 Islam Salikhanov
Islam Salikhanov Maria C. Katapodi
Maria C. Katapodi Gulnara Kunirova2‡
Gulnara Kunirova2‡ Byron L. Crape
Byron L. Crape
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Public Health, 03 August 2023
Sec. Public Health Policy
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1186107
This article is part of the Research TopicPublic Health Challenges in Post-Soviet Countries During and Beyond COVID-19View all 17 articles
Approximately 60 million people require palliative care worldwide, and nearly 80% of them live in low- and middle-income countries (LMICs). Providing palliative care in remote and rural areas of LMICs requires special consideration to ensure equitable access to healthcare. This perspective aims to deliver pragmatic, context-oriented policy recommendations designed to improve palliative care outcomes in Kazakhstan by capitalizing on existing resources and considering its unique geopolitical and sociocultural context. With approximately half of the population in Kazakhstan residing in remote and rural regions, the provision of healthcare services – specifically palliative care – mandates particular attention to ensure equal access to high-quality care. To understand challenges of implementing palliative care in remote and rural regions of Kazakhstan and to propose tailored solutions, 29 key stakeholders, including family caregivers, health professionals, and palliative care administrators, were identified in five regions of Kazakhstan. The main challenges encountered by family caregivers include lack of palliative care skills, the need for home-based care from mobile services, and high out-of-pocket expenditures. The challenges highlighted by healthcare providers and administrators were the lack of formal education in palliative care, shortage of opioids, and limited societal awareness and state support. Based on challenges elaborated from stakeholders and existing literature in palliative care and family caregiving, this perspective advocates against replicating the strategies implemented in high-income countries. Family caregivers play a critical role in implementing affordable and efficient palliative care in resource-limited settings. Enhancing their competencies through digital training and increasing access to palliative care services through mobile teams are tailored and localized solutions that address specific challenges in Kazakhstan. It is postulated that these recommendations may find utility in other LMICs, potentially benefiting nearly 48 million individuals who require these services.
WHO defines palliative care as an approach that enhances quality of life of patients and their families facing life-threatening illnesses (1). It aims to alleviate suffering through early identification, comprehensive assessment, and pain management, while also addressing physical, psychosocial, and spiritual problems (1). This care philosophy affirms life, accepting dying as a normal process, providing support for an active life until death, and extending support to the family throughout and after the patient’s illness (1). Approximately 60 million people need palliative care worldwide in 2020, and nearly 80% of them live in low- and middle-income countries (LMICs) (2–4). Despite growing demand, access to palliative care in LMICs remains limited. The demand for palliative care in LMICs is projected to double by 2060, yet these countries lack the necessary infrastructure to establish and distribute these services, especially in rural and remote areas (4, 5). According to the United Nations, 3 billion people worldwide who live in rural and remote areas face significant challenges such as poverty and limited access to healthcare and education, creating critical challenges for policymakers and development organizations (6). The Lancet Commission on the Value of Death suggested that strengthening palliative care services in LMICs requires comprehensive approaches that consider the unique challenges faced by communities in these settings and leverage innovative solutions to improve access to care (3).
Investing in palliative care in LMICs has the potential to improve health equity worldwide (2, 3). WHO estimates that only 14% of patients worldwide who need palliative care have access to such services, primarily in countries with more robust economies (7). This leads to an unequal distribution of suffering among patients and their families, especially among those who are economically disadvantaged, socially excluded, or reside in remote and rural regions. Palliative care in LMICs can improve the quality of life of patients and their family caregivers by increasing access to medications essential for pain and symptom management (8, 9). Studies in Kenya, India, and Bangladesh found that introducing palliative care services in rural districts led to long-term cost-savings, as patients received home- and community-based care, reducing the need for costly hospitalizations and other healthcare services (4, 10). Palliative care services can contribute to health equity by addressing the underlying social determinants of health, such as poverty, lack of access to services, and discrimination (6, 11). As the demand for palliative care in LMICs increases, it is important to identify tailored local solutions. Adopting the strategies and approaches of high-income countries is neither feasible nor sustainable due to limited resources and lack of healthcare infrastructure in LMICs.
There has been significant attention dedicated to the challenges faced by palliative care patients in remote regions. These challenges are well-documented in the literature, as evident in 30 systematic reviews published with the last 9 years, which emphasize the need to develop healthcare solutions tailored to LMICs (8, 12–38). However, there is significant lack of recommendations for the development of context-specific and tailored solutions suitable and sustainable for resource-limited nations (2, 3, 39). Despite the fact that the majority of palliative care patients in LMICs reside in remote rural areas, the literature lacks recommendations on how to address the distinct challenges they face within their unique cultural, economic, financial, and national contexts in LMICs (2, 3, 19).
The Lancet Commission on the Value of Death underscores the significant role of community healthcare workers in providing palliative care in remote and rural regions. However, even though this approach has demonstrated its effectiveness in higher income settings, it may not necessarily be feasible in LMICs due to shortages of workforce, funding, and infrastructure (2, 3, 22). Hence, there is a need to generate research-based insights that can foster the development of recommendations uniquely adapted to the conditions of these rural and remote settings, thereby, better serving the majority of palliative care patients in LMICs (2, 3, 22, 40). Therefore, this perspective aims to deliver pragmatic, context-oriented policy recommendations designed to improve palliative care outcomes in Kazakhstan by capitalizing on existing resources and considering its unique geopolitical and sociocultural context. While the Lancet Commission provides a broader framework for the development of healthcare solutions, this perspective provides context-specific, tailored recommendations that are solidly grounded in the challenges reported by stakeholders in resource-limited settings of Kazakhstan (2, 3).
Situated in Central Asia, Kazakhstan is a low-middle income country characterized by a unique geography that significantly impacts healthcare delivery. Spread across 2.7 million km2 with a sparse population of only seven individuals per km2, Kazakhstan’s vast and disperse demographic landscape presents considerable challenges to accessing health services, especially for the nine million inhabitants residing in remote and rural areas (41).1 This problem is notably acute in palliative care delivery, a burgeoning need fueled by the country’s demographic shift towards an increasingly aging population – a trend consistent with other LMICs (42). Despite an estimated 107,000 individuals currently requiring palliative care services, the resources remain scarce (4, 43). With only 45 physicians and 101 nurses serving 1,925 palliative care beds, the Quality of Death Index places Kazakhstan 50th out of 80 countries (44). As reported by the World Hospice Palliative Care Alliance, Kazakhstan’s palliative care system is only at a preliminary stage of integration into the healthcare system, indicating a pressing need for development to meet national requirements and international standards (4, 43). Since 2016, Kazakhstan implements ‘The Road Map of Palliative Care Development,’ a strategy outlining key steps for policy development, educational initiatives, and service implementation, all tailored to enhance palliative care services uniquely suited to the country’s context (45).
This perspective examines the challenges of developing palliative care services in Kazakhstan, as an example of developing such services in LMICs that are searching for affordable solutions to transform their own healthcare system. According to the Lancet Commission Report, lack of data hinders the evaluation of palliative care services in LMICs (3). Addressing this challenge requires research on stakeholder needs, i.e., family caregivers of terminal patients, healthcare providers, and policy makers (46, 47). This Perspective presents a comprehensive synthesis of challenges faced by key stakeholders in palliative care in Kazakhstan, and offers suggestions for improving palliative care outcomes in resource-limited and remote and rural settings. Our suggestions could be relevant to other LMICs in Central Asia beyond Kazakhstan.
We identified 29 key stakeholders in palliative care in Kazakhstan between August 2021 and April 2022, and assessed their needs regarding palliative care services, along with the challenges they encountered. Supplementary Table S1 provides a comprehensive overview of the demographic characteristics of our diverse group of stakeholders, which includes family caregivers, physicians, nurses, and administrators. Stakeholders were identified from three hospices and three cancer centers located in five different regions of Kazakhstan, spanning the northern, southern, and eastern parts of the country. Only one cancer center and two hospices were located in the major cities of Astana and Almaty, respectively. We assessed their needs and challenges through semi-structured interviews conducted in Russian (Supplementary Table S2). All participants were fluent in the language. Following data collection, we utilized a descriptive content analysis approach to identify the key challenges faced by palliative care stakeholders. Supplementary Table S3 contains representative quotes from participants across all stakeholder groups, illustrating the key insights that emerged during the interviews. The procedures adhered to the good research practice guidelines of the Medical Research Council (50). The Nazarbayev University Institutional Research Ethics Committee (IREC413/24052021) approved the study.
The key stakeholders comprised 12 adult family caregivers, 12 healthcare providers, and 5 administrators of palliative care services. Family caregivers assisted with palliative procedures (such as massage, hygiene, prevention of bedsores, etc.) for terminally ill cancer patients who had been receiving inpatient palliative care for at least 14 days. The healthcare providers, consisting of five physicians, five nurses, and two psychologists, each had a minimum of 3 years of experience in palliative care. Both family caregivers and healthcare providers were recruited from the same facilities. The administrators, who were employed by Non-Governmental Organizations (NGOs), frequently interacted with the Ministry of Health and participated in policymaking, each having a minimum of 5 years of experience in palliative care services.
Figure 1 summarizes the factors influencing family caregivers’ perceptions of palliative care, reflecting their understanding of the patients’ experiences and perceptions. This figure presents the challenges reported by family caregivers and further elaborated on by healthcare providers and administrators. The goal is to demonstrate that future policies and interventions should be tailored to address the factors negatively affecting perceptions about palliative care, such as inadequate referrals from healthcare providers. Reflecting on the roadmap for palliative care development in Kazakhstan, we outline specific challenges to providing palliative care in the country and suggest recommendations to address these issues (48).
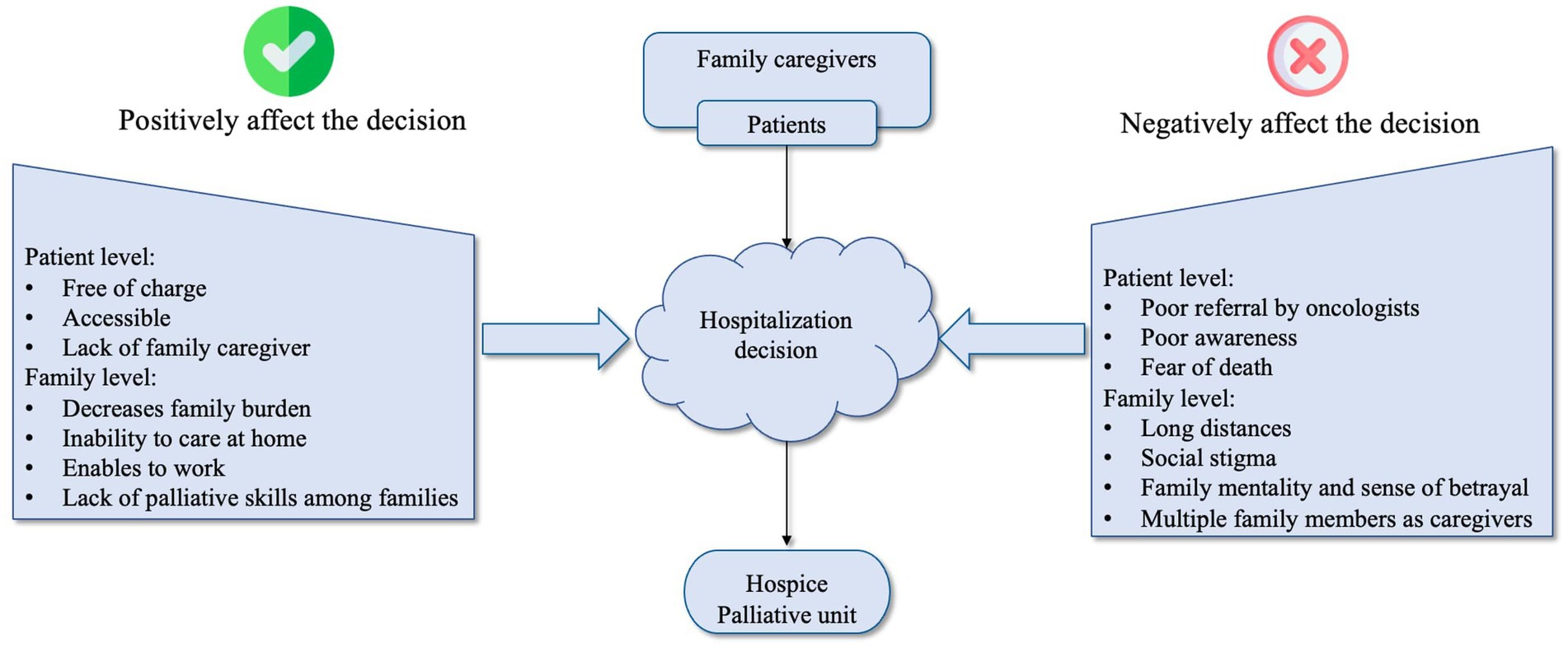
Figure 1. Factors associated with the decision to receive inpatient palliative care.
Palliative care services in Kazakhstan, encompassing both inpatient and outpatient settings, are heavily dependent on family caregivers. This is particularly the case in remote and rural areas where half of the population resides. However, most family caregivers lack the knowledge and practical skills related to patient care. Although nursing staff provide demonstrations of basic procedures in inpatient settings, these are very unsystematic. A terminal cancer diagnosis and the subsequent necessity for family caregiving often result in a significant loss of income for the entire family, either due to the patient’s inability to work or the family caregiver leaving their job to provide care. Most family caregivers favor home-based care and support from mobile teams over inpatient palliative care services. Home-based care would enable many of them, especially in remote and rural areas, to minimize long-distance travel to inpatient services, retain jobs, and minimize the loss of income for the entire family. However, mobile teams are largely unavailable, e.g., there is only one mobile team that covers the palliative care needs of Almaty, a city with a population of two million.
The lack of sufficient state funding and universal health coverage results in high out-of-pocket medical expenses, which consume a large portion of family income. This financial burden further exacerbates catastrophic health expenditures for families living in remote and rural areas and increases inequalities, with some families being able to afford more expensive treatment, equipment, and consumables than others.
The formal education of healthcare providers in palliative care is insufficient due to a shortage of academics and other teaching staff with expertise in this field. Only a small number of physicians and other healthcare providers have received training abroad through state-funded educational programs. The majority of training is acquired ‘on the job’, which often results in a poor understanding of the nature of palliative care. This issue is particularly impactful on the nursing workforce, where heavy workloads and unmet expectations can lead to burnout and a high turnover rate among new nurses. Remote and rural areas suffer disproportionately from these issues because trained specialists typically prefer to seek employment in larger cities rather than rural areas (2, 49).
The lack of formal education of healthcare providers in palliative care often leads to a fear of prescribing opioids (opiophobia) among physicians and oncologists (50, 51). In Kazakhstan, 95% of terminally ill patients suffer from severe pain at the end of their lives and do not have access to opioids (48). The problem has been exacerbated by increased government control in attempt to combat drug trafficking. Few medications are available for pain control, including only weak opioids and small amounts of oral morphine, making access to pain medication difficult in remote and rural areas. This leads to many avoidable hospitalizations as patients are forced to be admitted to a hospice or palliative unit to receive opioids.
A general lack of awareness about palliative care within the broader population presents another barrier to the development and delivery of effective services. Misunderstandings about the role of palliative care often create false expectations that patients will receive curative treatment. These unmet expectations can lead to stigmatization of palliative care services and foster anger and hostility towards healthcare providers. This issue is exacerbated in remote and rural areas where healthcare awareness is generally lower. The absence of robust and comprehensive policies and regulations regarding palliative care in Kazakhstan has led to the development of these services without active governmental involvement. As a result, palliative care often remains unincorporated into existing healthcare systems, leading to issues such as a lack of accountability, insufficient quality control, and limited availability and accessibility of palliative services (7). Stakeholders suggest that the key to further developing palliative care involves enhancing cooperation between stakeholders and the government, as well as garnering increased support from governmental organizations.
Palliative care in Kazakhstan is currently delivered in various settings, such as hospices, palliative units of cancer centers, sparse mobile teams, and single palliative beds in general hospitals (48). The understanding of, and approach to, palliative care varies greatly across these settings. To address the establishment and expansion of palliative care in Kazakhstan, both horizontal and vertical integration of the existing diverse services should be implemented (Figure 2).
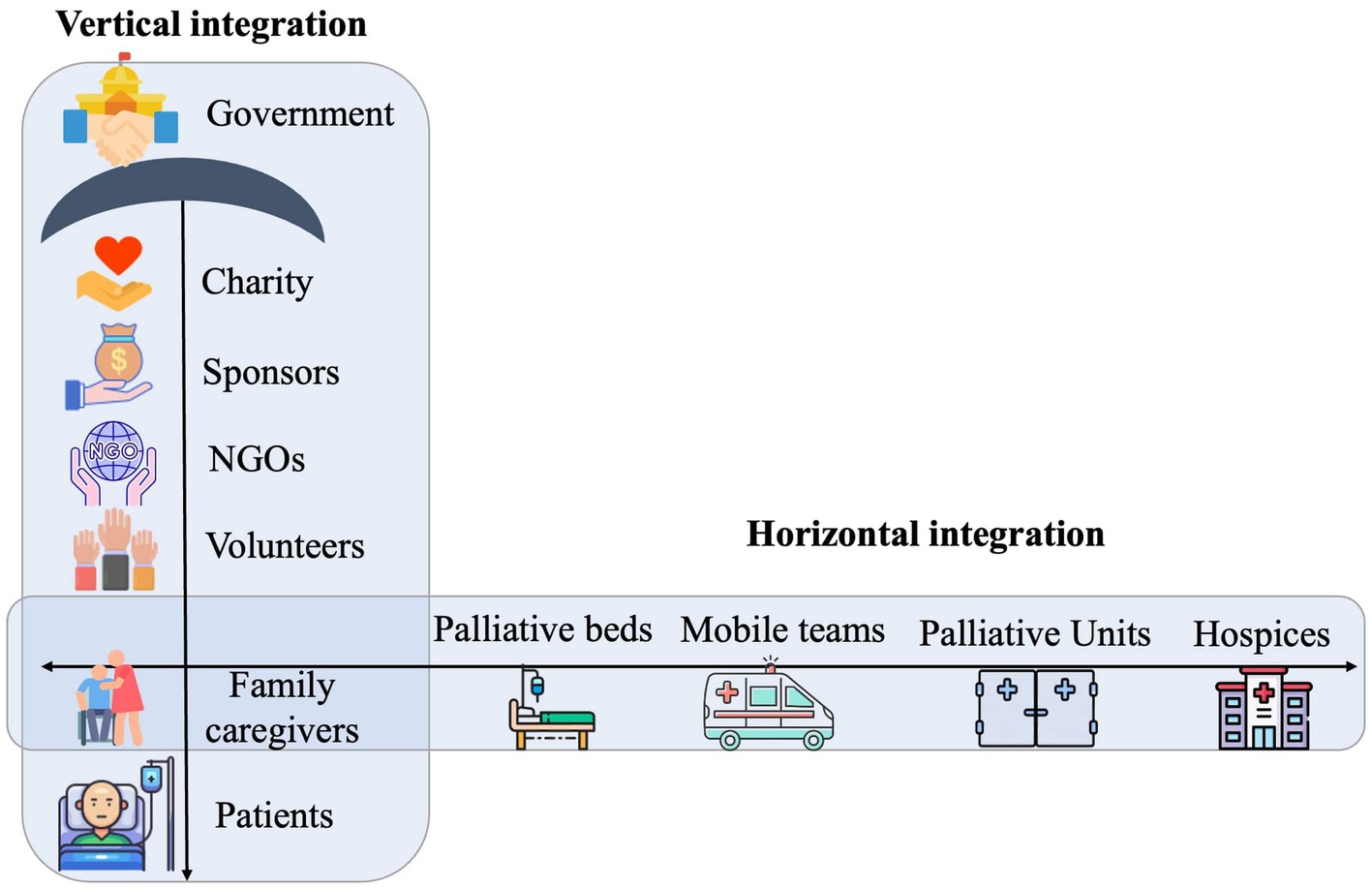
Figure 2. Vertical and horizontal integration of palliative care services.
Horizontal integration aims for the standardization and consistency of palliative care delivery across different settings such as mobile teams, hospices, and palliative care units. This would include a uniform approach to medical procedures, pain and symptom management, medication availability, spiritual patient support, and comprehensive family caregiver assistance, which encompasses skills training, psychosocial support, and grief counseling.
For instance, out of 1,900 palliative beds in the country, 1,100 are single beds scattered across various units (e.g., general therapy, pulmonology) and dispersed over a vast geographical area. Data on these single palliative beds is scarce, making it challenging to understand the differences and effectiveness of these services. Implementing horizontal integration could involve redistributing these single beds into newly established hospices or increasing the number of mobile units, with the aim of achieving a consistent understanding and practice of palliative care across all settings. The focus should be on creating or maintaining a homelike environment with significant family caregiver involvement.
Vertical integration, on the other hand, refers to a hierarchical structure of palliative care stakeholders and parties involved, with the government taking the leading role in policymaking (as shown on p.37 of the Global Atlas of Palliative Care) (4). The government would form a policy umbrella over other parties involved, such as NGOs, charities, and volunteers. Vertical integration could enable smoother policymaking and more clearly defined roles in palliative care management and decision making. In Kazakhstan’s current palliative care scenario these roles are not well defined, while NGOs often assume a leading role in palliative care policy and funding. The absence of the Ministry of Health as a major stakeholder is a limitation of this perspective, considering its crucial role as a primary healthcare stakeholder with responsibilities in shaping policies and distributing resources.
Improving family caregivers’ competencies through training and expanding access to palliative care via home-based mobile services can be both financially feasible and cost-effective, especially in remote and rural areas of Kazakhstan and potentially other LMICs. Home-based care not only reduces costs compared to inpatient care but also enhances patient outcomes by increasing access to essential care and reducing hospitalizations (52). Increasing the number of mobile teams would also help address disparities in accessing these services in remote and rural areas, where traditional healthcare facilities may be limited or non-existent (9, 40, 52). Given that the majority of palliative patients in Kazakhstan are cared for by their families, equipping family caregivers with proper training can support them in delivering high-quality home-based care. This approach not only lessens the burden and financial strain associated with terminal disease but also ensures optimal use of scarce resources at both family and societal levels (53). Training programs could focus on enhancing caregivers’ knowledge and self-efficacy in basic palliative care procedures, such as hygiene and feeding, while also offering resources to support them psychologically and address caregiver burden (54, 55). Guided by mobile teams, trained caregivers will be more capable of managing pain, preventing bedsores, and addressing other symptoms. Leveraging the surge of digital technologies in the post-Covid-19 era, online and m-Health courses could reach family caregivers even in remote and rural areas of Kazakhstan and other LMICs (56, 57).
The literature extensively emphasizes the importance of family caregiver training and support, particularly in LMICs (3, 53–56, 58–62). Family caregivers are acknowledged as integral to long-term care, and all health professionals are encouraged to incorporate them into care teams and provide enhanced support to families (63).2 The growing body of evidence underscores the need to address the challenges faced by family caregivers in these contexts, thus reinforcing our recommendations for enhancing competencies and implementing comprehensive programs for family caregivers in Kazakhstan (3). The sense of coherence, rituals, traditions, and long-term mutual support that families and communities provide to the dying or grieving cannot be replaced by healthcare professionals (3). Education platforms for family caregivers have already demonstrated the feasibility of achieving significant enhancement in the well-being of patients and their families (64, 65). In rural and remote areas, family caregivers struggle with inadequate healthcare infrastructure and, even more, with a shortage of qualified healthcare personnel. Therefore, they should be given particular attention in the context of palliative training (66). In 2017, it was estimated that in the US alone, 41 million family caregivers provided 34 billion hours of care, corresponding to an economic value of $470 billion (63). Given these estimates and that palliative care relies heavily on family caregivers in Kazakhstan, our recommendation for supporting and training them becomes imperative for LMICs.
Increased opportunities to educate healthcare providers and access to pain medication are interconnected key components of the horizontal integration of palliative services, promoting a consistent approach to care delivery in different contexts of remote and rural regions (67). Training in palliative care would help minimize variations in care provision, enabling uniform approach to effective use of medication for pain management, symptom control, and psychosocial support across all settings. By integrating pain management into the horizontal axis of palliative care services, healthcare providers can ensure that patients receive the care they need regardless of their geographic location or socioeconomic status. This entails streamlining bureaucratic procedures related to the import and distribution of pain medications to reduce delays and ensure their availability.
Local production of pain medications could lower costs and lessen the disproportionate economic impact of fluctuating exchange rates on LMICs. The successful implementation of strategies for affordable local morphine production in Uganda in 2003 exemplifies the importance of promoting local production of pain medication. This strategy significantly improves the quality of life of patients and family caregivers and remains affordable for LMICs (68).3 In Uganda, the cost of 110 days of pain management with oral morphine equals the price of a loaf of bread, thereby providing essential pain relief and ensuring a satisfactory quality of life for all palliative patients until death (68). The Kazakhstan Association of Palliative Care successfully engaged the Ministry of Health and the Police Department to facilitate a five-fold increase in the availability of fentanyl patches. This accomplishment underscores the importance of advocacy and collaboration in addressing the country’s palliative care needs. Annual awareness-raising campaigns organized by the Kazakhstan Association of Palliative Care, supported by hospices, hospital units, physician organizations, and NGOs, attract hundreds of volunteers and generate considerable social media attention. These campaigns advocate for an integrated approach to palliative care, emphasizing its long-term societal benefits (69).4
Our recommendations, based on the unique challenges and needs of LMICs, prioritize the efficient use of available resources. In this perspective, we argue against adopting a universal approach that merely replicates the expensive strategies of high-income countries, as it is neither sustainable nor advisable. Instead, we endorse the adoption of more nuanced, tailored, and context-specific approaches. Some specific practices, interventions, and policies prevalent in high-income countries (HICs) might be adaptable or translatable for palliative care interventions in LMICs. These may include:
Low-cost medications: some HICs use expensive medications for symptom management. In LMICs, affordable, generic, and essential medications should be prioritized, and alternative treatments that are more accessible should be explored.
Nonspecialized workforce: HICs often have a specialized workforce dedicated to palliative care. In LMICs, training non-specialist healthcare providers such as primary care providers and nurses in palliative care principles may be more feasible and sustainable, enabling them to provide care within their communities with the assistance of family caregivers.
Basic infrastructure: HICs may have specialized facilities for end-of-life care. In LMICs, integrating palliative care services into existing hospices or developing home-based services may be a more feasible approach, especially with the assistance of family caregivers.
Integrated care systems: some HICs have multiple uncoordinated palliative care providers. In LMICs, it is vital to develop a coordinated, collaborative approach that engages all stakeholders in optimizing resources and ensuring continuity of care. Creating a centralized system that connects healthcare providers, NGOs, and government agencies can help coordinate and optimize resources and ensure more efficient care provision.
Replicating strategies of HICs could lead to the misallocation of scarce resources and the introduction of policies that do not resonate with local populations’ needs, thereby hindering the development of palliative care services in LMICs (70, 71). The insights gained from the current advancements in palliative care in Kazakhstan present invaluable lessons about the challenges and opportunities inherent in developing such services in other LMICs. These insights highlight the importance of crafting local solutions to cater to the unique needs of these populations, with family caregivers as an integral part of these solutions.
Target 3.8 of the United Nations Sustainable Development Goals underlines the objective of attaining universal health coverage by 2030, which includes access to crucial health services and protection from financial risks (72).5 However, the realization of universal health coverage is unattainable without palliative care. Despite the evidence-based nature of this perspective, we intentionally focused on formulating tailored policy recommendations in response to the well-documented challenges. By highlighting these key challenges and recommendations, this perspective can provide guidance to health authorities and policymakers in LMICs striving to improve palliative care within their communities. A shift towards community-based care can reduce healthcare costs, improve patients’ access to care – especially those who might otherwise lack it – and enhance the overall well-being and quality of life of remote and rural communities in LMICs.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Nazarbayev University Institutional Research Ethics Committee (IREC413/24052021). The patients/participants provided their written informed consent to participate in this study.
IS conceived and designed the analysis, collected the data, analyzed the data, and wrote the paper. MK conceived and designed the analysis, contributed data and analysis tools, and wrote the paper. GK collected the data and wrote the paper. BC conceived and designed the analysis and wrote the paper. All authors contributed to the article and approved the submitted version.
This project has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 801076 for IS, and Swiss Cancer League KLS-4294-08-2017, PI: MK for the CASCADE study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1186107/full#supplementary-material
1. ^https://data.worldbank.org/indicator/EN.POP.DNST?end=2020&locations=KZ&start=1961&view=chart
2. ^http://resource.nlm.nih.gov/101767885
3. ^https://www.hospice-africa.org/uganda/
4. ^https://www.thewhpca.org/events-2021/item/1750-meters-above-sea-level-whpcday21-in-almaty
5. ^https://unstats.un.org/sdgs/metadata/?Text=&Goal=3&Target=3.8
1. Integrating palliative care and symptom relief into primary health care: a WHO guide for planners, implementers and managers. Geneva: World Health Organization (2018) Licence: CC BY-NC-SA 3.0 IGO.
2. Knaul, FM, Farmer, PE, Krakauer, EL, De Lima, L, Bhadelia, A, Jiang Kwete, X, et al. Alleviating the access abyss in palliative care and pain relief – an imperative of universal health coverage: the lancet commission report. 391, Lancet. Lancet Publishing Group; (2018). 1391–1454. doi: 10.1016/S0140-6736(17)32513-8
3. Sallnow, L, Smith, R, Ahmedzai, SH, Bhadelia, A, Chamberlain, C, Cong, Y, et al. Report of the lancet commission on the value of death: bringing death back into life. Lancet. (2022) 399:837. doi: 10.1016/S0140-6736(21)02314-X
4. Connor, SR, Morris, C, and Jaramillo, E. Global atlas of palliative care 2nd edition global atlas of palliative care at the end of life global atlas of palliative care. 2nd ed (2020) Available at: www.thewhpca.org.
5. Sleeman, KE, de Brito, M, Etkind, S, Nkhoma, K, Guo, P, Higginson, IJ, et al. The escalating global burden of serious health-related suffering: projections to 2060 by world regions, age groups, and health conditions. Lancet Glob Health. (2019) 7:e883–92. doi: 10.1016/S2214-109X(19)30172-X
6. Bukhman, G, Mocumbi, AO, Atun, R, Becker, AE, Bhutta, Z, Binagwaho, A, et al. The lancet NCDI poverty commission: bridging a gap in universal health coverage for the poorest billion. 396, Lancet. Lancet Publishing Group; (2020). 991–1044. doi: 10.1016/S0140-6736(20)31907-3
7. Poudel, A, Kc, B, Shrestha, S, and Nissen, L. Access to palliative care: discrepancy among low-income and high-income countries. J Glob Health. (2019) 9:20309. doi: 10.7189/jogh.09.020309
8. Potts, M, Cartmell, KB, Nemeth, L, Bhattacharjee, G, and Qanungo, S. A systematic review of palliative care intervention outcomes and outcome measures in low-resource countries. 55, J Pain Symptom Manag. Elsevier Inc.; (2018). 1382–1397e7. doi: 10.1016/j.jpainsymman.2017.12.487
9. Biswas, J, Faruque, M, Banik, PC, Ahmad, N, and Mashreky, SR. Quality of life of the cancer patients receiving home-based palliative care in Dhaka city of Bangladesh. PLoS One. (2022) 17:e0268578. doi: 10.1371/journal.pone.0268578
10. Reid, EA, Kovalerchik, O, Jubanyik, K, Brown, S, Hersey, D, and Grant, L. Is palliative care cost-effective in low-income and middle-income countries? A mixed-methods systematic review. BMJ Support Palliat Care. (2019) 9:120–9. doi: 10.1136/bmjspcare-2018-001499
11. Brant, JM, and Silbermann, M. Global perspectives on palliative care for cancer patients: not all countries are the same. Curr Oncol Rep. (2021) 23:60. doi: 10.1007/s11912-021-01044-8
12. Li, WW, Chhabra, J, and Singh, S. Palliative care education and its effectiveness: a systematic review. 194, Public Health, Elsevier B.V.; (2021). 96–108. doi: 10.1016/j.puhe.2021.02.033
13. Ohinata, H, Aoyama, M, and Miyashita, M. Complexity in the context of palliative care: a systematic review. 11, Ann Palliative Med. AME Publishing Company; (2022). 3231–3246. doi: 10.21037/apm-22-623
14. Phongtankuel, V, Meador, L, Adelman, RD, Roberts, J, Henderson, CR, Mehta, SS, et al. Multicomponent palliative care interventions in advanced chronic diseases: a systematic review. 35, Am J Hospice Palliative Med. SAGE Publications Inc.; (2018). 173–183. doi: 10.1177/1049909116674669
15. Reigada, C, Pais-Ribeiro, JL, Novella, A, and Gonçalves, E. The caregiver role in palliative care: a systematic review of the literature. Health Care Curr Rev. (2015) 03:1000143. doi: 10.4172/2375-4273.1000143
16. Chi, NC, and Demiris, G. A systematic review of telehealth tools and interventions to support family caregivers. J Telemed Telecare. (2015) 21:37–44. doi: 10.1177/1357633X14562734
17. Gabriel, I, Creedy, D, and Coyne, E. A systematic review of psychosocial interventions to improve quality of life of people with cancer and their family caregivers. Nurs Open. (2020) 7:1299–312. doi: 10.1002/nop2.543
18. Wang, T, Molassiotis, A, and Chung, BPM. Unmet care needs of advanced cancer patients and their informal caregivers: a systematic review. BMC Palliat Care. (2018) 17:96. doi: 10.1186/s12904-018-0346-9
19. Suntai, Z, Won, CR, and Noh, H. Access barrier in rural older adults’ use of pain management and palliative care services: a systematic review. Am J Hosp Palliat Care. (2021) 38:494–502. doi: 10.1177/1049909120959634
20. Cruz-Oliver, DM, Pacheco Rueda, A, Viera-Ortiz, L, Washington, KT, and Oliver, DP. The evidence supporting educational videos for patients and caregivers receiving hospice and palliative care: a systematic review. Patient Educ Couns. (2020) 103:1677–91. doi: 10.1016/j.pec.2020.03.014
21. Mulcahy Symmons, S, Ryan, K, and Aoun, SM. Decision-making in palliative care: patient and family caregiver concordance and discordance-systematic review and narrative synthesis [published online ahead of print, 2022 mar 22]. BMJ Support Palliat Care. (2022) 2022:003525. doi: 10.1136/bmjspcare-2022-003525
22. Rainsford, S, MacLeod, RD, Glasgow, NJ, Phillips, CB, Wiles, RB, and Wilson, DM. Rural end-of-life care from the experiences and perspectives of patients and family caregivers: a systematic literature review. Palliat Med. (2017) 31:895–912. doi: 10.1177/0269216316685234
23. Gonella, S, Basso, I, De Marinis, MG, Campagna, S, and Di Giulio, P. Good end-of-life care in nursing home according to the family carers' perspective: a systematic review of qualitative findings. Palliat Med. (2019) 33:589–606. doi: 10.1177/0269216319840275
24. Abu-Odah, H, Molassiotis, A, and Liu, J. Challenges on the provision of palliative care for patients with cancer in low- and middle-income countries: a systematic review of reviews. BMC Palliat Care. (2020) 19:55. doi: 10.1186/s12904-020-00558-5
25. Bennardi, M, Diviani, N, and Gamondi, C. Palliative care utilization in oncology and hemato-oncology: a systematic review of cognitive barriers and facilitators from the perspective of healthcare professionals, adult patients, and their families. BMC Palliat Care. (2020) 19:47. doi: 10.1186/s12904-020-00556-7
26. Rainsford, S, MacLeod, RD, and Glasgow, NJ. Place of death in rural palliative care: a systematic review. Palliat Med. (2016) 30:745–63. doi: 10.1177/0269216316628779
27. González-Fraile, E, Ballesteros, J, Rueda, JR, Santos-Zorrozúa, B, Solà, I, and McCleery, J. Remotely delivered information, training and support for informal caregivers of people with dementia. Cochrane Database Syst Rev. (2021) 1:CD006440. doi: 10.1002/14651858.CD006440.pub3
28. Rosa, WE, Ferrell, BR, and Mazanec, P. Global integration of palliative nursing education to improve health crisis preparedness. J Contin Educ Nurs. (2021) 52:130. doi: 10.3928/00220124-20210216-07
29. Ahn, S, Romo, RD, and Campbell, CL. A systematic review of interventions for family caregivers who care for patients with advanced cancer at home. Patient Educ Couns. (2020) 103:1518. doi: 10.1016/j.pec.2020.03.012
30. McCauley, R, McQuillan, R, Ryan, K, and Foley, G. Mutual support between patients and family caregivers in palliative care: a systematic review and narrative synthesis. Palliat Med. (2021) 35:875. doi: 10.1177/0269216321999962
31. MacRae, MC, Fazal, O, and O'Donovan, J. Community health workers in palliative care provision in low-income and middle-income countries: a systematic scoping review of the literature. BMJ Glob Health. (2020) 5:e002368. doi: 10.1136/bmjgh-2020-002368
32. Kavalieratos, D, Corbelli, J, Zhang, D, Dionne-Odom, JN, Ernecoff, NC, Hanmer,, et al. Association between palliative care and patient and caregiver outcomes: a systematic review and meta-analysis. JAMA. (2016) 316:2104–14. doi: 10.1001/jama.2016.16840
33. Mou, H, Wong, MS, and Prof, CWT. Effectiveness of dyadic psychoeducational intervention for stroke survivors and family caregivers on functional and psychosocial health: a systematic review and meta-analysis. Int J Nurs Stud. (2021) 120:103969. doi: 10.1016/j.ijnurstu.2021.103969
34. Leng, M, Zhao, Y, Xiao, H, Li, C, and Wang, Z. Internet-based supportive interventions for family caregivers of people with dementia: systematic review and meta-analysis. J Med Internet Res. (2020) 22:e19468. doi: 10.2196/19468
35. Farina, N, Page, TE, Daley, S, Brown, A, Bowling, A, Basset, T, et al. Factors associated with the quality of life of family carers of people with dementia: a systematic review. Alzheimers Dement. (2017) 13:572–81. doi: 10.1016/j.jalz.2016.12.010
36. Chi, NC, Barani, E, Fu, YK, Nakad, L, Gilbertson-White, S, Herr, K, et al. Interventions to support family caregivers in pain management: a systematic review. J Pain Symptom Manag. (2020) 60:630–656.e31. doi: 10.1016/j.jpainsymman.2020.04.014
37. Monteiro, AMF, Santos, RL, Kimura, N, Baptista, MAT, and Dourado, MCN. Coping strategies among caregivers of people with Alzheimer disease: a systematic review. Trends Psychiatr Psychother. (2018) 40:258–68. doi: 10.1590/2237-6089-2017-0065
38. Reid, E, Ghoshal, A, Khalil, A, Jiang, J, Normand, C, Brackett, A, et al. Out-of-pocket costs near end of life in low- and middle-income countries: a systematic review. PLoS Glob Public Health. (2022) 2:5. doi: 10.1371/journal.pgph.0000005
39. O'Brien, V, Jenkins, LS, Munnings, M, Grey, H, North, Z, Schumann, H, et al. Palliative care made visible: developing a rural model for the Western Cape Province, South Africa. Afr J prim health care. Fam Med. (2019) 11:e1–e11. doi: 10.4102/phcfm.v11i1.2147
40. Bakitas, M, Allen Watts, K, Malone, E, Dionne-Odom, JN, McCammon, S, Taylor, R, et al. Forging a new frontier: providing palliative care to people with cancer in rural and remote areas. J Clin Oncol. (2020) 38:963–73. doi: 10.1200/JCO.18.02432
41. The World Bank. Population density – Kazakhstan. (2020). Available at: https://data.worldbank.org/indicator/EN.POP.DNST?end=2020&locations=KZ&start=1961&view=chart
42. Arkhangelsky, V, Denisenko, M, Elizarov, V, Zhusupov, B, and Moldakulova, G. Population analysis of the Republic of Kazakhstan. (2019). Available at: https://kazakhstan.unfpa.org
43. Finkelstein, EA, Bhadelia, A, Goh, C, Baid, D, Singh, R, Bhatnagar, S, et al. Cross country comparison of expert assessments of the quality of death and dying 2021. J Pain Symptom Manag. (2022) 63:e419–29. doi: 10.1016/j.jpainsymman.2021.12.015
45. Callaway, MV, Connor, SR, and Foley, KM. World Health Organization public health model: a roadmap for palliative care development. J Pain Symptom Manag. (2018) 55:S6–S13. doi: 10.1016/j.jpainsymman.2017.03.030
46. Nkhoma, KB, Ebenso, B, Akeju, D, Adejoh, S, Bennett, M, Chirenje, M, et al. Stakeholder perspectives and requirements to guide the development of digital technology for palliative cancer services: a multi-country, cross-sectional, qualitative study in Nigeria, Uganda and Zimbabwe. BMC Palliat Care. (2021) 20:4. doi: 10.1186/s12904-020-00694-y
47. Xiao, J, Brenneis, C, and Fassbender, K. Stakeholder perspectives towards implementing the national framework on palliative care in Canada. Health Policy. (2022) 126:576–83. doi: 10.1016/j.healthpol.2022.01.011
48. Kunirova, G, and Shakenova, A. Palliative Care in Kazakhstan. J Pain Symptom Manag. (2018) 55:S36–40. doi: 10.1016/j.jpainsymman.2017.03.028
49. Lalani, N, and Cai, Y. Palliative care for rural growth and wellbeing: identifying perceived barriers and facilitators in access to palliative care in rural Indiana. BMC Palliat Care. (2021) 21:25. doi: 10.1186/s12904-022-00913-8
50. Berterame, S, Erthal, J, Thomas, J, Fellner, S, Vosse, B, Clare, P, et al. Use of and barriers to access to opioid analgesics: a worldwide, regional, and national study. Lancet. (2016) 387:1644–56. doi: 10.1016/S0140-6736(16)00161-6
51. International narcotics control board. Report of the international narcotics control board on the availability of internationally controlled drugs: Ensuring adequate access for medical and scientific purposes. United Nations; (2011). 74.
52. McCaffrey, N, Agar, M, Harlum, J, Karnon, J, Currow, D, and Eckermann, S. Is home-based palliative care cost-effective? An economic evaluation of the palliative care extended packages at home (PEACH) pilot. BMJ Support Palliat Care. (2013) 3:431–5. doi: 10.1136/bmjspcare-2012-000361
53. Hudson, P, and Aranda, S. The Melbourne family support program: evidence-based strategies that prepare family caregivers for supporting palliative care patients. BMJ Support Palliat Care. (2014) 4:231–7. doi: 10.1136/bmjspcare-2013-000500
54. Kristanti, MS, Setiyarini, S, and Effendy, C. Enhancing the quality of life for palliative care cancer patients in Indonesia through family caregivers: a pilot study of basic skills training. BMC Palliat Care. (2017) 16:4. doi: 10.1186/s12904-016-0178-4
55. Kirkpatrick, AJ, Donesky, D, and Kitko, LA. A systematic review of Interprofessional palliative care education programs. J Pain Symptom Manag. (2023) 65:e439–66. doi: 10.1016/j.jpainsymman.2023.01.022
56. Blusi, M, Dalin, R, and Jong, M. The benefits of e-health support for older family caregivers in rural areas. J Telemed Telecare. (2014) 20:63–9. doi: 10.1177/1357633X13519901
57. Pleasant, M, Molinari, V, Dobbs, D, Meng, H, and Hyer, K. Effectiveness of online dementia caregivers training programs: a systematic review. Geriatr Nurs. (2020) 41:921–35. doi: 10.1016/j.gerinurse.2020.07.004
58. Yang, L. Family caregivers’ experiences of interaction with people with mild-to-moderate dementia in China: a qualitative study. (2020)
59. Basnyat, I, and Chang, L. Tensions in support for family caregivers of people with dementia in Singapore: a qualitative study. Dementia. (2021) 20:2278–93. doi: 10.1177/1471301221990567
60. Barlund, AS, André, B, Sand, K, and Brenne, AT. A qualitative study of bereaved family caregivers: feeling of security, facilitators and barriers for rural home care and death for persons with advanced cancer. BMC Palliat Care. (2021) 20:7. doi: 10.1186/s12904-020-00705-y
61. Mei, YX, Lin, B, Zhang, W, Yang, DB, Wang, SS, Zhang,, et al. Benefits finding among Chinese family caregivers of stroke survivors: a qualitative descriptive study. BMJ Open. (2020) 10:e038344. doi: 10.1136/bmjopen-2020-038344
62. Sakanashi, S, Fujita, K, and Konno, R. Components of empowerment among family caregivers of community-dwelling people with dementia in Japan: a qualitative research study. J Nurs Res. (2021) 29:e155. doi: 10.1097/JNR.0000000000000430
63. Reinhard, SC, Feinberg, LF, Houser, A, Choula, R, and Evans, M. Valuing the invaluable: 2019 update – AARP insight on the issues. (2015). Available at: http://resource.nlm.nih.gov/101767885
64. Griffiths, PC, Kovaleva, M, Higgins, M, Langston, AH, and Hepburn, K. Tele-savvy: an online program for dementia caregivers. Am J Alzheimers Dis Other Dement. (2018) 33:269–76. doi: 10.1177/1533317518755331
65. Rodriguez, K, Fugard, M, Amini, S, Smith, G, Marasco, D, Shatzer, J, et al. Caregiver response to an online dementia and caregiver wellness education platform. J Alzheimers Dis Rep. (2021) 5:433–42. doi: 10.3233/ADR-200292
66. Haier, J, Sleeman, J, and Schäfers, J. Editorial series: cancer care in low- and middle-income countries. Clin Exp Metastasis. (2019) 36:477–80. doi: 10.1007/s10585-019-10003-4
67. Bassah, N, Seymour, J, and Cox, K. A modified systematic review of research evidence about education for pre-registration nurses in palliative care. BMC Palliat Care. (2014) 13:56. doi: 10.1186/1472-684X-13-56
68. Merriman, Anne. Hospice Africa Uganda. Available at: https://www.hospice-africa.org/uganda/
69. Kunirova, Gulnara. World Hospice & Palliative Care day in Kazakhstan. (2021). Available at: https://www.thewhpca.org/events-2021/item/1750-meters-above-sea-level-whpcday21-in-almaty
70. Puchalski, LM, Khan, S, Moore, JE, Timmings, C, van Lettow, M, and Vogel, JP. Evidence products. J Clin Epidemiol. (2016) 76:229–37. doi: 10.1016/j.jclinepi.2016.02.017
71. Olufadewa, I, Adesina, M, and Ayorinde, T. Global health in low-income and middle-income countries: a framework for action. Lancet Glob Health. (2021) 9:e899–900. doi: 10.1016/S2214-109X(21)00143-1
72. United Nations. SDG indicator metadata. (2021); Available at: https://unstats.un.org/sdgs/metadata/?Text=&Goal=3&Target=3.8
Keywords: palliative care, stakeholders, challenges, family caregivers, LMICs
Citation: Salikhanov I, Katapodi MC, Kunirova G and Crape BL (2023) Improving palliative care outcomes in remote and rural areas of LMICs through family caregivers: lessons from Kazakhstan. Front. Public Health. 11:1186107. doi: 10.3389/fpubh.2023.1186107
Edited by:
Natalya Glushkova, Al-Farabi Kazakh National University, KazakhstanReviewed by:
Narelle Warren, Monash University, AustraliaCopyright © 2023 Salikhanov, Katapodi, Kunirova and Crape. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Islam Salikhanov, aXNsYW0uc2FsaWtoYW5vdkB1bmliYXMuY2g=
†These authors share first authorship
‡ORCID: Islam Salikhanov, https://orcid.org/0000-0002-0437-3125
Maria C. Katapodi, https://orcid.org/0000-0003-3903-3750
Gulnara Kunirova, https://orcid.org/0000-0001-5501-7174
Byron L. Crape, https://orcid.org/0000-0002-4663-1874
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.