
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 07 July 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1192155
This article is part of the Research TopicThe Role of Media and Communications in Vaccine Hesitancy during the COVID-19 PandemicView all 4 articles
 Celso Machado Júnior1,2*
Celso Machado Júnior1,2* Daielly Melina Nassif Mantovani3
Daielly Melina Nassif Mantovani3 Luísa Veras de Sandes-Guimarães1Maria do Carmo Romeiro1Cristiane Jaciara Furlaneto1,2
Luísa Veras de Sandes-Guimarães1Maria do Carmo Romeiro1Cristiane Jaciara Furlaneto1,2 Roberto Bazanini2
Roberto Bazanini2Background: Vaccine hesitancy is a phenomenon that can interfere with the expansion of vaccination coverage and is positioned as one of the top 10 global health threats. Previous studies have explored factors that affect vaccine hesitancy, how it behaves in different locations, and the profile of individuals in which it is most present. However, few studies have analyzed the volatility of vaccine hesitancy.
Objective: Identify the volatility of vaccine hesitancy manifested in social media.
Methods: Twitter’s academic application programming interface was used to retrieve all tweets in Brazilian Portuguese mentioning the COVID-19 vaccine in 3 months (October 2020, June 2021, and October 2021), retrieving 1,048,576 tweets. A sentiment analysis was performed using the Orange software with the lexicon Multilingual sentiment in Portuguese.
Results: The feelings associated with vaccine hesitancy were volatile within 1 month, as well as throughout the vaccination process, being positioned as a resilient phenomenon. The themes that nurture vaccine hesitancy change dynamically and swiftly and are often associated with other topics that are also affecting society.
Conclusion: People that manifest the vaccine hesitancy present arguments that vary in a short period of time, what demand that government strategies to mitigate vaccine hesitancy effects be agile and counteract the expressed fear, by presenting scientific arguments.
Vaccine hesitancy (VH) is a global phenomenon that has a major impact on population health. According to the World Health Organization (WHO), it is among the top 10 threats to global health. (1–3). The establishment of the strategic advisory group of experts (SAGE) by the World Health Organization (WHO) in 2012 was the first effort to understand, monitor, and find solutions for VH (3). Since its establishment, there has been increased interest in research related to VH (4–6), with the number of papers addressing ‘vaccine’ or ‘vaccination’ in the title increasing from 3.3% in 2019 to 8.3% in 2021 (4).
The term vaccine hesitancy is still under development and is subject to controversy. The initial proposal from the World Health Organization (WHO) indicates VH as a behavioral phenomenon, where individuals neither accept nor completely reject the possibility of vaccination (7, 8). The divergence that is established in the definition of the term VH lies in the understanding that it is not a social behavior, but rather “a state of indecisiveness regarding the decision to become vaccinated” (3), a position shared by other researchers (9).
Vaccine hesitancy is a global phenomenon. Still, public acceptance of the vaccine varies depending on the region (10). Countries in Asia have higher rates of vaccine acceptance (Malaysia with an acceptance of 94.3%, Indonesia of 93.3%, and China of 91.3%) compared to Europe (France with an acceptance of 58.9%, Poland of 56.3%, and Italy of 53.7%) and the United States (acceptance of 56.9%), which have lower levels of vaccine acceptance (11).
VH is positioned as a complex and dynamic social phenomenon, for which the influencing factors are still being researched (9, 11). Sex, educational level, age, geographical location, income, professional occupation, race and ethnicity (12), living with five or more people (13), pregnancy (14), being a health professional, and having previous vaccination experience (15) are among the factors that influence VH. Research studies establish other factors, such as group and individual aspects that involve a lower understanding of the risk, lower fear of contamination, believing that the disease is not serious, and not having heart diseases, as influencing factors of VH (16). The concepts of cognition or affection, behavior, and decision making have also been related to VH (3), which is also identified as linked to government credibility, incorporating aspects related to wanting more data for decision making, doubts about vaccine efficacy and safety, feeling that personal rights are being infringed upon, and lack of trust in the government and health care institutions (14, 15).
The factors influencing VH are proposed from two constructs: the HBM (12) and the 7C (17). The HBM construct examines the influence of perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy on VH (18), which are mostly conditional on the prevalence of demographic, psychosocial, and structural variables (12). While the 7C construct points to trust, complacency, convenience (or constraints), risk calculation, collective responsibility, compliance, and conspiracy as factors driving VH (9, 17, 19).
The VH in Brazil is a phenomenon that originated before the COVID-19 pandemic and evolved from 2016 (20). It is possible to identify this decline in vaccination coverage in the analysis of mandatory vaccination for Human Papillomavirus (HPV) among girls aged 9 to 14 years, which showed a vaccination coverage rate of 83.4% for the first dose and only 55 0.6% in the second dose. For the general Brazilian vaccination system in 2021, the coverage rate considering all vaccines made available by the public network was 59% of citizens (21). In Brazil, there are studies that show significant variability of information about the population’s VH. Among the studies that analyzed VH in Brazil, one stands out, which consolidates the analysis of eleven other studies on the subject, in which a variation from 8.2 to 34% of vaccine hesitancy for COVID-19 was found (22), the consolidation of these studies, indicated an average vaccine hesitancy of 11.1%. A justification for the discrepancy identified in these studies is based on the large territorial extension of the country, with locations that present different behaviors in relation to the general average of the country. In this sense, research carried out in the Brazilian state of Maranhão identified a rate of hesitation to vaccinate against the SARS-CoV-2 virus of 17.5% (23), which is higher in comparison with an average of 11.1% (22).
Overall, previous studies have addressed the factors influencing VH and its variation across locations. However, it is unclear whether VH is subject to the volatility of people’s decision to take the vaccine, as public sentiment is volatile (24), or if the influence of digital media platforms on the decision to take the vaccine (25). Therefore, the objective of this study was to identify the variability of vaccine hesitancy manifested in social media. Overall, based on the papers reviewed, this is one of the first studies to explore the volatility of VH using social media as a data source, a context that meets the view that public sentiment tends to be volatile toward VH (24). It is also worth noting, the existence of studies that, relying on Twitter databases, have analyzed people’s sentiment toward COVID-19 (26–28) and toward the COVID-19 vaccine (29–31).
A dataset was obtained from Twitter’s Application Programming Interface (API). The data search was divided into three periods delimited by the months of October 2020, June 2021, and October 2021, and encompassed Brazilian data. The months of data collection were defined to identify different moments of the vaccination process for COVID-19. Additionally, each month’s data was divided into one-week periods, with October 2020 and June 2021 having five analysis periods, and October 2021 having four. The keywords used to search the tweets were “COVID-19,” “vaccine” and “vaccination” in Brazilian Portuguese. This data collection technique has been observed in similar studies (26, 27, 31–33). Opted to use Brazilian Portuguese, as the research is being carried out by a group of Brazilian researchers, who seek to identify mechanisms for predicting future pandemics. The capture of the text, only in Brazilian Portuguese, excluding tweets generated in Portuguese from other countries, as well as the use only of tweets generated from the Brazilian territory, was possible using the knowledge-based model, which captures a wide variety of locative references from tweets, like proposed by Martínez and Pascual (34). It is worth mentioning, that the authors of this article make a collaborative effort to expand knowledge on the subject, approaching productive research groups that address the theme of vaccine hesitancy and coping with COVID-19 (35–40). Thus, the findings of this research make up a contribution to the mosaic of international studies that address VH, however, caveats must be taken when generalizing their findings, because they are characteristic of the Brazilian population.
The exported data had issues with character encoding (accents and other special formats) and provided a date formatting presented as year, day, month, hour (including minutes and seconds) that is different from the Brazilian standards. To correct these issues, it was necessary to use the R software to help edit the data, since the database had over 1 million observations. During data extraction, were removed all duplicate tweets and the same tweet from the same user. After this step, the data were exported from R as a.csv file, generating one file per month analyzed. It is worth mentioning, that in this study, there are no independent or dependent variables, since the paper focused on text sentiment analysis.
The.csv data was imported into the Orange Data Mining software to conduct the sentiment analysis, an unsupervised text mining technique (without an initial reference/classification as the initial input into the software) that aims to extract the emotion present in a message.
In the Orange software, the text corpus was pre-processed to remove stop words (prepositions, pronouns, etc.). Only whole words without numbers or other characters (Regexp) are maintained. Specific features of the Twitter language (for example, the use of hashtag and at signs) are identified and URLs removed from the text.
The sentiment analysis was performed with the help of the software Orange, in which a sentiment analysis was initially performed with the Multilingual sentiment lexicon in Brazilian Portuguese, which contains a previous mapping of words categorized as positive and negative. It is noteworthy, that the research addresses the feelings of the Brazilian population, so the generalization of its findings must be carried out with reservations. In this method, each word is categorized as negative, positive, or neutral and the overall sentiment score of the text is calculated (positive words-negative words/total words). Each tweet was assigned a score for sentiment that ranged from −1 to 1, where a classification above 0 = positive, below 0 = negative, and equal to 0 = neutral. Since the article is specifically focused on vaccine hesitancy, the analysis presented below involved the manual selection of a few tweets that showed adherence to the topic, according to the definitions presented in the literature. Due to the size (over 1 million tweets) and subject of the database, it would be impossible to perform this analysis automatically, using only the tweets related to vaccine hesitancy. The approach adopted presents similarities with studies on this subject (29, 30, 41, 42).
The sentiment analysis of the VH was performed in three different periods of the vaccination process, which are presented in charts divided into 1-week periods. This distribution was planned to observe the sentiment of VH in short periods (week) within the same month, and in longer intervals (over 4 months). The analysis relied on the selection of 1.047.018 tweets adhering to the topic of vaccine hesitancy. However, the overall sentiment of the analyzed tweets for October 2020 was −0.0438, for June 2021 was −0.0510, and for October 2021 was −0.0519. The overall sentiment was therefore slightly negative in all periods.
In October 2020, the availability of a vaccine for COVID-19 was identified in the Brazilian media. Three vaccine possibilities were discussed, those offered by Pfizer/Biontech, Oxford/AstraZeneca, and Sinovac/Butantan (CoronaVac). Subsequently other possible vaccines to be purchased by Brazil were identified. However, only these three vaccines were employed in greater volume. The sentiment analysis was developed initially by the researchers’ perspective (presented in the sentiment analysis performed) and then by the score provided by the Orange Software (sentiment score column). The purpose of this double analysis was to identify the alignment of the researchers’ perception with that obtained later in the analysis developed in the Orange software. From this perspective, some differences in positioning were identified between the analyses, however, without contrasts (variation between negative and positive, as the divergences were centered on the neutral sentiment). For this research, each divergence was analyzed individually, and used to deepen the understanding of the data and broaden the discussion. Table 1 presents the sentiment analysis for October 2020. It is noteworthy that the sentiment analysis is focused on VH and not on other aspects pointed out in the tweets. The sentences that exemplify the sentiment identified and presented in the first columns of the tables were translated from Portuguese to English to present the research by the authors.
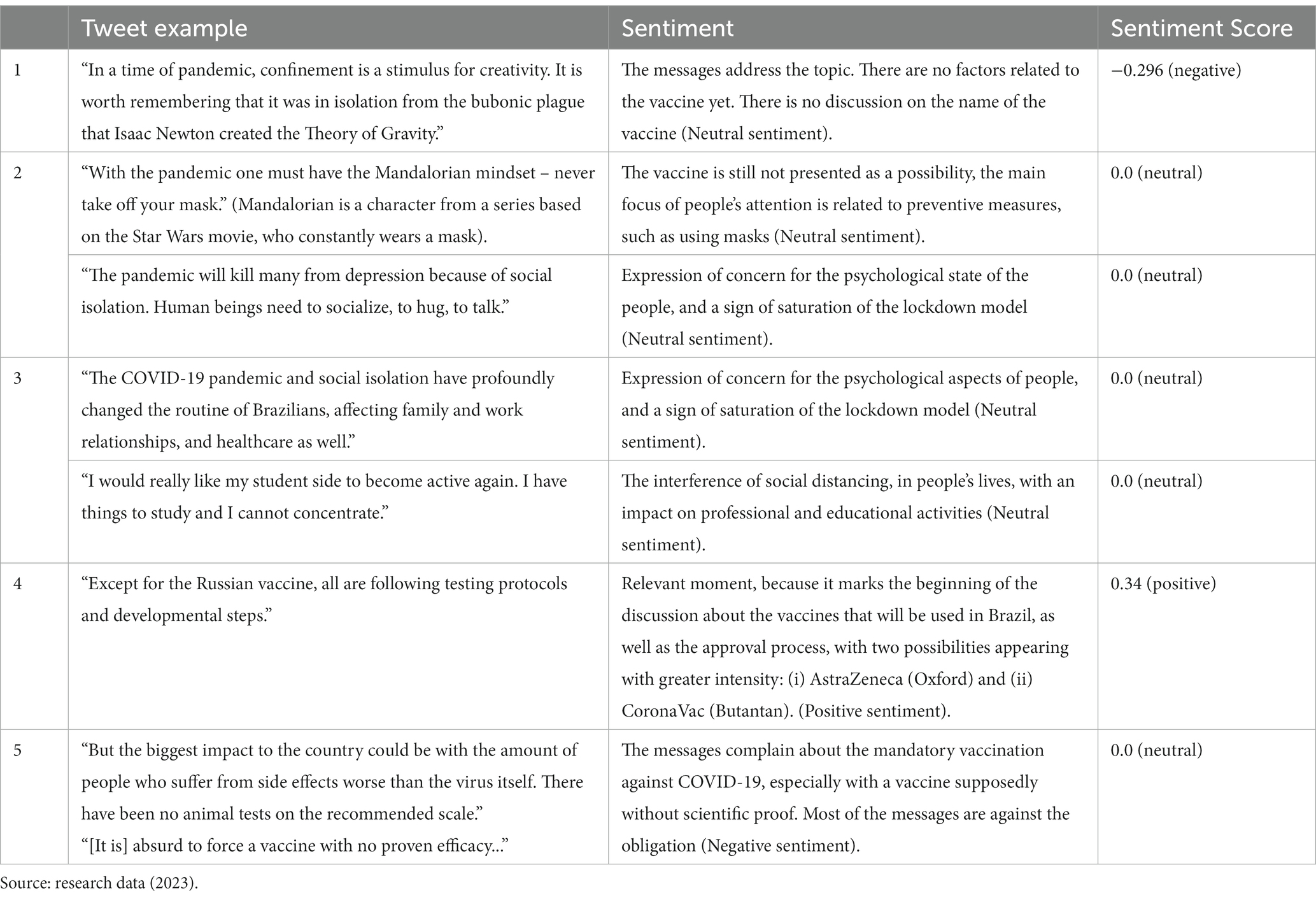
Table 1. Sentiment analysis of the COVID-19 vaccine in October 2020.
The data show the onset of vaccine topic within the spectrum of solutions for the COVID-19 pandemic in Brazil. In the first insertion the VH phenomenon is already observed, focusing on the efficacy of the vaccines that are being proposed. The data show an alternation between negative, neutral, and positive sentiments; however, with a prevailing neutral positioning.
According to the Brazilian government priority planning, COVID-19 vaccines began to be delivered in January 2021 through prioritizing health care workers and the older adults. By June 2021, most of the population identified as priority population had already received the first dose of the COVID-19 vaccine. Thus, the vaccination process was already within reach of the population, however, still following the planned schedule of making the vaccine available in an order of decreasing age. Table 2 presents the sentiment analysis in June 2021.
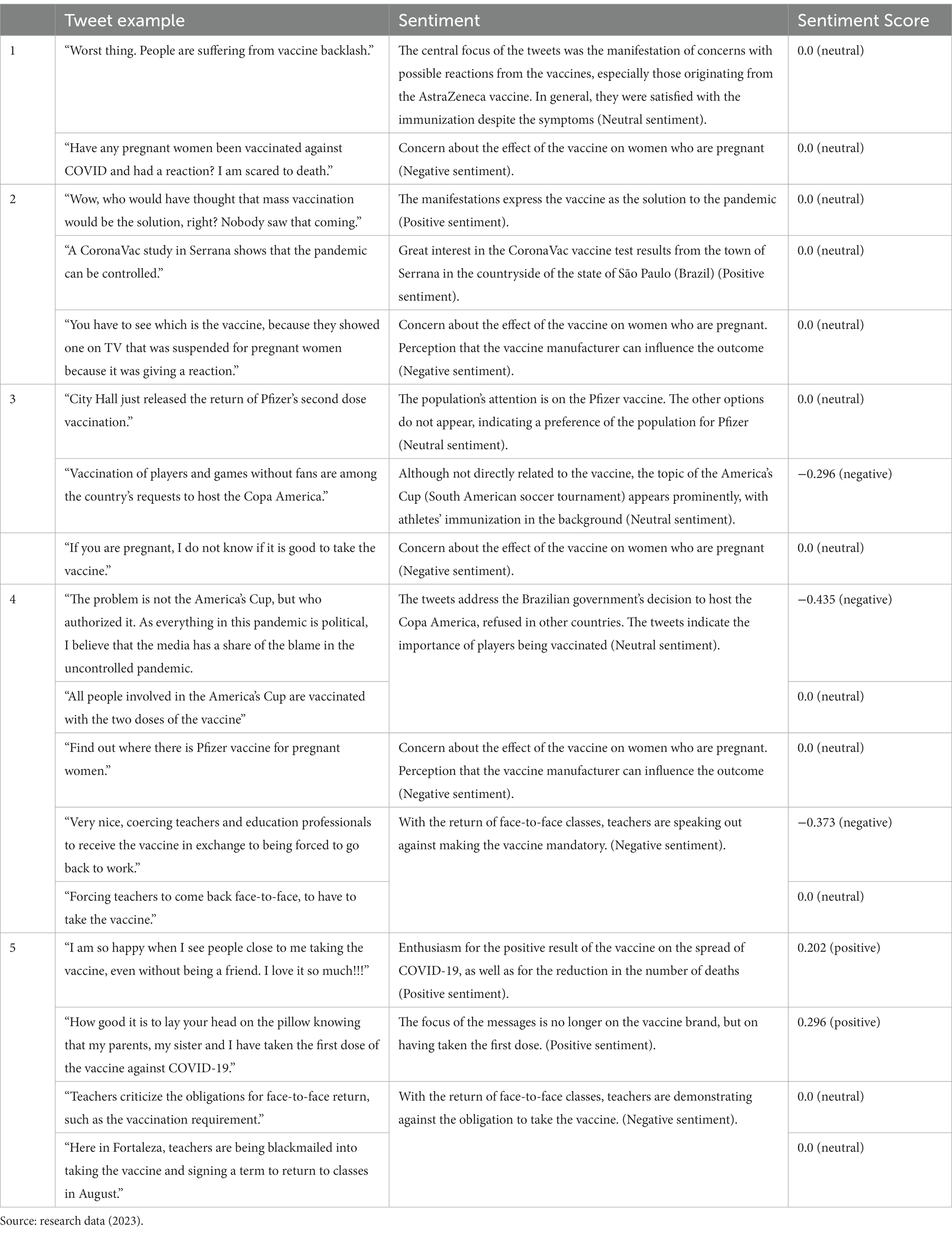
Table 2. Sentiment analysis of the COVID-19 vaccine in June 2021.
The data reflect an intense period of the vaccination process, with most of the tweets addressing this topic. The sentiment expressed is positive and adherent to the vaccination process promoted by the Brazilian government. The tweets present three interesting features and approaches, despite dealing with a common trend, which are: (i) the positive result of the CoronaVac vaccine (Sinovac/Butantan) tests carried out in the city of Serrana is expressed as a positive sentiment; (ii) despite the positive result of the CoronaVac vaccine, the population preferred the Pfizer/Biontech vaccine; (iii) people are satisfied for having taken the first dose of the COVID-19 vaccine and being close to taking the second dose. These analyzed aspects are intertwined in the understanding of the benefits resulting from taking the vaccine. However, two specific groups with VH are identified, the pregnant women and the teachers in the education network. The hesitation of pregnant women permeates the concern of the vaccines affecting the pregnancy or the fetus. In this context, there are discussions as to which vaccine is the safest. In the case of teachers, it is worth noting that classes were paralyzed in Brazil in March 2020, when classroom activities were expected to return in August 2021, causing concern among teachers. In this approach, it is possible to have a double interpretation of the data. The first one is related to the VH, while the second is related to the hesitation of returning to the classroom, regardless of having taken the vaccine. However, under both terms the vaccine is positioned as an element of argumentation for the hesitation expressed by the teachers. Table 3 presents the sentiment analysis for October 2021.
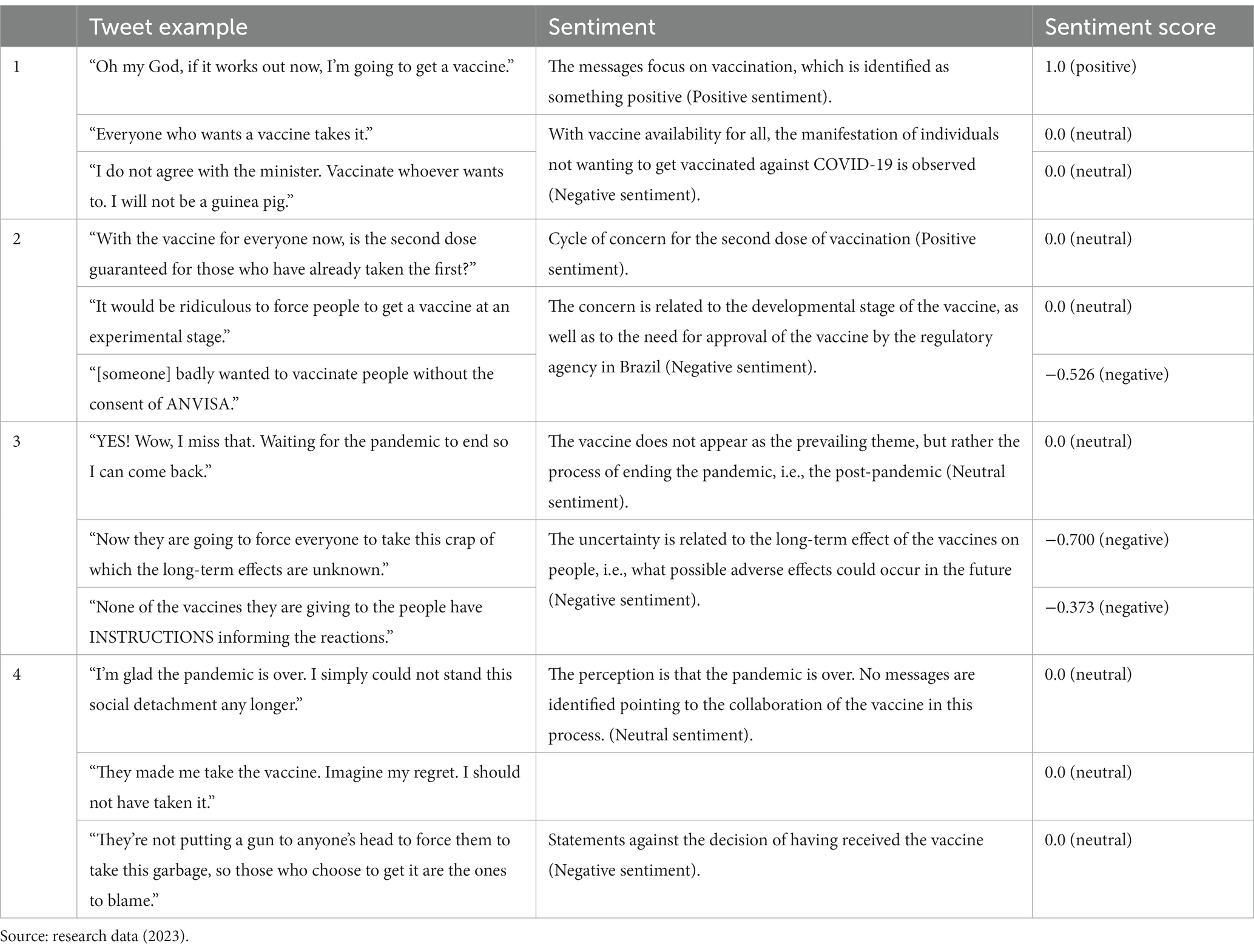
Table 3. Sentiment analysis of the COVID-19 vaccine in October 2021.
The data for October 2021 portray a period of a more advanced stage of the population vaccination process. This period showed a greater VH manifestation, probably due to the availability of the vaccine for everyone, encouraging those who are more resistant to the vaccine to manifest with greater intensity. The data show an alternation between negative and neutral sentiments, with little occurrence of positive sentiments. This indicates that almost a year after the beginning of the vaccination process VH still exists, consisting of a resilient phenomenon that, therefore, should be the object of planning and actions aimed at its mitigation. The tweets also indicate the expectation for the end of the COVID-19 pandemic. In this perspective, the vaccination process, added to other factors such as the reduction of infection, reduction of deaths, desire to return to normal activities, with the potential interaction among these factors, have set an important milestone for people to interpret the period as the end of the pandemic. It is worth mentioning, that these characteristics observed in the tweets, as well as the brands of vaccines available, the period and priority of vaccination of the population, are related to characteristics of the vaccination process in Brazil, thus presenting intrinsic limitations of generalization of the findings of this research.
Previous studies have revealed that vaccine hesitancy (VH) is a dynamic phenomenon influenced by many variables that impact it in a positive or negative way (9, 11). The variables that influence VH operate differently in each region depending on characteristics of the society (10, 11). Residents of sub-Saharan Africa, for example, feared being victims of vaccine experimentation (43).
Vaccine hesitancy research studies show variations in vaccine acceptance rates for COVID-19 (10, 11, 44). Note that VH is not a behavior, but rather a state of indecision (3, 9), thus subject to temporal factors (45) and changes resulting from the dissatisfaction or satisfaction of society concerning access to information and actions of the government (44). The identification of factors that collaborate with or mitigate VH stand out for enabling the expansion of vaccination coverage, and thus facilitating the achievement of the theoretical 90% or higher rate needed to establish collective immunity (46).
The first set of data analyzed shows the period before the vaccination process began (October 2020). The data indicate that this period was characterized by an initial phase of indifference to vaccine-related aspects and greater attention to the protocols adopted by society. At the end of this period, the manifestations of feelings related to the vaccine, both positive and negative, can be observed. Since it is a new vaccine, the reservations are related to the adverse effects resulting from its use and to its efficacy. The identified resistance occurs in the context of a new product, for which little is known concerning efficiency and potential adverse effects (11, 15, 16, 47). These initial manifestations express concerns with the source of the vaccine, i.e., with which laboratory is developing it, highlighting the need for the government to establish partnerships with research and production laboratories to provide as much information as possible. Subsequent evidence showed that some vaccines were imperfect or even had a declining protection index, thus favoring new COVID-19 outbreaks (48). In Brazil some politicians assured that the vaccine made contamination impossible, which increased VH when the first cases of contamination by COVID-19 of vaccinated people surfaced. From this perspective, the lack of trust in the government increased VH (1, 10, 14, 15, 25, 49). The inappropriate manifestation of politicians regarding the vaccine strengthens VH, impacting trust in the government and in the COVID-19 vaccine. This suggests that politicians should base their communications on evidence provided by the experts and not on their own feelings about vaccination.
The second block of data analyzed concerns the month of June 2021, which is marked by a significant portion of the Brazilian population having already received at least the first dose of the vaccine. Meanwhile, VH was expressed as negative sentiments toward the vaccine. In this interval, three phenomena associated with the VH in relation to the COVID-19 vaccine stood out: pregnant women, the Copa América being held in Brazil (soccer championship between the national teams of South American countries), and the return to school.
The suitability of the COVID-19 vaccine for pregnant women was a dominant theme throughout the period. VH was expressed in questioning the suitability of vaccines in general as well as the suitability of one of the vaccines available (50). However, in both VH motivations, it is possible to ponder that doubting the suitability of the vaccine for pregnant women may cause this negative sentiment toward the vaccine to overflow to the society.
Another aspect that pervaded the tweets in the analyzed period was the Copa América being held in Brazil. In this case, a negative aspect regarding the event was observed, as the risks and appropriateness of holding the tournament were questioned. From this perspective, the manifestation of HV was not identified. On the contrary, a concern for the vaccination of the tournament players was observed. Thus, the calculation of contamination risk and collective responsibility acted as elements of positive reinforcement for vaccination (17, 51). Additionally, the attention given to sport-related activities during a pandemic outbreak can positively influence social connections and relieve psychological stress (52).
Another interesting aspect observed in this period involves primary and secondary school teachers. Some teachers interpreted the need to get vaccinated as a coercion to return to classroom activities in schools. From this perspective, VH is not explicitly perceived. However, the teachers’ fear of returning to the classroom heightened VH in general. We can thus infer that their professional activity is influencing the vaccination process (12, 15), and causing the feeling that their personal rights are being infringed upon (15). In Brazil, primary and secondary education is largely the responsibility of municipal and state governments, which halted school classes in 2020. In turn, studies indicate that students in schools, with greater confidence in the management of the pandemic, tend to be more willing to be vaccinated (53). This block of analysis (June 2021) shows the possibility of observing multiple social factors interfering with VH at short time intervals (1 month).
This period is also a turning point as the pandemic is concerned, namely the proximity of the end of the crisis. At the end of June 2021, the beginning of manifestations alluding to the approach of the end of the COVID-19 pandemic are identified, and most of them relate this event to the COVID-19 vaccination process, i.e., there is a positive feeling toward vaccination and its influence on the end of the crisis.
The third block of analyzed data includes tweets from October 2021. In this period a significant portion of the population had already been vaccinated, and in many cases including the second dose. Given the advanced stage of vaccination, the COVID-19 vaccine was already available to the entire population. Until then, vaccination followed a decreasing schedule in relation to people’s age, so the older adults had priority. In this perspective, we have the VH manifestations resulting from vaccine availability (14). Such availability caused those who were hesitant to manifest their opinion with greater intensity. Despite the existence of COVID-19 variants circulating in Brazil, we did not encounter any manifestation of VH related to this issue (48).
An interesting fact is that the increased occurrence of HIV manifestations in the period when vaccination is completed may be associated with the occurrence of reinfection and shorter duration of the immunity provided by the vaccine, which contradicts the initial information provided by politicians to the population (54). Other plausible explanations for this increase are the prohibition of access of those who did not get the vaccine to certain public places and the political discussion of establishing a mandatory vaccination “passport” for the population. These actions highlight the association of VH with government policies (1, 14, 15, 24), with the efficiency and potential adverse effects of the vaccine (11, 14, 15, 47), and, in many cases, with the short time of vaccine development (16). In this period, one can also observe the manifestation of regret for having taken the vaccine. This characteristic establishes an important point of future investigation, as it constitutes a new attitude of people that differs from hesitation before the fact – the “vaccine regret” (VR). The VR can affect the VH and drive people to avoid getting booster doses.
It is worth mentioning, that no studies were identified in the literature that presented the concept of VR. Thus, this study establishes a new perspective to be analyzed in future studies. However, when performing a search in the literature, the term “anticipated regret” was identified (55, 56). Anticipated regret is related to the feeling that we may regret a decision in the future, and in this condition, it’s can potentially be used as a predictor of vaccine behavior (57).
Typically, studies of anticipated regret are related to anticipated regret in decisions to vaccinate against Human Papillomavirus (HPV) (58, 59) and address the antagonism between the daughter’s anticipated regret of becoming more sexually active after vaccination and regret by inaction if the daughter develops an HPV infection if she is not vaccinated (60). However, this concept was also used in a study of vaccination against influenza (61) and COVID-19 (58).
The joint analysis of the three researched periods made it possible to identify that the VH manifests itself continuously and in association with themes that are affecting society, thus characterizing it as a social and dynamic phenomenon (9, 10). In manifestations expressed in the social media, the VH was associated with vaccine manufacturers and related to the public sentiment (9, 24). Thus, social media is positioned as an important channel for to manifest VH (10, 25). Therefore, it should also be a resource used by the government to disseminate information that reduces VH. The VH is volatile on social media, as it appears related to various social topics that change very quickly. Thus, the government’s action on social media to reduce VH must be agile so as not to distance itself from the topics that are being addressed. It is important to emphasize, that if the government does not quickly combat tweets that encourage vaccine hesitancy, these messages can lead to an adverse result in the vaccination process, regardless of the frequency of communication (52). This perspective validates VH as a social process under the influence of multiple meanings and logics, circumscribed to the individual and collectivity.
Agile government efforts may prevent occurrences such as the one observed in France, where a vaccine uptake level that positively fluctuated between 62.0 and 77.1% in March and April 2021 reduced to a markedly lower level of 58.9% in June 2021, likely due to concerns related to vaccine safety and efficacy (54, 62, 63). Notably, the potential positive association between trust in the government and COVID-19 vaccination involves sociopolitical factors related to public health policy implementation (64).
In vaccine hesitancy analyses, it becomes relevant to incorporate the position of healthcare workers (HCW) in the vaccination process. The inclusion of HCW in the effort to reduce VH comes from the fact that people trust these professionals and follow their guidelines (65–67). The influence of HCW guidance on reducing VH is significant (68) and proved to be important when coping with the COVID-19 pandemic. A study carried out in June 2020, with the population that presented VH for COVID-19, indicated that 51.9% presented VH even after the indication of HCW vaccination (68). The same study was carried out in June 2021, and it was identified that this value had reduced to 35.8% (68), that is, during the pandemic the population increased its confidence in health professionals, and in their recommendations for the vaccination.
The influence of the HCW, for the reduction of VH, with the population, can be compromised if these professionals also present this hesitation. There is no consensus on the dimension of VH in HCW, however two surveys stand out. The global survey, which analyzed 35 studies in the area, indicated a variation between 4.3 and 72% of VH in HCW, depending on the country in which they operated (69). Another survey, which analyzed HCW according to their training, identified an average of 8.1% of VH among HCW, with the categories with the lowest VH indices being Physicians (3.1%) and Nurses (6.5%) (68). In this perspective, it is worth noting that the HCW also have VH, however, they do not express their concerns due to institutional and social pressures (70). Thus, the unspoken vaccine hesitancy of HCW is identified as an element of attention of health systems, as it can influence the reduction of confidence in the vaccine by the public.
Two relevant aspects of the participation of HCWs in the HV mitigation process are thus identified: the first is that they influence people’s decision to take the vaccine, so this aspect should be used in favor of awareness campaigns. The second aspect indicates that HCW may have unspoken vaccine hesitancy, which requires health system managers to establish awareness programs, with this specific public, that include autonomy and freedom to express their hesitations.
The attention devoted to COVID-19 VH research should support ongoing efforts begun by the WHO in 2012 (3), aimed at defining, monitoring, and mitigating VH. The benefit of the cooling of the COVID-19 pandemic should not impact the importance of VH research, as there are other infections that spread in waves, affecting all of society. One example is the influenza virus responsible for infecting 1 billion people per year (48, 71), resulting in 290,000 to 650,000 influenza-related respiratory deaths (72).
This study defines vaccine hesitancy as a complex and dynamic social phenomenon, subject to several influencing factors. Among the considerations and findings of this research are the arguments presented by society for not getting vaccinated, which vary over short periods of time, surely within the period of a month. Thus, actions aimed at reducing vaccine hesitancy must be agile in capturing the concerns that permeate society, and in presenting information that encourages people to take the vaccine. In Brazil, vaccine hesitancy studies are still in the initial phase, so this research presents itself as a strength, for Brazilian society, which has its own cultural traits. This characteristic establishes limitations, when applying the knowledge developed in this study, in countries with cultures other than Brazilian.
The origin of the data did not allow raising variables common to other studies, such as: age, sex, education, professional occupation, race and ethnicity. In this perspective, this study presents additional information on vaccine hesitancy. Additionally, the data from this study refer to the Brazilian population, so caveats should be established in generalizing the findings of this research to other populations.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://docs.google.com/spreadsheets/d/1getfuzuxOFc_4V_TT_vm2TZHrxe3efUK/edit?usp=share_link&ouid=117126578285990502154&rtpof=true&sd=true.
Ethical review and approval were not required for the study of human participants in accordance with local legislation and institutional requirements. Data were collected from social media preserving anonymity.
CM, DM, LS-G, MR, CF, and RB were involved in the analysis and interpretation of the data. CM, DM, and LS-G did the drafting of the article. CM and LS-G performed the statistical analysis. DM, MR, CM, and RB improved the quality of the English of the manuscript. CF wrote the final version all the manuscript. All authors revisited critically the manuscript for intellectual content, approved the version to be published and agree to be responsible for all aspects of the work, and involved in the conception and design of the study.
This work was funded by a Research Incentive Scholarship offered by the University of São Paulo – USP.
We would like to thank University of São Paulo for its support.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Nuwarda, RF, Ramzan, I, Weekes, L, and Kayser, V. Vaccine hesitancy: contemporary issues and historical background. Vaccine. (2022) 10:e1595. doi: 10.3390/vaccines10101595
2. Larson, HJ. Defining and measuring vaccine hesitancy. Nat Human Behav. (2022) 6:1609–10. doi: 10.1038/s41562-022-01484-7
3. Bussink-Voorend, D, Hautvast, JL, Vandeberg, L, Visser, O, and Hulscher, ME. A systematic literature review to clarify the concept of vaccine hesitancy. Nat Hum Behav. (2022) 6:1634–48. doi: 10.1038/s41562-022-01431-6
4. Attwell, K, Hannah, A, and Leask, J. COVID-19: talk of ‘vaccine hesitancy’ lets governments off the hook. Nature. (2022) 602:574–7. doi: 10.1038/d41586-022-00495-8
5. Calac, AJ, Haupt, MR, Li, Z, and Mackey, T. Spread of COVID-19 vaccine misinformation in the ninth inning: retrospective observational infodemic study. Jmir Infodemiol. (2022) 2:e33587. doi: 10.2196/33587
6. Hartert, TV, and Ortiz, JR. Need for improved global measurement of early childhood respiratory syncytial virus disease. Lancet. (2022) 399:1993–5. doi: 10.1016/S0140-6736(22)00623-7
7. Fisher, KA, Bloomstone, SJ, Walder, J, Crawford, S, Fouayzi, H, and Mazor, KM. Attitudes toward a potential SARS-CoV-2 vaccine: a survey of U.S. adults. Ann Intern Med. (2020) 173:964–73. doi: 10.7326/M20-3569
8. World Health Organization. Report of the SAGE working group on vaccine hesitancy. (2014). Available at: (https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_!nal.pdf).
9. Wiysonge, CS, Ndwandwe, D, Ryan, J, Jaca, A, Batouré, O, Anya, BPM, et al. Vaccine hesitancy in the era of COVID-19: could lessons from the past help in divining the future? Hum Vaccin Immunother. (2022) 18:1–2. doi: 10.1080/21645515.2021.1893062
10. Karafillakis, E, Van Damme, P, Hendrickx, G, and Larson, HJ. COVID-19 in Europe: new challenges for addressing vaccine hesitancy. Lancet. (2022) 399:699–701. doi: 10.1016/S0140-6736(22)00150-7
11. Sallam, M. COVID-19 vaccine hesitancy worldwide: a concise systematic review of vaccine acceptance rates. Vaccine. (2021) 9:1–14. doi: 10.3390/vaccines9020160
12. Limbu, YB, Gautam, RK, and Pham, L. The health belief model applied to COVID-19 vaccine hesitancy: a systematic review. Vaccine. (2022) 10:1–13. doi: 10.3390/vaccines10060973
13. Fajar, JK, Sallam, M, Soegiarto, G, Sugiri, YJ, Anshory, M, Wulandari, L, et al. Global prevalence and potential influencing factors of COVID-19 vaccination hesitancy: a meta-analysis. Vaccine. (2022) 10:1–20. doi: 10.3390/vaccines10081356
14. Truong, J, Bakshi, S, Wasim, A, Ahmad, M, and Majid, U. What factors promote vaccine hesitancy or acceptance during pandemics? A systematic review and thematic analysis. Health Promot Int. (2022) 37:daab105. doi: 10.1093/heapro/daab105
15. Peterson, CJ, Lee, B, and Nugent, K. COVID-19 vaccination hesitancy among healthcare workers - a review. Vaccine. (2022) 10:1–30. doi: 10.3390/vaccines10060948
16. Aw, J, Seng, JJB, Seah, SSY, and Low, LL. COVID-19 vaccine hesitancy - a scoping review of literature in high-income countries. Vaccine. (2021) 9:1–21. doi: 10.3390/vaccines9080900
17. Geiger, M, Rees, F, Lilleholt, L, Santana, AP, Zettler, I, Wilhelm, O, et al. Measuring the 7Cs of vaccination readiness. Eur J Psychol Assess. (2022) 38:261–9. doi: 10.1027/1015-5759/a000663
18. Rosenstock, IM. Historical origins of the health belief model. Health Educ Monogr. (1974) 2:328–35. doi: 10.1177/109019817400200403
19. Betsch, C, Schmid, P, Heinemeier, D, Korn, L, Holtmann, C, and Böhm, R. Beyond confidence: development of a measure assessing the 5C psychological antecedents of vaccination. PLoS One. (2018) 13:e0208601. doi: 10.1371/journal.pone.0208601
20. Sociedade Brasileira de Imunizantes (SBIm). Especialistas se reúnem para debater o fenômeno da hesitação vacinal no Brasil. (2021). Available at: (https://sbim.org.br/noticias/1619-especialistas-se-reunem-para-debater-o-fenomeno-da-hesitacao-vacinal-no-brasil).
21. de Fortaleza, Prefeitura. I Fórum Hesitação em Vacinar alerta sobre a importância da participação da sociedade nas campanhas de imunização. (2023). Available at: https://www.fortaleza.ce.gov.br/noticias/i-forum-hesitacao-em-vacinar-alerta-sobre-a-importancia-da-participacao-da-sociedade-nas-campanhas-de-imunizacao (Accessed May 13, 2023).
22. Leite, ESF, Martins, MG, and Martins, CMDCR. Hesitação vacinal e seus fatores associados no contexto da pandemia de COVID-19 no Brasil. Cadernos Prospecção. (2023) 16:484–502. doi: 10.9771/cp.v16i2.50880
23. Oliveira, BLCAD, Campos, MAG, Queiroz, RCDS, Alves, MTSSDB, Souza, BFD, Santos, AMD, et al. Prevalência e fatores associados à hesitação vacinal contra a COVID-19 no Maranhão. Brasil Revist Saúde Pública. (2021) 55:1:12. doi: 10.11606/s1518-8787.2021055003417
24. Pertwee, E, Simas, C, and Larson, HJ. An epidemic of uncertainty: rumors, conspiracy theories and vaccine hesitancy. Nat Med. (2022) 28:456–9. doi: 10.1038/s41591-022-01728-z
25. Larson, HJ, and Murray CJ, GE. The vaccine-hesitant moment. N Engl J Med. (2022) 387:58–65. doi: 10.1056/NEJMra2106441
26. Dubey, AD. Twitter sentiment analysis during COVID-19 outbreak. (2020). Available at: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3572023
27. Priyadarshini, I, Mohanty, P, Kumar, R, Sharma, R, Puri, V, and Singh, PK. A study on the sentiments and psychology of twitter users during COVID-19 lockdown period. Multimed Tools Appl. (2022) 81:27009–31. doi: 10.1007/s11042-021-11004-w
28. Singh, C, Imam, T, Wibowo, S, and Grandhi, S. A deep learning approach for sentiment analysis of COVID-19 reviews. Appl Sci. (2022) 12:3709. doi: 10.3390/app12083709
29. Nezhad, ZB, and Deihimi, MA. Twitter sentiment analysis from Iran about COVID 19 vaccine. Diabetes Metab Syndr Clin Res Rev. (2022) 16:102367. doi: 10.1016/j.dsx.2021.102367
30. Marcec, R, and Likic, R. Using twitter for sentiment analysis towards AstraZeneca/Oxford, Pfizer/BioNTech and Moderna COVID-19 vaccines. Postgrad Med J. (2022) 98:544–50. doi: 10.1136/postgradmedj-2021-140685
31. Niu, Q, Liu, J, Kato, M, Shinohara, Y, Matsumura, N, Aoyama, T, et al. Public opinion and sentiment before and at the beginning of COVID-19 vaccinations in Japan: twitter analysis. JMIR Infodemiol. (2022) 2:e32335. doi: 10.2196/32335
32. Qorib, M, Oladunni, T, Denis, M, Ososanya, E, and Cotae, P. COVID-19 vaccine hesitancy: text mining, sentiment analysis and machine learning on COVID-19 vaccination twitter dataset. Expert Syst Appl. (2023) 212:118715. doi: 10.1016/j.eswa.2022.118715
33. Chauhan, U, and Shah, A. Topic modeling using latent Dirichlet allocation. ACM Comput Surv. (2022) 54:1–35. doi: 10.1145/3462478
34. Martínez, NJF, and Pascual, CP. Knowledge-based rules for the extraction of complex, fine-grained locative references from tweets. Revista Electron Linguist Aplicada. (2020) 19:136–63.
35. Umakanthan, S, Sahu, P, Ranade, AV, Bukelo, MM, Rao, JS, Abrahao-Machado, LF, et al. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad Med J. (2020) 96:753–8. doi: 10.1136/postgradmedj-2020-138234
36. Umakanthan, S, Patil, S, Subramaniam, N, and Sharma, R. COVID-19 vaccine hesitancy and resistance in India explored through a population-based longitudinal survey. Vaccine. (2021) 9:1064. doi: 10.3390/vaccines9101064
37. Umakanthan, S, Senthil, S, John, S, Madhavan, MK, Das, J, Patil, S, et al. The effect of statins on clinical outcome among hospitalized patients with COVID-19: a multi-centric cohort study. Front Pharmacol. (2022) 13:1–11. doi: 10.3389/fphar.2022.742273
38. Umakanthan, S, and Lawrence, S. Predictors of COVID-19 vaccine hesitancy in Germany: a cross-sectional, population-based study. Postgrad Med J. (2022) 98:756–64. doi: 10.1136/postgradmedj-2021-141365
39. Umakanthan, S, Bukelo, MM, Bukelo, MJ, Patil, S, Subramaniam, N, and Sharma, R. Social environmental predictors of COVID-19 vaccine hesitancy in India: a population-based survey. Vaccine. (2022) 10:1749. doi: 10.3390/vaccines10101749
40. Umakanthan, S, Bukelo, MM, and Gajula, SS. The commonwealth Caribbean COVID-19: regions resilient pathway during pandemic. Front Public Health. (2022) 10:844333. doi: 10.3389/fpubh.2022.844333
41. Nia, ZM, Ahmadi, A, Bragazzi, NL, Woldegerima, WA, Mellado, B, Wu, J, et al. A cross-country analysis of macroeconomic responses to COVID-19 pandemic using twitter sentiments. PLoS One. (2022) 17:e0272208. doi: 10.1371/journal.pone.0272208
42. Reshi, AA, Rustam, F, Aljedaani, W, Shafi, S, Alhossan, A, Alrabiah, Z, et al. COVID-19 vaccination-related sentiments analysis: a case study using worldwide twitter dataset. Healthcare. (2022) 10:411. doi: 10.3390/healthcare10030411
43. Anjorin, AA, Odetokun, IA, Abioye, AI, Elnadi, H, Umoren, MV, Damaris, BF, et al. Will Africans take COVID-19 vaccination? PLoS One. (2021) 16:e0260575. doi: 10.1371/journal.pone.0260575
44. Kanyanda, S, Markhof, Y, Wollburg, P, and Zezza, A. Acceptance of COVID-19 vaccines in sub-Saharan Africa: evidence from six national phone surveys. BMJ Open. (2021) 11:e055159. doi: 10.1136/bmjopen-2021-055159
45. Groves, HE, Piché-Renaud, PP, Peci, A, Farrar, DS, Buckrell, S, Bancej, C, et al. The impact of the COVID-19 pandemic on influenza, respiratory syncytial virus, and other seasonal respiratory virus circulation in Canada: a population- based study. Lancet Region Health Am. (2021) 1:100015. doi: 10.1016/j.lana.2021.100015
46. Fontanet, A, and Cauchemez, S. COVID-19 herd immunity: where are we? Nat Rev Immunol. (2020) 20:583–4. doi: 10.1038/s41577-020-00451-5
47. Solís Arce, JS, Warren, SS, Meriggi, NF, Scacco, A, McMurry, N, Voors, M, et al. COVID-19 vaccine acceptance and hesitancy in low-and middle-income countries. Nat Med. (2021) 27:1385–94. doi: 10.1038/s41591-021-01454-y
48. Majeed, B, David, JF, Bragazzi, NL, McCarthy, Z, Grunnill, MD, Heffernan, J, et al. Mitigating co-circulation of seasonal influenza and COVID-19 pandemic in the presence of vaccination: a mathematical modeling approach. Front Public Health. (2023) 10:1–20. doi: 10.3389/fpubh.2022.1086849
49. Soares, P, Rocha, JV, Moniz, M, Gama, A, Laires, PA, Pedro, AR, et al. Factors associated with COVID-19 vaccine hesitancy. Vaccine. (2021) 9:1–14. doi: 10.3390/vaccines9030300
50. Silva, MC, Silva, NCH, Ferreira, ALCG, Ferreira, FCG, Melo, MIB, Silva, LMX, et al. Neutralizing antibodies against SARS-CoV-2 in Brazilian pregnant women vaccinated with one or two doses of BNT162b2 mRNA vaccine (Pfizer/WyethTM). Front Public Health. (2023) 10:1–7. doi: 10.3389/fpubh.2022.1054460
51. Bussink-Voorend, D, Hautvast, JL, Vandeberg, L, Visser, O, and Hulscher, ME. A systematic literature review to clarify the concept of vaccine hesitancy. Nature human. Behaviour. (2022) 6:1634–48. doi: 10.1038/s41562-022-01431-6
52. Shan, D, Xu, J, Liu, T, Zhang, Y, Dai, Z, Zheng, Y, et al. Subjective attitudes moderate the social connectedness in esports gaming during COVID-19 pandemic: a cross-sectional study. Front Public Health. (2022) 10:1–10. doi: 10.3389/fpubh.2022.1020114
53. Xiong, Y, Weng, X, Snyder, B, Ma, L, Cong, M, Miller, EL, et al. Perceptions and knowledge regarding the COVID-19 pandemic between US and China: a mixed methods study. Glob Health. (2022) 18:1–14. doi: 10.1186/s12992-022-00864-y
54. Takoudjou Dzomo, GR, Mbario, E, Djarma, O, Soumbatingar, N, Madengar, M, Djimera, N, et al. Predictors of COVID-19 vaccine hesitancy in Chad: a cross-sectional study. Front Public Health. (2023) 10:1–18. doi: 10.3389/fpubh.2022.1063954
55. Caso, D, Carfora, V, Starace, C, and Conner, M. Key factors influencing Italian mothers’ intention to vaccinate sons against HPV: the influence of trust in health authorities, anticipated regret and past behaviour. Sustainability. (2019) 11:e6879. doi: 10.3390/su11236879
56. Grodzicka, ED. Taking vaccine regret and hesitancy seriously. The role of truth, conspiracy theories, gender relations and trust in the HPV immunisation programmes in Ireland. J Cult Res. (2021) 25:69–87. doi: 10.1080/14797585.2021.1886422
57. Pokharel, M, Lillie, HM, Nagatsuka, K, Barbour, JB, Ratcliff, CL, and Jensen, JD. Social media narratives can influence vaccine intentions: the impact of depicting regret and character death. Comput Hum Behav. (2023) 141:e107612:107612. doi: 10.1016/j.chb.2022.107612
58. Christy, SM, Winger, JG, Raffanello, EW, Halpern, LF, Danoff-Burg, S, and Mosher, CE. The role of anticipated regret and health beliefs in HPV vaccination intentions among young adults. J Behav Med. (2016) 39:429–40. doi: 10.1007/s10865-016-9716-z
59. Penţa, MA, Crăciun, IC, and Băban, A. The power of anticipated regret: predictors of HPV vaccination and seasonal influenza vaccination acceptability among young Romanians. Vaccine. (2020) 38:1572–8. doi: 10.1016/j.vaccine.2019.11.042
60. Ziarnowski, KL, Brewer, NT, and Weber, B. Present choices, future outcomes: anticipated regret and HPV vaccination. Prev Med. (2009) 48:411–4. doi: 10.1016/j.ypmed.2008.10.006
61. Pan, Y, Ng, CT, and Cheng, TCE. Effect of free-riding behavior on vaccination coverage with customer regret. Comput Ind Eng. (2021) 159:e107494:107494. doi: 10.1016/j.cie.2021.107494
62. Schwarzinger, M, Watson, V, Arwidson, P, Alla, F, and Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: a survey experiment based on vaccine characteristics. Lancet Public Health. (2021) 6:e210–21. doi: 10.1016/S2468-2667(21)00012-8
63. Sallam, M. COVID-19 vaccine hesitancy worldwide: a concise systematic review of vaccine acceptance rates. Vaccine. (2021) 9:160. doi: 10.3390/vaccines9020160
64. Chung, GKK, Chan, L, Chan, SM, Chen, JK, Wong, H, and Chung, YN. The impact of trust in government on pandemic management on the compliance with voluntary COVID-19 vaccination policy among adolescents after social unrest in Hong Kong. Front Public Health. (2022) 10:1–12. doi: 10.3389/fpubh.2022.992895
65. Solís Arce, JS, Warren, SS, Meriggi, NF, Scacco, A, McMurry, N, Voors, M, et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat Med. (2021) 27:1385–94. doi: 10.1038/s41591-021-01454-y
66. Fu, C, Wei, Z, Pei, S, Li, S, Sun, X, and Liu, P. Acceptance of and preference for COVID-19 vaccination in healthcare workers: a comparative analysis and discrete choice experiment. MedRxiv. (2020) 4:1–35. doi: 10.1101/2020.04.09.20060103
67. Maltezou, HC, Pavli, A, Dedoukou, X, Georgakopoulou, T, Raftopoulos, V, Drositis, I, et al. Determinants of intention to get vaccinated against COVID-19 among healthcare personnel in hospitals in Greece. Infect. Disease Health. (2021) 26:189–97. doi: 10.1016/j.idh.2021.03.002
68. Lazarus, JV, Wyka, K, White, TM, Picchio, CA, Rabin, K, Ratzan, SC, et al. Revisiting COVID-19 vaccine hesitancy around the world using data from 23 countries in 2021. Nat Commun. (2022) 13:3801–14. doi: 10.1038/s41467-022-31441-x
69. Biswas, N, Mustapha, T, Khubchandani, J, and Price, JH. The nature and extent of COVID-19 vaccination hesitancy in healthcare workers. J Community Health. (2021) 46:1244–51. doi: 10.1007/S10900-021-00984-3
70. Heyerdahl, LW, Dielen, S, Nguyen, T, van Riet, C, Kattumana, T, Simas, C, et al. Doubt at the core: unspoken vaccine hesitancy among healthcare workers. Lancet Regional Health Europe. (2022) 12:100289–2. doi: 10.1016/j.lanepe.2021.100289
71. Paget, J, Spreeuwenberg, P, Charu, V, Taylor, RJ, Iuliano, AD, Bresee, J, et al. Global mortality associated with seasonal influenza epidemics: new burden estimates and predictors from the GLaMOR project. J Glob Health. (2019) 9:9. doi: 10.7189/jogh.09.020421
72. World Health Organization. Influenza (seasonal). World Health Organization (2022). Available online at: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (Accessed February 10, 2023).
Keywords: vaccine hesitancy, COVID-19, social media, sentiment analysis, vaccine regret
Citation: Machado Júnior C, Mantovani DMN, de Sandes-Guimarães LV, Romeiro MC, Furlaneto CJ and Bazanini R (2023) Volatility of the COVID-19 vaccine hesitancy: sentiment analysis conducted in Brazil. Front. Public Health. 11:1192155. doi: 10.3389/fpubh.2023.1192155
Edited by:
Ke Jiang, Elon University, United StatesReviewed by:
Srikanth Umakanthan, The University of the West Indies St. Augustine, Trinidad and TobagoCopyright © 2023 Machado Júnior, Mantovani, de Sandes-Guimarães, Romeiro, Furlaneto and Bazanini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Celso Machado Júnior, Y2Vsc28uanVuaW9yQG9ubGluZS51c2NzLmVkdS5icg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.