
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 25 July 2023
Sec. Public Health and Nutrition
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1166787
 Cristina Bouzas1,2,3
Cristina Bouzas1,2,3 Rosario Pastor2,4
Rosario Pastor2,4 Silvia García1,2,3
Silvia García1,2,3 Margalida Monserrat-Mesquida1,2,3
Margalida Monserrat-Mesquida1,2,3 Miguel Ángel Martínez-González1,5
Miguel Ángel Martínez-González1,5 Jordi Salas-Salvadó1,6
Jordi Salas-Salvadó1,6 Dolores Corella1,7
Dolores Corella1,7 Helmut Schröder8,9J. Alfredo Martínez1,10,11
Helmut Schröder8,9J. Alfredo Martínez1,10,11 Ángel M. Alonso-Gómez1,12Julia Wärnberg1,13
Ángel M. Alonso-Gómez1,12Julia Wärnberg1,13 Jesús Vioque9,14Dora Romaguera1,3
Jesús Vioque9,14Dora Romaguera1,3 José Lopez-Miranda1,15
José Lopez-Miranda1,15 Ramon Estruch1,16
Ramon Estruch1,16 Francisco J. Tinahones1,17
Francisco J. Tinahones1,17 José Lapetra1,18Lluís Serra-Majem1,19
José Lapetra1,18Lluís Serra-Majem1,19 Blanca Riquelme-Gallego9,20
Blanca Riquelme-Gallego9,20 Anny Romero-Secin21,22
Anny Romero-Secin21,22 Xavier Pintó1,23
Xavier Pintó1,23 José J. Gaforio9,24Pilar Matía25Josep Vidal26Miriam Zapatero27
José J. Gaforio9,24Pilar Matía25Josep Vidal26Miriam Zapatero27 Lidia Daimiel28
Lidia Daimiel28 Emilio Ros1,29Ana García-Arellano5,30
Emilio Ros1,29Ana García-Arellano5,30 Nancy Babio1,6Inmaculada Gonzalez-Monje7
Nancy Babio1,6Inmaculada Gonzalez-Monje7 Olga Castañer1,8Itziar Abete1,11Lucas Tojal-Sierra1,12Juan Carlos Benavente-Marín1,13Antonio Signes-Pastor9,14Jadwiga Konieczna1,3Antonio García-Ríos1,15
Olga Castañer1,8Itziar Abete1,11Lucas Tojal-Sierra1,12Juan Carlos Benavente-Marín1,13Antonio Signes-Pastor9,14Jadwiga Konieczna1,3Antonio García-Ríos1,15 Sara Castro-Barquero1,16
Sara Castro-Barquero1,16 José C. Fernández-García1,17José Manuel Santos-Lozano1,18
José C. Fernández-García1,17José Manuel Santos-Lozano1,18 Maira Bes-Rastrollo5Cristina Mestres1,6Patricia Guillem-Saiz1,7Albert Goday1,8Leire Goicolea-Güemez1,12Estanislao Puig-Aguiló31
Maira Bes-Rastrollo5Cristina Mestres1,6Patricia Guillem-Saiz1,7Albert Goday1,8Leire Goicolea-Güemez1,12Estanislao Puig-Aguiló31 Miguel Ruiz-Canela5Antoni Palau-Galindo1,6,32
Miguel Ruiz-Canela5Antoni Palau-Galindo1,6,32 Montse Fitó1,8
Montse Fitó1,8 Josep A. Tur1,2,3* on behalf of the PREDIMED-Plus investigators
Josep A. Tur1,2,3* on behalf of the PREDIMED-Plus investigatorsBackground: A major barrier to a healthy diet may be the higher price of healthy foods compared to low-quality foods.
Objectives: This study aimed to assess the association between the monetary cost of food and diet quality in Spanish older adults at high risk of cardiovascular disease.
Methods: Cross-sectional analysis was carried out in Spanish older adults (n = 6,838; 48.6% female). A validated food frequency questionnaire was used to assess dietary intake. Metabolic syndrome severity, adherence to the Mediterranean diet (MedDiet), adherence to a provegetarian dietary pattern, and dietary inflammatory index were assessed. The economic cost of the foods was obtained from the Spanish Ministry of Agriculture Fisheries and Food database (2015–2017, the period of time when the participants were recruited). The total cost of diet adjusted per 1,000 kcal was computed.
Results: The healthier dietary pattern was associated with a higher cost of the diet. Higher adherence to the MedDiet, anti-inflammatory diet, and the healthy version of the provegetarian dietary pattern were related to higher costs of the diet.
Conclusion: Higher diet quality was associated with a higher dietary cost of the diet per 1,000 kcal/day. Food prices can be an important component of interventions and policies aimed at improving people's diets and preventing diet-related chronic diseases.
Clinical trial registry number: The trial was registered in 2014 at the International Standard Randomized Controlled Trial (ISRCT; http://www.isrctn.com/ISRCTN89898870) with the number 89898870.
The promotion of healthy diets should be part of population strategies to reduce the burden of chronic diseases. Plant-based diets (provegetarian or flexitarian) in which plant-derived foods are preferentially consumed, but not exclusively, have been associated with a lower risk of obesity (1–3), and other diseases, such as type 2 diabetes mellitus (4). An operational definition of a provegetarian diet was initially proposed in the setting of the PREDIMED primary prevention trial, and it was found to be longitudinally associated with lower all-cause mortality (5). The consumption of vegetables, nuts, and whole grains, typical foods of the Mediterranean Diet (MedDiet), was associated with lower levels of inflammation and a lower risk of metabolic syndrome (MetS) (6, 7). An inverse association was also found between adherence to MedDiet and the incidence of the different components of MetS (8, 9). Therefore, the MedDiet has been widely recognized as an optimal eating pattern (balanced, varied, healthy, personalized, appetizing, and functional), and scientific evidence has demonstrated its health benefits, especially in the prevention and control of non-communicable diseases (10–16).
However, a major barrier to eating a healthy diet may be the higher price of these foods. Several studies showed that high adherence to a healthy dietary pattern is associated with higher monetary costs (17–19), and other studies showed that economic constraints lead to the consumption of diets with high energy density (20, 21).
To our knowledge, only one study assessed the association between the cost of diet and the consumption of recommended servings of fruits and vegetables in young adults with MetS (21, 22). However, no studies have been published evaluating the association between diet cost and adherence to MedDiet in older adults with MetS.
This study aimed to assess the association between the monetary cost of food and diet quality in Spanish older non-institutionalized adults with MetS.
A cross-sectional analysis of baseline data of the PREDIMED-Plus trial is shown. The PREDIMED-Plus is an ongoing 6-year, controlled, parallel-group, multicenter, randomized trial conducted in 23 Spanish sites. The trial aimed to assess the effect on cardiovascular disease morbimortality of combined dietary intervention and physical activity. The study protocol can be found at http://predimedplus.com/ (23). The trial was registered at the International Standard Randomized Controlled Trial (ISRCT; http://www.isrctn.com/ISRCTN89898870) with the number 89898870.
Eligible participants were community-dwelling adults aged between 55 and 75 years (60–75 for women), with a body mass index (BMI) between 27 and 40 kg/m2 and meeting at least three MetS criteria according to the updated harmonized definition of the International Diabetes Federation and the American Heart Association and National Heart, Lung, and Blood Institute (23). Exclusion criteria are available elsewhere (24).
A total of 9,677 adults were contacted, of which 6,874 met inclusion/exclusion criteria and were included in the study as illustrated by a flow chart (Figure 1). The institutional review boards of the 23 participating centers approved the study protocol, and all participants provided written informed consent.
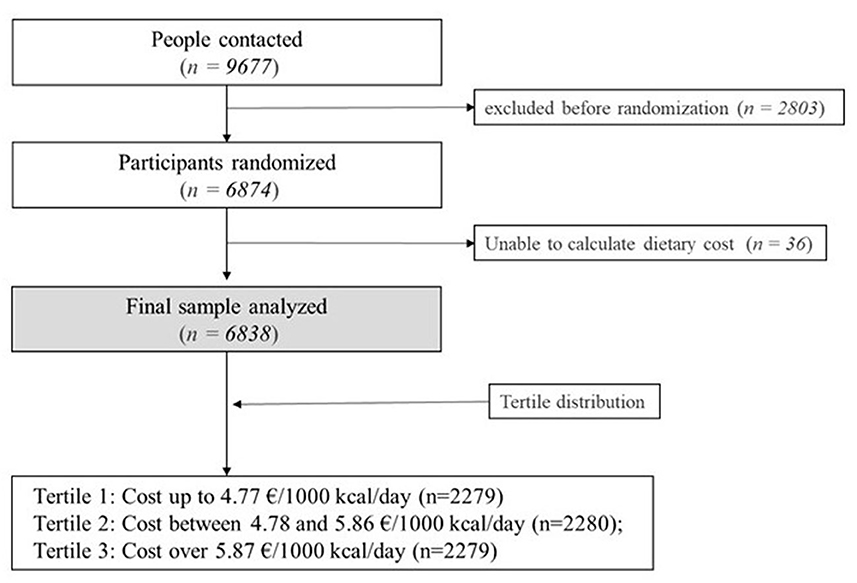
Figure 1. Flow chart of participants.
A validated semi-quantitative 143-item food frequency questionnaire (FFQ) was used to assess dietary intake (https://pubmed.ncbi.nlm.nih.gov/20105389/) (25). Trained dietitians administered in person the questionnaire to participants. For each item, the usual portion size was established, and nine consumption frequencies were available, ranging from “never or almost never” to “≥6 times/day”. Food consumption was obtained by adding grams consumed of each item included in the food group. Diet composition was obtained by multiplying the portion size by the frequency and each by the food composition available in Spanish food composition tables (26).
The Household Consumption Database of the Spanish Ministry of Agriculture, Fisheries and Food (27) was used to obtain food prices, which were handled similarly to a previous study (28). This dataset includes the average prices of each food per month in the Spanish region. It offers the mean price for the region as a whole, including cities and rural areas. The average price of each food item in Spain between 2015 and 2017 was calculated. When an item of the FFQ included several foods, the average was calculated to estimate the cost of the item as a whole. Then, intakes of each food item (in grams or milliliters) were multiplied by its corresponding price in grams.
Then, the price of the diet was further adjusted by energy density to avoid bias due to amount of food consumed. The more food one eats the more the diet costs. Hence, data were adjusted by energy intake as an indicator of both, the amount of food consumed and energy requirements. Therefore, data in this study are expressed in €/1,000 kcal/day.
It was not possible to calculate the economic cost of the diet for 36 subjects, and accordingly, they were excluded. Therefore, 6,838 subjects were included in this study, as shown in Figure 1. For statistical analysis, participants were classified in tertiles according to their cost of the diet per 1,000 kcal (€/1,000 kcal/day). Tertile 1 included participants expending up to 4.77 €/1,000 kcal/day (n = 2,279). Tertile 2 included participants expending between 4.78 and 5.86 €/1,000 kcal/day (n = 2,280). Tertile 3 included participants expending over 5.87 €/1,000 kcal/day (n = 2,279).
Adherence to an energy-reduced MedDiet was assessed by a 17-item Mediterranean diet questionnaire, in which each item is related to a food habit (29). FFQ was used to assess each parameter's intake, and DII was calculated as previously described (30, 31). Negative scores are related to the anti-inflammatory dietary pattern, while positive scores are related to the pro-inflammatory pattern.
Provegetarian dietary patterns were calculated as previously described (32). FFQ was used to assess each parameter's intake. Foods were divided into animal foods, healthy plant foods, and less healthy plant foods. For the assessment of healthy provegetarian food patterns, positive scores were attributed to healthy plant foods, and reverse scores were attributed to the other two groups. For unhealthy provegetarian food patterns, positive scores were attributed to less healthy plant food, and reverse scores to the other two groups. Healthy and unhealthy provegetarian food patterns could both range from 18 to 90.
Sociodemographic data (age, sex, educational level, and marital status), as well as smoking habit, medical history, and current medication, were obtained. Blood pressure was measured in triplicate, in a seated position, with a semi-automatic oscillometer (Omron HEM-705CP, Lake Forest, IL, USA). Overnight fasting blood samples were obtained and analyzed by standard enzymatic methods. Total cholesterol, HDL-cholesterol, triglycerides, and fasting plasma glucose were measured. LDL-cholesterol was calculated according to the Friedewald formula. Abdominal obesity was assessed by measuring the waist circumference halfway between the last rib and the iliac crest using an anthropometric tape. The validated Minnesota-REGICOR short physical activity questionnaire assessed physical activity. The metabolic equivalent of task (MET) was calculated by multiplying the minutes spent in each activity by the intensity of the activity. It is shown as energy expenditure in the article (33).
The metabolic syndrome severity score (MetSSS) was derived from waist circumference, HDL-cholesterol, triglycerides in the blood, blood pressure (systolic and diastolic), and glucose. It was calculated as previously described (34).
Statistical analyses were performed with the Statistical Package for Social Sciences version 28.0 (SPSS Inc., Chicago, IL, USA). Data distribution was assessed by Kolmogorov–Smirnov test. Data were expressed as mean and standard deviation (SD) for quantitative variables and sample size and percentage for categorical variables. A p-value under 0.01 was considered statistically significant. One-way ANOVA and Bonferroni's post hoc analysis were used to assess differences among tertiles of the economic cost of the diet for quantitative variables. Kruskal–Wallis non-parametric tests were also performed for quantitative variables, with Dunn–Bonferroni post hoc analysis (data available in Supplementary material). Differences in prevalence among groups were tested using χ2. Analysis was furthermore adjusted by sex and education, as they appeared to be confounders for some analysis. Sex was only adjusted by education and vice-versa.
Logistic regression was used to assess the association between several dietary patterns/MetSSS (dependent variable) and the economic cost of the diet (€/1,000 kcal/day) (independent variable). Each dependent variable was categorized into two categories. Cutoff points were percentile 50 for healthy and unhealthy provegetarian dietary patterns and for MetSSS. The cutoff for DII was 0, as it is the cutoff for clinical relevance (30). The cutoff for Mediterranean diet adherence was categorized as low-to-medium adherence (scores 0–10) and high adherence (scores 11–17), as previously described (35). For each variable, crude and adjusted odds ratio (OR) were calculated. We estimated OR (95% confidence intervals) for dietary patterns and MetSSS, both adjusted by sex, age, and educational level.
Pearson's correlations between the cost of the diet and adherence to several dietary patterns were performed. Correlation analysis was adjusted by age, sex, and educational level and is shown as several graphs in the Supplementary material.
Table 1 shows sociodemographic characteristics and the incidence of MetS components according to the economic cost of the diet per 1,000 kcal. Female participants, as well as those who live alone, were more likely to expend more money on their diet. Lower energy intakes and higher levels of energy expenditure were related to higher costs of the diet per 1,000 kcal/day. Higher education and non-smokers spent more money on their diet. The cost of the diet was directly associated with hyperglycemia and abdominal obesity prevalence and inversely associated with hypertriglyceridemia and low HDL-cholesterol prevalence.
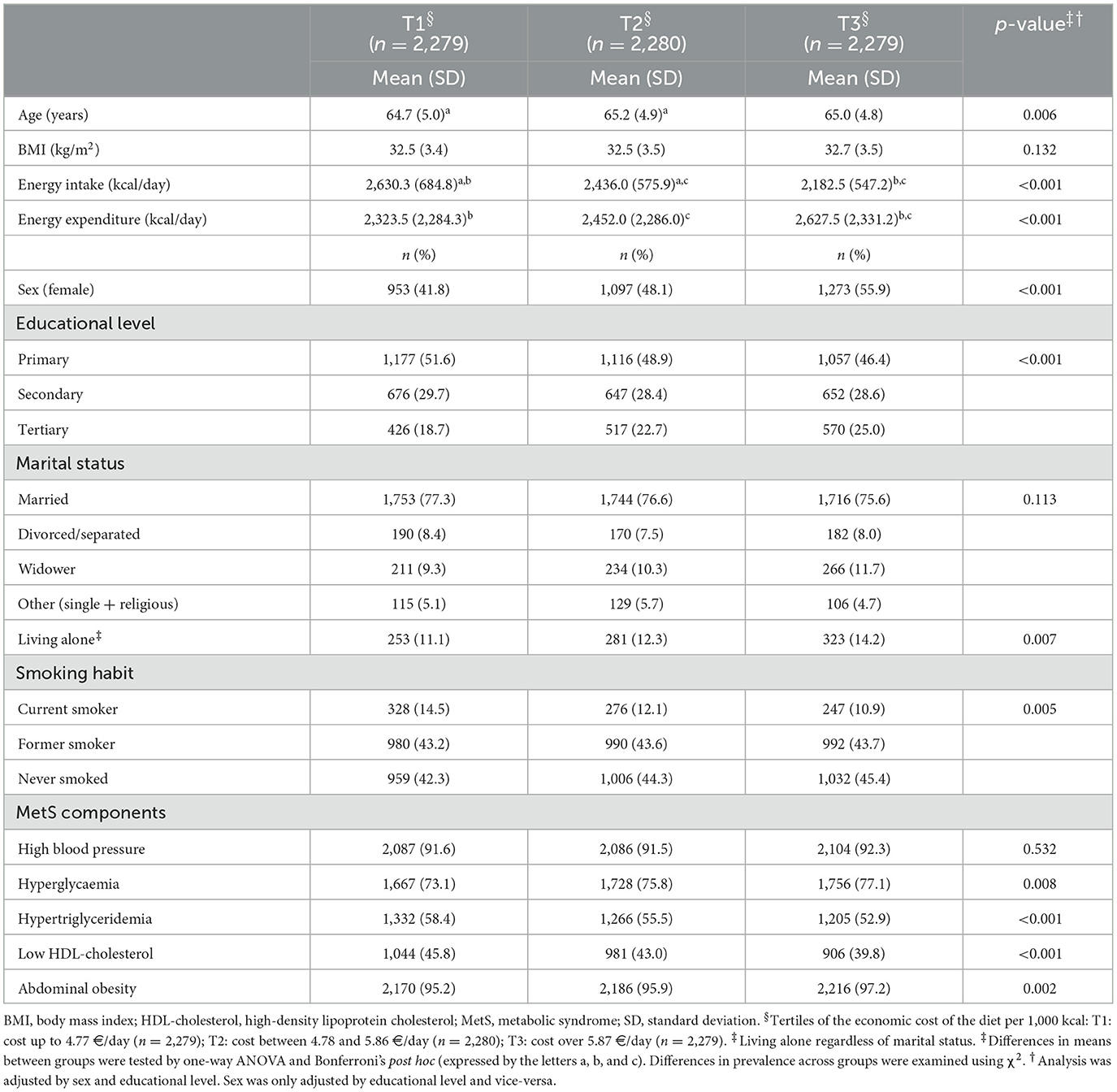
Table 1. Sociodemographic characteristics according to the economic cost of the diet per 1,000 kcal.
Adjusted analysis revealed that sex and educational level were confounder factors for most of the sociodemographic variables. Age, energy intake, and expenditure were not related to the economic cost of the diet after adjustment by either or both variables. Moreover, the adjusted analysis revealed that living alone was only relevant for women and those with a middle education level, whereas smoking habit was relevant in the economic cost of the diet for men and with a low-middle education level. Among MetS parameters, hyperglycemia, hypertriglyceridemia, and abdominal obesity prevalence were more related to the economic cost of the diet only for men, while HDL-cholesterol was related to both sexes. Hypertriglyceridemia, HDL-cholesterol, and abdominal obesity were related to the economic cost of the diet only in the lower levels of education (data not shown).
Food intake according to the cost of the diet is shown in Table 2. The higher cost of the diet was related to a higher intake of fruits and vegetables, whole grains, fish and seafood, white and processed meat, coffee and tea, artificially sweetened beverages, and alcoholic drinks. As the cost of the diet was lower, the intake of several foods was higher: potatoes and refined cereals, eggs, milk and dairy, fats, and oils (including olive oil), sweets and pastries, and convenience foods. Cheaper diets were more energetically dense than more expensive diets.
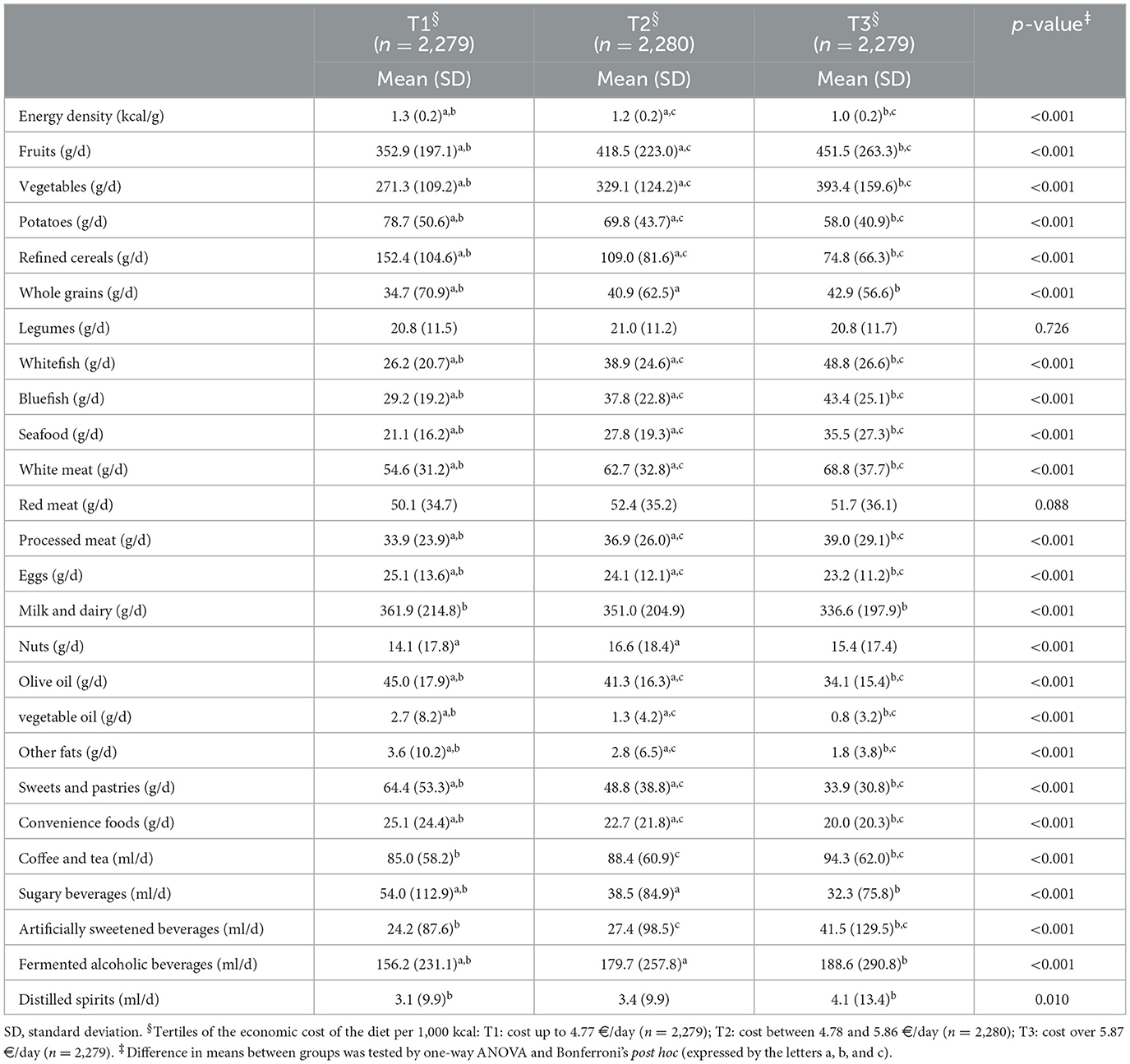
Table 2. Food intake according to the economic cost of the diet per 1000 kcal.
Tables 3, 4 show the association between the cost of the diet and adherence to dietary patterns. As adherence to MedDiet increases, so does the cost of the diet. Accordingly, more anti-inflammatory patterns are related to the higher cost of the diet. More unhealthy plant-based foods were related to the lower cost of the diet. A higher diet quality, measured either by adherence to MedDiet or DII, was associated with a higher economic cost of the diet per 1,000 kcal/day. High adherence to MedDiet and an anti-inflammatory dietary pattern were more likely when the cost of the diet was higher compared to the lower cost [OR (95% CI): MedDiet: T2: 2.05 (1.75–2.40), T3: 3.59 (3.07–4.18), and anti-inflammatory DII: T2: 1.71 (1.52–1.92), T3: 2.37 (2.10–2.67)].
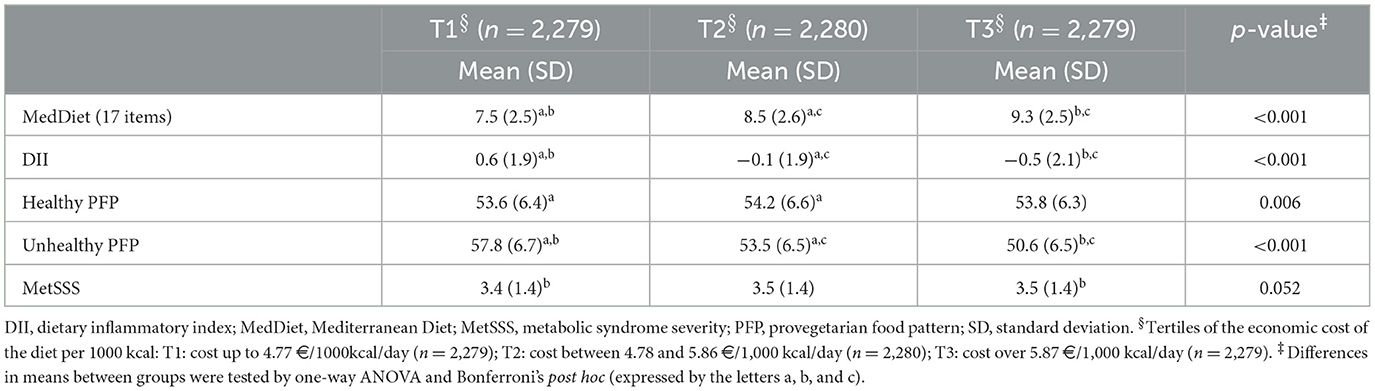
Table 3. Adherence to healthy diets and health status according to the economic cost of the diet per 1,000 kcal.
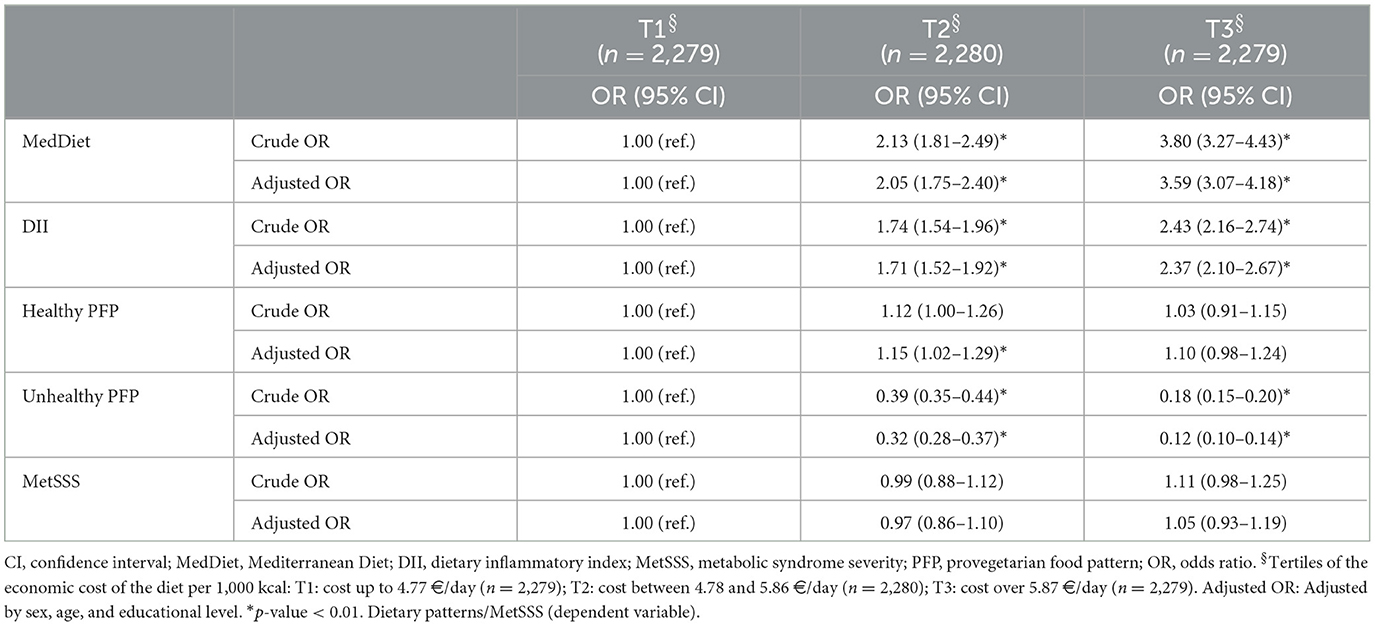
Table 4. Association between adherence to healthy diets and health status and the economic cost of the diet per 1,000 kcal.
Pearson's correlations between the cost of the diet and adherence to several dietary patterns were performed as graphs (see Supplementary material). The cost of the diet positively correlated with MedDiet adherence and inversely correlated with unhealthy provegetarian dietary patterns and with DII. In other words, adherence to MedDiet increased when the cost of the diet increased. As the cost of the diet increased, the unhealthy provegetarian dietary pattern decreased. The inflammatory potential of the diet became more anti-inflammatory when the cost of the diet increased.
Current findings showed that higher diet quality, measured either by adherence to MedDiet, by adherence to a healthy provegetarian dietary pattern, or by a low inflammatory index, was associated with a higher diet cost per 1,000 kcal/day. These results showed in previous studies on the adult population are consistent with those of the current study with older adults, which shows the strength of these findings (36–39).
In addition to other factors that may influence diet quality, such as nutrition knowledge, food accessibility and availability, current results confirm that economic resources, and food prices can be an important component of interventions and policies aimed at improving population diets and preventing diet-related chronic diseases (40, 41). Healthier diets at lower costs could be achieved by purchasing foods in a street market (42).
The scientific literature reflected estimates of savings in medical care that would mean greater adherence to the MedDiet. Thus, in an economic model published in 2019, those results showed that increasing the percentage of the population adhering to MedDiet by 20% produced annual savings in cardiovascular disease-related costs in the United States and Canada. Moreover, when adherence increased to 80%, savings continued to increase proportionately (43).
A positive association between the cost of the adjusted diet per 1,000 kcal and the prevalence of abdominal obesity was also observed. However, the current analysis adjusted for sex and educational level showed that this association was only relevant for men. When the analysis delved into the reasons for this positive association between the prevalence of abdominal obesity and the cost of diet in men, it was found that current participants who were abdominally obese at the beginning of the study consumed higher amounts of processed meats and alcoholic beverages, both fermented and distilled, than those who did not show abdominal obesity (data not shown). Our results show that participants with higher monetary expenditure on foods also had the lowest energy density in their diet. The group with the higher expenditure consumed more alcoholic beverages; however, they also had more fruits, vegetables, and meat, which are products more expensive than others. Furthermore, the “cheaper” diets were more energy dense and included more foods with a high energy density and low nutritional value such as sugary sweetened beverages, sweets, pastries, and convenience foods. When the association between diet cost and some food groups was evaluated, processed meats and alcoholic beverages were associated with higher monetary expenditures. Moreover, it cannot rule out the existence of reverse causation because of the cross-sectional design. A previous study associated protein intake with a higher cost of the diet, regardless of overall diet quality. Nevertheless, the source of the protein consumed seemed to have an impact on diet quality. Animal protein sources with lower salt, saturated fat, and added sugars were associated with higher diet quality (42).
The literature showed that the usual consumption of light to moderate alcoholic beverages, mainly red wine, is associated with a lower risk of total mortality, coronary artery disease, diabetes mellitus, congestive heart failure, and stroke. However, higher levels of alcohol consumption were associated with increased cardiovascular risk (43). Several studies showed that light to moderate alcohol consumption was not associated with increased adiposity, while excessive alcohol consumption was more related to weight gain (44). Previous studies showed a positive association between the consumption of processed meats and the incidence of obesity and central obesity (45).
In a study conducted with Spanish adults in 2016 (46), no positive association was found between the cost of the energy-adjusted diet, weight changes, and BMI, which coincided with those found in this study. The authors then reported an association of increased diet cost with a decrease in body weight and BMI, but these associations were no longer present when the models were adjusted for energy density. Current results are also in agreement with previous findings from a Spanish cohort where participants who spent more money on food adjusted by energy intake had higher BMI (46). On the other hand, a previous study performed in Japan did not find any association between caloric expenditure and the energy-adjusted cost of the diet (47). This was not the case for our participants. The higher the money spent on food (adjusted by energy density), the higher the calories spent on physical activity. Even though this variable was estimated from a questionnaire, a clinically relevant difference was found in that analysis. Socioeconomic status plays a role in health (48, 49), which might explain why people who spend more money on food have more money available because they belong to a higher socioeconomic status. Higher socioeconomic status is also related to higher levels of physical activity (50).
In this study, the cost of the diet was inversely proportional to the prevalence of hypertriglyceridemia and low HDL-cholesterol per 1,000 kcal. The adjusted analysis showed that hypertriglyceridemia was related to the economic cost of diet in men and low levels of education, while HDL-cholesterol was related to the economic cost of diet in both sexes and low educational levels. These results agree with those previously published that showed that lower cardiovascular risk was associated with greater adherence to healthy eating patterns (1–3, 8, 9). The current and previous studies both show that healthy dietary patterns are more expensive.
This study showed that women living alone and subjects with higher education had higher costs of their diet adjusted for 1,000 kcal. The adjusted analysis also revealed that sex and educational level were confounding factors for most of the outcomes. Other previous studies conducted on adults showed the same positive association between diet cost and educational level (51, 52). Published studies also reported sex differences when adjusting the cost of the diet per 1,000 kcal (52–54). However, when the current cost of the diet according to sex without adjusting for energy was assessed, it was observed that men had more dietary expenditure than women (data not shown). This pattern likely reflects that energy intake and diet are related. In this sense, the current results showed that the lower energy intakes were related to a higher cost of the diet per 1,000 kcal, but after the adjustment considering the covariates of sex and education, this relationship ceased to be significant.
Previous studies conducted in children or youth populations associated a healthier diet with a greater cost. The low sociocultural and socioeconomic level of the parents was related to a lower amount of money spent on food, and therefore, to unhealthier diets (48, 49). Healthier and more expensive diets in children were achieved by a varied diet, richer in fish and fruits, with a lower energy density (48). However, this association was true for poor or moderate diet quality, when measured by adherence to MedDiet. Within the range of high diet quality, the cost was similar (49). Therefore, MedDiet can be a dietary pattern easy to maintain and cost-limited when adherence is high.
Finally, the current higher cost of the diet was related to higher consumption of some food characteristics of MedDiet, such as fruits and vegetables, whole grains, and fish and seafood. These results are in line with those shown in previous studies (22, 55). It is important to note that not all foods with high nutrient density have a high cost; so, it is possible to design a diet following the Mediterranean dietary pattern using the lowest monetary cost options in each food group. It should be highlighted the importance of legumes as a good nutrient quality and a low-price food group in the context of a healthy dietary pattern. Moreover, only the healthy provegetarian dietary pattern was not associated with dietary costs, in agreement with a previous study conducted in Spain (56). It was the only index that was not significant, as those participants with the highest adherence to the MedDiet spent on average 1.42 €/day more than those with the poorest adherence.
This study provides information on the monetary costs of the diet and their association with the quality of the diet measured by different indices. Currently, this issue is gaining relevance in public health worldwide, due to the current economic crisis in many Mediterranean countries, with the need for designing nutritional education programs that integrate healthy diets with more profitable options.
The main limitation of this study is that the level of economic income of the participants was not analyzed, so it was not possible to analyze its relationship with the quality of the diet. Such an analysis would have been interesting, as several studies have previously shown, that economic constraints lead to the consumption of less healthy diets that are characterized by high energy density (20, 21). Another limitation was the validity and reliability of dietary consumption data from surveys, being well known for the potential for bias (57–59). Moreover, FFQ does not include all specifications of each product consumed, which only allows us to calculate a median of cost between similar products that match the FFQ category. For example, under the category of sweetened beverages, there are several brands usually consumed and several flavors, which differ in cost. Average prices for Spain between 2015 and 2017 were used because the participants in the study were recruited in this period. A final limitation is that this study was observational and cross-sectional, and its design does not allow for establishing causal inferences; hence, only associations were made.
Higher diet quality, as measured by adherence to the MedDiet or a low inflammatory index, was associated with a higher dietary cost per 1,000 kcal/day. Lower dietary expenditures were associated with a higher prevalence of hypertriglyceridemia and low HDL-cholesterol levels. Therefore, food prices can be an important component of interventions and policies aimed at improving people's diets and preventing diet-related chronic diseases.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Research Ethics Committee from all recruitment centers approved the study protocol, according to the ethical standards of the Declaration of Helsinki. All participants provided written informed consent. All centers have the ethics approval and consent from all the Ethics Committee, and within them, the Ethics Committee of Research of Balearic Islands (ref. CEIC-IB2251/14PI). The patients/participants provided their written informed consent to participate in this study.
CB and RP conducted the statistical analyses and drafted the manuscript. CB, RP, and JT made substantial contributions to the conception and design of the manuscript. All authors contributed substantially to the acquisition of data or analysis and interpretation of data, revised the manuscript critically for important intellectual content, and approved the final version to be published.
The PREDIMED-Plus trial was supported by the European Research Council (Advanced Research Grant 2013–2018, 340918) to MM-G and the official funding agency for biomedical research of the Spanish government, ISCIII, through the Fondo de Investigación para la Salud (FIS), which is co-funded by the European Regional Development Fund (five coordinated FIS projects led by JS-S and JVid, including the following projects: PI13/00673, PI13/00492, PI13/00272, PI13/01123, PI13/00462, PI13/00233, PI13/02184, PI13/00728, PI13/01090, PI13/01056, PI14/01722, PI14/00636, PI14/00618, PI14/00696, PI14/01206, PI14/01919, PI14/00853, PI14/01374, PI14/00972, PI14/00728, PI14/01471, PI16/00473, PI16/00662, PI16/01873, PI16/01094, PI16/00501, PI16/00533, PI16/00381, PI16/00366, PI16/01522, PI16/01120, PI17/00764, PI17/01183, PI17/00855, PI17/01347, PI17/00525, PI17/01827, PI17/00532, PI17/00215, PI17/01441, PI17/00508, PI17/01732, PI17/00926, PI19/00957, PI19/00386, PI19/00309, PI19/01032, PI19/00576, PI19/00017, PI19/01226, PI19/00781, PI19/01560, PI19/01332, PI20/01802, PI20/00138, PI20/01532, PI20/00456, PI20/00339, PI20/00557, PI20/00886, and PI20/01158), the Especial Action Project entitled: Implementación y evaluación de una intervención intensive sobre la actividad física Cohorte PREDIMED-Plus grant to JS-S, the Recercaixa Grant to JS-S (2013ACUP00194), Grants from the Consejería de Salud de la Junta de Andalucía (PI0458/2013, PS0358/2016, and PI0137/2018), a Grant from the Generalitat Valenciana (PROMETEO/2017/017 and PROMETEO 2021/21), a SEMERGEN Grant, EU-COST Action CA16112, Grants (FOLIUM, PRIMUS, SYNERGIA, and LIBERI) from Balearic Islands Health Research Institute (IDISBA), funds from the European Regional Development Fund (CIBEROBN CB06/03 and CB12/03), and from the European Commission (EAT2BENICE_H2020_SFS2016). Fundació La Marató TV3 (project ref. 201630.10). CB received a Margalida Comas Grant and a Juan de la Cierva Grant. The funding sponsors had no role in the design of the study, in the collection, analyses, or interpretation of the data; in the writing of the manuscript; and in the decision to publish the results. JS-S was partially supported by ICREA under the ICREA Academia programme.
The authors especially thank the PREDIMED-Plus participants for their enthusiastic collaboration, the PREDIMED-Plus personnel for outstanding support, and the personnel of all associated primary care centers for their exceptional effort. CIBEROBN, CIBERESP, and CIBERDEM are initiatives of Instituto de Salud Carlos III, Spain. We thank the PREDIMED-Plus Biobank Network, part of the National Biobank Platform of Instituto de Salud Carlos III for storing and managing biological samples.
JS-S reports serving on the board of and receiving grant support through his institution from the International Nut and Dried Fruit Council, and Eroski Foundation. Reports serving in the Executive Committee of the Instituto Danone Spain and on the Scientific Committee of the Danone International Institute. He has received research support from Patrimonio Comunal Olivarero, Spain and Borges SA, Spain. Reports receiving consulting fees or travel expenses from Danone; Eroski Foundation, Instituto Danone, Spain, and Abbot Laboratories.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer MM-A declared a shared affiliation with the author BR-G to the handling editor at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1166787/full#supplementary-material
Supplementary Figure 1. Correlation between dietary cost and MedDiet adherence.
Supplementary Figure 2. Correlation between dietary cost and MedDiet adherence.
Supplementary Figure 3. Correlation between dietary cost and MedDiet adherence.
Supplementary Table 1. Sociodemographic characteristics according to economic cost the diet per 1,000 kcal.
Supplementary Table 2. Food intake according to economic cost of diet per 1,000 kcal.
Supplementary Table 3. Adherence to healthy diets and health status according to economic cost of the diet per 1,000 kcal.
1. Chen Z, Schoufour J, Rivadeneira F, Lamballais S, Ikram M, Franco O, et al. Plant-based diet and adiposity over time in a middle-aged and elderly population: the rotterdam study. Epidemiology. (2019) 30:303–10. doi: 10.1097/EDE.0000000000000961
2. Turner-McGrievy G, Mandes T, Crimarco A. A plant-based diet for overweight and obesity prevention and treatment. J Geriatr Cardiol. (2017) 14:369–74. Available online at: https://www.researchgate.net/publication/317712121_A_plant-based_diet_for_overweight_and_obesity_prevention_and_treatment
3. Huang R, Huang C, Hu F, Chavarro J. Vegetarian Diets and Weight Reduction: a Meta-Analysis of Randomized Controlled Trials. J Gen Intern Med. (2016) 31:109–16. doi: 10.1007/s11606-015-3390-7
4. Chen Z, Zuurmond M, van der Schaft N, Nano J, Wijnhoven A, Ikram M, et al. Plant versus animal based diets and insulin resistance, prediabetes and type 2 diabetes: the Rotterdam Study. Eur J Epidemiol. (2018) 33:883–93. doi: 10.1007/s10654-018-0414-8
5. Martínez-González M, Sánchez-Tainta A, Corella D, Salas-Salvadó J, Ros E, Arós F, et al. A provegetarian food pattern and reduction in total mortality in the Prevención con Dieta Mediterránea (PREDIMED) study. Am J Clin Nutr. (2014) 100:320S−8S. doi: 10.3945/ajcn.113.071431
6. Giugliano D, Ceriello A, Esposito K. The effects of diet on inflammation: emphasis on the metabolic syndrome. J Am Coll Cardiol. (2006) 48:677–85. doi: 10.1016/j.jacc.2006.03.052
7. Ahlwalia N, Andreeva V, Kesse-Guyot E, Hercberg S. Dietary patterns, inflammation and the metabolic syndrome. Diabetes Metab. (2013) 39:99–110. doi: 10.1016/j.diabet.2012.08.007
8. Finicelli M, Squillaro T, Di Cristo F, Di Salle A, Melone M, Galderisi U, et al. Metabolic syndrome, Mediterranean diet, and polyphenols: Evidence and perspectives. J Cell Physiol. (2019) 234:5807–26. doi: 10.1002/jcp.27506
9. Di Daniele N, Noce A, Vidiri M, Moriconi E, Marrone G, Annicchiarico-Petruzzelli M, et al. Impact of Mediterranean diet on metabolic syndrome, cancer and longevity. Oncotarget. (2017) 8:8947–79. doi: 10.18632/oncotarget.13553
10. Martínez-González M, Salas-Salvadó J, Estruch R, Corella D, Fitó M, Ros E. Benefits of the mediterranean diet: insights from the PREDIMED study. Prog Cardiovasc Dis. (2015) 58:50–60. doi: 10.1016/j.pcad.2015.04.003
11. Sofi F, Abbate R, Gensini G, Casini A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: an updated systematic review and meta-analysis. Am J Clin Nutr. (2010) 92:1189–96. doi: 10.3945/ajcn.2010.29673
12. Schröder H. Protective mechanisms of the Mediterranean diet in obesity and type 2. J Nutr Biochem. (2007) 18:149–60. doi: 10.1016/j.jnutbio.2006.05.006
13. Estruch R, Ros E, Salas-Salvadó J, Covas M, Corella D, Arós F, et al. Primary prevention of cardiovascular disease with a mediterranean diet supplemented with extra-virgin olive oil or nuts. N Engl J Med. (2018) 378:e34. doi: 10.1056/NEJMoa1800389
14. Giannini C, Diesse L, D'Adamo E, Chiavaroli V, de Giorgis T, Di lorio C, et al. Influence of the Mediterranean diet on carotid intima-media thickness in hypercholesterolaemic children: a 12-month intervention study. Nutr Metab Cardiovasc Dis. (2014) 24:75–82. doi: 10.1016/j.numecd.2013.04.005
15. Salas-Salvadó J, Fernández-Ballart J, Ros E, Martínez-González M, Fitó M, Estruch R, et al. Effect of a Mediterranean diet supplemented with nuts on metabolic syndrome status: one-year results of the PREDIMED randomized trial. Arch Intern Med. (2008) 168:2449–58. doi: 10.1001/archinte.168.22.2449
16. Dijkstra S, Neter J, van Stralen M, Knol D, Brouwer I, Huisman M, et al. The role of perceived barriers in explaining socio-economic status differences in adherence to the fruit, vegetable and fish guidelines in older adults: a mediation study. Public Health Nutr. (2015) 18:797–808. doi: 10.1017/S1368980014001487
17. Monsivais P, Scarborough P, Lloyd T, Mizdrak A, Luben R, Mulligan A, et al. Greater accordance with the Dietary Approaches to Stop Hypertension dietary pattern is associated with lower diet-related greenhouse gas production but higher dietary costs in the United Kingdom. Am J Clin Nutr. (2015) 102:138–45. doi: 10.3945/ajcn.114.090639
18. Bukambu E, Lieffers JRL, Ekwaru JP, Veugelers PJ, Ohinmaa A. The association between the cost and quality of diets of children in Canada. Can J Public Health. (2020) 111:269–77. doi: 10.17269/s41997-019-00264-7
19. Darmon N, Briend A, Drewnowski A. Energy-dense diets are associated with lower diet costs: a community study of French adults. Public Health Nutr. (2004) 7:21–7. doi: 10.1079/PHN2003512
20. Drewnowski A, Darmon N. The economics of obesity: dietary energy density and energy cost. Am J Clin Nutri. (2005) 8:265S−73S. doi: 10.1093/ajcn.82.1.265S
21. Carlson A, Dong D. Association between total diet cost and diet quality is limited. J Agric Res Econom. (2014) 39:47–68. doi: 10.22004/ag.econ.168259
22. Clark R, Famodu O, Barr M, Hagedorn R, Ruseski J, White J, et al. Monetary cost of the myplate diet in young adults: higher expenses associated with increased fruit and vegetable consumption. J Nutr Metab. (2019) 2019:2790963. doi: 10.1155/2019/2790963
23. Martínez-González M, Buil-Cosiales P, Corella D, Bulló M, Fitó M, Vioque J, et al. Cohort profile: design and methods of the PREDIMED-Plus randomized trial. Int J Epidemiol. (2019) 48:387–388. doi: 10.1093/ije/dyy225
24. Alberti K, Grundy S, Zimmet P, Cleeman J, Donato K, Fruchart J, et al. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; National heart, lung, and blood institute; American heart association; World heart federation; International. Pratice Guideline. (2009) 120:1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644
25. Fernández-Ballart J, Piñol J, Zazpe I, Corella D, Carrasco P, Toledo E, et al. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br J Nutr. (2010) 103:1808–18016. doi: 10.1017/S0007114509993837
26. Moreiras O, Cabrera L, Cuadrado C. Tablas de Composición de alimentos (Spanish Food Composition Tables). 17th ed Madrid: Pirámide. (2015).
27. Ministerio de, Agricultura, Pesca y, Alimentación. Base de Datos de Consumo en Hogares. Available online at: https://www.mapa.gob.es/app/consumo-en-hogares/consulta11.asp (accessed July 15, 2022).
28. de Mello AV, Sarti FM, Fisberg RM. How to estimate food prices and diet costs in population-based studies? Front Nutr. (2021) 8:728553. doi: 10.3389/fnut.2021.728553
29. Schröder H, Zomeño MD, Martínez-González MA, Salas-Salvadó J, Corella D, Vioque J, et al. Validity of the energy-restricted Mediterranean Diet Adherence Screener. Clin Nutr. (2021) 40:4971–9. doi: 10.1016/j.clnu.2021.06.030
30. Ruiz-Canela M, Bes-Rastrollo M, Martínez-González MA. The role of dietary inflammatory index in cardiovascular disease, metabolic syndrome and mortality. Int J Mol Sci. (2016) 17:1265. doi: 10.3390/ijms17081265
31. Bouzas C, Bibiloni M, Garcia S, Mateos D, Martínez-González M, Salas-salvadó J, et al. Desired weight loss and its association with health, health behaviors and perceptions in an adult population with weight excess: One-year follow-up. Front Nutr. (2022) 9:848055. doi: 10.3389/fnut.2022.848055
32. Gómez-Donoso C, Martínez-González M, Martínez J, Gea A, Sanz-Serrano J, Perez-Cueto F, et al. Provegetarian food pattern emphasizing preference for healthy plant-derived foods reduces the risk of overweight/obesity in the SUN cohort. Nutrients. (2019) 11:1553. doi: 10.3390/nu11071553
33. Molina L, Sarmiento M, Peñafiel J, Donaire D, Garcia-Aymerich J, Gomez M, et al. Validation of the regicor short physical activity questionnaire for the adult population. PLoS ONE. (2017) 12:e0168148. doi: 10.1371/journal.pone.0168148
34. Wiley J, Carrington M. A metabolic syndrome severity score: A tool to quantify cardio-metabolic risk factors. Prev Med. (2016) 88:188–95. doi: 10.1016/j.ypmed.2016.04.006
35. Galilea-Zabalza I, Buil-Cosiales P, Salas-Salvadó J, Toledo E, Ortega-Azorín C, Díez-Espino J, et al. Mediterranean diet and quality of life: Baseline cross-sectional analysis of the PREDIMED-PLUS trial. PLoS ONE. (2018) 13:e0198974. doi: 10.1371/journal.pone.0198974
36. Mackenbach J, Dijstra S, Dijkstra S, Beulens J, Seidell J, Snijder M, et al. Socioeconomic and ethnic differences in the relation between dietary costs and dietary quality: the HELIUS study. Nutr J. (2019) 18:21. doi: 10.1186/s12937-019-0445-3
37. Rubini A, Vilaplana-Prieto C, Yeguas-Rosa L, Hernández-González M, Félix-García F, Félix-redondo F, et al. Assessment of the cost of the mediterranean diet in a low-income region: adherence and relationship with available incomes. BMC Public Health. (2022) 22:58. doi: 10.1186/s12889-022-12583-5
38. Schröder H, Marrugat J, Covas M. High monetary costs of dietary patterns associated with lower body mass index: a population-based study. Int J Obes (Lond). (2006) 30:1574–9. doi: 10.1038/sj.ijo.0803308
39. López C, Martínez-González M, Sánchez-Villejas A, Alonso A, Pimenta A, Bes-Rastrollo M. Costs of Mediterranean and western dietary patterns in a Spanish cohort and their relationship with prospective weight change. J Epidemiol Community Health. (2009) 63:920–7. doi: 10.1136/jech.2008.081208
40. Mozaffarian D, Angell S, Lang T, Rivera J. Role of government policy in nutrition-barriers to and opportunities for healthier eating. BMJ. (2018) 361:k2426. doi: 10.1136/bmj.k2426
41. Eyles H, Mhurchu C, Nghiem N, Blakely T. Food pricing strategies, population diets, and non-communicable disease: a systematic review of simulation studies. PLoS Med. (2012) 9:e1001353. doi: 10.1371/journal.pmed.1001353
42. de Mello AV, Sarti FM, Barros MBA, Goldbaum M, Cesar CLG, Fisberg RM. Differences in cost-effectiveness of adherence to nutritional recommendations: why, where, and what? Int J Environ Res Public Health. (2022) 20:772. doi: 10.3390/ijerph20010772
43. Jones J, Abdullah M, Wood D, Jones P. Economic modeling for improved prediction of saving estimates in healthcare costs from consumption of healthy foods: the Mediterranean-style diet case study. Food Nutr Res. (2019) 63:3418. doi: 10.29219/fnr.v63.3418
44. O'Keefe J, Bhatti S, DiNicolantonio J, Lavie C. Alcohol and cardiovascular health: the dose makes the poison…or the remedy. Mayo Clin Proc. (2014) 89:382–393. doi: 10.1016/j.mayocp.2013.11.005
45. Traversy G, Chaput J. Alcohol consumption and obesity: an update. Curr Obes Rep. (2015) 4:122–30. doi: 10.1007/s13679-014-0129-4
46. Schelesinger S, Neuenschwander M, Schwedhelm C, Hoffman G, Bechthold A, Boeing H, et al. Food groups and risk of overweight, obesity, and weight gain: a systematic review and dose-response meta-analysis of prospective studies. Adv Nutr. (2019) 10:205–18. doi: 10.1093/advances/nmy092
47. Schröeder H, Serra-Majen L, Subirana I, Izquierdo-Pulido M, Fitó M, Elousa R. Association of increased monetary cost of dietary intake, diet quality and weight management in Spanish adults. Br J Nutr. (2016) 115:817–22. doi: 10.1017/S0007114515005048
48. Murakami K Sasaki S Takahashi Y Uenishi K Japan Dietetic Students' Study for Nutrition and Biomarkers Group. Monetary cost of self-reported diet in relation to biomarker-based estimates of nutrient intake in young Japanese women. Public Health Nutr. (2009) 12:1290–7. doi: 10.1017/S1368980008003923
49. Rydén PJ, Hagfors L. Diet cost, diet quality and socio-economic position: how are they related and what contributes to differences in diet costs? Public Health Nutr. (2011) 14:1680–92. doi: 10.1017/S1368980010003642
50. Schröder H, Gomez SF, Ribas-Barba L, Pérez-Rodrigo C, Bawaked RA, Fíto M, et al. Monetary diet cost, diet quality, and parental socioeconomic status in spanish youth. PLoS ONE. (2016) 11:e0161422. doi: 10.1371/journal.pone.0161422
51. Jerome GJ, Boyer WR, Bustamante EE, Kariuki J, Lopez-Jimenez F., Paluch AE., et al. Increasing equity of physical activity promotion for optimal cardiovascular health in adults: a scientific statement from the American Heart Association. Circulation. (2023) 10:1951–1962. doi: 10.1161/CIR.0000000000001148
52. Okubo H, Murakami K, Sasaki S. Monetary value of self-reported diets and associations with sociodemographic characteristics and dietary intake among Japanese adults: analysis of nationally representative surveys. Public Health Nutr. (2016) 19:3306–18. doi: 10.1017/S1368980016001695
53. Timmis K, Hulme C, Cade J. The monetary value of diets consumed by British adults: an exploration into sociodemographic differences in individual-level diet costs. Public Health Nutr. (2015) 18:151–9. doi: 10.1017/S1368980013002905
54. Maillot M, Darmon N, Vieux F, Drewnowski A. Low energy density and high nutritional quality are each associated with higher diet costs in French adults. Am J Clin Nutr. (2007) 86:690–6.
55. Monsivais P, Drewnowski A. Lower-energy-density diets are associated with higher monetary costs per kilocalorie and are consumed by women of higher socioeconomic status. J Am Diet Assoc. (2009) 109:814–22. doi: 10.1016/j.jada.2009.02.002
56. Fresán U, Martínez-González MA, Segovia-Siapco G, Sabaté J, Bes-Rastrollo M. A three-dimensional dietary index (nutritional quality, environment and price) and reduced mortality: The “Seguimiento Universidad de Navarra” cohort. Prev Med. (2020) 137:106124. doi: 10.1016/j.ypmed.2020.106124
57. Fresán U, Martínez-González MA, Sabaté J, Bes-Rastrollo M. Global sustainability (health, environment and monetary costs) of three dietary patterns: results from a Spanish cohort (the SUN project). BMJ Open. (2019) 9:e021541. doi: 10.1136/bmjopen-2018-021541
58. Arija V, Abellana R, Ribot B, Ramón JM. Biases and adjustments in nutritional assessments from dietary questionnaires. Nutr Hosp. (2015) 31:113–8. doi: 10.3305/nh.2015.31.sup3.8759
Keywords: monetary cost, Mediterranean diet, provegetarian dietary pattern, dietary inflammatory index, metabolic syndrome
Citation: Bouzas C, Pastor R, García S, Monserrat-Mesquida M, Martínez-González MÁ, Salas-Salvadó J, Corella D, Schröder H, Martínez JA, Alonso-Gómez ÁM, Wärnberg J, Vioque J, Romaguera D, Lopez-Miranda J, Estruch R, Tinahones FJ, Lapetra J, Serra-Majem L, Riquelme-Gallego B, Romero-Secin A, Pintó X, Gaforio JJ, Matía P, Vidal J, Zapatero M, Daimiel L, Ros E, García-Arellano A, Babio N, Gonzalez-Monje I, Castañer O, Abete I, Tojal-Sierra L, Benavente-Marín JC, Signes-Pastor A, Konieczna J, García-Ríos A, Castro-Barquero S, Fernández-García JC, Santos-Lozano JM, Bes-Rastrollo M, Mestres C, Guillem-Saiz P, Goday A, Goicolea-Güemez L, Puig-Aguiló E, Ruiz-Canela M, Palau-Galindo A, Fitó M and Tur JA (2023) Association of monetary diet cost of foods and diet quality in Spanish older adults. Front. Public Health 11:1166787. doi: 10.3389/fpubh.2023.1166787
Received: 16 February 2023; Accepted: 26 June 2023;
Published: 25 July 2023.
Edited by:
Flavia Mori Sarti, University of São Paulo, BrazilReviewed by:
Miguel Mariscal-Arcas, University of Granada, SpainCopyright © 2023 Bouzas, Pastor, García, Monserrat-Mesquida, Martínez-González, Salas-Salvadó, Corella, Schröder, Martínez, Alonso-Gómez, Wärnberg, Vioque, Romaguera, Lopez-Miranda, Estruch, Tinahones, Lapetra, Serra-Majem, Riquelme-Gallego, Romero-Secin, Pintó, Gaforio, Matía, Vidal, Zapatero, Daimiel, Ros, García-Arellano, Babio, Gonzalez-Monje, Castañer, Abete, Tojal-Sierra, Benavente-Marín, Signes-Pastor, Konieczna, García-Ríos, Castro-Barquero, Fernández-García, Santos-Lozano, Bes-Rastrollo, Mestres, Guillem-Saiz, Goday, Goicolea-Güemez, Puig-Aguiló, Ruiz-Canela, Palau-Galindo, Fitó and Tur. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Josep A. Tur, cGVwLnR1ckB1aWIuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.