 Shou Liu
Shou Liu Fei Wang
Fei Wang Sha Sha3†
Sha Sha3† Hong Cai
Hong Cai Chee H. Ng
Chee H. Ng Yuan Feng
Yuan Feng Yu-Tao Xiang
Yu-Tao Xiang- 1Department of Public Health, Medical College, Qinghai University, Xining, Qinghai, China
- 2Guangdong Mental Health Center, Guangdong Provincial People's Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, Guangdong, China
- 3Beijing Key Laboratory of Mental Disorders, The National Clinical Research Center for Mental Disorders, Beijing Anding Hospital, The Advanced Innovation Center for Human Brain Protection, Capital Medical University, Beijing, China
- 4Unit of Psychiatry, Department of Public Health and Medicinal Administration, Institute of Translational Medicine, Faculty of Health Sciences, University of Macau, Macau, China
- 5Centre for Cognitive and Brain Sciences, University of Macau, Macau, China
- 6Department of Psychiatry, The Melbourne Clinic and St Vincent's Hospital, University of Melbourne, Richmond, VIC, Australia
Background: High altitude is known to have a significant impact on human physiology and health, therefore, understanding its relationship with quality of life is an important research area. This study compared the quality of life (QOL) in older adults living in high and low altitude areas, and examined the independent correlates of QOL in those living in a high altitude area.
Methods: Older adults living in three public nursing homes in Xining (high altitude area) and one public nursing home in Guangzhou (low altitude area) were recruited. The WHOQOL-BREF was used to measure the QOL.
Results: 644 older adults (male: 39.1%) were included, with 207 living in high altitude and 437 living in low altitude areas. After controlling for the covariates, older adults living in the high altitude area had higher QOL in terms of physical (P = 0.035) and social domains (P = 0.002), but had lower QOL in psychological (P = 0.009) domain compared to their counterparts living in the low altitude area. For older adults living in the high altitude area, smoking status was associated with higher social QOL (P = 0.021), good financial status was associated with higher physical QOL (P = 0.035), and fair or good health status was associated with higher physical (p < 0.001) and psychological QOL (P = 0.046), while more severe depressive symptoms were associated with lower QOL.
Conclusion: Appropriate interventions and support to improve depressive symptoms and both financial and health status should be developed for older adults living in high altitude areas to improve their QOL.
Introduction
Quality of life (QOL) is a widely used health outcome with multiple dimensions that involve subjective sense of mental and physical status, social roles and functioning, personal relationships, and environmental factors (1). Among different age groups, QOL in older adults is a topic of concern (2). During the past decade, the research on QOL in older adults has mainly focused on its relationships with impairments of body function (3), physical and mental illnesses (4), cognitive deficits (5), and increased social and economic burden (6).
Previous studies found that unhealthy lifestyle factors (e.g., heavy smoking and drinking) were associated with lowered QOL (7–10) that was moderated by impaired physical (11, 12) and mental health status (13, 14). In addition, cognitive impairment was common among older adults living in high altitude areas, which was not associated with QOL in this population (5). In contrast, the influence of certain environmental factors on QOL is relatively less well-understood or studied. Living at high altitude has well-known impacts on health status due to hypobaric hypoxia in high-altitude areas for both local residents and those who recently arrived (15, 16). Some studies found that genetic factors in long-term high altitude residents could play a role in adapting to their local environment better than those living in other areas (17–21). Further, other studies examined the direct impact of high altitude on health including the influence of living in moderate altitude areas on the reproductive function (22), metabolic syndrome (23), and other cardiometabolic functions (24). Overall, acute mountain sickness is the most common discomfort experienced by newcomers to high altitude areas, which is associated with sleep problems and headache, dizziness, nausea and vomiting, sleep disturbance and fatigue (15). Chronic mountain sickness (CMS) that affects local residents in high altitude areas is related to a progressive loss of ventilatory rate, which naturally occurs with age and result in excessive hypoxemia and polycythemia (25). Some studies found that residents living in high altitude areas were more likely to suffer from high-altitude polycythemia (26), high-altitude pulmonary hypertension (27), congenital cardiac anomalies (28, 29), chronic kidney (30), and rheumatoid arthritis (31) due to hypoxia compared to those living in low altitude areas, all of which are negatively associated with QOL.
On the other hand, moderate altitude levels could have positive effects on sugar metabolism and blood pressure. For example, inhabitants living in the Valley of Mexico (2,240 m above sea level) were found to breathe 29% more on average and have 10% higher hemoglobin concentrations compared to residents living near sea level. Young adults in Mexico City had an SaO2 between 92 and 94% vs. 97% among those living at sea level (32). It is likely that lung growth, development during pregnancy and infancy, and other physiological adaptations are enhanced in moderate altitude levels, although solid evidence is still needed. However, for people with respiratory diseases, residing at moderate altitudes could result in worsening hypoxemia and clinical deterioration (32).
To date there have been no comparative studies on the influence of living in high altitude areas on QOL in older adults. This study hence compared the QOL in older adults living in high and low altitude areas and explored the correlates of QOL in those living in high altitude area.
Methods
Study design and participants
This was part of a cross-sectional, comparative study on mental health in older adults living in high and low altitude areas (33). The surveys were conducted from September 1st to November 31st in 2019 in three public nursing homes in Xining that is the capital city of Qinghai province with an average altitude of 2,300 m (high altitude area), and one public nursing home in Guangzhou which is the capital city of Guangdong province with an average altitude of 10 m (low altitude area). Older adults included in this study were living in the selected nursing homes, aged 60 years or above and able to understand the purpose and content of the assessment. Those with severe cognitive problems (e.g., dementia and severe head injury) as determined by a review of health records were excluded. The study protocol was approved by the Ethical Committee of the University of Macau. Written informed consent were provided by all participants.
Instruments
Basic sociodemographic and clinical characteristics, such as age, gender, marital status, education level, perceived financial and health status, and having a religion and major medical conditions, were collected in an interview and confirmed by a review of health records. QOL was measured using the validated Chinese version of the WHO Quality of Life brief version–WHOQOL-BREF (34, 35) that consists of 26 items covering four domains: physical, psychological, social relationships, and environment. Each item were scored from 1 to 5 points (36), with a higher score indicating higher QOL.
The validated Chinese version of the Patient Health Questionnaire (PHQ-9) (37, 38) was used to measure the severity of depression. The PHQ-9 consists of nine items with each scored from 0 = “not at all”, 1 = “several days” to 2 = “more than half of the days” and 3 = “nearly every day”. The PHQ-9 total score ranges from 0 to 27, with a higher score indicating more severe depression.
Data analyses
The sociodemographic and clinical characteristics of older adults living in the high and low altitude areas were compared using chi-square test, two independent samples t-test and Mann-Whitney U-test as appropriate. Then QOL between older adults living in the high and low altitude areas was compared using analysis of covariance (ANCOVA) after controlling for those that significantly differed in univariate analyses. The associations between socio-demographic and clinical characteristics and QOL in older adults living in high altitude area were examined using two independent samples t-test, analysis of variance, chi-square test, and Pearson correlation analysis. Finally, multiple linear regression analyses were used to analyze the independent correlates of QOL in older adults living in the high altitude area. Each of the physical, psychological, social relationships, and environmental QOL was the dependent variable, while demographic and clinical variables that significantly differed in univariate analyses were entered as the independent variables. IBM SPSS Statistics for Windows, version 24.0 (IBMCorp., Armonk, N.Y., USA) was used to analyze data. P-value was set at 0.05 (two-tailed).
Results
Altogether, 644 older adults were included, with 207 in high and 437 in low altitude areas who completed the assessment. There were significant differences between older adults living high and low altitude areas in terms of age, education, religion, perception of financial status, perception of health status, number of major medical conditions, psychological QOL and PHQ-9 total score (Table 1). ANCOVA revealed that after controlling for variables that significantly differed in the univariate analyses, older adults living in high altitude area had significantly higher physical [F(1, 644) = 4.46, P = 0.035] and social QOL [F(1, 644) = 9.30, P = 0.002], and lower psychological QOL [F(1, 644) = 6.94, P = 0.009] compared to those living in low altitude area. There was no group difference in environmental [F(1, 644) = 0.32, P = 0.570] QOL.
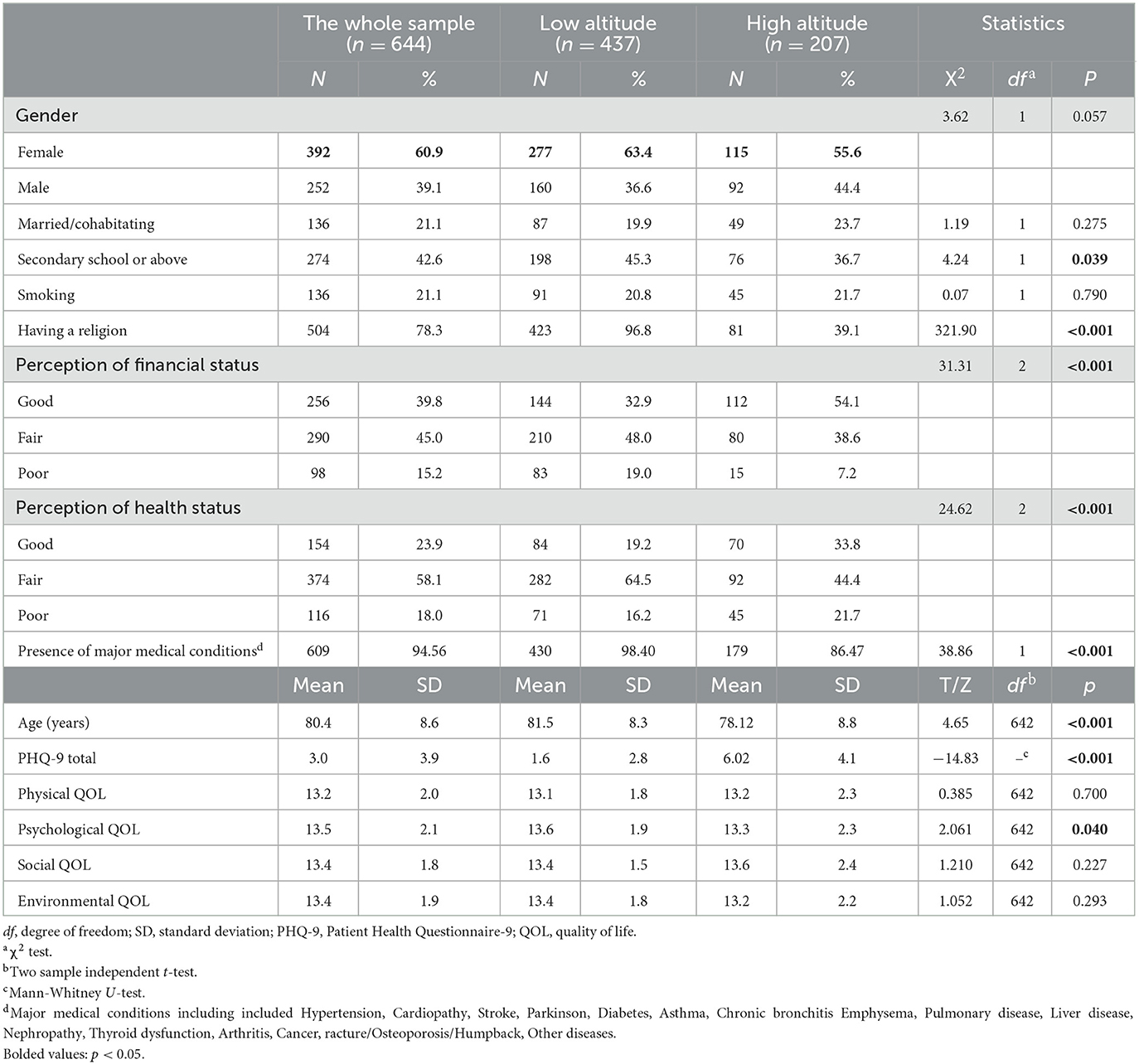
Table 1. Basic demographic and clinical characteristics of the whole sample.
Table 2 shows the associations between basic and clinical demographic characteristics and QOL domains in older adults living in high altitude areas. Male gender was significantly associated with physical and psychological QOL, while smoking status, perceived health status and depressive symptoms were associated with all four QOL domains. Perceived financial status, medical conditions and age were also associated with physical QOL.
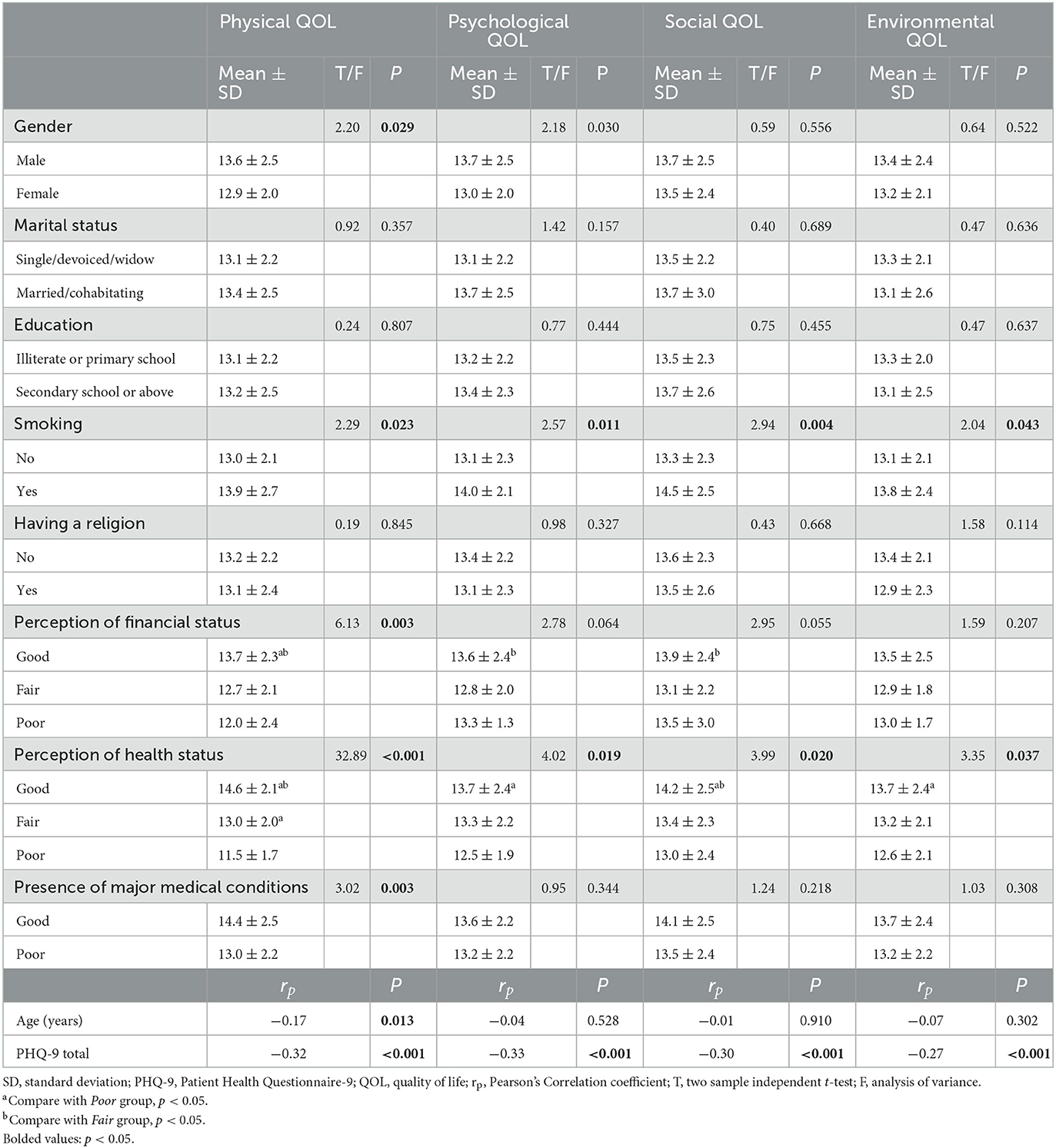
Table 2. Associations between socio-demographic characteristics and QOL domains in older adults in high altitude region.
Table 3 presents the results of multiple linear regression analyses in older adults living in high altitude areas. For older adults living in high altitude area, smoking status was associated with higher social QOL (β = 0.16, 95% CI: 0.14–1.74, P = 0.021), while good financial status was associated with higher physical QOL (β = 0.24, 95% CI: 0.08–2.16, P = 0.035), fair or good health status were associated with higher physical QOL (fair health status: β = 0.30, 95%CI: 0.71–2.09, p < 0.001; good health status: β = 0.54, 95%CI: 1.89–3.39, p < 0.001) and psychological QOL (β = 0.18, 95% CI: 0.02–1.68, P = 0.046), and more severe depressive symptoms were associated with lower physical (β = −0.19, 95% CI: −0.17 to −0.04, P = 0.002), psychological (β = −0.29, 95% CI: −0.23 to −0.08, P < 0.001), social (β = −0.26, 95% CI: −0.24 to −0.07, P < 0.001), and environmental QOL (β = −0.23, 95% CI: −0.20 to −0.05, P = 0.001).
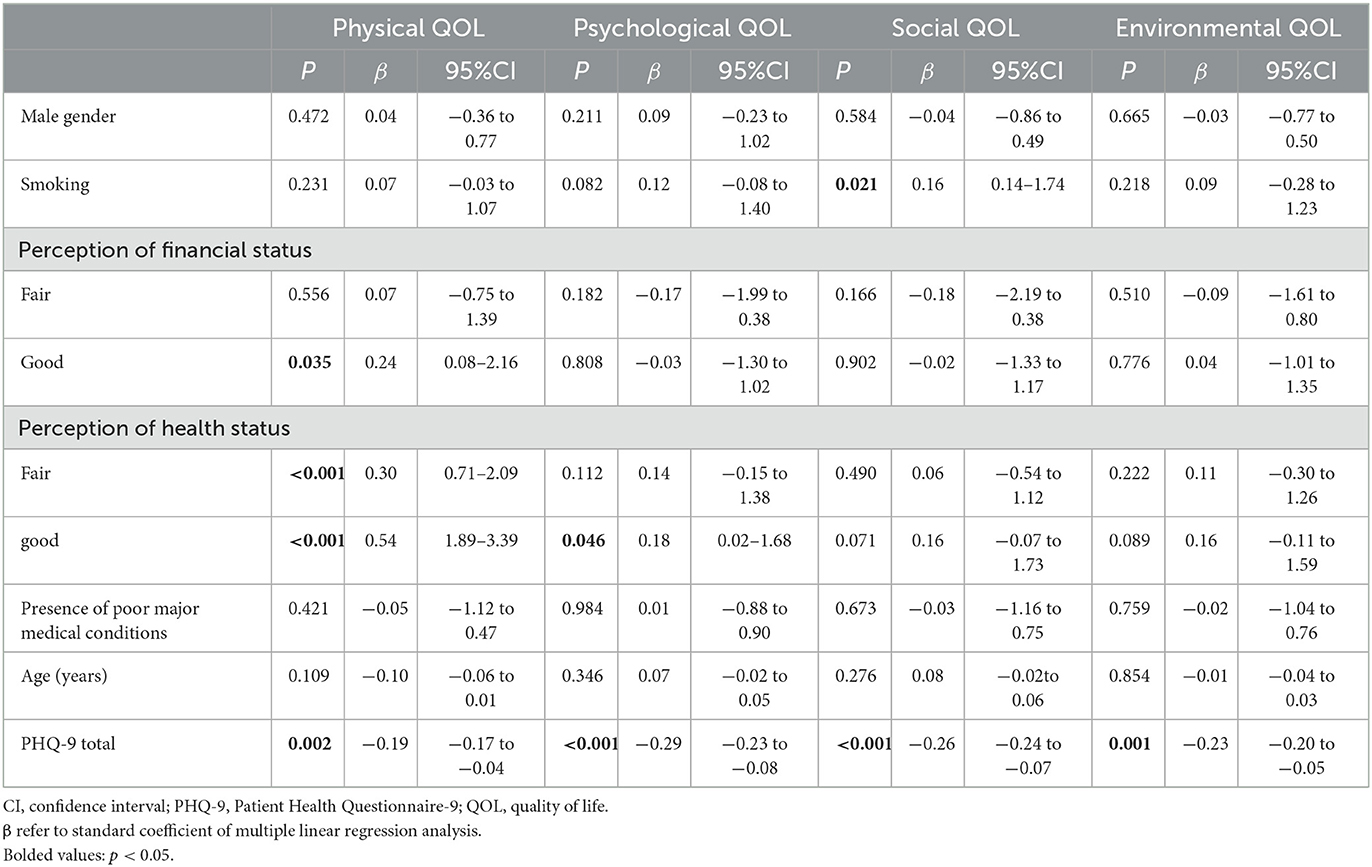
Table 3. Socio-demographic correlates of QOL in older adults living in high altitude region (by multiple linear regression analysis).
Discussion
This was the first comparative study of older adults that examined the association between living at high altitude areas and QOL. We found that older adults living in high altitude area had higher physical and social QOL, but lower psychological QOL compared to their counterparts living in low altitude area. For older adults living in high altitude area, smoking status, perceived financial and health status, and depressive symptoms were associated with QOL.
Older adults living in high altitude area had lower psychological QOL than those living in low altitude area, which could be due to increased risk of psychological and psychiatric sequelae of residing in high altitude areas, such as sleep disturbances (33, 39), stress, depression, anxiety (40) and even suicide (41). This was partly supported by our study findings in that those with more severe depressive symptoms were more likely to have lower QOL. Moreover, high psychological stress could also contribute to poor physical health such as heart disease (42) and cancer (43), which in turn could further lower psychological QOL.
There are several possible reasons for the association between high altitude and increased risk of psychiatric symptoms. Living at high altitude is associated with hypobaric hypoxia, which could impair brain functions over time (44) and increase the likelihood of psychiatric comorbidities including depression (40). In addition, persons living at high altitude are exposed to chronic hypoxia, which could lead to a number of physical diseases, such as high-altitude polycythemia (26), high-altitude pulmonary hypertension (27), and congenital cardiac anomalies (28, 29). All these factors could increase the risk of mental health problems due to the respective burden of the disease and treatment which could lower QOL.
Unexpectedly, our study revealed that adults living in a high altitude area had higher QOL in both physical and social domains but no difference in environmental domain compared to their counterparts living in low altitude area. This could be explained by the following reasons. QOL is largely determined by the gap between one's expectation and actual experiences (45). In the past decade, the central Chinese government has allocated substantial budget and health resources to improve the health service systems and living conditions for the population living in Qinghai-Tibet Plateau, particularly cities such as Xining city where this study was conducted. Therefore, the participants' experiences in terms of physical, social and environmental aspects would be expected to improve, which would match or even exceed their earlier expectations. However, like most areas across China, the implementation of mental health promotion and services (e.g., the Psychological Care Project for Older Adults) were still under-developed in the community which might influence psychological QOL. In addition, environmental and social factors could play an important role on QOL (46). In developed areas such as in Guangzhou (low altitude area), crowded living, noise pollution, fast working pace, competitive pressure and stress of high living cost could negatively influence QOL; in contrast, these factors were less evident in economically under-developed area such as Xining (high altitude area), which might partly explain the finding that adults living in high altitude area had higher QOL in both physical and social domains.
Several sociodemographic and clinical characteristics were associated with QOL in this study. Smoking could increase the risk of a range of physical diseases (47–49), which in turn could lowered QOL (50, 51). However, surprisingly older adults who smoke had higher social QOL in this study. In traditional Chinese culture, smoking and drinking are common social behaviors used to enhance social networks, facilitate interpersonal interactions, increase social activity of older people to reduce loneliness (52–54), all of which could improve QOL. Consequently, compared to those who do not smoke, older adults who smoke usually have a better social network and supports (55, 56), which could improve QOL in the social domain. As expected, older adults with better perceived financial and health status were more likely to have higher QOL. Better financial situation and health status are usually associated with greater level of health literacy and access to healthcare services (57, 58) as well as good social support (59) in older adults, all of which could improve QOL.
There are several limitations in this study. First, due to the cross-sectional study design, causal relationship between QOL and other variables could not be examined. Second, for logistical reasons, the participants were invited from nursing homes and those with obvious cognitive problems were excluded, which would limit the generalizability of the findings. Finally, some variables related to QOL, such as treatment of physical diseases, were not examined.
In conclusion, our study of older adults found a significant association between living at high altitude and QOL. Older adults living in a high altitude area had higher physical and social QOL, but lower psychological QOL. Appropriate interventions to address depressive symptoms (e.g., increase access to community mental health services), and support to improve financial and health status should be developed for older adults living in high altitude areas to improve their QOL.
Data availability statement
The datasets presented in this article are not readily available because the Clinical Research Ethics Committee of University of Macau that approved the study prohibits the authors from making publicly available the research dataset of clinical studies. Requests to access the datasets should be directed to eHl1dGx5QGdtYWlsLmNvbQ==.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethical Committee of the University of Macau. The patients/participants provided their written informed consent to participate in this study.
Author contributions
YF and Y-TX: study design. SL, FW, SS, HC, and Y-TX: collection, analyses, and interpretation of data. SL and Y-TX: drafting of the manuscript. CN: critical revision of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The study was supported by the National Science and Technology Major Project for investigational new drug (2018ZX09201-014), the Beijing Hospitals Authority Clinical Medicine Development of special funding support (XMLX202128), the University of Macau (MYRG2019-00066-FHS; MYRG2022-00187-FHS), and the Natural Science Foundation of Qinghai Province (2019-ZJ-906).
Acknowledgments
The authors are grateful to all participants and clinicians involved in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Felce D, Perry J. Quality of life: its definition and measurement. Res Dev Disabil. (1995) 16:51–74. doi: 10.1016/0891-4222(94)00028-8
2. Zheng X, Xue Y, Dong F, Shi L, Xiao S, Zhang J, et al. The association between health-promoting-lifestyles, and socioeconomic, family relationships, social support, health-related quality of life among older adults in china: a cross sectional study. Health Qual Life Outcomes. (2022) 20:1–8. doi: 10.1186/s12955-022-01968-0
3. Öztürk ZA, Türkbeyler IH, Abiyev A, Kul S, Edizer B, Yakaryilmaz FD, et al. Health-related quality of life and fall risk associated with age-related body composition changes; sarcopenia, obesity and sarcopenic obesity. Intern Med J. (2018) 48:973–81. doi: 10.1111/imj.13935
4. Gothe NP, Ehlers DK, Salerno EA, Fanning J, Kramer AF, McAuley E. Physical activity, sleep and quality of life in older adults: influence of physical, mental and social well-being. Behav Sleep Med. (2020) 18:797–808. doi: 10.1080/15402002.2019.1690493
5. Liu S, Wang F, Zhang C, Zhang Q, Dang ZC, Ng CH, et al. Cognitive impairment and its associated factors in older adults living in high and low altitude areas: a comparative study. Front Psychiatry. (2022) 13:871414. doi: 10.3389/fpsyt.2022.871414
6. Picco L, Achilla E, Abdin E, Chong SA, Vaingankar JA, McCrone P, et al. Economic burden of multimorbidity among older adults: impact on healthcare and societal costs. BMC Health Serv Res. (2016) 16:173. doi: 10.1186/s12913-016-1421-7
7. Lanuza F, Morales G, Hidalgo-Rasmussen C, Balboa-Castillo T, Ortiz MS, Belmar C, et al. Association between eating habits and quality of life among Chilean university students. J Am Coll Health. (2020) 70:280–6. doi: 10.1080/07448481.2020.1741593
8. Lee YY, Wang P, Abdin E, Chang S, Shafie S, Sambasivam R, et al. Prevalence of binge drinking and its association with mental health conditions and quality of life in Singapore. Addict Behav. (2020) 100:106114. doi: 10.1016/j.addbeh.2019.106114
9. Milic M, Gazibara T, Pekmezovic T, Kisic Tepavcevic D, Maric G, Popovic A, et al. Tobacco smoking and health-related quality of life among university students: mediating effect of depression. PLoS ONE. (2020) 15:e0227042. doi: 10.1371/journal.pone.0227042
10. Xu J, Qiu J, Chen J, Zou L, Feng L, Lu Y, et al. Lifestyle and health-related quality of life: a cross-sectional study among civil servants in China. BMC Public Health. (2012) 12:1–9. doi: 10.1186/1471-2458-12-330
11. Pei M, Aguiar R, Pagels AA, Heimbürger O, Stenvinkel P, Bárány P, et al. Health-related quality of life as predictor of mortality in end-stage renal disease patients: an observational study. BMC Nephrol. (2019) 20:144. doi: 10.1186/s12882-019-1318-x
12. Sajobi TT, Wang M, Awosoga O, Santana M, Southern D, Liang Z, et al. Trajectories of health-related quality of life in coronary artery disease. Circ Cardiovasc Qual Outcomes. (2018) 11:e003661. doi: 10.1161/CIRCOUTCOMES.117.003661
13. Berkley AS, Carter PA, Yoder LH, Acton G, Holahan CK. The effects of insomnia on older adults' quality of life and daily functioning: a mixed-methods study. Geriatr Nurs. (2020) 41:832–8. doi: 10.1016/j.gerinurse.2020.05.008
14. Yang JJ, Cai H, Xia L, Nie W, Zhang Y, Wang S, et al. The prevalence of depressive and insomnia symptoms, and their association with quality of life among older adults in rural Areas in China. Front Psychiatry. (2021) 12:727939. doi: 10.3389/fpsyt.2021.727939
15. Hackett PH, Roach RC. High-altitude illness. N Engl J Med. (2001) 345:107–14. doi: 10.1056/NEJM200107123450206
16. Luks AM, Swenson ER, Bärtsch P. Acute high-altitude sickness. Eur Respir Rev. (2017) 26:160096. doi: 10.1183/16000617.0096-2016
17. Beall CM. Detecting natural selection in high-altitude human populations. Respir Physiol Neurobiol. (2007) 158:161–71. doi: 10.1016/j.resp.2007.05.013
18. Beall CM. Hemoglobin, altitude, and sensitive Swiss men. Blood. (2020) 135:984–5. doi: 10.1182/blood.2020005251
19. Simonson TS, Yang Y, Huff CD, Yun H, Qin G, Witherspoon DJ, et al. Genetic evidence for high-altitude adaptation in Tibet. Science. (2010) 329:72–5. doi: 10.1126/science.1189406
20. Strohl KP. Lessons in hypoxic adaptation from high-altitude populations. Sleep Breath. (2008) 12:115–21. doi: 10.1007/s11325-007-0135-9
21. Wu T, Kayser B. High altitude adaptation in Tibetans. High Alt Med Biol. (2006) 7:193–208. doi: 10.1089/ham.2006.7.193
22. Cho JI, Basnyat B, Jeong C, Di Rienzo A, Childs G, Craig SR, et al. Ethnically Tibetan women in Nepal with low hemoglobin concentration have better reproductive outcomes. Evol Med Public Health. (2017) 2017:82–96. doi: 10.1093/emph/eox008
23. Strauss-Blasche G, Riedmann B, Schobersberger W, Ekmekcioglu C, Riedmann G, Waanders R, et al. Vacation at moderate and low altitude improves perceived health in individuals with metabolic syndrome. J Travel Med. (2004) 11:300–4. doi: 10.2310/7060.2004.19106
24. Wee J, Climstein M. Hypoxic training: clinical benefits on cardiometabolic risk factors. J Sci Med Sport. (2015) 18:56–61. doi: 10.1016/j.jsams.2013.10.247
25. Monge CC, ArreguiA, Leon-Velarde F. Pathophysiology and epidemiology of chronic mountain sickness. Int J Sports Med. 13(S 1):S79–81. doi: 10.1055/s-2007-1024603
26. Hancco I, Bailly S, Baillieul S, Doutreleau S, Germain M, Pépin J-L, et al. Excessive erythrocytosis and chronic mountain sickness in dwellers of the highest city in the world. Front Physiol. (2020) 11:773. doi: 10.3389/fphys.2020.00773
27. Gou Q, Shi R, Zhang X, Meng Q, Li X, Rong X, et al. The prevalence and risk factors of high-altitude pulmonary hypertension among native Tibetans in Sichuan Province, China. High Alt Med Biol. (2020) 21:327–35. doi: 10.1089/ham.2020.0022
28. Han S, Wei C-y, Hou Z-l, Li Y-x, Ding Y-c, Guang X-f, et al. Prevalence of congenital heart disease amongst schoolchildren in southwest China. Indian Pediatr. (2020) 57:138–41. doi: 10.1007/s13312-020-1731-z
29. Ma LG, Chen QH, Wang YY, Wang J, Ren ZP, Cao ZF, et al. Spatial pattern and variations in the prevalence of congenital heart disease in children aged 4-18 years in the Qinghai-Tibetan Plateau. Sci Total Environ. (2018) 627:158–65. doi: 10.1016/j.scitotenv.2018.01.194
30. Luks AM, Johnson RJ, Swenson ER. Chronic kidney disease at high altitude. J Am Soc Nephrol. (2008) 19:2262–71. doi: 10.1681/ASN.2007111199
31. Zhang Q, Liu Q, Lin C, Baima Y, Li H, Gong H, et al. The prevalence of rheumatoid arthritis in middle-aged and elderly people living in Naqu City, Tibet, Autonomous Region of China. J Orthop Surg Res. (2020) 15:1–6. doi: 10.1186/s13018-020-01883-4
32. Pérez-Padilla JR. Adaptation to moderate altitude hypoxemia: the example of the valley of Mexico. Rev Investi Clín. (2022) 74:4–15. doi: 10.24875/RIC.21000159
33. Liu S, Chow IHI, Lu L, Ren YM, Yang HL, Jian SY, et al. Comparison of sleep disturbances between older nursing home residents in high- and low-altitude areas. J Geriatr Psychiatry Neurol. (2020) 33:370–6. doi: 10.1177/0891988719892335
34. WHO. Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychol Med. (1998) 28:551–8. doi: 10.1017/S0033291798006667
35. Xia P, Li N, Hau KT, Liu C, Lu Y. Quality of life of Chinese urban community residents: a psychometric study of the mainland Chinese version of the WHOQOL-BREF. BMC Med Res Methodol. (2012) 12:37. doi: 10.1186/1471-2288-12-37
36. Skevington SM, Lotfy M, O'Connell KA. The World Health Organization's WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. (2004) 13:299–310. doi: 10.1023/B:QURE.0000018486.91360.00
37. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
38. Wang W, Bian Q, Zhao Y, Li X, Wang W, Du J, et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. (2014) 36:539–44. doi: 10.1016/j.genhosppsych.2014.05.021
39. Sakamoto R, Okumiya K, Norboo T, Tsering N, Yamaguchi T, Nose M, et al. Sleep quality among elderly high-altitude dwellers in Ladakh. Psychiatry Res. (2017) 249:51–7. doi: 10.1016/j.psychres.2016.12.043
40. Kious BM, Bakian A, Zhao J, Mickey B, Guille C, Renshaw P, et al. Altitude and risk of depression and anxiety: findings from the intern health study. Int Rev Psychiatry. (2019) 31:637–45. doi: 10.1080/09540261.2019.1586324
41. Brenner B, Cheng D, Clark S, Camargo CA Jr. Positive association between altitude and suicide in 2584 US counties. High Alt Med Biol. (2011) 12:31–5. doi: 10.1089/ham.2010.1058
42. Wirtz PH, von Känel R. Psychological stress, inflammation, and coronary heart disease. Curr Cardiol Rep. (2017) 19:1–10. doi: 10.1007/s11886-017-0919-x
43. Hayes JD, Dinkova-Kostova AT, Tew KD. Oxidative stress in cancer. Cancer Cell. (2020) 38:167–97. doi: 10.1016/j.ccell.2020.06.001
44. Huang BY, Castillo M. Hypoxic-ischemic brain injury: imaging findings from birth to adulthood. Radiographics. (2008) 28:417–39. doi: 10.1148/rg.282075066
45. Carr AJ, Gibson B, Robinson PG. Measuring quality of life: Is quality of life determined by expectations or experience? Bmj. (2001) 322:1240–3. doi: 10.1136/bmj.322.7296.1240
46. Sugiyama T, Thompson CW, Alves S. Associations between neighborhood open space attributes and quality of life for older people in Britain. Environ Behav. (2009) 41:3–21. doi: 10.1177/0013916507311688
47. Fielding JE. Smoking: health effects and control (1). N Engl J Med. (1985) 313:491–8. doi: 10.1056/NEJM198508223130807
48. Ng R, Sutradhar R, Yao Z, Wodchis WP, Rosella LC. Smoking, drinking, diet and physical activity-modifiable lifestyle risk factors and their associations with age to first chronic disease. Int J Epidemiol. (2020) 49:113–30. doi: 10.1093/ije/dyz078
49. Ricci NA, Francisco CO, Rebelatto MN, Rebelatto JR. Influence of history of smoking on the physical capacity of older people. Arch Gerontol Geriatr. (2011) 52:79–83. doi: 10.1016/j.archger.2010.02.004
50. Goldenberg M, Danovitch I, IsHak WW. Quality of life and smoking. Am J Addict. (2014) 23:540–62. doi: 10.1111/j.1521-0391.2014.12148.x
51. Toghianifar N, Najafian J, Pooya A, Rabiei K, Eshrati B, Anaraki J, et al. Association of smoking status with quality of life in a cross-sectional population-based sample of Iranian adults: Isfahan Healthy Heart Program. Asia Pac J Public Health. (2012) 24:786–94. doi: 10.1177/1010539511403800
52. Ding L, Liang Y, Tan ECK, Hu Y, Zhang C, Liu Y, et al. Smoking, heavy drinking, physical inactivity, and obesity among middle-aged and older adults in China: cross-sectional findings from the baseline survey of CHARLS 2011-2012. BMC Public Health. (2020) 20:1062. doi: 10.1186/s12889-020-08625-5
53. Wang Q, Zhang Y, Wu C. Alcohol consumption and associated factors among middle-aged and older adults: results from China Health and Retirement Longitudinal Study. BMC Public Health. (2022) 22:322. doi: 10.1186/s12889-022-12718-8
54. Yang G, Wang Y, Wu Y, Yang J, Wan X. The road to effective tobacco control in China. Lancet. (2015) 385:1019–28. doi: 10.1016/S0140-6736(15)60174-X
55. Bian Y. Guanxi and the allocation of urban jobs in China. China Q. (1994) 140:971–99. doi: 10.1017/S0305741000052863
56. Pan Z. Socioeconomic predictors of smoking and smoking frequency in urban China: evidence of smoking as a social function. Health Promot Int. (2004) 19:309–15. doi: 10.1093/heapro/dah304
57. Hadisuyatmana S, Maulana MR, Makhfudli M. Poor financial support and lack of knowledge, and neglect among female elders who lived in extended families. J Ners. (2016) 11:220–3. doi: 10.20473/jn.V11I22016.220-223
58. Hamiduzzaman M, De Bellis A, Abigail W, Kalaitzidis E. The social determinants of healthcare access for rural elderly women-A systematic review of quantitative studies. Open Public Health J. (2017) 10:244–66. doi: 10.2174/1874944501710010244
Keywords: older adults, high altitude, depression, quality of life, low altitude
Citation: Liu S, Wang F, Sha S, Cai H, Ng CH, Feng Y and Xiang Y-T (2023) A comparison of quality of life between older adults living in high and low altitude areas. Front. Public Health 11:1184967. doi: 10.3389/fpubh.2023.1184967
Received: 16 March 2023; Accepted: 23 June 2023;
Published: 20 November 2023.
Edited by:
Petra Heidler, IMC University of Applied Sciences Krems, AustriaReviewed by:
Nikolaus Christoph Netzer, University of Innsbruck, AustriaLisa Theresa Dam, University of Applied Sciences Burgenland, Austria
Copyright © 2023 Liu, Wang, Sha, Cai, Ng, Feng and Xiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuan Feng, MTk1NTgwNTFAcXEuY29t; Chee H. Ng, Y25nQHVuaW1lbGIuZWR1LmF1
†These authors have contributed equally to this work