely provision of accurate information about menstruation and its management within supportive social environments that are free from menstrual stigma, as implied by this study, can enhance women’s capacity to manage menstrual hygiene (14).
Moreover, early-reproductive age is a critical period for women’s reproductive health and poor MH during this period may be indicative of various infections or other health conditions (15). There have been numerous studies on Bangladeshi schoolchildren and teenagers, but none have looked specifically at how early-reproductive-aged women in Bangladesh feel and know about MH. This study evaluates the knowledge, attitudes, and practices of early reproductive women concerning MH, which will assist policymakers and planners in making successful decisions by taking into account the needs of women today. The study’s conclusions will be useful in preventing menstrual disorders, infections, and difficulties associated with menstruation, as well as in promoting menstrual health by altering lifestyle and quality of life.
2 Materials and methods
2.1 Study area
The study was carried out in different parts of Bangladesh by self-reported questionnaire-based cross-sectional survey. Data was collected from Dhaka, Rajshahi, Chittagong, Sylhet and Barisal regions of Bangladesh between July and December 2022.
2.2 Sample size
The sample size was calculated using the following equation:
Here,
n = number of samples.
z = 1.96 (95% confidence level).
p = prevalence estimate (50% or 0.5) (as no study found).
q = (1-p).
d = precession of the prevalence estimate (10% of 0.05).
We expected that the current study’s prevalence estimate (p) would be 50%. A sample size of 423.5 ≈ 424 people was estimated based on a 10% non-response rate. This estimate was exceeded by our sample size. However, 1,214 participants were recruited to ensure the strength of the study.
2.3 Study design, participants, and procedure
The current study utilized a cross-sectional survey design based on self-reported questionnaires, conducted between July and December 2022. The participants were enrolled using a non-probability sampling (convenient sampling) technique (16). Each participant took approximately 10–15 min to complete the interview. Initially, 1,310 participants attended the surveys. After removing incomplete responses, the final analysis included 1,214 surveys. The data were gathered using a paper-based semi-structured questionnaire written in Bangla (the participant’s native language) from house to house. As MH is a very sensitive issue, the data was collected only by female research assistants and strict confidentiality was maintained.
A pilot test was carried out with 10 participants from the same population (target group) to determine the acceptability and transparency of the questionnaire. Following the pilot testing, a few minor adjustments were incorporated into the questionnaire. These data were not included in the final analysis. The first page of the questionnaire had an informed consent statement attached to it that explained the study’s objectives, procedures, and the participant’s right to decline participation. Before starting the survey, “participants were asked to provide informed consent (i.e., “Are you willing to participate in this study voluntarily and spontaneously?”). The inclusion criteria of the participants included: (i) women at early reproductive age (18 to 35 years of age) (17), (ii) experienced menstruation at their reproductive age, and (iii) living in Bangladesh. The participants below 18 years and over 35 years were excluded at the time of the interview.
2.4 Measures
2.4.1 Socio-demographic measures and determinants of menstruation and MH
Socio-demographic information was gathered by questions about age (later categorized as 18–24 years and 25–35 years), marital status (married/unmarried), education (below university/ university level), occupation (student/unemployed/employed/others), place of residence (Rural/Urban), family category (up to 4 members/more than 4 members), monthly family income (less than 15,000 Bangladeshi Taka [BDT]/1500BDT to 30,000 BDT/more than 30,000 BDT), Having children (yes/no), (OCP) oral contraceptive usage (yes/no).
2.4.2 Health-related measures and determinants of MH
Body Mass Index [BMI] (underweight/normal/overweight) [height and weight were measured by scales and then BMI was calculated], daily sleeping time (Less than 7 h/7 to 9 h/More than 9 h), smoking status (yes/no), alcohol intake (yes/no), social media usage in a day (less than 2 h/2 to 5 h/more than 5 h).
2.4.3 Menstruation and MH-related measures
Menstruation starting age (8 to 11 years/12 to 14 years/more than 14 years), type of menstruation (regular/irregular), the average duration of menstruation (less than 3 days/3 to 6 days/7 or more days).
2.4.4 Knowledge, attitudes, and practices measures
A total of 19 questions regarding knowledge (6-item), attitudes (7-item), and practices (6-item) toward MH, were used in the present study which were adopted from previous literature through extensive literature review (3, 18–20).
Six-item questions with three options (e.g., yes/no/do not know) related to knowledge regarding MH and its health effects were asked to the participants (e.g., “Is menstruation/menstrual cycle a physical process?,” “Are menstruations/menstrual cycle under the influence of hormones”) (see details in Figure 1). During analysis, “yes” responses were coded as “1”; whereas “no” and “do not know” responses were coded as “0.” The total score was obtained by summating the scores of all items and ranges from 0–6, with a higher score indicating a higher level of knowledge. In addition, sources of knowledge regarding menstruation/period were also recorded from the participants.
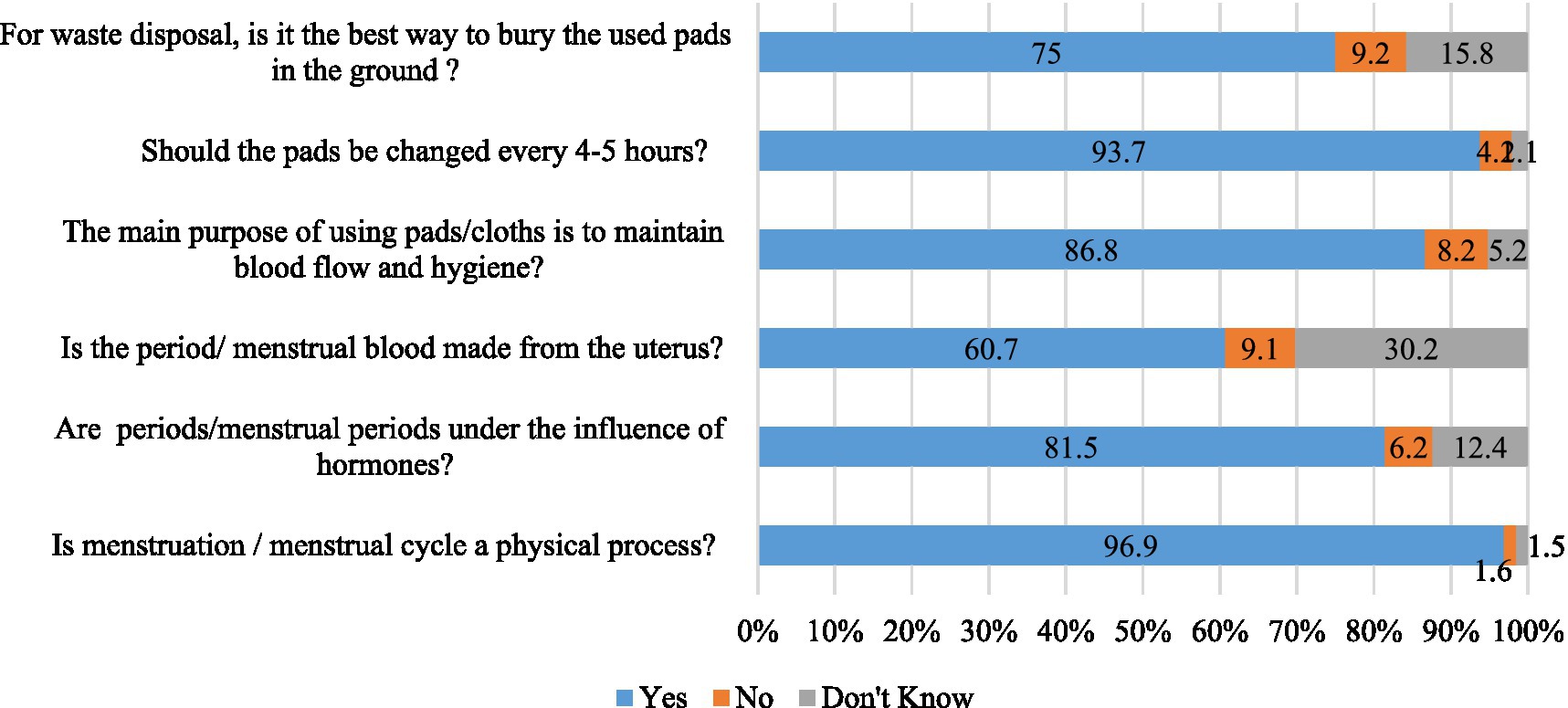
Figure 1. Knowledge regarding MH and menstruation.
To assess the attitudes toward MH, seven questions were used with a three-point Likert scale (e.g., 0 = disagree, 1 = neutral, 2 = agree). Examples of such questions include: “A girl should be happy after having a menstruation for the first time.,” “It is very important to keep the body clean with clean water and soap during the menstruation” (see details in Figure 2). The total score was obtained by summating the scores of all items and ranges from 0–14, with the higher score indicating a greater level of positive attitudes.
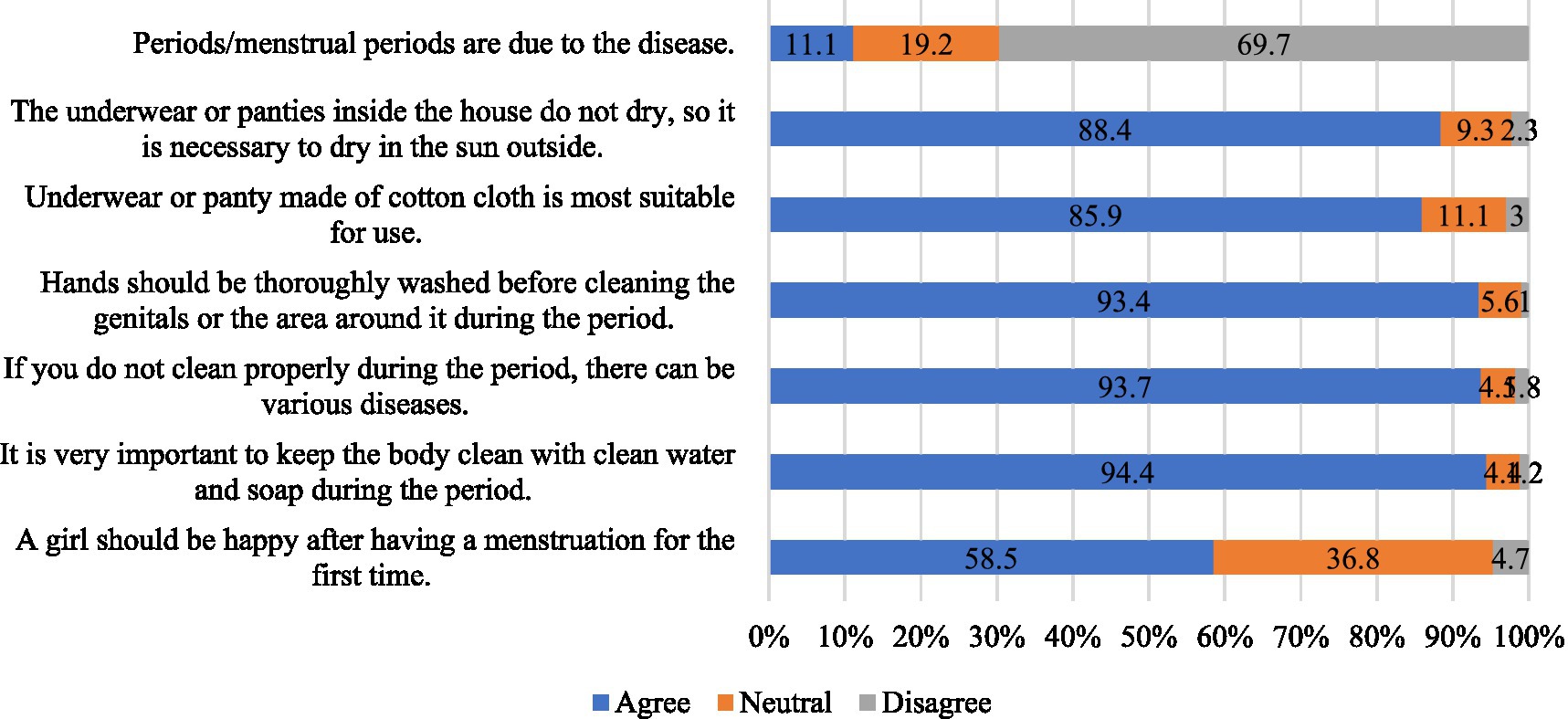
Figure 2. Attitude regarding MH and menstruation.
To document the practices status, the participants were asked six questions (e.g., “Do you go to school/college/university during menstruation regularly?,” “Do you change the pad every 4–6 h during the menstruation?,” “Do you change the underwear or panties 3–4 times a day during the menstruation?”) (see details in Figure 3) with three possible responses (e.g., never, sometimes, always). During analysis, “never” responses were coded as “0,” “sometimes” responses were coded as “1,” and “always” were coded as “2.” The total score was obtained by summating the scores of all items and ranges from 0–12, with a higher score indicating a higher level of practices.
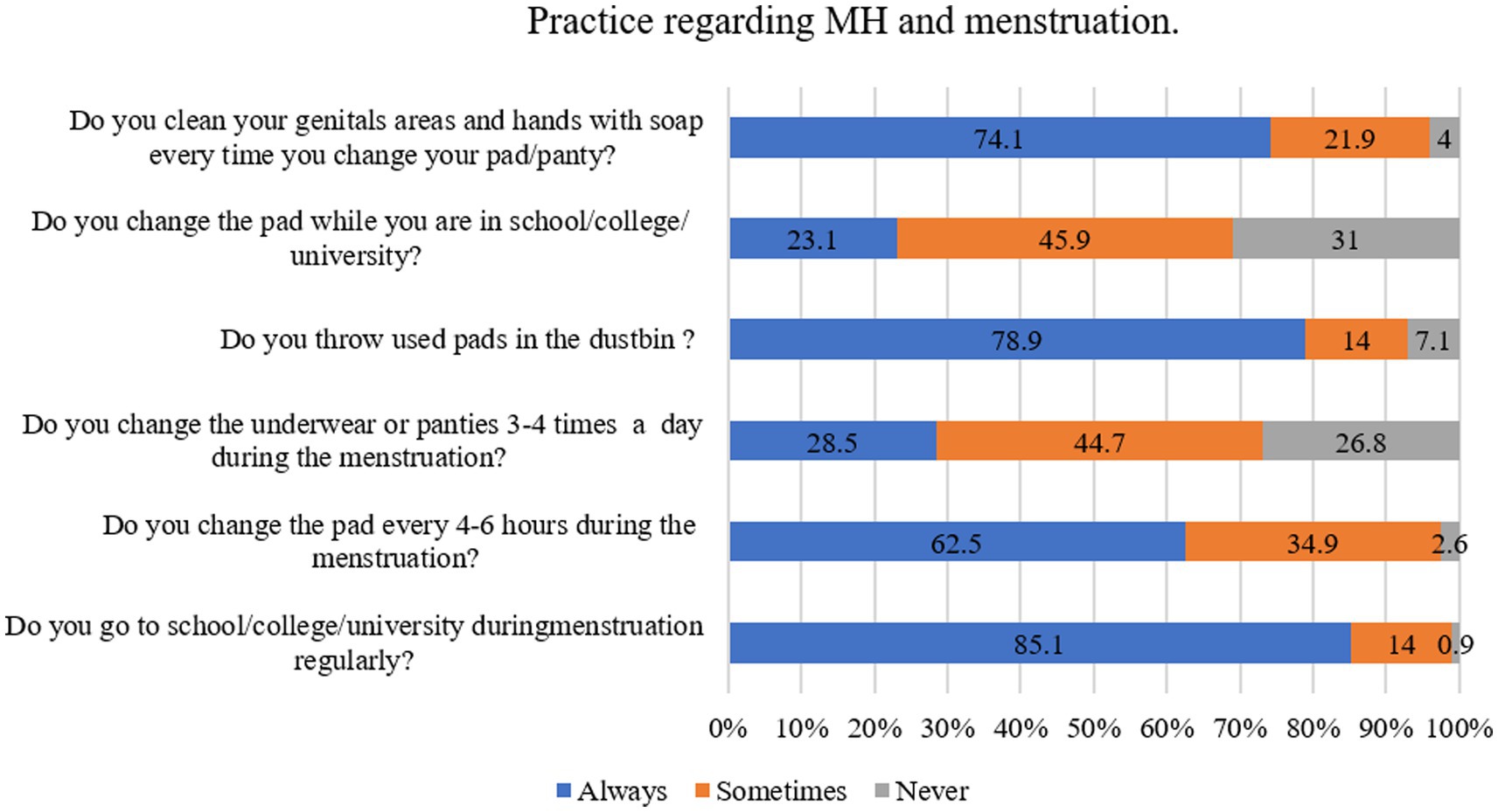
Figure 3. Practice regarding MH and menstruation.
2.5 Statistical analysis
The data were analyzed using Statistical Package for Microsoft Excel (version 2021), Social Sciences (SPSS version 25.0), and STATA (version 15.0). Cleaning, coding, and sorting were performed using the help of Microsoft Excel. Then, the Excel file was imported in the SPSS software and the descriptive statistics (i.e., frequencies, percentages, means, and standard deviations) were computed. Finally, bivariate and multivariable linear regression analyses were performed using the STATA including the total scores of knowledge, attitudes, and practices measures. A value of p less than 0.05 was regarded as significant for all of the analyses.
2.6 Ethics statement
The survey was carried out in accordance with the Helsinki Declaration of 1975. The Ethics Review Committee of the Faculty of Biological Science and Technology, Jessore University of Science and Technology, Jessore-7408, Bangladesh examined and approved the study protocol [Ref: ERC/FB ST/JUST/2022-l -0 L]. All respondents were informed of the study’s goal, procedure, and ability to withdraw their data. Prior to completing the study, each participant provided informed consent. Participants were advised that all of their information would be kept anonymous and confidential.
3 Results
3.1 General characteristics of the participants
A total of 1,214 participants were included in the final analysis. Of them, the majority were aged between 18 to 24 years (87.4%), unmarried (83.9%), had a monthly family income of more than 30,000 BDT (45.9%), and were students (87%). 91.4% had a university level of education, 79.2% were from nuclear families and 82.2% were from urban areas. Most women did not have any children (94.23%), and did not use any oral contraceptive (94.0%). 96.2% of women had normal BMI and 59.80% of women had an average daily sleeping time of 7 to 9 h. The majority reported that they did not smoke (96.8%) and did not take alcohol 97.69%. The proportion of the participants who reported using social media 2 to 5 h in a day was 58.2%. 75% of women reported that their menstrual cycle began between the ages of 12 and 14. The majority of women (76.7%) have regular menstruation, and 75.1% of them claimed their menstruation lasted between three and six days (Table 1).
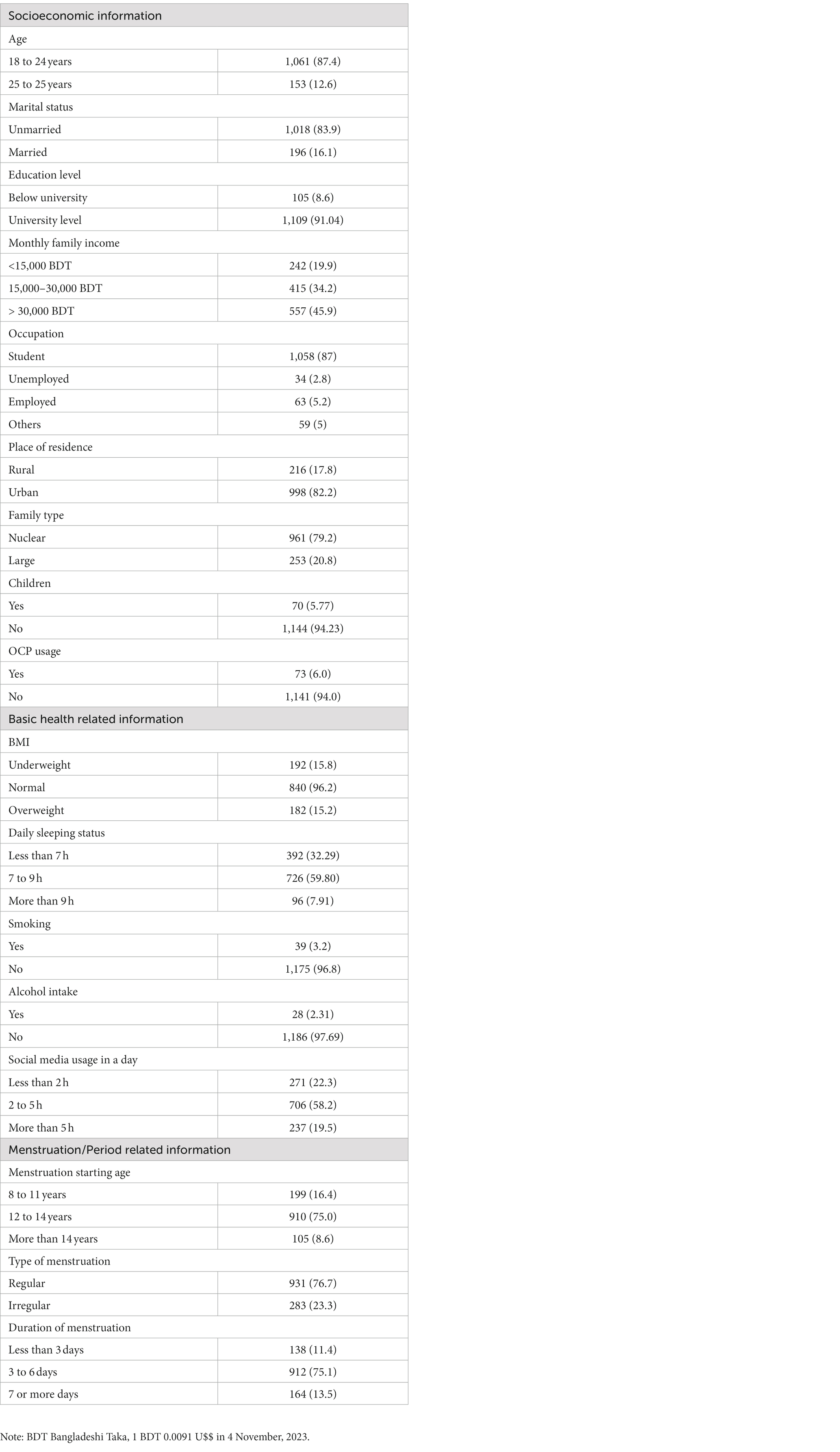
Table 1. General characteristics of the population.
3.2 Knowledge regarding menstruation and MH
The mean score of the knowledge items was 4.9 (SD = 1.51) out of 6, indicating an overall correct percentage of 81.66%. As per as multiple linear regression analysis, the positively predicting factors of knowledge score included: (i) having education at the university level (ꞵ = 0.12, p < 0.024) in reference to ‘below university’, (ii) being a student (ꞵ = 0.14, p = 0.013) in reference to ‘other occupation’, (iii) living with a nuclear/small family (ꞵ = 0.08, p = 0.003) in reference to ‘large’, (iv) having daily sleeping time of less than 7 h (ꞵ = 0.13, p = 0.017) in reference to ‘more than 9 h’, and (v) not taking alcohol (ꞵ = 0.06, p = 0.023) in reference to ‘yes’ (Table 2). Figure 4 demonstrates the sources of knowledge regarding menstruation and MH.
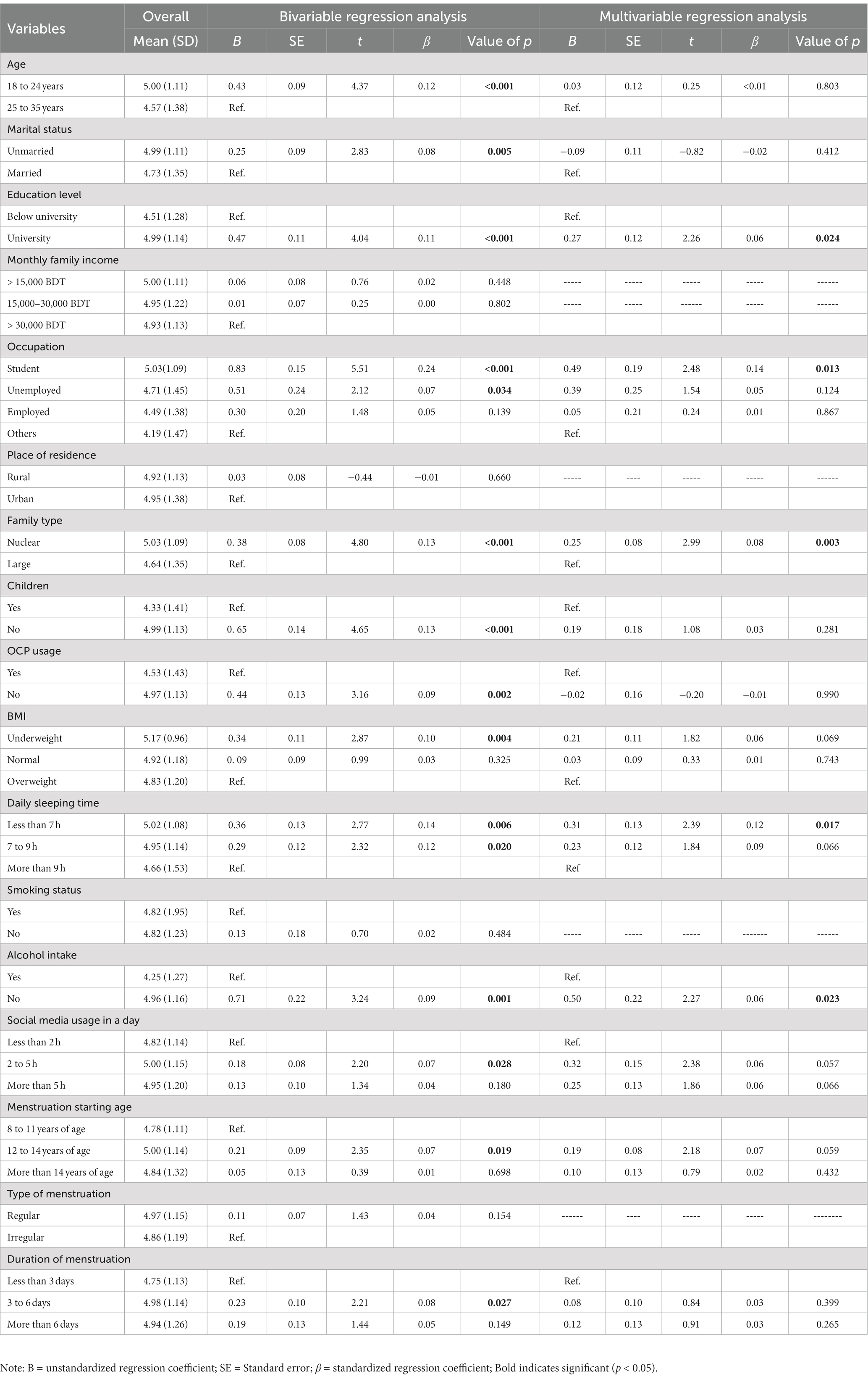
Table 2. Regression analysis predicting knowledge.
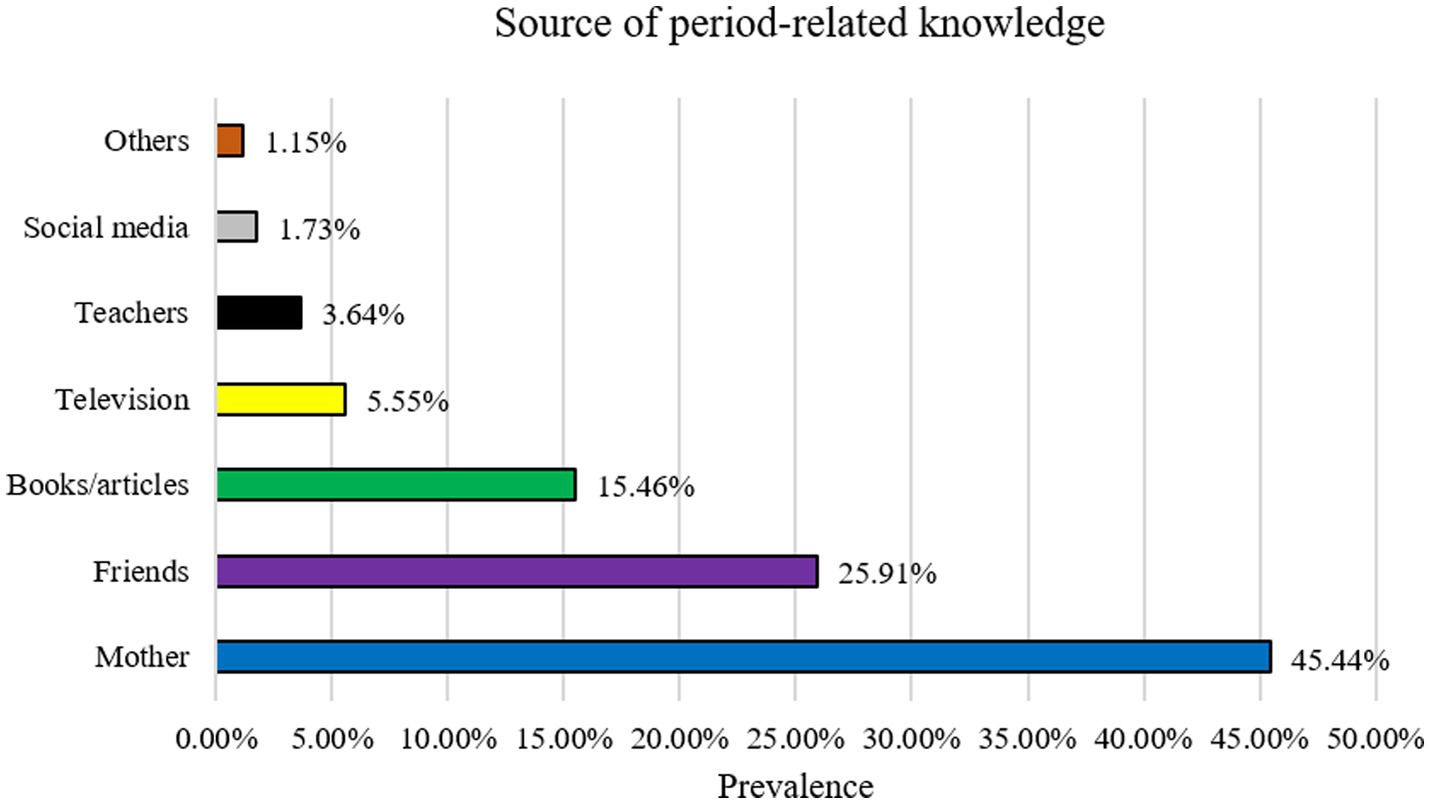
Figure 4. Source of period-related knowledge.
3.3 Attitudes regarding menstruation and MH
The mean score of the attitudes items was 12.58 (SD = 1.57) out of 14, indicating an overall correct percentage of 89.86%. As per as multiple linear regression analysis, the positively predicting factors of attitudes score included: (i) having age between 18 to 24 years (ꞵ = 0.16, p < 0.001) in reference to ‘25 to 35 years’, (ii) being a student (ꞵ = 0.13, p = 0.020) in reference to ‘other occupation’, (iii) living with a nuclear/small family (ꞵ = 0.10, p = 0.003) in reference to ‘large’, (iv) smoker (ꞵ = 0.05, p = 0.035) in reference to ‘non-smoker’, (v) not taking alcohol (ꞵ = 0.05, p = 0.035) in reference to ‘yes’, and (vi) having regular type of menstruation (ꞵ = 0.05, p = 0.002) in reference to ‘irregular’ (Table 3).
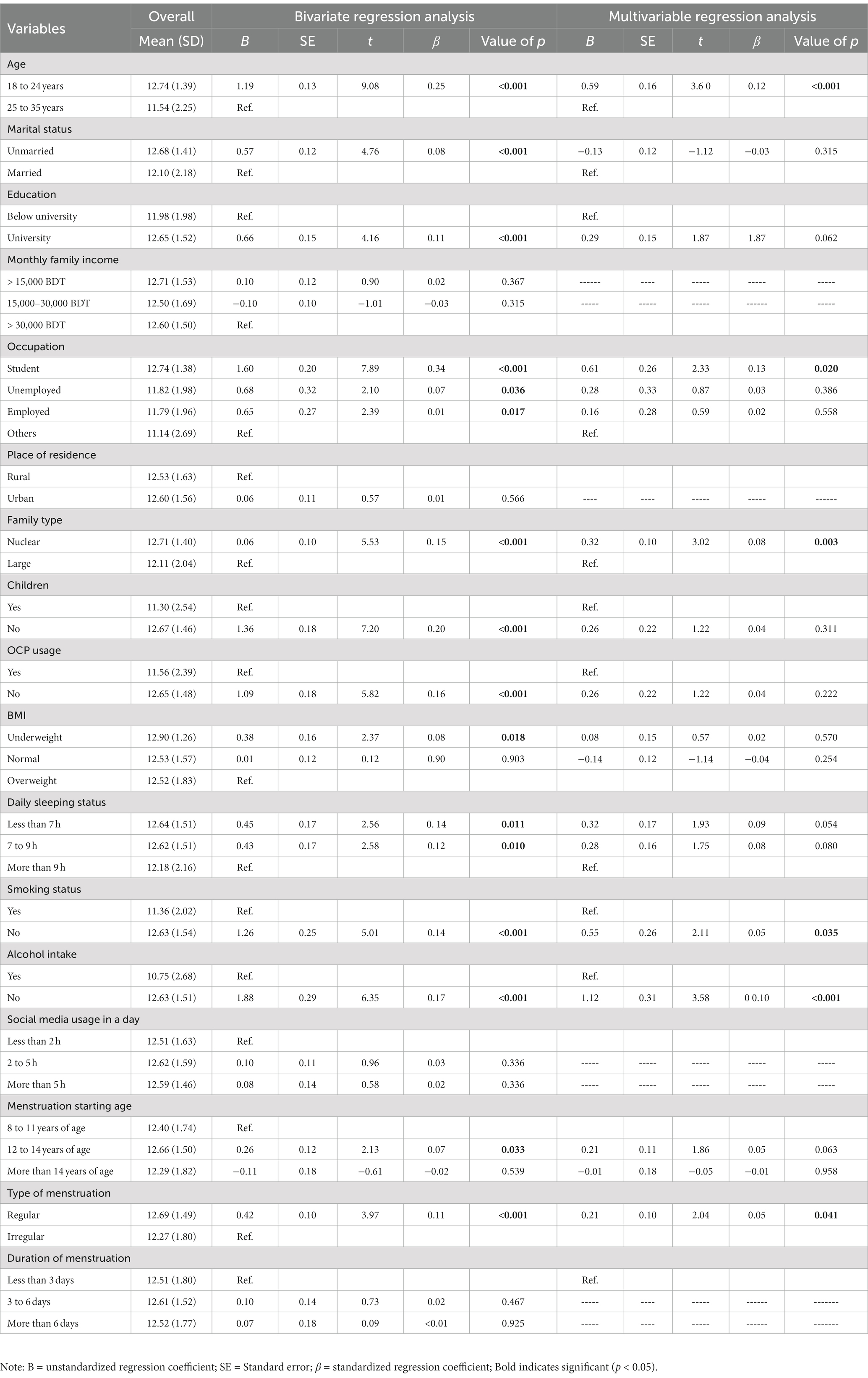
Table 3. Regression analysis predicting attitude.
3.4 Practices regarding menstruation and MH
The mean score of the practices items was 8.80 (SD = 1.87) out of 12, indicating an overall correct percentage of 73.33%.As per as multiple linear regression analysis, the positively predicting factors of attitudes score included: (i) having age between 25 to 35 years (ꞵ = 0.06, p < 0.035) in reference to ‘ss18 to 24 years’, (ii) having education at the university level (ꞵ = 0.07, p = 0.013) in reference to ‘below university’, (iii) living in an urban area (ꞵ = 0.05, p = 0.035) in reference to ‘rural’, (iv) living with a large family (ꞵ = 0.07, p = 0.010) in reference to ‘nuclear’, (v) having duration of menstruation between 3 to 6 days (ꞵ = 0.07, p = 0.032) in reference to ‘more than 6 days’ (Table 4).
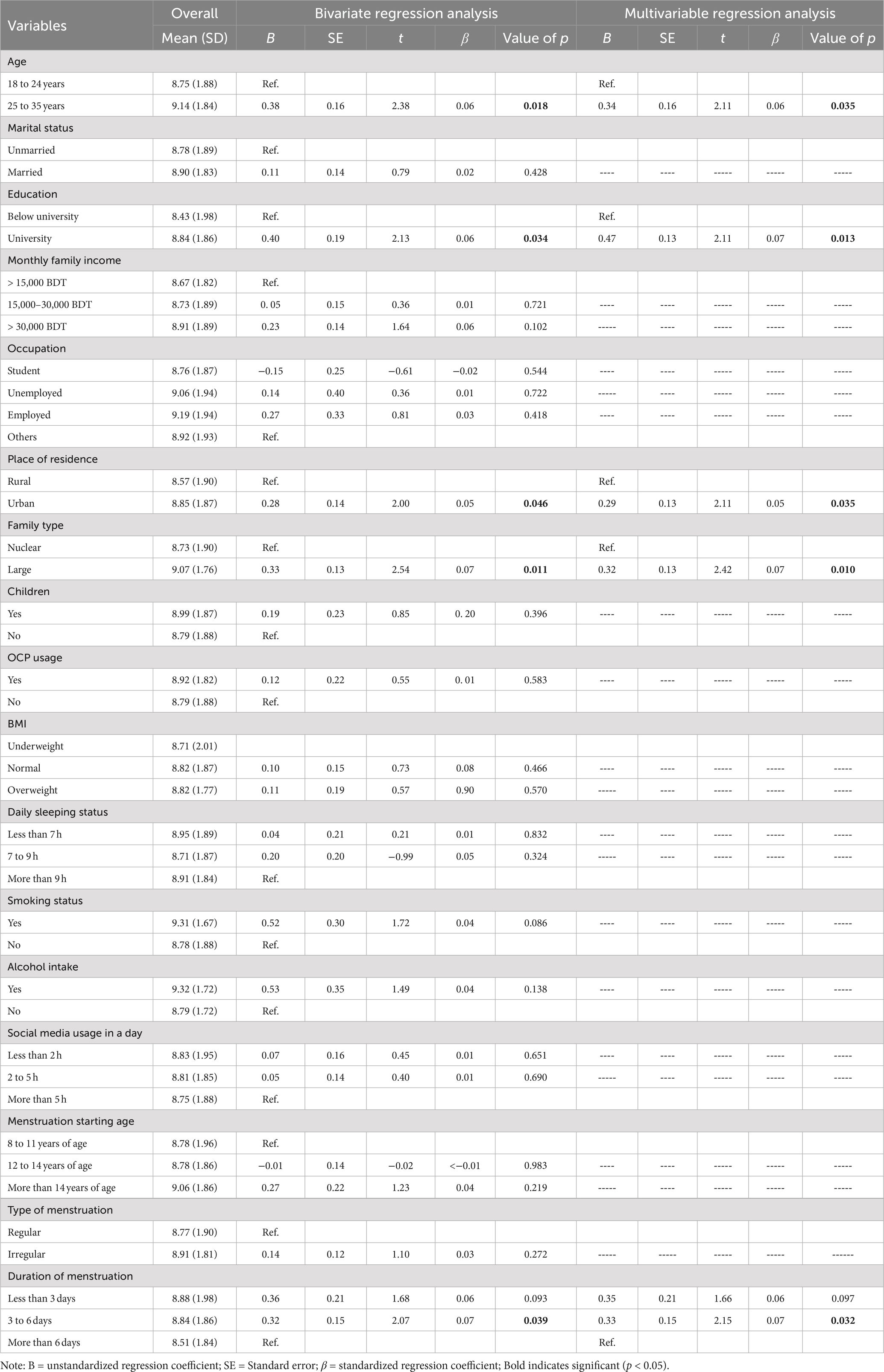
Table 4. Regression analysis predicting practice.
4 Discussion
MH management difficulties for women in low-income countries have earned global attention as a public health issue in recent years (12, 21). Bangladeshi women during their early reproductive years are exposed to significant risks of compromised menstrual health, primarily stemming from factors such as limited awareness, suboptimal MH practices, inadequate MH knowledge, and the presence of social stigma (3, 22). Therefore, the current study evaluated the knowledge, attitudes, and practices of early reproductive women in Bangladesh concerning mental health.
Based on the results presented, it can be inferred that the participants in this study had relatively good knowledge, positive attitudes, and appropriate practices regarding menstruation and MH. The predictors for higher knowledge scores were having education at the university level, being a student, living with a nuclear/small family, having daily sleeping time of less than 7 h, and not taking alcohol. For attitudes, the predictors were having age between 18 to 24 years, being a student, living with a nuclear/small family, not taking alcohol, and having regular type of menstruation. For practices, the predictors were having age between 25 to 35 years, having education at the university level, living in an urban area, living with a large family, and having a duration of menstruation between 3 to 6 days.
4.1 Comparison with other studies
The study’s findings were compared to previous research on knowledge, attitudes, and practices regarding MH among different study populations. Several studies have investigated the predictors of knowledge and attitudes toward menstruation and MH in different populations, and some of these studies have reported similar findings to the current study (20, 23).
Regarding education, a study conducted among female high school students in Nigeria found that those with higher levels of education had better knowledge and attitudes toward menstruation and MH practices (24). Similarly, a study among female university students in Malaysia reported that those with higher education levels had better knowledge and more positive attitudes toward MH (25). This is likely attributed to the awareness and knowledge fostered by higher education. Previous studies have indicated that education plays a significant role in promoting better understanding of menstruation and mental health (26, 27).
The finding that being a student is a positive predictor for both knowledge and attitudes toward menstruation and MH is consistent with previous studies. A study conducted among urban women in India found that being a student was significantly associated with better knowledge and attitudes toward MH practices (28). Another study among female high school students in Nepal reported that students had better knowledge and more positive attitudes toward MH than non-students (20). The new Bangladeshi curriculum offers improved access to comprehensive sexual and reproductive health education, particularly benefiting students who now receive information about proper menstrual hygiene practices (29).
The current study also found that living with a nuclear/small family was a positive predictor of both knowledge and attitudes toward menstruation and MH. This finding is consistent with a study among adolescent girls in Ghana, which reported that girls from nuclear families had better knowledge and more positive attitudes toward MH than those from extended families (30) because of the focused attention and education they receive within smaller family units, which allows for better guidance and awareness-building on this subject (31).
Our study found sleep status less than 7 h is a positive predicting factor of MH related knowledge. Excessive sleep or disrupted sleep patterns can hinder cognitive functioning and concentration, potentially leading to reduced attention to menstrual hygiene education and challenges in establishing consistent hygiene habits due to disrupted daily routine (32, 33). Further study is needed for more clarification.
The finding that not taking alcohol is a positive predictor of both knowledge and attitudes toward menstruation and MH. Excessive alcohol consumption can impair cognitive functions and decision-making abilities, potentially leading to misinformation or neglect of proper menstrual hygiene practices, while also diminishing the importance placed on menstrual health and hygiene due to its effects on mood and judgment (34, 35).
In terms of attitudes, the finding that having age between 18 to 24 years is a positive predictor is consistent with a study among women at Delhi in India, which reported that younger women had more positive attitudes toward MH than older (28). The finding that having regular type of menstruation is a positive predictor of attitudes toward menstruation and MH is consistent with a study among girls in India, which reported that those with regular menstrual cycles had more positive attitudes toward MH (36).
The finding that residing in a nuclear or small family positively predicts favorable attitudes toward menstruation and menstrual hygiene is intriguing. This could be attributed to the possibility that women in smaller families have increased opportunities for discussing menstruation and menstrual hygiene with family members, resulting in higher levels of knowledge and comprehension (37). Opposite result was found in a study conducted among adolescent girls of a urban slum in Assam, India (38). Overall, these findings suggest that there are certain demographic and behavioral factors that may influence attitudes toward menstruation and MH, and that interventions targeting these factors may be effective in improving attitudes and promoting menstrual health.
Regarding age, some studies have found that younger women tend to have better MH practices compared to older women, while others have found the opposite. For instance, a study conducted in India found that younger women were more likely to use sanitary pads, dispose of them properly, and wash their genitals during menstruation compared to older women (39). On the other hand, a study conducted in Korea found no association between age and MH practices (40). Younger generations tend to have increased access to comprehensive sexual and reproductive health education by new Bangladeshi curriculum, which includes information on proper MH practices (29).
Regarding education level, the findings of this study are consistent with previous research that found higher education to be associated with better MH practices (5). It is quite usual that higher education teaches us to be clean and healthy. The finding that living in an urban area is a positive predictor of appropriate practices is consistent with some studies that have found that urban women tend to have better MH practices compared to rural women (4).
According to our study living with a large family is a positive predictor of appropriate practices is in line with an Indian study (38). Because in Bangladeshi culture grandparents have a funny and interesting relationship with their grandchildren. Usually they teach grandchildren abut MH practices and sex education (41). It contradicts with an Ethiopian study that have found that living in smaller families is associated with better MH practices (15). Moreover, A Bangladeshi study found no association between good MH practices and family size (42).
According to our findings, Mother, Friends, Books/articles, Television, teacher, and social media were mentioned to be used as a common source of obtaining information about Menstruation and MH. Mother was reported as the most frequently used source of gaining knowledge regarding menstruation which is consistent with an earlier study from Bangladesh (42). Prior study related to our finding which depicted that people prefer having MH related information from close one like mother and best friends but they usually do not like to share these incidences in social media (Facebook, WhatsApp, etc.) (43, 44).
Overall, the study reveals that early reproductive-aged women in Bangladesh generally possess good knowledge, positive attitudes, and appropriate practices regarding menstrual hygiene. Factors such as higher education, student status, living in nuclear/small families, adequate sleep, and not consuming alcohol are associated with better knowledge and attitudes. This information can guide policymakers and planners in developing targeted interventions to further improve menstrual hygiene practices and promote women’s reproductive health, aligning with sustainable development goals related to water and sanitation, health, and gender equality.
4.2 Limitations
The study has several limitations that should be acknowledged. Firstly, the use of convenience sampling may introduce selection bias and limit the generalizability of the findings to the broader population. Secondly, collected data can be subject to recall bias/response and social desirability bias, potentially affecting the accuracy of responses because of self-reported measures. Additionally, the cross-sectional design of the study prevents establishing causal relationships and understanding changes over time. A longitudinal or prospective study will be helpful in this context. Moreover, the lack of a comparison group and limited generalizability to other regions or countries restricts the applicability of the findings. It is important to consider these limitations when interpreting the results and drawing conclusions.
5 Conclusion
In conclusion, this study highlights the need for targeted interventions that address the gaps in knowledge and practices related to MH among women. Efforts to improve MH practices should focus not only on educating women but also on addressing the social and environmental factors that influence these practices. Such interventions could include school-based education programs, community-based awareness campaigns, and policies that promote access to affordable MH products.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The survey was carried out in accordance with the Helsinki Declaration of 1975. The Ethics Review Committee of the Faculty of Biological Science and Technology, Jessore University of Science and Technology, Jessore-7408, Bangladesh examined and approved the study protocol [Ref: ERC/FB ST/JUST/2022-l -0l]. All respondents were informed of the study’s goal, procedure, and ability to withdraw their data. Prior to completing the study, each participant provided informed written consent. Participants were advised that all of their information would be kept anonymous and confidential.
Author contributions
AS, MM, and MA: conceptualization. AS, SD, MM, and MA: methodology and resources. AS and SD: data curation, formal analysis, and investigation. AS, SD, AA, SM, MH, and AP: writing – original draft preparation. MM and MA: writing – review and editing and supervision. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors would like to express the most profound gratitude to all of the respondents who participated in this study. Additionally, authors also would like to thank all the research assistants for helping data collection voluntarily: Asha Afrin, Drishti Deb Nath, Jannatul Arobia, Mst Murshida Khatun, Nayema Suchana, Pranti Chowdhury, Shabnaj Mustari, Shumaiya Shammmi Bili, and Zhilik Das.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1238290/full#supplementary-material
References
1. Sweet, MG, Schmidt-Dalton, TA, Weiss, PM, and Madsen, KP. Evaluation and management of abnormal uterine bleeding in premenopausal women. Am Fam Physician. (2012) 85:35–43.
2. Madziyire, MG, Magure, TM, and Madziwa, CF. Menstrual cups as a menstrual management method for low socioeconomic status women and girls in Zimbabwe: a pilot study. Women’s Reprod Heal. (2018) 5:59–65. doi: 10.1080/23293691.2018.1429371
3. Balqis, M, Arya, IFD, and Ritonga, MNA. Knowledge, attitude and practice of menstrual hygiene among high schools students in Jatinangor. Althea Med J. (2016) 3:230–8. doi: 10.15850/amj.v3n2.783
4. Das, P, Baker, KK, Dutta, A, Swain, T, Sahoo, S, das, BS, et al. Menstrual hygiene practices, WASH access and the risk of urogenital infection in women from Odisha, India. PLoS One. (2015) 10:e0130777. doi: 10.1371/journal.pone.0130777
5. Torondel, B, Sinha, S, Mohanty, JR, Swain, T, Sahoo, P, Panda, B, et al. Association between unhygienic menstrual management practices and prevalence of lower reproductive tract infections: a hospital-based cross-sectional study in Odisha, India. BMC Infect Dis. (2018) 18:473. doi: 10.1186/s12879-018-3384-2
6. Sahiledengle, B, Atlaw, D, Kumie, A, Tekalegn, Y, Woldeyohannes, D, and Agho, KE. Menstrual hygiene practice among adolescent girls in Ethiopia: a systematic review and meta-analysis. PLoS One. (2022) 17:e0262295. doi: 10.1371/journal.pone.0262295
7. Janoowalla, H, Keppler, H, Asanti, D, Xie, X, Negassa, A, Benfield, N, et al. The impact of menstrual hygiene management on adolescent health: the effect of go! Pads on rate of urinary tract infection in adolescent females in Kibogora, Rwanda. Int J Gynaecol Obstet. (2020) 148:87–95. doi: 10.1002/ijgo.12983
8. Ademas, A, Adane, M, Sisay, T, Kloos, H, Eneyew, B, Keleb, A, et al. Does menstrual hygiene management and water, sanitation, and hygiene predict reproductive tract infections among reproductive women in urban areas in Ethiopia? PLoS One. (2020) 15:e0237696. doi: 10.1371/journal.pone.0237696
9. Alam, M-U, Sultana, F, Hunter, EC, Winch, PJ, Unicomb, L, Sarker, S, et al. Evaluation of a menstrual hygiene intervention in urban and rural schools in Bangladesh: a pilot study. BMC Public Health. (2022) 22:1100. doi: 10.1186/s12889-022-13478-1
10. Sumpter, C, and Torondel, B. A systematic review of the health and social effects of menstrual hygiene management. PLoS One. (2013) 8:e62004. doi: 10.1371/journal.pone.0062004
11. Kaur, R, Kaur, K, and Kaur, R. Menstrual hygiene, management, and waste disposal: practices and challenges faced by girls/women of developing countries. J Environ Public Health. (2018) 2018:1730964–9. doi: 10.1155/2018/1730964
12. Patel, K, Panda, N, Sahoo, KC, Saxena, S, Chouhan, NS, Singh, P, et al. A systematic review of menstrual hygiene management (MHM) during humanitarian crises and/or emergencies in low- and middle-income countries. Front Public Health. (2022) 10:1018092. doi: 10.3389/fpubh.2022.1018092
13. Mehjabeen, D, Hunter, EC, Mahfuz, MT, Mobashara, M, Rahman, M, and Sultana, F. A qualitative content analysis of rural and Urban School students’ menstruation-related questions in Bangladesh. Int J Environ Res Public Health. (2022) 19:140. doi: 10.3390/ijerph191610140
14. UNICEF. (2019). Guidance on menstrual health and hygiene. Available at: https://www.unicef.org/documents/guidance-menstrual-health-and-hygiene. (Accessed April 4, 2023).
15. Belayneh, Z, and Mekuriaw, B. Knowledge and menstrual hygiene practice among adolescent school girls in southern Ethiopia: a cross-sectional study. BMC Public Health. (2019) 19:1595. doi: 10.1186/s12889-019-7973-9
16. Siddique, AB, Nath, SD, Islam, MS, Khan, TH, Pardhan, S, Amin, MZ, et al. Financial difficulties correlate with mental health among Bangladeshi residents amid COVID-19 pandemic: findings from a cross-sectional survey. Front Psych. (2021) 12:1–10. doi: 10.3389/fpsyt.2021.755357
17. Svetlana, E, Natalia, A, and Anzhelika, B. Indicators of an ovarian reserve in women of early reproductive age with PCOS depending on the phenotype. Horm Mol Biol Clin Investig. (2019) 39:5–13. doi: 10.1515/hmbci-2018-0081
18. Sharma, N, Sharma, P, Sharma, N, Wavare, RR, Gautam, B, and Sharma, M. A cross sectional study of knowledge, attitude and practices of menstrual hygiene among medical students in North India. J Phytopharm. (2013) 2:28–37. doi: 10.31254/phyto.2013.2505
19. Fehintola, FO, Fehintola, AO, Aremu, AO, Idowu, A, Ogunlaja, OA, and Ogunlaja, IP. Assessment of knowledge, attitude and practice about menstruation and menstrual hygiene among secondary high school girls in Ogbomoso, Oyo state, Nigeria. Int J Reprod Contraception Obstet Gynecol. (2017) 6:1726. doi: 10.18203/2320-1770.ijrcog20171932
20. Yadav, RN, Joshi, S, Poudel, R, and Pandeya, P. Knowledge, attitude, and practice on menstrual hygiene management among school adolescents. J Nepal Health Res Counc. (2018) 15:212–6. doi: 10.3126/jnhrc.v15i3.18842
21. Nwankwo, ONO, Mokogwu, N, Agboghoroma, O, Ahmed, FO, and Mortimer, K. Knowledge, attitudes and beliefs about the health hazards of biomass smoke exposure amongst commercial food vendors in Nigeria. PLoS One. (2018) 13:e0191458–14. doi: 10.1371/journal.pone.0191458
22. Alam, M-U, Luby, SP, Halder, AK, Islam, K, Opel, A, Shoab, AK, et al. Menstrual hygiene management among Bangladeshi adolescent schoolgirls and risk factors affecting school absence: results from a cross-sectional survey. BMJ Open. (2017) 7:e015508. doi: 10.1136/bmjopen-2016-015508
23. Marván, ML, and Alcalá-Herrera, V. Age at menarche, reactions to menarche and attitudes towards menstruation among Mexican adolescent girls. J Pediatr Adolesc Gynecol. (2014) 27:61–6. doi: 10.1016/j.jpag.2013.06.021
24. Nnennaya, EU, Atinge, S, Dogara, SP, and Ubandoma, RJ. Menstrual hygiene management among adolescent school girls in Taraba state, Nigeria. Afr Health Sci. (2021) 21:842–51. doi: 10.4314/ahs.v21i2.45
25. Al Ajeel, LY, Chong, MC, Tang, LY, Wong, LP, and Al Raimi, AM. The effect of health education on knowledge and self-care among Arabic schoolgirls with primary dysmenorrhea in Malaysia. J Nurse Pract. (2020) 16:762–7. doi: 10.1016/j.nurpra.2020.07.025
26. Ameade, EPK, and Garti, HA. Relationship between female university students’ knowledge on menstruation and their menstrual hygiene practices: a study in tamale, Ghana. Adv Prev Med. (2016) 2016:1–10. doi: 10.1155/2016/1056235
27. Mohammed, S, and Larsen-Reindorf, RE. Menstrual knowledge, sociocultural restrictions, and barriers to menstrual hygiene management in Ghana: evidence from a multi-method survey among adolescent schoolgirls and schoolboys. PLoS One. (2020) 15:e0241106. doi: 10.1371/journal.pone.0241106
28. Goel, P, Kumar, R, Meena, GS, and Garg, S. Association of sociodemographic characteristics with KAP regarding menstrual hygiene among women in an urban area in Delhi. Trop J Obstet Gynaecol. (2018) 35:158–64. doi: 10.4103/TJOG.TJOG_58_17
29. Du, KC, Mohosin, AB, Amin, A, and Hasan, MT. Influence of education on sexual and reproductive health service utilization for persons with disabilities in nationwide Bangladesh: an explanatory sequential mixed-methods study. Reprod Health. (2022) 19:46. doi: 10.1186/s12978-022-01352-7
30. Boakye-Yiadom, A, Aladago, DA, Beweleyir, J, Mohammed, HB, Salifu, MF, and Asaarik, M. Assessing the knowledge, attitude and practice of menstrual hygiene management among junior high schools adolescent females in the Yendi municipality in the northern region of Ghana. Eur Sci J. (2018) 14:467. doi: 10.19044/esj.2018.v14n36p467
31. Sharma, S, Mehra, D, Kohli, C, Singh, MM, Shantanu, S, and Mehra, D. Menstrual hygiene practices among adolescent girls in a resettlement colony of Delhi: a cross-sectional study. Int J Reprod Contracept Obs Gynecol. (2017) 6:1945–51. doi: 10.18203/2320-1770.ijrcog20171954
32. Kolovos, S, Jimenez-Moreno, AC, Pinedo-Villanueva, R, Cassidy, S, and Zavala, GA. Association of sleep, screen time and physical activity with overweight and obesity in Mexico. Eat Weight Disord. (2021) 26:169–79. doi: 10.1007/s40519-019-00841-2
33. Nowakowski, S, Meers, J, and Heimbach, E. Sleep and Women’s health. Sleep Med Res. (2013) 4:1–22. doi: 10.17241/smr.2013.4.1.1
34. Ahmed Shallo, S, Willi, W, and Abubeker, A. Factors affecting menstrual hygiene management practice among school adolescents in ambo, Western Ethiopia, 2018: a cross-sectional mixed-method study. Risk Manag Healthc Policy. (2020) 13:1579–87. doi: 10.2147/RMHP.S267534
35. Carroll, HA, Lustyk, MKB, and Larimer, ME. The relationship between alcohol consumption and menstrual cycle: a review of the literature. Arch Womens Ment Health. (2015) 18:773–81. doi: 10.1007/s00737-015-0568-2
36. Hoerster, KD, Chrisler, JC, and Rose, JG. Attitudes toward and experience with menstruation in the US and India. Women Health. (2003) 38:77–95. doi: 10.1300/J013v38n03_06
37. Deshpande, TN, Patil, SS, Gharai, SB, Patil, SR, and Durgawale, PM. Menstrual hygiene among adolescent girls – a study from urban slum area. J Fam Med Prim Care. (2018) 7:1439–45. doi: 10.4103/jfmpc.jfmpc_80_18
38. Sonowal, P, Talukdar, K, and Saikia, H. Sociodemographic factors and their association with menstrual hygiene practices among adolescent girls in urban slums of Dibrugarh town, Assam. J Fam Med Prim care. (2021) 10:4446–51. doi: 10.4103/jfmpc.jfmpc_703_21
39. Roy, A, Paul, P, Saha, J, Barman, B, Kapasia, N, and Chouhan, P. Prevalence and correlates of menstrual hygiene practices among young currently married women aged 15-24 years: an analysis from a nationally representative survey of India. Eur J Contracept Reprod Heal Care. (2021) 26:1–10. doi: 10.1080/13625187.2020.1810227
40. Choi, H, Lim, N-K, Jung, H, Kim, O, and Park, H-Y. Use of menstrual sanitary products in women of reproductive age: Korea nurses’ health study. Osong public Heal Res Perspect. (2021) 12:20–8. doi: 10.24171/j.phrp.2021.12.1.04
41. Yusuf, M. Grandparents as educators: a study of socio-cultural and religion perspectives. Procedia Soc Behav Sci. (2014) 140:337–42. doi: 10.1016/j.sbspro.2014.04.431
42. Ha, MAT, and Alam, MZ. Menstrual hygiene management practice among adolescent girls: an urban-rural comparative study in Rajshahi division, Bangladesh. BMC Womens Health. (2022) 22:86. doi: 10.1186/s12905-022-01665-6
43. Sooki, Z, Shariati, M, Chaman, R, Khosravi, A, Effatpanah, M, and Keramat, A. The role of mother in informing girls about puberty: a meta-analysis study. Nurs Midwifery Stud. (2016) Inpress:e30360. doi: 10.17795/nmsjournal30360
Keywords: menstruation, menstrual hygiene, knowledge, attitudes, practices, health effect, Bangladesh, early-reproductive age
Citation: Siddique AB, Deb Nath S, Mubarak M, Akter A, Mehrin S, Hkatun MJ, Parvine Liza A and Amin MZ (2023) Assessment of knowledge, attitudes, and practices regarding menstruation and menstrual hygiene among early-reproductive aged women in Bangladesh: a cross-sectional survey. Front. Public Health. 11:1238290. doi: 10.3389/fpubh.2023.1238290
Edited by:
Chakema Carmack, University of Houston, United StatesReviewed by:
Lindsay Kelland, Rhodes University, South AfricaKshitij Karki, G.T.A. Foundation, Nepal
Shobha Shah, SEWA Rural, India
Copyright © 2023 Siddique, Deb Nath, Mubarak, Akter, Mehrin, Hkatun, Parvine Liza and Amin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abu Bakkar Siddique, YWJ1YmFra2Fyc2FtcmF0MTAxMEBnbWFpbC5jb20=
†ORCID: Abu Bakkar Siddique https://orcid.org/0000-0002-1573-8281