 Hui Zhang1
Hui Zhang1 Changdong Zhao
Changdong Zhao Xiuqing Li
Xiuqing Li- 1Department of Gastroenterology and Hepatology, Lianyungang Second People's Hospital, Lianyungang, China
- 2Department of Gastroenterology and Hepatology, Affiliated Lianyungang Oriental Hospital of Xuzhou Medical University, Lianyungang, China
- 3Department of Gastroenterology and Hepatology, The Third People's Hospital of Zhenjiang, Zhenjiang, China
Objective: Gastrointestinal cancer is the leading cause of cancer-related death in China, and its early screening is largely recommended by healthcare workers. This study investigated the knowledge, attitudes, and practice (KAP) of healthcare workers on early gastrointestinal cancer (EGC).
Methods: This cross-sectional study was conducted on healthcare workers who volunteered to participate from 30 hospitals in China between September and December 2022. A self-administered questionnaire including 37 questions was developed.
Results: A total of 545 completed questionnaires were finally obtained. Healthcare workers had moderate knowledge level [9.22 ± 1.80 (65.88±12.89%), total score: 14], positive attitude [21.84 ± 2.67 (91.01 ± 11.14%), total score: 24], and excellent practice level [19.07 ± 4.43 (79.47 ± 18.44%), total score: 24] on EGC. Pearson's correlation analysis suggested that knowledge score was positively correlated with attitude (r = 0.264, P < 0.001) and practice score (r = 0.140, P = 0.001), and higher attitude score was significantly correlated with higher practice score (r = 0.380, P < 0.001), which were supported and reinforced by structural equation modeling. In addition, subgroup analysis showed that knowledge scores might be influenced by sex, age, education, type of hospital, type of occupation, professional title, and years of working (all P < 0.05); attitude scores might be influenced by years of working (P < 0.05); and practice scores were statistically distinct among groups of different sex, department, and years of working (all P < 0.05).
Conclusion: Healthcare workers have moderate knowledge level, positive attitude, and excellent practice levels on EGC. Good knowledge and positive attitude might be correlated with excellent practice. KAP level might be influenced by sociodemographic characteristics.
1. Introduction
Gastrointestinal cancer refers to malignant carcinoma that affects the digestive system, including the gastrointestinal tract and accessory organs. Globally, the age-standardized incidence rate (ASIR) of gastrointestinal cancer was as high as 61.9% per 100,000 person-years in 2019 (1). Common gastrointestinal cancers are recognized as the leading cause of cancer-related death, accounting for 36.2% of overall cancer mortality (2). Based on Cancer Statistics in China 2015, cancers of the esophagus, stomach, colorectum, liver, and pancreas ranked among the top contributors to cancer-related death (3). Under the abovementioned circumstance, efficient intervention could be of priority to palliate the mortality and public health burden of gastrointestinal cancer. The early stage of cancer functions as a critical time window for detection and treatment, during which proper management could largely prolong the survival time of cancer patients (4). Early gastrointestinal cancers (EGC) are limited to the mucosa or submucosa without invading muscularis propria, and timely treatment could greatly exert positive effects on a 5-year survival rate and prognosis (5, 6).
A series of screening methods were available for the detection of EGC, such as barium-meal photofluorography, endoscopic examination, and serological biomarker testing. Despite the increasing number of individuals involved in the screening of gastrointestinal cancer, the population coverage remains to be elevated and the early detection rate is still unsatisfactory (7). Deficiency in clinicians and medical facilities, imbalance in socioeconomic development, and inadequate public awareness of gastrointestinal cancer screening could to some extent account for such phenomenon. In addition, individuals might be reluctant to undergo screening because of insufficient knowledge, the invasiveness of examination, physical discomfort, and emotional concerns (8). Therefore, promoting the screening rate would be urgently needed for the better prevention and control of EGC.
In China, individual screening of gastrointestinal cancer is largely carried out according to the healthcare workers' suggestions during routine consultations (7). In addition, the knowledge and attitude of healthcare workers toward gastrointestinal cancer could determine their prescription process, which further impacts the individual involvement in screening. Therefore, a better understanding of knowledge, attitude, and practice (KAP) among healthcare workers is necessary to formulate feasible strategies and perform effective intervention programs. Previous literature suggested that there was a need for improvement in the KAP regarding cancer diagnosis and treatment. For example, although healthcare workers were aware of the importance of cervical cancer prevention, the attitudes and practices toward screening were negative (9). Furthermore, while nurses had sufficient knowledge about breast cancer, they still required additional information on cancer risk estimation (10). However, there is a dearth of KAP for gastrointestinal cancer among healthcare workers in China to date. Additionally, sociodemographic factors might serve as modifiers of KAP toward cancers, however, which remained undetermined on the KAP related to gastrointestinal cancer (11). In this study, we aimed to provide a reference of Chinese healthcare workers' KAP of gastrointestinal cancer and related sociodemographic factors.
2. Materials and methods
2.1. Study design and participants
This cross-sectional study was conducted from September to December 2022 and included healthcare workers from 30 hospitals in Jiangsu Province, aiming to enhance the generalizability of the findings. A simple random sampling method was used to select healthcare workers from each hospital who volunteered to participate in the study. The hospital's information is shown in Supplementary Table 2. This study was approved by the institutional ethics committee of The Second People's Hospital of Lianyungang City in Jiangsu Province, and the informed consent of the participants was obtained.
2.2. Questionnaire
The questionnaire was designed according to guidelines, including the China Guideline for Screening, Early Detection and Early Treatment of Gastric Cancer (2022, Beijing), China Guideline for Screening, Early Detection and Early Treatment of Esophageal Cancer (2022, Beijing), and Guideline for the Diagnosis and Treatment of Esophageal Cancer (2022 Edition). Then, the questionnaire was modified according to the suggestions of five experts, and then, the pilot survey was performed on a small scale (48 questionnaires were dispatched).
The final questionnaire was a Chinese version that collected data from 37 questions in four dimensions (Supplementary Table 1). Specifically, the sociodemographic characteristics dimension consisted of 10 questions, the knowledge dimension included 14 questions, the attitude dimension included 7 questions, and the practice dimension included 6 questions. Every correct answer in the knowledge dimension was scored by 1 point, and a wrong or unclear answer was scored by 0 point, ranging from 0 to 14 points. For attitude and practice dimensions, the answers were scored from 0 to 4 points, and the range of the total score was provided (0 to 24); the seventh question was not included because of unable to be scored and described only. The knowledge dimension of our study encompassed a comprehensive understanding of gastrointestinal cancer, including its definition (items 1–5), risk factors (items 6–7), early detection (item 8), treatment options (items 9–13), and prevention (item 14). Participants' attitudes toward gastrointestinal cancer were assessed to gauge their perspectives (items 2 and 3), beliefs (items 1, 5), and emotional responses (items 4 and 6) toward this disease. Additionally, participants' practices were examined to evaluate their behaviors and actions concerning the prevention (items 1–3), diagnosis (item 4), and treatment (items 5 and 6) of gastrointestinal cancer.
2.3. Procedures
The online questionnaire based on the SoJump application of WeChat was used for the survey, and a QR code was generated to allow the data collection through WeChat. Participants logged in by scanning the QR code sent by WeChat and then completed the questionnaire. To guarantee the quality and completeness of the questionnaire survey, each IP address could only submit the questionnaire once, and all questions in the questionnaire were mandatory. The completeness, internal coherence, and reasonableness of all questionnaires were checked by the investigators.
2.4. Statistical analysis
Stata 17.0 (Stata Corporation, College Station, TX, USA) software was used for the statistical analysis. A descriptive analysis of the general characteristics of the participants and the KAP scores was performed as follows: Continuous variables in a normal distribution (KAP scores) were described by mean ± standard deviation (SD), and the maximum and minimum values were also reported. The hundred-mark system (HMS) of the KAP score was calculated by the following formula: sum of the knowledge score—minimum possible score)/range of the knowledge score. Categorical data including the demographic characteristics and answers to different questions were described by n (%). For the knowledge dimension, the HMS score of ≤50% was defined as “low knowledge level,” 50–85% was defined as “moderate knowledge level,” and >85% is defined as “high knowledge level.” For the attitude dimension, the HMS score <30% indicates “negative attitude,” 30%−60% indicates “neutral attitude,” and >60% indicates “positive attitude.” For the practice dimension, the HMS score <25% is defined as “poor practice,” 25%−50% is defined as “general practice,” 51%−75% is defined as “good practice,” and >75% is defined as “excellent practice.” The data's normality was evaluated through Kolmogorov–Smirnov test. When the data followed a normal distribution, the comparison between the two groups was conducted using Student's t-test, while analysis of variance (ANOVA) was employed for comparisons among multiple groups. In cases where the data exhibited a skewed distribution, the Mann–Whitney U test was utilized for comparing two groups, and the Kruskal–Wallis analysis of variance was employed for comparing multiple groups. Pearson correlation analysis was used to assess the correlation in the three dimensions. The differences in the knowledge, attitude, and practice of EGC were compared in healthcare workers with different general characteristics. Structural equation modeling (SEM) analysis was further conducted to explore the direct and indirect associations between sociodemographic characteristics and KAP scores. A two-sided P-value of <0.05 was considered statistically significant.
3. Results
The pilot survey findings (N = 48) demonstrated high internal consistency in the KAP dimensions, with Cronbach's α values of 0.896, 0.821, and 0.902, respectively. The Kaiser–Meyer–Olkin (KMO) measure for the KAP dimensions was 0.803, 0.841, and 0.889, respectively. The validity and reliability of the questionnaire were assessed, revealing a Cronbach's α of 0.873 and a KMO of 0.720. As shown in Supplementary Table 3, strong reliability and adequate internal consistency measures in the design of the questionnaire were observed. The results from Bartlett's test and the KMO values provided support for conducting factor analysis, indicating robust construct validity.
A total number of 545 questionnaires were collected for analysis. The majority of participants (66.98%) were between 31 and 50 years old, and most subjects were women (72.48%) and obtained educational attainments of technical secondary school or junior college (80.00%). Participants working in tertiary public hospitals accounted for 70.28%, and nearly half of the whole population (41.83%) were affiliated to the internal medicine department. The occupation of participants was mainly doctor (42.86%) and nurse (48.19%), and 64.95% of them owned the professional title of medium or above. Years of working were mainly distributed in ≥11 years (62.93%). Although upper gastrointestinal disease was reported in more than half of participants or their family and friends (57.25%), gastrointestinal cancer (such as esophageal or gastric cancer) occurred uncommonly among participants' families (11.19%) (Table 1).
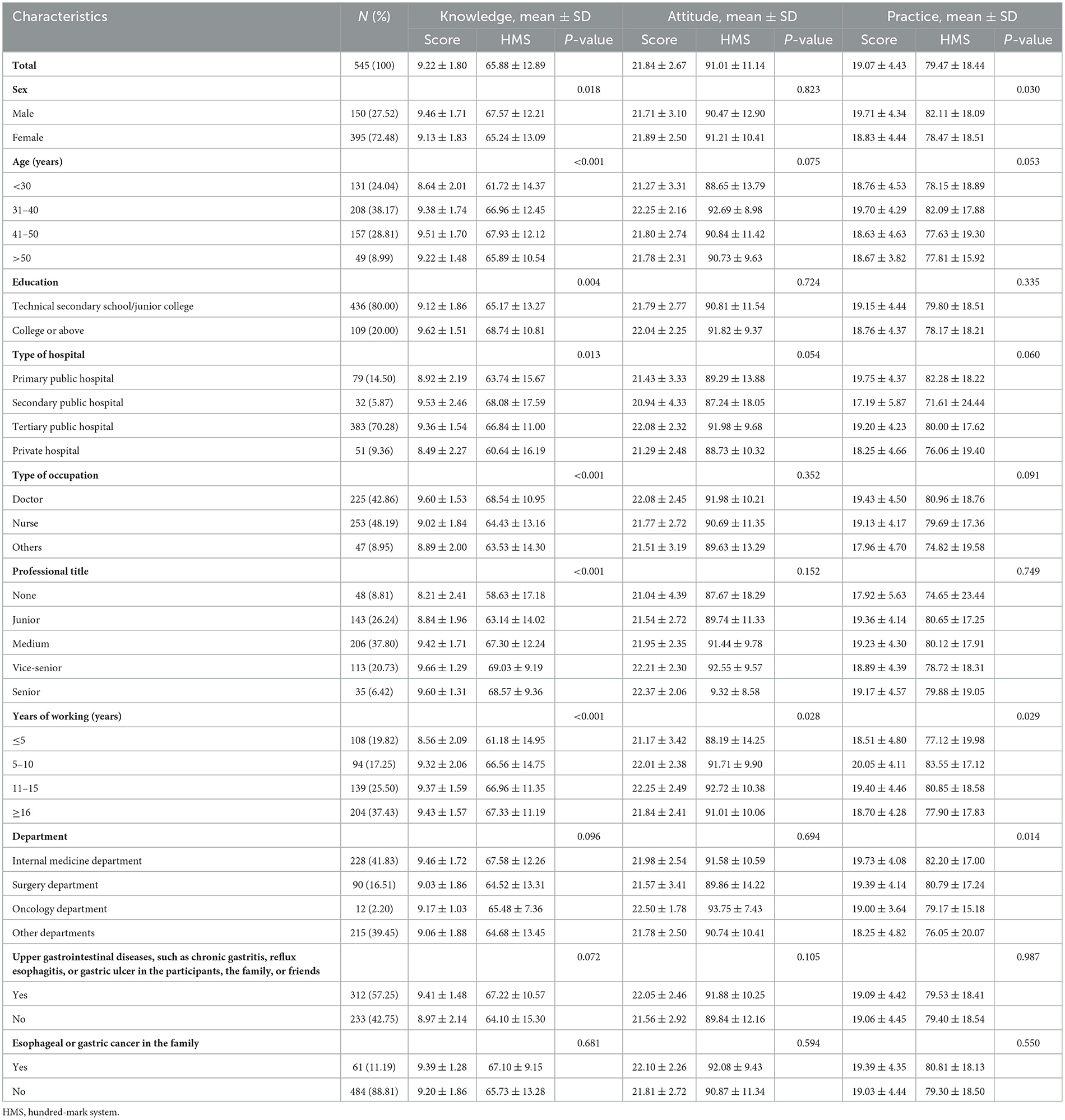
Table 1. Baseline characteristics of the participants.
The mean knowledge, attitude, and practice score was 9.22 ± 1.80 (65.88±12.89%, total score: 14), 21.84 ± 2.67 (91.01±11.14%, total score: 24), and 19.07 ± 4.43 (79.47±18.44%, total score: 24) among all respondents. In addition, subgroup analysis revealed that knowledge scores differed significantly among groups of different sex, age, education, type of hospital, type of occupation, professional title, and years of working (all P < 0.05); attitude scores were distinctly disparate among groups of different years of working (P < 0.05) (those with long years of working, such as 11–15 years, had more positive attitude); and practice scores were statistically distinct among groups of different sex, department, and years of working (all P < 0.05) (Table 1).
The correct rate of knowledge dimension ranged from 6.97% to 96.33%. Most participants (96.33%) agreed that to prevent EGC, the following items should be paid additional attention to daily living: appropriate dietary structure, personal hygiene, regular diet, avoiding heavy smoking or drinking, and defecating every day. However, only 6.97% of them knew that EGC is mainly treated endoscopically, including endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD), of which EMR is more frequently used (Table 2). Based on the cutoff value, as high as 86.24% of respondents were assigned to a group of moderate knowledge level.
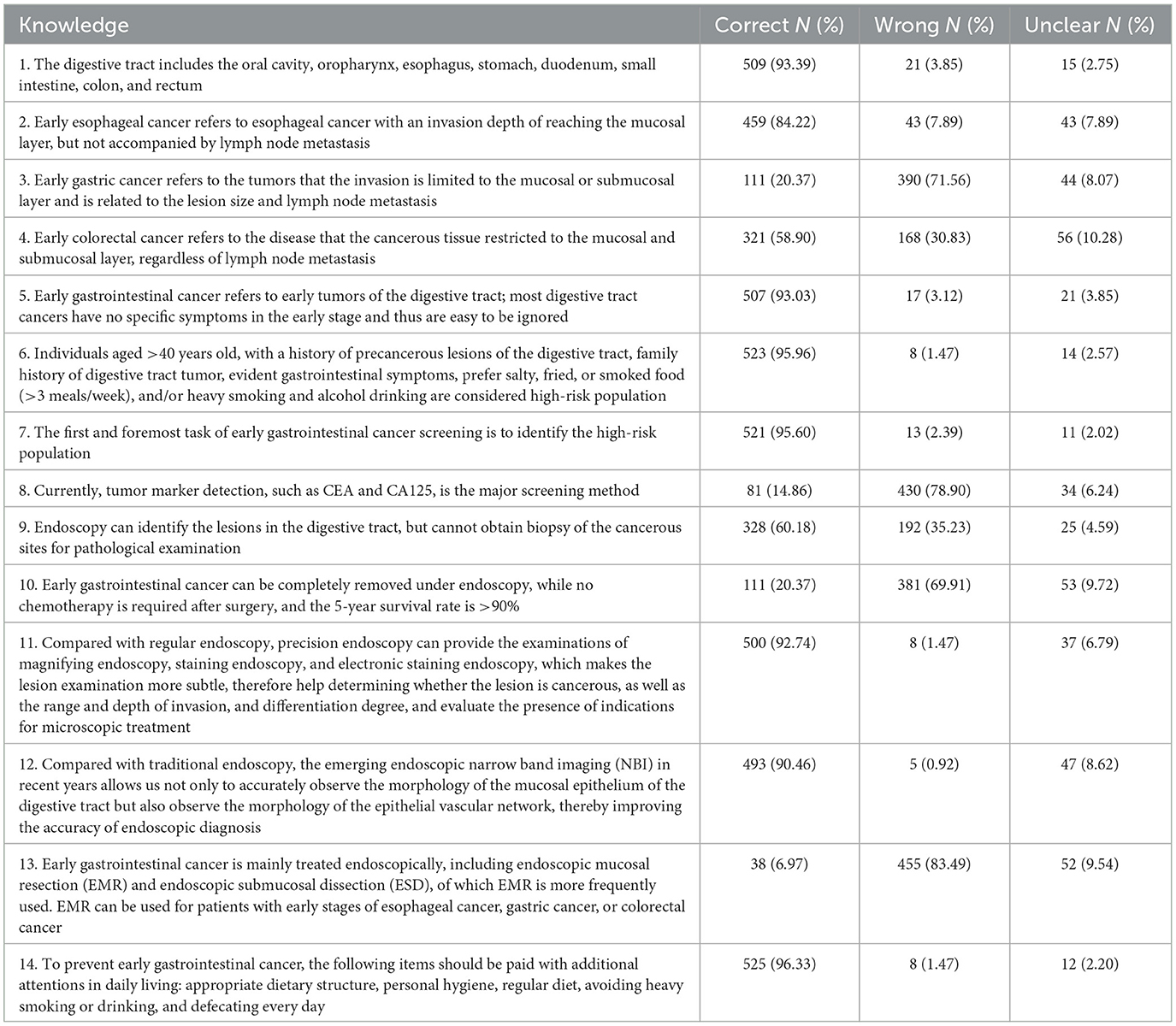
Table 2. Knowledge dimension of the participants.
The majority of participants held the answers of “Highly agree” or “Agree” in the attitude dimension, with a proportion from 82.75% to 99.08%. Most respondents (99.08%) would be willing to popularize the knowledge of EGC. However, subtly less population (82.75%) held positive attitude toward that esophageal cancer and stomach cancer can be radically treated or completely cured (Table 3). Overall, 99.27% of participants owned a good attitude level. Additionally, the majority of participants agreed that unhealthy eating habits and lifestyle, gastrointestinal disease, and family history were associated with gastrointestinal cancer (Table 4).

Table 3. Attitude dimension of the participants.
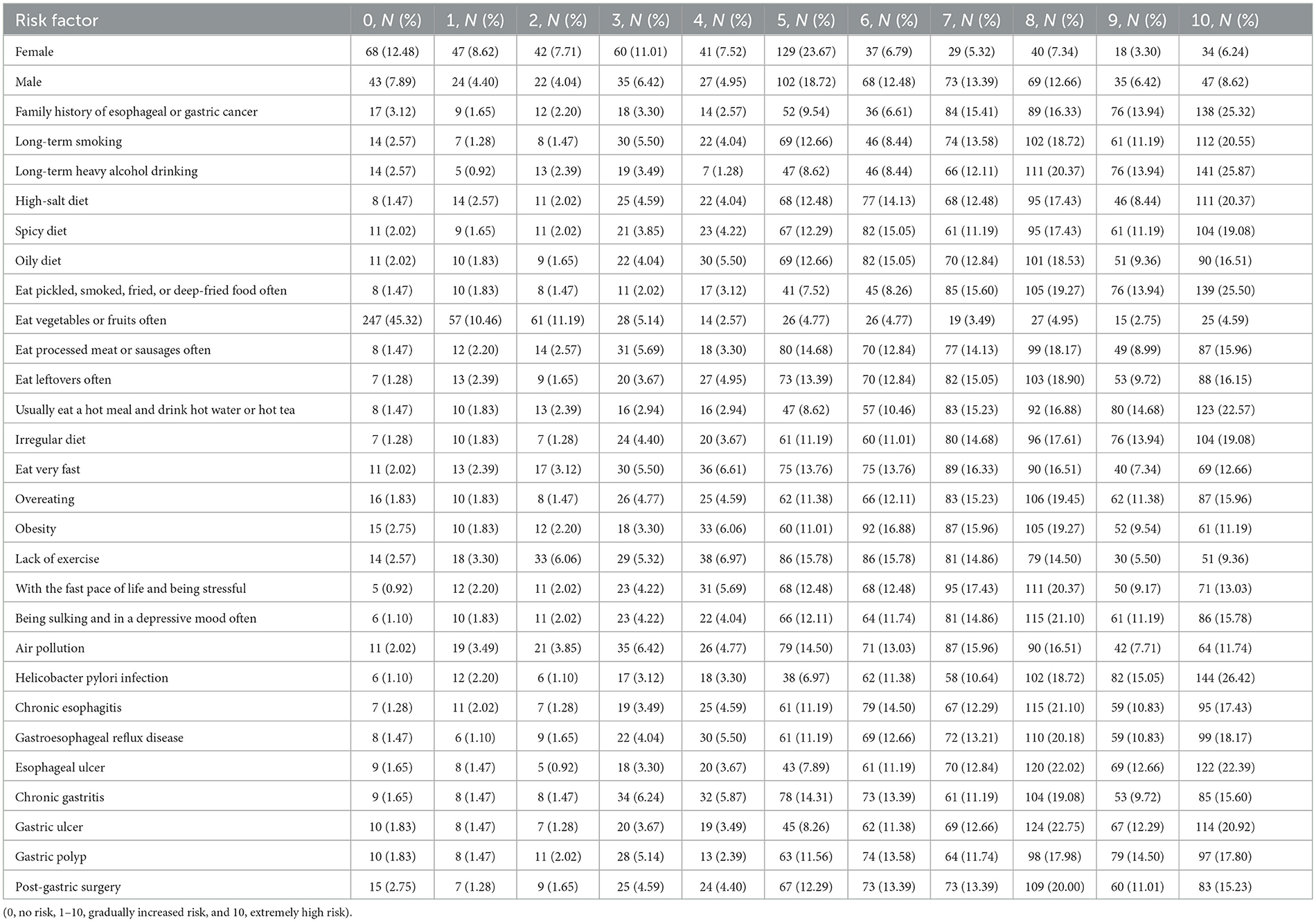
Table 4. The detailed answers to the question “A7. Which of the followings do you consider to be risk factors of gastrointestinal cancer?”
More than half of the whole population chose “Always” or “Often” in the practice dimension (Table 5). Most subjects (93.77%) gave positive responses toward propagating knowledge of EGC to patients. In addition, the lowest frequency of participants (67.71%) would actively participate in the popularization of knowledge on the importance of EGC screening as possible. The proportion of respondents with excellent practice ranked at the top (58.53%), followed by good (33.76%) and general practice (7.34%).
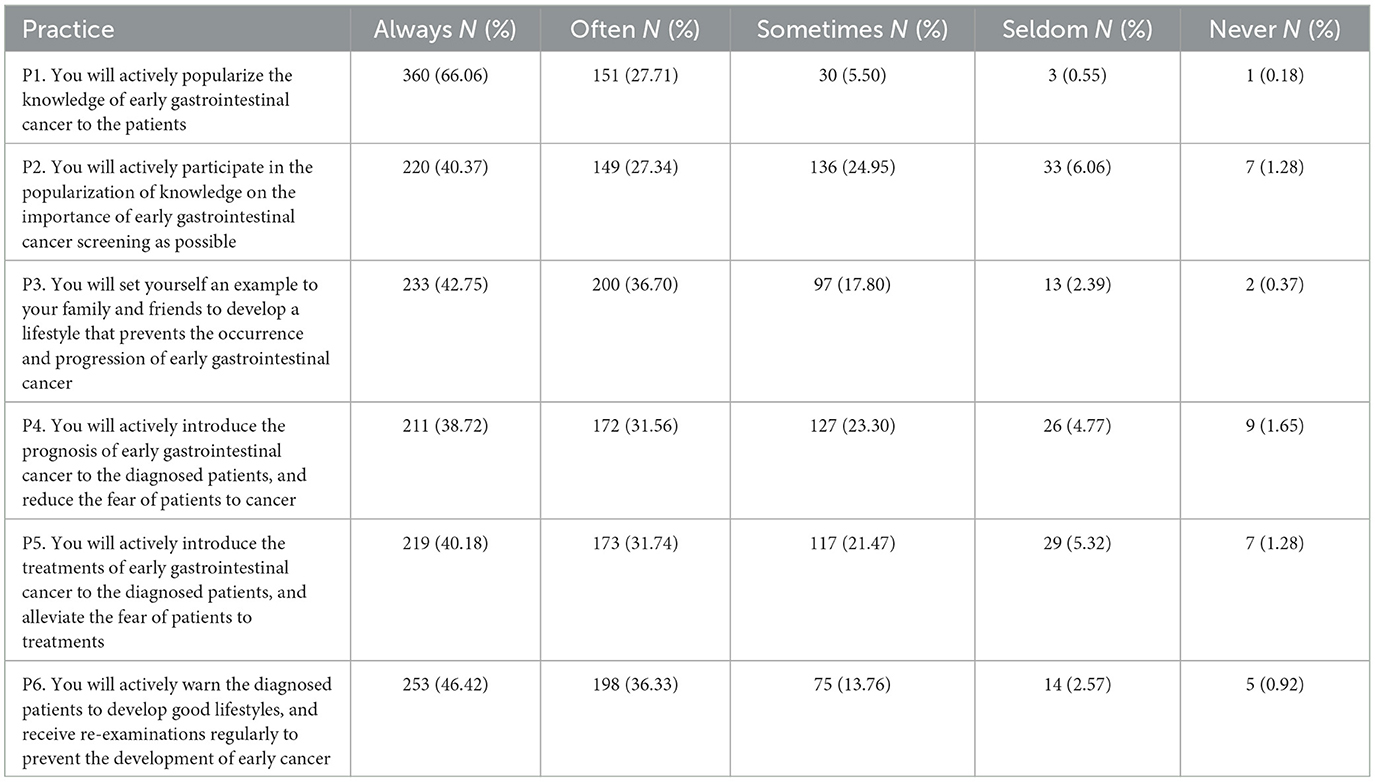
Table 5. Practice dimension of the participants.
Pearson correlation analysis further revealed that knowledge score was positively correlated with both attitude (r = 0.264, P < 0.001) and practice score (r = 0.140, P = 0.001), and higher attitude score was significantly correlated with higher practice score (r = 0.380, P < 0.001) (Table 6). Moreover, the findings from the goodness-of-fit analysis indicated that the observed data aligned well with the proposed model, demonstrating consistency between the relationships among variables (Table 7). In addition, it was observed that professional title had a direct positive association with knowledge (path coefficient = 0.42, 95%CI: 0.21, 0.63, P < 0.001), while it had an indirect positive association with attitude (path coefficient = 0.16, 95%CI: 0.07, 0.26, P = 0.001) and practice score (path coefficient = 0.15, 95%CI: 0.04, 0.27, P = 0.010). Additionally, directly positive associations were found between knowledge and attitude (path coefficient = 0.38, 95%CI: 0.26, 0.50, P < 0.001), as well as between attitude and practice scores (path coefficient = 0.62, 95%CI: 0.48, 0.75, P < 0.001). In addition, a higher knowledge score was indirectly associated with higher practice score (path coefficient = 0.24, 95%CI: 0.14, 0.33, P < 0.001) (Table 8; Figure 1). These results from SEM supported and reinforced the main findings presented in the Pearson correlation analysis.
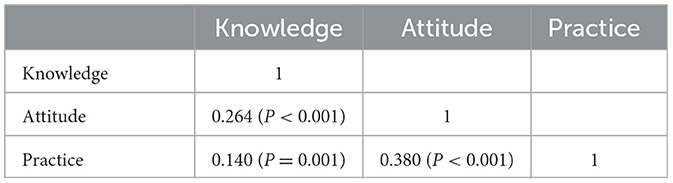
Table 6. Correlation analysis of KAP scores.
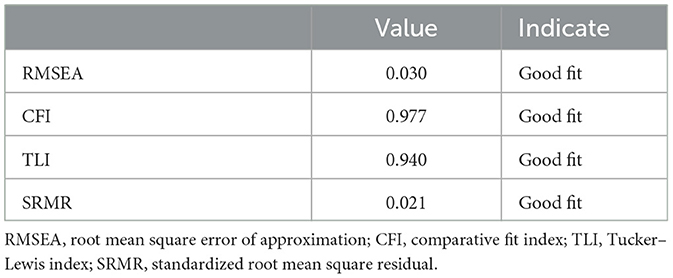
Table 7. Goodness of fit of SEM.
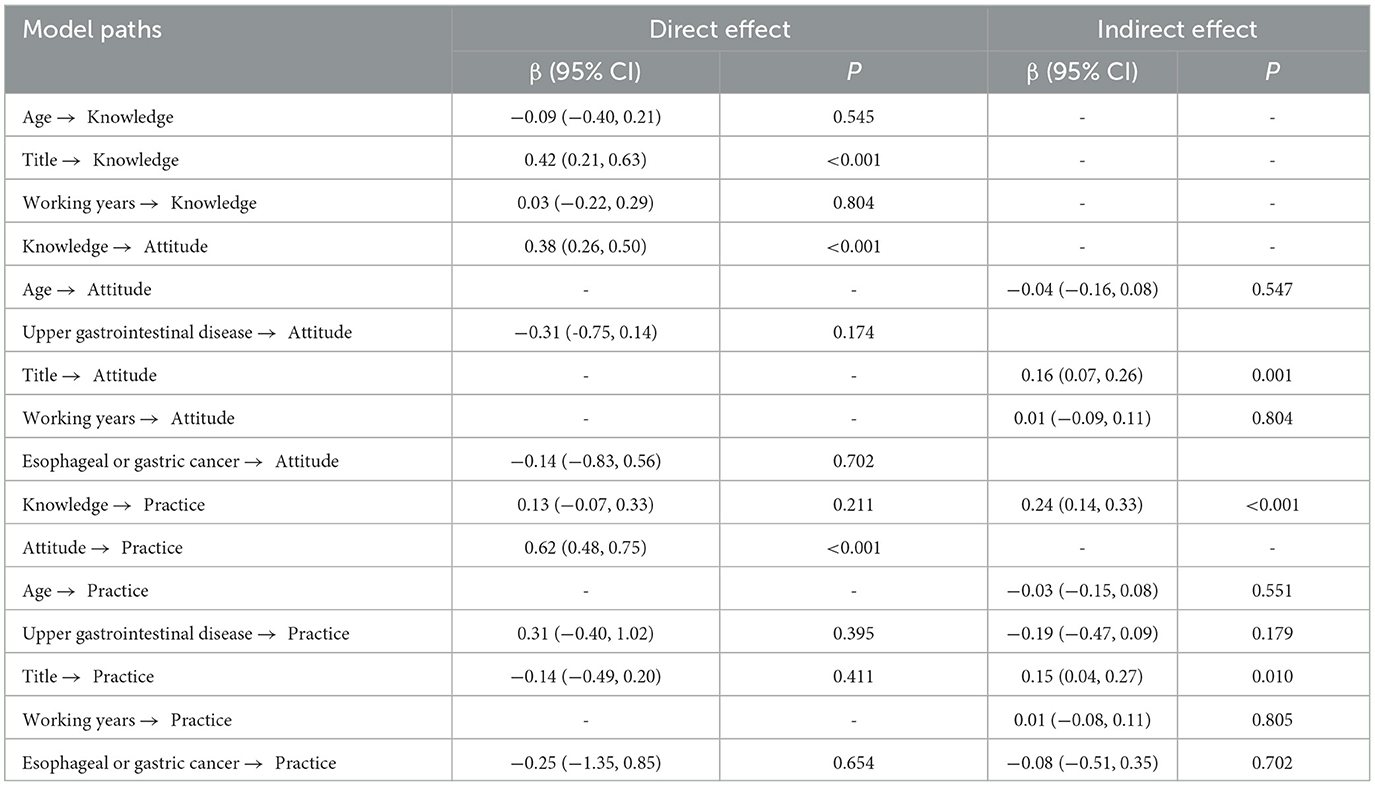
Table 8. The direct and indirect estimates of SEM.
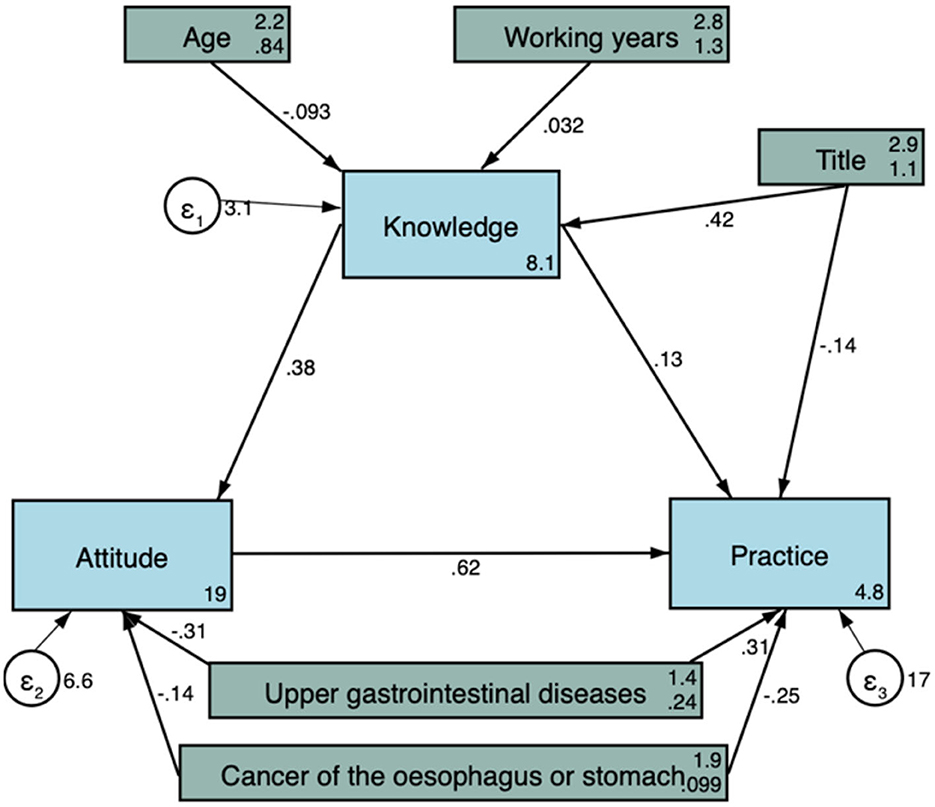
Figure 1. Structural equation model showing the associations between sociodemographic factors and KAP scores. All variables are observed variables. The direction of causality is indicated by single-headed arrows. The standardized path coefficients are presented alongside the arrows.
4. Discussion
This study suggested that healthcare workers in China have moderate knowledge level, positive attitude, and excellent practice level on EGC. Good knowledge and positive attitude might be correlated with excellent practice. In addition, the KAP level might be influenced by sociodemographic characteristics. These findings might provide cues for hospitals about targeted educational intervention toward healthcare workers on EGC.
The high reliability of the questionnaire indicated consistent measurement of the underlying construct, and the adequate internal consistency suggested strong correlations among items within each construct. Furthermore, the results from Bartlett's test and KMO values supported the conduct of factor analysis, assessing the proportion of variance attributed to underlying factors. The robust construct validity observed confirmed the accurate measurement of intended constructs and was further supported by the factor analysis, revealing the underlying factor structure. These findings aligned with previous research emphasizing the importance of assessing reliability, internal consistency, and construct validity in questionnaire design (12, 13).
The participants obtained moderate knowledge of gastrointestinal cancer, who had a good understanding of cancer symptoms and prevention, but were unfamiliar with early-stage screening and treatment. Consistent with the present study, studies from Australia, China, Saudi Arabia, and Spain also corroborated the insufficient knowledge of gastrointestinal cancer screening among the population (14–17). In this study, we observed that the knowledge score would significantly increase or show an increment tendency as participants had advanced age, higher education level, superior professional titles, and long years of working. Similarly, Wong (18) found that lower educational attainment showed negative associations with knowledge of colorectal cancer screening. Alshammari and Alenazi (14) observed that respondents more than 50 years old had better knowledge regarding colorectal cancer. In addition, the association of mean knowledge rank with the physician's job title was also reported (19). These results could be interpreted that participants intended to obtain adequate knowledge of gastrointestinal cancer for the sake of an academic certificate or career promotion. However, Aldukhayel and Alsudairi (19) reported a negative association between knowledge and years of experience, which conflicted with our findings. Population heterogeneity, differences in socioeconomic background, and methodology diversity could account for the discrepancy. In addition, male healthcare workers scored better than their female counterparts in the knowledge dimension, which was in agreement with the finding of Demyati (20) but in conflict with the study of Mosli and Alnahdi (21). It could be attributed to the fact that common gastrointestinal cancers, such as gastric and colorectal cancer, were more prevalent among men; therefore, male participants were more likely to search and receive related knowledge (22, 23).
Compared with previous studies, the participants herein had higher attitude levels, especially in the propagation of knowledge on EGC (15, 17). As the screening of early-stage gastrointestinal cancer, such as gastroscopy, is carried out through opportunistic screening in China, mass participation is heavily influenced by individual self-consciousness (24, 25). Furthermore, participants' understanding of disease and action of taking hospital treatment are mainly impacted by healthcare providers; therefore, positive attitude toward gastrointestinal cancer among healthcare workers could help cancer prevention and control. We also observed that participants with years of working more than 5 years owned more positive attitudes compared with those with shorter years of working. In concordance with the study of Aldukhayel and Alsudairi (19), it supported the hypothesis that increased years of experience could contribute to overall awareness and correct attitude toward gastrointestinal cancer.
In accordance with the present study, more than half of the participants were with excellent practice scores in our study (26, 27). Most respondents were willing to popularize the information of EGC; however, reduced number of them were likely to propagate the early-stage screening. The above results could be explained by the inadequate knowledge of EGC screening among healthcare workers. Male healthcare workers were more active in the dissemination of gastrointestinal cancer prevention and treatment than female colleagues, partly due to higher knowledge scores among male subjects. Consistently, male subjects exhibited more enthusiasm for bowel cancer screening according to the research of Holden and Frank (28). However, Wang and Lin (29) reported that the female gender was positively associated with colorectal cancer screening. The aforementioned conflict could be derived from different sociodemographic characteristics, regional culture, and questionnaire design. Years of working were observed as an independent factor of practice score. It was understandable that expertise gets enhanced with the increment of years of working, which further exerts positive impacts on real-world practice. In addition, individuals with gastrointestinal discomfort tend to seek medical advice in the internal medicine department; therefore, healthcare workers in the internal medicine department could more frequently popularize gastrointestinal cancer and recommend screening.
It was noteworthy that knowledge was positively correlated with attitude, which was in agreement with previous literature (30, 31). As attitude included constituent of cognition, obtained knowledge helps formulate rational and lasting beliefs (32). Furthermore, subjects with higher knowledge and attitude scores were inclined to participate in practice more actively. Attitude helps to form judgment and evaluate the response to certain behavior; therefore, positive attitude could make practice more easily (33). Our results indicated that educational intervention could be of priority to target healthcare workers with female gender, <30 years old, lower education degree, private hospital, nurse occupation, junior job title, and shorter years of working.
This study first investigated the KAP status of EGC among healthcare workers in China and provided valuable information for future strategy formulation. In addition, several influential factors of KAP scores were identified, which facilitated targeted intervention. Based on the positive correlations among KAP scores, targeted educational intervention was proposed for the prevention and control of gastrointestinal cancer. However, several limitations also existed in our study. First, convenient sampling was adopted for participant collection, which could to some extent weaken the generalizability of results. Second, the sample size was relatively limited. Multi-center studies with larger sample sizes and higher response rates were needed to validate our findings.
In conclusion, healthcare workers in China have moderate knowledge level, positive attitude, and excellent practice level on EGC. Good knowledge and positive attitude might be correlated with excellent practice. KAP level might be influenced by sociodemographic characteristics. Targeted education could be further proposed to promote the overall knowledge, attitude, and practice of gastrointestinal cancer on EGC.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the Second People's Hospital of Lianyungang City in Jiangsu Province (# 2022016). The patients/participants provided their written informed consent to participate in this study.
Author contributions
CZ and YW carried out the studies, participated in collecting data, and drafted the manuscript. DW and CS performed the statistical analysis and participated in its design. HZ and XL participated in the acquisition, analysis, or interpretation of data and draft the manuscript. All authors read and approved the final manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1191699/full#supplementary-material
References
1. Hong MZ Li JM, Chen ZJ, Lin XY, Pan JS, Gong LL. Global burden of major gastrointestinal cancers and its association with socioeconomics, 1990–2019. Front Oncol. (2022) 12:942035. doi: 10.3389/fonc.2022.942035
2. Collaborators GBDCoD. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1736–88. doi: 10.1016/S0140-6736(18)32203-7
3. Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, et al. Cancer statistics in China, 2015. CA Cancer J Clin. (2016) 66:115–32. doi: 10.3322/caac.21338
4. Hinestrosa JP, Kurzrock R, Lewis JM, Schork NJ, Schroeder G, Kamat AM, et al. Early-stage multi-cancer detection using an extracellular vesicle protein-based blood test. Commun Med. (2022) 2:29. doi: 10.1038/s43856-022-00088-6
5. Coda S, Lee SY, Gotoda T. Endoscopic mucosal resection and endoscopic submucosal dissection as treatments for early gastrointestinal cancers in Western countries. Gut Liver. (2007) 1:12–21. doi: 10.5009/gnl.2007.1.1.12
6. Reim D, Loos M, Vogl F, Novotny A, Schuster T, Langer R, et al. Prognostic implications of the seventh edition of the international union against cancer classification for patients with gastric cancer: the western experience of patients treated in a single-center European institution. J Clin Oncol. (2013) 31:263–71. doi: 10.1200/JCO.2012.44.4315
7. Xu H, Li W. Early Detection of gastric cancer in China: progress and opportunities. Cancer Biol Med. (2022) 19:1622–8. doi: 10.20892/j.issn.2095-3941.2022.0655
8. Alhuzaim W, Alosaimi M. M., Almesfer A, Shahrani NMA H., Alali A, Alibrahim KIF, et al. Saudi patients' knowledge, behavior, beliefs, self-efficacy and barriers regarding colorectal cancer screening. Int J Pharm Res Allied Sci. (2020) 9:14–20.
9. Mutyaba T, Mmiro FA, Weiderpass E. Knowledge, attitudes and practices on cervical cancer screening among the medical workers of Mulago Hospital, Uganda. BMC Med Educ. (2006) 6:13. doi: 10.1186/1472-6920-6-13
10. O. Odusanya OOTO. Breast cancer knowledge, attitudes and practice among nurses in Lagos, Nigeria. Acta Oncologica. (2001) 40:844–8. doi: 10.1080/02841860152703472
11. Akhigbe AO, Omuemu VO. Knowledge, attitudes and practice of breast cancer screening among female health workers in a Nigerian Urban City. BMC Cancer. (2009) 9:203. doi: 10.1186/1471-2407-9-203
12. Iversen HH, Holmboe O, Bjertnæs OA. The cancer patient experiences questionnaire. (Cpeq): reliability and construct validity following a national survey to assess hospital cancer care from the patient perspective. BMJ Open. (2012) 2:1437. doi: 10.1136/bmjopen-2012-001437
13. Oltedal S, Garratt A, Bjertnaes Ø, Bjørnsdottìr M, Freil M, Sachs M. The Norpeq patient experiences questionnaire: data quality, internal consistency and validity following a norwegian inpatient survey. Scand J Public Health. (2007) 35:540–7. doi: 10.1080/14034940701291724
14. Alshammari SA, Alenazi HA, Alshammari HS. Knowledge, attitude and practice towards early screening of colorectal cancer in Riyadh. J Family Med Prim Care. (2020) 9:2273–80. doi: 10.4103/jfmpc.jfmpc_290_20
15. Christou A, Thompson SC. Colorectal cancer screening knowledge, attitudes and behavioral intention among indigenous Western Australians. BMC Public Health. (2012) 12:528. doi: 10.1186/1471-2458-12-528
16. Gimeno-Garcia AZ, Quintero E, Nicolas-Perez D, Jimenez-Sosa A. Public awareness of colorectal cancer and screening in a Spanish population. Public Health. (2011) 125:609–15. doi: 10.1016/j.puhe.2011.03.014
17. Liu Q, Zeng X, Wang W, Huang RL, Huang YJ, Liu S, et al. Awareness of risk factors and warning symptoms and attitude towards gastric cancer screening among the general public in china: a cross-sectional study. BMJ Open. (2019) 9:e029638. doi: 10.1136/bmjopen-2019-029638
18. Wong FMF. Factors associated with knowledge, attitudes, and practice towards colorectal cancer and its screening among people aged 50–75 years. Int J Environ Res Public Health. (2021) 18:4100. doi: 10.3390/ijerph18084100
19. Aldukhayel AM, Alsudairi HA, Alhomidani RA, Almutairi NS, Alturki FM, Almehmadi RG, et al. Knowledge and attitude of primary healthcare physicians toward colorectal cancer screening in Qassim Region, Saudi Arabia. Int J Med Develop Count. (2021) 5:1784–90.
20. Demyati E. Knowledge, attitude, practice, and perceived barriers of colorectal cancer screening among family physicians in national guard health affairs, Riyadh. Int J Family Med. (2014) 2014:457354. doi: 10.1155/2014/457354
21. Mosli M, Alnahdi Y, Alghamdi A, Baabdullah M, Hadadi A, Khateery K, et al. Knowledge, attitude, and practices of primary health care physicians toward colorectal cancer screening. Saudi J Gastroenterol. (2017) 23:330–6. doi: 10.4103/sjg.SJG_1_17
22. White A, Ironmonger L, Steele RJC, Ormiston-Smith N, Crawford C, Seims A, et al. Review of sex-related differences in colorectal cancer incidence, screening uptake, routes to diagnosis, cancer stage and survival in the UK. BMC Cancer. (2018) 18:906. doi: 10.1186/s12885-018-4786-7
23. Lou L, Wang L, Zhang Y, Chen G, Lin L, Jin X, et al. Sex difference in incidence of gastric cancer: an international comparative study based on the global burden of disease study 2017. BMJ Open. (2020) 10:e033323. doi: 10.1136/bmjopen-2019-033323
24. Di L, Wu H, Zhu R, Li Y, Wu X, Xie R, et al. Multi-disciplinary team for early gastric cancer diagnosis improves the detection rate of early gastric cancer. BMC Gastroenterol. (2017) 17:147. doi: 10.1186/s12876-017-0711-9
25. Shen L, Zhou C, Liu L, Zhang L, Lu D, Cai J, et al. Application of oral contrast trans-abdominal ultrasonography for initial screening of gastric cancer in rural areas of China. Dig Liver Dis. (2017) 49:918–23. doi: 10.1016/j.dld.2017.04.008
26. Alghamdi AA, Almutairi AH, Aldosari FS, Al-Owayed AM, AlOtaibi HK, Alghamdi TA, et al. Knowledge, attitude, and practice of colorectal cancer screening among primary healthcare physicians in Riyadh second health cluster. Cureus. (2022) 14:e32069. doi: 10.7759/cureus.32069
27. Malek AI, Abdelbagi M, Odeh L, Alotaibi AT, Alfardan MH, Barqawi HJ. Knowledge, attitudes and practices of adults in the united arab emirates regarding helicobacter pylori induced gastric ulcers and cancers. Asian Pac J Cancer Prev. (2021) 22:1645–52. doi: 10.31557/APJCP.2021.22.5.1645
28. Holden CA, Frank O, Li M, Manocha R, Caruso J, Turnbull D, et al. Engagement of general practice in an Australian organised bowel cancer screening program: a cross-sectional survey of knowledge and practice. Asian Pac J Cancer Prev. (2020) 21:2099–107. doi: 10.31557/APJCP.2020.21.7.2099
29. Wang MY, Lin GZ Li Y, Dong H, Liao YH, Liu HZ, et al. Knowledge, attitudes, preventive practices and screening intention about colorectal cancer and the related factors among residents in Guangzhou, China. Asian Pac J Cancer Prev. (2017) 18:3217–23. doi: 10.22034/APJCP.2017.18.12.3217
30. Tahani B, Manesh SS. Knowledge, attitude and practice of dentists toward providing care to the geriatric patients. BMC Geriatr. (2021) 21:399. doi: 10.1186/s12877-021-02343-2
31. Al-Qerem W, Hammad A, Jarab A. M MS, Amawi HA, Ling J, et al. Knowledge, attitudes, and practice with respect to antibiotic use among pharmacy students: a cross-sectional study. Eur Rev Med Pharmacol Sci. (2022) 26:3408–18. doi: 10.26355/eurrev_202205_28834
32. Raina S. Assessment of knowledge, attitude, and practice in health care delivery. N Am J Med Sci. (2013) 5:249–50. doi: 10.4103/1947-2714.109226
Keywords: early gastrointestinal cancer, healthcare workers, knowledge, attitude, practice, cross-sectional study
Citation: Zhang H, Zhao C, Song C, Wu Y, Wei D and Li X (2023) Knowledge, attitude, and practice of healthcare workers on early gastrointestinal cancer in China. Front. Public Health 11:1191699. doi: 10.3389/fpubh.2023.1191699
Received: 22 March 2023; Accepted: 14 June 2023;
Published: 06 July 2023.
Edited by:
Kingston Rajiah, Ulster University, United KingdomReviewed by:
Jaiberth Antonio Cardona-Arias, University of Antioquia, ColombiaYin Zhu, The First Affiliated Hospital of Nanchang University, China
Copyright © 2023 Zhang, Zhao, Song, Wu, Wei and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiuqing Li, lxq19792003@126.com