
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 14 September 2023
Sec. Disaster and Emergency Medicine
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1166317
 Andrea Duarte-Díaz1,2†
Andrea Duarte-Díaz1,2† Mariana Aparicio Betancourt3,4*†
Mariana Aparicio Betancourt3,4*† Laura Seils3
Laura Seils3 Carola Orrego2,3,4
Carola Orrego2,3,4 Lilisbeth Perestelo-Pérez2,5
Lilisbeth Perestelo-Pérez2,5 Jaime Barrio-Cortes6,7,8
Jaime Barrio-Cortes6,7,8 María Teresa Beca-Martínez8
María Teresa Beca-Martínez8 Carlos Jesús Bermejo-Caja9,10
Carlos Jesús Bermejo-Caja9,10 Ana Isabel González-González2,6,11
Ana Isabel González-González2,6,11Introduction: Identifying stakeholders’ needs is crucial to informing decisions and policy development. This study aims to identify healthcare and social-related needs and effective strategies associated with COVID-19 from the first-person perspectives of patients and healthcare providers.
Methods: Cross-sectional online survey design including qualitative open-ended questions, conducted in primary care and hospital settings across Spain, with 12 out of 19 regions represented. Adults aged 18 years and older, who (a) resided in Spain and had a history of COVID-19 or (b) worked as healthcare providers delivering direct or indirect care for people with COVID-19 in Spanish primary care or hospitals during 2020 were eligible to participate. Recruitment was conducted via social-media networks (Twitter, LinkedIn, and WhatsApp) and communication channels of key organizations including patient and professional associations and groups. A total of 182 people were invited to complete the surveys and 76 people completed the surveys (71% women), of which 33 were home-isolated patients, 14 were hospitalized patients, 16 were primary care professionals, and 13 were hospital care professionals.
Results: A total of 327 needs and 86 effective strategies and positive aspects were identified across surveys and classified into the following overarching themes: (i) Accessibility, (ii) Basic needs, (iii) Clinical care, (iv) Person-and-family centered care, (v) Caring for the healthcare professional, (vi) Protocolization, information, health campaigns, and education, (vii) Resource availability, (viii) and Organizational needs/strategies.
Discussion: Findings indicate the Spanish health and social care systems were generally unprepared to combat COVID-19. Implications for research, practice, and policy focus on integrating first-person perspectives as best practice to identify, prioritize and address needs to increase health and social care systems capacity and preparedness, as well as providing well-co-coordinated responses across government, healthcare, and non-government sectors to promote and protect the physical and mental health of all.
The new coronavirus infectious disease (COVID-19) was first reported on December 2019, in Wuhan, China. The World Health Organization (WHO) declared the outbreak a pandemic shortly after, on March 11, 2020, because of the quick spread and severity of the disease (1, 2). The disease burden and mortality, the worsening of mental health and well-being, the delay of necessary and urgent care, and the acute economic paralysis caused by COVID-19, placed great pressure on society, public health and health systems (3–7).
The global health, social and economic crisis that ensued, exposed deficiencies in health systems and tested their public health preparedness and response capacity (8–10). The unprecedented nature of this novel coronavirus impacted the capacity of health systems to respond to the pandemic rapidly and effectively, with adequate personnel, equipment, medicines, and facilities (11–13). Limited or inadequate resources and ineffective public health policies, financial instability, and health information and communication challenges, impacted appropriate service delivery, particularly affecting the workforce, patients, and their family members (14).
The SARS-CoV-2 virus spread rapidly in Spain (15), one of Europe’s most affected countries, with 3,898,035 cases and 370,489 deaths notified as of July 7, 2021 (16). The first confirmed patient was diagnosed on January 31, 2020 (17) and by March 14, 2020, cases were confirmed in all Spanish regions. Spain declared a state of alarm on March 14, 2020, and introduced a hard nation-wide lockdown. By late-March 2020, hospitals were overwhelmed with COVID-19 patients, and intensive care units (ICU) in Catalunya, Comunidad de Madrid, Castilla-La Mancha, and Castilla y León were almost at full capacity, despite efforts to outnumber beds available. The burden of confirmed cases in ICUs was as high as in Italy and far above any other European countries (18). To combat the spread of the virus, on March 30, 2020 all non-essential workers were ordered to remain at home. On April 2, 2020, almost 1,000 people died due to COVID-19 in only 24 h, the highest number reached in one day (19). Health facilities in the worst affected regions were struggling, with ICUs still reaching capacity, an overall deficit in bed capacity, and insufficient number of health professionals, personal protective equipment (PPE) and ventilators. Catalunya, Comunidad de Madrid and other Spanish regions canceled non-emergency surgery and delayed non-COVID-19 urgent and follow-up care in primary care and hospitals because they were overwhelmed. COVID-19 telephone helplines collapsed in some regions. Healthcare professionals were redeployed, medical students were recruited, and retired healthcare workers were urged to return to work due to personnel shortages. In addition, the Spanish government took control of private health services, and military installations and hotels were used for public health purposes (15). The health crisis, along with public health safety measures introduced, such as social distancing, stay-at-home-orders, or school closures, severely impacted health professionals, as well as patients and their families (20).
In early-mid April, the number of patients in ICUs started to decrease in several Spanish regions including Comunidad de Madrid, Castilla-La Mancha, Principado de Asturias and Galicia (19). By mid-May 2020, the daily death count had fallen below 100 patients, and June 1, 2020 was the first day without deaths by COVID-19. Spanish health systems started to recover their normal functioning during June and the state of alarm regulations ended on June 21, 2020 (19).
The strict regulations enforced during the pandemic, however, affected the Spanish society and health system beyond the immediate impact of disease and deaths. This resulted in a decrease in the quality of health services and person-centered care, as well as extensive job losses and hardship, all of which caused a health, social, and economic critical situation (21, 22).
Given the profound multilevel impact of the pandemic, identifying and addressing COVID-19-related needs is warranted. This work is part of a larger COVID-19 needs project that seeks to explore healthcare and social-related needs during the care pathway of people with a history of COVID-19 to inform policy-making, clinical practice, and future research. The present study addresses the need elucidated by our previous work (14) to identify needs associated with COVID-19 from first-person perspectives. Here we aim to identify healthcare and social-related needs and effective strategies associated with COVID-19 from the perspective of patients and the healthcare providers involved in their care, in primary and hospital care settings in Spain.
A cross-sectional online survey design including qualitative open-ended questions was used to identify COVID-19 healthcare and social-related needs and effective strategies in Spain from the perspective of patients and healthcare providers.
Adults aged 18 years and older who (a) resided in Spain and had a history of COVID-19 and required home isolation or hospital admission, and/or (b) worked as healthcare providers, delivering direct or indirect care for people with COVID-19, in Spanish primary care or hospitals during 2020, were eligible to participate in this study. Participants were excluded if they were unable or refused to provide informed consent.
Four ad hoc surveys using open-ended questions were designed by the research team, targeting (1) people with a history of COVID-19 isolated at home, (2) people with a history of COVID-19 who were hospitalized, (3) primary care professionals involved in the care of people with COVID-19, and (4) hospital care professionals involved in the care of people with COVID-19. Surveys were designed based on the healthcare and social-related needs associated with COVID-19 identified after the literature review conducted by our research team (14), a patient perspective, and the expert opinion of the research team, a multidisciplinary team representing the following disciplines: psychology, speech-language pathology, physical therapy, nursing, medicine, neuroscience, quality improvement, patient safety, and healthcare administration. Each survey consisted of three main sections: Informed consent, sociodemographic questions, and a set of four to six qualitative open-ended questions allowing participants to provide detailed responses related to difficulties, areas for improvement, or unmet needs throughout the patient care pathway, as well as an additional question related to effective strategies and positive aspects. Professionals’ surveys included two additional questions related to their work and personal environment. Stages and categories captured by the open-ended questions varied by survey and are listed in Table 1. Prior to distribution, the surveys were iteratively reviewed by the research team. Surveys were developed with SurveyMonkey® and distributed via email. Surveys were designed so participants had to answer each question in a section before proceeding to the next section to ensure there was no missing data from skipped questions. Each survey lasted approximately 10–20 min (Supplementary material S1 provides the Spanish to English translated survey questionnaires).
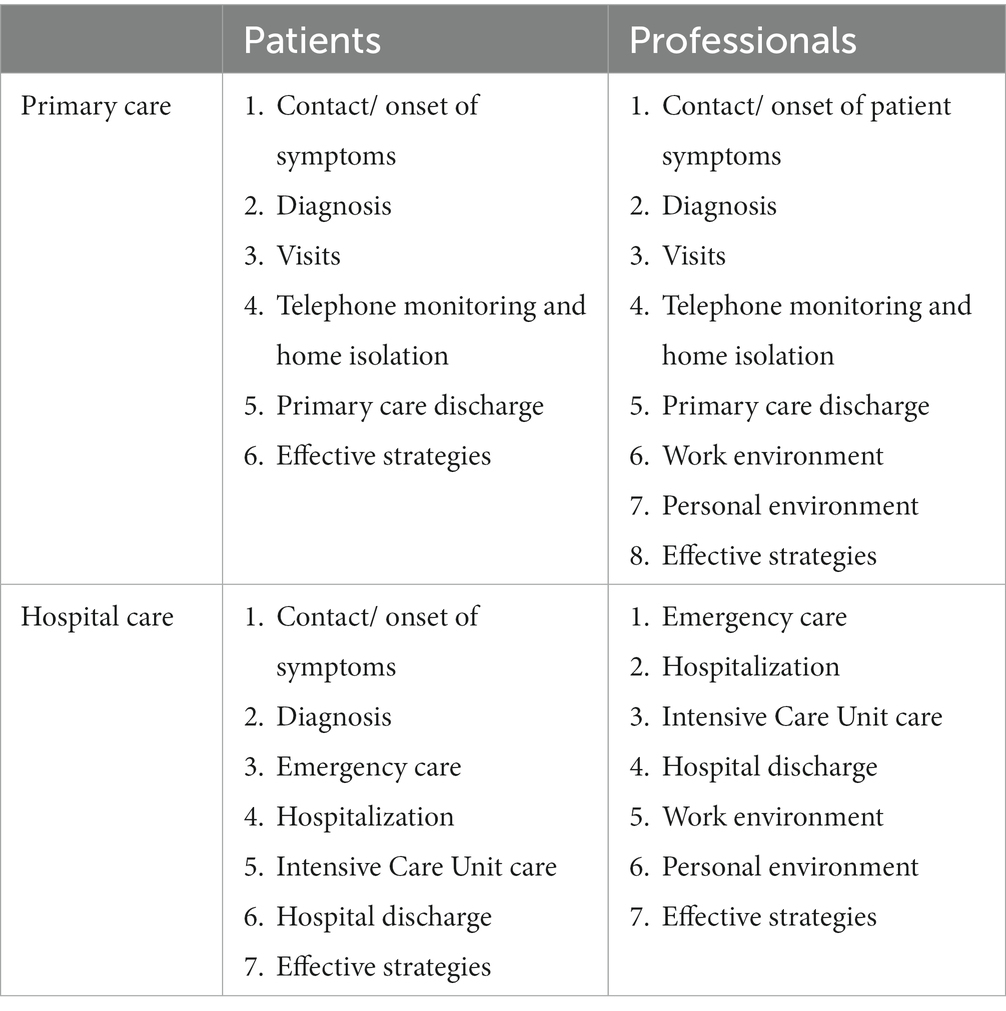
Table 1. Stages and categories captured by the open-ended questions in each of the four surveys.
The surveys were open from March 23, 2021, to July 2, 2021. They were launched during the fourth COVID-19 wave in Spain (March 15 – June 19) to gather the perspectives of patients and professionals regarding current and past healthcare and social-related needs and effective strategies associated with the pandemic. We attempted to obtain representation across Spanish regions, from patients across the age span and in need of different clinical services (e.g., ICU admission), and from multiple professional disciplines (medical doctors, nurses, and if possible one other discipline). Regions were divided into four groups, of four to six regions each, based on the percentage of COVID-19 cases in Spain according to the Institute of Health Carlos III (ISCIII) COVID-19 report as of March 17, 2021 (23): 0–1% (Principado de Asturias, Canarias, Cantabria, Ceuta, La Rioja, Melilla), 2–3% (Aragón, Islas Baleares, Extremadura, Comunidad Foral de Navarra), 4–6% (Castilla y León, Castilla-La Mancha, Galicia, Región de Murcia, País Vasco), and greater than 6% (Range: 13–18%) (Andalucía, Catalunya, Comunidad de Madrid, Comunidad Valenciana). We aimed to obtain responses from at least two region groups per survey. Surveys were closed based on thematic saturation, representation of different sociodemographic characteristics (region group, age, professional occupation, and ICU admission), and time elapsed.
Participants first completed a patient or professional registration form using Google® Forms, after which the research team verified whether participants met inclusion criteria and sent a follow-up email with the respective survey link(s), if appropriate. One reminder email was sent at least one week after the initial email. Eligible participants then had the opportunity to access the consent form and information sheet describing the research and the procedures for ensuring data confidentiality via the survey link(s). Once informed consent was provided, participants were allowed to complete the remaining sections of the survey. The research team provided technical assistance to complete the surveys when requested.
Recruitment focused on disseminating study information together with the registration form links via social networks (Twitter, LinkedIn, WhatsApp), as well as via the various communication channels of key organizations including the researchers’ home institutions (Avedis Donabedian Foundation, FAD; Evaluation and Planning Service of the Canary Islands Health Service, SESCS; Participa y Decide sobre tu Salud, PyDeSalud; Servicio Madrileño de Salud, SERMAS), and patient and professional associations and groups (e.g., Andalusian platform of patients affected by long-COVID; Spanish Society of Family and Community Medicine, semFYC). We relied on convenience and snowballing methods; while we exploited personal and professional contacts, we also sent cold emails as well as tagged influencers and groups to personal and institutional posts on Twitter and LinkedIn.
The data sets were downloaded from SurveyMonkey® into Microsoft® Excel. Responses with 100% of missing qualitative data were excluded from the analysis. Qualitative data were exported to Microsoft® Word and thematically analyzed by two reviewers using a mixed inductive-deductive essentialist or realist approach to identify themes at a semantic level. Thematic analysis is a qualitative analytic method “for identifying, analyzing, and reporting patterns (themes) within data” (24).
Reviewers first familiarized themselves with the data, by actively reading, re-reading, and discussing the data. Subsequently, a first reviewer (ADD) generated initial codes, and combined the codes into identified healthcare and social-related needs and effective strategies associated with COVID-19. Codes, needs, and strategies were then reviewed in-depth by a second reviewer (MAB). During a third round of revision, reviewers discussed and reached consensus to develop a final list of needs and strategies by subgroup. For each survey, needs were divided by the pre-established categories in the care pathway and an additional transversal category was created during the consensus round. The data analysis process and the final lists of needs and strategies were shared with the research team and further refined. Additionally, to ensure comprehensibility, each final list of patient needs (isolated at home or requiring hospital admission) was reviewed by a COVID-19 patient. As a result of the feedback, minor wording modifications were made to improve clarity. These lists of needs are the basis for a set of follow-up quantitative surveys developed to prioritize and obtain consensus over the identified needs.
For the purposes of this work, we completed four additional coding passes to classify the identified needs across surveys into overarching themes and subthemes. A first approach to classifying the needs into themes and subthemes was completed by a third reviewer (CBJ), and discussed with the initial two reviewers (ADD, MAB). ADD or MAB subsequently conducted an in-depth coding pass of the identified needs, after which coding was validated by either MAB or ADD during the third coding pass. During the fourth and final round of revision, the initial two reviewers discussed and reached consensus. The codebook was further developed, refined, and discussed throughout the coding process and needs were recoded as needed. Identified needs were coded in more than one subtheme when deemed necessary. Similarly, effective strategies were coded (MAB) into the aforementioned themes and subthemes and validated by a second reviewer (ADD). Disagreements were resolved by consensus.
One patient with a history of COVID-19 isolated at home was interviewed over the phone to describe her journey of care and associated healthcare and social-related needs, to inform the design of the surveys. Two additional patients were involved in reviewing the identified patient needs. Articles and reports published as a result of the larger COVID-19 needs research project will be shared with the patients involved and they will be encouraged to disseminate the results widely.
Of the 196 registration forms received (103 patient forms and 93 professional forms), twelve did not meet inclusion criteria: six people who responded the patient registration form had no history of COVID-19, and six professionals who responded the professional registration form worked outside of primary or hospital care (e.g., nursing home, psychiatric center). Accordingly, 184 people were invited to complete the survey(s) via email, of which two email addresses were incorrect. Of the 105 survey responses received, 29 were excluded due to missing 100% of the qualitative data. A total of 76 people completed the surveys and were included in the analysis: 33 home-isolated patients with COVID-19, 14 hospitalized patients with COVID-19, 16 primary care professionals, and 13 hospital care professionals.
Overall, we obtained representation from all four region groups, with 12 of the 19 Spanish regions represented. Patients’ subgroups had representation from 12 of 19 Spanish regions and all four region groups, while professionals’ subgroups had representation from 7 of 19 Spanish regions and 3 of 4 region groups. The most represented region was Comunidad de Madrid (n = 30, 15 patients and 15 professionals; 39.47%), followed by Catalunya (n = 13, 9 patients and 4 professionals; 17.11%) and Castilla y León (n = 10, 9 patients and 1 professional; 13.16%). Figure 1 summarizes the distribution of participants by Spanish region.
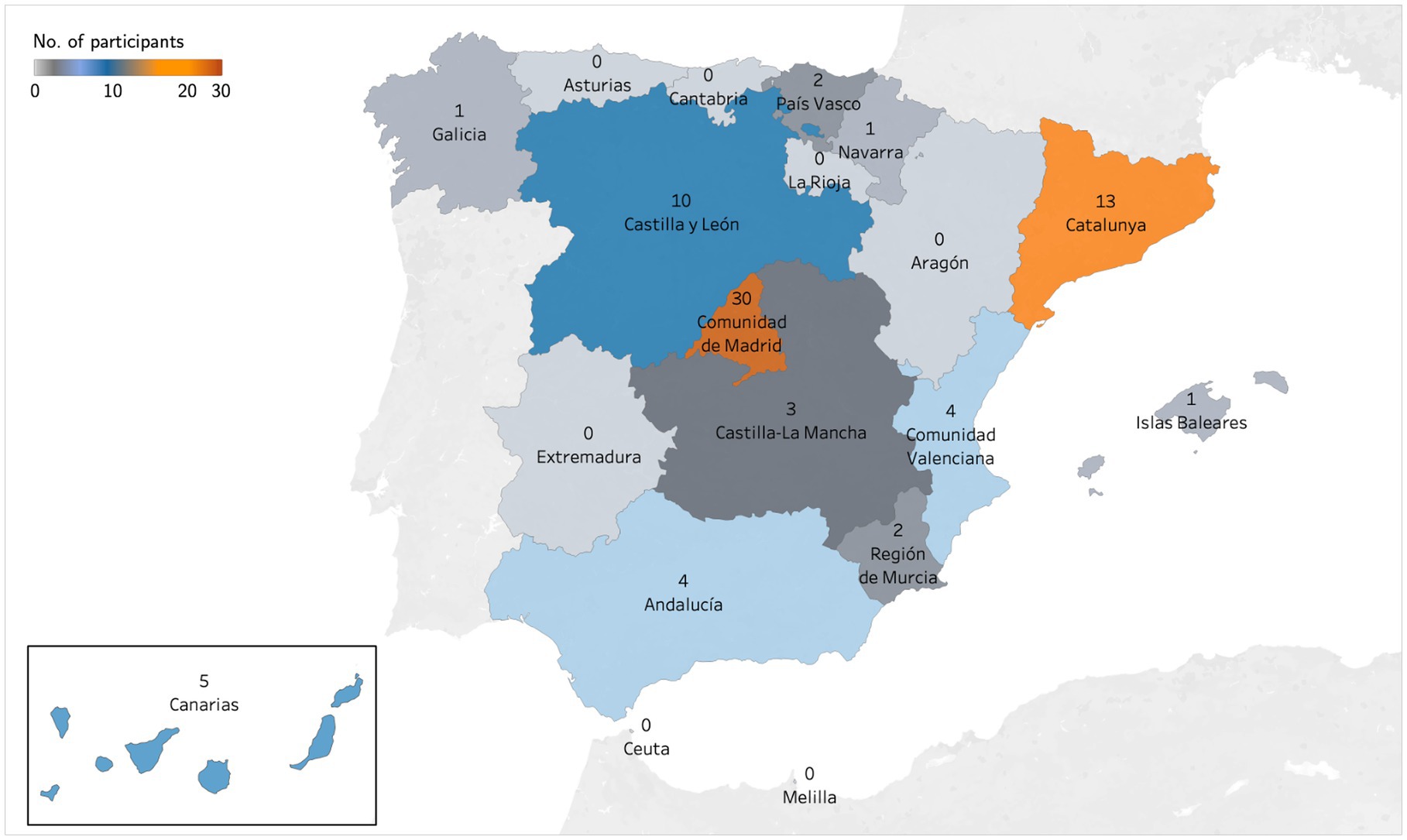
Figure 1. Distribution of participants by Spanish region.
The mean age of the whole sample was 46.73 years (SD = 12.15) and 71.05% were women. Most patients (n = 39; 82.98%), including those isolated at home and those hospitalized, had an associate’s degree or higher. The majority of professionals were physicians (n = 21; 72.41%) or nurses (n = 7; 24.14%), with only one responder employed in a different discipline (i.e., psychology). Patients who participated in the surveys were diagnosed with COVID-19 or first presented COVID-19 symptoms from March 7, 2020 to April 11, 2021. Less than half of the COVID-19 patients (n = 19; 40.43%) reported fully recovering, with 2 to 270 days of symptom duration (M = 39.95, SD = 61.25). On the other hand, 59.57% (n = 28) of patients had not fully recovered from COVID-19 symptoms when they responded to the survey between March and July, 2021, and still had persistent symptoms including changes in smell and taste perception, muscle and joint pain, fatigue, dyspnea and cognitive impairment. Table 2 provides a description of the sociodemographic characteristics by study subgroup.
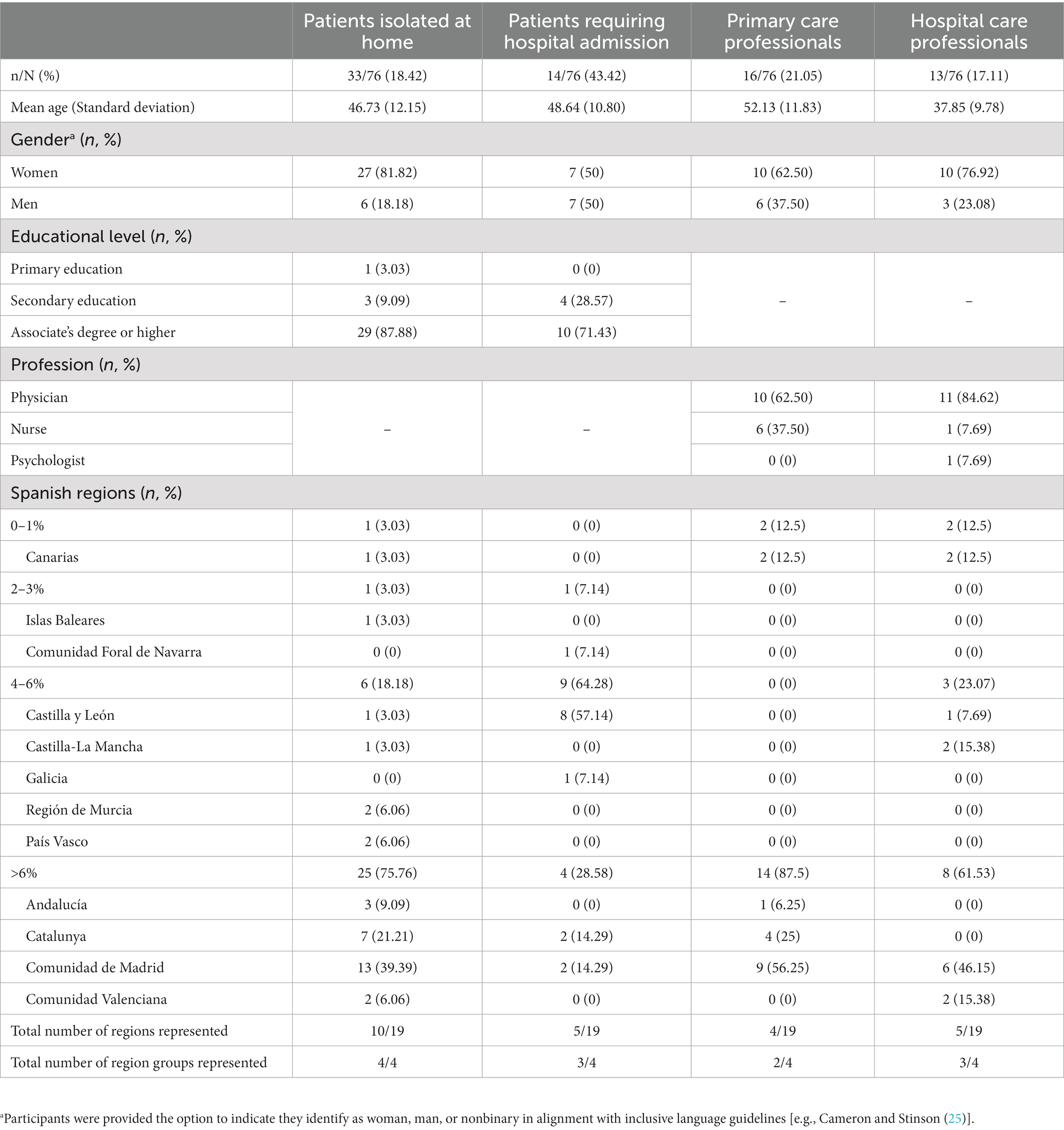
Table 2. Sociodemographic characteristics by study subgroup.
We focused on the perceived healthcare and social COVID-19-related needs of patients and professionals in primary and hospital care in Spain. Thematic data analysis in this study led to the identification of 81 needs reported by home-isolated patients, 62 needs reported by hospitalized patients, 94 needs reported by primary care professionals, and 90 needs reported by hospital care professionals, for a total of 327 needs across surveys. Identified needs were classified across eight themes and 32 subthemes (Table 3; Supplementary material S2 provides the Spanish to English translated list of needs).
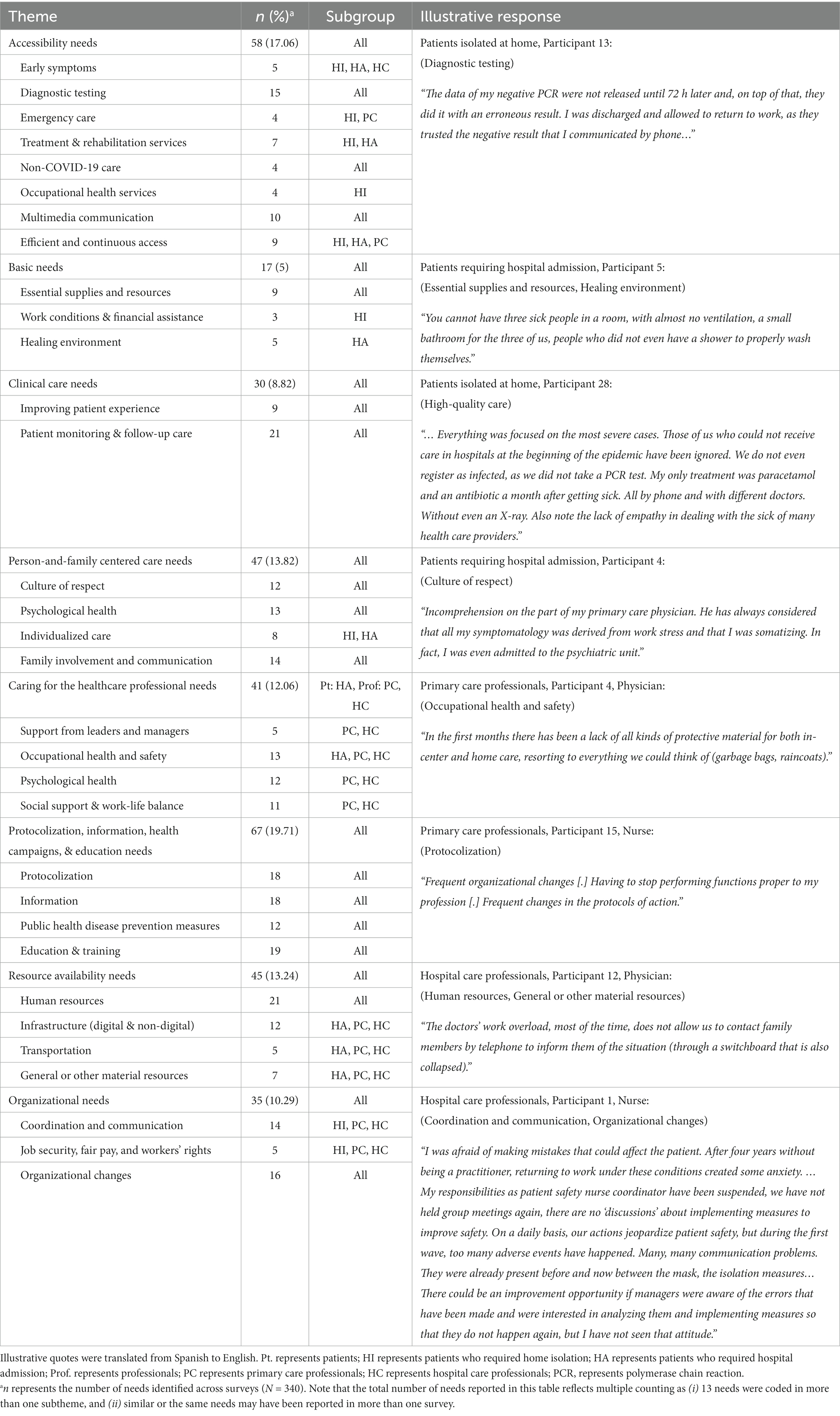
Table 3. Key themes and subthemes of COVID-19 healthcare and social-related needs.
Representatives from the four population subgroups reported 58 accessibility needs (17.06%). As soon as the first symptoms appear, citizens must be able to rapidly contact health services and providers to aid in early detection via multiple communication media, and obtain quick access to accurate diagnostic tests and results close to their homes or at-home. Patients emphasized access to diagnostic tests and results should also be extended to close contacts. Additionally, patients stressed the importance of being able to contact emergency services when needed, including on weekends and holidays, and via a variety of channels. Whereas home-isolated patients underscored the importance of immediate access to urgent medical transport, hospital professionals requested prompt attention from emergency services for transporting patients to the hospital in the event of an emergency. Once a diagnosis has been confirmed, patients indicated the need to access an adequate treatment plan, access the providers in charge of their care, and rehabilitation services, particularly in the event of long-term COVID-19 complications. Patients isolated at home also emphasized the importance of having easy and quick access to Occupational Health Services (OHS) after a diagnosis in order to request sick leave, and similarly, primary care professionals suggested online access to OHS could help avoid displacing home-isolated patients to healthcare centers. Moreover, addressing non-COVID-19 healthcare needs of COVID-19 and/or non-COVID-19 patients also emerged as a need from the perspective of both patients and professionals (e.g., chronic diseases, palliative care, care for people with mobility impairments). Overall, all participants highlighted the need for multiple communication media, based on patients’ needs and preferences, such as videoconferences, home visits, in-person, or phone calls, in order to timely access health services. Finally, it was noted by both patients and primary care professionals that access to care must be efficient and continuous. To make this possible, there is a need to reduce waiting times in primary care, emergency care, and with specialists in hospital settings, improve communication, provide timely in-person care and care during extended hours, prioritize cases, have sufficient personnel, and provide administrative solutions to exceptional cases.
Seventeen (5%) basic needs were identified by participants from all subgroups. Needs related to the provision of essential supplies and resources were reported by all participants. While hospital care professionals indicated hospitalized patients required access to their personal belongings, hospitalized patients requested adequate food service and bathroom facilities, as well as assistance with personal hygiene. In turn, primary care professionals and home-isolated patients, reported patients isolated at home required access to facilities to safely isolate themselves from other household members, as well as support during isolation such as caring for dependents or with domestic tasks (e.g., home-delivery of food and medicine, cleaning, etc.). Additionally, patients who were isolated at home emphasized the importance of flexible working conditions, including remote work, and financial support to deal with the economic consequences of isolation. Moreover, a healing hospital environment emerged as a subtheme for hospitalized patients, who indicated the need to reduce environmental stressors such as noise and poor air quality, to minimize patient movement, and the need for rapid access to a hospital room.
Clinical care needs (n = 30, 8.82%) were identified by all subgroups. To ensure patients receive high-quality care and to improve the patient experience, first and foremost, improvements in the diagnosis phase are required, including increased diagnostic test reliability, and implementation of a wide testing strategy that includes testing asymptomatic persons who are close contacts. Next, patients must have access to effective treatment plans from the onset of symptoms, even if they are in home isolation. Improvements in information provision for patients and their caregivers on the treatment and discharge plans are also needed; written, simple, and easy to understand information is key. Moreover, rigorous and continuous patient monitoring for patients in home isolation with or without a confirmed diagnosis and hospitalized patients, as well as follow-up care to ensure patient compliance, symptom control, and continuity of care are also required, as reported by all subgroups.
Forty-seven (13.82%) needs identified by all subgroups were classified in the Person-and-family centered care theme. All subgroups placed emphasis on building a culture of respect characterized by empathy, respect, affectionate and effective communication, active listening, shared decision-making, and trusting relationships. Mental health and emotional support for patients and their loved ones during home isolation, hospitalization, ICU admission, and post-hospital discharge emerged as another subtheme stressed by all subgroups. Primary care professionals also expressed the need to embrace health from a social perspective that includes accessible public health initiatives to promote mental health. Additionally, patients noted the importance of individualized care, particularly in relation to communicating with the same professional during their care journey, treatment and discharge decisions adapted to their specific circumstances, adapting communication to patients’ needs and preferences, and support scheduling medical appointments. Finally, all subgroups emphasized the need to keep loved ones involved and in continuous communication with patients and professionals throughout the patient care journey (e.g., verbal and written information sharing, communicating via phone or videoconference, hospital visits). In-person visits were particularly stressed for children, older adults, disabled people, and terminally ill people by professionals.
Forty-one (12.06%) needs, primarily reported by primary and hospital care professionals, were concerned with caring for the healthcare professional. Real support from leaders and managers and recognition of the work of professionals were seen as crucial. To this end, professionals requested face-to-face visits by management, good coordination, adaptive leaders, and comprehension. Additionally, occupational health and safety was reported as a main priority for professionals. Key elements identified included the provision and proper use of adequate PPE that does not hinder visibility and comfort, which was also identified as a need by hospitalized patients; implementation of organizational preventive actions and strategies and improving adherence to such measures; reduced work shifts and a reasonable workload allowing for time to rest during and outside the work environment; working within healthcare providers’ usual scope of practice or receiving appropriate redeployment training; and the option to carry out low-risk work for professionals particularly vulnerable to COVID-19. Caring for professionals’ psychological health emerged as another subtheme. Further, primary and hospital care professionals emphasized the need for continuous proactive evaluation of physical and psychological health and tangible actions to address needs, as well as support to manage stress, anxiety, fear of infection, continuous isolation, and the COVID-19 crisis in general for themselves and their families. Finally, professionals noted the need for work-life balance, and for organizations to provide social support to care for dependents and when infected with COVID-19 (lodging, food, financial assistance, etc.). The need for social connection and public health measures to reduce stigmatization also emerged.
One fifth of needs (n = 67, 19.71%) recognized the need for protocolization, information, public health disease prevention measures, and education and training. Patients and professionals required clear, accessible, effective, and adequately implemented protocols and decision algorithms throughout the journey of care. Although all participants stressed the importance for the existence and continuous update of protocols, professionals emphasized the need to avoid unnecessary changes, for managers to highlight the relevant changes, as well as to maintain certain degree of flexibility (e.g., based on clinical judgment, shared-decision making). Additionally, clear action protocols for specific circumstances and vulnerable populations, such as caring for a nursing infant when the caregiver has COVID-19 or for the protection of vulnerable people when reentering the workforce, were required by home-isolated patients. Information about how to proceed in specific situations and more broadly, consistent, concise, up-to-date, and clear information about COVID-19 provided by healthcare professionals, public health, and communication media was needed for patients, their relatives, and citizens (e.g., early detection of symptoms, when and how to isolate, infection control, antibody generation and possibility of reinfection, legal information related to medical discharge and work reinstatement). Although informational needs were reported by all subgroups, they were mainly stressed by patients. Moreover, public health measures using multiple modes of communication (e.g., verbal and written instructions, video tutorials, etc.) to prevent the spread of the disease, avoid the spread of fear and misinformation, and reduce stigmatization of people infected with COVID-19 were also needed. Finally, all subgroups identified gaps in the education and training of professionals related to early identification of symptoms and diagnosis, patient monitoring and follow-up care, long COVID, redeployment, correct donning and doffing PPE in different settings, telehealth, counseling and communication with patients and their relatives, resident training, and knowledge and practices concerning COVID-19 more broadly.
Forty-five (13.24%) needs reported by all subgroups were about availability of human and material resources to meet the rise in demand for care and avoid the saturation of health systems. Participants in all subgroups identified the need to hire additional qualified staff including healthcare providers (e.g., to maintain reasonable workloads and work shifts, avoid redeployments, provide non-COVID-19 care, improve triage and diagnostic testing for early identification and separation of suspected COVID-19 patients, provide support with activities of daily living, improve patient monitoring of COVID-19 and non-COVID-19 cases, improve communication with relatives), administrative personnel (e.g., to improve contact tracing, appointment management), IT staff, support personnel to deliver food and other essential resources to patients isolated at home, and mental health professionals for patients, family members, and citizens. Subthemes related to material resources availability included transportation, digital and nondigital infrastructure, and general or other material resources. Transportation resources were needed for both patients (e.g., ambulances, after hospital discharge) and professionals (e.g., during isolation, to health centers, for home-care services). The need to improve digital technologies and for the provision of sufficient and adequate spaces (to preserve privacy, separate cases, non-COVID-19 treatment, increase bed and ICU capacity) were also noted by professionals and hospitalized patients. Other material resources required reported mainly by professionals, included reagents, diagnostic tests, access to x-rays and ultrasounds in primary care, and face masks for patients, professionals and citizens.
Thirty-five (10.29%) needs reported by all subgroups focused on coordination and communication, work conditions, and organizational changes. Home-isolated patients and primary and hospital care professionals highlighted the need for improved intra- and inter-professional coordination and communication within departments, within health centers, between health services, and/or between health authorities and health providers, to: improve early detection and disease prevention; improve patient monitoring, follow-up care, and patient care more broadly; improve work conditions; and promote knowledge exchange between professionals. Professionals and home-isolated patients also reported needs related to job security, fair pay, sick leave, and workers’ rights including “maintenance of work conditions or consensual changes” (e.g., place of work, schedules, shifts, tasks). Organizational changes to better address the COVID-19 crisis and future global threats were also identified by all subgroups. Patients and professionals reported the need to improve contact tracing, and to reduce or prevent medical errors (e.g., related to diagnosis) by improving organization. Additionally, professionals also reported the need to avoid pauses or delays in non-COVID-19 care; improve patient monitoring; promote patient safety; reduce the need to improvise and the saturation of health systems (by, e.g., having primary care provide a treatment plan, increase automation of tasks); improve quality control measures and quality improvement more broadly by, for example establishing a systematic and continuous evaluation of service needs and implementing the necessary actions to address them; develop adaptive capacity; and improve decision-making processes to involve frontline professionals and organizational transparency.
Although the present study primarily focused on identifying needs, effective strategies and positive aspects related to the COVID-19 patient care pathway were also reported. A total of 86 effective strategies and positive aspects were reported across surveys: 22 by home-isolated patients, 9 by hospitalized patients, 35 by primary care professionals, and 20 by hospital care professionals. Effective strategies and positive aspects were classified across seven themes and 21 subthemes (all of the aforementioned themes except the Basic needs theme) (Table 4; Supplementary material S3 provides the Spanish to English translated list of effective strategies and positive aspects).
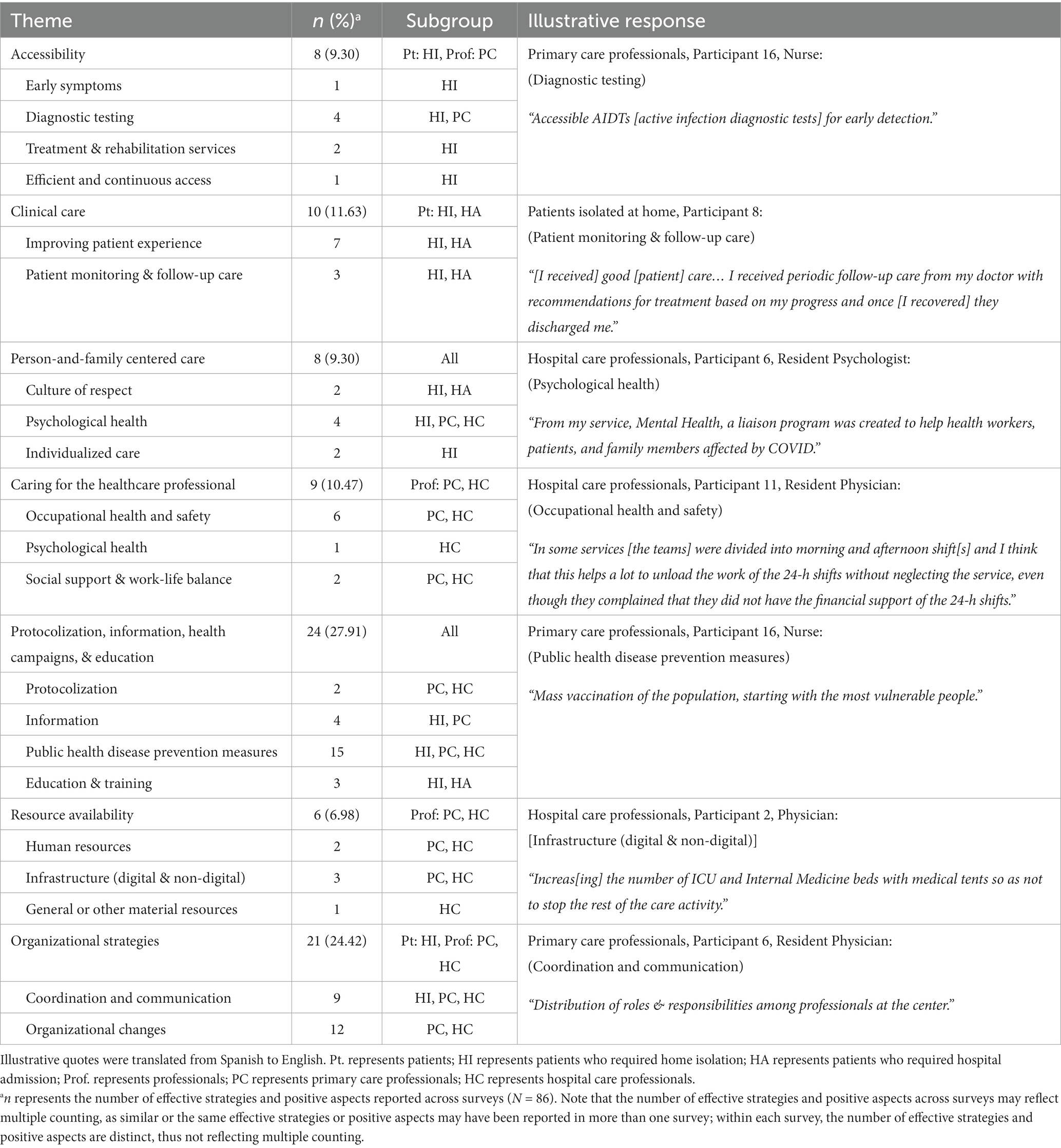
Table 4. Key themes and subthemes of COVID-19 healthcare and social-related effective strategies and positive aspects.
Thirty-one (36.04%) effective strategies and positive aspects were reported by patients. These focused on Accessibility, including access to health services/providers to aid in early detection, access to rapid diagnostic testing, access to treatment and rehabilitation services to address physical and cognitive symptoms, and efficient and continuous access to healthcare providers via phone; Clinical care, including improving patient experience and satisfaction, effective and prompt treatment, and rigorous patient monitoring and follow-up care; Person-and-family centered care, including providing individualized and empathetic care, and establishing community support networks; Protocolization, information, health campaigns, and education by investing in research, keeping citizens well-informed, continuous training of healthcare personnel on COVID-19 including long-COVID, and public health disease prevention measures such as contact tracing and quick isolation of confirmed or suspected cases; and Organizational strategies, including improving coordination between health services and effective referrals.
On the other hand, fifty-five (63.95%) effective strategies and positive aspects were reported by professionals. Strategies focused on Accessibility to diagnostic testing for early detection; Person-and-family centered care, including establishing community support networks and mental health programs for patients and their relatives; Caring for the healthcare professional by ensuring sufficient and appropriate use of PPE, enforcing stringent hygiene, ventilation, and other biosecurity measures, reorganizing work shifts, developing mental health programs for professionals and their relatives, and establishing community support; Protocolization, information health campaigns, and education, including developing and adapting protocols as needed, providing up-to-date information for patients and professionals via multiple channels, learning of and sharing local care networks/resources with patients, and public health disease prevention measures such as performing diagnostic tests outdoors, limiting the maximum occupancy capacity, rapid isolation of confirmed or suspected cases, public awareness campaigns, mass screening, diagnostic testing, and vaccination, effective and efficient contact tracing, and enforcing biosecurity measures such as mandatory use of masks and social distancing; Resource availability, including hiring additional personnel, adapting outdoor and indoor spaces and ensuring the availability of other material resources to meet the demand for care; and Organizational strategies, including improving collaboration within teams, centers, health services, and neighborhoods, effective referrals, redistributing roles and responsibilities, permitting changes in appointments, adaptive capacity of the team and the organization, timely implementation of changes, increasing telephone appointments, implementing effective screening and diagnostic protocols, and establishing closed circuits for COVID-19 patients and independent working groups for professionals.
As part of a larger mixed methods project seeking to explore COVID-19-related healthcare and social needs, the present study explored the needs and effective strategies associated with COVID-19 from the perspective of patients and healthcare providers in two different healthcare settings: Primary care and hospitals. A total of 327 needs and 86 effective strategies and positive aspects were identified based on first-person perspectives and classified into the following eight overarching themes: (i) Accessibility, (ii) Basic needs, (iii) Clinical care, (iv) Person-and-family-centered care, (v) Caring for the healthcare professional, (vi) Protocolization, information, health campaigns, and education, (vii) Resource availability, (viii) and Organizational needs/strategies. Of interest, most of the effective strategies reported by the participants overlapped with the identified needs, highlighting the importance of prioritizing and addressing the needs identified (the association between identified needs and effective strategies is further discussed in Section 4.1).
Overall, health and social systems of care were generally unprepared for a crisis like the COVID-19 pandemic (15, 26); this was also the case for Spanish systems of care. Our findings strongly align with the Health Foundation’s dimensions of quality and are discussed accordingly, highlighting the need for care to be safe, effective, caring, responsive and personalized, and for healthcare organizations and systems to be well-led, sustainably resourced, and equitable (27).
More specifically, our findings elucidate the need to deliver safer and more effective care by providing services informed by consistent and up-to-date information and protocols, adequately training professionals, and establishing effective public health measures. In particular, the need for efficient, effective and easy-to-implement protocols was highlighted across settings, together with the need for more responsive and personalized person-and-family-centered care based on shared-decision making, illustrating the importance of developing adaptive expertise within our systems of care. Healthcare protocolization and standardization can aid in ensuring that patients receive evidence-based care and that medical errors are kept to a minimum. Protocols and guidelines, however, are not foolproof solutions to medical decision-making, and clinicians are increasingly faced with new challenges that cannot be met with standard solutions (28). Promoting the development of adaptive expertise among healthcare professionals will allow them to engage in innovative problem-solving, as needed, to meet their patients’ and their families’ specific needs. This can lead to improved patient outcomes, as well as more efficient and effective use of healthcare resources. Finally, the need for effective public health measures to keep citizens well-informed, slow the spread of the virus, and protect and promote mental and physical health was also identified by both patients and professionals. Although strict regulations helped decrease community transmission, they also had significant health, economic, social and psychological consequences, such as decreased access to non-COVID-19 care, job loss, disruptions to education, and increased mental health problems, that must be considered in the future to minimize the overall negative impact on the well-being of the population (29–32).
Further, the need to deliver more caring services embedded within a culture of respect, in which people are treated with compassion and dignity, and that places value on active listening, effective communication, and building trusting relationships was identified. Similarly, the importance of taking care of healthcare professionals’ physical and emotional health also emerged, which was implications for professionals and patients as previous research indicates the emotional healthcare culture impacts patient safety and quality patient care (33).
Moreover, results showed the need for organizations and systems to be (i) well-led, driven by real support from leaders and managers and recognition of the work of professionals; (ii) sustainably resourced, focused on identifying and addressing gaps in human and material resources to meet the rise in demand for care and avoid the saturation of health systems, and (iii) equitable, to reduce inequalities in vulnerable populations such as nursing infants, people in low-income households, older adults, disabled people, and terminally-ill people, and to ensure access to high-quality care and outcomes for all. The COVID-19 pandemic has revealed the importance of seamless collaboration between health and social systems of care. The virus has put a strain on both systems, with healthcare facilities overwhelmed by the number of patients requiring treatment and social systems struggling to support those affected by the pandemic. In order to effectively manage the pandemic and provide optimal care for patients, it is crucial for health and social care systems to work together smoothly and in concert. This includes sharing information and resources, coordinating efforts, and ensuring that patients receive comprehensive care. In Spain, the necessity to improve coordination between services has been widely recognized (34, 35). Recent work (36) has advocated for a new approach to care that establishes a coordinated, comprehensive, person-and-family-centered social and health care model, that provides rehabilitation services, long-term care, and palliative care, and includes a health and social services catalog managed by professionals, joint protocols of action, referral procedures between sectors, and discharge planning strategies to ensure continuity of care in the home environment. Also, a coordinated, multidisciplinary approach to care is essential for the complex and multifactorial impairments associated with the post-acute sequelae of the SARS-CoV-2 infection that affects various aspects of physical, cognitive, and mental health (37). Ultimately, the quality of care delivered depends to a high degree on a well-functioning network and good intra- and interprofessional collaboration and coordination. The identified needs in this study highlight these very issues in the current healthcare system.
The following section discusses the association between the needs and effective strategies identified. To note, although participants were asked to report both COVID-19 healthcare and social-related needs and effective strategies, they were not explicitly instructed to match them. Moreover, even though the surveys were open from March 23, 2021 to July 2, 2021, they gathered perspectives regarding needs and strategies associated with waves one through four of the pandemic. At least partly because of this, some of the identified needs were also reported as effective strategies and some have already been addressed in a large-scale, while some of the reported effective strategies continue to hold the potential to address some of the identified needs and to enhance health emergency preparedness. In addition to the date of survey completion, diversity in responses may also be related to individual needs and preferences, as well as variations in healthcare centers and regions, reflecting the dynamic and evolving nature of the COVID-19 pandemic in different contexts and over time.
Next, we illustrate how some of the reported strategies may address some of the identified needs related to patient-monitoring and follow-up care (Clinical care); psychological health and individualized care (Person-and-family centered care); occupational health and safety, and social support and work-life balance (Caring for the healthcare professional); information and public health disease prevention measures (Protocolization, information, health campaigns and education); infrastructure (Resource availability); and coordination between different services (Organizational strategies/needs).
Related to Clinical care, establishing rigorous and frequent patient monitoring and follow-up care, with the physician managing the case, could effectively address several of the identified needs. This approach would potentially enable improvements in monitoring for patients with a history of probable COVID-19 and enhance monitoring after the acute phase of the disease, ensuring comprehensive care throughout the recovery process. In fact, continuity of care, or repeated contact between an individual patient and a doctor, is associated with increased adherence to treatment, reduced hospital use, and greater patient satisfaction (38–40). Moreover, this approach would facilitate the implementation of control measures to verify understanding and adherence to guidelines for proper isolation, which would promote public health and minimize the risk of transmission.
Furthermore, creating community support networks can address various unmet patient needs related to Person-and-family centered care. They have been shown to help communities reduce the psychological impact related to infectious disease outbreaks (41). By addressing health from a social perspective, these networks promote holistic well-being, combat loneliness, and prioritize the needs of vulnerable populations. Specific to the COVID-19 pandemic, these networks could offer emotional and practical support for patients and their relatives during home isolation and hospitalization, and provide information and strategies to caregivers. Similarly, implementing a liaison mental health program to support individuals impacted by COVID-19, including patients and family members, can provide essential psychological support in the short, medium, and long term (42). This type of programs could offer coping strategies, resources, and comprehensive care for all affected individuals. An additional effective strategy to enhance person-and-family centered care involves the provision of individualized care via comprehensive care plans. This approach could facilitate appropriate discharge planning based on symptoms and limitations, as well as provide support in scheduling rehabilitation and other medical appointments following hospitalization. By implementing such plans, patients and their families could receive personalized care and support throughout the recovery process, promoting a more holistic approach to healthcare.
For healthcare professionals, community support networks can also play a crucial role in mitigating the impact of the pandemic on their mental health and in facilitating the implementation of measures for effective family reconciliation. These networks could provide support for child care, and also afford professionals the opportunity to engage in activities unrelated to COVID-19, allowing them much-needed respite. Additionally, implementing specific liaison mental health programs for healthcare workers has also been shown to support their mental health, and can equip them with strategies for coping with the fear of infection, continuous isolation due to working closely with COVID-19 patients, increased workload, redeployment, and managing stress, anxiety, and depression in a rapidly changing landscape (42, 43). Further, mental health programs could facilitate addressing the identified need for continuous proactive evaluation of healthcare providers’ physical and psychological health, and enable organizations to take tangible actions to address chronic burnout, post-traumatic stress, and other complications. Splitting teams into morning and afternoon shifts, for example, was reported as an effective strategy to support the well-being of healthcare professionals, by promoting essential rest time, effective workload management, and reduced working hours. Other tangible actions to support healthcare workers’ mental health include expanding basic need resources and services (e.g., child care, food, alternative housing options), recharge/rest spaces, and additional training programs in the workplace (44).
In relation to information and public health disease prevention measures, contact tracing teams have emerged as effective strategies according to home-isolated patients and primary care professionals. These teams could play a crucial role in ensuring correct symptom identification, providing information on the disease, protection measures, and isolation guidelines. Additionally, awareness campaigns that promote inclusive messages and avoid stigmatizing messages, were also reported as an effective public health strategy that could effectively address several identified needs such as, reducing discrimination in the workplace upon returning from a COVID-19 leave and preventing the spread of fear through the media. By fostering understanding and empathy while promoting health recommendations, these campaigns could help create a supportive environment, dispel misinformation, and mitigate the spread of COVID-19 and negative social consequences.
Moreover, participants reported increasing the number of ICU and internal medicine beds with temporary structures as an effective strategy related to Resource availability. This strategy would enable the provision of proper care by increasing surge capacity. Doing so would facilitate the separation of COVID-19 and non-COVID-19 patients, ensuring the continuation of non-COVID-19 care and minimizing the risk of transmission within healthcare facilities (45).
Lastly, increased coordination between different healthcare services was highlighted as an effective organizational strategy for enhancing follow-up care. Enhancing coordination could help avoid duplication, ensure necessary controls are in place, improve communication between healthcare professionals, and facilitate easy access to medical records. Ultimately, these measures would contribute to improvements in the quality of patient care and a more streamlined healthcare system.
A key strength of this study lies in the use of a rich data source on COVID-19 health and social -related needs based on the perspectives of patients and professionals. In addition to including first-person perspectives in the surveys, patients were involved in the survey design process and in revising the final lists of identified patient needs. Finally, our work captures the needs and effective strategies associated with the first four waves of COVID-19, from its inception to July 2021. This provides the opportunity to identify needs and strategies that may help prepare health systems for future public health emergencies, as well as more current needs that may need to be addressed or strategies that need to be more widely implemented to improve the quality of care today.
Our study, however, is not without limitations. First, the depth of the open-ended responses obtained was limited by the cross-sectional survey design. Nonetheless, the design was selected as participation in the study required minimal time commitment (10–20 min at one time point only), while allowing us to identify a broad set of COVID-19 healthcare and social-related needs based on the first-person perspectives of patients and professionals in Spain. Second, our study was not designed to detect changes in needs over time; in fact, some of the needs reported by the participants were also reported as effective strategies and others have already been addressed, such as access to and appropriate use of PPE (46). Third, although we identified a plethora of needs and strategies, we did not identify the level of importance associated with each of them. Finally, although our survey response rate of 41.8% falls within the documented average survey response rate of 35–53% (47), we had difficulties efficiently recruiting participants from all Spanish regions (seven of the 19 Spanish regions were not represented), from a wide range of disciplines (profession was mainly limited to nurses and physicians), and participants younger than 27 and older than 69 years, thereby limiting the generalizability of our findings. Nevertheless, surveys were closed based on thematic saturation.
Moving forward, it will be important to identify improvement priorities, taking into consideration all stakeholders’ views. To this end, the 327 needs identified during this study will form the basis for a follow-up quantitative study focused on prioritizing and obtaining consensus over the identified needs, identifying the resources needed to address these needs, and estimating the associated costs. Additionally, future work should also aim to include other stakeholders’ perspectives, such as family members and policymakers; assess differences in needs by region; and assess which of the identified needs persist, which have been addressed, and which novel needs have emerged. Finally, improvement recommendations for healthcare organizations and systems using an integrated whole-system approach to ensure sustained improvements are warranted (27).
Our findings have important implications for future clinical practice and policy (See Table 5 for a summary of recommendations). Altogether, we would recommend thoughtful and deliberate consideration of healthcare professionals’ and patients’ perspectives as best practice in organizational decision-making and policymaking, particularly for global crises of such magnitude. Henceforth, organizations and policymakers should actively integrate previously identified healthcare professionals’ and patients’ needs when choosing and implementing their COVID-19 policy packages. Addressing these needs is an essential intervention to mitigate the effects of the current and future public health emergencies. The COVID-19 pandemic has presented unprecedented needs and challenges that require well-co-coordinated responses across governments, healthcare services, and non-government sectors that consider both the possible benefits and harms, to find a balance between reducing the socioeconomic impact and protecting the physical and mental health of all sectors of the population.
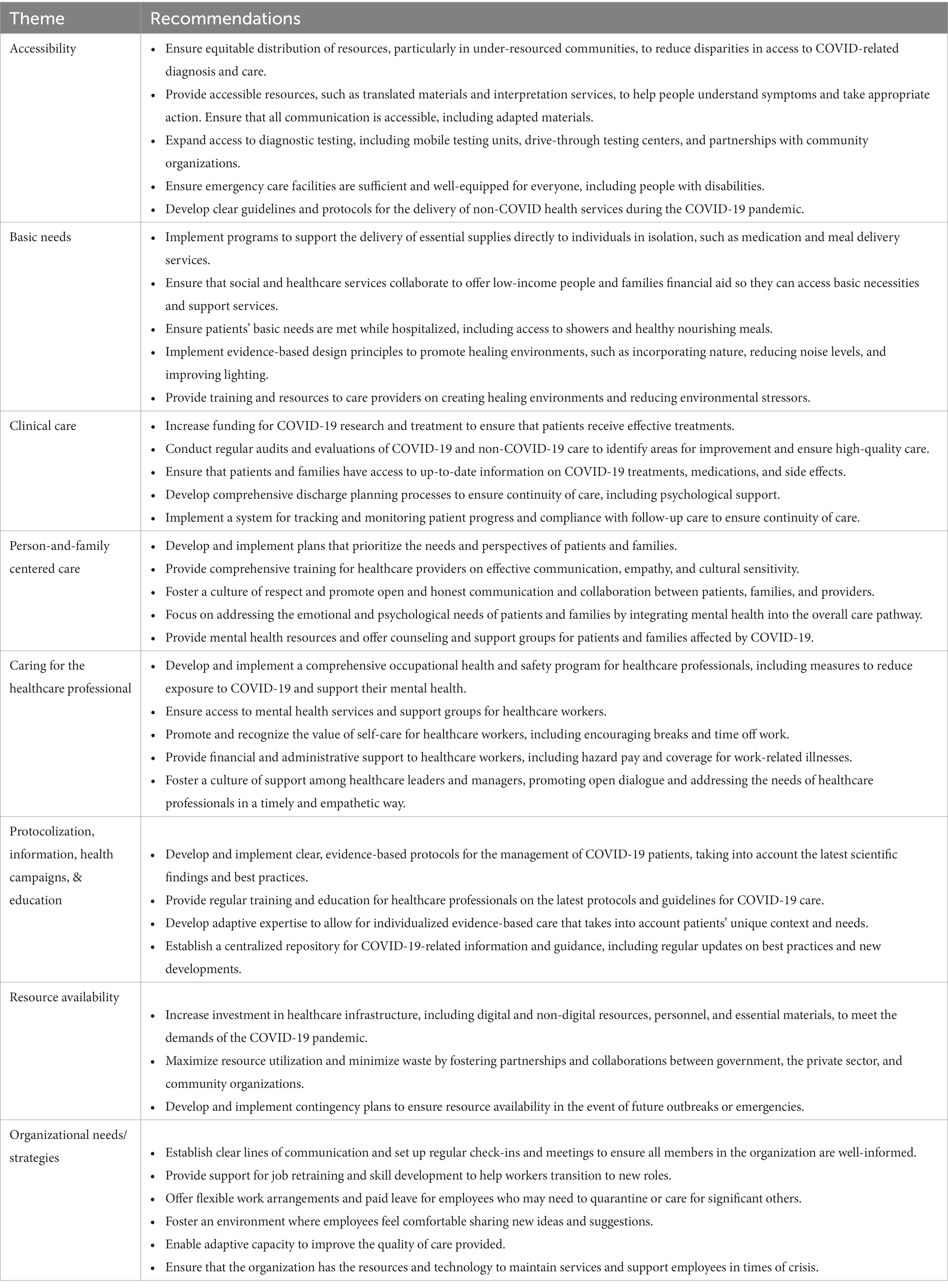
Table 5. Summary of recommendations for practice and policy.
Here we identify key themes and subthemes related to healthcare and social-related needs and effective strategies associated with COVID-19 from the point of view of patients and professionals in Spanish hospital and primary care settings. Results support the need to provide care that is accessible, high-quality, person-and-family centered, caring, and well-informed, and for organizations and systems to be well-equipped, well-led, and with adapting capacity, to improve the physical and mental health of all. This work will inform healthcare leaders, managers and policy-makers about the main needs and effective strategies perceived by patients and professionals to enable better future preparedness for resilience and contingency planning by administrations and organizations at different levels of care.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study was reviewed and approved by Hospital Universitario 12 de Octubre Research Ethics Committee (No. 20/608). All participants provided electronic informed consent to participate in this study.
AD-D, MAB, CO, LP-P, and AG-G: conceptualization and methodology. AD-D and MAB: data curation. AD-D, MAB, and CB-C: formal analysis. AG-G: funding acquisition. AD-D, MAB, CO, LP-P, JB-C, MB-M, CB-C, and AG-G: investigation. MAB and CO: project administration. CO, LP-P, and AG-G: resources and supervision. AD-D, MAB, and LS: visualization. AD-D, MAB, LS, JB-C, and MB-M: writing – original draft. AD-D, MAB, LS, CO, LP-P, JB-C, MB-M, CB-C, and AG-G: writing – review and editing. All authors revised drafts of the manuscript and approved the final version.
This work was funded by the Foundation for Biosanitary Research and Innovation in Primary Care (FIIBAP) and the Regional Ministry of Health of the Community of Madrid through non-refundable grants from the credits awarded to the Community of Madrid by the Spanish Government Fund COVID-19, included in Order HAC/667/2020.
We would like to thank the patients and the healthcare providers who participated in this study. Special thanks to Lilly Lichaa for her first-person perspective on the needs associated with the COVID-19 patient journey and to the COVID-19 patients who reviewed the identified patient needs. We are also appreciative of affiliated research staff, specifically, the following FAD staff: Óscar Córdova, for support with the project’s website, Assumpta Pons, Ester Llach, and Caterina Fernàndez, for support with the, flyer design, SurveyMonkey, recruitment, and/or email management, and to Ana Blanco Rubio for assistance with survey content development; and to COVID-19 needs collaborators Almudena Molina for providing feedback on the surveys, and Sofía Garrido for providing feedback on an early draft of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1166317/full#supplementary-material
1. Hui, DS , Iazhar, E , Madani, TA , Ntoumi, F , Kock, R , Dar, O, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health — the latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. 91:264–6. doi: 10.1016/j.ijid.2020.01.009
2. WHO . (2020) WHO announces COVID-19 outbreak a pandemic. Available at: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (Accessed April 21, 2022).
3. WHO . (2020). Strengthening the health systems response to COVID-19: policy brief: recommendations for the WHO European region (1 April 2020). Available at: https://www.who.int/europe/publications/i/item/WHO-EURO-2020-806-40541-54465 (Accessed December 15, 2022).
4. CDC . (2020). Estimated disease burden of COVID-19. Centers for Disease Control and Prevention. Available at: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/burden.html (Accessed December 15, 2022).
5. Vindegaard, N , and Benros, ME . COVID-19 pandemic and mental health consequences: systematic review of the current evidence. Brain Behav Immun. (2020) 89:531–42. doi: 10.1016/j.bbi.2020.05.048
6. The Lancet Rheumatology . Too long to wait: the impact of COVID-19 on elective surgery. Lancet Rheumatol. (2021) 3:e83. doi: 10.1016/S2665-9913(21)00001-1
7. Evans, DB , and Over, M . (2022). The economic impact of COVID-19 in low- and middle-income countries. Center for Global Development | Ideas to Action. Available at: https://www.cgdev.org/blog/economic-impact-covid-19-low-and-middle-income-countries (Accessed December 15, 2022).
8. Litewka, SG , and Heitman, E . Latin American healthcare systems in times of pandemic. Dev World Bioeth. (2020) 20:69–73. doi: 10.1111/dewb.12262
9. Burau, V , Falkenbach, M , Neri, S , Peckham, S , Wallenburg, I , and Kuhlmann, E . Health system resilience and health workforce capacities: comparing health system responses during the COVID-19 pandemic in six European countries. Int J Health Plann Manag. (2022) 37:2032–48. doi: 10.1002/hpm.3446
10. Burke, S , Parker, S , Fleming, P , Barry, S , and Thomas, S . Building health system resilience through policy development in response to COVID-19 in Ireland: from shock to reform. Lancet Reg Health Eur. (2021):100223. doi: 10.1016/j.lanepe.2021.100223
11. Vasileiou, E . Fighting a war without weapons? Lessons from the COVID-19 outbreak. World Med Health Policy. (2021) 13:383–90. doi: 10.1002/wmh3.431
12. Xu, H , Intrator, O , and Bowblis, JR . Shortages of staff in nursing homes during the COVID-19 pandemic: what are the driving factors? J Am Med Dir Assoc. (2020) 21:1371–7. doi: 10.1016/j.jamda.2020.08.002
13. Alqahtani, F , Khan, A , Alowais, J , Alaama, T , and Jokhdar, H . Bed surge capacity in Saudi hospitals during the COVID-19 pandemic. Disaster Med Public Health Prep. (2021) 16:2446–52. doi: 10.1017/dmp.2021.117
14. Aparicio Betancourt, M , Duarte-Díaz, A , Vall-Roqué, H , Seils, L , Orrego, C , Perestelo-Pérez, L, et al. Global healthcare needs related to COVID-19: an evidence map of the first year of the pandemic. Int J Environ Res Public Health. (2022) 19:10332. doi: 10.3390/ijerph191610332
15. Legido-Quigley, H , Mateos-García, JT , Campos, VR , Gea-Sánchez, M , Muntaner, C , and McKee, M . The resilience of the Spanish health system against the COVID-19 pandemic. Lancet Public Health. (2020) 5:e251–2. doi: 10.1016/S2468-2667(20)30060-8
16. Equipo COVID19 . (2021) Informe no 86 Situación de COVID-19 en España a 7 de julio de 2021. RENAVE. CNE. CNM (ISCIII); [cited 2022 Dec 21]. Available at: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Paginas/Informes_Previos_Covid-12_2021.aspx (Accessed December 21, 2022).
17. Linde, P. (2020). Sanidad confirma en La Gomera el primer caso de coronavirus en España. El País. Available at: https://elpais.com/sociedad/2020/01/31/actualidad/1580509404_469734.html (Accessed December 15, 2022).
18. Dong, E , Du, H , and Gardner, L . An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect Dis. (2020) 20:533–4. doi: 10.1016/S1473-3099(20)30120-1
19. Centro de Coordinación de Alertas y Emergencias Sanitarias (CCAES) . (2020) Enfermedad por nuevo coronavirus, COVID-19. Resumen de la situación. Actualizaciones de la enfermedad por SARS-CoV-2 (COVID-19). Ministerio de Sanidad. Available at: https://www.sanidad.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/home.htm (Accessed December 09, 2022).
20. Chang, AY , Cullen, MR , Harrington, RA , and Barry, M . The impact of novel coronavirus COVID-19 on noncommunicable disease patients and health systems: a review. J Intern Med. (2021) 289:450–62. doi: 10.1111/joim.13184
21. Ocaña, C , Bandrés, E , Chuliá, E , Fernández, MJ , Malo, MÁ , Rodríguez, JC, et al. Impacto social de la pandemia en España. Una evaluación preliminar. Madrid: FUNCAS (2020).
22. Faggioni, MP , González-Melado, FJ , and Pietro, MLD . National health system cuts and triage decisions during the COVID-19 pandemic in Italy and Spain: ethical implications. J Med Ethics. (2021) 47:–7. doi: 10.1136/medethics-2020-106898
23. Equipo COVID19 . (2021) Informe no 70. Situación de COVID-19 en España a 17 de marzo de 2021. RENAVE. CNE. CNM (ISCIII). Available at: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Paginas/Informes_Previos_Covid-12_2021.aspx (Accessed December 14, 2022).
24. Braun, V , and Clarke, V . Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
25. Cameron, JJ , and Stinson, DA . Gender (mis)measurement: guidelines for respecting gender diversity in psychological research. Soc Personal Psychol Compass. (2019) 13. doi: 10.1111/spc3.12506
26. Muñoz Moreno, R , Chaves-Montero, A , Morilla-Luchena, A , and Zquez-Aguado, O . COVID-19 and social services in Spain. PLoS One. (2020) 15:e0241538. doi: 10.1371/journal.pone.0241538
27. The Health Foundation . (2021) Quality improvement made simple – The Health Foundation. Available at: https://www.health.org.uk/publications/quality-improvement-made-simple (Accessed January 26, 2023).
28. Cutrer, WB , and Ehrenfeld, JM . Protocolization, standardization and the need for adaptive expertise in our medical systems. J Med Syst. (2017) 41:200. doi: 10.1007/s10916-017-0852-y
29. Alfonso Viguria, U , and Casamitjana, N . Early interventions and impact of COVID-19 in Spain. Int J Environ Res Public Health. (2021) 18:4026. doi: 10.3390/ijerph18084026
30. Lau, VI , Dhanoa, S , Cheema, H , Lewis, K , Geeraert, P , Lu, D, et al. Non-COVID outcomes associated with the coronavirus disease-2019 (COVID-19) pandemic effects study (COPES): a systematic review and meta-analysis. PLoS One. (2022) 17:e0269871. doi: 10.1371/journal.pone.0269871
31. Cano-Valderrama, O , Morales, X , Ferrigni, CJ , Martín-Antona, E , Turrado, V , García, A, et al. Acute care surgery during the COVID-19 pandemic in Spain: changes in volume, causes and complications. A multicentre retrospective cohort study. Int J Surg. (2020) 80:157–61. doi: 10.1016/j.ijsu.2020.07.002
32. Amador, M , Matias-Guiu, X , Sancho-Pardo, G , Martinez, JC , De La, T-MJC , Saiz, AP, et al. Impact of the COVID-19 pandemic on the care of cancer patients in Spain. ESMO Open. (2021) 6:100157. doi: 10.1016/j.esmoop.2021.100157
33. Sokol-Hessner, L , Folcarelli, PH , Annas, CL , Brown, SM , Fernandez, L , Roche, SD, et al. A road map for advancing the practice of respect in health care: the results of an interdisciplinary modified Delphi consensus study. Jt Comm J Qual Patient Saf. (2018) 44:463–76. doi: 10.1016/j.jcjq.2018.02.003
34. Peña-Longobardo, LM , Oliva-Moreno, J , García-Armesto, S , and Hernández-Quevedo, C . The Spanish long-term care system in transition: ten years since the 2006 dependency act. Health Policy. (2016) 120:1177–82. doi: 10.1016/j.healthpol.2016.08.012
35. Ruano, JM , and Díaz-Tendero, A . COVID-19 and the structural vulnerabilities in the Spanish health and long-term care systems. Eur Polit Sci. (2023) 22:395–405. doi: 10.1057/s41304-022-00381-x
36. Vicente, FF . La atención y coordinación sociosanitaria: hacia una nueva cultura del cuidado. Enferm Clínica Engl Ed. (2020) 30:291–4. doi: 10.1016/j.enfcli.2020.09.001
37. Parker, A , Brigham, E , Connolly, B , McPeake, J , Agranovich, A , Kenes, M, et al. Addressing the post-acute sequelae of SARS-CoV-2 infection: a multidisciplinary model of care. Lancet Respir Med. (2021) 9:1328–41. doi: 10.1016/S2213-2600(21)00385-4
38. Barker, I , Steventon, A , and Deeny, SR . Association between continuity of care in general practice and hospital admissions for ambulatory care sensitive conditions: cross sectional study of routinely collected, person level data. BMJ. (2017):j84. doi: 10.1136/bmj.j84
39. Gray, DP , Evans, P , Sweeney, K , Lings, P , Seamark, D , Seamark, C, et al. Towards a theory of continuity of care. J R Soc Med. (2003) 96:160–6. doi: 10.1177/014107680309600402
40. Baker, R , and Streatfield, J . What type of general practice do patients prefer? Exploration of practice characteristics influencing patient satisfaction. Br J Gen Pract J R Coll Gen Pract. (1995) 45:654–9.
41. Tayyib, NM . An action plan to address the mental health impact of COVID-19 on communities: five effective strategies. Psychol Serv. (2022) 19:5–16. doi: 10.1037/ser0000575
42. Schaefert, R , Stein, B , Meinlschmidt, G , Roemmel, N , Blanch, J , Boye, B, et al. COVID-19-related consultation-liaison (CL) mental health services in general hospitals: a perspective from Europe and beyond. J Psychosom Res. (2023) 167:111183. doi: 10.1016/j.jpsychores.2023.111183
43. Horn, M , Granon, B , Vaiva, G , Fovet, T , and Amad, A . Role and importance of consultation-liaison psychiatry during the COVID-19 epidemic. J Psychosom Res. (2020) 137:110214. doi: 10.1016/j.jpsychores.2020.110214
44. David, E , DePierro, JM , Marin, DB , Sharma, V , Charney, DS , and Katz, CL . COVID-19 pandemic support programs for healthcare workers and implications for occupational mental health: a narrative review. Psychiatry Q. (2022) 93:227–47. doi: 10.1007/s11126-021-09952-5
45. Capolongo, S , Gola, M , Brambilla, A , Morganti, A , Mosca, EI , and Barach, P . COVID-19 and healthcare facilities: a Decalogue of design strategies for resilient hospitals. Acta Bio Medica Atenei Parm. (2020) 91:50–60. doi: 10.23750/abm.v91i9-S.10117
46. Linde, P , and Grasso, D . (2021). COVID-19: Spain struggling to contain third coronavirus wave as more infectious strain takes hold | society | EL PAÍS English edition. Available at: https://english.elpais.com/society/2021-01-25/spain-struggling-to-contain-third-coronavirus-wave-as-more-infectious-strain-takes-hold.html (Accessed January 31, 2023).
Keywords: COVID-19, needs assessment, health services, social services, patients, health personnel, public health, Spain
Citation: Duarte-Díaz A, Aparicio Betancourt M, Seils L, Orrego C, Perestelo-Pérez L, Barrio-Cortes J, Beca-Martínez MT, Bermejo-Caja CJ and González-González AI (2023) COVID-19 healthcare and social-related needs from the perspective of Spanish patients and healthcare providers: a qualitative analysis of responses to open-ended questions. Front. Public Health. 11:1166317. doi: 10.3389/fpubh.2023.1166317
Edited by:
Satish Chandrasekhar Nair, Tawam Hospital, United Arab EmiratesReviewed by:
Eva Turk, St. Pölten University of Applied Sciences, AustriaCopyright © 2023 Duarte-Díaz, Aparicio Betancourt, Seils, Orrego, Perestelo-Pérez, Barrio-Cortes, Beca-Martínez, Bermejo-Caja and González-González. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariana Aparicio Betancourt, bWFwYXJpY2lvQGZhZHEub3Jn
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.