 Sandra León-Herrera1,2
Sandra León-Herrera1,2 Rosa Magallón-Botaya1,3
Rosa Magallón-Botaya1,3 Bárbara Oliván-Blázquez1,2*
Bárbara Oliván-Blázquez1,2* Lucía Sagarra-Romero4
Lucía Sagarra-Romero4 Carlos Martín Jaurrieta1
Carlos Martín Jaurrieta1 Fátima Méndez-López1
Fátima Méndez-López1- 1Institute for Health Research Aragón (IIS Aragón), Zaragoza, Spain
- 2Department of Psychology and Sociology, University of Zaragoza, Zaragoza, Spain
- 3Department of Medicine, Faculty of Medicine, University of Zaragoza, Zaragoza, Spain
- 4GAIAS Research Group, Department of Health Sciences, Faculty of Health Sciences, Zaragoza, Spain
Background: Long COVID is a multisystemic condition which affects quality of life and implies a multidisciplinary treatment approach. There is still limited evidence on management techniques for this syndrome. “Telerehabilitation” could be an important tool when addressing the symptoms of this patients with the aim of increasing their quality of life. The purpose of this trial is to analyse the effectiveness of an online multimodal rehabilitation programme to improve the symptomatology of people with long COVID and their quality of life.
Methods: A pragmatic randomised controlled trial will be performed with two parallel groups: (1) usual treatment by the primary care practitioner (Treatment as usual, TAU; control group) and (2) TAU plus the use of an online multimodal rehabilitation programme, including videoconferences and content published on a Moodle platform (intervention group). The data will be collected before and after the intervention. A follow-up will take place 3 months later.
Discussion: There is still a lack of knowledge regarding the management of the symptoms of long COVID. This creates the need to add scientific evidence about the care of this disease, considering that multidisciplinary social and health teams can offer the necessary care so that these patients can recover their previous quality of life.
Clinical trial registration: The protocol for this study was registered with the ISRCTN Registry [registration number: ISRCTN15414370] on 28 December 2022.
1. Introduction
In March 2020, when the coronavirus disease 2019 (COVID-19) pandemic was declared, hardly anyone would have thought that this disease would affect the physical and mental health of the entire world in the way that it did, and that it could even be considered a chronic condition (1, 2) As the pandemic has progressed, we have seen that after the initial acute infection by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), some people develop a long-lasting multi-organ syndrome with various symptoms (general, respiratory, neurological, cardiovascular, gastrointestinal and psychosocial symptoms), a phenomenon that also occurs with many other viral disorders. The World Health Organization (WHO) called this condition “long COVID” (3–5). In the long term, these symptoms lead to a significant decline in the functional status and quality of life of people who experience them. Indeed, these symptoms limit the ability of people to perform basic activities of daily living (ADL), such as bathing or dressing, as well as occupational, social and leisure activities (6–8).
People with long COVID exhibit heterogenous symptoms and this multisystemic condition implies the need for a multidisciplinary treatment approach (9, 10). In current clinical practice, the treatment is based on managing the symptoms and the affected systems of each patient (11). In other words, a single care strategy is not possible for all people with long COVID; it is necessary to develop personalised care programmes (12).
Several guidelines about the management of long COVID have already been published (13–17). However, these clinical guidelines are not fully supported by scientific evidence, leading to a large practice gap (17). This lack of knowledge about the management and treatment of symptoms by general practitioners (GPs) has led to people with long COVID feeling that their concerns are not being taken seriously (18). Consequently, these patients have expressed their willingness to try anything (over-the-counter medications, different types of therapy, home remedies, dietary changes, supplements, etc.) to ameliorate the disabling symptoms. These types of measures can be harmful if they are not supervised by a qualified medical professional, a fact that supports the urgent need to generate evidence concerning the clinical management of long COVID (19, 20). However, this also shows that in the research carried out about long COVID, it is crucial to listen to the narratives and experiences of patients, turning them into co-producers of scientific knowledge (21).
There have been significant technological advances in recent years (22). The use of technology has been raised as an alternative to provide various rehabilitation services remotely (23). This approach increased especially during the COVID-19 confinement, when face-to-face contact between patients and health care professionals was limited, and the population was highly virtualized (24, 25). This type of care is commonly called ‘telerehabilitation’, a promising means that includes different techniques, among which are messages or phone calls, videoconferences or the use of Internet platforms (26). These types of programmes make it possible to provide, in real or deferred time, safe and supervised care at the patient’s home or other important environments (27). The advantages of telerehabilitation include greater participation and commitment on the part of the patients, a more rigorous follow-up of the intervention, personalisation of the treatment plans and, above all, a good perception on the part of those who receive it, because it favours accessibility and reduced waiting times (28).
Although more studies are needed to guarantee an adequate level of scientific evidence, telerehabilitation could represent an important element in the comprehensive rehabilitation of patients in the acute phase and with sequelae of COVID-19 (10). Aiyegbusi et al. (29) already indicated that videoconferences could be an effective tool in the follow-up of people with long COVID and that, as long as it is feasible, digital therapy programmes could be implemented through a platform that includes non-pharmacological interventions, such as respiratory rehabilitation. Moreover, Samper-Pardo et al. (30) are studying the use of mobile applications to improve the quality of life of people with long COVID, and Ozduran et al. (31) are analysing the effectiveness of YouTube videos to manage pain, a very significant symptom in this patient population.
This trial will investigate long COVID and its management by multidisciplinary social health care teams. The objective is to analyse the effectiveness of a multimodal rehabilitation programme, with online and in-person components, to ameliorate the characteristic symptoms of long COVID and, consequently, to improve quality of life. A secondary objective is to analyse the factors associated with the effectiveness of this intervention in people with long COVID.
2. Methods
2.1. Research design and study registration
This pragmatic randomized controlled trial will include two parallel groups: (1) usual treatment by the primary care practitioner (Treatment as usual, TAU; control group) and (2) TAU plus the use of an online multimodal rehabilitation programme (intervention group). The results will be reported by following a pre-established plan based on the CONSORT guidelines (32) to compare the two groups. Figure 1 shows a systematic overview of the study.
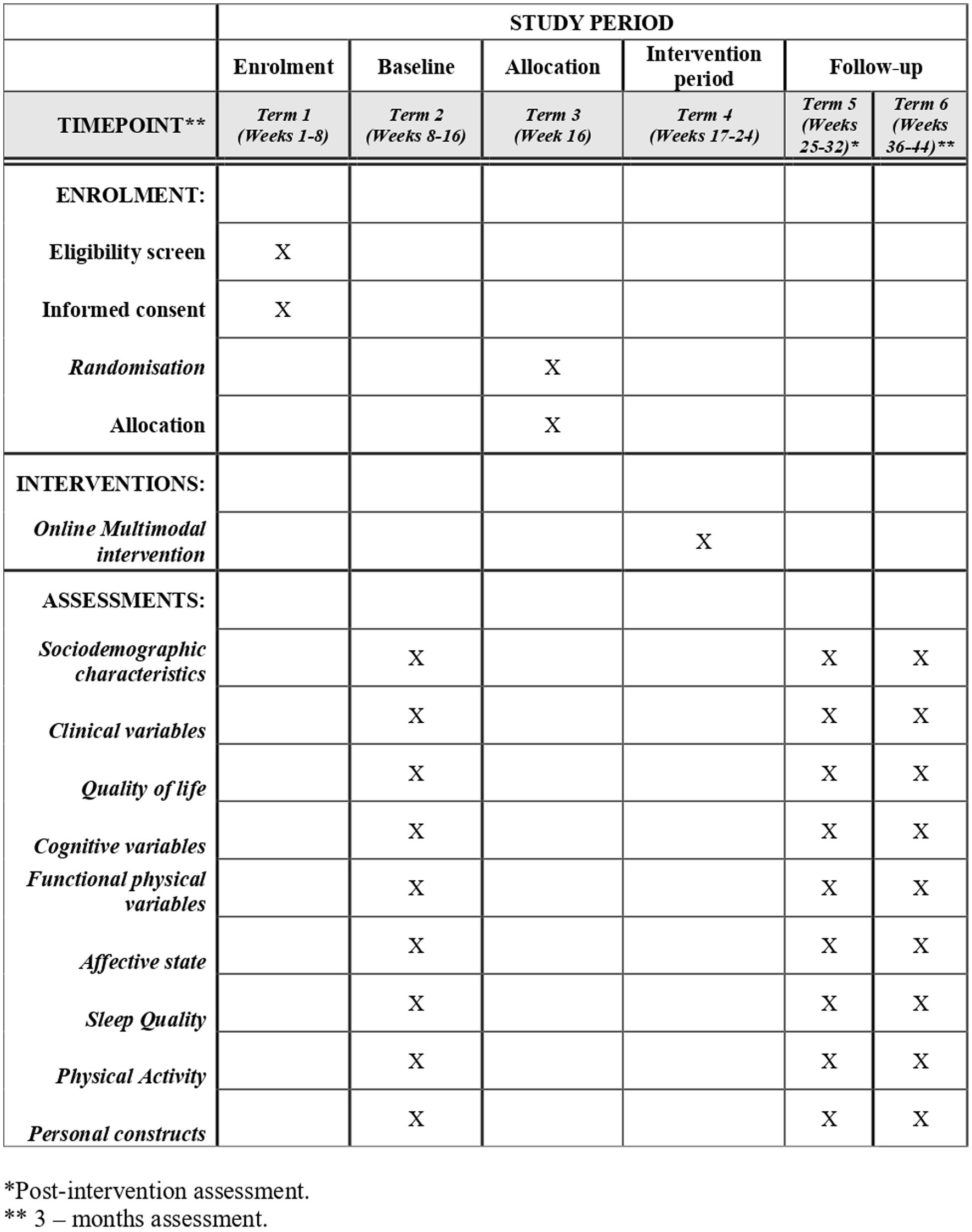
Figure 1. SPIRIT schedule of enrolment, allocation, intervention and assessments.
The protocol for this study was registered with the ISRCTN Registry (registration number: ISRCTN15414370) on 28 December 2022, and is being reported using the SPIRIT (Standard Protocol Elements: Recommendations for Interventional Trials) (Supplementary materials).
2.2. Patient inclusion and sample size
The study population will follow the following inclusion criteria: (1) people over 18 and under 80 years of age; (2) with persistent COVID symptoms for at least 3 months since acute infection, and are not explained by an alternative diagnosis; (3) who are part of long COVID associations in Spain. The exclusion criteria will be the presence of a serious uncontrolled medical illness that may interfere with adherence to the rehabilitation programme; receiving structured rehabilitation or psychotherapeutic treatment by health care professionals; participation in another clinical trial in the last 6 months; considerable risk of suicide; pregnancy or lactation; and the presence of any medical, psychological or social problems that could seriously affect the patient’s participation in the study.
The research team will inform the presidents of the different Spanish long COVID associations about this project; they will then pass the information to the members of these organisations. Those interested in participating should contact the project researchers by using the contact details provided in the invitation letter sent to the associations. The evaluating researcher will then contact the participant and determine whether the patient can be included in the study (based on the inclusion and exclusion criteria). Recruitment and baseline assessments will be carried out until the sample size has been reached.
In accordance with the results obtained in the literature (33), to detect a mean difference of 20 points on the physical scale of the 36-Item Short Form Health Survey Questionnaire (SF-36), with a standard deviation (SD) between the groups of 36.16, an alpha value of 0.05 and a power of 80%, 53 subjects per group will need to be recruited (106 subjects in total). We will increase this value by 10% to cover potential losses in the study, so the minimum sample required will be 116 subjects. Considering a mental scale, to detect a mean difference of 20 points, with an SD of 29.99 between the groups, an alpha value of 0.05 and a power of 80%, 35 subjects per group will need to be recruited (70 subjects in total). This number will be increased by 10% to counter possible losses, so the sample size is 77 subjects. Based on these calculations, the minimum sample required for the study will be 58 subjects per group (116 subjects in total). The sample size has been calculated using the Fisterra Guide for Determination of sample size (34). The formulae used have been added as Supplementary materials.
At the time of writing 90 participants (77.5% of the target sample size) have been recruited.
2.3. Randomisation, allocation and masking of the study groups
Patients will be randomised once baseline data have been collected. Individual randomisation will be performed by an independent statistician using a computer-generated random number sequence with no restrictions. The sequence will be concealed throughout the study. Given the nature of the interventions, the patients will not be blind to their allocation. The information for the random allocation sequence will be implemented by phone by a research assistant (RA), who will state the type of treatment assigned for each new patient. The participants in the intervention group will be informed about what the intervention is and where and when they should carry it out. In addition, the RA will request that participants do not inform other researchers of their group allocation.
2.4. Data collection and monitoring
A RA will collect the data, and another will enter and encode the identification data. All RAs handling the data will be blind to patient allocation, as will the RA performing outcome assessment and data analysis. All the information collected will be treated in accordance with the provisions of the current legislation on the protection of personal data.
Any serious unexpected adverse event or result will be discussed by the trial management committee (the authors of this protocol). There are no plans to discontinue or modify the interventions, to improve adherence or to promote participant retention. The committee will monitor enrolment, treatment, attrition rates and any concerns related to the study. The reasons for abandonment will also be recorded.
2.5. Intervention
Patients assigned to the control group will follow the treatment as usual provided by their GP.
Patients assigned to the intervention group will follow the treatment as usual provided by their GP and will participate in a multidisciplinary online multimodal rehabilitation programme. The programme will be aimed at addressing the symptoms of people with long COVID and improving their quality of life. This objective will be pursued by providing exercises and therapeutic recommendations related to physical activity, respiratory rehabilitation, cognitive rehabilitation, diet, sleep hygiene, use of community resources and emotional management.
2.5.1. Intervention tools
The rehabilitation will be carried out through two techniques that are typically used in telerehabilitation programmes. On the one hand, a group videoconference will be convened weekly, in which follow-up and personalisation of the contents of the intervention will be carried out. On the other hand, a Moodle (Modular Object-Oriented Dynamic Learning Environment) Platform will be used as support; it will contain all of the content provided to patients during the videoconferences.
The programme will consist of eight videoconference sessions (one per week) of approximately 1.5 h each through the Google Meet application. Three groups will be planned for each session so that patients can choose which group to attend according to their availability, and with the goal of achieving the maximum possible assistance. In addition, dividing all patients into three smaller intervention groups (a maximum of 18 people per group) will make the intervention more individualised.
The sessions will be oriented towards managing each type of symptomatology (cognitive, respiratory, physical, etc.) while addressing the different impacts on quality of life (work, social and emotional impact) and offering recommendations that can positively influence the health of this type of population (Table 1). The same content will be provided in all three groups. The sessions will not be recorded. If a person misses a session, he/she will be able to make up for it during the schedule of one of the other two groups.
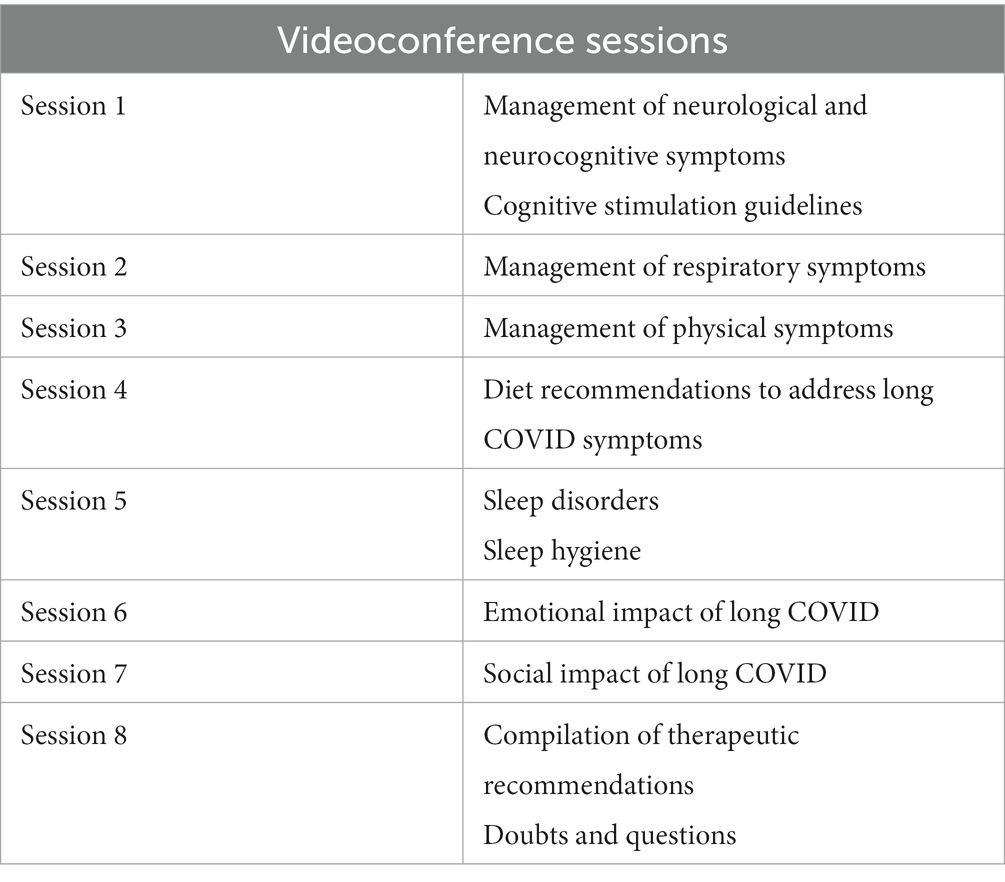
Table 1. Content of the videoconference sessions.
Also, a Moodle Platform will be created, where all the material and content provided throughout the telerehabilitation programme will be available. The platform will be divided into eight sections, whose name and content will coincide with each videoconference session (Table 1). For example, in the first section, patients will be able to find content related to the neurocognitive symptoms of long COVID and how to deal with them. This same subject will be discussed during the first videoconference of the programme.
Patients will be able to find the following content on the Moodle Platform:
• Access links to videoconferences (Google Meet application);
• PowerPoint presentations displayed during videoconferences;
• Lists of exercises and therapeutic recommendations, including cognitive exercise books, respiratory physiotherapy videos, list of diet recommendations, etc.;
• Forums to debate and interact on aspects addressed during the videoconference;
• Other resources of interest (news, glossary of terms, web pages or social networks of interest, etc.).
Instructions for how to access the weekly videoconferences and the online platform will be provided to each patient before starting the intervention, both verbally (by phone) and in writing (by email).
To carry out the rehabilitation programme, patients may use any of their personal devices: mobile phone, computer, tablet, etc., although the health team will recommend using a computer in order to avoid visual fatigue, especially when performing cognitive exercises.
In the event that any of the patients have difficulties accessing videoconferences or the platform, the rehabilitation team will try to solve them as soon as possible together with the patient.
2.5.2. Content of the online multimodal rehabilitation programme
The content of each of programme sessions will be based on scientific evidence that aims to address the symptoms of long COVID and, therefore, to improve quality of life of this patient population (13–17). The patients must adapt this intervention to their state of health, choosing the recommendations and advice that correspond to their symptoms and their specific health problems derived from this disease. Those recommendations or exercises that may cause some harm or discomfort to the participants must be discontinued immediately.
The multimodal rehabilitation sessions will consist of the following content:
2.5.2.1. Approach to neurological and neurocognitive symptoms
Neurological symptoms are very prevalent in people with long COVID. These may include tiredness, sleep disorders, movement disorders, paraesthesia and cognitive deficits (35). The latter have been defined with the term “brain fog’”, which is characterised by feeling slow, confused and disoriented; having difficulties staying focused; presenting some forgetfulness; and the inability to find the correct word (36, 37). Currently, no specific treatment has been approved for this cognitive impairment in people with long COVID, although it has been determined that cognitive stimulation may be useful in some cases (38).
The content of this session will include: a description of the types of neurological symptoms typical of long COVID; treatment of neurocognitive symptoms; the benefits of performing cognitive stimulation exercises; personalised recommendations about what cognitive exercises can be practiced, and how and when to do it; and implementation of these treatments.
2.5.2.2. Approach to respiratory symptoms
Long COVID often includes respiratory symptoms. The most common are usually shortness of breath, coughing and chest pain (39). Physiotherapy programmes focused on improving respiratory function can be useful in managing these persistent symptoms (40).
The content of this session will include: a description of the types of respiratory symptoms of long COVID; treatment of respiratory symptoms; the benefits of performing breathing exercises; personalised recommendations about what breathing exercises can be practiced, and how and when to do it; and implementation of these treatments.
Patients will be advised to use a pulse oximeter during these exercises. Whenever the patients experience any anomaly in the pulse oximeter values (resting oxygen saturation < 88%) (41) as well as any sensation of pain or pressure in the chest, they should automatically stop performing these exercises and consult what happened with the health professional during the sessions so that he/she can personalize the exercises to that specific person.
2.5.2.3. Approach to physical symptoms
People with long COVID describe drastically reduced physical function. Hence, it becomes difficult or impossible for them to perform some ADL (42). Research on physical activity and long COVID is still insufficient, although there is scientific evidence for benefits in other pathologies with similar characteristics. Existing recommendations on physical activity and long COVID emphasise the importance of personalised care based on the symptoms that each person presents (43, 44).
The content of this session will include: a description of the types of physical symptoms of long COVID; treatment of physical symptoms; the benefits of physical activity; personalised recommendations about what activity and physical exercises can be practiced, and how and when to do it; and implementation of these treatments.
As with the breathing exercises, patients will be recommended to use a pulse oximeter while performing physical exercises, as well as to stop performing the exercises and consult a professional when noticing any abnormality in the values or any type of pain.
2.5.2.4. Recommendations for a healthy diet
The Clinical Guide for Long COVID patient care of the Spanish Society of General and Family Physicians (SEMG) recommends considering food and diet in the management of this disease to fill possible nutritional deficiencies (16). Some nutrients such as folic acid, vitamin D, omega-3 fatty acids and vitamin B12, present in the Mediterranean diet, are involved in the proper functioning of metabolism and the immune system, so they could be useful in the recovery process of these patients (45, 46).
The content of this session will include: recommendations for a healthy diet based mainly on adherence to the classic Mediterranean diet.
2.5.2.5. Approach to sleep and rest disorders
Sleep disorders (decreased sleep quality, daytime sleepiness, insomnia, sleep apnoea, nightmares, etc.) are common among the persistent symptoms of long COVID (47).
The content of this session will include: a description of the types of sleep disorders present in long COVID; information about different treatments for sleep disorders; a sleep hygiene programme; and recommendations for sleep and rest.
2.5.2.6. Managing emotional impact
There is extensive research on the emotional impact on people with persistent symptoms of COVID-19. Anxiety, depression, post-traumatic stress disorder, mood fluctuations and sleep disorders are some of the consequences that long COVID can have on the mental health of people who have the disease (48).
The content of this session will include: a description of the emotional impact of long COVID; treatments aimed at addressing the emotional impact; recommendations about emotional management; an explanation of the first steps to take to meditate; and implementation of two meditation dynamics.
2.5.2.7. Behavioural activation and promotion of participation in the community
The limiting persistent symptoms of long COVID, the consequences on mental health and the reduction in quality of life have a great impact on the organisation of the lives of people with this disease. They are limited in their ability to perform basic ADL, as well as their occupational, social and leisure activities in the community. This isolation is increased by feelings such as fear or uncertainty, barriers to accessing the health system or stigmatisation (7, 8, 49).
The content of this session will include: a description and examples of community health assets (HA); the benefits of using resources offered by the community itself; and personalised recommendations about what community resources can be used, and how and when to do it.
2.5.2.8. Compilation of important aspects, resolution of doubts, and farewell
The last session, held the last week of the programme, will aim at collecting the most important therapeutic recommendations and at resolving doubts and questions that have arisen and that have not already been resolved in the previous sessions.
It is important to highlight that although each session is mainly aimed at addressing a specific type of symptomatology or impact on quality of life, the exercises described in the previous sessions will continue to be carried out and doubts that arise will be resolved. For example, in session 1, some cognitive stimulation guidelines will be explained, and cognitive stimulation exercises will be provided to patients to perform at home. In session 2, the patients will be able to express problems that have arisen when carrying out these exercises at home, and the therapist will even be able to carry out some other exercises to evaluate the progress of the patients with these symptoms.
2.6. Outcomes and measures
Data will be collected from questionnaires completed by the patients at the beginning and the end of the intervention. The assessors who administer the questionnaires will call and make an appointment with the patients following a list of first and last names arranged alphabetically and will not know the type of treatment given to each patient. Once the intervention is finished, an RA will contact the study participants and make an appointment to complete the questionnaires again. Hence, the effect that the intervention has had on the symptoms and quality of life will be evaluated. A follow-up will also be carried out after 3 months. The instruments that will be used are listed in Table 2. All assessments will last between 30 and 45 min per patient. If any of the patients experience cognitive fatigue and feel unwell due to the long duration of the assessments, they may be stopped and continued another day.
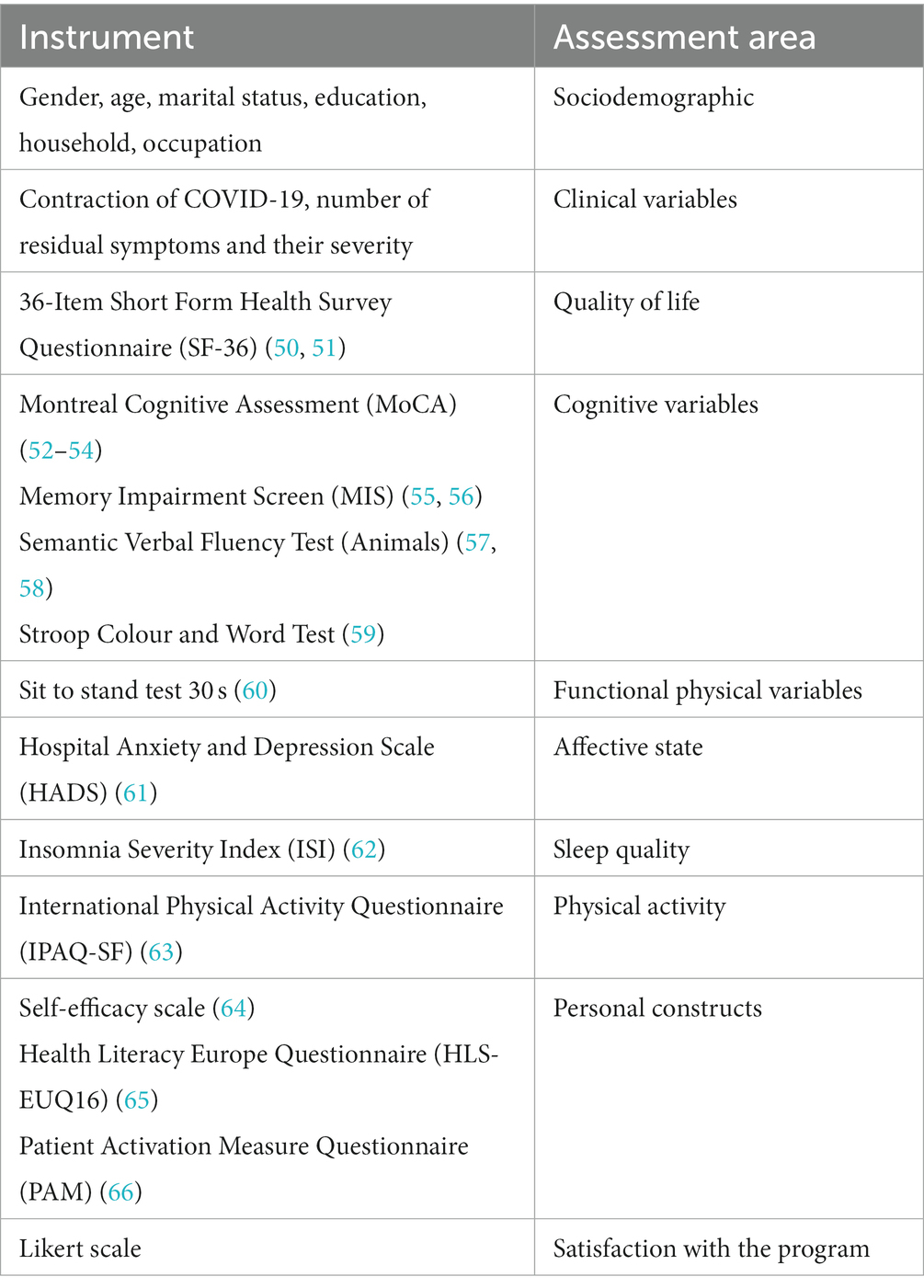
Table 2. Study variables and measurement instruments.
2.6.1. Primary outcome
The main variable will be quality of life, evaluated through the SF-36 (67). This questionnaire measures eight dimensions of health: physical function, physical role, aches and pains, general health, vitality, social function, emotional role and mental health; it also includes a declared health evolution item. The eight dimensions define two main components of health: a physical summary component and a mental summary component. In them, scores above or below 50 indicate, respectively, a better or worse state of health than the mean of the reference population. Items are scored on a Likert-type scale from 1 to 3.5 or 6, depending on the type of item. The total score of the eight scales ranges from 0 to 100, with higher scores indicating better health. The validated Spanish version of the questionnaire will be used (68).
2.6.2. Secondary outcomes
2.6.2.1. Sociodemographic variables
Age, gender, marital status, education, household and occupation will be collected.
2.6.2.2. Clinical variables
The date of contracting COVID-19 and the number and severity of persistent symptoms measured by Visual Analog Scale (69) will be collected. Persistent symptoms include: low-grade fever (37–38°C), fever (> 38°C), chills without fever, headaches, dizziness, tiredness or fatigue, sore throat, cough, dyspnoea, loss of smell and/or taste, blurred vision and other eye problems (dry eyes, increased dioptres, conjunctivitis), bruising, hair loss, tachycardia, myalgia, joint pain, orthostatic hypotension, chest pain, back pain (cervical, thoracic and/or lumbar), gastrointestinal symptoms, urinary symptoms (overactive bladder, infections), neurological symptoms (spasms, tingling, etc.), cognitive impairment (memory loss, reduced attention, mental fog), altered menstrual cycle, loss of libido or erectile dysfunction, and other symptoms that the participants consider persistent (70–72).
2.6.2.3. Cognitive variables
The official Spanish version of the Montreal Cognitive Assessment (MoCA) (52–54) will be used to assess the presence of cognitive impairment in the participants of this study. This is a test with adequate internal consistency (Cronbach’s alpha = 0.76) and assesses six cognitive domains: memory, visuospatial capacity, executive function, attention/concentration/working memory, language and orientation. Of the total score of 30 points, a correction of one point can be made in the case of subjects with less than 12 years of schooling. The cut-off point of this scale for the detection of mild cognitive impairment in its original version is 26. This test has been used in previous research to assess cognitive impairment in people with long COVID (73, 74).
The presence of short-term memory impairment will be measured by using the Spanish version of the Memory Impairment Screen (MIS). This short test assesses the presence of memory disturbances by testing free recall (without clues) or selective recall (with semantic clues) of four words. Dementia screening has adequate interobserver (0.85) and test–retest (0.81) reliability. One point is awarded per word recalled with the help of semantic clues, and two points per word obtained by free recall. The total score ranges from 0 to 8, with a score of ≤4 points indicating possible deterioration (55, 56).
The Semantic Verbal Fluency Test (Animals) will be used to assess whether verbal fluency is affected. The test–retest reliability is 0.68. This test consists of counting the number of correct words within the ‘Animals’ category, reproduced for 1 min. Normally, a healthy person will be able to reproduce about 16 words per minute (57, 58).
The Stroop Colour and Word Test will be used to assess processing speed. This test consists of three phases spread over three different pages. On the first page, the words “red”, “green” and “blue” are printed in black ink, randomly repeated in columns. On the second page, the element “XXXX” appears repeatedly and in columns, printed in red, green or blue ink. On the third page, the words “red”, “green” and “blue” are printed in red, green or blue, but the words do not match the colour in which they are printed. The patient must, by columns, read words or name the ink colours as quickly as possible for 45 s (75, 76). There are scales corrected for age (7–80 years) to calculate the total score for this test. In the various existing versions, this test has shown consistent reliability, obtaining indices of 0.85, 0.81 and 0.69 for the three direct scores (59).
2.6.2.4. Functional physical variables
The Sit to Stand Test will be used to measure the strength and endurance of the lower limbs (60). The 30-s version of this test will be used; it is specifically designed to detect respiratory diseases (58). It evaluates endurance at high power or speed in terms of muscular endurance or strength by recording the number of times a person can stand up and sit down completely in 30 s. This instrument had good test–retest reliability (0.84 < R < 0.92). The 30-s Sit to Stand Test has been translated into Spanish and used in patients with COVID-19 (77).
2.6.2.5. Affective variables
The affective state will be evaluated by using the Hospital Anxiety and Depression Scale (HADS) questionnaire (61). This is a self-report-based scale designed to screen for depression and anxiety disorders in primary care settings. It consists of 14 items that assess symptoms of anxiety and depression (HADS-A and HADS-D, respectively), each item corresponding to a 4-point scale (0–3), with a score range from 0 to 21 for anxiety symptoms and depression symptoms. Higher scores indicate more severe symptoms. To facilitate its use in international trials, this test has been translated into multiple languages, including Spanish (78).
2.6.2.6. Sleep quality
The Insomnia Severity Index (ISI) will be used to measure the participants’ sleep quality (60). This is a self-report that measures the patient’s perception of nocturnal and daytime symptoms of insomnia: difficulty falling asleep or staying asleep, waking up early in the morning, satisfaction with the current sleep pattern, interference with the daily functioning, perceived impairment attributed to sleep deprivation and level of distress or worry caused by the lack. This scale has seven items, each of which is scored from 0 to 4. The total score ranges from 0 to 28, with a higher score indicating more severe insomnia. The Spanish version of the ISI (79) has shown adequate internal consistency (Cronbach’s alpha = 0.82). This test has already been used in other studies about long COVID (80).
2.6.2.7. Personal constructs
Self-efficacy will be measured by using the Self-Efficacy Scale-12 (64). The original scale consists of 17 items that are scored using a 5-point Likert scale. Woodruff and Cashman (81) derived a factor structure representing the three aspects underlying the scale: willingness to initiate the behaviour (“Initiative”), willingness to strive to complete the behaviour (“Effort”) and persistence in the face of adversity (“Persistence”). These are the three factors that this scale evaluates. Five items have been excluded due to low item-remainder correlations and ambiguous wording, resulting in a 12-item version (GSES-12). The total scale has a Cronbach’s alpha of 0.69, and its internal consistency is 0.64 for “Initiative”, 0.63 for “Effort” and 0.64 for “Persistence” (82).
The Health Literacy Europe Questionnaire (HLS-EUQ16) will be used to measure the health literacy of the participants (79). This is defined as the motivation of the population, their knowledge and their individual capacity to understand and make decisions regarding the promotion and maintenance of their health. The questionnaire consists of 16 items, each scored from 1 (very easy) to 4 (very difficult). The total score is obtained by adding the scores of all the items. The final score can be converted into a dichotomous answer: very difficult and difficult = 0; easy and very easy = 1. Poorer health literacy is indicated by higher scores. The official Spanish version presents high consistency (Cronbach’s alpha = 0.982) (83).
The activation of the patient about his own health will be measured by using the Patient Activation Measure (PAM) (66). This tool evaluates the skills, knowledge and confidence perceived by the patient when carrying out health self-management activities. It comprises 13 items that are evaluated on a Likert-type scale from 1 (totally disagree) to 4 (totally agree). The resulting score ranges from 13 to 52, with higher scores indicating higher levels of activation. There is only one official version in Spanish that applies to patients with chronic disease. It has a reliability of 0.98 and a parametric discrimination index of 6.64 (84).
2.6.2.8. Personal satisfaction with the content and tools
In the last assessment, using a Likert-type scale from 0 to 10, the level of satisfaction both with the content of the program and with the tools used for its development will be assessed.
2.7. Statistical analysis
First, a descriptive analysis (frequencies and percentages for categorical variables; and means and standard deviation for continuous variables) and a univariate analysis [one-way analysis of variance (ANOVA) for quantitative variables and the chi-square test for qualitative variables] will be used to examine the data and to test whether there are baseline differences between the groups after randomisation. Second, to answer the main objective—whether there are differences between treatment groups regarding their effectiveness in improving quality of life, linear mixed-effects models (LMEMs) (85) will be used. Cohen’s d will be calculated from the estimated mean values of SF-36 and its standard deviations (SD) at baseline (86). Moreover, LMEMs with the same aforementioned components will be used to analyse whether there are differences between the groups with respect to the improvement of the secondary variables.
The results from the trial will be presented as regression coefficients for predicting change in primary and secondary outcomes with 95% confidence intervals. LMEMs will be tested against a Bonferroni-adjusted alpha level of 0.01 (0.05/5) (87).
Data collection and statistical analysis will be performed by using Excel software, R statistical software (version 3.6.2) (88) and SPSS software (version 25.0) (89).
3. Discussion
The number of people with long COVID, most of them young and without previous pathologies, continues to increase. However, due to the limited scientific evidence, this pathology is still largely unknown in primary care, and patients still find it difficult to receive recognition, support, medical evaluation and treatment for this condition (90, 91).
There is no standard protocol for the treatment of long COVID. Programmes are being designed with the aim of improving the physical health and mental well-being of these patients; however, some key points such as the content of these programmes, the method of offering them and their duration, among other factors, are still being investigated. These programmes include pharmacological treatments and other approaches such as pulmonary and cardiac rehabilitation, fatigue treatment, etc. These types of disease management are primarily directed at symptom control (92).
Long COVID is considered a multisystem syndrome, and > 100 different symptoms—general, physical, respiratory, cognitive, psychological, etc.—have been reported. Hence, the treatment approach requires an interdisciplinary vision that includes, among others, physical rehabilitation, cognitive rehabilitation, respiratory physiotherapy and psychological intervention, and whose objective is to recover the functional state prior to the disease. In addition, due to the heterogeneity of each case, rehabilitation programmes must be personalised (1, 93).
In recent years, especially during the COVID-19 pandemic when face-to-face contact was limited, the use of digital technology has optimised traditional medical care, improving safety, efficacy and adherence to treatments (94).
The evidence supports the use of digital interventions, highlighting their potential in the control of persistent physical and psychological symptoms of COVID-19, and improving the quality of life of people with these symptoms (9, 28, 95–98). However, Rinn et al., in their scoping review, state that research is still needed on individualized digital interventions that better suit the requirements of these patients (99).
To the best of our knowledge, this is the first randomised controlled trial that will be carried out with the objective of analysing the effectiveness of an interdisciplinary and online multimodal intervention, through videoconferences, in addressing the symptoms of people with Long COVID and in improving their quality of life.
This project has strengths and limitations. Among the strengths are that its national and remote character through videoconferences will offer people with long COVID the opportunity to expand their support network and to learn about similar experiences and resources offered in other communities. The online platform used for support will give the patients access to all of the content, and the videoconferences will promote adherence to the programme, as well as the personalisation of the therapeutic recommendations offered in it. Among the limitations of the study are possible technological barriers as well as the lack of knowledge and skills related to information and communication technologies by some users. Another limitation may be the possible dropout of study participants, which might happen due to reinfections that cause their health status to worsen, or to the search for other face-to-face, individualised and more personalised health care resources during the study. Nonetheless, the reasons for dropout and other problems that may arise throughout the research project will be collected by the researchers in accordance with the Mechanisms of Action in Group-based Intervention (MAGI) framework (100).
4. Ethics and dissemination
Ethical approval was granted by the Clinical Research Ethics Committee of Aragon (PI22/482). The procedures carried out for the production of this work were adjusted to the ethical standards of the aforementioned committee and with the 1975 Declaration of Helsinki.
Study participants will receive written information about the conditions of the study, voluntary participation, the right to leave the study at any time, data security, and the publication of anonymized results. In addition, all subjects will sign a written informed consent form; their data will be anonymised and used only for research purposes. The study participants will be informed of the results. The ethics committee will be notified of any modification or change in the protocol.
The trial results will be submitted for publication in peer-reviewed journals. In addition, the study and its results will be disseminated through conferences conferences and researchcongresses.
5. Conclusion
There is still a great lack of knowledge regarding the management of long COVID and its myriad symptoms. Hence, there is an urgent need to continue increasing the scientific evidence and to delve into this disease, considering that the multidisciplinary socio-sanitary teams can offer the necessary care so that these patients achieve their recovery.
Ethics statement
Ethical approval was granted by the Clinical Research Ethics Committee of Aragon (PI22/482). Written informed consent to participate in this study will be obtained from the patients/participants prior to their participation.
Author contributions
SL-H, RM-B, BO-B, and FM-L designed the study protocol with important contributions of LS-R and CMJ. SL-H and BO-B wrote the main manuscript text. All authors contributed to the article and approved the submitted version.
Funding
This work is supported by Carlos III Health Institute, grant number PI21/01356, FEDER Funds “Another way to make Europe.” The funders have no role in study design, data collection, analysis, decision to publish or manuscript preparation. The funding organisation will conduct an audit trial once a year.
Acknowledgments
We wish to thank the Aragonese Primary Care Research Group (GAIAP, B21_23R) that is part of the Department of Innovation, Research and University in the Government of Aragón (Spain) and the Institute for Health Research Aragón (IIS Aragón); the Research Network on Chronicity, Primary Care and Health Promotion (RICAPPS, RD21/0016/0005) that is part of the Results-Oriented Cooperative Research Networks in Health (RICORS) (Carlos III Health Institute); and Feder Funds “Another way to make Europe”.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1222888/full#supplementary-material
References
1. Yong, SJ. Long COVID or post-COVID-19 syndrome: putative pathophysiology, risk factors, and treatments. Infect Dis (Lond). (2021) 53:737–54. doi: 10.1080/23744235.2021.1924397
2. Taheri, M, Esmaeili, A, Irandoust, K, Mirmoezzi, M, Souissi, A, Laher, I, et al. Mental health, eating habits and physical activity levels of elite Iranian athletes during the COVID-19 pandemic. Sci Sports. (2023) 38:527–33. doi: 10.1016/j.scispo.2023.01.002
3. Subramanian, A, Nirantharakumar, K, Hughes, S, Myles, P, Williams, T, Gokhale, KM, et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat Med. (2022) 28:1706–14. doi: 10.1038/s41591-022-01909-w
4. Lai, CC, Hsu, CK, Yen, MY, Lee, PI, Ko, WC, and Hsueh, PR. Long COVID: an inevitable sequela of SARS-CoV-2 infection. J Microbiol Immunol Infect. (2022) 56:1–9. doi: 10.1016/j.jmii.2022.10.003
5. Lechner-Scott, J, Levy, M, Hawkes, C, Yeh, A, and Giovannoni, G. Long COVID or post COVID-19 syndrome. Mult Scler Relat Disord. (2021) 55:103268. doi: 10.1016/j.msard.2021.103268
6. Malik, P, Patel, K, Pinto, C, Jaiswal, R, Tirupathi, R, Pillai, S, et al. Post-acute COVID-19 syndrome (PCS) and health-related quality of life (HRQoL)-a systematic review and meta-analysis. J Med Virol. (2022) 94:253–62. doi: 10.1002/jmv.27309
7. Ramakrishnan, RK, Kashour, T, Hamid, Q, Halwani, R, Tleyjeh, IM, Ben, A, et al. Unraveling the mystery surrounding post-acute sequelae of COVID-19. Front Immunol. (2021) 12:12. doi: 10.3389/fimmu.2021.686029
8. Fernández-de-las-Peñas, C, Martín-Guerrero, JD, Florencio, LL, Navarro-Pardo, E, Rodríguez-Jiménez, J, Torres-Macho, J, et al. Clustering analysis reveals different profiles associating long-term post-COVID symptoms, COVID-19 symptoms at hospital admission and previous medical co-morbidities in previously hospitalized COVID-19 survivors. Infection. (2023) 51:61–9. doi: 10.1007/s15010-022-01822-x
9. Harenwall, S, Heywood-Everett, S, Henderson, R, Godsell, S, Jordan, S, Moore, A, et al. Post-COVID-19 syndrome: improvements in health-related quality of life following psychology-led interdisciplinary virtual rehabilitation. J Prim Care Community Health. (2021) 12:215013192110676. doi: 10.1177/21501319211067674
10. Bernal-Utrera, C, Montero-Almagro, G, Anarte-Lazo, E, Gonzalez-Gerez, JJ, Rodriguez-Blanco, C, and Saavedra-Hernandez, M. Therapeutic exercise interventions through telerehabilitation in patients with post COVID-19 symptoms: a systematic review. J Clin Med. (2022) 11:7521. doi: 10.3390/jcm11247521
11. Banerjee, I, Robinson, J, and Sathian, B. Treatment of long COVID or post COVID syndrome: a pharmacological approach. Nepal J Epidemiol. (2022) 12:1220–3. doi: 10.3126/nje.v12i3.48532
12. Fischer, A, Badier, N, Zhang, L, Elbéji, A, Wilmes, P, Oustric, P, et al. Long COVID classification: findings from a clustering analysis in the predi-COVID cohort study. Int J Environ Res Public Health. (2022) 19:16018. doi: 10.3390/ijerph192316018
13. World Physiotherapy. Respuesta de World Physiotherapy al COVID-19. Documento informativo 9. Abordajes de rehabilitación seguros para las personas que padecen COVID persistente: actividad física y ejercicio. London, UK: World Physiotherapy (2021).
14. Venkatesan, P. NICE guideline on long COVID. Lancet Respir Med. (2021) 9:129. doi: 10.1016/S2213-2600(21)00031-X
15. Yelin, D, Moschopoulos, CD, Margalit, I, Gkrania-Klotsas, E, Landi, F, Stahl, JP, et al. ESCMID rapid guidelines for assessment and management of long COVID. Clin Microbiol Infect. (2022) 28:955–72. doi: 10.1016/j.cmi.2022.02.018
16. Sociedad Española de Médicos Generales y de Familia (SEMG). Guía Clínica Para Atención de COVID Persistente. Madrid, Spain: SEMG (2021).
17. World Health Organization. (2021). Regional Office for Europe. Support for rehabilitation: self-management after COVID-19-related illness, second edition. Available at: https://apps.who.int/iris/handle/10665/344472 (Accessed February 17, 2023).
18. Koc, HC, Xiao, J, Liu, W, Li, Y, and Chen, G. Long COVID and its management. Int J Biol Sci. (2022) 18:4768–80. doi: 10.7150/ijbs.75056
19. Brown, K, Yahyouche, A, Haroon, S, Camaradou, J, and Turner, G. Long COVID and self-management. Lancet. (2022) 399:355. doi: 10.1016/S0140-6736(21)02798-7
20. Veliz, PT, Zhou, W, Smith, S, and Larson, JL. Substance use and the self-management of persistent symptoms of COVID-19. Subst Use Misuse. (2023) 58:835–40. doi: 10.1080/10826084.2023.2184208
21. Miyake, E, and Martin, S. Long COVID: online patient narratives, public health communication and vaccine hesitancy. Digit Health. (2021) 7:7. doi: 10.1177/20552076211059649
22. Barrera-Algarín, E, Sarasola, JL, Sarasola Fernández, A, and Vallejo, AA. Escala de Aceptación Tecnológica en Trabajadores Sociales: Ventajas en el uso de las tecnologías de teletrabajo. Acciones e investigaciones sociales. (2022) 43:91–123. doi: 10.26754/ojs_ais/accioninvestigsoc.2022437423
23. Estebanez-Pérez, MJ, Pastora-Bernal, JM, and Martín-Valero, R. The effectiveness of a four-week digital physiotherapy intervention to improve functional capacity and adherence to intervention in patients with long COVID-19. Int J Environ Res Public Health. (2022) 19:9566. doi: 10.3390/ijerph19159566
24. Romaszko-Wojtowicz, A, Maksymowicz, S, Jarynowski, A, Jaśkiewicz, Ł, Czekaj, Ł, and Doboszyńska, A. Telemonitoring in long-COVID patients-preliminary findings. Int J Environ Res Public Health. (2022) 19:5268. doi: 10.3390/ijerph19095268
25. Taheri, M, Irandoust, K, Reynoso-Sánchez, LF, Muñoz-Helú, H, Cruz-Morales, KN, Torres-Ramírez, R, et al. Effects of home confinement on physical activity, nutrition, and sleep quality during the COVID-19 outbreak in amateur and elite athletes. Front Nutr. (2023) 10:10. doi: 10.3389/fnut.2023.1143340
26. He, J, and Yang, T. In the era of long COVID, can we seek new techniques for better rehabilitation? Chronic Dis Transl Med. (2022) 8:149–53. doi: 10.1002/cdt3.42
27. Reis, N, Dias, MJC, Sousa, L, Agostinho, I, Ricco, MT, Henriques, MA, et al. Telerehabilitation in the transitional care of patients with sequelae associated with COVID-19: perception of Portuguese nurses. Int J Environ Res Public Health. (2022) 19:17096. doi: 10.3390/ijerph192417096
28. Valverde-Martínez, MÁ, López-Liria, R, Martínez-Cal, J, Benzo-Iglesias, MJ, Torres-Álamo, L, and Rocamora-Pérez, P. Telerehabilitation, a viable option in patients with persistent post-COVID syndrome: a systematic review. Healthcare (Basel). (2023) 11:187. doi: 10.3390/healthcare11020187
29. Aiyegbusi, OL, Hughes, SE, Turner, G, Rivera, SC, McMullan, C, Chandan, JS, et al. Symptoms, complications and management of long COVID: a review. J R Soc Med. (2021) 114:428–42. doi: 10.1177/01410768211032850
30. Samper-Pardo, M, León-Herrera, S, Oliván-Blázquez, B, Benedé-Azagra, B, Magallón-Botaya, R, Gómez-Soria, I, et al. Development and validation of a mobile application as an adjuvant treatment for people diagnosed with long COVID-19: protocol for a co-creation study of a health asset and an analysis of its effectiveness and cost-effectiveness. Int J Environ Res Public Health. (2022) 20:462. doi: 10.3390/ijerph20010462
31. Ozduran, E, and Büyükçoban, S. A content analysis of the reliability and quality of Youtube videos as a source of information on health-related post-COVID pain. PeerJ. (2022) 10:e14089. doi: 10.7717/peerj.14089
32. Schulz, KF, Altman, DG, and Moher, D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMC Med. 8:8(18). doi: 10.1186/1741-7015-8-18
33. Chen, CH, Chen, YJ, Tu, HP, Huang, MH, Jhong, JH, and Lin, KL. Benefits of exercise training and the correlation between aerobic capacity and functional outcomes and quality of life in elderly patients with coronary artery disease. Kaohsiung J Med Sci. (2014) 30:521–30. doi: 10.1016/j.kjms.2014.08.004
34. Pita Fernández, S. (2023) Guía: Determinación del tamaño muestral - Fisterra. Available at: https://www.fisterra.com/formacion/metodologia-investigacion/determinacion-tamano-muestral/ (Accessed July 17, 2023).
35. Pinzon, RT, Wijaya, VO, Al, JA, Nunsio, PN, and Buana, RB. Persistent neurological manifestations in long COVID-19 syndrome: a systematic review and meta-analysis. J Infect Public Health. (2022) 15:856–69. doi: 10.1016/j.jiph.2022.06.013
36. De Luca, R, Bonanno, M, and Calabrò, RS. Psychological and cognitive effects of long COVID: a narrative review focusing on the assessment and rehabilitative approach. J Clin Med. (2022) 11:6554. doi: 10.3390/jcm11216554
37. Orfei, MD, Porcari, DE, D’Arcangelo, S, Maggi, F, Russignaga, D, and Ricciardi, E. A new look on long-COVID effects: the functional brain fog syndrome. J Clin Med. (2022) 11:5529. doi: 10.3390/jcm11195529
38. Altuna, M, Sánchez-Saudinós, MB, and Lleó, A. Cognitive symptoms after COVID-19. Neurol Perspect. (2021) 1:S16–24. doi: 10.1016/j.neurop.2021.10.005
39. Daines, L, Zheng, B, Pfeffer, P, Hurst, JR, and Sheikh, A. A clinical review of long-COVID with a focus on the respiratory system. Curr Opin Pulm Med. (2022) 28:174–9. doi: 10.1097/MCP.0000000000000863
40. García-Saugar, M, Jaén-Jover, C, Hernández-Sánchez, S, Poveda-Pagán, EJ, and Lozano-Quijada, C. Recommendations for outpatient respiratory rehabilitation of long COVID patients. An Sist Sanit Navar. (2022) 45:e0978. doi: 10.23938/ASSN.0855
41. ACSM. Guidelines for exercise testing and prescription 11th. Paper Knowledge Toward a Media History of Documents (2022);7(2):107–115. Available at: https://www.worldcat.org/title/1232233224
42. Humphreys, H, Kilby, L, Kudiersky, N, and Copeland, R. Long COVID and the role of physical activity: a qualitative study. BMJ Open. (2021) 11:e047632. doi: 10.1136/bmjopen-2020-047632
43. Wright, J, Astill, SL, and Sivan, M. The relationship between physical activity and long COVID: a cross-sectional study. Int J Environ Res Public Health. (2022) 19:5093. doi: 10.3390/ijerph19095093
44. Jimeno-Almazán, A, Pallarés, JG, Buendía-Romero, Á, Martínez-Cava, A, Franco-López, F, Sánchez-Alcaraz Martínez, BJ, et al. Post-COVID-19 syndrome and the potential benefits of exercise. Int J Environ Res Public Health. (2021) 18:5329. doi: 10.3390/ijerph18105329
45. Rothenberg, E. Coronavirus disease 19 from the perspective of ageing with focus on nutritional status and nutrition management-a narrative review. Nutrients. (2021) 13:1294. doi: 10.3390/nu13041294
46. Nguyen-Hoang, A. Nutrition therapy for long COVID. Br J Nurs. (2021) 30:S28–9. doi: 10.12968/bjon.2021.30.21.S28
47. Scarpelli, S, De Santis, A, Alfonsi, V, Gorgoni, M, Morin, CM, Espie, C, et al. The role of sleep and dreams in long-COVID. J Sleep Res. (2023) 32:e13789. doi: 10.1111/jsr.13789
48. Samper-Pardo, M, Oliván-Blázquez, B, Magallón-Botaya, R, Méndez-López, F, Bartolomé-Moreno, C, and León-Herrera, S. The emotional well-being of long COVID patients in relation to their symptoms, social support and stigmatization in social and health services: a qualitative study. BMC Psychiatry. (2023) 23:68. doi: 10.1186/s12888-022-04497-8
49. Tíscar-González, V, Sánchez-Gómez, S, Lafuente Martínez, A, Peña Serrano, A, Twose López, M, Díaz Alonso, S, et al. Experiences and impact on the quality of life of people with long COVID. Gac Sanit. (2022) 37:102247. doi: 10.1016/j.gaceta.2022.102247
50. Alonso, J, Prieto, L, and Antó, JM. The Spanish version of the SF-36 health survey (the SF-36 health questionnaire): an instrument for measuring clinical results. Med Clin (Barc). (1995) 104:771–6.
51. Alonso, J, Regidor, E, Barrio, G, Prieto, L, Rodríguez, C, and de la Fuente, L. Population reference values of the Spanish version of the health questionnaire SF-36. Med Clin (Barc). (1998) 111:410–6.
52. Lozano Gallego, M, Hernández Ferrándiz, H, Turró Garriga, O, Pericot Nierga, I, López-Pausa, S, and Vilalta Franch, J. Validación del Montreal Cognitive Assessment (MoCA): test de cribado para el deterioro cognitivo leve. Datos preliminares. Alzheimer Real Invest Demenc. (2009) 43:4–11.
53. Gomez-Moreno, SM, Cuadrado, ML, Cruz-Orduña, I, Martínez-Acebes, EM, Gordo-Mañas, R, Fernández-Pérez, C, et al. Validation of the Spanish-language version of the Montreal cognitive assessment as a screening test for cognitive impairment in multiple sclerosis. Neurologia. (2022) 37:726–34. doi: 10.1016/j.nrleng.2019.11.007
54. Nasreddine, ZS, Phillips, NA, Bédirian, V, Charbonneau, S, Whitehead, V, Collin, I, et al. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. (2005) 53:695–9. doi: 10.1111/j.1532-5415.2005.53221.x
55. Terrón Cuadrado, C, Peña Casanova, J, Manero, RM, Böhm, P, Gramunt Fombuena, N, and Quiñones, US. Versión española del Memory Impairment Screen (MIS): datos normativos y de validez discriminativa. Neurología. (2005) 20:402–11. Available at: https://dialnet.unirioja.es/servlet/articulo?codigo=1334310
56. Pérez-Martinez, DA, Baztán, JJ, González-Becerra, M, and Socorro, A. Evaluation of the diagnostic value of a Spanish adaptation of the Buschke memory impairment screen in the detection of dementia and cognitive impairment. Rev Neurol. (2005) 40:644–8. doi: 10.33588/rn.4011.2004644
57. Harrison, JE, Buxton, P, Husain, M, and Wise, R. Short test of semantic and phonological fluency: normal performance, validity and test-retest reliability. Br J Clin Psychol. (2000) 39:181–91. doi: 10.1348/014466500163202
58. Ardila, A, Ostrosky-Solís, F, and Bernal, B. Cognitive testing toward the future: the example of semantic verbal fluency (ANIMALS). Int J Psychol. (2006) 41:324–32. doi: 10.1080/00207590500345542
59. Stroop, Golden CJ. Test de Colores y Palabras. Manual (3a Ed). Madrid; (2001). Available at: https://web.teaediciones.com/STROOP-Test-de-Colores-y-Palabras---Edicion-Revisada.aspx (Accessed July 14, 2023).
60. Csuka, M, and McCarty, DJ. Simple method for measurement of lower extremity muscle strength. Am J Med. (1985) 78:77–81. doi: 10.1016/0002-9343(85)90465-6
61. Zigmond, AS, and Snaith, RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
62. Bastien, C. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. (2001) 2:297–307. doi: 10.1016/s1389-9457(00)00065-4
63. Kim, Y, Park, I, and Kang, M. Convergent validity of the international physical activity questionnaire (IPAQ): meta-analysis. Public Health Nutr. (2013) 16:440–52. doi: 10.1017/S1368980012002996
64. Sherer, M, Maddux, JE, Mercandante, B, Prentice-Dunn, S, Jacobs, B, and Rogers, RW. The self-efficacy scale: construction and validation. Psychol Rep. (1982) 51:663–71. doi: 10.2466/pr0.1982.51.2.663
65. Sørensen, K, Pelikan, JM, Röthlin, F, Ganahl, K, Slonska, Z, Doyle, G, et al. Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Public Health. (2015) 25:1053–8. doi: 10.1093/eurpub/ckv043
66. Hibbard, JH, Stockard, J, Mahoney, ER, and Tusler, M. Development of the patient activation measure (PAM): conceptualizing and measuring activation in patients and consumers. Health Serv Res. (2004) 39:1005–26. doi: 10.1111/j.1475-6773.2004.00269.x
67. Vilagut, G, Ferrer, M, Rajmil, L, Rebollo, P, Permanyer-Miralda, G, Quintana, JM, et al. El Cuestionario de Salud SF-36 español: una década de experiencia y nuevos desarrollos. Gac Sanit. (2005) 19:135–50. doi: 10.1157/13074369
68. López-García, E, Banegas, JR, Pérez-Regadera, AG, Gutiérrez-Fisac, JL, Alonso, J, and Rodríguez-Artalejo, F. Valores de referencia de la versión española del Cuestionario de Salud SF-36 en población adulta de más de 60 años. Med Clin (Barc). (2003) 120:568–73. doi: 10.1016/S0025-7753(03)73775-0
69. Bijur, PE, Silver, W, and Gallagher, EJ. Reliability of the visual analog scale for measurement of acute pain. Acad Emerg Med. (2001) 8:1153–7. doi: 10.1111/j.1553-2712.2001.tb01132.x
70. Vaes, AW, Machado, FVC, Meys, R, Delbressine, JM, Goertz, YMJ, Van Herck, M, et al. Care dependency in non-hospitalized patients with COVID-19. J Clin Med. (2020) 9:2946. doi: 10.3390/jcm9092946
71. Greenhalgh, T, Knight, M, A’Court, C, Buxton, M, and Husain, L. Management of post-acute covid-19 in primary care. BMJ. (2020) 370:m3026. doi: 10.1136/bmj.m3026
72. National Health Service (NHS). Long-term effects of coronavirus (long COVID). London, UK: NHS (2022).
73. Cristillo, V, Pilotto, A, Cotti Piccinelli, S, Bonzi, G, Canale, A, Gipponi, S, et al. Premorbid vulnerability and disease severity impact on long-COVID cognitive impairment. Aging Clin Exp Res. (2022) 34:257–60. doi: 10.1007/s40520-021-02042-3
74. Del Brutto, OH, Rumbea, DA, Recalde, BY, and Mera, RM. Cognitive sequelae of long COVID may not be permanent: a prospective study. Eur J Neurol. (2022) 29:1218–21. doi: 10.1111/ene.15215
75. Periáñez, JA, Lubrini, G, García-Gutiérrez, A, and Ríos-Lago, M. Construct validity of the Stroop color-word test: influence of speed of visual search, verbal fluency, working memory, cognitive flexibility, and conflict monitoring. Arch Clin Neuropsychol. (2021) 36:99–111. doi: 10.1093/arclin/acaa034
76. Scarpina, F, and Tagini, S. The Stroop color and word test. Front Psychol. (2017) 8:8. doi: 10.3389/fpsyg.2017.00557
77. Hidayati, ERN, Suharti, A, Suratinoyo, AT, Zahra, SR, and Nusdwinuringtyas, N. Feasibility of the modified 30-second sit-to-stand test in an isolation ward of moderate COVID-19. Medical Journal of Indonesia. (2021) 30:306–10. doi: 10.13181/mji.bc.215477
78. Herrero, MJ, Blanch, J, Peri, JM, De Pablo, J, Pintor, L, and Bulbena, A. A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen Hosp Psychiatry. (2003) 25:277–83. doi: 10.1016/s0163-8343(03)00043-4
79. Fernandez-Mendoza, J, Rodriguez-Muñoz, A, Vela-Bueno, A, Olavarrieta-Bernardino, S, Calhoun, SL, Bixler, EO, et al. The Spanish version of the insomnia severity index: a confirmatory factor analysis. Sleep Med. (2012) 13:207–10. doi: 10.1016/j.sleep.2011.06.019
80. Orrù, G, Bertelloni, D, Diolaiuti, F, Mucci, F, Di Giuseppe, M, Biella, M, et al. Long-COVID syndrome? A study on the persistence of neurological, psychological and physiological symptoms. Healthcare (Basel). (2021) 9:575. doi: 10.3390/healthcare9050575
81. Woodruff, SL, and Cashman, JF. Task, domain, and general efficacy: a reexamination of the self-efficacy scale. Psychol Rep. (1993) 72:423–32. doi: 10.2466/pr0.1993.72.2.423
82. Bosscher, RJ, and Smit, JH. Confirmatory factor analysis of the general self-efficacy scale. Behav Res Ther. (1998) 36:339–43. doi: 10.1016/s0005-7967(98)00025-4
83. Nolasco, A, Barona, C, Tamayo-Fonseca, N, Irles, MÁ, Más, R, Tuells, J, et al. Health literacy: psychometric behaviour of the HLS-EU-Q16 questionnaire. Gac Sanit. (2018) 34:399–402. doi: 10.1016/j.gaceta.2018.08.006
84. Moreno Chico, C. González de Paz L, Monforte Royo C. Adaptación y Validación de la Escala (PAM13), Evaluación de la Activación “Patient Activation Measure 13”, en una Muestra de Pacientes Crónicos Visitados en CAP Rambla Mútua Terrassa; XXIV Premi d’infermeria. Terrasa, Spain: Mútua Terrassa (2018).
85. Singer, JD, and Willett, JB. Applied longitudinal data analysis: modeling change and event occurrence. Oxford: Oxford University Press (2003)
86. McGough, JJ, and Faraone, SV. Estimating the size of treatment effects: moving beyond p values. Psychiatry. (2009) 6:21–9.
87. Haynes, W. Bonferroni correction In: W Dubitzky, O Wolkenhauer, KH Cho, and H Yokota, editors. Encyclopedia of systems biology. New York, NY: Springer (2013). 154.
88. R Core Team. R: A language and environment for statistical computing. R foundation for statistical computing. Vienna, Austria; (2018). Available at: https://www.R-project.org/
90. Sisó-Almirall, A, Brito-Zerón, P, Ferrín, LC, Kostov, B, Moreno, AM, Mestres, J, et al. Long COVID-19: proposed primary care clinical guidelines for diagnosis and disease management. Int J Environ Res Public Health. (2021) 18:4350. doi: 10.3390/ijerph18084350
91. Ziauddeen, N, Gurdasani, D, O’Hara, ME, Hastie, C, Roderick, P, Yao, G, et al. Characteristics and impact of long COVID: findings from an online survey. PLoS One. (2022) 17:e0264331. doi: 10.1371/journal.pone.0264331
92. Greenhalgh, T, Sivan, M, Delaney, B, Evans, R, and Milne, R. Long COVID-an update for primary care. BMJ. (2022) 378:e072117. doi: 10.1136/bmj-2022-072117
93. Ashton, R, Ansdell, P, Hume, E, Maden-Wilkinson, T, Ryan, D, Tuttiett, E, et al. COVID-19 and the long-term cardio-respiratory and metabolic health complications. Rev Cardiovasc Med. (2022) 23:53. doi: 10.31083/j.rcm2302053
94. Flannery, T, Brady-Sawant, H, Tarrant, R, Davison, J, Shardha, J, Halpin, S, et al. A mixed-methods evaluation of a virtual rehabilitation program for self-management in post-COVID-19 syndrome (long COVID). Int J Environ Res Public Health. (2022) 19:12680. doi: 10.3390/ijerph191912680
95. Cahalan, R, Meade, C, and Mockler, S. SingStrong—a singing and breathing retraining intervention for respiratory and other common symptoms of long COVID: a pilot study. Can J Respir Ther. (2022) 58:20–7. doi: 10.29390/cjrt-2021-074
96. Dalbosco-Salas, M, Torres-Castro, R, Rojas Leyton, A, Morales Zapata, F, Henríquez Salazar, E, Espinoza Bastías, G, et al. Effectiveness of a primary care telerehabilitation program for post-COVID-19 patients: a feasibility study. J Clin Med. (2021) 10:4428. doi: 10.3390/jcm10194428
97. Kortianou, EA, Tsimouris, D, Mavronasou, A, Lekkas, S, Kazatzis, N, Apostolara, ZE, et al. Application of a home-based exercise program combined with tele-rehabilitation in previously hospitalized patients with COVID-19: a feasibility, single-cohort interventional study. Pneumonologie. (2022) 35:1–10. doi: 10.18332/pne/146521
98. Samper-Pardo, M, León-Herrera, S, Méndez-López, F, Domínguez-García, M, and Sánchez-Recio, R. Effectiveness of a telerehabilitation intervention using recovery APP of long COVID patients: a randomized, three-month follow-up clinical trial. Sci Rep. (2023) 13:7943. doi: 10.1038/s41598-023-35058-y
99. Rinn, R, Gao, L, Schoeneich, S, Dahmen, A, Anand Kumar, V, Becker, P, et al. Digital interventions for treating post-COVID or long-COVID symptoms: scoping review. J Med Internet Res. (2023) 25:e45711. doi: 10.2196/45711
100. Borek, AJ, Abraham, C, Greaves, CJ, Gillison, F, Tarrant, M, Morgan-Trimmer, S, et al. Identifying change processes in group-based health behaviour-change interventions: development of the mechanisms of action in group-based interventions (MAGI) framework. Health Psychol Rev. (2019) 13:227–47. doi: 10.1080/17437199.2019.1625282
Keywords: long COVID-19, telerehabilitation, multimodal, multidisciplinary, quality of life, effectiveness
Citation: León-Herrera S, Magallón-Botaya R, Oliván-Blázquez B, Sagarra-Romero L, Jaurrieta CM and Méndez-López F (2023) Online multimodal rehabilitation programme to improve symptoms and quality of life for adults diagnosed with long COVID-19: a Randomised Clinical Trial protocol. Front. Public Health. 11:1222888. doi: 10.3389/fpubh.2023.1222888
Edited by:
Nyi Nyi Naing, Sultan Zainal Abidin University, MalaysiaReviewed by:
Nirmal Surya, Epilepsy Foundation India, IndiaArwel Wyn Jones, Alfred Hospital, Australia
Tsuyoshi Tatemoto, Tokyo Bay Rehabilitation Hospital, Japan
Morteza Taheri, University of Tehran, Iran
Copyright © 2023 León-Herrera, Magallón-Botaya, Oliván-Blázquez, Sagarra-Romero, Jaurrieta and Méndez-López. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bárbara Oliván-Blázquez, Ym9saXZhbkB1bml6YXIuZXM=