
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 06 September 2023
Sec. Public Health and Nutrition
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1223111
This article is part of the Research Topic Nutrition in the Prevention and Treatment of Cardiovascular Diseases View all 11 articles
 Adrian Kwaśny1
Adrian Kwaśny1 Katarzyna Łokieć2
Katarzyna Łokieć2 Bartosz Uchmanowicz3
Bartosz Uchmanowicz3 Agnieszka Młynarska4
Agnieszka Młynarska4 Jacek Smereka5*
Jacek Smereka5* Michał Czapla5,6,7
Michał Czapla5,6,7Background: Nutritional status is related to the length of hospitalization of patients with atrial fibrillation (AF). The aim of this study is to assess the prognostic impact of nutritional status and body mass index on length of hospital stay (LOHS) among patients with AF relative to their sex.
Methods: A retrospective analysis of the medical records of 1,342 patients admitted urgently with a diagnosis of AF (ICD10: I48) to the Cardiology Department (University Hospital in Wroclaw, Poland) between January 2017 and June 2021.
Results: In the study group, women were significantly older than men (72.94 ± 9.56 vs. 65.11 ± 12.68, p < 0.001). In an unadjusted linear regression model, malnutrition risk was a significant independent predictor of prolonged hospitalization in men (B = 1.95, p = 0.003) but not in women. In the age-adjusted linear regression model, malnutrition risk was a significant independent predictor of prolonged hospitalization in men (B = 1.843, p = 0.005) but not in women. In the model adjusted for age and comorbidities, malnutrition risk was a significant independent predictor of prolonged hospitalization in men only (B = 1.285, p = 0.043). In none of the models was BMI score a predictor of LOHS in either sex.
Conclusion: The risk of malnutrition directly predicts the length of hospital stays in men but not women. The study did not find a relationship between body mass index and length of hospital stay in both women and men.
Atrial fibrillation (AF) is estimated to affect about 2–4% of the adult population, and the incidence is projected to continue to increase up to 4-fold by 2050 (1–3). Both malnutrition and overweight and obesity are challenges to modern public health in developed and developing countries (4). Excess body weight is associated with high cardiovascular risk, risk of prolonged hospitalization and mortality (5–7). Despite knowledge on the subject, malnutrition remains one of the most common causes of death in developing countries. In 70% of cases, nutritional deterioration occurs during hospitalization (8, 9). Several publications indicate an association between AF incidence and overweight and obesity. Studies show a relationship between AF risk and body weight; overweight and underweight were associated with higher arrhythmia events during the follow-up period. It was confirmed that body mass index (BMI), waist circumference, hip circumference and body surface area, among others, were independent predictors of atrial fibrillation (10–12). Thacker et al. observed that higher BMI was an independent factor in arrhythmia progression from paroxysmal or persistent AF to fixed AF, in contrast to other factors (13). Also, a higher BMI score is an independent factor in the progression of arrhythmias from paroxysmal to sustained atrial fibrillation, in contrast to other cardiovascular risk factors (14). Pathak et al. showed that a 10% weight loss in obese patients resulted in a sixfold greater likelihood of maintaining sinus rhythm than patients with no change in body weight values (15). Although some researchers have described a phenomenon occurring among AF patients called the “obesity paradox” concerning deaths from all causes and those from cardiovascular causes, there is an inverse relationship between overweight/obesity and better cardiovascular prognosis at long-term follow-up (16, 17). There are studies showing gender differences in AF (18, 19). However, data on the relationship between nutritional status, gender and length of hospitalization in AF are scarce. This thread has not been sufficiently explored, justifying the need for such observations.
The aim of this study is to assess the prognostic impact of NRS-2002 and body mass index on length of hospital stay (LOHS) among patients with AF relative to their sex.
A retrospective analysis of the medical records of 1,342 patients admitted urgently with a diagnosis of AF (ICD10: I48) to the Cardiology Department (Institute of Heart Diseases, University Hospital in Wroclaw, Poland) between January 2017 and June 2021 was conducted.
Medical records of all patients who met the following inclusion criteria were included in the analysis: emergency admission to the cardiology department for AF (primary reason for hospital admission), BMI and Nutritional Risk Screening 2002 (NRS-2002) score noted in medical records at the time of admission, age ≥18 years old. Finally, data from 1,342 patients were analyzed, such as NRS-2002 score, Body Mass Index (BMI) score, comorbidities: heart failure (HF), chronic kidney disease (CKD), arterial hypertension (HT), diabetes mellitus (DM), thyroid disease (TD), history of cerebral stroke; acute coronary syndrome (ACS) and length of hospital stay (LOHS). Comorbidities and past medical conditions have been recorded by a doctor in the patient’s medical record when the patient is admitted to the hospital.
Risk of malnutrition was assessed using the screening tools NRS-2002 (20). This tool assesses impaired nutritional status (0–3 points) and severity of disease (0–3 points). If the patient’s age ≥70 years, the patient receives 1 point more. The risk of malnutrition was found when the patient received ≥3 points (20). The WHO criteria for indicating nutritional status are used to classify patients as obese (BMI ≥ 30), pre-obese (BMI 25–29.9), normal body weight (BMI 18.5–24.9), and underweight (BMI < 18.5) (21). Both the NRS-2002 and the BMI score were assessed and recorded in the patient’s medical record by the physician at the time of admission to the hospital.
The study was conducted following the principles of the Declaration of Helsinki and approved by the independent Bioethics Committee of Wroclaw Medical University, protocol no. KB-837/2022. The study followed the STROBE guidelines (Strengthening the Reporting of Observational Studies in Epidemiology).
Distributions of quantitative variables were summarized with mean, standard deviation, median and quartiles. In contrast, distributions of qualitative variables were summarized with the number and percent of occurrence for each value. Chi-squared test (with Yates’ correction for 2 × 2 tables) was used to compare qualitative variables among groups. In the case of low values in contingency tables, Fisher’s exact test was used instead. Mann–Whitney test was used to compare quantitative variables between two groups. Logistic regression was used to analyze the impact of quantitative variables on dichotomous outcomes. All clinical variables recorded in medical records at hospital admission were used to construct a multivariate model. Odds ratios (OR) with 95% confidence intervals were shown. The significance level for all statistical tests was set to 0.05. R 4.2.2. was used for computations.
All 1,342 patients were included in the analysis. In the first step, a comparison was made concerning gender. A comparison of the groups by gender is shown in Table 1. Women were significantly older than men (72.94 ± 9.56 vs. 65.11 ± 12.68, p < 0.001). Women were also significantly more likely than men to suffer from CKD, thyroid disease and stroke history. This group also had a higher risk of malnutrition (11.09% vs. 3.99%, p < 0.001).
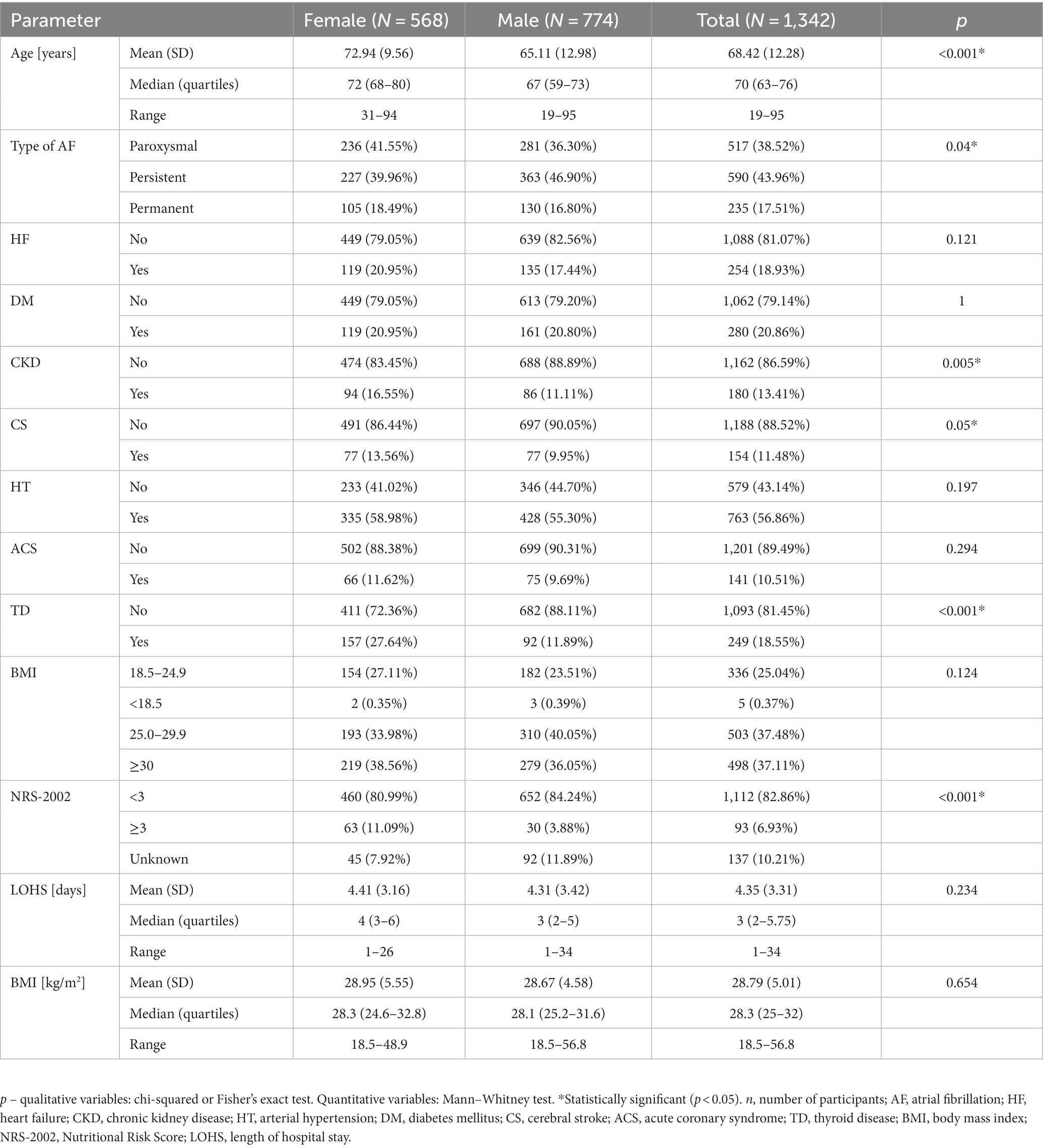
Table 1. Comparison of patient characteristics by sex.
Patients of each gender were divided into two groups according to WHO criteria: obese (BMI ≥ 30) and non-obese (BMI < 30). Women with obesity were significantly more likely to be younger and have DM compared to women in the non-obese group. Women with obesity were significantly less likely to have CKD, CS and less likely to have malnutrition risk, according to NRS-2002, compared to the obese group. Obese men were significantly younger than non-obese men. Obese men were less often at risk in malnutrition (Table 2).
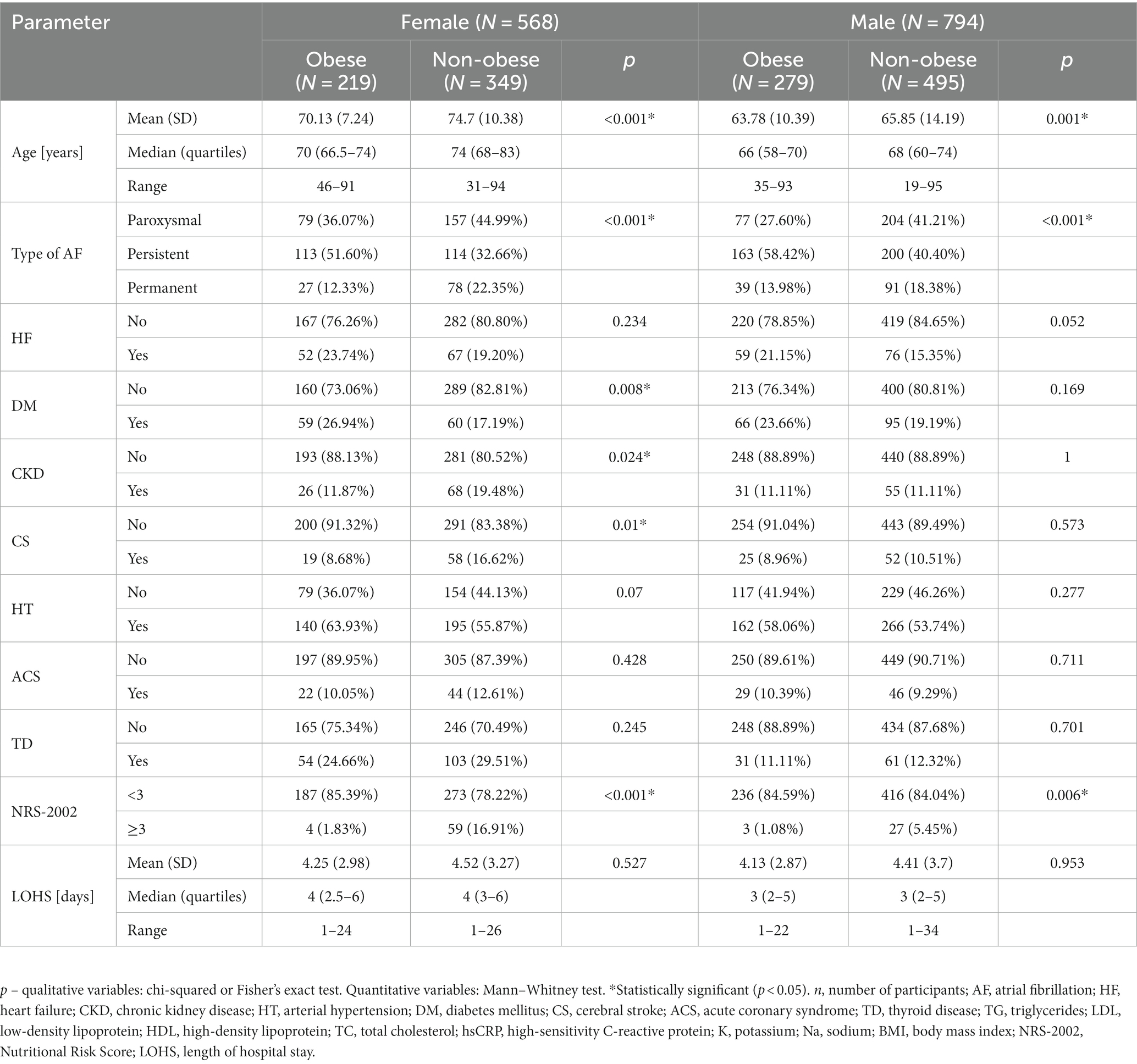
Table 2. Comparison of patient characteristics by absence or presence of obesity.
Women at risk for malnutrition were significantly older. They also were more likely to have CKD and less likely to have HT and TD, and had a lower BMI compared to the group without malnutrition risk. Men at risk of malnutrition were less likely to have diseases such as DM and HT. Men in this group also lower BMIs than men at no malnutrition risk (Table 3).
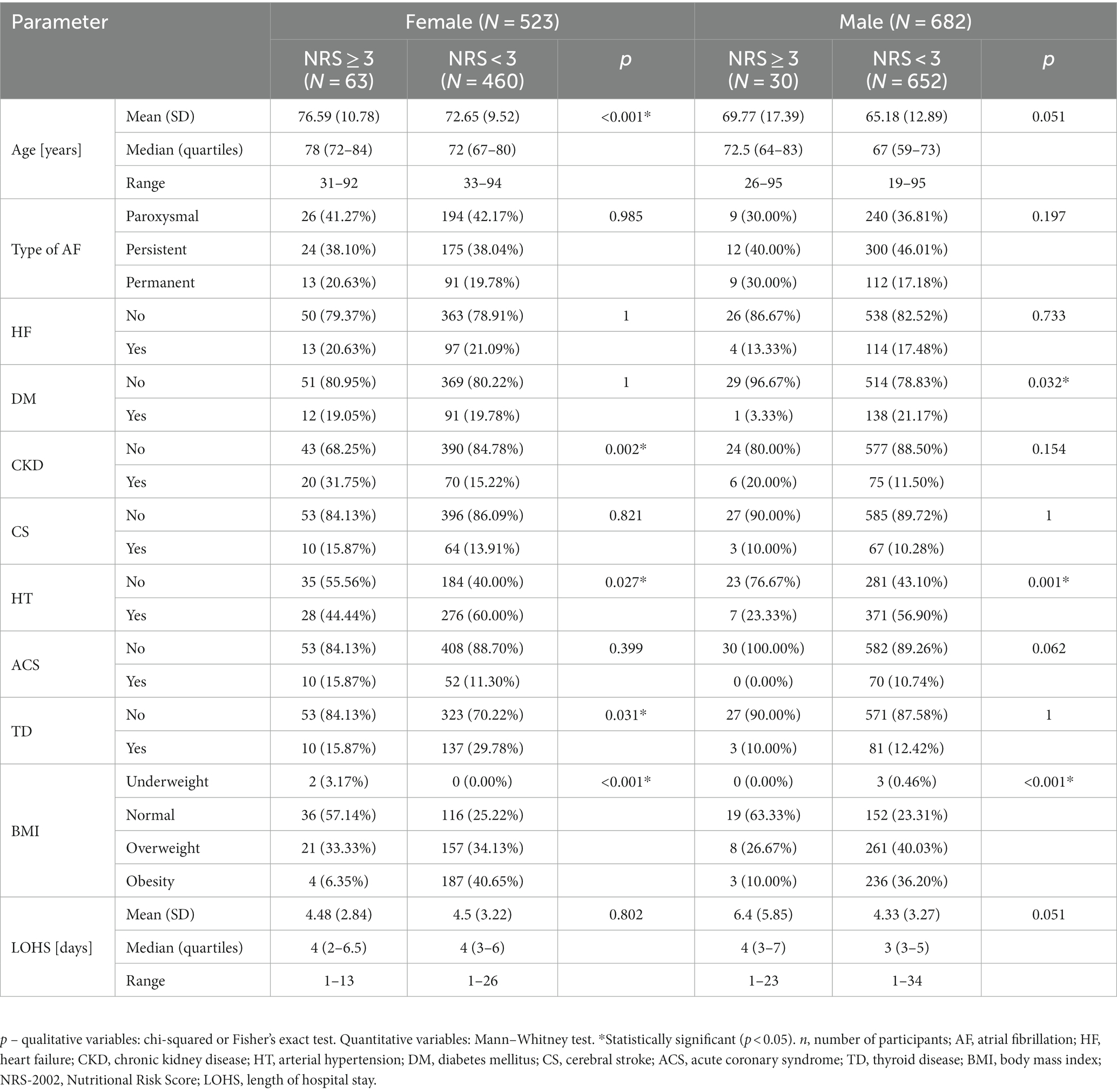
Table 3. Group comparison concerning malnutrition risk.
For women, a multivariate linear regression model showed that none of the analyzed characteristics was a significant independent predictor of hospitalization length. However, for men, a significant independent predictor of prolonged hospitalization was the risk of malnutrition (B = 1.95; p = 0.003), which prolonged hospitalization by an average of almost 1.95 days (Table 4). In an age-adjusted linear regression model, this proved to be a significant independent predictor of LOHS in both women (B = 0.072, p < 0.001) and men (B = 0.035, p = 0.001). In addition, in men, the risk of malnutrition remained a significant independent predictor (B = 1.843, p = 0.005), which on average prolonged hospitalization by 1.843 days (Table 4).
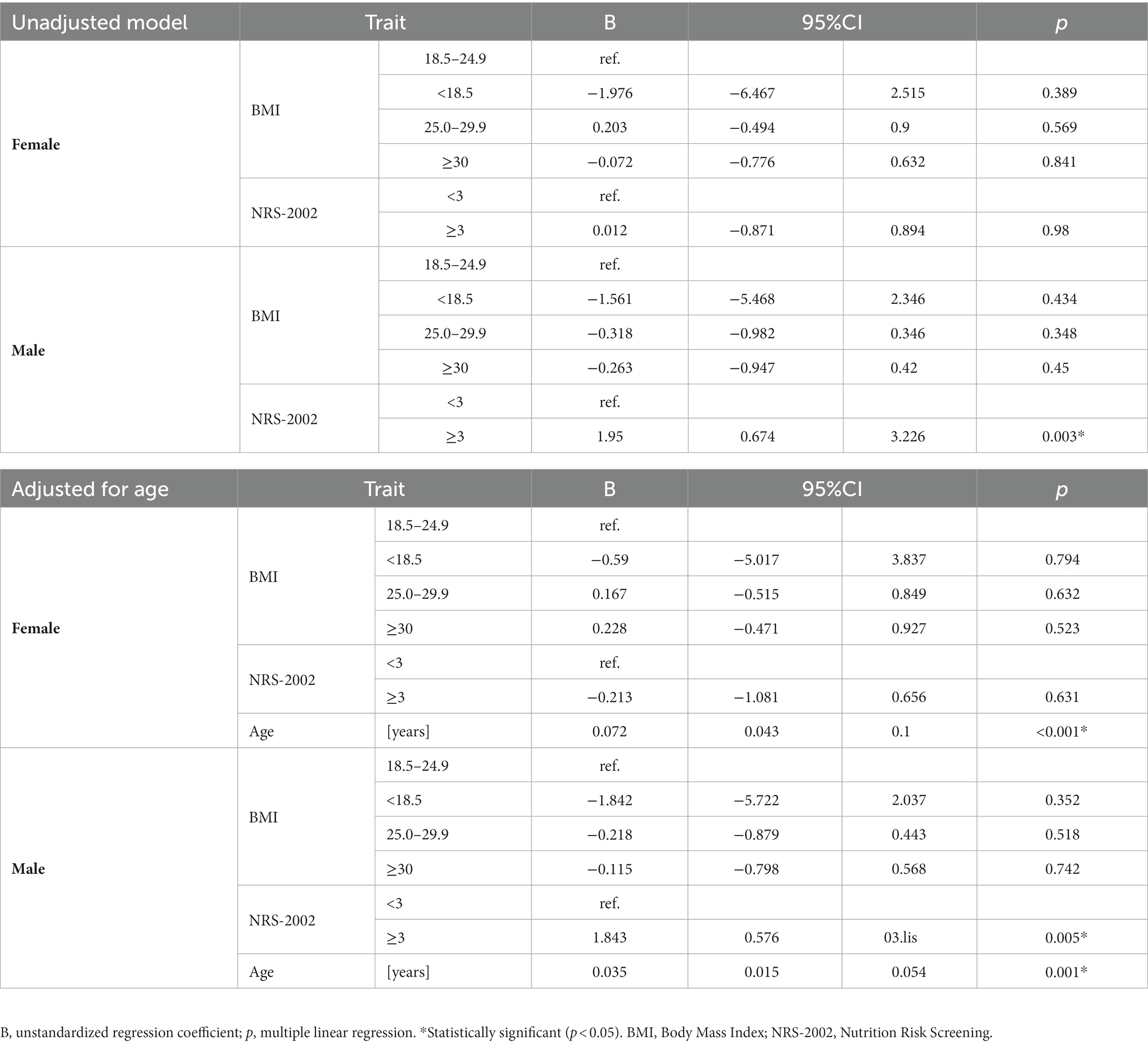
Table 4. Effect of BMI and NRS-2002 on LOHS – unadjusted and adjusted for age.
For female patients, a multivariate linear regression model showed that significant independent predictors of length of hospitalization are age (B = 0.075), persistent AF (B = 0.717), and HT (B = −0.751). In male patients, independent predictors of length of hospitalization are age (B = 0.029), persistent AF (B = −0.612), permanent AF (B = 1.217), history of stroke (B = −1.598), and HT (B = −0.979). Still, despite the addition of comorbidities to the model, the risk of malnutrition was a significant independent factor affecting the length of hospitalization (B = 1.285, p = 0.043) in men (Table 5).
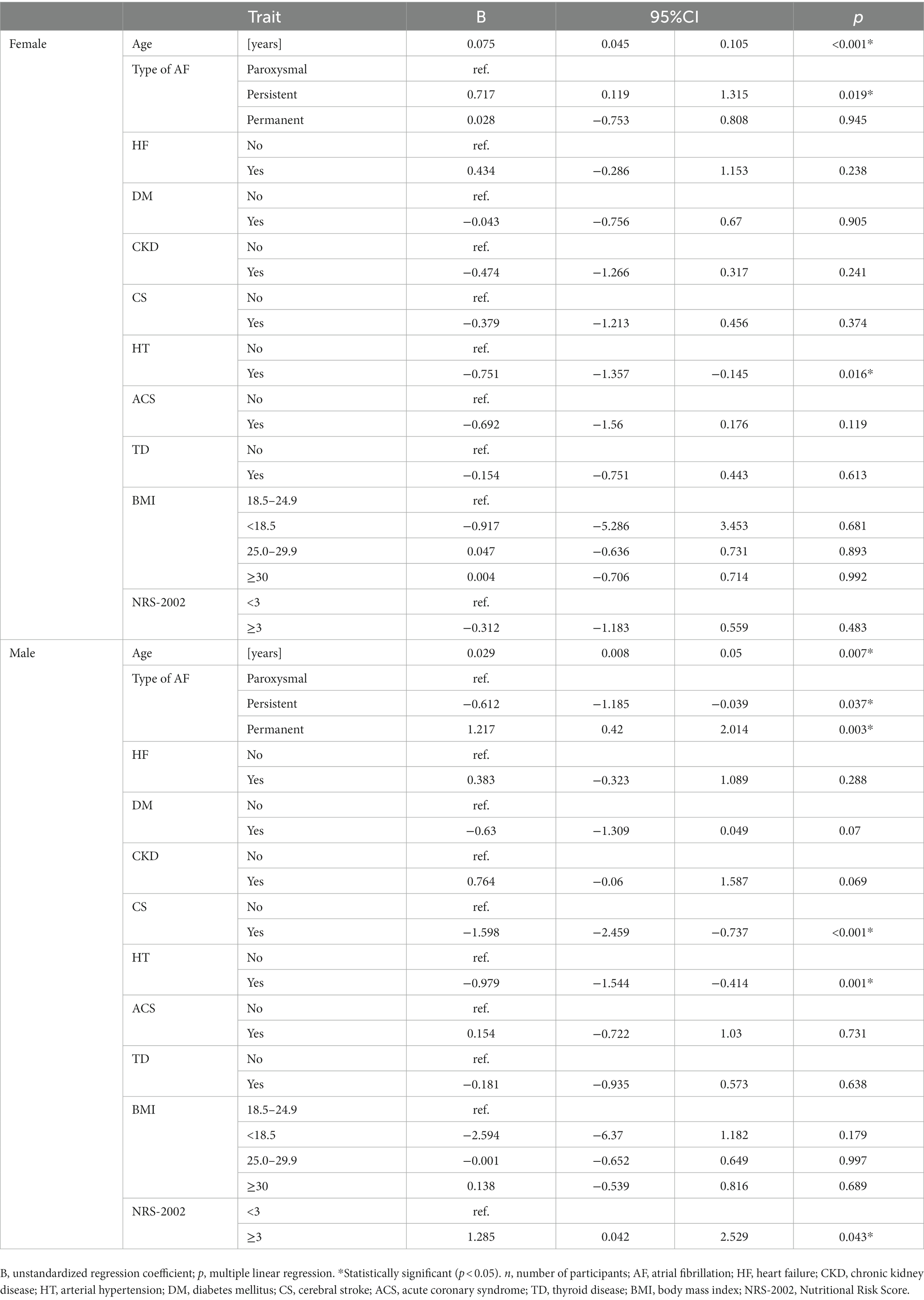
Table 5. Effect of BMI and NRS-2002 on LOHS in men and women – adjusted model.
The impact of nutritional status on CVD is widely reported in the scientific literature. Its effects can range from the risk of cardiovascular events, presentation of symptoms, condition treatment methods, length of hospitalization and influence patient prognosis. The association of obesity with AF and the effect of weight reduction on its course is well known (22). It is also known that being underweight can be an independent risk factor for AF, and the association of BMI with AF risk takes a “U” shape (23). Scientific reports are also increasingly pointing out the gender differences present in atrial fibrillation (24). However, to the best of our knowledge, this study is one of the few to evaluate gender differences in the effect of nutritional status on the length of hospitalization in patients with AF, highlighting the complexity of this problem.
In the study, a multivariate linear regression model showed that malnutrition risk, as determined by the NRS-2002 scale, was a significant independent predictor of prolonged LOHS in men (B = 1.285, p = 0.005). No such effect was demonstrated in women. We also noted no effect of BMI score on LOHS for either sex. A study by Cheng et al. confirmed the impact of malnutrition on clinical outcomes, which showed that moderate to severe malnutrition is an independent predictor of adverse prognosis among older adult patients with non-valvular AF (25). The impact on LOHS was also evaluated in the work of Alturi et al., where it was shown that protein-calorie malnutrition in patients with AF could prolong hospital stay by 2.76 days (26). When comparing the groups in relation to the risk of malnutrition, statistically significant differences in the length of hospitalization in both men and women were not registered. However, the length of hospitalization is prolonged in the group of men with NRS ≥ 3 (6.4 vs. 4.33), which, although not statistically significant, may be clinically relevant and affect the total cost of treatment.
The risk of malnutrition can be studied using several different tools. Zhu et al. evaluated the effect of malnutrition assessed by the nutritional status score (CONUT score) and geriatric nutritional risk index (GNRI) on AF recurrence in patients after ablation procedures. They found that malnourished patients were more likely to experience AF recurrence (27). Malnutrition can also affect the increased risk of complications. Kim et al. showed that it increases the risk of complications in AF patients undergoing catheter ablation. The overall complication rate was more marked among malnourished women (7.1%) than malnourished men (3.7%) (28). Monitoring patients’ nutritional status is essential to the medical care process, as it can deteriorate during a hospital stay (29). The assessment should be performed at the time of admission to the hospital and during hospitalization. This is because it has been shown that a drop in category on the Subjective Global Assessment (SGA) or significant weight loss during the first week of hospitalization may be associated with a greater likelihood of a longer hospital stay (30).
In our study, only males had malnutrition risk according to NRS-2002 as a significant independent predictor of LOHS. Although this hypothesis requires further research, it may be influenced by different body fat content relative to gender. It is indicated that with similar BMI, the body fat percentage in men is lower than in women (31). In our study, we also found no effect of BMI on LOHS in either sex, which seems to confirm the lack of reflection of body composition in the BMI parameter. This is because it does not consider body fat, muscle mass or water content but only the patient’s weight-to-height ratio.
Researchers identify multiple determinants of prolonged hospital stay for patients with AF. Independent predictors of LOHS include acute coronary syndromes, acute decompensated heart failure, heart failure with reduced ejection fraction, and elevated NT-proBNP levels (32). Sex differences in AF are related to comorbidities, the influence of sex hormones, differences in electrophysiology, endothelial dysfunction, and pro-inflammatory signalling, among other factors (33). Researchers indicate that women with AF have a larger left atrial diameter, which affects their mortality (34), prolonged hospitalization time compared to men after ablation (35), and a higher risk of AF recurrence after radiofrequency catheter ablation (35). Women with AF also report poorer overall quality of life (36). Although in our study, BMI results were not a factor in the length of hospitalization, it should be noted that many authors show a positive association between the occurrence of AF and obesity, overweight and underweight (37–39). Also, in the study we conducted, there were no deaths; however, it is worth noting that increasingly researchers are pointing to gender differences in the incidence of mortality and the course of atrial fibrillation (40, 41). Renoux et al. showed that AF mortality was higher in males (10.0, 95% CI 9.8 to 10.1) than in females (8.5, 95% CI 8.3 to 8.6) (40). Our findings of gender differences in the effects of BMI and NRS on LOHS in patients with AF justify the need for further prospective studies in this area, highlighting the complexity of factors affecting the length of hospitalization.
This study had several limitations. The percentage of male patients at risk for malnutrition was low at 3.88%. In addition, due to the study’s retrospective nature, among other factors, patients’ body composition was not analyzed by electrical bioimpedance or anthropometric measurements were not taken. The patient’s body composition was not assessed in the present study, only the NRS-2002 score and BMI. Anthropometric differences between genders may affect prognosis, which may have been a limitation of this study. Due to restrictions on access to patients’ data under Polish law, the long-term survival of patients with AF could not be assessed.
The risk of malnutrition according to the NRS-2002 directly predicts the length of hospital stays in men but not women. The study did not find a relationship between body mass index and length of hospital stay in both women and men. Because the number of participants were at risk of malnutrition, these results should be interpreted within the context of each patient. Additional independent predictors of length of hospitalization for female patients independent predictors of length of hospitalization are age, persistent AF, hypertension and in male patient’s age, persistent AF, permanent AF, history of stroke and hypertension. Undoubtedly, the impact of NRS-2002 and BMI results in patients hospitalized in the cardiology department due to atrial fibrillation relative to sex requires further investigation.
The original contributions presented in this study are included in the article, further inquiries can be directed to the corresponding author.
AK and MC: conceptualization, methodology, validation, formal analysis, resources, writing-original draft preparation, and writing-review and editing. AK and KŁ: software. MC, BU, AM, KŁ, and JS: investigation. AK: data curation. AK and AM: visualization. MC: supervision. KŁ: project administration. JS: funding acquisition. All authors contributed to the article and approved the submitted version.
The study was funded by the Ministry of Science and Higher Education of Poland under the statutory grant of the Wroclaw Medical University (SUBZ.E250.23.020).
There were no other contributors to the article than the authors. Certified English language services were provided.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hindricks, G, Potpara, T, Dagres, N, Arbelo, E, Bax, JJ, Blomström-Lundqvist, C, et al. Corrigendum to: 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European heart rhythm association (EHRA) of the ESC. Eur Heart J. (2021) 42:4194. doi: 10.1093/eurheartj/ehab648
2. Benjamin, EJ, Muntner, P, Alonso, A, Bittencourt, MS, Callaway, CW, Carson, AP, et al. Heart disease and stroke Statistics-2019 update: a report from the American Heart Association. Circulation. (2019) 139:e56–e528. doi: 10.1161/CIR.0000000000000659
3. Camm, AJ, Lip, GYH, de Caterina, R, Savelieva, I, Atar, D, Hohnloser, SH, et al. 2012 focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation. Developed with the special contribution of the European heart rhythm association. Eur Heart J. (2012) 33:2719–47. doi: 10.1093/eurheartj/ehs253
4. Westergren, A, Wann-Hansson, C, Börgdal, EB, Sjölander, J, Strömblad, R, Klevsgård, R, et al. Malnutrition prevalence and precision in nutritional care differed in relation to hospital volume – a cross-sectional survey. Nutr J. (2009) 8:20. doi: 10.1186/1475-2891-8-20
5. Czapla, M, Juárez-Vela, R, Łokieć, K, Wleklik, M, Karniej, P, and Smereka, J. The association between nutritional status and length of hospital stay among patients with hypertension. Int J Environ Res Public Health. (2022) 19:5827. doi: 10.3390/ijerph19105827
6. Kałużna-Oleksy, M, Krysztofiak, H, Migaj, J, Wleklik, M, Dudek, M, Uchmanowicz, I, et al. Relationship between nutritional status and clinical and biochemical parameters in hospitalized patients with heart failure with reduced ejection fraction, with 1-year follow-up. Nutrients. (2020) 12:2330. doi: 10.3390/nu12082330
7. Czapla, M, Uchmanowicz, I, Juárez-Vela, R, Durante, A, Kałużna-Oleksy, M, Łokieć, K, et al. Relationship between nutritional status and length of hospital stay among patients with atrial fibrillation – a result of the nutritional status heart study. Front Nutr. (2022) 9:1086715. doi: 10.3389/fnut.2022.1086715
8. Budzyński, J, and Anaszewicz, M. The associations between atrial fibrillation and parameters of nutritional status assessment in the general hospital population – a cross-sectional analysis of medical documentation. Kardiologia Pol Pol Heart J. (2017) 75:231–9. doi: 10.5603/KP.a2016.0182
9. Rahman, A, Wu, T, Bricknell, R, Muqtadir, Z, and Armstrong, D. Malnutrition matters in Canadian hospitalized patients: malnutrition risk in hospitalized patients in a tertiary care center using the malnutrition universal screening tool. Nutr Clin Pract Off Publ Am Soc Parenter Enter Nutr. (2015) 30:709–13. doi: 10.1177/0884533615598954
10. Sun, X, Boyce, SW, Hill, PC, Bafi, AS, Xue, Z, Lindsay, J, et al. Association of body mass index with new-onset atrial fibrillation after coronary artery bypass grafting operations. Ann Thorac Surg. (2011) 91:1852–8. doi: 10.1016/j.athoracsur.2011.03.022
11. Wang, X, Zhou, C, Li, Y, Li, H, Cao, Q, and Li, F. Prognostic value of frailty for older patients with heart failure: a systematic review and meta-analysis of prospective studies. Biomed Res Int. (2018) 2018:e8739058. doi: 10.1155/2018/8739058
12. Zhao, M, Song, L, Zhao, Q, Chen, Y, Li, B, Xie, Z, et al. Elevated levels of body mass index and waist circumference, but not high variability, are associated with an increased risk of atrial fibrillation. BMC Med. (2022) 20:215. doi: 10.1186/s12916-022-02413-1
13. Thacker, EL, McKnight, B, Psaty, BM, Longstreth, WT, Dublin, S, Jensen, PN, et al. Association of body mass index, diabetes, hypertension, and blood pressure levels with risk of permanent atrial fibrillation. J Gen Intern Med. (2013) 28:247–53. doi: 10.1007/s11606-012-2220-4
14. Tsang, TSM, Barnes, ME, Miyasaka, Y, Cha, SS, Bailey, KR, Verzosa, GC, et al. Obesity as a risk factor for the progression of paroxysmal to permanent atrial fibrillation: a longitudinal cohort study of 21 years. Eur Heart J. (2008) 29:2227–33. doi: 10.1093/eurheartj/ehn324
15. Pathak, RK, Middeldorp, ME, Meredith, M, Mehta, AB, Mahajan, R, Wong, CX, et al. Long-term effect of goal-directed weight management in an atrial fibrillation cohort: a long-term follow-up study (LEGACY). J Am Coll Cardiol. (2015) 65:2159–69. doi: 10.1016/j.jacc.2015.03.002
16. Overvad, TF, Rasmussen, LH, Skjøth, F, Overvad, K, Lip, GYH, and Larsen, TB. Body mass index and adverse events in patients with incident atrial fibrillation. Am J Med. (2013) 126:640.e9–640.e17. doi: 10.1016/j.amjmed.2012.11.024
17. Huxley, RR, Misialek, JR, Agarwal, SK, Loehr, LR, Soliman, EZ, Chen, LY, et al. Physical activity, obesity, weight change, and risk of atrial fibrillation: the atherosclerosis risk in communities study. Circ Arrhythm Electrophysiol. (2014) 7:620–5. doi: 10.1161/CIRCEP.113.001244
18. Siddiqi, HK, Vinayagamoorthy, M, Gencer, B, Ng, C, Pester, J, Cook, NR, et al. Sex differences in atrial fibrillation risk: the VITAL rhythm study. JAMA Cardiol. (2022) 7:1027–35. doi: 10.1001/jamacardio.2022.2825
19. Wong, GR, Nalliah, CJ, Lee, G, Voskoboinik, A, Chieng, D, Prabhu, S, et al. Sex-related differences in atrial remodelling in patients with atrial fibrillation: relationship to ablation outcomes. Circ Arrhythm Electrophysiol. (2022) 15:e009925. doi: 10.1161/CIRCEP.121.009925
20. Kondrup, J, Allison, SP, Elia, M, Vellas, B, and Plauth, M. Educational and clinical practice committee, European Society of Parenteral and Enteral Nutrition (ESPEN). ESPEN guidelines for nutrition screening 2002. Clin Nutr Edinb Scotl. (2003) 22:415–21. doi: 10.1016/s0261-5614(03)00098-0
21. WHO Consultation on Obesity (1999: Geneva S, Organization WH. Obesity: Preventing and managing the global epidemic: Report of a WHO consultation. World Health Organization; (2000). Available at: https://apps.who.int/iris/handle/10665/42330. Accessed December 31, 2022
22. Aldaas, OM, Lupercio, F, Han, FT, Hoffmayer, KS, Krummen, D, Ho, G, et al. Meta-analysis of effect of modest (≥10%) weight loss in management of overweight and obese patients with atrial fibrillation. Am J Cardiol. (2019) 124:1568–74. doi: 10.1016/j.amjcard.2019.08.009
23. Kang, SH, Choi, EK, Han, KD, Lee, SR, Lim, WH, Cha, MJ, et al. Underweight is a risk factor for atrial fibrillation: a nationwide population-based study. Int J Cardiol. (2016) 215:449–56. doi: 10.1016/j.ijcard.2016.04.036
24. Andrade, JG, Deyell, MW, Lee, AYK, and Macle, L. Sex differences in atrial fibrillation. Can J Cardiol. (2018) 34:429–36. doi: 10.1016/j.cjca.2017.11.022
25. Cheng, N, Dang, A, Lv, N, He, Y, and Wang, X. Malnutrition status in patients of very advanced age with nonvalvular atrial fibrillation and its impact on clinical outcomes. Nutr Metab Cardiovasc Dis NMCD. (2019) 29:1101–9. doi: 10.1016/j.numecd.2019.06.021
26. Abstract 13638: Protein calorie malnutrition is an adverse prognostic marker in atrial fibrillation patients: An analysis of the National Inpatient Sample Registry|circulation. Available at: https://www.ahajournals.org/doi/abs/10.1161/circ.144.suppl_1.13638. Accessed May 7, 2023
27. Zhu, S, Zhao, H, Zheng, M, and Peng, J. The impact of malnutrition on atrial fibrillation recurrence post ablation. Nutr Metab Cardiovasc Dis NMCD. (2021) 31:834–40. doi: 10.1016/j.numecd.2020.12.003
28. Kim, D, Shim, J, Kim, YG, Yu, HT, Kim, TH, Uhm, JS, et al. Malnutrition and risk of procedural complications in patients with atrial fibrillation undergoing catheter ablation. Front Cardiovasc Med. (2021) 8:8:736042. doi: 10.3389/fcvm.2021.736042
29. Rinninella, E, Cintoni, M, de Lorenzo, A, Anselmi, G, Gagliardi, L, Addolorato, G, et al. May nutritional status worsen during hospital stay? A sub-group analysis from a cross-sectional study. Intern Emerg Med. (2019) 14:51–7. doi: 10.1007/s11739-018-1944-5
30. Lima, J, Teixeira, PP, Eckert I Da, C, Burgel, CF, and Silva, FM. Decline of nutritional status in the first week of hospitalization predicts longer length of stay and hospital readmission during 6-month follow-up. Br J Nutr. (2021) 125:1132–9. doi: 10.1017/S0007114520003451
31. Jackson, AS, Stanforth, PR, Gagnon, J, Rankinen, T, Leon, AS, Rao, DC, et al. The effect of sex, age and race on estimating percentage body fat from body mass index: the heritage family study. Int J Obes Relat Metab Disord J Int Assoc Study Obes. (2002) 26:789–96. doi: 10.1038/sj.ijo.0802006
32. Vîjan, AE, Daha, IC, Delcea, C, and Dan, GA. Determinants of prolonged length of hospital stay of patients with atrial fibrillation. J Clin Med. (2021) 10:3715. doi: 10.3390/jcm10163715
33. Odening, KE, Deiß, S, Dilling-Boer, D, Didenko, M, Eriksson, U, Nedios, S, et al. Mechanisms of sex differences in atrial fibrillation: role of hormones and differences in electrophysiology, structure, function, and remodelling. Eur Eur Pacing Arrhythm Card Electrophysiol J Work Groups Card Pacing Arrhythm Card Cell Electrophysiol Eur Soc Cardiol. (2019) 21:366–76. doi: 10.1093/europace/euy215
34. Proietti, M, Raparelli, V, Basili, S, Olshansky, B, and Lip, GYH. Relation of female sex to left atrial diameter and cardiovascular death in atrial fibrillation: the AFFIRM trial. Int J Cardiol. (2016) 207:258–63. doi: 10.1016/j.ijcard.2016.01.169
35. Kloosterman, M, Chua, W, Fabritz, L, al-Khalidi, HR, Schotten, U, Nielsen, JC, et al. Sex differences in catheter ablation of atrial fibrillation: results from AXAFA-AFNET 5. Eur Eur Pacing Arrhythm Card Electrophysiol J Work Groups Card Pacing Arrhythm Card Cell Electrophysiol Eur Soc Cardiol. (2020) 22:1026–35. doi: 10.1093/europace/euaa015
36. Silva, RL, Guhl, EN, Althouse, AD, Herbert, B, Sharbaugh, M, Essien, UR, et al. Sex differences in atrial fibrillation: patient-reported outcomes and the persistent toll on women. Am J Prev Cardiol. (2021) 8:100252. doi: 10.1016/j.ajpc.2021.100252
37. Anzai, T, Grandinetti, A, Katz, AR, Hurwitz, EL, Wu, YY, and Masaki, K. Paradoxical association between atrial fibrillation/flutter and high cholesterol over age 75 years: the Kuakini Honolulu heart program and Honolulu-Asia aging study. J Electrocardiol. (2021) 65:37–44. doi: 10.1016/j.jelectrocard.2020.12.008
38. Bang, CN, Greve, AM, Abdulla, J, Køber, L, Gislason, GH, and Wachtell, K. The preventive effect of statin therapy on new-onset and recurrent atrial fibrillation in patients not undergoing invasive cardiac interventions: a systematic review and meta-analysis. Int J Cardiol. (2013) 167:624–30. doi: 10.1016/j.ijcard.2012.08.056
39. Goette, A, Bukowska, A, Lillig, CH, and Lendeckel, U. Oxidative stress and microcirculatory flow abnormalities in the ventricles during atrial fibrillation. Front Physiol. (2012) 3:236. doi: 10.3389/fphys.2012.00236
40. Renoux, C, Patenaude, V, and Suissa, S. Incidence, mortality, and sex differences of non-valvular atrial fibrillation: a population-based study. J Am Heart Assoc. (2014) 3:e001402. doi: 10.1161/JAHA.114.001402
Keywords: nutritional status, obesity, malnutrition, sex difference, body mass index, atrial fibrillation
Citation: Kwaśny A, Łokieć K, Uchmanowicz B, Młynarska A, Smereka J and Czapla M (2023) Sex-related differences in the impact of nutritional status on length of hospital stay in atrial fibrillation: a retrospective cohort study. Front. Public Health. 11:1223111. doi: 10.3389/fpubh.2023.1223111
Edited by:
Zhendong Liu, Shandong First Medical University, ChinaReviewed by:
Jin-Yu Sun, Nanjing Medical University, ChinaCopyright © 2023 Kwaśny, Łokieć, Uchmanowicz, Młynarska, Smereka and Czapla. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jacek Smereka, amFjZWsuc21lcmVrYUB1bXcuZWR1LnBs
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.