 Roman Gabrhelík1,2*
Roman Gabrhelík1,2* Morten Hesse3
Morten Hesse3 Blanka Nechanská1,2
Blanka Nechanská1,2 Marte Handal4,5Viktor Mravčík1,2
Marte Handal4,5Viktor Mravčík1,2 Christian Tjagvad5Birgitte Thylstrup3
Christian Tjagvad5Birgitte Thylstrup3 Abdu Kedir Seid3Anne Bukten5Thomas Clausen5Svetlana Skurtveit4,5
Abdu Kedir Seid3Anne Bukten5Thomas Clausen5Svetlana Skurtveit4,5- 1First Faculty of Medicine, Department of Addictology, Charles University, Prague, Czechia
- 2Department of Addictology, General University Hospital in Prague, Prague, Czechia
- 3Centre for Alcohol and Drug Research, Aarhus University, Aarhus, Denmark
- 4Norwegian Institute of Public Health, Oslo, Norway
- 5Norwegian Centre for Addiction Research, University of Oslo, Oslo, Norway
Background: Opioid maintenance treatment (OMT) has the potential to reduce mortality rates substantially. We aimed to compare all-cause and overdose mortality among OMT patients while in or out of OMT in two different countries with different approaches to OMT.
Methods: Two nation-wide, registry-based cohorts were linked by using similar analytical strategies. These included 3,637 male and 1,580 female patients enrolled in OMT in Czechia (years 2000–2019), and 6,387 male and 2,078 female patients enrolled in OMT in Denmark (years 2007–2018). The direct standardization method using the European (EU-27 plus EFTA 2011–2030) Standard was employed to calculate age-standardized rate to weight for age. All-cause and overdose crude mortality rates (CMR) as number of deaths per 1,000 person years (PY) in and out of OMT were calculated for all patients. CMRs were stratified by sex and OMT medication modality (methadone, buprenorphine, and buprenorphine with naloxone).
Results: Age-standardized rate for OMT patients in Czechia and Denmark was 9.7/1,000 PY and 29.8/1,000 PY, respectively. In Czechia, the all-cause CMR was 4.3/1,000 PY in treatment and 10.8/1,000 PY out of treatment. The overdose CMR was 0.5/1,000 PY in treatment and 1.2/1,000 PY out of treatment. In Denmark, the all-cause CMR was 26.6/1,000 PY in treatment and 28.2/1,000 PY out of treatment and the overdose CMR was 7.3/1,000 PY in treatment and 7.0/1,000 PY out of treatment.
Conclusion: Country-specific differences in mortality while in and out of OMT in Czechia and Denmark may be partly explained by different patient characteristics and treatment systems in the two countries. The findings contribute to the public health debate about OMT management and may be of interest to practitioners, policy and decision makers when balancing the safety and accessibility of OMT.
Introduction
Opioid use disorders (OUD) are linked to elevated mortality rates among users of opioids across regions (1, 2). Mortality among regular illicit opioid (e.g., heroin) users is nearly 15 times higher compared with their peers, with higher mortality during out-of-treatment periods than during treatment (1). This is further accentuated by the opioid crisis that has unfolded and evolved in the U.S. (3) and other countries. Among the causes of mortality, overdose deaths stand out as the foremost factor among people who use extramedical opioids (4) or people in opioid maintenance treatment (OMT) (5).
OMT is the first-line treatment for OUD. Generally, OMT is a well-established treatment approach following international guidelines (6). Despite the overall increase of OMT coverage in European countries over the past decade, differences in coverage among countries remain, e.g., with France exceeding 80% coverage, while Latvia and Romania show suboptimal coverage with only about 10% of high-risk opioid users receiving OMT (7). While some patients receive medication from a general practitioner, specialized OMT clinics that combine medication with psychosocial care may be more suitable for patients who may benefit from more complex services offered (8). The regimen of these services and the prevailing system of OMT varies within each country, across countries, and over time (7).
Over the past few decades, an increasing number of countries, such as Denmark and Norway, have embraced a more inclusive approach to OMT. This approach is characterized by extensive treatment coverage and less stringent criteria for remaining in treatment, which has resulted in higher retention rates (9). A recent comprehensive review on treatment structure by Kourounis et al. (10) addressed how treatment systems differ in terms of barriers, treatment access, demands placed on patients during treatment, and the degree to which patients had an influence on treatment goals as well as the kinds of services they could receive. The authors conclude that low-threshold harm reduction treatment services are linked to better treatment outcomes than high-threshold treatment services that require patients to submit urine tests, to attend counseling, and are generally more inflexible (10).
There is evidence from both experimental and observational studies that OMT contributes to the reduction in mortality rates among patients in OMT compared to patients who discontinue or terminate OMT (11, 12). Nevertheless, national settings with differences in OMT coverage, clinical practice, and OMT medication modality on the one hand, and individual factors such as age and sex on the other, may be associated with differences in treatment outcomes including all-cause and overdose mortality rates (7).
Methadone and buprenorphine are currently the most widely used medications in OMT in Europe and elsewhere (13). Currently, in Europe, methadone is prescribed to 61% of patients in OMT, buprenorphine to 37%, and other types of medications including slow-release oral morphine to less than 4% (14). While methadone has been used in OMT for nearly five decades in Denmark (9) and over three decades in Czechia (15), buprenorphine first became available in 1999 in Denmark (16) and in 2000 in Czechia (15). Buprenorphine with naloxone was available a few years later (7). As opposed to the full mu-agonist methadone, buprenorphine is a partial agonist and was therefore introduced as a safety measure (17, 18). Naloxone, a non-selective opiate antagonist, in combination with buprenorphine was introduced as a strong deterrent to parenteral use, nevertheless, the expectations we not necessarily met (19). Previous studies showed that the use of buprenorphine in OMT was associated with a lower risk of both all-cause and overdose mortality compared to methadone (20), and recent systematic reviews and meta-analyses suggest lower all-cause mortality and overdose mortality risk related to buprenorphine both in and out OMT. However, this field lacks long-term, nation-wide studies, in particular those that include buprenorphine with naloxone.
Nation-wide OMT registers with detailed information on an individual level about time of enrolment in treatment, discontinuation, re-entry, and termination of OMT medication exist in Czechia and Denmark (21), and may be linked to information on time of death and causes of death obtained from nation-wide mortality registries. Furthermore, these two countries represent distinct treatment settings. Denmark adopts a more liberal and inclusive approach, whereas Czechia employs a more stringent treatment framework (9, 15, 22, 23). Examining mortality rates within and outside of OMT for each country individually can yield valuable insights for shaping clinical approaches.
The aim of this study was to investigate mortality rates among OMT patients during periods of both being in and out of OMT, within two countries that represent distinct treatment approaches. Specifically, within each of the two national OMT cohorts, we aimed to investigate the crude mortality rates (CMR) related to: (i) treatment status (episodes in and out of OMT); (ii) sex; (iii) cause of death (overdose or non-overdose); and (iv) OMT medication modality (methadone, buprenorphine, or buprenorphine with naloxone).
Methods
Study design
We used a prospective cohort approach linking the data sources by using the unique civil registration number assigned to all residents in both countries (21).
OMT setting
Czechia
OMT has been available as standard treatment in Czechia since 2000. The procedures for OMT are defined in the Standards for Substitution Treatment (24).
In 2017, the OMT patient rate in Czechia was 0.6 per 1,000 population (7). OMT medication can be prescribed by any physician regardless of specialization, but under a strict prescription regime applied for controlled substances. None of the types of OMT medications are formally preferred in clinical guidelines. Buprenorphine is a widespread medication since methadone is available as magistral medicine only in 12 specialized treatment centres. Approximately 50 OMT providers, predominantly general psychiatry or general practitioner practices, are officially registered for the use of buprenorphine (24). As opposed to methadone, buprenorphine was not covered by the national health insurance plan, and patients had to pay for their own OMT medication (25). Generally, OMT programmes (especially methadone programmes) apply strict rules regarding treatment compliance and illicit drug use, and urine testing is therefore an integral part of the treatment regime. Annually, approximately 500 OMT episodes (out of approximately 2,500 patients registered annually) are terminated, with half of them excluded from treatment due to non-adherence (22).
Denmark
Denmark was one of the first countries in Europe that introduced OMT (in 1970), and one of the first countries that focused on achieving high treatment coverage and retention through a more inclusive approach. In 2017, Denmark had an OMT patient rate of 1.7 per 1,000 population (7). The increased accessibility of OMT progressed throughout the 1990s and 2000s. It has been characterized by a great number of enrolled patients with OUD, one of the highest prescription rates of methadone in Europe (26), and more liberal control measures with regards to concurrent use of alcohol and other drugs, as these measures were regarded as potential barriers to treatment uptake and retention (26). To facilitate greater inclusion, supervised intake of OMT medication, urine testing, and other safety measures have been minimized. Further, compared to many other countries, patients receiving OMT in Denmark often have more influence on choice of medication and doses, and number of take-home doses are often higher compared with many other countries (26). However, the individual choice and self-management may at times be challenged in clinical settings in order to adhere to the overall OMT guidelines (27). In 2008 (revised in 2017), the Danish Health Authority published the first guidelines on medications used as part of OMT and emphasized that buprenorphine with naloxone should be used as the drug of first choice for people with OUD who had not previously been enrolled in OMT (28). Since then, prescribing buprenorphine with naloxone to OMT patients has been prioritized, although older patients in particular have expressed their preferences for methadone over buprenorphine (29).
Study population and study period
In Czechia, we included data from 1,580 females and 3,637 males who had been prescribed OMT medication at any time during the study period from January 1st 2000 to December 31st 2019.
In Denmark, we included 2,078 females and 6,387 males who had been prescribed OMT medication during the study period at any time from January 2nd 2007 to December 31st 2018. A total of 22 OMT patients who died during the study period were excluded from the analysis because of missing data on either cause or date of death.
Data sources
In Czechia and Denmark, both data on exposure (OMT treatment) and outcome (death) were retrieved from national registers (20). Reporting to these registers is mandatory for the relevant professionals in both countries. A personal identification number is registered for each record, which enables linking data from various health registers at the individual level.
Czechia (21):
The national registry of addiction treatment
The national registry of addiction treatment (NRAT) contains information on patients in OMT, including diagnoses, OMT treatment details, and basic socio-demographic data of all patients.
The information system on deaths
The information system on deaths (ISZEM) is a general mortality register, which includes information on deaths of individuals with permanent or long-term residence in Czechia. The data is based on the information provided in the death certificate. The ISZEM contains the underlying and contributing causes of death based on ICD-10 codes. The data have been available in electronic form since 1994.
Denmark (21):
The Danish registry of drug abusers undergoing treatment
The registry contains information on individuals enrolled in treatment of drug use disorders due to illicit drug use since 1996. The register contains brief socio-demographic information, information on past year drug use, and dates of admission and discharge, and provides information to the european monitoring centre for drugs and drug addiction (EMCDDA) treatment demand indicator.
Cause of death registry
Dates and causes of death were identified using the general mortality register (30) that includes sex, age, and the underlying cause and contributing causes of death based on the ICD-10.
Operationalization of OMT
OMT patients were classified as in treatment or out of treatment. In treatment refers to the period that the individual patient was enrolled in OMT and was eligible to receive OMT medication. Out of treatment refers to the period that the individual patient was in between OMT treatment episodes or between the end of OMT episode and the end of follow-up if no new treatment episode was initiated (Figure 1).
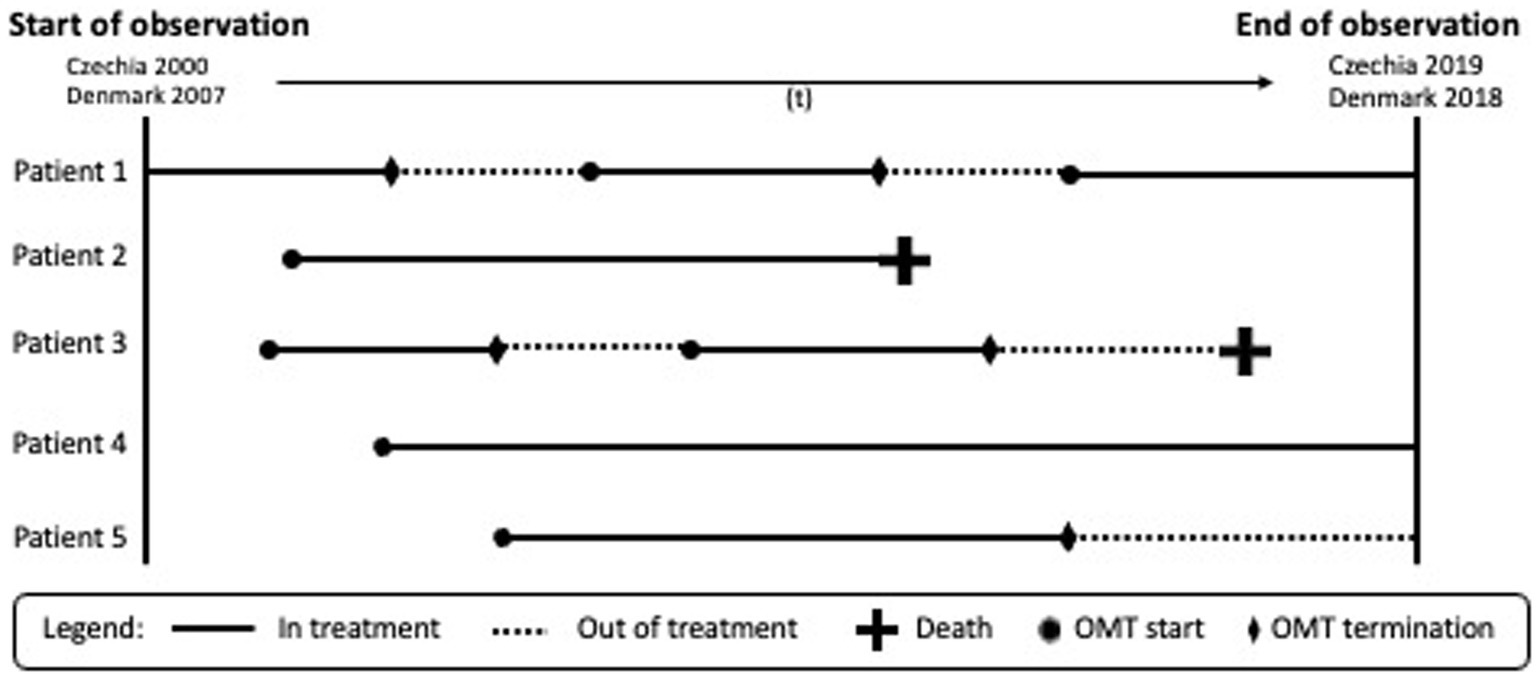
Figure 1. Examples of scenarios of patient trajectories in the opioid maintenance treatment (OMT) used in this study.
Analytic strategy
Statistical procedures included descriptive analyses of both study populations. The crude mortality rates (CMR) and 95% confidence intervals (CI) were calculated as the number of deaths per 1,000 person years (PY) in treatment and out of treatment (31) (see Figure 1). We calculated the time in treatment as the sum of days between treatment start and stop or the end of follow-up (i.e., death or end of observation). Time out of treatment was calculated as the sum of days between discharge from the treatment to the day of enrolment in a new treatment episode or from the treatment stop to the end of follow-up (i.e., death or end of observation).
Based on EMCDDA selection B, overdose was defined as deaths, where the underlying cause was mental and behavioural disorders caused by illicit drug use (dg. F11–F19 without F13, F17 and F18), or accidental, intentional, or undetermined illicit drug poisoning, i.e., a combination of the mechanism of death listed under X or Y with the diagnoses for substance poisoning (dg. T40 and T43.6) (32).
The direct standardization method using EU-27 + EFTA standard population 2011–2030 was employed to standardize for age (33).
The study period was 2000–2019 in Czechia and 2007–2018 in Denmark. Therefore, we performed sensitivity analysis on in treatment and out of treatment CMR in Czechia for the same period as in Denmark (2007–2018).
Statistical analyses were performed using SPSS (version 24) (34) and Stata (version 16) (35).
Ethics statement
Approval from the Ethics committee in Czechia (no. 36/19GrantAZVVES20201.LFUK) has been obtained. In Denmark, ethical evaluation of studies utilizing quality assurance data is not required by law but was approved by the data authority (Journal number: 2013540288, updated March 13th, 2020). No human studies are presented in this manuscript.
Results
In Czechia, 1,580 (30.3%) out of 5,219 OMT patients were females, while 2,078 (24.5%) out of 8,465 OMT patients were females in Denmark (Table 1). The average age at first enrolment in OMT in study periods was more than 10 years lower in the Czech cohort compared with the Danish cohort. In Czechia, the proportion of patients who received methadone or buprenorphine as the initial medication was almost the same (38.4 and 38.7%, respectively), while 22.9% received buprenorphine with naloxone. In Denmark, 79.5% of patients initiated OMT with methadone.
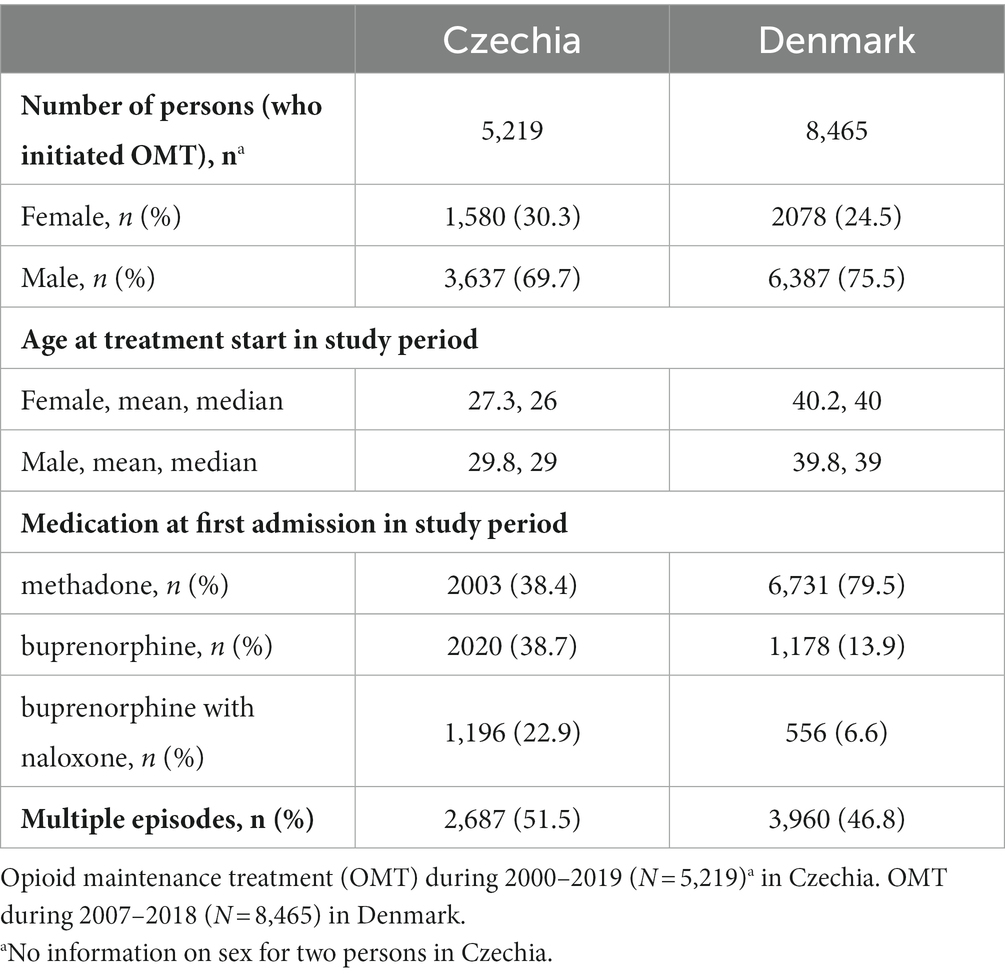
Table 1. Characteristic of the study population.
In Czechia, 8.1% (421) of OMT patients (5,219) died during the study period (Table 2). In Denmark, 18.0% (1,526) of OMT patients (8,465) died during the study period.
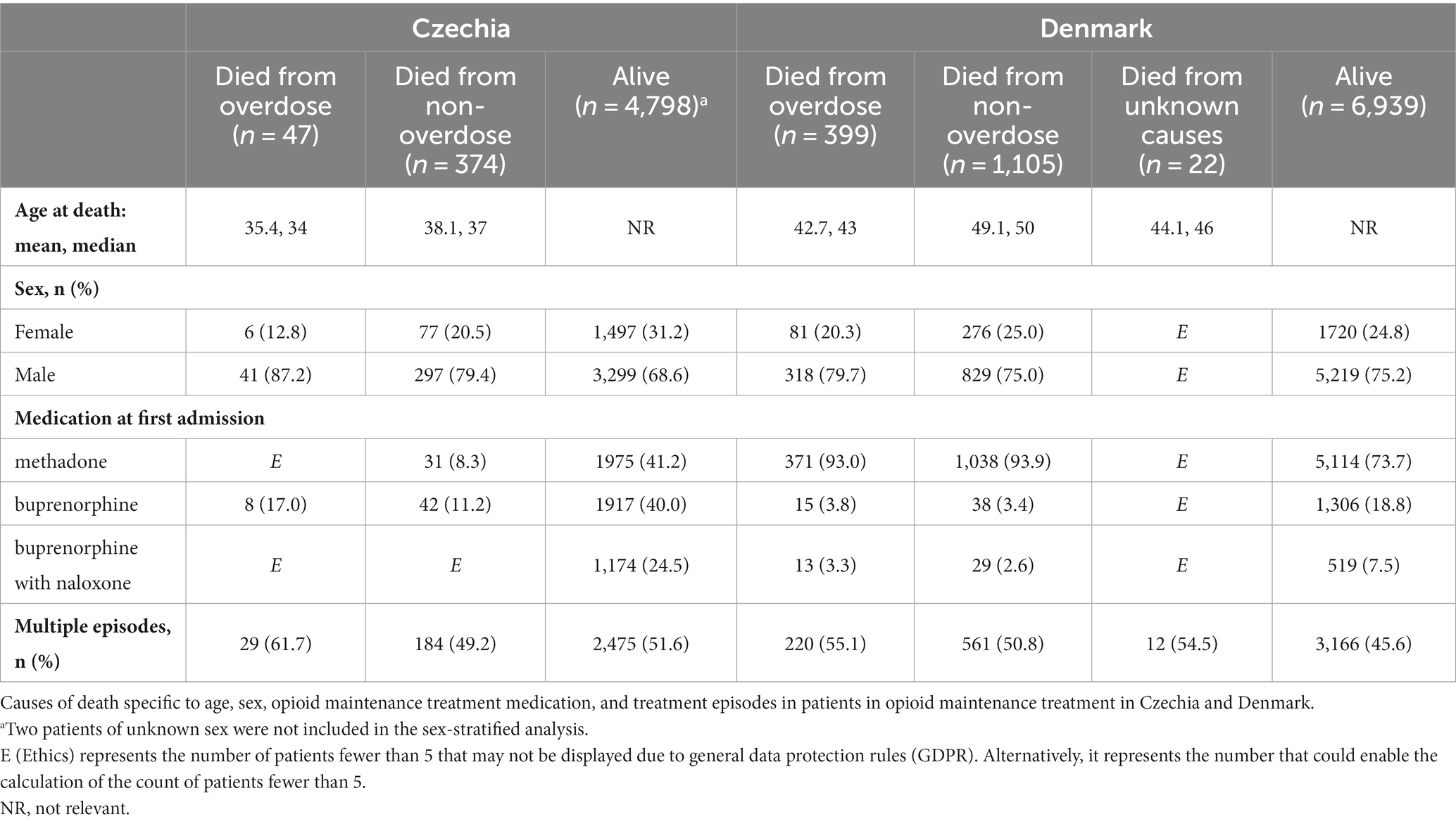
Table 2. Characteristic of study population.
In Czechia, a quarter of all deaths occurred while in treatment, the CMR was 4.3/1,000 PY (females 3.0/1,000 PY, males 4.9/1,000 PY), the all-cause CMR out of treatment was higher (10.8/1,000 PY; females 6.7/1,000 PY, male 12.6/1,000 PY) (Table 3). The proportion of overdose deaths in treatment was 11.3% with an overdose-specific CMR of 0.5/1,000 PY. Overall, there were less than five poisoning by methadone (T40.3) overdose deaths among OMT patients.
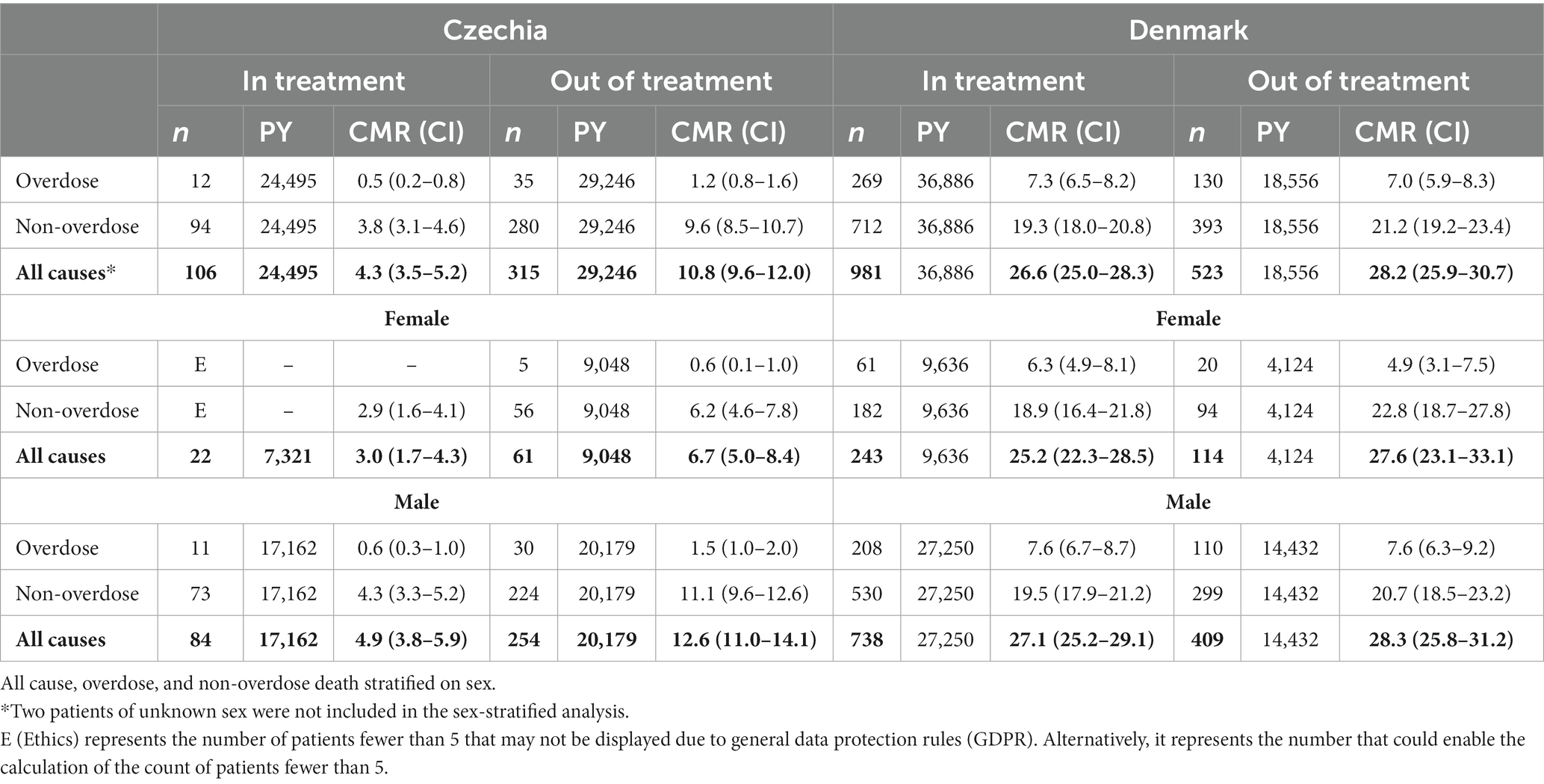
Table 3. Crude mortality rate (CMR) per 1,000 person-years and 95% confidence interval (CI) in treatment and out of treatment in Czechia and in Denmark.
In Denmark, 65.2% of deaths occurred while in treatment. The all-cause CMR in treatment was 26.6/1,000 PY, and out of treatment 28.2/1,000 PY. The proportion of overdose deaths in treatment was 27.4% while overdose-specific CMR was 7.3/1,000 PY. Poisoning by methadone (T40.3) in overdose deaths was found in 63.9% of female and 62.0% of male OMT patients while in treatment as opposed to 40.0% of females and 35.5% of males out of treatment.
In Czechia, all-cause CMR in treatment was quite similar across the types of OMT medication; methadone 3.8/1,000 PY (CI 95% 2.5–5.0), buprenorphine 4.9/1,000 PY (3.5–6.2), buprenorphine with naloxone 4.3/1,000 PY (2.5–6.0).
In Denmark, all-cause CMR in treatment specific to types of OMT medication was the highest for methadone 29.6/1,000 PY (27.8–31.5) and comparable for buprenorphine 8.2/1,000 PY (5.7–11.9) and buprenorphine with naloxone 10.8/1,000 PY (7.2–16.4).
Age-standardized mortality rate for OMT patients in Czechia and Denmark was 9.7/1,000 PY and 29.8/1,000 PY, respectively. Age-standardized overdose mortality rate for OMT patients in Czechia was 0.6/1,000 PY and 5.2/1,000 PY for Denmark.
Sensitivity analysis on CMR in Czechia for the same period as in Denmark (2007–2018) showed similar results as for the longer observation period (2000–2019). In treatment, the CMR was 4.6/1,000 PY (females 2.7/1,000 PY, males 5.4/1,000 PY), while the all-cause CMR out of treatment was (11.6/1,000 PY; females 7.2/1,000 PY, males 13.5/1,000 PY) (Supplementary Table S1).
Discussion
In this large cohort study involving over 13,000 patients ever enrolled in OMT, we found higher mortality rates both in and out of OMT among patients in Denmark than in Czechia. The proportion of overdose deaths while in OMT was nearly 15 times higher among Danish patients than their Czech counterparts. In contrast to previous studies (1), the all-cause mortality rate in Denmark was similar for patients while in OMT as compared to patients while out of OMT. In Czechia, CMR remained consistent across all three OMT medication modalities (methadone, buprenorphine, and buprenorphine with naloxone), while in Denmark, the highest CMR was associated with methadone usage.
The key finding of this study was that the elevated CMR within the Danish OMT cohort was comparable to the rates observed outside of OMT. This pattern held true for both overdose and non-overdose deaths, as well as across both female and male participants. In Czechia, the all-cause mortality rate was more than two times higher out of treatment than in treatment, as has been observed in multiple other settings, such as Norway and Australia (36). Out of treatment mortality was higher for males than females, while the sex difference was not as prominent in treatment. In Denmark, sex differences in mortality were not so pronounced either in or out of treatment.
The population of OMT patients in Denmark was approximately 10 years older on average at the time of enrolment in OMT compared with Czechia. This difference could explain the higher mortality in Denmark. However, even after age standardization of crude mortality rates the differences between mortality rates remained.
The significant differences in overdose deaths between Czechia and Denmark may be attributed to differences in OMT systems. The OMT settings differ markedly in Czechia and Denmark, with the Danish system being more inclusive (9). There may be positive benefits of this more liberal approach, such as the inclusion of a larger proportion of people with OUD who may be severely dependent or less likely to abstain from use of illicit drugs while in OMT as well as an overall higher treatment participation rate. The rate of patients receiving OMT in Denmark was nearly three times higher than that in Czechia (per 1,000 population in 2017) (7). Nevertheless, the unexpectedly elevated rates of both all-cause and overdose mortality rates among Danish OMT patients prompt inquiries into the efficacy of the treatment approach.
Alongside Denmark’s more liberal and inclusive OMT approach, methadone stands out as the most commonly prescribed OMT medication in the country. Patients treated with methadone had both higher all-cause mortality rates in Denmark compared with patients treated with buprenorphine or buprenorphine with naloxone. The pharmacological properties of methadone, a full mu-opioid agonist, might explain at least some of the high overdose mortality rate in patients treated with methadone. Poisoning by methadone in the overdose death group was high both while in treatment (over 60%) and while out of treatment (nearly 40%) in Denmark. The inclusivity of the OMT system in Denmark, along with its minimum requirements for supervised intake of OMT medication, urine testing, or other safety measures (9, 26) combined with the pharmacological properties of methadone, might be linked to this finding. In Denmark, OMT medication can be administered at OMT clinics or dispensed at pharmacies where there is less supervision of intake. A recent Danish cohort study on dispensing of OMT medication at pharmacies highlighted the risks associated with such a practice in the Danish context (23). The study found that after having methadone or buprenorphine dispensed at a pharmacy, adverse outcomes, including all-cause mortality, increased. Thus, this practice may also have contributed to the high in-treatment mortality found in Denmark. In this regard, naloxone, with its pharmacological properties (37), may help to effectively respond to overdoses and overdose deaths (38, 39).
Our findings indicate that there is a potential for improvement in clinical practices by applying a systematic evaluation and monitoring of mortality risk, increased involvement of psychosocial services, and enhanced safety measures to manage overdoses and other health risks. The differences between the Czech and Danish clinical approaches are substantial; one approach focuses more on safety and restrictions while the other focuses more on inclusion and reduced control measures (9, 22, 23). It may be that many patients who relapse to harmful drug use are excluded from treatment in Czechia. Thus, periods of relapse are likely to be more prevalent in treatment in Denmark and more prevalent while out of treatment in Czechia. Expelling patients from treatment while they are experiencing a symptom-intense period or not responding clinically to these symptom-intense situations while patients are in treatment are suboptimal treatment approaches. Thus, the key to lower mortality rates in OMT patients may be found in a more balanced liberalization of the treatment system that both seeks to include people with OUD, despite unstable adherence and periodic excesses in substance use, and to prioritize clinically safe treatment practices, including closer clinical patient monitoring. For example, the move toward more inclusive OMT in Norway has been achieved without an increase in mortality rates (36).
We should not think of the three main features in OMT - access, safety, and quality - as mutually exclusive, but rather as important dimensions of treatment that must be addressed and optimized. This would indeed be in accordance with the Dole, Nyswander, and Kreek recommendations for OMT from the 1960s (40).
Strengths and limitations
This study was unique because we were able to apply similar analytic approaches to study differences in mortality of OMT patients based on a comparison of nation-wide patient cohorts from two countries with different OMT settings. Further, we were able to study mortality rates among those in and out of OMT and while using different OMT medications (methadone, buprenorphine, and buprenorphine with naloxone) by causes of death (overdose, non-overdose), age, and sex. Information about OMT patients was drawn from the nation-wide health and population-based registers in Czechia and Denmark, minimizing selection and information bias. Finally, yet importantly, the information from the registers includes the specific dates for entering, terminating, and re-entering OMT on an individual patient level. Thus, the individual patient follow-up can be precisely calculated with respect to CMR. Additionally, this study provided new information on mortality rates linked to buprenorphine with naloxone.
Our study also had limitations. The main limitation is that some important clinical information was not included in this study (41, 42), including concurrent legal and illegal substance use while in or out of treatment, some demographic and socio-cultural variables in the dataset, or data on OMT medication doses and medication compliance. In general, data from the Czech and Danish registers are highly compatible. However, some types of data were missing. For example, information about 34 Danish patients (29 females) who died and could not be included in the CMR analysis may have resulted in an underestimation of mortality rate in Denmark, especially for females. These individuals were not included in the analyses because we did not have sufficient data on, for instance, cause of death or date of death. In addition, there might be differences in coding of overdose deaths; in Czechia, overdoses may be coded as accidents or self-harm to a greater extent than in Denmark. Finally, the study period in Denmark was between 2007 and 2018 with considerable proportion of patients enrolled in OMT before 2007. This may have resulted in higher age of Danish patients at treatment start in the study period.
Conclusion
We observed significant differences in all-cause and overdose mortality rates in patients while in or out of OMT in Czechia and Denmark. Higher mortality rates were observed across the different types of OMT medication as well as in both sexes in the Danish cohort compared to the Czech cohort. These differences may be attributed to the clinical characteristics in both patient populations and to differences in clinical practice in OMT in the two countries. The findings are indicative and call for more studies on risk factors related to premature mortality as well as risk management.
In Denmark, provision of liberal access to OMT did not necessarily lead to expected reduction in overdose deaths while in treatment. In Czechia, more inclusive clinical practice might lead to higher OMT coverage. Perhaps, a better balance of patient safety and access to OMT would lead to a reduced risk of overdose deaths.
Our study shows how important yet challenging it is to extrapolate mortality estimates from one setting to another and to generalize findings across settings and populations. The findings contribute to the discussion about OMT management and may be of interest to practitioners as well as policy and decision makers when balancing the safety and accessibility of OMT.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: this project uses third-party data derived from State government registries and databases, which are ultimately governed by their ethics committees and data custodians. Thus, any requests to share these data will be subject to formal approval from each data source used in this project. Czechia: Requests for data sharing/case pooling may be directed to the corresponding author RG on email: cm9tYW4uZ2FicmhlbGlrQGxmMS5jdW5pLmN6. Denmark: Requests for data sharing/case pooling may be directed to bWguY3JmQHBzeS5hdS5kaw==. Requests to access these datasets should be directed to cm9tYW4uZ2FicmhlbGlrQGxmMS5jdW5pLmN6; bWguY3JmQHBzeS5hdS5kaw==.
Ethics statement
The studies involving humans were approved by the study has been reviewed and approved by the responsible ethics committee (the respective reference numbers are: 36/19GrantAZVVES20201.LFUK). For Denmark, the project is not under the legislation for ethical evaluation, since it is based entirely on administrative data, but the data has been approved by the data authority (Journal number: 2013540288, updated March 13, 2020). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
SS, RG, and MoH designed the study. SS and BN analyzed the Czech data. MoH and AS analyzed the Danish data. All authors contributed to the interpretation of data, refinement of the paper, read, and approved the final version of the manuscript.
Funding
The study was supported by the Ministry of Health of the Czech Republic, grant no. NU20-09-00066; an umbrella funding for the Centre for Alcohol and Drug Research, provided by the Ministry of The Ministry of Social Affairs, Housing and Senior Citizens, Denmark. Charles University (grant no. Cooperatio-Health sciences/1LF); and by the Research Council of Norway (grant no. 320360).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1179763/full#supplementary-material
References
1. Degenhardt, L, Bucello, C, Mathers, B, Briegleb, C, Ali, H, Hickman, M, et al. Mortality among regular or dependent users of heroin and other opioids: a systematic review and meta-analysis of cohort studies: mortality among opioid users. Addiction. (2011) 106:32–51. doi: 10.1111/j.1360-0443.2010.03140.x
2. Vereinte Nationen, B. für D. und V. (2018). World drug report 2018. Available at: https://www.unodc.org/wdr2018/
3. Compton, WM, and Jones, CM. Epidemiology of the U.S. opioid crisis: the importance of the vector. Ann N Y Acad Sci. (2019) 1451:130–43. doi: 10.1111/nyas.14209
4. Larney, S, Tran, LT, Leung, J, Santo, T, Santomauro, D, Hickman, M, et al. All-cause and cause-specific mortality among people using Extramedical opioids: a systematic review and Meta-analysis. JAMA Psychiatry. (2020) 77:493. doi: 10.1001/jamapsychiatry.2019.4170
5. Degenhardt, L, Larney, S, Randall, D, Burns, L, and Hall, W. Causes of death in a cohort treated for opioid dependence between 1985 and 2005: mortality among opioid-dependent people. Addiction. (2014) 109:90–9. doi: 10.1111/add.12337
6. World Health Organization, International Narcotics Control Board, and United Nations Office on Drugs and Crime. Guidelines for the psychosocially assisted pharmacological treatment of opioid dependence World Health Organization (2009).
7. European Monitoring Centre for Drugs and Drug Addiction. (2021). Balancing access to opioid substitution treatment with preventing the diversion of opioid substitution medications in Europe: challenges and implications. Publications Office. Available at: https://data.europa.eu/doi/10.2810/312876
8. Davoli, M, Amato, L, Clark, N, Farrell, M, Hickman, M, Hill, S, et al. The role of Cochrane reviews in informing international guidelines: a case study of using the grading of recommendations, assessment, development and evaluation system to develop World Health Organization guidelines for the psychosocially assisted pharmac: Cochrane and GRADE for addiction guidelines. Addiction. (2015) 110:891–8. doi: 10.1111/add.12788
9. Tjagvad, C, Skurtveit, S, Linnet, K, Andersen, LV, Christoffersen, DJ, and Clausen, T. Methadone-related overdose deaths in a Liberal opioid maintenance treatment Programme. Eur Addict Res. (2016) 22:249–58. doi: 10.1159/000446429
10. Kourounis, G, Richards, BDW, Kyprianou, E, Symeonidou, E, Malliori, M-M, and Samartzis, L. Opioid substitution therapy: lowering the treatment thresholds. Drug Alcohol Depend. (2016) 161:1–8. doi: 10.1016/j.drugalcdep.2015.12.021
11. Santo, T, Clark, B, Hickman, M, Grebely, J, Campbell, G, Sordo, L, et al. Association of Opioid Agonist Treatment with all-Cause Mortality and Specific Causes of death among people with opioid dependence: a systematic review and Meta-analysis. JAMA Psychiatry. (2021) 78:979. doi: 10.1001/jamapsychiatry.2021.0976
12. Sordo, L, Barrio, G, Bravo, MJ, Indave, BI, Degenhardt, L, Wiessing, L, et al. Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies. BMJ. (2017) j1550. doi: 10.1136/bmj.j1550
13. European Monitoring Centre for Drugs and Drug Addiction. (2017). Health and social responses to drug problems: a European guide. Publications Office. Available at: https://data.europa.eu/doi/10.2810/244934
14. European Monitoring Centre for Drugs and Drug Addiction. (2019). European drug report 2019: trends and developments. Publications Office. Available at: https://data.europa.eu/doi/10.2810/191370
15. Malinovská, J, and Mravčík, V. Problem opioid use in the Czech Republic from a historical perspective: times are changing but opioid pharmaceuticals remain. Adiktologie. (2018) 18:215–22.
16. Thiesen, H, and Hesse, M. Buprenorphine treatment in Denmark. Nordic Stud Alcohol Drugs. (2004) 21:152–5. doi: 10.1177/145507250402101s16
17. Coe, MA, Lofwall, MR, and Walsh, SL. Buprenorphine pharmacology review: update on Transmucosal and long-acting formulations. J Addict Med. (2019) 13:93–103. doi: 10.1097/ADM.0000000000000457
18. Greenwald, MK, Comer, SD, and Fiellin, DA. Buprenorphine maintenance and mu-opioid receptor availability in the treatment of opioid use disorder: implications for clinical use and policy. Drug Alcohol Depend. (2014) 144:1–11. doi: 10.1016/j.drugalcdep.2014.07.035
19. Blazes, CK, and Morrow, JD. Reconsidering the usefulness of adding naloxone to buprenorphine. Front Psych. (2020) 11:549272. doi: 10.3389/fpsyt.2020.549272
20. Hickman, M, Steer, C, Tilling, K, Lim, AG, Marsden, J, Millar, T, et al. The impact of buprenorphine and methadone on mortality: a primary care cohort study in the United Kingdom: burpenorphine vs methadone on mortality risk. Addiction. (2018) 113:1461–76. doi: 10.1111/add.14188
21. Gabrhelík, R, Handal, M, Mravčík, V, Nechanská, B, Tjagvad, C, Thylstrup, B, et al. Opioid maintenance treatment in the Czech Republic, Norway and Denmark: a study protocol of a comparative registry linkage study. BMJ Open. (2021) 11:e047028. doi: 10.1136/bmjopen-2020-047028
22. Chomynová, P, Grohmannová, K, Dvořáková, Z, Rous, Z, and Černíková, T. Souhrnná zpráva o závislostech v České republice 2022 [Summary Report on Addictions in the Czech Republic in 2022]. Praha: Úřad vlády České republiky (2023).
23. Hesse, M, Thylstrup, B, Seid, AK, Tjagvad, C, and Clausen, T. A retrospective cohort study of medication dispensing at pharmacies: administration matters! Drug Alcohol Depend. (2021) 225:108792. doi: 10.1016/j.drugalcdep.2021.108792
24. Ministerstvo zdravotnictví ČR. (2008). Věstník MZ ČR částka 3/2008—Standard substituční léčby [Journal of the Ministry of Health of the Czech Republic issue 3/2008—Standard of substitution treatment]. Available at: https://www.mzcr.cz/wp-content/uploads/wepub/2035/6204/Věstník%2003_2008.pdf
25. Mravčík, V, Janíková, B, Drbohlavová, B, Popov, P, and Pirona, A. The complex relation between access to opioid agonist therapy and diversion of opioid medications: a case example of large-scale misuse of buprenorphine in the Czech Republic. Harm Reduct J. (2018) 15:1. doi: 10.1186/s12954-018-0268-0
26. Frank, VA, Bjerge, B, and Houborg, E. Shifts in opioid substitution treatment policy in Denmark from 2000–2011. Subst Use Misuse. (2013) 48:997–1009. doi: 10.3109/10826084.2013.797838
27. Bjerge, B, Nielsen, B, and Frank, VA. Rationalities of choice and practices of care: substitution treatment in Denmark. Contemp Drug Probl. (2014) 41:57–90. doi: 10.1177/009145091404100104
28. Sundhedsstyrelsen [The Danish Board of Health]. Evaluering af ordning med lægeordineret heroin til stofmisbrugere 2010–2012 [Evaluation of pharmaceutical heroin for people with opioid addiction 2010-2012]. Denmark:Copenhagen. (2013).
29. Thylstrup, B., Schrøder, S., Pedersen, MM., and Ludvigsen, KB. Brugernes tilfredshed med substitutionsbehandlingen [Patients’ satisfaction with Substitution Treatment]. Socialministeriet [The Ministry of Social Services], Denmark:Copenhagen. (2015).
30. Helweg-Larsen, K. The Danish register of causes of death. Scand J Public Health. (2011) 39:26–9. doi: 10.1177/1403494811399958
31. Bukten, A, Skurtveit, S, Waal, H, and Clausen, T. Factors associated with dropout among patients in opioid maintenance treatment (OMT) and predictors of re-entry. A national registry-based study. Addict Behav. (2014) 39:1504–9. doi: 10.1016/j.addbeh.2014.05.007
32. European Monitoring Centre for Drugs and Drug Addiction. (2009). Standard protocol version 3.2 for the EU Member States to collect data and report figures for the Key indicator drug-related deaths. Lisbon, European Monitoring Centre for Drugs and Drug Addiction. Available at: https://www.emcdda.europa.eu/system/files/publications/615/DRD_Standard_Protocol_version_3.2_216365.pdf
33. European Commission. Eurostat. (2013). Revision of the European standard population: Report of Eurostat’s task force: 2013th edition. Publications Office. Available at: https://data.europa.eu/doi/10.2785/11470
36. Bukten, A, Stavseth, MR, and Clasuen, T. From restrictive to more liberal: variations in mortality among patients in opioid maintenance treatment over a 12-year period. BMC Health Serv Res. (2019) 19:553. doi: 10.1186/s12913-019-4382-9
37. Kim, HK, and Nelson, LS. Reducing the harm of opioid overdose with the safe use of naloxone: a pharmacologic review. Expert Opin Drug Saf. (2015) 14:1137–46. doi: 10.1517/14740338.2015.1037274
38. McDonald, R, and Strang, J. Are take-home naloxone programmes effective? Systematic review utilizing application of the Bradford Hill criteria. Addiction. (2016) 111:1177–87. doi: 10.1111/add.13326
39. Moustaqim-Barrette, A, Dhillon, D, Ng, J, Sundvick, K, Ali, F, Elton-Marshall, T, et al. Take-home naloxone programs for suspected opioid overdose in community settings: a scoping umbrella review. BMC Public Health. (2021) 21:597. doi: 10.1186/s12889-021-10497-2
41. Gabrhelík, R, Skurtveit, S, Nechanská, B, Handal, M, Mahic, M, and Mravčík, V. Prenatal methamphetamine exposure and adverse neonatal outcomes: a Nationwide cohort study. Eur Addict Res. (2020) 27:97–106. doi: 10.1159/000509048
42. Mravčík, V, Nechanská, B, Gabrhelík, R, Handal, M, Mahic, M, and Skurtveit, S. Socioeconomic characteristics of women with substance use disorder during pregnancy and neonatal outcomes in their newborns: a national registry study from the Czech Republic. Drug Alcohol Depend. (2020) 209:107933. doi: 10.1016/j.drugalcdep.2020.107933
Keywords: opioid agonist treatment, opioid maintenance treatment, methadone, buprenorphine, buprenorphine with naloxone, treatment outcomes, mortality, registry-based study
Citation: Gabrhelík R, Hesse M, Nechanská B, Handal M, Mravčík V, Tjagvad C, Thylstrup B, Seid AK, Bukten A, Clausen T and Skurtveit S (2023) Large variations in all-cause and overdose mortality among >13,000 patients in and out of opioid maintenance treatment in different settings: a comparative registry linkage study. Front. Public Health. 11:1179763. doi: 10.3389/fpubh.2023.1179763
Edited by:
Barna Konkolÿ Thege, Waypoint Centre for Mental Health Care, CanadaReviewed by:
Máté Kapitány-Fövény, Semmelweis University, HungaryZachary Kasper, Washington University in St. Louis, United States
Copyright © 2023 Gabrhelík, Hesse, Nechanská, Handal, Mravčík, Tjagvad, Thylstrup, Seid, Bukten, Clausen and Skurtveit. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roman Gabrhelík, cm9tYW4uZ2FicmhlbGlrQGxmMS5jdW5pLmN6