 Xiao Huang
Xiao Huang Jiahui Deng
Jiahui Deng Wenbin Liu
Wenbin Liu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 29 June 2023
Sec. Aging and Public Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1182268
Objective: To compare the sex differences in cognitive function and its influencing factors among Chinese older adults.
Method: We conducted a cross-sectional study by using data from the China Longitudinal Healthy Longevity Survey (CLHLS). According to the 32 provinces and 4 municipalities directly under the Central Government of China, 3–5 counties or districts were randomly selected in each province or city (except Tibet), and then 1–3 villages or streets were randomly selected in each county or district, from which the target population was sampled. Mini Mental State Examination (MMSE) was used to assess the cognitive function of 9,262 older adults aged 65 and above in China. Descriptive analysis was applied to demonstrate the participants’ demographic characteristics, health-related behaviors, social and non-social activity, disease status, mental and sleep condition. And then, univariate and multifactor analyses were performed to validate different risk factors for cognitive function, respectively in the general population, male older adults and female older adults.
Result: The older adults with cognitive impairment accounted for 10.4% of the total population. There are significant differences in cognitive function between male and female older adults. The odds of cognitive impairment in older adult women was 1.291 times that of older adult men (OR = 1.291, 95%CI: 1.084–1.538). Among the male older adults, those who were older, highly educated, spouseless, had depressive symptoms, and lacked social activities were more likely to have cognitive impairment, whereas among the female older adults, those who were older, highly educated, and lacked social activities were more likely to have cognitive impairment.
Conclusion: Overall, there are subtle differences in potential influencing factors for cognitive function between the male older adults and female older adults. Attention should be paid to the different cognitive protection measures for the older adults with different sexes.
Cognitive function impairment is a prevalent geriatric syndrome affecting the older adults (1). Older adult individuals with mild cognitive function impairment may experience severe symptoms, and those with severe cognitive function impairment may progress to dementia or Alzheimer’s disease (AD), resulting in the inability to complete daily tasks and live independently (2). This situation is even more serious in China as it has become an aging society (3), and the number of Chinese individuals aged 60 or older is projected to reach 488 million by 2050, representing 35.6% of the total population (4). Since cognitive function impairment not only diminishes the quality of life of the older adults, but also exert burden of caregiving responsibilities on their family and the social care system (5, 6), understanding the shifting trends in cognitive function is essential for preserving social stability in an aging population.
Current research focuses primarily on analyzing demographic factors (7–9) and interpreting the effects of socioeconomic (10–12) and physiological factors on cognitive function in the older adults (13, 14). Some existing studies begin to measure the relationship between cognitive function and age and sex of the older adults. Many studies have confirmed that age and sex are important factors affecting cognition (15). In the study of healthy behaviors and lifestyles, some studies have found that smoking affects cognitive levels. Some components of nicotine and nicotine can temporarily improve cognitive function, but heavy smoking has been linked to cognitive function impairment and decline in middle age (16, 17). In addition, heavy drinking can lead to neurocognitive deficits, which can lead to mild anterograde amnesia and temporary cognitive deficits (18, 19). On the level of social participation, recently investigators have examined the effects of the degree of social isolation affects the cognition of the older adults (20, 21). Some studies have pointed out that a higher frequency of participation in social activities can help slow down the occurrence of cognitive dysfunction in the older adults (22, 23).
In terms of physical health, studies have found that physically active older adults have a lower risk of disability, functional limitations, and cognitive decline (24), and there is a negative correlation between the number of chronic diseases and cognitive decline (25). And when it comes to mental health, some studies have shown that symptoms of depression and anxiety can lead to cognitive decline (26, 27), and the quantity and quality of sleep conditions will change with the increase of age, and lack of sleep conditions will lead to decreased cognitive function (28, 29).
However, relatively few of these studies on the factors that influence cognitive function in the older adults consider sex differences. Although numerous studies have confirmed that age and sex are essential risk factors (15), sex differentiation analyses for specific categories of cognitive function are scarce. Thus, studying sex differences in cognitive function is conducive to understanding the cognitive frailty and health gap of all older adults, so that cognitive frailty can be accurately prevented and controlled based on the sex characteristics of older adults.
Therefore, this study utilized data from the 2017–2018 wave of Chinese Longitudinal Healthy Longevity Survey (CLHLS) in the present cross-sectional study. It included a large national representative sample of over 65-year-olds in determining the factors associated with cognitive function in the Chinese older adults and analyzed sex differences to increase our knowledge of cognitive health in the older adults.
We conducted a cross-sectional study.In this study, the data set was retrieved from the Chinese Longitudinal Health and Longevity Survey (CLHLS), which was conducted by the Chinese Center for Disease Control and Prevention and directed by the Center for Healthy Aging and Development of Peking University and Duke University (30). It investigates several influential social, health, and longevity behaviors and biological and environmental risk factors (31). Initiated in 1998, the CLHLS conducted seven waves of surveys in 22 sample areas across 31 provincial administrative units from 2000 to 2018. The sample represents approximately 85% of the total population in China (32).
The questionnaire inquired about physical and mental health, lifestyle, family composition, and health care. The previous evaluation demonstrated that the CLHLS data are complete, authentic, and reliable (33).
Most of the participants in 2017–2018 wave of CLHLS were 65 years old and above. According to the design of this study, the inclusion criteria were older adults who completed the MMSE scale in its entirety, excluding those who were unable to complete the scale properly due to hearing and speech impairment, bedridden coma, mental illness, pathological brain injury, etc. In addition, samples with missing values in health-related behaviour, social engagement, systemic somatic diseases and mental and sleep condition were eliminated. Finally, 9,262 older adults aged 65 years and over were included in the study. More details about the participants in our study are shown in Supplementary Figure 1.
The Mini-Mental State Examination (MMSE) is one of the most widely used cognitive screening scales including orientation (time orientation, place orientation), memory (immediate memory, short-term memory), calculation, language (naming, repetition, listening comprehension, reading comprehension, writing), visual space, application and attention tests (34), which plays an important role in the diagnosis of cognitive impairment. Taking Chinese culture and socioeconomic development status into account, the CLHLS applied the Chinese version of MMSE to test the cognitive function of all respondents, which consists of 13 question items with total scores ranging from 0 to 30. Lower scores indicate poorer cognitive function. The validity and reliability of the Chinese MMSE has been verified (35–37). More details about the Chinese version of the MMSE are shown in Table 1.
Given that the MMSE score is susceptible to interference from educational attainment (38), this study adopt a more reasonable and accurate method to set the criterion of cognitive impairment according to different educational levels rather than setting a single standard for all participants (39, 40). If the respondents had no formal education, a score of 17 or less was considered cognitive impairment; if they had 1–6 years of education, a score of 20 or less was considered a cognitive impairment; If they had more than 6 years of education, a score of 24 or less was considered cognitive impairment; otherwise, it is considered normal cognitive function (41).
In this study, risk factors for cognitive impairment in the older adults were categorized into five sets as follows:
1. Demographic characteristics, including sex, age, household registration, educational attainment and marital status;
2. Health-related behavior, including smoking, drinking and exercising;
3. Social engagement: ① “social activity,” such as Tai chi, square dancing, consort visit, other outdoor activities, playing cards or mahjong, and other social activities; ② “non-social activity,” such as housework, gardening and raising pets, reading books and newspapers, raising poultry and livestock, and watching television and listening to the radio;
4. Systemic somatic diseases: ① Circulatory system, including hypertension, heart disease and dyslipidemia; ② Endocrine system: diabetes mellitus; ③ Respiratory system: including bronchitis, emphysema, asthma, pneumonia and tuberculosis; ④ Nervous system: including stroke, cerebrovascular disease, Parkinson’s disease and epilepsy; ⑤ Urinary system: chronic nephritis; ⑥ Digestive system: including gastrointestinal ulcer, cholecystitis, cholelithiasis and hepatitis; ⑦ Exercise system: arthritis; ⑧ Immune system: rheumatism or rheumatoid arthritis; ⑨ Sensory organ: cataract or glaucoma; ⑩ Other types;
5. Mental and sleep condition: Depression scale (CESD-10) was utilized to measure the degree of depression among middle-aged and older adult individuals (42). The items of this scale include: “Do you get upset about petty things?” “Do you have a hard time concentrating?,” “Are you feeling sad or depressed?” Each scale item has four levels: “Never,” “Rarely,” “Sometimes,” and “Often or always” with scores of 0, 1, 2, and 3, respectively. For CESD-10, 12 points are the best cutoff point in China (scores≥12 points are identified as “With depressive symptoms”; scores<12 points denote “Without depressive symptoms”); While sleep condition was measured by the item “How is your sleep quality right now?” and divided into three status as “good,” “average” and “bad.”
In this study, categorical variables were described by frequency and percentage, and continuous variables were described by mean ± standard deviation. The cognitive function of the overall older adults were divided into two groups (normal cognitive function and impaired cognitive function) according to the MMSE scores. Comparisons of categorical information between the two groups were made using chi-square tests, whereas group comparisons of continuous information were made using t-tests. Factors with p < 0.05 in the univariate analysis were included in the multifactor logistic regression model, and all independent variables were involved in building the model, thus exploring the influential factors associated with cognitive impairment in the older adults. SPSS 23.0 was used to perform all of the statistical analyses. The level of statistical significance was set as p = 0.05.
The participants’ demographic data including household registration, age, marital status, educational attainment, sleep quality, smoking, drinking, exercise, cognitive ability, depression, participation in social activities, and chronic diseases, were demonstrated in Table 2. The total number of participants was 9,262, with 4,581 male and 4,681 female. In general, most older adults (70.6%) were from rural areas, with a generally low level of education. And they had very good sleep quality, and most people did not smoke (83%) or drink (83.1%), and without doing exercise (62.3%). Only a minority (10.4%) had cognitive impairment, and nearly half of the older adults had depression symptoms. Approximately 70% of older adults did not engage in social activities. More than 90% of the older adults suffered from various chronic diseases.
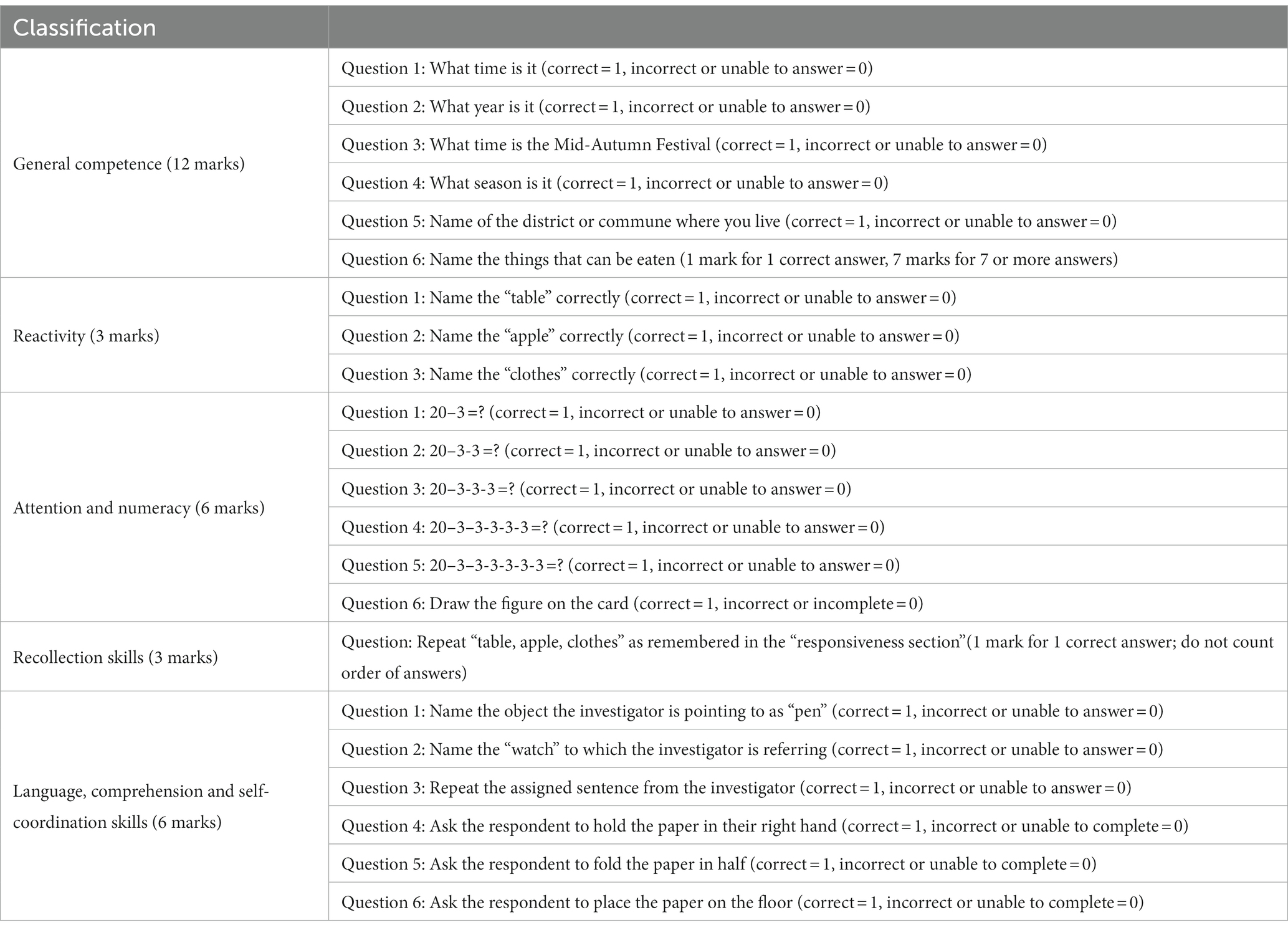
Table 1. The specific content and scoring rules of MMSE scale.
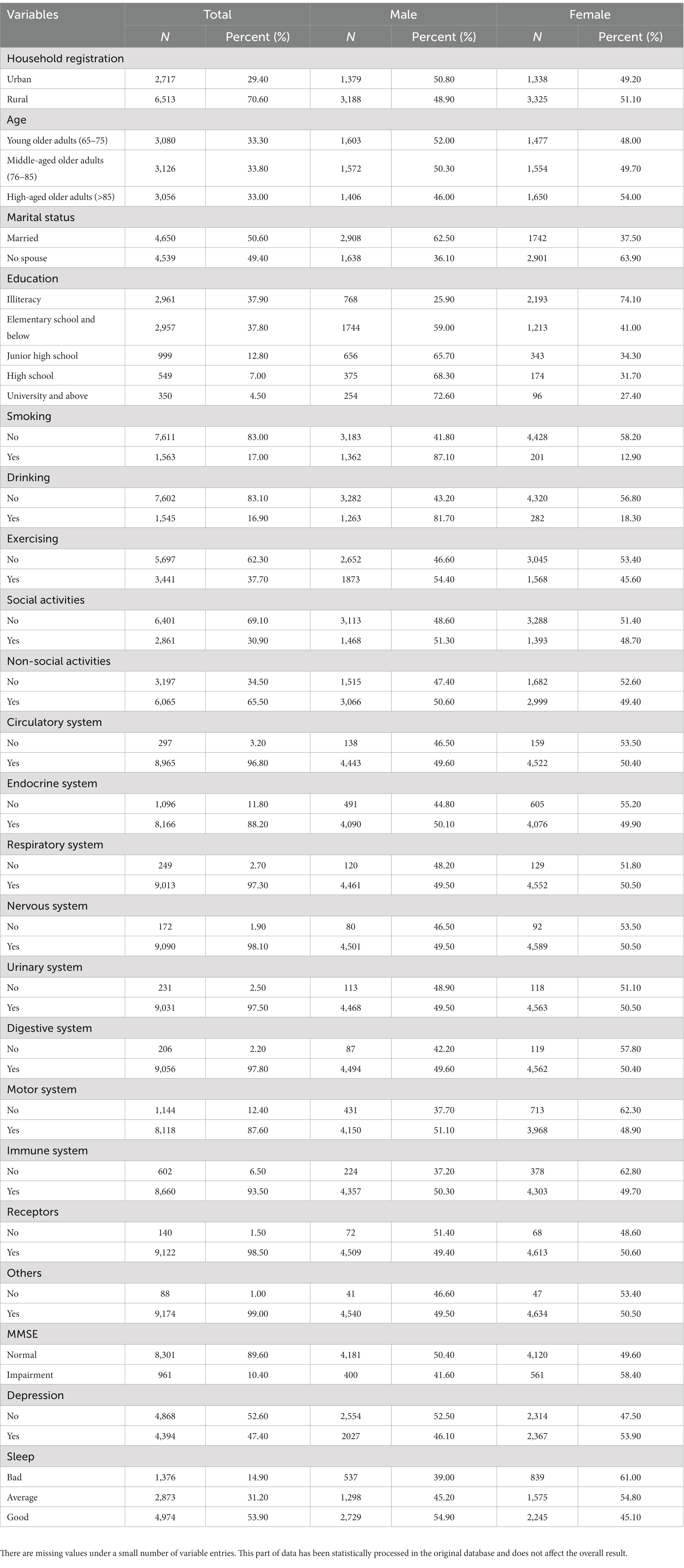
Table 2. Characteristics of the participants.
The equations should be inserted in editable format from the equation editor. The cognitive scores using MMSE scale were compared between male and female. Table 3 shows that significant differences existed not only in total scores of MMSE cognitive, but also in general competence, reactivity, attention and numeracy, recollection skills, language, comprehension and self-coordination skills (p < 0.05).
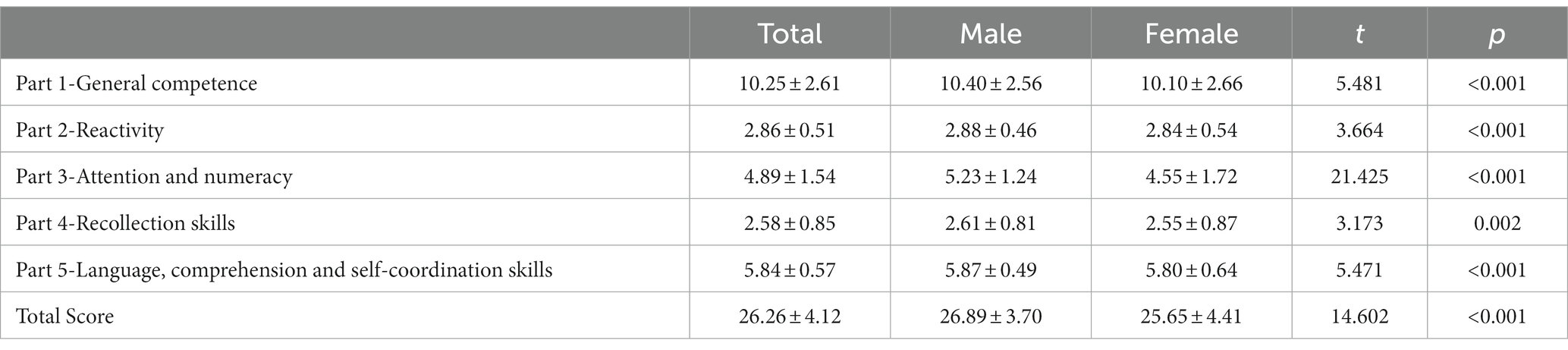
Table 3. Differences between scores of cognitive function in male older adults and female older adults.
In all older adults data (Table 4), there were significant differences between cognitively normal and cognitively impaired older adults in risk factors such as sex, age, marital status, educational attainment, sleep condition, smoking, drinking, exercising, depressive symptoms, social participation, chronic diseases of digestive system and other chronic diseases (p < 0.05); However, there were no significant differences between the two groups in household registration, the presence of chronic diseases such as the circulatory system, endocrine system, respiratory system, nervous system, urinary system, motor system, immune system, and receptor (p > 0.05).
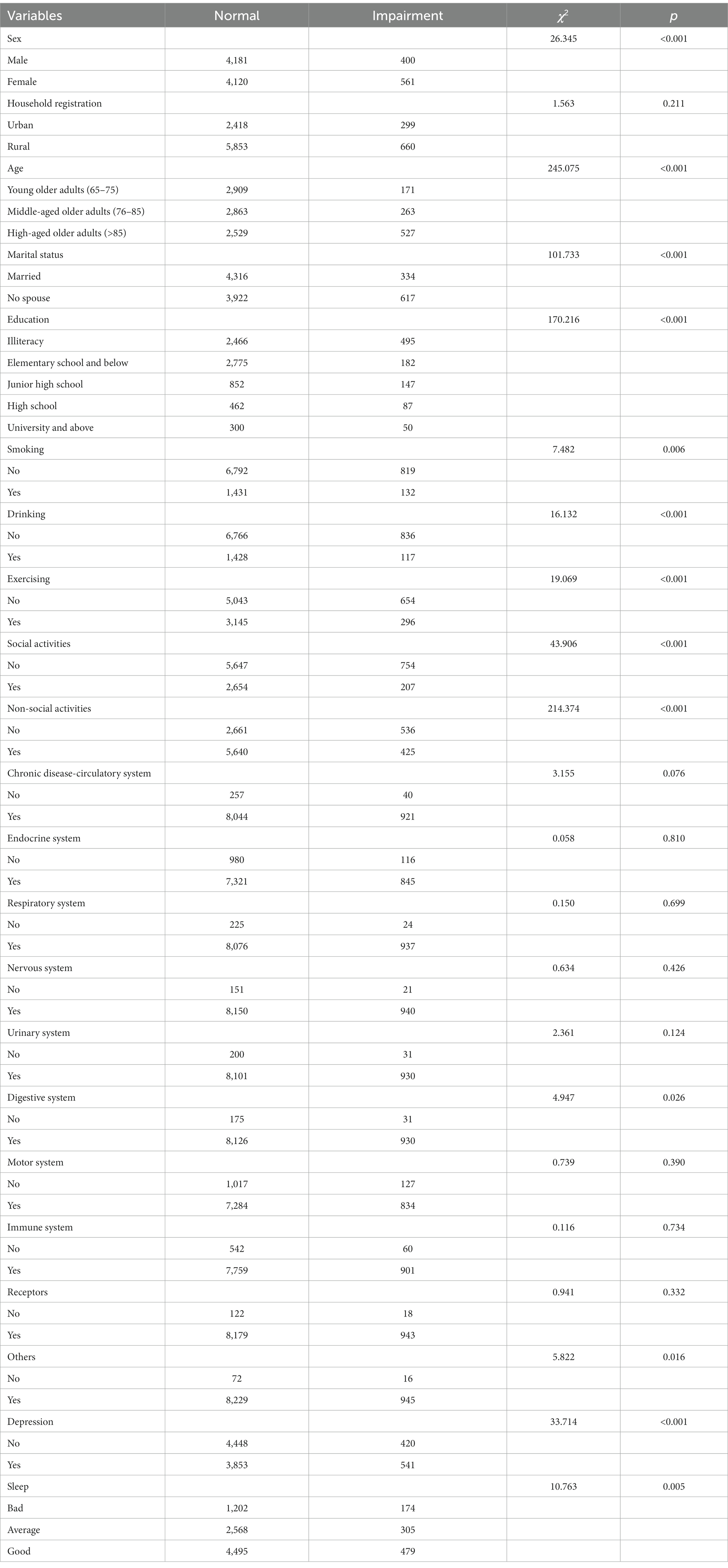
Table 4. Univariate analysis of factors influencing cognitive function in all older adults.
Compared with all older adults, the male older adults were equally affected by age, marital status, educational attainment, sleep condition, drinking, exercising, depressive symptoms, and social participation (p < 0.05); In contrast, there was a significant difference in the household registration of the male older adults (p < 0.05), but no significant difference in smoking and carrying all chronic diseases (p > 0.05) (Shown in column 5 of Table 5).
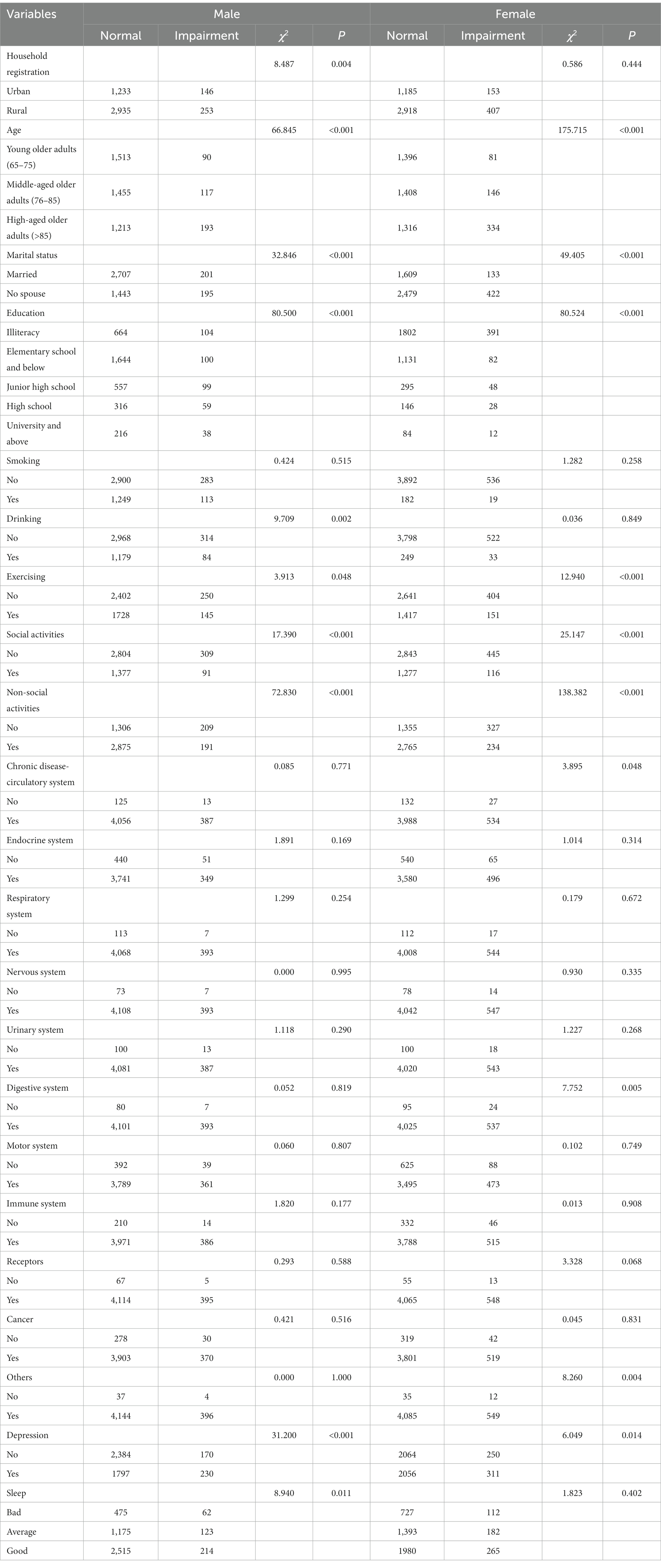
Table 5. Univariate analysis of factors influencing cognitive function in male older adults and female older adults.
Among the female older adults, the common risk factors with the male older adults included age, marital status, educational attainment, exercise, depressive symptoms, social participation (p < 0.05), but there were significant differences in the chronic diseases of circulation and digestive system among the female older adults (p < 0.05); However, there were no significant differences in household registration, sleep condition, smoking and drinking (p > 0.05) (Shown in column 9 of Table 5).
Among all older adults data, sleep condition, smoking, drinking and exercising have no significant effect on cognitive ability (p > 0.05); The odds of cognitive impairment in female older adults was 1.291 times higher than that in male older adults (OR = 1.291, 95% CI: 1.084–1.538); Ageing had a significant effect on cognitive ability (p < 0.05); The odds of the older adults without a spouse suffering from cognitive impairment was 1.211 times higher than that of the married older adults (OR = 1.211, 95%CI: 1.013–1.446); Educational attainment had impacted on cognitive ability (p < 0.05); The older adults with depressive symptoms were 1.348 times more likely to have cognitive impairment than those without depressive symptoms (OR = 1.348, 95%CI: 1.162–1.564); Older adults who participate in social activities (Tai chi, square dancing, consort visit, other outdoor activities, playing cards or mahjong, and other social activities) were 0.766 times less likely to suffer from cognitive impairment than those who have not participated in these activities (OR = 0.766, 95%CI: 0.64–0.917); Older adults who participate in non-social activities (housework, gardening and raising pets, reading books and newspapers, raising poultry and livestock, and watching television and listening to the radio) suffer from cognitive impairment was 0.524 times lower (OR = 0.524, 95%CI: 0.445–0.618) than that of the older adults who have not participated in these activities; Digestive system and other chronic diseases had no effect on cognitive ability (p > 0.05) (Shown in column 2 and 3 of Table 6).
Among male older adults, household registration, sleep condition, drinking, exercising and participating in social activities had no significant effect on cognitive ability (p > 0.05); Ageing had a significant influence on cognitive ability in male older adults (p < 0.05); The unmarried male older adults were 1.351 times more likely to have cognitive impairment than married male older adults (OR = 1.351, 95%CI: 1.054–1.733);Educational attainment had impacted on cognitive ability in male older adults (p < 0.05); The odds of suffering from cognitive impairment for those male older adults with depressive symptoms was 1.70 times higher than that of the older adults without depressive symptoms (OR = 1.7, 95%CI: 1.35–2.139); The older adults who participate in non-social activities were 0.492 times less likely to suffer from cognitive impairment than those who have not participated in these activities (OR = 0.492, 95%CI: 0.383–0.632) (Shown in column 4 and 5 of Table 6).
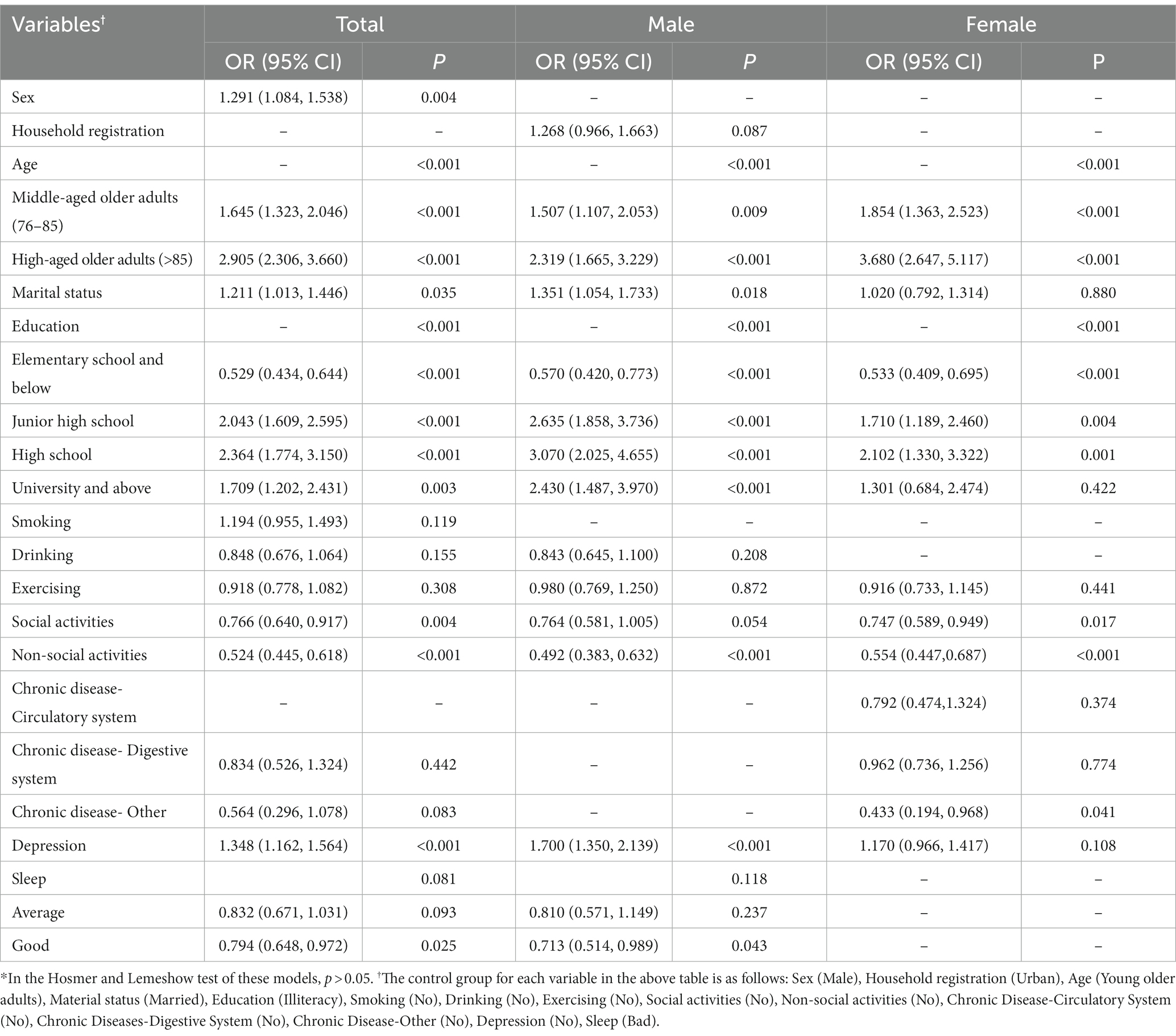
Table 6. Multifactorial analysis of factors influencing cognitive function in older adults.
In female older adults, marital status, exercising, presence of depressive symptoms, presence of the circulatory system and digestive system chronic disease had no significant influence on cognitive ability (p > 0.05);Ageing had a significant influence on cognitive ability in female older adults (p < 0.05); Educational attainment had impacted on cognitive ability in female older adults (p < 0.05); Female older adults who participate in social activities was 0.747 times lower than that of the female older adults who have not participated in these activities on suffering from cognitive impairment (OR = 0.747, 95%CI: 0.589–0.949); The odds of cognitive impairment in female older adults who participate in non-social activities was 0.554 times lower than that of the female older adults who have not participated in these activities (OR = 0.554, 95%CI: 0.447–0.687); Cognitive impairment in female older adults with other chronic diseases was 0.433 times lower than that in female older adults without chronic diseases (OR = 0.433, 95%CI: 0.194–0.968) (Shown in column 6 and 7 of Table 6).
To bridge the knowledge gap of differences in cognitive function by sex, this study used a multivariate analysis to explain the factors affecting cognitive function in older Chinese adults by parsing data from the 2017–2018 China Longitudinal Healthy Living Survey (CLHLS). From the final findings, it indicated that sex, age, marital status, and educational attainment significantly affect older adults cognitive function. And it is evident that older female with higher education at an advanced age are more likely to have cognitive impairment compared to the older male. These results not only reveal sex differences in cognitive function, but also provide practical guidance in promoting the cognitive health of this older adults group.
From the perspective of sex differences affecting cognition, the same factors affecting the male older adults and female older adults are: age, education attainment and social activities. Our findings indicate that the odds of cognitive dysfunction increases with age. Normal human aging can lead to a decline in cognitive function. To a physiologically healthy level, gray matter atrophy in the medial prefrontal cortex, which is associated with cognitive function, increases with age (43). The decline of brain structure and function with aging is the main cause of cognitive decline in the older adults (44).
As for the relationship between educational attainment and cognitive ability, our findings indicate that older adults with a high school diploma or higher are more likely to suffer from cognitive impairment than their illiterate counterparts, which is contrary to previous research findings that individuals with a higher level of education are more resistant to the aging process, diseases associated with aging, and brain and cognitive impairment (45, 46). However, recent studies also have pointed out that educational attainment is not associated with long-term rates of change in any cognitive domain, with studies stating that education is only associated with cognitive performance and not with cognitive decline (47). And many studies have emphasized the need to also take into account the influence of genetic factors, socioeconomic background, and socio-cultural background when analyzing the association between educational attainment and cognitive function (48–50). In light of the contradictory findings, the connection between early education and cognitive impairment in the older adults requires further investigation.
There is growing evidence that a healthy lifestyle can reduce the rate of cognitive decline with age and delay the onset of cognitive symptoms associated with age-related disorders (51). Participating in social activities is associated with improved acting ability and hand, eye, and foot coordination, among other body functions. In addition, at the molecular and cellular level, physical activity directly affects the expression of neurotransmitters and neurotrophic factors, thereby influencing synaptic plasticity as well as cellular state. Moreover, it can influence cellular inflammation and oxidative stress through hormonal regulation, which in turn affects cognition and brain health (52). And playing cards and mahjong has been shown to have a protective effect on cognitive function in the older adults (53, 54). These previous researches showing that participation in social and non-social activities protects the cognition of the older adults also supports the conclusions of our study.
In terms of the different influences on cognitive function between male and female older adults, we found that female older adults were weaker than the male older adults in each of the cognitive function scores. Studies show that decreased estrogen levels in older women are associated with cognitive dysfunction (55, 56). The decrease in estrogen will decrease blood flow to the cerebral cortex and glucose metabolism and uptake by neurons in the hippocampus, thereby increasing neuronal damage and impairing cognitive function (57). For traditional Chinese cultural and historical reasons, women in this study were significantly disadvantaged compared to men in terms of educational opportunities, nutritional intake, and occupational achievement, thereby limiting women’s cognitive maintenance and further development (58).
And simultaneously, there are sex differences in marital status and depression between male and female older adults. We found that cognitive impairment is more prevalent among male older adults without spouses than among male older adults with spouses, but marital status has no significant effect on cognitive function among female older adults. Previous research has demonstrated that family relationships are one of the most influential factors in the cognitive function of the older adults (59). A stable marriage ensures older adults receive excellent daily care and social support. Spiritual and marital support tends to be lacking in older adult individuals who are divorced or living alone, which can lead to loneliness and negative outlooks on life, resulting in psychological and cognitive impairments. Our research indicates that older men may have a greater need for family support, particularly from their partners. Those who lack such support are more likely to experience cognitive impairment (60).
Male older adults with depression symptoms were more likely (1.7 times) to have cognitive impairment than the general population (1.348 times), whereas depressive status had no effect on cognitive function in the female older adults. It indicates that the effect of depressive symptoms on cognitive dysfunction is more significant in male older adults than in female older adults. Cognitive impairment is relatively prevalent among the older adults with symptoms of depression, whereas cognitive impairment is less prevalent among the older adults who engage in social or non-social activities. There are sex differences in the structure and function of specific brain regions in depressed patients, according to research. The prefrontal limbic loop is primarily aberrant in female depressed patients, whereas the prefrontal striatum loop is primarily aberrant in male depressed patients. Moreover, the cortico-limbic striatum system abnormalities differ between male and female patients with major depression (61, 62).
This research also has some limitations. Most of the influencing factors of cognitive function involved in this study are selected based on previous studies, but our study is based on the questions in the CLHLS questionnaire. For the analysis of cognitive influencing factors in the older adults population, we only selected the cross-sectional study in 2018 based on the CLHLS database, and more samples may be needed to confirm the sex difference. The size of the questionnaire is limited, and there are many influencing factors that cannot be investigated, so the influencing factors we can select are limited. The cognitive profile of older people changes dynamically over time, however, this study is a cross-sectional study and the data is still not comprehensive. And there are various risk factors that affect cognitive profiles, but variables such as individual socio-economic base, health care conditions, experience before reaching old age, personality traits and healthy diet structure are not addressed in this study. Therefore, future studies need to further integrate tracking data from different time points, conduct longitudinal analyses of the cognitive profile of Chinese older adults and attempt to include more comprehensive variables as well as explore the interaction mechanisms of the included variables.
This study elucidates the factors affecting cognitive function in the older adults from the perspective of sex. There are cognitive function differences between the sexes among the older adults. Physiologically and medically, the male older adults with high education, no spouse, depressive symptoms, and lack of social activities and the female older adults with high education and lack of social activities are in a vulnerable position. In order to meet the health needs of various groups, it is necessary to develop targeted medical and social health promotion activities that consider vulnerable groups and pay attention to the gap between groups.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary material.
The Duke University Research Ethics Committee and Peking University approved CLHLS’s Human Subject Protection Plan. Prior to the survey, all CLHLS survey participants provided written informed consent. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
WL and XH conceived and designed the study. XH, WL, and JD done the data acquisition, analysis, and interpretation. All authors contributed to the article and approved the submitted version.
This study is supported by the Natural Science Foundation of Fujian Province (Grant No. 2021 J01245) and the Distinguished Young Scientific Research Talents Plan in Universities of Fujian Province (Grant No. 2018B030).
We thank all the participants in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1182268/full#supplementary-material
1. Magnuson, A, Sattar, S, Nightingale, G, Saracino, R, Skonecki, E, and Trevino, KM. A practical guide to geriatric syndromes in older adults with Cancer: a focus on falls, cognition, Polypharmacy, and depression. Am Soc Clin Oncol Educ Book. (2019) 39:e96–e109. doi: 10.1200/EDBK_237641
2. Crimmins, EM, Saito, Y, and Kim, JK. Change in cognitively healthy and cognitively impaired life expectancy in the United States: 2000–2010. SSM Popul Health. (2016) 2:793–7. doi: 10.1016/j.ssmph.2016.10.007
3. Fang, EF, Xie, C, Schenkel, JA, Wu, C, Long, Q, Cui, H, et al. A research agenda for ageing in China in the 21st century (2nd edition): focusing on basic and translational research, long-term care, policy and social networks. Ageing Res Rev. (2020) 64:101174. doi: 10.1016/j.arr.2020.101174
4. Fang, EF, Scheibye-Knudsen, M, Jahn, HJ, Li, J, Ling, L, Guo, H, et al. A research agenda for aging in China in the 21st century. Ageing Res Rev. (2015) 24:197–205. doi: 10.1016/j.arr.2015.08.003
5. Wu, C, Gao, L, Chen, S, and Dong, H. Care services for elderly people with dementia in rural China: a case study. Bull World Health Organ. (2016) 94:167–73. doi: 10.2471/BLT.15.160929
6. Hu, X, Gu, S, Sun, X, Gu, Y, Zhen, X, Li, Y, et al. Cognitive ageing trajectories and mortality of Chinese oldest-old. Arch Gerontol Geriatr. (2019) 82:81–7. doi: 10.1016/j.archger.2019.01.018
7. van Gelder, BM, Tijhuis, M, Kalmijn, S, Giampaoli, S, Nissinen, A, and Kromhout, D. Marital status and living situation during a 5-year period are associated with a subsequent 10-year cognitive decline in older men: the FINE study. J Gerontol Ser B Psychol Sci Soc Sci. (2006) 61:P213–9. doi: 10.1093/geronb/61.4.P213
8. Hayden, KM, Reed, BR, Manly, JJ, Tommet, D, Pietrzak, RH, Chelune, GJ, et al. Cognitive decline in the elderly: an analysis of population heterogeneity. Age Ageing. (2011) 40:684–9. doi: 10.1093/ageing/afr101
9. Yaffe, K, Peltz, CB, Ewing, SK, McCulloch, CE, Cummings, SR, Cauley, JA, et al. Long-term cognitive trajectories and mortality in older women. J Gerontol A Biol Sci Med Sci. (2016) 71:1074–80. doi: 10.1093/gerona/glw003
10. Dartigues, J-F, Gagnon, M, Letenneur, L, Barberger-Gateau, P, Commenges, D, Evaldre, M, et al. Principal lifetime occupation and cognitive impairment in a French elderly cohort (Paquid). Am J Epidemiol. (1992) 135:981–8. doi: 10.1093/oxfordjournals.aje.a116410
11. Lee, S. Education, other socioeconomic indicators, and cognitive function. Am J Epidemiol. (2003) 157:712–20. doi: 10.1093/aje/kwg042
12. Andel, R, Vigen, C, Mack, WJ, Clark, LJ, and Gatz, M. The effect of education and occupational complexity on rate of cognitive decline in Alzheimer’s patients. J Int Neuropsychol Soc. (2006) 12:147–52. doi: 10.1017/S1355617706060206
13. Wang, H, Fang, C, Cai, L, Dong, B, and Deng, J. Chronic kidney disease and cognitive impairment among the very old in China. Aging Clin Exp Res. (2016) 28:475–82. doi: 10.1007/s40520-015-0433-1
14. Falck, RS, Best, JR, Davis, JC, Eng, JJ, Middleton, LE, Hall, PA, et al. Sleep and cognitive function in chronic stroke: a comparative cross-sectional study. Sleep. (2019) 42:zsz040. doi: 10.1093/sleep/zsz040
15. Lu, J, Guo, QQ, Wang, Y, Zuo, ZX, and Li, YY. The evolutionary stage of cognitive frailty and its changing characteristics in old adults. J Nutr Health Aging. (2021) 25:467–78. doi: 10.1007/s12603-020-1560-8
16. Levin, ED, McClernon, FJ, and Rezvani, AH. Nicotinic effects on cognitive function: behavioral characterization, pharmacological specification, and anatomic localization. Psychopharmacology. (2006) 184:523–39. doi: 10.1007/s00213-005-0164-7
17. Campos, MW, Serebrisky, D, and Castaldelli-Maia, JM. Smoking and cognition. Curr Drug Abuse Rev. (2017) 9:76–9. doi: 10.2174/1874473709666160803101633
18. Schuckit, MA. Alcohol-use disorders. Lancet. (2009) 373:492–501. doi: 10.1016/S0140-6736(09)60009-X
19. Mukherjee, S. Alcoholism and its effects on the central nervous system. Curr Neurovasc Res. (2013) 10:256–62. doi: 10.2174/15672026113109990004
20. Cornwell, EY, and Waite, LJ. Measuring social isolation among older adults using multiple indicators from the NSHAP study. J Gerontol Ser B Psychol Sci Soc Sci. (2009) 64B:i38–46. doi: 10.1093/geronb/gbp037
21. Evans, IEM, Llewellyn, DJ, Matthews, FE, Woods, RT, Brayne, C, and Clare, L. On behalf of the CFAS-Wales research team. Social isolation, cognitive reserve, and cognition in healthy older people. PLoS One. (2018) 13:e0201008. doi: 10.1371/journal.pone.0201008
22. Jia, R, Liang, J, Xu, Y, and Wang, Y. Effects of physical activity and exercise on the cognitive function of patients with Alzheimer disease: a meta-analysis. BMC Geriatr. (2019) 19:181. doi: 10.1186/s12877-019-1175-2
23. Sun, B, Zhao, Y, Lu, W, and Chen, Y. The relationship of malnutrition with cognitive function in the older Chinese population: evidence from the Chinese longitudinal healthy longevity survey study. Front Aging Neurosci. (2021) 13:766159. doi: 10.3389/fnagi.2021.766159
24. Cunningham, C, O' Sullivan, R, Caserotti, P, and Tully, MA. Consequences of physical inactivity in older adults: a systematic review of reviews and meta-analyses. Scand J Med Sci Sports. (2020) 30:816–27. doi: 10.1111/sms.13616
25. Socal, MP, and Trujillo, AJ. Links between chronic illness and late-life cognition: evidence from four Latin American countries. J Aging Health. (2018) 30:262–304. doi: 10.1177/0898264316674557
26. Calabrese, C, Gregory, WL, Leo, M, Kraemer, D, Bone, K, and Oken, B. Effects of a standardized Bacopa monnieri extract on cognitive performance, anxiety, and depression in the elderly: a randomized, double-blind, placebo-controlled trial. J Altern Complement Med. (2008) 14:707–13. doi: 10.1089/acm.2008.0018
27. Kim, JH, Kim, Y, Kwon, J, and Park, E-C. Association between changes in depressive state and cognitive function. Int J Environ Res Public Health. (2019) 16:4944. doi: 10.3390/ijerph16244944
28. Scullin, MK, and Bliwise, DL. Sleep, cognition, and normal aging: integrating a half century of multidisciplinary research. Perspect Psychol Sci. (2015) 10:97–137. doi: 10.1177/1745691614556680
29. Gava, G, Orsili, I, Alvisi, S, Mancini, I, Seracchioli, R, and Meriggiola, MC. Cognition, mood and sleep in menopausal transition: the role of menopause hormone therapy. Medicina. (2019) 55:668. doi: 10.3390/medicina55100668
30. Zhang, Y, Xiong, Y, Yu, Q, Shen, S, Chen, L, and Lei, X. The activity of daily living (ADL) subgroups and health impairment among Chinese elderly: a latent profile analysis. BMC Geriatr. (2021) 21:30. doi: 10.1186/s12877-020-01986-x
31. Yue, Z, Xiang, N, Li, H, and Liu, E. The evolution trend of availability of China’s community-based care services and its impact on the cognitive function of elderly people: 2008-2018. Int J Equity Health. (2021) 20:203. doi: 10.1186/s12939-021-01544-w
32. Wang, W, Chen, J, Jin, X, Ping, Y, and Wu, C. Association between indoor ventilation frequency and cognitive function among community-dwelling older adults in China: results from the Chinese longitudinal healthy longevity survey. BMC Geriatr. (2022) 22:106. doi: 10.1186/s12877-022-02805-1
33. Zhang, H, Wang, Y, Wu, D, and Chen, J. Evolutionary path of factors influencing life satisfaction among Chinese elderly: a perspective of data visualization. Data. (2018) 3:35. doi: 10.3390/data3030035
34. Zhou, L, Lin, Z, Jiao, B, Liao, X, Zhou, Y, Li, H, et al. Consistency analysis and conversion model establishment of mini-mental state examination and Montreal cognitive assessment in Chinese patients with Alzheimer’s disease. Front Psychol. (2022) 13:990666. doi: 10.3389/fpsyg.2022.990666
35. An, R, and Liu, GG. Cognitive impairment and mortality among the oldest-old Chinese: cognitive impairment and mortality among the oldest-old Chinese. Int J Geriatr Psychiatry. (2016) 31:1345–53. doi: 10.1002/gps.4442
36. Zeng, Y, Feng, Q, Hesketh, T, Christensen, K, and Vaupel, JW. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: a cohort study. Lancet. (2017) 389:1619–29. doi: 10.1016/S0140-6736(17)30548-2
37. Lv, Y-B, Gao, X, Yin, Z-X, Chen, H-S, Luo, J-S, Brasher, MS, et al. Revisiting the association of blood pressure with mortality in oldest old people in China: community based, longitudinal prospective study. BMJ. (2018) 361:k2158. doi: 10.1136/bmj.k2158
38. Pellicer-Espinosa, I, and Díaz-Orueta, U. Cognitive screening instruments for older adults with low educational and literacy levels: a systematic review. J Appl Gerontol. (2022) 41:1222–31. doi: 10.1177/07334648211056230
39. Angevaren, M, Aufdemkampe, G, Verhaar, H, Aleman, A, and Vanhees, L. Physical activity and enhanced fitness to improve cognitive function in older people without known cognitive impairment In:. Cochrane database of systematic reviews. Chichester, UK: John Wiley & Sons, Ltd (2008). CD005381.
40. Manly, JJ, Tang, M-X, Schupf, N, Stern, Y, Vonsattel, J-PG, and Mayeux, R. Frequency and course of mild cognitive impairment in a multiethnic community. Ann Neurol. (2008) 63:494–506. doi: 10.1002/ana.21326
41. Cui, G-H, Yao, Y-H, Xu, R-F, Tang, H-D, Jiang, G-X, Wang, Y, et al. Cognitive impairment using education-based cutoff points for CMMSE scores in elderly Chinese people of agricultural and rural Shanghai China: education-based cutoff points for CMMSE scores. Acta Neurol Scand. (2011) 124:361–7. doi: 10.1111/j.1600-0404.2010.01484.x
42. Williams, MW, Li, C-Y, and Hay, CC. Validation of the 10-item Center for Epidemiologic Studies Depression Scale Post. Stroke. (2020) 29:105334. doi: 10.1016/j.jstrokecerebrovasdis.2020.105334
43. Greenwood, PM. The frontal aging hypothesis evaluated. J Int Neuropsychol Soc. (2000) 6:705–26. doi: 10.1017/S1355617700666092
44. Lockhart, SN, and DeCarli, C. Structural imaging measures of brain aging. Neuropsychol Rev. (2014) 24:271–89. doi: 10.1007/s11065-014-9268-3
45. Stern, Y. The concept of cognitive reserve: a catalyst for research. J Clin Exp Neuropsychol. (2003) 25:589–93. doi: 10.1076/jcen.25.5.589.14571
46. Whalley, LJ, Deary, IJ, Appleton, CL, and Starr, JM. Cognitive reserve and the neurobiology of cognitive aging. Ageing Res Rev. (2004) 3:369–82. doi: 10.1016/j.arr.2004.05.001
47. Zahodne, LB, Glymour, MM, Sparks, C, Bontempo, D, Dixon, RA, MacDonald, SWS, et al. Education does not slow cognitive decline with aging: 12-year evidence from the Victoria longitudinal study. J Int Neuropsychol Soc. (2011) 17:1039–46. doi: 10.1017/S1355617711001044
48. Lin, Z, Desai, S, and Chen, F. The emergence of educational Hypogamy in India. Demography. (2020) 57:1215–40. doi: 10.1007/s13524-020-00888-2
49. Fletcher, J, Topping, M, Zheng, F, and Lu, Q. The effects of education on cognition in older age: evidence from genotyped siblings. Soc Sci Med. (2021) 280:114044. doi: 10.1016/j.socscimed.2021.114044
50. Walhovd, KB, Fjell, AM, Wang, Y, Amlien, IK, Mowinckel, AM, Lindenberger, U, et al. Education and income show heterogeneous relationships to lifespan brain and cognitive differences across European and US cohorts. Cereb Cortex. (2022) 32:839–54. doi: 10.1093/cercor/bhab248
51. Murman, D. The impact of age on cognition. Semin Hear. (2015) 36:111–21. doi: 10.1055/s-0035-1555115
52. Erickson, KI, Hillman, C, Stillman, CM, Ballard, RM, Bloodgood, B, Conroy, DE, et al. Physical activity, cognition, and brain outcomes: a review of the 2018 physical activity guidelines. Med Sci Sports Exerc. (2019) 51:1242–51. doi: 10.1249/MSS.0000000000001936
53. Zhang, H, Peng, Y, Li, C, Lan, H, Xing, G, Chen, Z, et al. Playing mahjong for 12 weeks improved executive function in elderly people with mild cognitive impairment: a study of implications for TBI-induced cognitive deficits. Front Neurol. (2020) 11:178. doi: 10.3389/fneur.2020.00178
54. Wang, J, Liu, N, and Zhao, X. Association of Playing Cards or mahjong with cognitive function in Chinese older adults. Int J Environ Res Public Health. (2022) 19:9249. doi: 10.3390/ijerph19159249
55. Morse, JK, Scheff, SW, and DeKosky, ST. Gonadal steroids influence axon sprouting in the hippocampal dentate gyrus: a sexually dimorphic response. Exp Neurol. (1986) 94:649–58. doi: 10.1016/0014-4886(86)90244-X
56. Neufang, S, Specht, K, Hausmann, M, Gunturkun, O, Herpertz-Dahlmann, B, Fink, GR, et al. Sex differences and the impact of steroid hormones on the developing human brain. Cereb Cortex. (2009) 19:464–73. doi: 10.1093/cercor/bhn100
57. Manly, JJ, Merchant, CA, Jacobs, DM, Small, SA, Bell, K, Ferin, M, et al. Endogenous estrogen levels and Alzheimer’s disease among postmenopausal women. Neurology. (2000) 54:833–7. doi: 10.1212/WNL.54.4.833
58. Lei, X, Smith, JP, Sun, X, and Zhao, Y. Gender differences in cognition in China and reasons for change over time: evidence from CHARLS. J Econ Ageing. (2014) 4:46–55. doi: 10.1016/j.jeoa.2013.11.001
59. Li, M, Guo, M, Stensland, M, and Dong, X. Family relationships and cognitive function among community-dwelling U.S. Chinese older adults. Res Aging. (2021) 43:37–46. doi: 10.1177/0164027520939250
60. Perkins, JM, Lee, H, James, KS, Oh, J, Krishna, A, Heo, J, et al. Marital status, widowhood duration, gender and health outcomes: a cross-sectional study among older adults in India. BMC Public Health. (2016) 16:1032. doi: 10.1186/s12889-016-3682-9
61. Kong, L, Chen, K, Womer, F, Jiang, W, Luo, X, Driesen, N, et al. Sex differences of gray matter morphology in cortico-limbic-striatal neural system in major depressive disorder. J Psychiatr Res. (2013) 47:733–9. doi: 10.1016/j.jpsychires.2013.02.003
62. Zaaijer, ER, van Dijk, L, de Bruin, K, Goudriaan, AE, Lammers, LA, Koeter, MWJ, et al. Effect of extended-release naltrexone on striatal dopamine transporter availability, depression and anhedonia in heroin-dependent patients. Psychopharmacology. (2015) 232:2597–607. doi: 10.1007/s00213-015-3891-4
Keywords: sex differences, cognitive function impairment, Chinese older adults, CLHLS, MMSE
Citation: Huang X, Deng J and Liu W (2023) Sex differences in cognitive function among Chinese older adults using data from the Chinese longitudinal healthy longevity survey: a cross-sectional study. Front. Public Health. 11:1182268. doi: 10.3389/fpubh.2023.1182268
Edited by:
Ana I. Duarte, University of Coimbra, PortugalReviewed by:
Sitong Chen, Victoria University, AustraliaCopyright © 2023 Huang, Deng and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wenbin Liu, d2VuYmlubGl1MTI2QDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.