 Riccardo Serra
Riccardo Serra Yasaman Etemadi
Yasaman Etemadi Marieke van Regteren Altena5
Marieke van Regteren Altena5 Corrado Barbui
Corrado Barbui Lorenzo Tarsitani
Lorenzo Tarsitani
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
POLICY AND PRACTICE REVIEWS article
Front. Public Health , 15 August 2023
Sec. Public Mental Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1215617
Background: The identification of interventions for rehabilitation and related evidence is a crucial step in the development of World Health Organization's (WHO) Package of Interventions for Rehabilitation (PIR). Interventions for rehabilitation may be particularly relevant in schizophrenia, as this condition is associated with a high risk of disability, poor functioning, and lack of autonomy. Aiming to collect evidence for the WHO PIR, we conducted a systematic review of Clinical Practice Guidelines (CPG) on interventions for rehabilitation of schizophrenia.
Methods: Methods for the systematic identification and critical appraisal of CPG were developed by WHO Rehabilitation Programme and Cochrane Rehabilitation under the guidance of WHO's guideline review committee secretariat. The Appraisal of Guidelines for Research & Evaluation Instrument (AGREE II) was used to evaluate the methodological quality of identified CPG.
Results: After full text screening, nine CPG were identified, for a total of 130 recommendations. Three were excluded because their total AGREE-II scores were below cut-off. Six CPG were approved by the Technical Working Group and included for data extraction. Only one CPG with specific focus on rehabilitation of schizophrenia was retrieved. Other CPG were general, including some recommendations on rehabilitation. Some CPG gave no indications on the assessment of rehabilitation needs. Discrepancies were detectable, with different CPG emphasizing different domains. Most recommendations addressed “symptoms of schizophrenia,” while “community and social life” was targeted by few recommendations. International CPG were often conceptualized for high-income countries, and CPG accounting for their implementation in lower income contexts were scarce. Quality of evidence was high/moderate for 41.54% (n = 54) of the recommendations, and very low only in two cases (1.52%). N = 45 (34.62%) were based on experts' opinion.
Conclusions: The concepts of recovery and rehabilitation in schizophrenia are relatively new in medical sciences and somewhat ill-defined. An unbalanced distribution in the domains addressed by available CPG is therefore understandable. However, the need for more focus in some areas of rehabilitation is obvious. More clarity is also required regarding which interventions should be prioritized and which are more feasible for global implementation in the rehabilitation of schizophrenia.
The World Health Organization (WHO) has the strategic priority of achieving Universal Health Coverage (UHC), that means “all people receive quality health services that meet their needs without being exposed to financial hardship in paying for the services” (1). UHC includes rehabilitation interventions among the services to be provided. As part of the WHO Rehabilitation 2030 call for action (2), the WHO Rehabilitation Programme has been developing a Package of Interventions for Rehabilitation (PIR) to support ministries of health in integrating rehabilitation services into health systems (3).
The development of the PIR takes a stepwise approach composed of five consecutive steps: (a) selection of health conditions considering amenability to and the need for rehabilitation, (b) identification of evidence-based interventions for rehabilitation, (c) development of the package with agreement on interventions along with resource requirement descriptions, (d) external peer review, and (e) production of the alpha version of the PIR (3). This paper reports on the second step, which includes the identification of interventions for rehabilitation and related evidence for the health conditions selected in the first step. Under WHO's Guideline Review Committee Secretariat guidance, the WHO Rehabilitation Programme and Cochrane Rehabilitation developed the corresponding methods. Underpinning evidence for the development of the PIR includes a series of systematic reviews of Clinical Practice Guidelines (CPG) for different health conditions selected. Interventions and related evidence identified from these CPG undergo a consensus process to select essential interventions in step 3, to be included in the final PIR. Information related to the provision of the interventions will be added. All information undergoes a review process before developing the final version of the PIR.
Schizophrenia has been selected as one of the priority targets of the PIR. Although not as common as other disabling conditions possibly affecting humans, psychosis resembles the historical antonomasia of mental disability due to its profound long-term effects on individuals, families, and societies. One in 135 people (0.72% of the population), or over 56 million people worldwide, are affected by schizophrenia (4). Proportions are larger in the adult population, due to an incidence peak between the age of 15 and 25 years (4–6). Schizophrenia affects the general population equally, with no substantial difference between males and females, or among urban, rural, and mixed sites (4). Schizophrenia may have a highly detrimental effect on the life of a person and their family, impacting the individual's existence on multiple levels. Especially if left untreated, this condition may progressively deteriorate the personal, familial, relational, educational, and occupational possibilities of a person, accounting for 13.4 million years of life lived with disability globally (6). Profound stigmatization for their condition and their symptoms is the rule rather than the exception for people with schizophrenia across countries, with consequences in terms of social exclusion, isolation, and frequent human rights violation (7–9). This deeply disabling condition is also related to higher odds of dying prematurely due to preventable causes, with a life expectancy of 20 years less than the general population (10, 11).
Despite the high risk of severe, lifelong problems that affect every area of life, around 15% of people with schizophrenia will eventually reach nearly complete recovery (12). The concept of recovery and the concept of rehabilitation share blurred boundaries, and need to be seen as two faces of the same coin. As Anthony (13) well-depicted with regards to recovery from mental illness “Recovery is what people with disabilities do. Treatment, case management, and rehabilitation are what helpers do to facilitate recovery.” Recovery may be related to several interventions, and an early approach is considered pivotal, as highlighted in the recent WHO World Mental Health Report (WMHR), which also emphasized that an holistic multidisciplinary rehabilitation process is key in this population, especially in the long term (14–16). According to WHO, “Rehabilitation helps a child, adult or older person to be as independent as possible in everyday activities and enables participation in education, work, recreation and meaningful life roles such as taking care of family” (17).
Finding a single definition of rehabilitation is challenging, and the differences between rehabilitation for physical and mental health problems add to the difficulty. Since rehabilitation services and techniques have started developing, they sprouted in a multitude of different approaches and theories, sometimes drifting from one another, and leaving a doubt on what rehabilitation actually is. A comprehensive perspective on what constitutes rehabilitation for mental disorders was provided in the consensus statement on psychosocial rehabilitation by the WHO in collaboration with the World Association for Psychosocial Rehabilitation in 1996 (18). In this document rehabilitation is described as “a process that facilitates the opportunity for individuals—who are impaired, disabled or handicapped by a mental disorder—to reach their optimal level of independent functioning in the community,” which is inextricably founded on the individual, the service, and the environment. These concepts kept evolving, broadening the focus not only on “functioning” as part of the social apparatus but also on regaining roles and meaning in each individual life. For example, the Person-Centered Psychiatric Rehabilitation model by Farkas and colleagues (19) states: “Without a process committed to supporting chosen roles and settings, functioning may be improved, but the individual's vision of a meaningful life may still not be achieved. Rehabilitation, therefore, works with social relationships, work, leisure, family life, higher education, and other student pursuits, using interventions that focus on increasing competencies or skills and providing environmental supports.” Similarly, regarding the rehabilitation of mental illness, the National Institute for Health and Care Excellence states: “the guiding principle is the belief that it is possible for someone to regain a meaningful life, despite serious mental illness… it refers to someone achieving the best quality of life they can, while living and coping with their symptoms. It is an ongoing process whereby the person is supported to build up their confidence and skills and resilience, through setting and achieving goals to minimize the impact of mental health problems on their everyday life.” Specifically for the WHO-PIR development, the definition of rehabilitation, used for both physical and mental health conditions, was: “Interventions aiming at improving functioning across all levels of functions (including body functions, activity, and participation) without targeting the cause of the health condition.” Regardless of the specific definition, health systems around the world are urged to put into place appropriate rehabilitation services for people with mental health conditions (16), taking into account the specific individuals, their background and social context, and the available individual and community resources.
Many interventions have shown to be effective as rehabilitation strategies for schizophrenia in well-designed randomized controlled trials. For example, a systematic review on rehabilitation interventions to promote recovery from schizophrenia, identified a total of 80 studies (nine of which were meta-analyses) which consistently provide evidence of the efficacy of interventions such as Cognitive Remediation, Family Psychoeducation, Social Skills Training, and Cognitive Therapy (20). Furthermore, although the healthcare gaps among countries around the world (21, 22), some of these interventions have been successfully implemented in low- and middle-income countries (23, 24). However, given the wide heterogeneity of existing interventions that can be considered as interventions for rehabilitation, policy makers, stakeholders, professionals, and service users may find it difficult to navigate through alternative intervention options and make informed decisions. Some CPG have been developed to organize and summarize existing evidence, but the field of rehabilitation in schizophrenia is still fragmented and somewhat contradictory in terms of recommendations. Therefore, as a base for the WHO PIR, we conducted a systematic review of existing CPG relevant to rehabilitation of people with schizophrenia.
This systematic review of CPG has been developed in full compliance with the methodology presented in the introductory WHO PIR protocol of research (3). These stages have been followed (Figure 1):
• Systematic literature search: CPG have been searched in the following databases: Guidelines International Network (GIN), Scotland's Guidelines International Network (G-I-N), United Kingdom's National Institute for Health and Care Excellence (NICE), Australia's National Health and Medical Research Council (NHMRC), Scottish Intercollegiate Guidelines Network (SIGN), Canadian Medical Association Infobase of Clinical Practice Guidelines (CPG Infobase), New Zealand Guidelines Group (NZGG), United States' National Guideline Clearinghouse (NGC), United Kingdom's eGuidelines, Psychinfo, Pubmed, Google scholar (first 250 results only). The search string used was: “(Guideline*) AND (schizophrenia OR Psychosis) AND (psychosocial OR rehabilitation OR recovery OR functioning).” A filter to include only publications in English language was applied. First search was performed in April 2020, and then it was re-run in March 2021. Only publications from 2010 were considered, aiming to include up-to-date recommendations only.
• Independent title and abstract screening of the retrieved manuscripts by two authors. The screening aimed at retrieving only CPG on schizophrenia. For the title and the abstract screening, inclusion criteria were as follows: “Does the manuscript present a guideline?” “Is the guideline specifically developed for the health condition of interest?” “Is the guideline a guideline on rehabilitation interventions?” “Is the guideline not older than 10 years?”. Only if all four questions were answered with “Yes” the screening author would endorse “Yes” for that reference. If at least one of the two authors had endorsed “Yes” that reference would proceed to the next step. The same was applied for both title and abstract screening.
• Independent full text screening. The full text screening applied the same previous criteria plus two more as follows: “Is it clear that there is no conflict of interest?” “Is information on the strength of the recommendation provided?”. If all questions were answered “yes” then the author would endorse “yes” for that reference. If at least one of the two authors had endorsed “Yes” that reference would be included in the next step.
• Independent evaluation of the CPG quality with the “Appraisal of Guidelines for Research and Evaluation” (AGREE II) tool by two authors (RS and YE) (25): a specific focus has been given to items 7, 8, 12, and 22 where the average result had to be >2 (AGREE/4), and to the items 4, 7, 8, 10, 12, 13, 15, 22, and 23 whose average sum score had to be >45 (AGREE/9). Evaluation discrepancies were confronted and an average grade of the two separate evaluation was applied.
• CPG fitting AGREE II criteria were given a final consensus for inclusion according to the using the WHO prioritization criteria (quality, publication time, multiprofessionality, comprehensiveness) (3).
• Data extraction was independently performed by two authors using a standardized form which includes information on the type of recommendation, dosage, target group, strength of recommendation and quality of the background evidence in support to the recommendation.
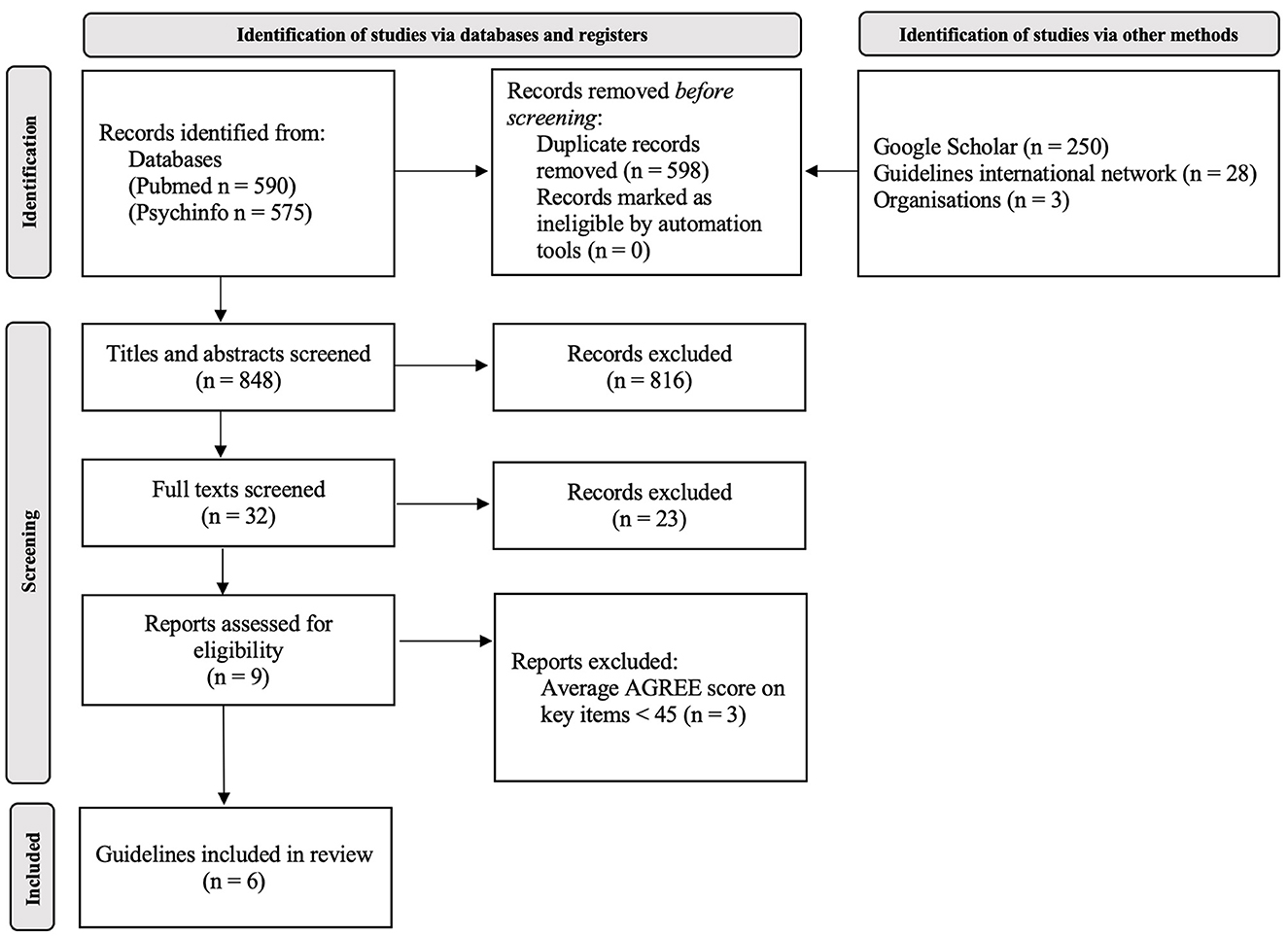
Figure 1. Results of the search and screening process for identification of suitable guidelines.
Topics/areas considered by the selected CPG into each main type of recommendation (assessment and intervention) have been extracted. Recommendations regarding the management of the acute phase of illness, recommendations on medications and side-effects, as well as service recommendations were excluded, therefore leading to a selection of non-drug-related recommendations on the long-term course of the treatment. The topics (functioning domains) from different CPG have been compared independently by two authors and integrated. If needed, agreement by discussion was reached involving a third author. The process has been repeated for all the CPG until final agreement on the topics was reached.
Results of the literature search are shown in Figure 1, in agreement with the PRISMA statement (26). A total of nine CPG were selected on the basis of abstract and full-text screening. Details on the abstract and full-text screening are shown in Supplementary Table 1. As shown in Table 1, three of these were excluded due to a total AGREE-II score <45 (27–29), leading to the inclusion of six guidelines (25). The six CPG were approved by the Technical Working Group and included for data extraction:
– German Association for Psychiatry, Psychotherapy and Psychosomatics Revised S3 guidelines on schizophrenia (DGPPN) (30).
– The American Psychiatric Association Practice Guideline for the Treatment of Patients with Schizophrenia (APA) (31).
– Scottish Intercollegiate Guidelines Network: management of schizophrenia (SIGN) (32).
– National Institute for Health and Care Excellence Psychosis and schizophrenia in children and young people: recognition and management (NICE-1) (33).
– National Institute for Health and Care Excellence Psychosis and schizophrenia in adults: prevention and management (NICE-2) (34).
– National Institute for Health and Care Excellence Rehabilitation for adults with complex psychosis (NICE-3) (35).
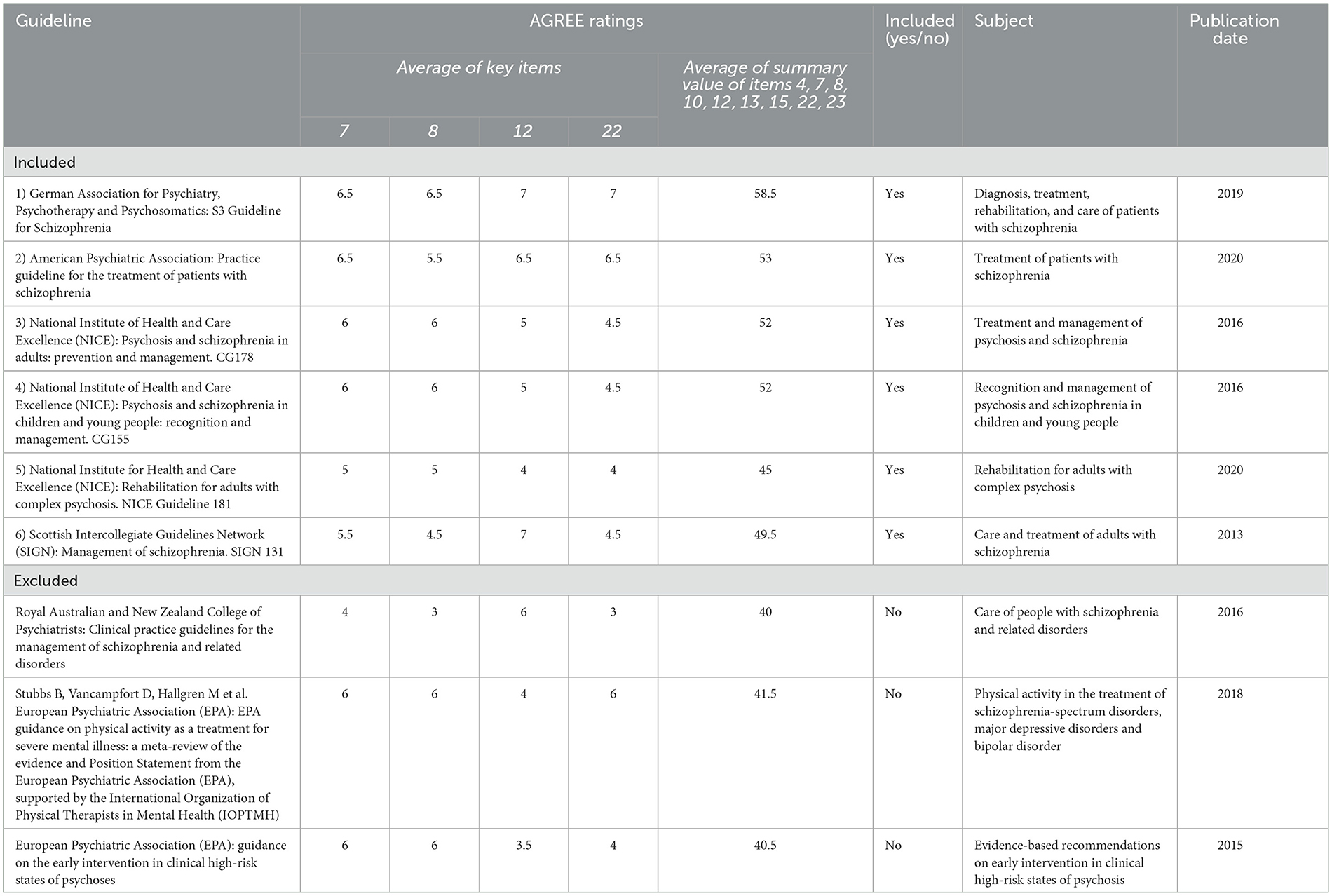
Table 1. Main characteristics of included and excluded guidelines of rehabilitation interventions for people with schizophrenia and related psychosis.
In addition to the selected CPG, relevant WHO guidelines including mhGAP Evidence-based recommendations for management of psychosis and bipolar disorders in non-specialized health settings as well as management of physical health conditions in adults with severe mental disorders were included for the development of PIR. However, these resources have not been included in this review.
The topics (functioning domains) extracted from included CPG are presented by type of recommendation (assessment/intervention) in Table 2. The original recommendations from included CPG, related quality of evidence (QoE) and the strength of recommendation (SoR) are presented in Table 3. As seen in Table 2, different topics of intervention are resumed in the first column, and each line presents the number of interventions on that specific topic for each included CPG. Recommendations are reported multiple times if the original recommendation included multiple target outcomes or multiple interventions for the same target. SoR and QoE are presented in a standardized fashion to avoid discrepancies in terms used among CPG. Rationale applied to this classification and original classifications are presented in Supplementary Table 2. Among all CPG, only NICE-3 had a specific focus on the rehabilitation of schizophrenia (35).
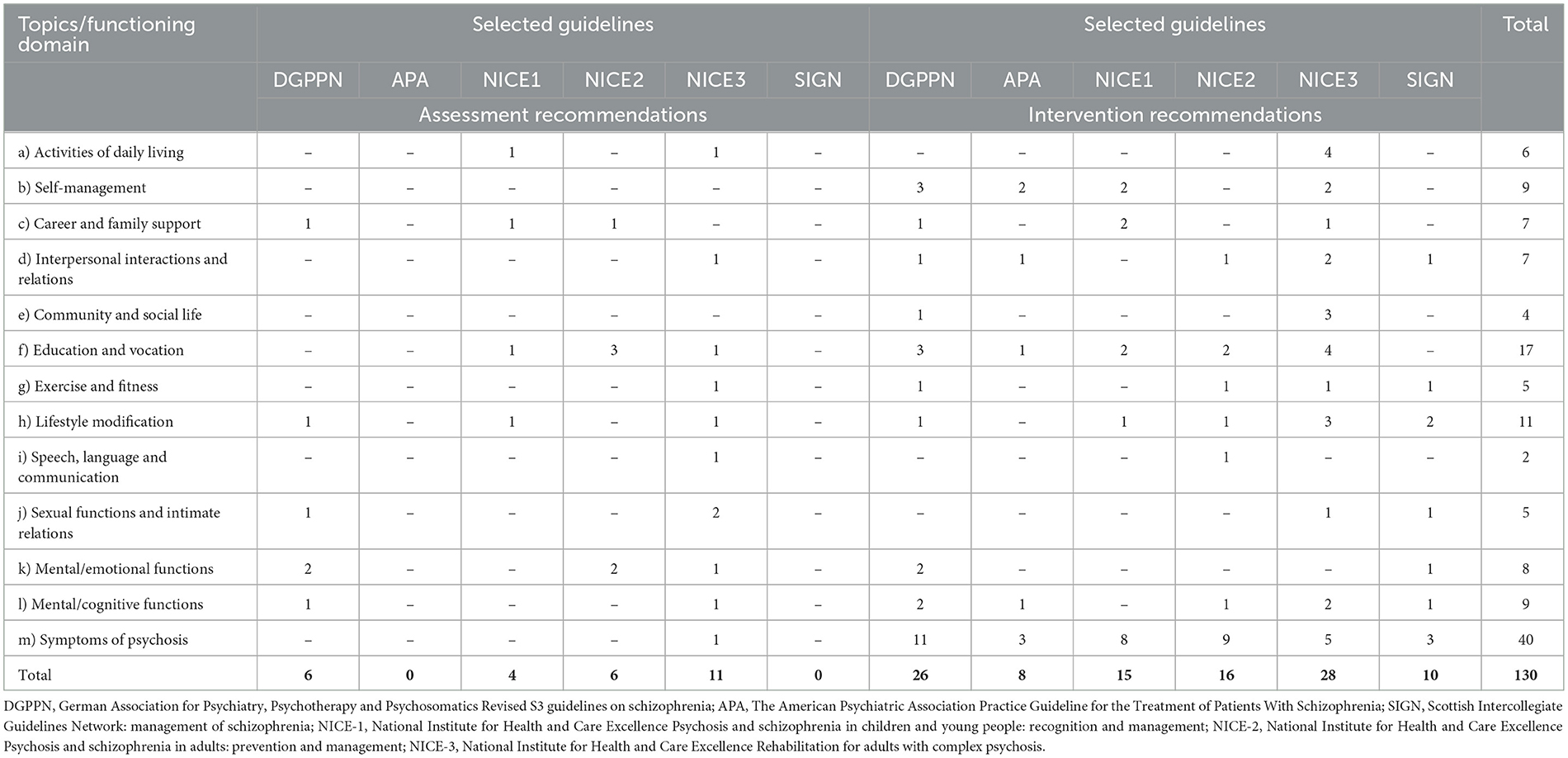
Table 2. Number of recommendations per topic (functioning domain) and recommendation type.

Table 3. Recommendations from selected CPG with reported strength of recommendation and quality of the evidence.
For assessment recommendations, “Mental/Emotional functions” and “Education and Vocation” were the functioning domains with the highest number of recommendations. Assessment recommendations for “Interpersonal interactions and relations,” “Exercise and fitness,” and “Speech, language and communication” were provided in NICE-3, and “Activities of daily living” in NICE-1 and NICE-3. In terms of providing specific assessment recommendations, “self-management” or “community and social life” domains were not addressed in the CPG.
Regarding intervention recommendations, all six CPG provided many recommendations addressing “symptoms of psychosis” which was the domain with the highest number of recommendations. A high number of interventions were also provided for “Education and Vocation” and “Self-management,” 12 and nine, respectively. All CPG, except for SIGN and NICE-1 respectively, addressed “Education and Vocation” as well as “Mental/cognitive functions” and “Interpersonal interactions and relations.” A total of six domains, out of 13 were targeted by low number of recommendations (4 or less) including “community and social life” (addressed by NICE-3), and “activities of daily living” (addressed by NICE-3 and DGPPN).
The QoE for given recommendations was high for 20.77% (n = 27) of the recommendations. The same number of recommendations had a moderate QoE (n = 27; 20.77%) while n = 20 (15.38%) had low QoE. Only two recommendations (1.52%) had very low QoE, and nine (6.92%) were based on U.K. prevalence studies. A total n = 45 (34.62%) of the recommendations is based on experts' opinions. Experts' opinions are used for recommendations on generally good clinical practice (e.g., informing carers on their statutory rights. See Table 3), as well as to support clinically available interventions in lack of sufficient available evidence (e.g., “We suggest offering cognitive remediation in combination with other psychosocial and rehabilitative treatment methods”). SoR is strong for more than half of the recommendations (n = 81; 62.3%). Within these strong recommendations, n = 25 is based on Experts' opinion. A minority of recommendations (n = 37; 28.46%) is conditional, while the rest (n = 12; 9.23%) indicates no strength of recommendation and is based on Experts' opinion.
In this systematic review we summarized existing recommendations from high-quality CPG on rehabilitation interventions for people with schizophrenia. Only one CPG with a specific focus on the rehabilitation of schizophrenia was found. This suggests a gap in current CPG production process, with a relative lack of information on this topic. This seems particularly relevant in view of the recent publication of the WHO World Mental Health Report (WMHR), which urges nations and professionals to work toward empowering people to regain independence and live a life in full autonomy through the implementation of recovery-oriented interventions, most of which may be categorized as rehabilitation interventions (16).
Despite the scarcity of CPG on rehabilitation of schizophrenia, we identified general CPG that included several recommendations that are, either directly or indirectly, relevant to the assessment of rehabilitation needs and to the provision of rehabilitation interventions. To our knowledge, this is the first systematic overview of recommendations in this important field of intervention, which will be used to inform the WHO PIR and, hopefully, it may also be of interest to countries and professionals aiming to fully implement the concept of rehabilitation, in line with the WHO WMHR.
In terms of quality of available evidence, only a minority of target domains and recommendations are supported by high-quality evidence. Notably, expert opinions often supported recommendations on good clinical practice as well as on specific interventions, even in absence of a supporting background body of evidence. This applies, for example, to recommendations on physical activity, or those on the combination of individual and family interventions, or those in favor of supported employment. Despite this relatively low quality of background evidence, the strength of many of these recommendations was strong. This is in line with current standards of CPG development, as in addition to the evidence base, other considerations, such as for example values, preferences, feasibility and equity considerations should also be considered in drafting recommendations and their strength. We note, therefore, that in the field of rehabilitation there is a discrepancy between the scarcity of data on one side, and the high value attributed to rehabilitation interventions by professionals and by a variety of different stakeholders, including people with living experience of mental health conditions, on the other side. Increasing research and knowledge about this complex subject could increase clarity on what the key elements of rehabilitation in schizophrenia are. Research in this field however is hard to conduct due to long follow-up times, heterogeneous settings, complex outcomes, and lack of resources.
Looking at the total number of recommendations on specific topics (functioning domains, Table 2), some areas are not addressed adequately by available CPG, for example “Activity of daily living,” “Interpersonal interactions and relations,” “Community and social life,” and “Carer and family support.” Conversely, we included 16 recommendations addressing “symptoms of psychosis.” This disbalance is probably related to the inconsistent definition of rehabilitation in this field, and to an increased difficulty in effectively research outcomes such as “community involvement and social life” (in opposition to the reduction of psychotic symptoms).
The concept of rehabilitation is tightly related to the concept of recovery which, in the field of mental health, gained prominence after the implementation of deinstitutionalization with ever greater relevance of community services and interventions to help people achieve recovery. Recovery from a mental illness has been described as “a deeply personal, unique process of changing one's attitudes, values, feelings, goals, skills, and/or roles. It is a way of living a satisfying, hopeful, and contributing life even with limitations caused by illness. Recovery involves the development of new meaning and purpose in one's life as one grows beyond the catastrophic effects of mental illness” (13). A more recent definition has been formulated by merging the professionals' most commonly cited themes describing the meaning of the term rehabilitation which reads: “A whole system approach to recovery from mental ill health which maximizes an individual's quality of life and social inclusion by encouraging their skills, promoting independence and autonomy in order to give them hope for the future and which leads to successful community living through appropriate support” (36). Ultimately, in accordance with the WHO WMHR, if recovery from a mental disorder is the process of regaining a better mental health, rehabilitation is the body of procedures helping the individual in this process and fostering the ability to connect, function, cope and thrive (16). Further promoting a switch of paradigm from a “hospital/asylum-centric” approach to a community-centered care at a policy-making level, will stimulate the research and implementation of rehabilitation techniques focusing on recovery rather than pure reduction of symptoms (15). Still, it has to be considered that schizophrenia is a lifelong condition characterized by prodromal and residual subclinical disturbances, having implications in chronic disability (37, 38), with a 3.5%−11% per month risk of abrupt relapse to the pre-treatment condition for treatment adherent and non-adherent people in treatment for psychoses respectively (39, 40). Therefore, the long-term management and reduction of key symptoms have to be taken into account in the rehabilitation of schizophrenia as one of the factors involved in long-term recovery.
This review needs to be interpreted in the light of some limitations. First, CPG should be considered with a recognition of their inherent limitations. These recommendations are formulated based on the currently available evidence and do not encompass all potential actions required to mobilize community resources and opportunities, strengthen social cohesion and social capital, and overall integrate formal and informal care services while considering the local context. Nonetheless, the absence of these considerations does not imply that such actions should be excluded from intervention programs. All parties involved should acknowledge the importance of tailoring rehabilitation projects to accommodate individual, familial, and cultural contexts, as well as the location of service delivery, in order to ensure effective implementation. Clinicians are therefore urged to make a concerted effort to integrate evidence-based CPG with the specific needs of individuals who have experienced mental disorders. By doing so, they can provide guidance that empowers individuals to utilize resources, tools, and opportunities that align with their personal aspirations, as well as their social and clinical circumstances. A second limitation is inherent to the systematic review methodology itself, due to the potential exclusion of titles, and therefore potentially relevant information, not emerging from the literature search. In this regard, the strings used for this research were developed on the basis of the WHO indication on the systematic search of literature for the development of the PIR for all conditions. Another limitation arises from the sole inclusion of English language CPG, which was driven by feasibility considerations. We recognize that the omission of CPG in other languages could pose a significant constraint, as the outcome of the current review may predominantly reflect Western practices. Consequently, contexts in which alternative approaches, involving for example non-specialist community workers, volunteers, activists, and peers, play pivotal roles may not have received sufficient visibility.
In conclusion, six CPG based on available evidence, relevant WHO guidelines and expert opinion will inform the development of the WHO PIR for schizophrenia and related psychosis. This review revealed an imbalance in the domains addressed and a lack of indications in poor-resource settings. Priority targets and interventions in the rehabilitation in schizophrenia are still unclear in terms of significance and feasibility.
The scientific community is called to embrace the challenge posed by the WHO WMHR 2022 (16). To promote a more thorough and holistic approach to rehabilitation in this field, it will be important to research on and implement pragmatic solutions in somewhat neglected areas of the rehabilitation of schizophrenia such as “Community and social life.” Within the WMHR logic, supporting people in accessing health and social services, such as psychosocial rehabilitation, housing, or welfare benefits, are all crucial aspects of care. All these actions ought to be carried out with the intention of fostering community involvement, engagement, and legal ability. The WHO PIR will help face this important challenge in the field of schizophrenia.
Conceptualization: RS, YE, CB, and LT. Methodology: YE, MR, CB, and LT. Software: RS and YE. Formal analysis: RS. Investigation: RS, YE, and MR. Resources: CB and LT. Data curation: RS, YE, MR, and LT. Writing—original draft preparation: RS and LT. Writing—review and editing: CB, YE, and MR. Project administration: YE, CB, and LT. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
YE and MR work for the World Health Organization (WHO) in Head Quarters, Geneva. They alone are responsible for the views expressed in this publication and they do not necessarily represent the views, decisions or policies of WHO.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1215617/full#supplementary-material
1. World Health Organization. Universal Health Coverage (UHC). (2019). Available online at: https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc) (accessed May 1, 2023).
2. World Health Organization. Rehabilitation 2030: A Call for Action 2019. Available online at: https://www.who.int/initiatives/rehabilitation-2030 (accessed May 1, 2023).
3. Rauch A, Negrini S, Cieza A. Toward strengthening rehabilitation in health systems: methods used to develop a WHO package of rehabilitation interventions. Arch Phys Med Rehabil. (2019) 100:2205–11. doi: 10.1016/j.apmr.2019.06.002
4. Saha S, Chant D, Welham J, McGrath J. A systematic review of the prevalence of schizophrenia. PLoS Med. (2005) 2:e141. doi: 10.1371/journal.pmed.0020141
5. (IHME), iohMaE,. Global Helath Data Exchange (GHDx) 2022. Available online at: http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2019-permalink/27a7644e8ad28e739382d31e77589dd7 (accessed May 1, 2023).
6. Charlson FJ, Ferrari AJ, Santomauro DF, Diminic S, Stockings E, Scott JG, et al. Global epidemiology and burden of schizophrenia: findings from the global burden of disease study 2016. Schizophr Bull. (2018) 44:1195–203. doi: 10.1093/schbul/sby058
7. Gerlinger G, Hauser M, De Hert M, Lacluyse K, Wampers M, Correll CU. Personal stigma in schizophrenia spectrum disorders: a systematic review of prevalence rates, correlates, impact and interventions. World Psychiatry. (2013) 12:155–64. doi: 10.1002/wps.20040
8. Lysaker PH, Davis LW, Warman DM, Strasburger A, Beattie N. Stigma, social function and symptoms in schizophrenia and schizoaffective disorder: associations across 6 months. Psychiatry Res. (2007) 149:89–95. doi: 10.1016/j.psychres.2006.03.007
9. Wigand ME, Orzechowski M, Nowak M, Becker T, Steger F. Schizophrenia, human rights and access to health care: a systematic search and review of judgements by the European Court of Human Rights. Int J Soc Psychiatry. (2021) 67:168–74. doi: 10.1177/0020764020942797
10. Bushe CJ, Taylor M, Haukka J. Mortality in schizophrenia: a measurable clinical endpoint. J Psychopharmacol. (2010) 24:17–25. doi: 10.1177/1359786810382468
11. Laursen TM, Nordentoft M, Mortensen PB. Excess early mortality in schizophrenia. Annu Rev Clin Psychol. (2014) 10:425–48. doi: 10.1146/annurev-clinpsy-032813-153657
12. Jaaskelainen E, Juola P, Hirvonen N, McGrath JJ, Saha S, Isohanni M, et al. A systematic review and meta-analysis of recovery in schizophrenia. Schizophr Bull. (2013) 39:1296–306. doi: 10.1093/schbul/sbs130
13. Anthony WA. Recovery from mental illness: the guiding vision of the mental health service system in the 1990s. Psychosoc Rehabil J. (1993) 16:11. doi: 10.1037/h0095655
14. Saraceno B, Caldas de Almeida JM. An outstanding message of hope: the WHO World Mental Health Report 2022. Epidemiol Psychiatr Sci. (2022) 31:e53. doi: 10.1017/S2045796022000373
15. Barbui C. The WHO World Mental Health Report 2022: a new standard of care is emerging. Mol Psychiatry. (2022) 28:4–5. doi: 10.1038/s41380-022-01788-0
16. World Health Organization. World Mental Health Report: Transforming Mental Health for All. Geneva: WHO. Licence: CC BY-NC-SA 3.0 IGO (2022).
17. World Health Organization. Rehabilitation 2021. Available online at: https://www.who.int/news-room/fact-sheets/detail/rehabilitation (accessed May 1, 2023).
18. World Health Organization. Psychosocial rehabilitation: a consensus statement. Int J Mental Health. (1997) 26:77–85 doi: 10.1080/00207411.1997.11449403
19. Farkas M, Anthony W, Montenegro R, Gayvoronskaya E. Person-centered psychiatric rehabilitation. In:Mezzich JE, Botbol M, Christodoulou GN, Cloninger CR, Salloum IM, , editors. Person Centered Psychiatry. Berlin: Springer (2017), p. 277–89. doi: 10.1007/978-3-319-39724-5_21
20. Morin L, Franck N. Rehabilitation interventions to promote recovery from schizophrenia: a systematic review. Front Psychiatry. (2017) 8:100. doi: 10.3389/fpsyt.2017.00100
21. Jablensky A, Sartorius N, Ernberg G, Anker M, Korten A, Cooper JE, et al. Schizophrenia: manifestations, incidence and course in different cultures. A World Health Organization ten-country study. Psychol Med Monogr Suppl. (1992) 20:1–97. doi: 10.1017/S0264180100000904
22. Hopper K, Wanderling J. Revisiting the developed versus developing country distinction in course and outcome in schizophrenia: results from ISoS, the WHO collaborative followup project. International Study of Schizophrenia. Schizophr Bull. (2000) 26:835–46. doi: 10.1093/oxfordjournals.schbul.a033498
23. Brooke-Sumner C, Petersen I, Asher L, Mall S, Egbe CO, Lund C. Systematic review of feasibility and acceptability of psychosocial interventions for schizophrenia in low and middle income countries. BMC Psychiatry. (2015) 15:19. doi: 10.1186/s12888-015-0400-6
24. Asher L, Patel V, De Silva MJ. Community-based psychosocial interventions for people with schizophrenia in low and middle-income countries: systematic review and meta-analysis. BMC Psychiatry. (2017) 17:355. doi: 10.1186/s12888-017-1516-7
25. consortium, ANs,. The AGREE II instrument [Electionic version] 2017. Available online at: www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf (accessed May 1, 2023).
26. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
27. Stubbs B, Vancampfort D, Hallgren M, Firth J, Veronese N, Solmi M, et al. EPA guidance on physical activity as a treatment for severe mental illness: a meta-review of the evidence and Position Statement from the European Psychiatric Association (EPA), supported by the International Organization of Physical Therapists in Mental Health (IOPTMH). Eur Psychiatry. (2018) 54:124–44. doi: 10.1016/j.eurpsy.2018.07.004
28. Schmidt SJ, Schultze-Lutter F, Schimmelmann BG, Maric NP, Salokangas RK, Riecher-Rossler A, et al. EPA guidance on the early intervention in clinical high risk states of psychoses. Eur Psychiatry. (2015) 30:388–404. doi: 10.1016/j.eurpsy.2015.01.013
29. Galletly C, Castle D, Dark F, Humberstone V, Jablensky A, Killackey E, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders. Aust N Z J Psychiatry. (2016) 50:410–72. doi: 10.1177/0004867416641195
30. Hasan A, Falkai P, Lehmann I, Janssen B, Wobrock T, Zielasek J, et al. [Revised S3 guidelines on schizophrenia: developmental process and selected recommendations]. Nervenarzt. (2020) 91:26–33. doi: 10.1007/s00115-019-00813-y
31. Keepers GA, Fochtmann LJ, Anzia JM, Benjamin S, Lyness JM, Mojtabai R, et al. The American Psychiatric Association practice guideline for the treatment of patients with schizophrenia. Am J Psychiatry. (2020) 177:868–72. doi: 10.1176/appi.ajp.2020.177901
32. Ali K, Fassnacht DB, Farrer L, Rieger E, Feldhege J, Moessner M, et al. What prevents young adults from seeking help? Barriers toward help-seeking for eating disorder symptomatology. Int J Eat Disord. (2020) 53:894–906. doi: 10.1002/eat.23266
33. National Collaborating Centre for Mental Health (UK). Psychosis and Schizophrenia in Children and Young People: Recognition and Management. Leicester: British Psychological Society (2013). Available online at: https://www.nice.org.uk/guidance/cg155
34. National Collaborating Centre for Mental Health (UK). Psychosis and Schizophrenia in Adults: Treatment and Management: Updated Edition 2014. London: National Institute for Health and Care Excellence (2014). Available online at: https://www.nice.org.uk/guidance/cg178
35. National Collaborating Centre for Mental Health (UK). Rehabilitation for Adults with Complex Psychosis. London: National Institute for Health and Care Excellence (2020). Available online at: https://www.nice.org.uk/guidance/ng181
36. Killaspy H, Harden C, Holloway F, King M. What do mental health rehabilitation services do and what are they for? A national survey in England. J Mental Health. (2005) 14:157–65. doi: 10.1080/09638230500060144
37. Harvey PD, Strassnig M. Predicting the severity of everyday functional disability in people with schizophrenia: cognitive deficits, functional capacity, symptoms, and health status. World Psychiatry. (2012) 11:73–9. doi: 10.1016/j.wpsyc.2012.05.004
38. Schultze-Lutter F. Subjective symptoms of schizophrenia in research and the clinic: the basic symptom concept. Schizophr Bull. (2009) 35:5–8. doi: 10.1093/schbul/sbn139
39. Csernansky JG, Schuchart EK. Relapse and rehospitalisation rates in patients with schizophrenia: effects of second generation antipsychotics. CNS Drugs. (2002) 16:473–84. doi: 10.2165/00023210-200216070-00004
Keywords: schizophrenia, psychosis, rehabilitation, systematic review, World Health Organization (WHO)
Citation: Serra R, Etemadi Y, van Regteren Altena M, Barbui C and Tarsitani L (2023) A systematic review of Clinical Practice Guidelines for the development of the WHO's Package of Interventions for Rehabilitation: focus on schizophrenia. Front. Public Health 11:1215617. doi: 10.3389/fpubh.2023.1215617
Received: 02 May 2023; Accepted: 28 July 2023;
Published: 15 August 2023.
Edited by:
Ellie Brown, The University of Melbourne, AustraliaReviewed by:
Irene Bighelli, Technical University of Munich, GermanyCopyright © 2023 Serra, Etemadi, van Regteren Altena, Barbui and Tarsitani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Riccardo Serra, cmljY2FyZG8uc2VycmFAdW5pcm9tYTEuaXQ=
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.