 Isabel Pemjean
Isabel Pemjean Fernanda Mediano
Fernanda Mediano Pedro Ferrer
Pedro Ferrer María Luisa Garmendia
María Luisa Garmendia Camila Corvalán
Camila Corvalán- 1Doctoral Program in Public Health, School of Public Health, University of Chile, Santiago, Chile
- 2Carolina Population Center, University of North Carolina, Chapel Hill, NC, United States
- 3Center for Research in Food Environments and Prevention of Nutrition-Related Diseases (CIAPEC), Institute of Nutrition and Food Technology, University of Chile, Santiago, Chile
Introduction: Food access is associated with dietary quality; however, people living in similar physical environments can have different food access profiles. Domestic environments may also influence how food access relates to dietary quality. We studied food access profiles of 999 low-middle income Chilean families with children during the COVID-19 lockdown and how these profiles relate to dietary quality; secondarily, we also explore the role of the domestic environment in this relationship.
Materials and methods: Participants of two longitudinal studies conducted in the southeast of Santiago, Chile, answered online surveys at the beginning and end of the COVID-19 pandemic lockdown. Food access profiles were developed by a latent class analysis considering food outlets and government food transfers. Children's dietary quality was estimated by self-reported compliance with the Chilean Dietary Guidelines of Americans (DGA) and daily ultra-processed food (UPF) consumption. Logistic and linear regressions were used to assess the association between food access profiles and dietary quality. Domestic environment data (i.e., the sex of the person who buys food and cooks, meal frequency, cooking skills, etc.) were incorporated in the models to assess their influence on the relationship between food access and dietary quality.
Results: We have categorized three food access profiles: Classic (70.2%), Multiple (17.9%), and Supermarket-Restaurant (11.9%). Households led by women are concentrated in the Multiple profile, while families from higher income or education levels are focused on the Supermarket-Restaurant profile. On average, children presented poor dietary quality, with a high daily UPF consumption (median = 4.4; IQR: 3) and low compliance with national DGA recommendations (median = 1.2; IQR: 2). Except for the fish recommendation (OR = 1.77, 95% CI:1.00–3.12; p: 0.048 for the Supermarket-Restaurant profile), the food access profiles were poorly associated with children's dietary quality. However, further analyses showed that domestic environment variables related to routine and time use influenced the association between food access profiles and dietary quality.
Conclusion: In a sample of low-middle income Chilean families, we identified three different food access profiles that presented a socioeconomic gradient; however, these profiles did not significantly explain children's dietary quality. Studies diving deeper into household dynamics might give us some clues on intra-household behaviors and roles that could be influencing how food access relates to dietary quality.
1. Introduction
Poor-quality diets are the leading risk factor for premature death globally, and improving diets could prevent one in five deaths (1). Difficulties in food acquisition (i.e., economic, physical, and social) (2) have been identified as one of the most critical variables concerning diet quality, particularly in low- and middle-income communities (3, 4). However, studies assessing the association between food access and specific health, or nutritional outcomes provide inconsistent results (5, 6). The lack of specificity in particular instruments and indicators (6, 7) may be responsible for the inability to differentiate between populations living in similar physical environments.
The food environment has been defined as “the interface that mediates people's food acquisition and consumption within the wider food system” (2). When considering the food environment, there are two main dimensions: external factors such as availability, prices, food properties, and marketing, as well as personal factors such as accessibility, affordability, convenience, and how desirable the food products are. For children and adolescents, this also includes their behaviors and those of their caregivers when procuring, preparing, and eating food (8). The domestic environment is a setting where personal and behavioral dimensions occur. It is the primary space where children socialize and learn about food tastes, preparation, and traditions (9). However, it is rarely explored (2, 10). Recent evidence suggests that domestic environment variables, such as gender (11), and intra-household relationships (12, 13), can reflect coping strategies (14, 15) that ultimately shape how food environments impact people's life (16).
In Chile, food insecurity is no longer an issue (17); however, excessive consumption of nutrients related to nutrition-related chronic diseases such as sugars, sodium, and saturated fats is a major concern (18). Evidence of dietary quality among children is particularly scarce but suggests large consumption of ultra-processed foods (19). Chile has a modern food system (20) characterized by an abundance of food, including the so-called ultra-processed foods (UPF) that have been related to a high risk of obesity and other chronic diseases (21). People live mostly in urban settings with a high concentration of market-based food sources, including many options to eat outside the home (22). Before the pandemic, supermarkets and markets were important food supply places in Latin-American countries (LAC) and Chile, with some peculiarities. Chile is one of the LAC countries with the highest expansion of supermarkets. Along with this growth, the sales of unhealthy processed foods have increased over the last decade (23). Supermarkets have replaced shopping in neighborhood grocery and convenience stores, which have now become places where people buy discretionary foods or ingredients to cook a single meal (24). Eating outside of the home or purchasing take-home foods from restaurants has also increased, particularly in high-income levels (24). In Santiago, the capital of Chile, open markets concentrate in low-middle-income sectors (25). Although they represent the main point of fruits, vegetables, and fish distribution (26), they currently offer all types of foods, including UPF. Chile also has strong social welfare and healthcare programs that consider the provision of free food through school and primary healthcare centers to groups with special nutritional needs, such as pregnant women, infants, and older adults.
In 2020, the country was hit by the COVID-19 pandemic, implementing rigorous confinement and lockdown measures, including curfews and school closures for the entire year. Food availability was not interrupted because of intense efforts to ensure food distribution and availability (27). Although open fairs were initially closed, they were quickly reopened. Additionally, agricultural production was declared an essential activity ensuring its continuity. However, food acquisition was hampered by restrictions on people's movement (20). To mitigate these effects, the government implemented food assistance measures: the school feeding program was replaced by the delivery of food boxes for in-home meal preparation, and a food box program targeted to low-income families was implemented at two points during the 1st year of the pandemic.
Thus, the current project aimed to describe food access profiles of low-middle income families participating in the longitudinal studies of the Center for Research in Food Environments and Prevention of Nutrition-Related Diseases (CIAPEC) conducted in the southeast area of Santiago, Chile, during the COVID-19 lockdown and how they relate to the dietary quality of children and adolescents during the same period; we secondarily explore how the domestic environment influenced this relationship.
2. Materials and methods
2.1. Study design
This was a longitudinal study. Food access and domestic food environment variables were collected from July to November 2020, (i.e., the first lockdown of Santiago), and dietary quality variables were measured in December 2020–February 2021, (i.e., lockdown opening) in households with children and adolescents participating in the CIAPEC cohorts. Data were primarily collected online (1582; 79.2%) and complemented with phone interviews (416; 20.8%).
2.2. Study participants
All families who participated in two longitudinal studies conducted in the Southeast area of Santiago in 2020 were invited to participate. The Growth and Obesity Cohort Study (GOCS) comprises children born in 2002–2003 recruited from public nursery schools in 2006. The inclusion criteria included being singleton term births, having birth weights between 2,500 and 4,500 g, and being free from conditions that affect growth (28). The Food Environment Chilean Cohort (FECHIC) includes children born in 2011–2012 and recruited in 2016 following the same recruitment procedures and inclusion criteria in the GOCS. According to the characterization of their neighborhoods of residence, households in both cohorts are considered low- and middle-income (29).
Only participants who continue to reside in the southeastern area of Santiago and who completed the sociodemographic and dietary sections of the surveys were included in this study. A sample of 999 households was obtained: 531 GOCS adolescents [17.6 years (SD 0.7), 54.8% girls] and 468 FECHIC children [8.8 years (SD 0.8), 51.9% girls]. Compared to the initial cohorts, participants did not differ significantly in age, sex, and nutritional status. However, maternal education was higher than in the initial cohorts, and more women participated only in the GOCS cohort.
This study was conducted following the Declaration of Helsinki, and the Ethics Committee of the Faculty of Medicine (University of Chile) approved his protocol.
2.3. Variables
Variables were defined as (1) outcomes: children's dietary quality; (2) predictors: food access profiles; (3) domestic environment variables; (a) food management; (b) COVID-19 pandemic routine modification (from now on, routine modification variables), and (4) sociodemographic covariables. The data collected related to the two weeks before the interview. In the case of FECHIC, the caregivers provided the data, while in the case of GOCS, the adolescents did it.
Dietary quality was measured by two variables: UPF consumption and accomplishment of the Chile dietary guidelines (DGA) (30). UPF consumption was measured with the NOVA score for the consumption of ultra-processed foods (31) that has been validated in Brazil (32) and in Chilean adolescents and young adults (under review data show good concordance with R24). The NOVA score is a 0 to 20-point scale: the consumption of each 20 UPF the previous day is counted as 1 point. DGA compliance is a 0 to 5-point scale where compliance with recommended consumption for each food group (fish, legumes, dairy, fruits and vegetables, and water) is counted as 1 point.
Food access profiles were estimated based on market-based food outlets (binary categorical variables of food purchase in the supermarket, open market, neighborhood grocery, larger food market, convenience store, pharmacy, bulk store, and restaurant), and government food transfers grouped into two binary categorical variables (received food support from the government before and during COVID-19). Given the urban nature of the study sample, we considered that own productions and harvested food did not apply as a food source in this context.
Sociodemographic variables included median household income according to Chilean minimum wage, head of household sex, mother's educational level, numerous households (more than three children), and sex and age of the child or adolescent.
We also explored the role of domestic environment variables: (1) food management: this set of variables included the sex of the main person in charge of buying and cooking food, with mastery of five or more cooking skills (boiling, steaming, frying, sautéing, grilling, baking/roasting, stewing, and microwaving) and the child meal frequency pattern (breakfast, lunch, and dinner). (2) Routine modification variables: This set of variables included increased hours dedicated to online work and housework, decreased hours dedicated to in-person work, and difficulties due to school closures in different areas. A more equitable gender distribution of food tasks (33, 34), the ability to prepare meals with a variety of cooking skills (35), and children having a meal frequency pattern have been described as protective factors for the child's quality diet (36). On the contrary, time constraints have been defined as risk factors for children's quality diet (37, 38). The COVID-19 lockdown measures (i.e., increased online work and school closures) raised household chores and stressed available time (39).
2.4. Statistical analysis
Quantitative variables were described as mean and standard deviation or as the median and interquartile range (if not normally distributed, assessed by the Shapiro–Wilk test) and categorical variables as number and percentage.
External food access profiles were elaborated with the latent class analysis (LCA). The LCA was chosen because the main food supply sites are considered a proxy for hidden socio-cultural variables (40). We incorporated the sociodemographic variables into the LCA model, so it reported the logistical/multinomial regression results between them and the food access profiles. This approach was preferred to estimating the model without covariates and then estimating their association with the covariates since the literature has shown that the latter produces downward biased estimates of the effects of the covariates (41). We estimated the degree of model's fit with one to three profiles (the model stopped converging at three profiles). Following the principle of parsimony and goodness-of-fit (Akaike Information Criteria and Bayesian Information Criteria), we selected the three latent class models with the following sociodemographic variables: median household income, head of household sex, and mother's educational level (all p-values <0.05). We assigned a name to each profile highlighting their food access differences using the item-response probabilities. Finally, households were assigned to a profile according to the posterior probability predictions (41, 42).
According to Gudicha et al. (43), a sample size of 999 is sufficient to obtain power over 95% in estimating three classes, even with a low association between the class and the indicator and unequal sizes between classes. This sample size would also allow us to find statistically significant small effect sizes assuming a power of 80% and an alpha error of 5% and also three predictors (44).
Associations between food access profiles and children's dietary quality were estimated using linear regression models for discrete variables and logistic regression models for categorical variables, adjusting for the sex and age of the child. To explore the effect of the domestic environment in these associations, we further adjusted the models by the domestic variables associated with the food access profiles. We incorporated the food management covariables first and then the routine modification variables. We compared the effects of the crude and adjusted regressions.
Associations between food access profiles and domestic food environment were estimated using multinomial regressions adjusted for the sex and age of the child. First, we estimated univariate models, and for each set of covariables (food management and routine modification), we retained those with a p-value of <0.05. Second, we estimated multivariable models for each set of covariables and retained those with a p-value <0.05.
For all analyses, interactions by the cohort study were tested and found non-significant; thus, analyses are combined for both cohorts.
All analyses were done with Stata v 16. All materials are available upon request to interested researchers.
3. Results
3.1. Descriptive results
Nine hundred and ninety-nine households participated in the study (Table 1). The median age of children was 13.5 years (IQR:9), with a similar number of girls and boys. Almost 2/3rds of the households (77.7%) received less than two minimum wages1 per month and 40.2% of the households received less than one. Women were the head of the household in almost half of the sample (47.2%), and they were also responsible for almost all food purchases (82.6%) and food preparation (92.3%).
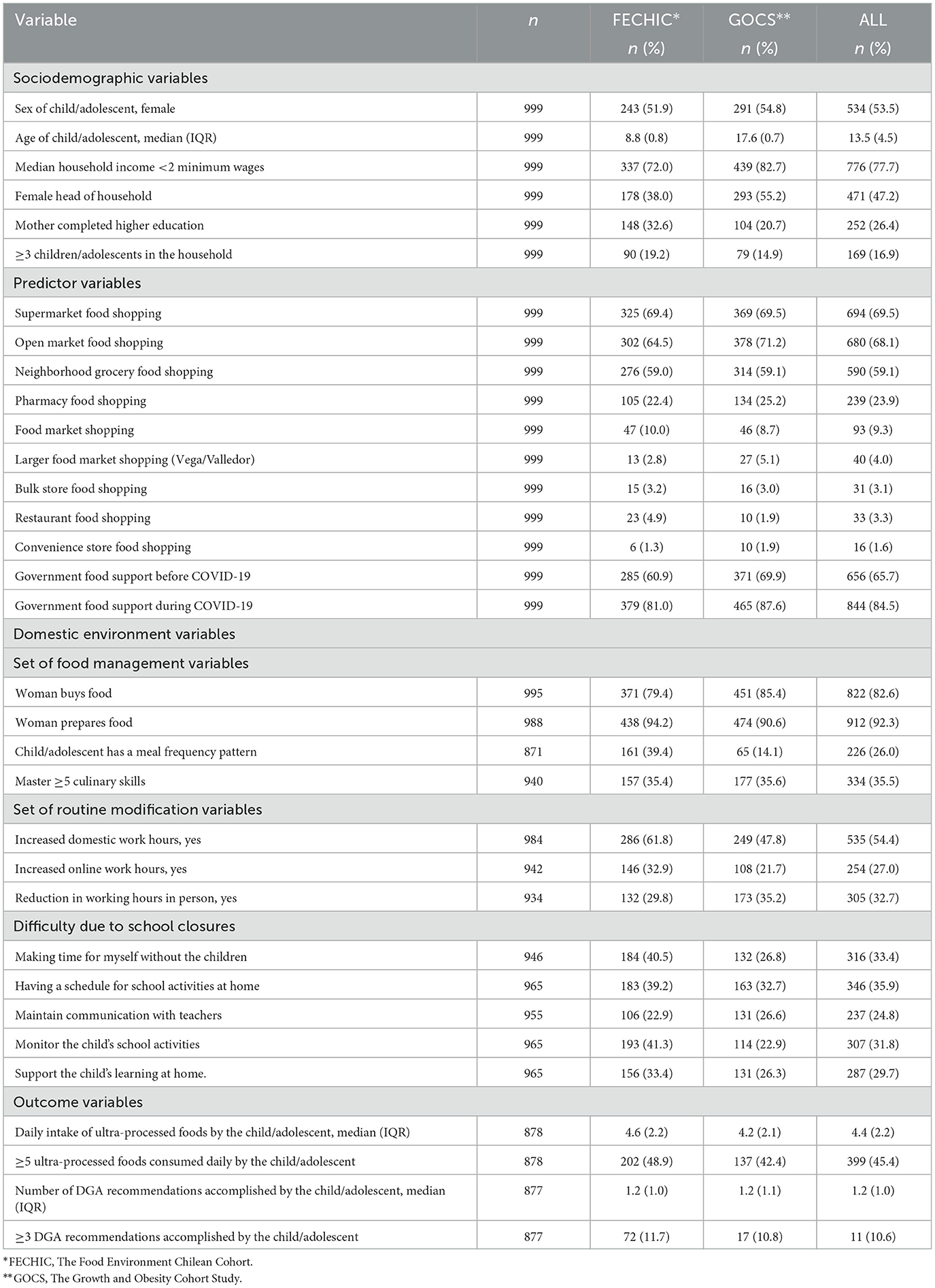
Table 1. Main variables from 999 households in southeastern Santiago, Chile.
During the first COVID-19 lockdown, almost a third (32.7%) of the households decreased in-person work, with a slightly lower increase in online work (27.0%). Conversely, hours dedicated to domestic work increased in more than half of the households (54.4%). One-third of them experienced some difficulty associated with the closing of the schools either having time for themselves without the child (33.4%), keeping a schedule for school activities at home (35.9%), or controlling the child's homework at home (31.8%).
On average, children presented poor diet quality, with a high UPF consumption [median = 4.4; (IQR:3); 45.4% >5 UPFs per day]; and low compliance with national DGA recommendations [median = 1.2 (IQR:2); 11.4% ≥3 DGA].
Regarding the places of food acquisition during the lockdown, households bought their food mainly in supermarkets (69.5%) and open markets (68.1%) and slightly less in neighborhood grocery stores (59.1%). However, pharmacies (23.9%) are also noteworthy for their high prevalence. Almost two-thirds of the study families received food support from the government before the pandemic (65.7%), and this figure increased to 84.5% during the pandemic.
3.2. Food access profiles
Three food access profiles were confirmed (Figure 1). They were differentiated mainly by the place of food acquisition although some differences were also observed regarding food assistance components. The most prevalent profile (701 households, 70.2%) was called Classic (profile 1) because it included households that mainly obtained food in open markets, supermarkets, and neighborhood grocery stores. The second most prevalent profile (17.9%) was denominated Multiple (profile 2) because it was characterized by households that buy food in different outlets, including pharmacies. Finally, the Supermarket-Restaurant profile (11.9%) (profile 3) included households in which food was primarily purchased in a supermarket, which also had higher participation of restaurants compared to the other profiles. The first two profiles concentrated on government food support (>70% pre-pandemic and ~100% in lockdown), while in the third profile, coverage was much lower (15% pre-pandemic and 50% in lockdown).
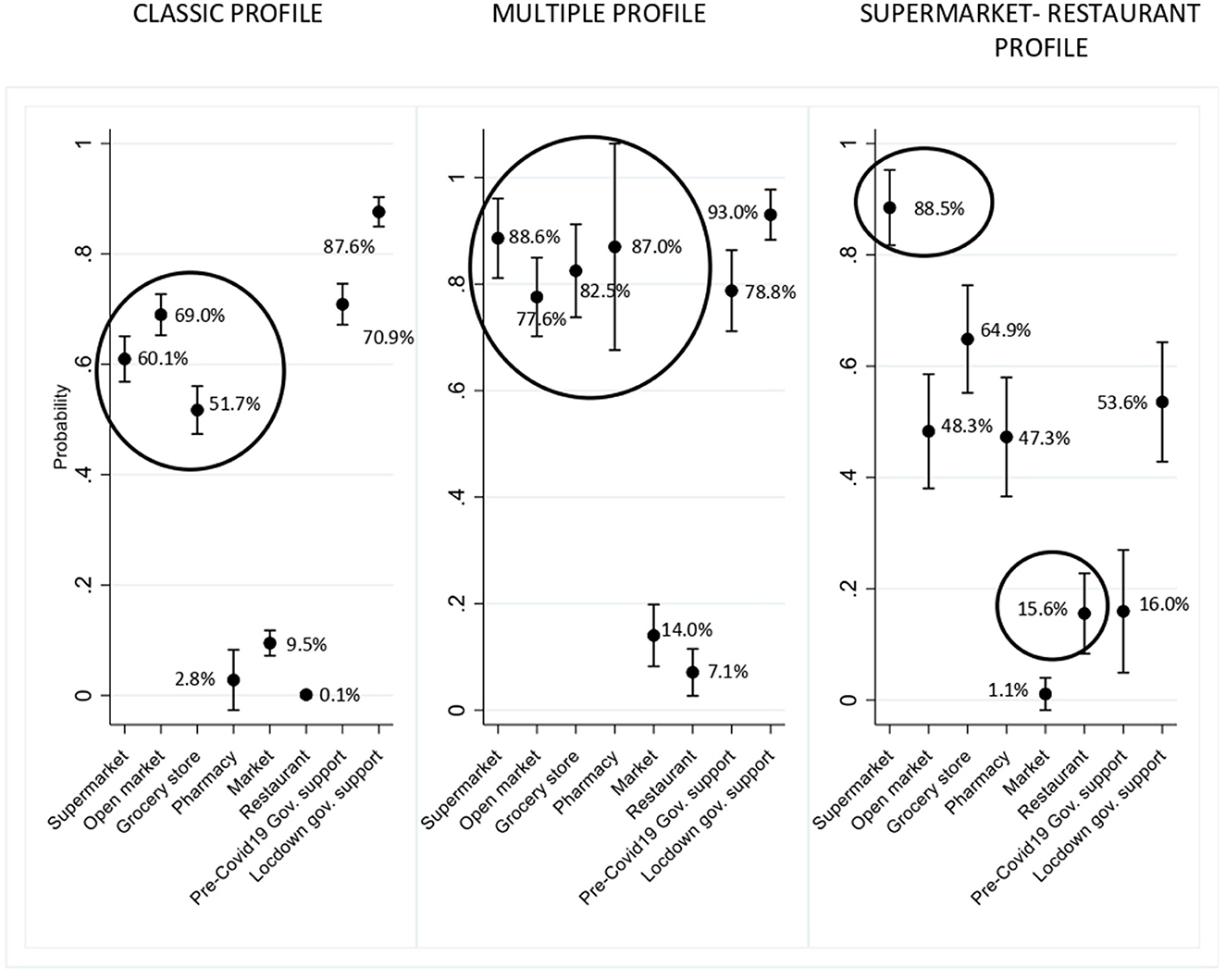
Figure 1. Food access profiles and main places of food access. 999 households in Southeastern Santigo, Chile.
The food access profiles were also related to sociodemographic variables (Table 2). Compared with the classic profile, households with a female head were more likely to be in the Multiple profile [RRR = 1.51; (CI: 0.99–2.32); p: 0.058]. Similarly, households with higher income and with higher maternal educational levels were more likely to be in the Supermarket-Restaurant profile [RRR = 12.30; (CI: 2.88–52.5); p: 0.001 and RRR = 4.58; (CI: 2.22–9.43); p: 0.000, respectively].
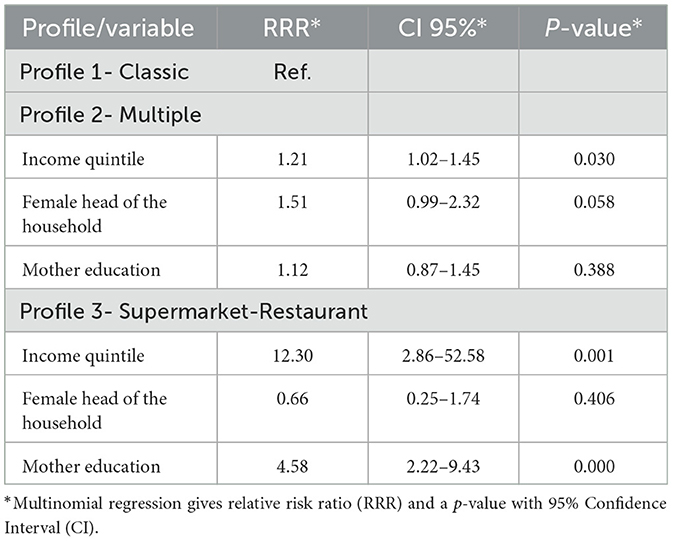
Table 2. External food access profiles by sociodemographic variables for 999 households in southeastern Santiago, Chile.
3.3. Food access profiles and child's dietary quality
We assessed the association between food access profiles and dietary quality (Table 4, unadjusted results). We observed that food access profiles were only associated with fish consumption (the Supermarket-Restaurant profile compared to the classic profile OR = 1.77; CI: 1.00–3.12; p: 0.048) and marginally with the overall compliance of DGA (Profile 3: coefficient = 0.17; CI: −0.04–0.39; p: 0.109).
3.4. Food access profiles and domestic environment characteristics
We also explored whether the domestic environment might influence these results. To do this, we first examined the association between the food access profiles and the domestic environment characteristics (food management and routine modification) (Table 3).
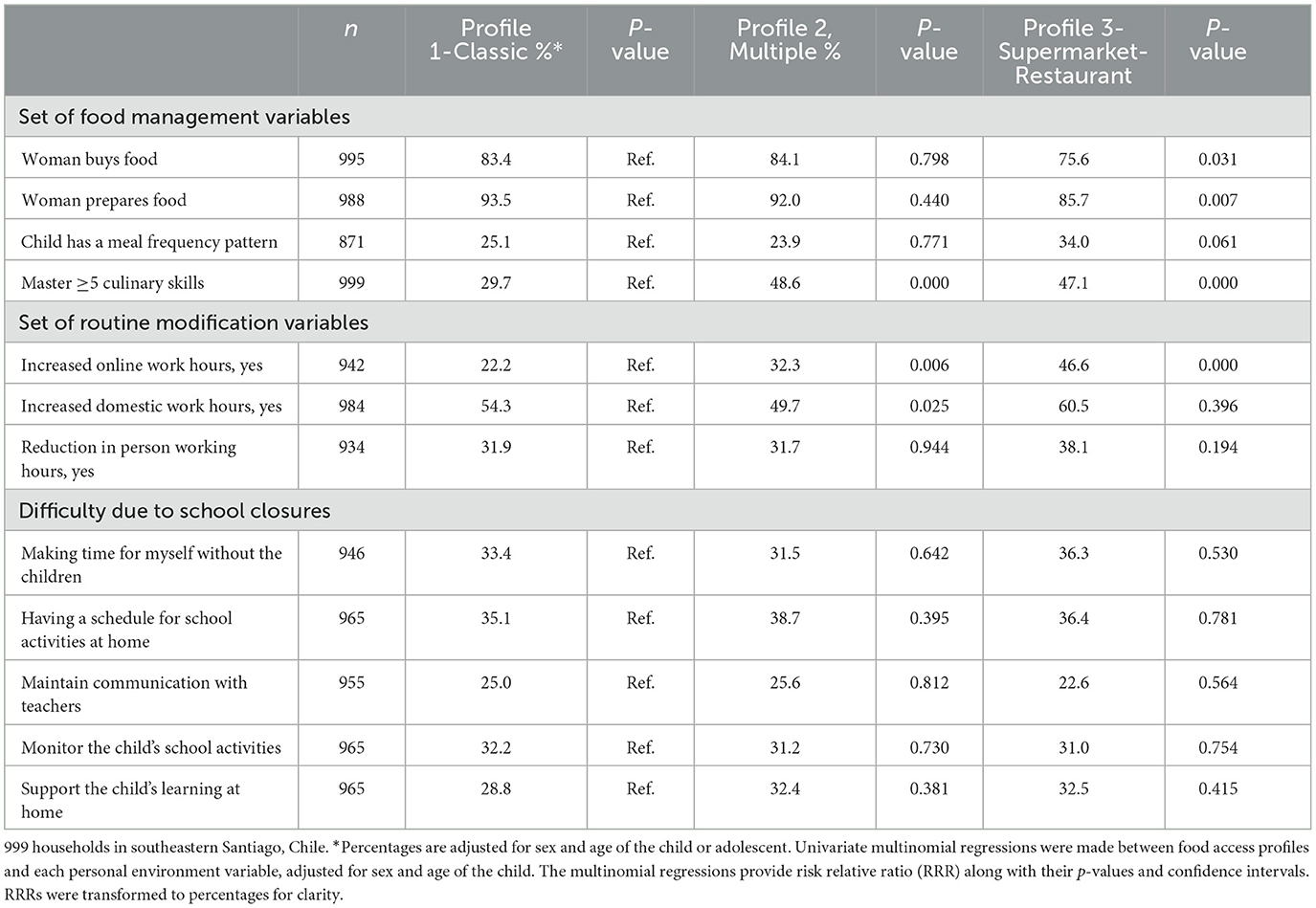
Table 3. Personal environment characteristics according to food access profiles.
In the set of food management characteristics, we found that most differences were concentrated between the Supermarket-Restaurant profile and the Classic one. The Supermarket-Restaurant profile concentrated on protective factors for children's diet quality: it was more frequent to find households with men in charge of preparing food (Profile 3: RRR = 2.11; CI:1.07–4.19; p: 0.032) and almost half of them had mastered a significant number of cooking skills [Profile 3: RRR = 2.16; (CI:1.44–3.25); p: 0.000]. The Multiple profile was only associated with mastering five or more culinary skills (Profile 2: RRR = 2.28; CI:1.63–3.21; p: 0.000).
In the set of routine modifications, we found that the Supermarket-Restaurant profile compared to the Classic one had a higher increase in online work during the pandemic [Profile 3: RRR = 3.25; (CI: 2.12–4.97); p: 0.000]. The Multiple profile also presented a significantly more increase in online work than the Classic profile [Profile 2: RRR = 1.79; (CI: 1.21–2.65); p: 0.004], but the increase in domestic work was significantly lower than in the Classic profile [Profile 2: RRR = 0.54; (CI: 0.33–0.89); p: 0.015], even after adjusting for other covariables. There were no significant differences between profiles concerning decreased in-person work and difficulties associated with school closures.
When adjusting the regressions by the food management variables retained, we did not observe changes in the results (Table 4). However, when adjusting the routine modification variables, we observed that in the Supermarket-Restaurant profile (i.e., the one whose routines were most impacted by the pandemic), the likelihood of compliance with the DGA (overall, fish, legumes, and dairy intake) increased. At the same time, no change was observed in compliance with fruit and vegetable intake and water consumption recommendations. As an example, the number of DGA recommendations accomplished increased from coefficient 0.17 (CI: −0.04 to 0.39; p: 0.109) in the univariate regression to coefficient 0.22 (CI: 0.00 to 0.44; p: 0.049) in the adjusted regression and the probability of consuming fish at least twice a week increased from OR = 1.77 (CI: −1.00 to 3.12; p: 0.048) to OR = 1.96 (CI: −1.09 to 3.52; p: 0.024). We did not observe significant changes in the Multiple profile associations when adjusting for domestic environment. No change was observed in UPF's intake.
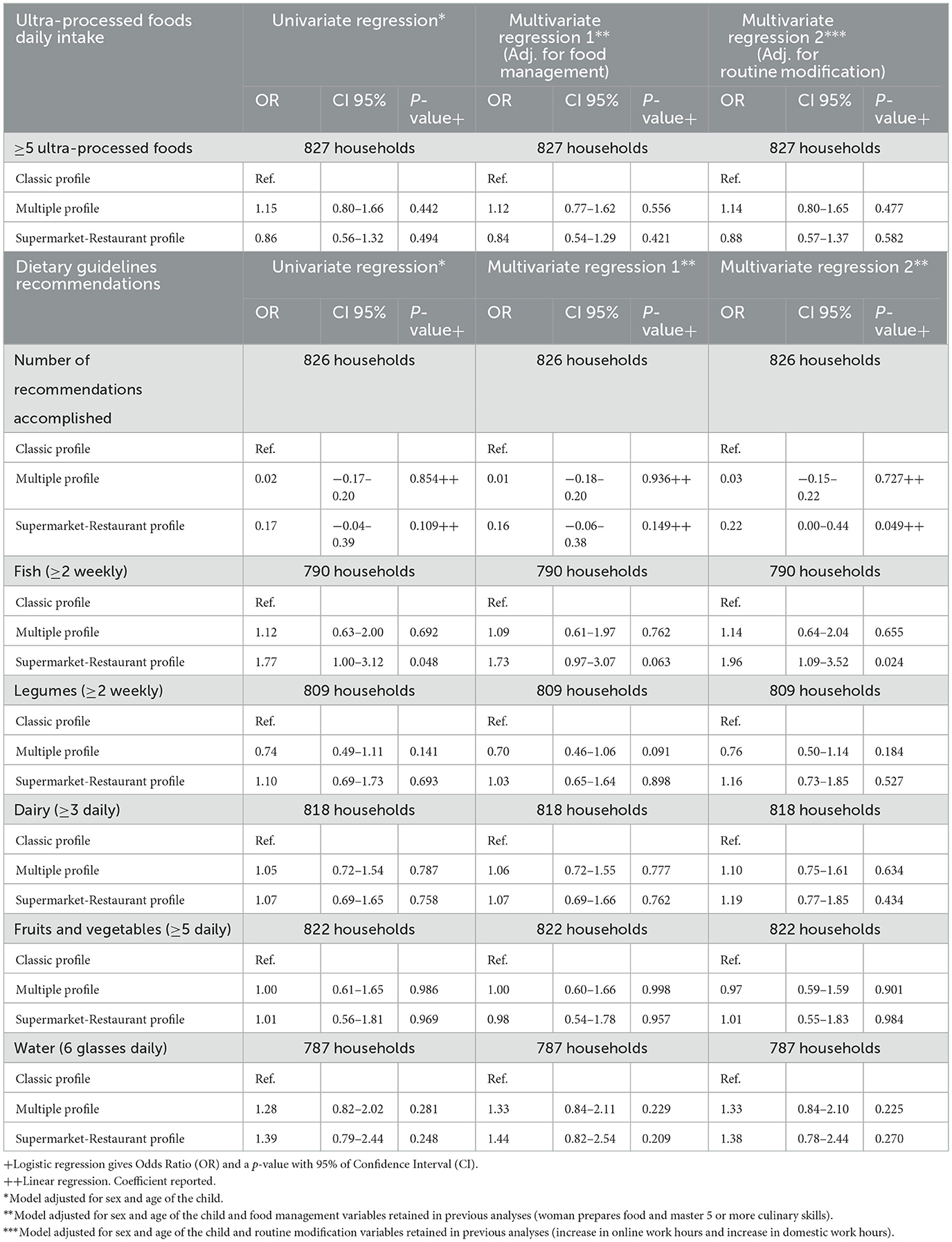
Table 4. Association of food access profiles and children's dietary quality (n = 999 households in southeastern Santiago, Chile), crude and adjusted results.
4. Discussion
In a sample of middle- and low-income Chilean households with children living in similar external food environments, we could identify three food access profiles that vary depending on socioeconomic characteristics of the household, including gender of the head of the household. Household's food access profiles were poorly associated with the children's dietary quality, but the domestic environment influenced how food access related to the quality of dietary intake.
The Classic profile, the most prevalent profile in this sample, accounted for traditional methods of food access among low- and middle-income households in Chilean urban cities, including a combination of food purchases on open markets, supermarkets, and grocery stores, together with high access to government food transfers. However, we also found two other food access profiles in our sample.
The Multiple food access profile was characterized by households who buy foods in multiple food outlets, including small retail businesses, local shops, and even pharmacies. Other studies in Brazil have reported an increase in pharmacy food purchases (45) as a response to time optimization (46). During the COVID-19 lockdown, time away from home was significantly reduced (i.e., families were allowed two 1-h leave per week). Possibly, the main places of food purchases diversification were related to the need to optimize time by making less planned and quicker purchases. In fact, this profile was slightly more prevalent in households with lower income and a greater number of women heads in the household supporting diversification of outlets as a way of coping with less time-resource. Similar coping strategies have been described for Latina mothers who navigate less healthy environments (13).
Finally, the Supermarket-Restaurant profile was characterized by the purchase of delivery food. In Chile as in other Latin American countries, eating away has been increasing in the past decades although the quality of the food purchased varies significantly depending on the socioeconomic classes. In Brazil, it has been reported that people of the highest income levels present the highest expenditure on out-of-home food (47). During the COVID-19 lockdown, there is evidence that families from higher educational levels and higher income were the ones that most frequently used digital channels to access food (48). In Chile, people buy time by buying ready-to-eat food or paying for a maid. Households that cannot afford to pay for food-time experienced more stress. Correspondingly, in this study, we observed that this profile was more frequent among families with higher education and income. Moreover, households in this profile were not part of food assistance programs before the pandemic, but their coverage increased given the difficulties created by the pandemic.
Our study also shows that the profiles were poorly related to the quality of the children's dietary intake. This is likely because this was a relatively homogeneous urban population, in which food availability in the external environment was assured. We observed that almost half of the sample consumed five or more UPFs daily, independently of the type of store where the profile accessed food. In the Brazilian case, Machado et al. (49), reported a positive association between purchasing foods at supermarkets and UPF consumption. However, in our results, the Supermarket-Restaurant profile was not associated with a higher UPF intake in these children. We believe these findings suggest that UPFs have penetrated all types of food stores including open markets. This is aligned with the results of Spires et al. (50) who studied three countries of high-, middle-, and low-income groups, showing that sweetened beverages and confectionaries had permeated all food outlets, independent of the country's income level. Food swamps—urban spaces with high-density unhealthy foods—are becoming a significant concern in countries facing post-transitional nutrition transition phases such as Chile and several Latin-American countries (51).
Overall, in our sample, consumption of healthy foods was low. Approximately 10% followed three or more DGA recommendations (52). This is in line with previous studies that have shown high consumption of UPF by Chilean adults and children and low consumption of healthy foods (18). This is also concordant with advanced stages of the nutrition transition in which increased industrialization of food systems, technological changes, globalization, and transnational food industry penetration has promoted a diet dominated by UPF that displaces the consumption of healthy foods, worldwide (53). Chile has recently implemented the Food Labeling and Advertising Law that considers multiple mutually reinforcing policies including the use of front-of-package warning labels, restricting child-directed marketing, and banning school sales of unhealthy foods to counteract the increase in UPF consumption (54). Initial data showed significant results (55–57); however, the fact that the consumption of UPF continues to be very high indicates the need of implementing complementary policies, also including the promotion of healthy food consumption. Furthermore, reports indicate that Chile had the worst dietary quality during the COVID-19 quarantine among 11 LAC countries (58). A recent evaluation of the Food Labeling and Advertisement Chilean Law reported that mothers from lower socioeconomic status found healthier foods financially inaccessible (59). Several studies have shown that a quality diet is more expensive than one based on UPF (60, 61). In the case of Chile, Cuadrado and García established in 2015 that a food basket that complies with DGA recommendations is 36.1% more expensive than a basic food basket (62). This implies that we must ensure food accessibility in terms of affordability. In the context of the global food crises, this will increasingly become a challenge for lower-income families in most countries (63).
We also demonstrated that the domestic environment's variables, such as changes in routine, could influence the impact of food access on the quality of children's diets. Mastering different culinary skills and having a meal structure have been described as protective factors of the children's diet (35, 36). Several studies from high-income countries have reported that these variables were reinforced by the parent's obligation to stay home during the lockdown as they had more time for food chores (64–66). Our results suggest the contrary since the effect of time disruption on the quality of children's intake was more important than the protective factors. This finding aligns with Jansen et al. (39) study in the US. They reported that households with children did not experience the diet-beneficial effects of the lockdown due to the increased stress levels experienced by parents (caused by the disruption of habits and school closures). On the contrary, the pressure was associated with a worsening of the children's intake.
Our results confirmed that the disruption of timing in domestic environments—produced by COVID-19—impaired the quality of children's diets. Time constraints have been described as a barrier to home cooking in the US (67), Ireland (68), and in general, in high-income countries (69). More evidence is needed in the context of middle-income countries. However, a study conducted in 10 low- and middle-income countries regarding the food and financial crisis in 2007 showed that time constraints could worsen dietary intake (70). A recent study conducted in adolescents shows that convenience emerges as a relevant determinant of food choices when food availability is no longer an issue (71). Our study shows that addressing time issues is needed to better understand barriers to healthy eating at the household level. Studies that can dive deeper into household dynamics might give us some clues on how to materialize these interventions (72).
Moreover, time in the domestic food environment is women's time. Worldwide and in Chile, mothers are the food gatekeepers. i.e., those responsible for the entire food cycle in the household (73, 74). Our results showed that women are almost exclusively responsible for buying and preparing food in all the external food access profiles. According to Clark et al. (75), the pandemic has had a more significant impact on women and has changed household dynamics. As a result, mothers are now taking on more and disproportionately caregiving responsibilities. In Australia, Craig and Churchill (76) reported that although both parents were forced to stay home, gender gaps in housework and care increased. Interestingly, we observed a higher share of this food gatekeeper role in the food access profile that seemed to have better dietary quality (i.e., Supermarket-Restaurant profile). This could indicate that incorporating more people in the household food cycle, i.e., more “personal times,” is a protective factor for the quality of the children's diet. As Constantinides et al. (77) established, it is crucial to incorporate gender equity in the food environment framework as their dynamics in the domestic environment affect the entire food cycle, primarily through time use (78, 79).
Remarkably, in the profile that gathered the women head of household (the Multiple one), although online work during the pandemic increased, the rise in domestic work was the smallest among the three profiles. These results suggest, on the one hand, that women heads of household have access to jobs that did not allow them to stay at home (informal jobs or jobs considered essential such as supermarket cashiers and stocking shelves, among others) (80). On the other hand, women's domestic responsibilities did not increase in this group because they were already very high even under normal pre-pandemic conditions (48). Notably, the quality of children's diet in this profile was not significantly lower than that of the other profiles. Evidence shows that these households were the most affected during the pandemic, particularly those of low income (81). Probably, women implement coping strategies, such as preparing meals in advance and using convenience foods (79), that allow them to maintain the dietary quality of their children even under disruptive conditions. These strategies are really the response to “juggling responsibilities,” and they might have negative implications for women's own health (79). Thus, incorporating a gender perspective into policies promoting healthier nutrition is currently imperative.
5. Limitations of the study
This study has several limitations that are worth mentioning. First, our self-reported dietary intake measurement could introduce potential biases, and using DGA for assessing dietary quality is limited. However, these methods are those traditionally used and can give us a fair idea of children's dietary quality. Second, in the latent class analyses, the names of the profiles are assigned by the researchers, which can lead to a “naming fallacy.” In this study, we named the profiles primarily according to their highest probability of food access and secondarily by highlighting their differences. Third, using a survey approach to the domestic environment is partial; qualitative research could help provide a deeper understanding of the role of the domestic environment. Fourth, the representativeness of this study is restricted to an urban area where food availability is assured. Moreover, we worked only with lower-middle socioeconomic households, but socioeconomic status directly influences diet quality. Further research, including households of other contexts, such as rural sectors and higher socioeconomic status, could improve our understanding of the external and domestic environment interactions in the children's dietary intake quality.
6. Conclusion
We found that food access was poorly related to the dietary quality of low-middle-income Chilean children and adolescents, highlighting that in this urban context, promoting healthier food environments requires interventions that restrict access to UPF foods and favor the affordability of fresh foods rather than just focusing on their availability. In the context of economic crisis and food price inflation, these measures will be particularly relevant for vulnerable groups. Moreover, our results suggest that to improve dietary quality, we also need to intervene intra-households' dynamics and roles that affect food access. Currently, the concentration of the food gatekeeper role on women and their lack of time to fulfill all their responsibilities is a risk factor for children's nutrition and for women's health. Thus, incorporating a gender perspective into nutritional interventions should be a priority to advance in ensuring better diets for all.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Comité de Ética de Investigación en Seres Humanos- Universidad de Chile - Facultad de Medicina. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author contributions
IP and CC conceptualize the study. CC provided essential materials and secure funding for the study. IP wrote the first draft of the manuscript. IP and PF conducted data analyses. CC, IP, FM, and MG contributed to the interpretation of the results. All authors contributed to the manuscript writing and read and approved the final manuscript.
Funding
This study was funded by Anid-COVID#0591, Fondecyt #1201633. IP has a fellowship from the National Agency for Research and Development (ANID): Beca Doctorado Nacional—Doctoral Fellowship Program/2019, Grant No. 21190133.
Acknowledgments
We wish to thank GOCS and FECHIC families, children, and adolescents for their participation and the Center for Research in Food Environments and Prevention of Nutrition-related Chronic Diseases (CIAPEC) team for their assistance in data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^The minimum wage in Chile to date was USD 400 aprox.
References
1. Afshin A, Sur PJ, Fay KA, Cornaby L, Ferrara G, Salama JS, et al. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. (2017). 393:1958–72. doi: 10.1016/S0140-6736(19)30041-8
2. Turner C, Kalamatianou S, Drewnowski A, Kulkarni B, Kinra S, Kadiyala S. Food environment research in low- and middle-income countries: a systematic scoping review. Adv Nutri. (2019) 4:31. doi: 10.1093/advances/nmz031
3. Wolfson JA, Ramsing R, Richardson CR, Palmer A. Barriers to healthy food access: Associations with household income and cooking behavior. Prev Med Rep. (2019) 13:298. doi: 10.1016/j.pmedr.2019.01.023
4. Miller V, Yusuf S, Chow CK, Dehghan M, Corsi DJ, Lock K, et al. Availability, affordability, and consumption of fruits and vegetables in 18 countries across income levels: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet Glob Health. (2016) 4:e695–703. doi: 10.1016/S2214-109X(16)30186-3
5. Mackenbach JD, Nelissen KGM, Dijkstra SC, Poelman MP, Daams JG, Leijssen JB, et al. A systematic review on socioeconomic differences in the association between the food environment and dietary behaviors. Nutrients. (2019) 11:2215. doi: 10.3390/nu11092215
6. Wilkins E, Morris M, Radley D, Griffiths C. Methods of measuring associations between the retail food environment and weight status: importance of classifications and metrics. SSM Popul Health. (2019) 8:100404. doi: 10.1016/j.ssmph.2019.100404
7. Cobb L, Appel L, Franco M, Jones-Smith J, Nur A, Anderson C. The Relationship of the local food environment with obesity: a systematic review of methods, study quality, and results. Obesity. (2015) 23:1331–44. doi: 10.1002/oby.21118
8. Fondo de las Naciones Unidas para la Infancia. las Naciones Unidas para la Infancia, The Global Alliance for Improved Nutrition. UNICEF Florida, Italia: The Innocenti Framework on Food Systems for Children and Adolescents | (2018).
9. Gálvez Espinoza P, Egaña D, Masferrer D, Cerda R. Propuesta de un modelo conceptual para el estudio de los ambientes alimentarios en Chile. Revista Panamericana de Salud Pública. (2017) 4:1–9. doi: 10.26633/RPSP.2017.169
10. Hawkes C, Fox E, Downs SM, Fanzo J, Neve K. Child-centered food systems: reorienting food systems towards healthy diets for children. Glob Food Sec. (2020) 27:100414. doi: 10.1016/j.gfs.2020.100414
11. Jabs J, Devine CM, Bisogni CA, Farrell TJ, Jastran M, Wethington E. Trying to find the quickest way: employed mothers' constructions of time for food. J Nutr Educ Behav. (2007) 39:18–25. doi: 10.1016/j.jneb.2006.08.011
12. Watts AW, Lovato CY, Barr SI, Hanning RM, Mâsse LC. Experiences of overweight/obese adolescents in navigating their home food environment. Public Health Nutr. (2015) 18:3278–86. doi: 10.1017/S1368980015000786
13. Colón-Ramos U, Monge-Rojas R, Cremm E, Rivera IM, Andrade EL, Edberg MC. How Latina mothers navigate a ‘food swamp' to feed their children: a photovoice approach. Public Health Nutr. (2017) 20:1941–52. doi: 10.1017/S1368980017000738
14. Mazarello Paes V, Ong KK, Lakshman R. Factors influencing obesogenic dietary intake in young children (0–6 years): systematic review of qualitative evidence. BMJ Open. (2015) 5:7396. doi: 10.1136/bmjopen-2014-007396
15. Tach L, Amorim M. Constrained, convenient, and symbolic consumption: neighborhood food environments and economic coping strategies among the urban poor. J Urban Health. (2015) 92:815–34. doi: 10.1007/s11524-015-9984-x
16. Pitt E, Gallegos D, Comans T, Cameron C, Thornton L. Exploring the influence of local food environments on food behaviours: a systematic review of qualitative literature. Public Health Nutr. (2017) 20:2393–405. doi: 10.1017/S1368980017001069
17. Organización de las Naciones Unidas para la Alimentación y la Agricultura. las Naciones Unidas para la Alimentación y la Agricultura. El estado de la inseguridad alimentaria en el mundo. FAO (2012).
18. Cediel G, Reyes M, da Costa Louzada ML, Martinez Steele E, Monteiro CA, Corvalán C, et al. Ultra-processed foods and added sugars in the Chilean diet (2010). Public Health Nutr. (2018) 21:125–33. doi: 10.1017/S1368980017001161
19. Araya C, Corvalán C, Cediel G, Taillie LS, Reyes M. Ultra-processed food consumption among chilean preschoolers is associated with diets promoting non-communicable diseases. Front Nutr. (2021) 8:127. doi: 10.3389/fnut.2021.601526
20. Jensen M. Transformación de los sistemas alimentarios en Chile. Estudios Internacionales. (2021) 53:61. doi: 10.5354/0719-3769.2021.59273
21. Pagliai G, Dinu M, Madarena MP, Bonaccio M, Iacoviello L, Sofi F. Consumption of ultra-processed foods and health status: a systematic review and meta-analysis. Br J Nutri. (2021) 125:308–18. doi: 10.1017/S0007114520002688
22. HLPE. Grupo de alto nivel de expertos en seguridad alimentaria y nutrición del Comité de Seguridad Alimentaria Mundial. Roma: La nutrición y los sistemas alimentarios (2017).
23. Organización Mundial de la Salud, Organización Panamericana de la Salud. Alimentos y bebidas ultraprocesados en América Latina: tendencias, efecto sobre la obesidad e implicaciones para las políticas públicas.
24. Astroza S, Guarda P, Carrasco JA. Modeling the relationship between food purchasing, transport, and health outcomes: evidence from Concepcion, Chile. J Choice Modell. (2022) 42:100341. doi: 10.1016/j.jocm.2021.100341
25. Mora R, Bosch F, Rothmann C, Greene M. In Proceedings of the Ninth International Space Syntax Symposium, Seoul, Korea. (2013).
27. Oficina de Estudios y Políticas Agrarias. Reporte COVID-19 abastecimiento e impacto rural Santiago. Santiago: ODEPA (2022).
28. Kain J, Corvalán C, Lera L, Galván M, Uauy R. Accelerated growth in early life and obesity in preschool chilean children. Obesity. (2009) 17:1603–8. doi: 10.1038/oby.2009.37
29. Ministerio de Desarrollo Social. Chile. Casen 2017- Encuesta de caracterización socioeconómica: Equidad de género. Chile: Síntesis de resultados (2018).
30. Ministerio de Salud. Guía alimentaria para la población chilena. Chile: Gobierno de Chile (2013).
31. Monteiro CA, Cannon G, Lawrence M, Costa Louzada ML, Pereira Machado P. Ultra-Processed Foods, Diet Quality, and Health Using the NOVA Classification System. Rome: FAO (2019).
32. Costa C, dos S, Faria FR de, Gabe KT, Sattamini IF, Khandpur N, Leite FHM, et al. Nova score for the consumption of ultra-processed foods: description and performance evaluation in Brazil. Rev Saude Publica. (2021) 55:1–9. doi: 10.11606/s1518-8787.2021055003588
33. Organización de las Naciones Unidas para la Alimentación y la Agricultura. Fortalecer las políticas sectoriales para mejorar los resultados en materia de seguridad alimentaria y nutrición. Nota de orientación sobre políticas. FAO (2018) 6.
34. Twyman J, Talsma EF, Togka K, Ferraboschi C, Brouwer ID. Gender equity considerations in food environments of low and middle income countries. A Scop Rev. (2020) 3:4225. doi: 10.2499/p15738coll2.134225
35. Metcalfe JJ, Leonard D. Reprint of “The relationship between culinary skills and eating behaviors: challenges and opportunities for parents and families.” Physiol Behav. (2018) 193:302–6. doi: 10.1016/j.physbeh.2018.07.006
36. Paoli A, Tinsley G, Bianco A, Moro T. The influence of meal frequency and timing on health in humans: the role of fasting. Nutrients. (2019) 11:719. doi: 10.3390/nu11040719
37. Monsivais P, Aggarwal A, Drewnowski A. Time spent on home food preparation and indicators of healthy eating. Am J Prev Med. (2014) 47:796. doi: 10.1016/j.amepre.2014.07.033
38. Berge JM, Arikian A, Doherty WJ, Neumark-Sztainer D. Healthful eating and physical activity in the home environment: results from multifamily focus groups. J Nutr Educ Behav. (2012) 44:123–31. doi: 10.1016/j.jneb.2011.06.011
39. Jansen E, Thapaliya G, Aghababian A, Sadler J, Smith K, Carnell S. Parental stress, food parenting practices and child snack intake during the COVID-19 pandemic. Appetite. (2021) 161:105119. doi: 10.1016/j.appet.2021.105119
40. Aggarwal A, Cook AJ, Jiao J, Seguin RA, Moudon AV, Hurvitz PM, et al. Access to supermarkets and fruit and vegetable consumption. Am J Public Health. (2014) 104:917. doi: 10.2105/AJPH.2013.301763
41. Magidson Ja, Vermunt J, Mafura J. Latent Class Analysis. Foundation entries. London: SAGE Research Methods Foundations. (2020).
42. Hagenaars J, McCutcheon A. Applied Latent Class Analysis. Hagenaars J, McCutcheon A, editors. London: Cambridge University Press (2002). doi: 10.1017/CBO9780511499531
43. Gudicha DW, Tekle FB, Vermunt JK. Power and sample size computation for Wald tests in latent class models. J Classif. (2016) 33:30–51. doi: 10.1007/s00357-016-9199-1
44. Cohen J. Statistical power analysis for the behavioral sciences. Routledge. (2013) 3:7587. doi: 10.4324/9780203771587
45. Serafim P, Borges CA, Cabral-Miranda W, Jaime PC. Ultra-processed food availability and sociodemographic associated factors in a Brazilian municipality. Front Nutr. (2022) 9:8089. doi: 10.3389/fnut.2022.858089
46. Caspi CE, Lenk K, Pelletier JE, Barnes TL, Harnack L, Erickson DJ, et al. Food and beverage purchases in corner stores, gas-marts, pharmacies and dollar stores. Public Health Nutr. (2017) 20:2587–97. doi: 10.1017/S1368980016002524
47. Rebouças BVL, de Vasconcelos TM, Sousa MHL, Sichieri R, Bezerra IN. Acquisition of food for away-from-home consumption in Brazil between 2002 and 2018. Cien Saude Colet. (2022) 27:3319–29. doi: 10.1590/1413-81232022278.04632022
48. Jara MF, Leyton B, Cuevas C, Gálvez Espinoza P. Women's perceptions about changes in food-related behaviours at home during COVID-19 pandemic in Chile. Public Health Nutr. (2021) 24:4377–86. doi: 10.1017/S1368980021002639
49. Machado PP, Claro RM, Martins APB, Costa JC, Levy RB. Is food store type associated with the consumption of ultra-processed food and drink products in Brazil? Public Health Nutr. (2018) 21:201–9. doi: 10.1017/S1368980017001410
50. Spires M, Berggreen-Clausen A, Kasujja FX, Delobelle P, Puoane T, Sanders D, et al. Snapshots of urban and rural food environments: EPOCH-based mapping in a high-, middle-, and low-income country from a non-communicable disease perspective. Nutrients. (2020) 12:484. doi: 10.3390/nu12020484
51. Bridle-Fitzpatrick S. Food deserts or food swamps? A mixed-methods study of local food environments in a Mexican city. Soc Sci Med. (2015) 142:202–13. doi: 10.1016/j.socscimed.2015.08.010
52. Albala C, Vio F, Kain J, Uauy R. Nutrition transition in Chile: determinants and consequences. Public Health Nutr. (2001) 5:123–8. doi: 10.1079/PHN2001283
53. Baker P, Machado P, Santos T, Sievert K, Backholer K, Hadjikakou M, et al. Ultra-processed foods and the nutrition transition: global, regional and national trends, food systems transformations and political economy drivers. Obes Rev. (2020) 21:126. doi: 10.1111/obr.13126
54. Corvalán C, Reyes M, Garmendia ML, Uauy R. Structural responses to the obesity and non-communicable diseases epidemic: update on the Chilean law of food labelling and advertising. Obes Rev. (2019) 20:367–74. doi: 10.1111/obr.12802
55. Stoltze FM, Reyes M, Smith TL, Correa T, Corvalán C, Carpentier FRD. Prevalence of child-directed marketing on breakfast cereal packages before and after Chile's food marketing law: a pre- and post-quantitative content analysis. Int J Environ Res Public Health. (2019) 16:4501. doi: 10.3390/ijerph16224501
56. Dillman Carpentier FR, Correa T, Reyes M, Taillie LS. Evaluating the impact of Chile's marketing regulation of unhealthy foods and beverages: preschool and adolescent children's changes in exposure to food advertising on television. Public Health Nutr. (2020) 23:747. doi: 10.1017/S1368980019003355
57. Taillie LS, Bercholz M, Popkin B, Reyes M, Colchero MA, Corvalán C. Changes in food purchases after the Chilean policies on food labelling, marketing, and sales in schools: a before and after study. Lancet Planet Health. (2021) 5:e526–33. doi: 10.1016/S2542-5196(21)00172-8
58. Durán-Agüero S, Ortiz A, Pérez-Armijo P, Vinueza-Veloz MF, Ríos-Castillo I, Camacho-Lopez S, et al. Quality of the diet during the COVID-19 pandemic in 11 Latin-American countries. J Health Popul Nutr. (2022) 41:33. doi: 10.1186/s41043-022-00316-8
59. Correa T, Fierro C, Reyes M, Taillie LS, Carpentier FRD, Corvalán C. Why don't you [Government] help us make healthier foods more affordable instead of bombarding us with labels? Maternal knowledge, perceptions, and practices after full implementation of the chilean food labelling law. Int J Environ Res Public Health. (2022) 19:4547. doi: 10.3390/ijerph19084547
60. Drewnowski A. The cost of US foods as related to their nutritive value. Am J Clin Nutr. (2010) 92:1181–8. doi: 10.3945/ajcn.2010.29300
61. Jones NR v., Conklin AI, Suhrcke M, Monsivais P. The growing price gap between more and less healthy foods: analysis of a novel longitudinal UK dataset. PLoS ONE. (2014) 9:9343. doi: 10.1371/journal.pone.0109343
62. Cuadrado C, García J. Estudio sobre el cálculo de indicadores para el monitoreo del impacto socioeconómico de las enfermedades no transmisibles en Chile. Santiago: Ministerio de Salud/Organización Panamericana de la Salud/ Comisión Económica para América Latina y el Caribe (2015). doi: 10.13140/RG.2.2.20955.57120
64. Coulthard H, Sharps M, Cunliffe L, van den Tol A. Eating in the lockdown during the Covid 19 pandemic) self-reported changes in eating behavior, and associations with BMI, eating style, coping and health anxiety. Appetite. (2021) 161:82. doi: 10.1016/j.appet.2020.105082
65. Loth KA, Hersch D, Trofholz A, Harnack L, Norderud K. Impacts of COVID-19 on the home food environment and eating related behaviors of families with young children based on food security status. Appetite. (2023) 180:6345. doi: 10.1016/j.appet.2022.106345
66. Adams EL, Caccavale LJ, Smith D, Bean MK. Food insecurity, the home food environment, and parent feeding practices in the era of COVID-19. Obesity. (2020) 28:2056–63. doi: 10.1002/oby.22996
67. Kolodinsky JM, Goldstein AB. Time use and food pattern influences on obesity. Obesity. (2011) 19:2327. doi: 10.1038/oby.2011.130
68. Lavelle F, McGowan L, Spence M, Caraher M, Raats MM, Hollywood L, et al. Barriers and facilitators to cooking from “scratch” using basic or raw ingredients: a qualitative interview study. Appetite. (2016) 107:383–91. doi: 10.1016/j.appet.2016.08.115
69. Mills S, White M, Brown H, Wrieden W, Kwasnicka D, Halligan J, et al. Health and social determinants and outcomes of home cooking: a systematic review of observational studies. Appetite. (2017) 111:116–34. doi: 10.1016/j.appet.2016.12.022
70. Scott-Villiers P, Chisholm C, Wanjiku A, Hossain N. Precarious lives: food, work and care after the global food crisis. (2016) 3:20. doi: 10.21201/2016.620020
71. Neufeld LM, Andrade EB, Ballonoff Suleiman A, Barker M, Beal T, Blum LS, et al. Food choice in transition: adolescent autonomy, agency, and the food environment. Lancet. (2022) 399:185–97. doi: 10.1016/S0140-6736(21)01687-1
72. Neve K, Hawkes C, Brock J, Spires M, Squires CG, Sharpe R, et al. Understanding Lived Experience of Food Environments to Inform Policy : An Overview of Research Methods. London: Centre for Food Policy, City, University of London (2021).
73. Wolfson JA, Ishikawa Y, Hosokawa C, Janisch K, Massa J, Eisenberg DM. Gender differences in global estimates of cooking frequency prior to COVID-19. Appetite. (2021) 161:105117. doi: 10.1016/j.appet.2021.105117
74. Instituto Nacional de Estadísticas de Chile. Principales Resultados Encuesta Nacional de Uso del Tiempo 2015. Chile: INE (2016).
75. Clark S, McGrane A, Boyle N, Joksimovic N, Burke L, Rock N, et al. “You're a teacher you're a mother, you're a worker”: Gender inequality during COVID-19 in Ireland. Gend Work Organ. (2021) 28:1352–62. doi: 10.1111/gwao.12611
76. Craig L, Churchill B. Working and caring at home: gender differences in the effects of COVID-19 on paid and unpaid labor in Australia. Femin Econ. (2020) 27:310–26. doi: 10.1080/13545701.2020.1831039
77. Constantinides SV, Turner C, Frongillo EA, Bhandari S, Reyes LI, Blake CE. Using a global food environment framework to understand relationships with food choice in diverse low- and middle-income countries. Glob Food Sec. (2021) 29:100511. doi: 10.1016/j.gfs.2021.100511
78. Downs SM, Ahmed S, Fanzo J, Herforth A. Food environment typology: Advancing an expanded definition, framework, and methodological approach for improved characterization of wild, cultivated, and built food environments toward sustainable diets. Foods. (2020) 3:532. doi: 10.3390/foods9040532
79. Mehta K, Booth S, Coveney J, Strazdins L. Feeding the Australian family: challenges for mothers, nutrition and equity. Health Promot Int. (2020) 35:771–8. doi: 10.1093/heapro/daz061
80. Gozzi N, Tizzoni M, Chinazzi M, Ferres L, Vespignani A, Perra N. Estimating the effect of social inequalities in the mitigation of COVID-19 across communities in Santiago de Chile. medRxiv. (2020) 4:1–9. doi: 10.1101/2020.10.08.20204750
Keywords: food environments, domestic food environment, food access, dietary quality, children, Chile
Citation: Pemjean I, Mediano F, Ferrer P, Garmendia ML and Corvalán C (2023) Food access, domestic environments, and dietary quality of low-middle income Chilean children during the COVID-19 pandemic. Front. Public Health 11:1164357. doi: 10.3389/fpubh.2023.1164357
Received: 12 February 2023; Accepted: 25 May 2023;
Published: 20 June 2023.
Edited by:
Juliana Souza Oliveira, Federal University of Pernambuco, BrazilReviewed by:
Chiza Kumwenda, University of Zambia, ZambiaLarissa Loures Mendes, Federal University of Minas Gerais, Brazil
Copyright © 2023 Pemjean, Mediano, Ferrer, Garmendia and Corvalán. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Camila Corvalán, Y2NvcnZhbGFuQGludGEudWNoaWxlLmNs
†Present address: Fernanda Mediano, Department of Psychology, Pontificia Universidad Católica de Chile, Santiago, Chile