 Carlos Roman1
Carlos Roman1 Diego Andrade2*Yenima Hernández3Zoila K. Salazar2,4Lizette Espinosa2Erika Campoverde2Lourdes Guallaizaca2
Diego Andrade2*Yenima Hernández3Zoila K. Salazar2,4Lizette Espinosa2Erika Campoverde2Lourdes Guallaizaca2 María Merchán2Miriam Sarmiento5Jonathan Brenner1
María Merchán2Miriam Sarmiento5Jonathan Brenner1- 1Diagnostic Department, MEDsan, Inc., Saint Petersburg, FL, United States
- 2Investigation Center for Health, Academic Unit of Health and Wellness, Catholic University of Cuenca (UCACUE), Cuenca, Ecuador
- 3Department of Mental Health, The Angels Mental Health Community, Tampa, FL, United States
- 4Medical Center Association for the Well-being of the Ecuadorian Family (APROFE), Cuenca, Ecuador
- 5Obstetrics Department, San Juan de Dios Hospital, Cuenca, Ecuador
Objectives: The study aims to identify the correlation between human papillomavirus (HPV) infection and sociodemographic and sexual reproductive health factors in Ecuadorian women from March to August 2019.
Methods: 120 women were randomly selected from two gynecological clinics to complete a questionnaire and provide a biospecimen. PCR-Hybridization was used to genotype 37 HPV serotypes in samples obtained by endo-cervical brushing for liquid-based cytology. Sociodemographic and sexual health data were collected through a validated questionnaire during a medical consultation. Mathematical modeling of HPV infection was done using bivariate logistic regression.
Results: 65.0% of the women sampled had an HPV infection; 74.3% of these women had co-infections with other HPV genotypes. Out of the women who were HPV positive, 75.6% were diagnosed with high-risk genotypes from HPV strains 18, 35, 52, and 66. Parity, immunosuppression, and use of oral contraception/intrauterine devices (IUDs) were identified as associated variables. The explanatory model had a sensitivity of 89.5% and a specificity of 73.8%.
Conclusion: The predominant strains of HPV among Ecuadorian women are diverse. The risk of HPV infection is a complex phenomenon where biological and psychosocial variables are integrated into a model. In populations with limited access to health services, low socioeconomic status, and negative sociocultural beliefs about sexually transmitted infections (STIs), surveys can be used as a pre-screening step for HPV infections. The diagnostic value of the model should be tested in multicenter studies that include women from all over the country.
1. Introduction
Human papillomavirus, the most common STI worldwide (1), is associated with genital, anal and oral cancers in men and women (2, 3). With over 200 HPV subtypes, at least 15 are considered to have a high oncogenic risk (4). Specifically, high-risk HPVs (hrHPV) are responsible for 70–90% of anogenital cancers in women (5). While HPV vaccination has greatly reduced the incidence rate and risk of mortality, the global burden of uterine cervical cancer (UCC) still exists; just shifted to countries with poor access to preventative measures. This creates a unique epidemiological pattern, where regions like Latin America are disproportionately affected. Currently, HPV is the leading cause of cervical cancer in the region with an incidence of infection twice as high as the global average (6).
There are a variety of risk factors associated with recurring HPV infections. Among these, early intercourse, number of sexual partners, and infrequent condom use are the most prevalent (7). Differences in prevalence due to sociodemographic factors including age, marital status, income level and race have also been documented (8). Additionally, health behaviors including poor diet, smoking (9), drug addiction, and inadequate hygiene contribute to the progression of HPV (10). Lack of information about HPV, inadequate access to testing, vaccination, and treatment have also been identified (11, 12).
Chronic infection of HPV strains 16 and 18 have been implicated in the majority of cervical cancer cases; a statistic that led to the creation of the HPV vaccinations, such as Gardasil and Cervarix (13). In Ecuador, while these vaccinations have substantially decreased HPV strains 16/18, the diversity of alternate high risk HPV strains has increased (14).
To reduce this incidence rate and premature mortality, this research aims to associate HPV infection in Ecuadorian women from Cuenca with sociodemographic, sexual-reproductive health and biological variables. Using this data, we aim to create a mathematical model that will aid in HPV pre-screening, contributing to Ecuador’s goal to reduce 25% of mortality from cancer by 2025 (15).
2. Materials and methods
2.1. Study design
This study includes a quantitative cross-sectional evaluation of women who attended two gynecology clinics in the city of Cuenca, Ecuador from March 2019 to August 2019.
The potential sample size was calculated using the sample size estimation formula for proportions in known populations plus 10% of estimated losses. The participating population size was estimated according to the volume of work activity of previous months in the gynecology service in that period. The rate of known HPV infection in the region was retrieved from previous studies.
The formula used is as follows:
Using random sampling, the patients were assigned sequential numbers upon arrival at the healthcare facility during the research period. Upon initial consultation, the medical professional assessed whether the participant met the following inclusion/exclusion criteria:
Inclusion criteria: current treatment at the respective healthcare facility; sexually active life; age between 18–65 years old; female.
Exclusion criteria: pregnancy; previous diagnosis of HPV infection or cervical cancer; treatment with immunosuppressive drugs.
The final sample in the study was 120 women.
2.2. Information collection
A patient questionnaire was used for the collection of sociodemographic and sexual-reproductive health data and was applied with reliability (Cronbach’s alpha = 0.79) and acceptable content validity (Aiken’s V of 0.82) (16). The questionnaire addressed age, place of residence, education level, personal income, alcohol and tobacco history, marital status, age of first coital intercourse, number of sexual partners, frequency of intercourse per month, access to gynecologic care, contraceptive use of condoms, IUDs or contraceptive pills, parity, history of STIs, and level of HPV awareness. Immunity was evaluated using 10 questions corresponding to symptoms of immunosuppression (tiredness/decay, allergies, eczema, skin abrasions, wounds that are slow to heal, loss of appetite, muscle pain, chills, headache, fever, respiratory infections, gastrointestinal infections, and sleepiness) (17) with a cutoff value over 5 points to be considered. The questionnaire was administered by a trained facilitator during medical consultation. The average response time was 14 min.
2.3. Biospecimen collection
The collection of biospecimens was carried out according to the protocols issued by the Ministry of Public Health (MSP) of Ecuador (15). Endocervical brushing was performed using SurePath® Liquid Based Cytology sampling kits according to manufacturer instructions [BD (18)]. The biological sample was taken by the gynecologist’s physician. The patient was in the supine ulnar position on the gynecological care table. The neck of the uterus was accessed with the help of a speculum and secretions were removed by swab. An endocervical brush was inserted, gently pressed against the wall of the cervix, rotated 5 times clockwise, and removed from the endocervical canal. The brush was then placed into a SurePath vial and refrigerated at 4-6°C until DNA extraction.
2.4. HPV detection
From the liquid-based sample, an aliquot was made in a laminar flow hood for the identification of HPV, by broad spectrum genotyping, using the 37 HPV GenoArray Diagnostic Kit (Hybribio® Diagnostics Ltd., Sheung Wan, Hong Kong). The kit detected the presence of 37 different HPV genotypes: 15 high (16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68), 6 low (6, 11, 42, 43, 44, 81 (CP8304)) and 16 undetermined risk (26, 34, 40, 54, 55, 57, 61, 67, 69, 70, 71, 72, 73, 82, 83, 84). HPV DNA was extracted from cervical cells using an alkaline lysis method. Samples were centrifuged for 10 min at 14000 rpm at 20°C, resuspended in 100 μL elution buffer, and stored at −20°C until PCR. The concentration and purity of DNA (OD260/OD280 1.6–1.8) was determined by Nanodrop 2000 (Thermo Fisher Scientific, CA, United States). This was followed by amplification, according to manufacturer recommendations, through conventional PCR and utilization of biotinylated PGMY primers (Thermocycler Applied Biosystems® /GeneAmp® 9,700). The PCR mix was prepared according to the manufacturer’s instructions to obtain a final reaction volume of 25 μL (23.25 μL PCR Mix, 0.75 μL of DNA Taq polymerase 5 U/μL and 1 μL of DNA). Amplification was performed with an initial denaturation at 95°C for 5 min (min), followed by 40 cycles of denaturation at 95°C for 20 s (s), annealing at 55°C for 30 s, and elongation at 72°C for 30 s, then a final elongation at 72°C for 5 min.
After amplification, the genetic material was denatured and subjected to membrane hybridization for 20 min using specific probes. All assays included a positive and a negative PCR control in addition to the hybridization control itself. The hybridization process was carried out using the HibriMax (Hybribio) kit according to the manufacturer instructions. This was conducted by washing, addition of streptavidin–horseradish peroxidase conjugate, membrane blocking, and addition of developer substrate (nitroblue tetrazolium-5-bromo-4-chloro3-indolyl phosphate). The membranes contained the immobilized probes of the genotypes of interest that hybridize with biotinylated amplified PCR products. Streptavidin–horseradish peroxidase conjugate was added to bind to the biotinylated PCR products. The direct visualization of the breakdown product (purple precipitate) from the addition of substrate nitroblue tetrazolium-5-bromo-4-chloro3-indolyl phosphate, was interpreted as positive for the corresponding HPV DNA type as indicated in the schematic diagram (Figure 1).
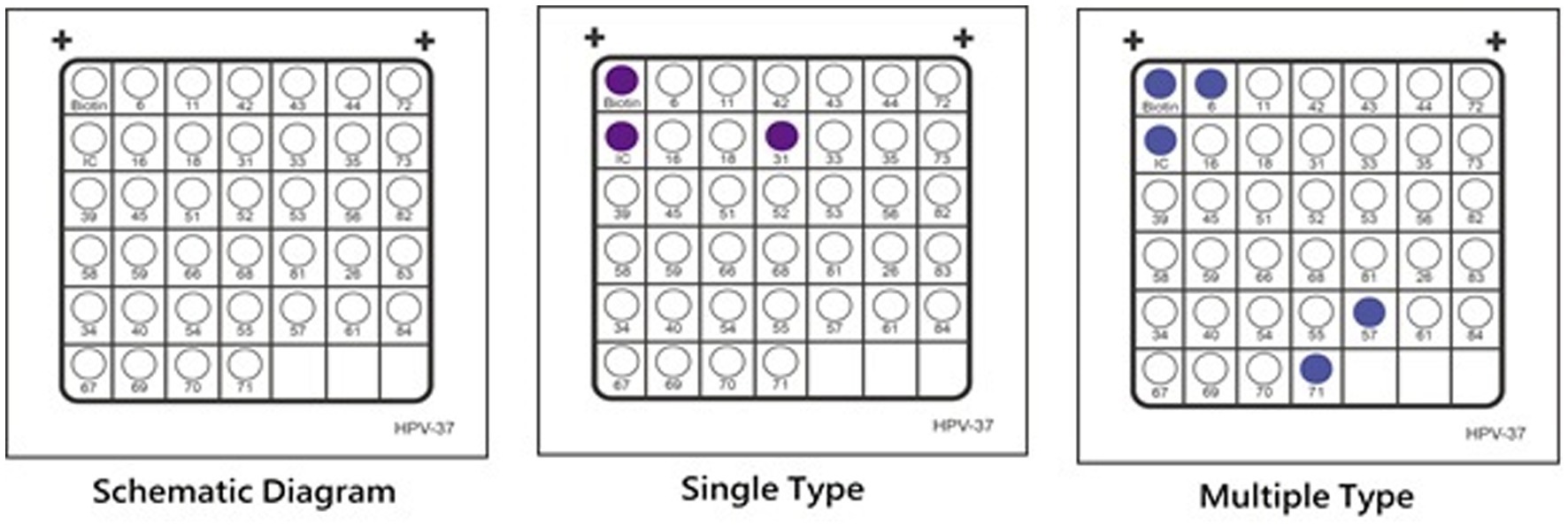
Figure 1. Schematic Diagram for HPV Genotyping Results: Retrieved from Hybridbio manufacturing information.
2.5. Statistical processing
Data was stored in an electronic database and processed using IBM SPSS 23.0 statistical software. Analysis of frequency and measures of central tendency position (mean, confidence intervals, percentiles) and dispersion (standard deviation, range) were used. Differences between groups were established using the Mann–Whitney or Kruskall-Wallis U test for determining whether sets are from the same distribution. Differences in proportions and bivariate association were estimated using cross tables (Z test for comparison of proportions by columns, X2 test, Cramer’s V). The risk estimation used odds ratio (OR) with confidence intervals from bivariate analysis and confirmed by binary logistic regression using the progressive Wald method. The significance level of all tests was less than or equal to 0.05. The equation that describes HPV infection probability derives from a mathematical model of binomial logistic regression.
2.6. Ethical aspects
The research protocol ensured informed consent and good practice established in the Declaration of Helsinki. Prior consent from all subjects involved was obtained by signature after the research objectives were presented orally and in writing. The anonymity and the will of the respondents and interviewees regarding the disclosure of information was respected. The research was reviewed and approved by the Catholic University of Cuenca Human Research Ethics Committee with resolution number CEISH 2018–09-017 R.
3. Results
3.1. Sociodemographic characterization
Sociodemographic results of the survey are shown in Table 1.
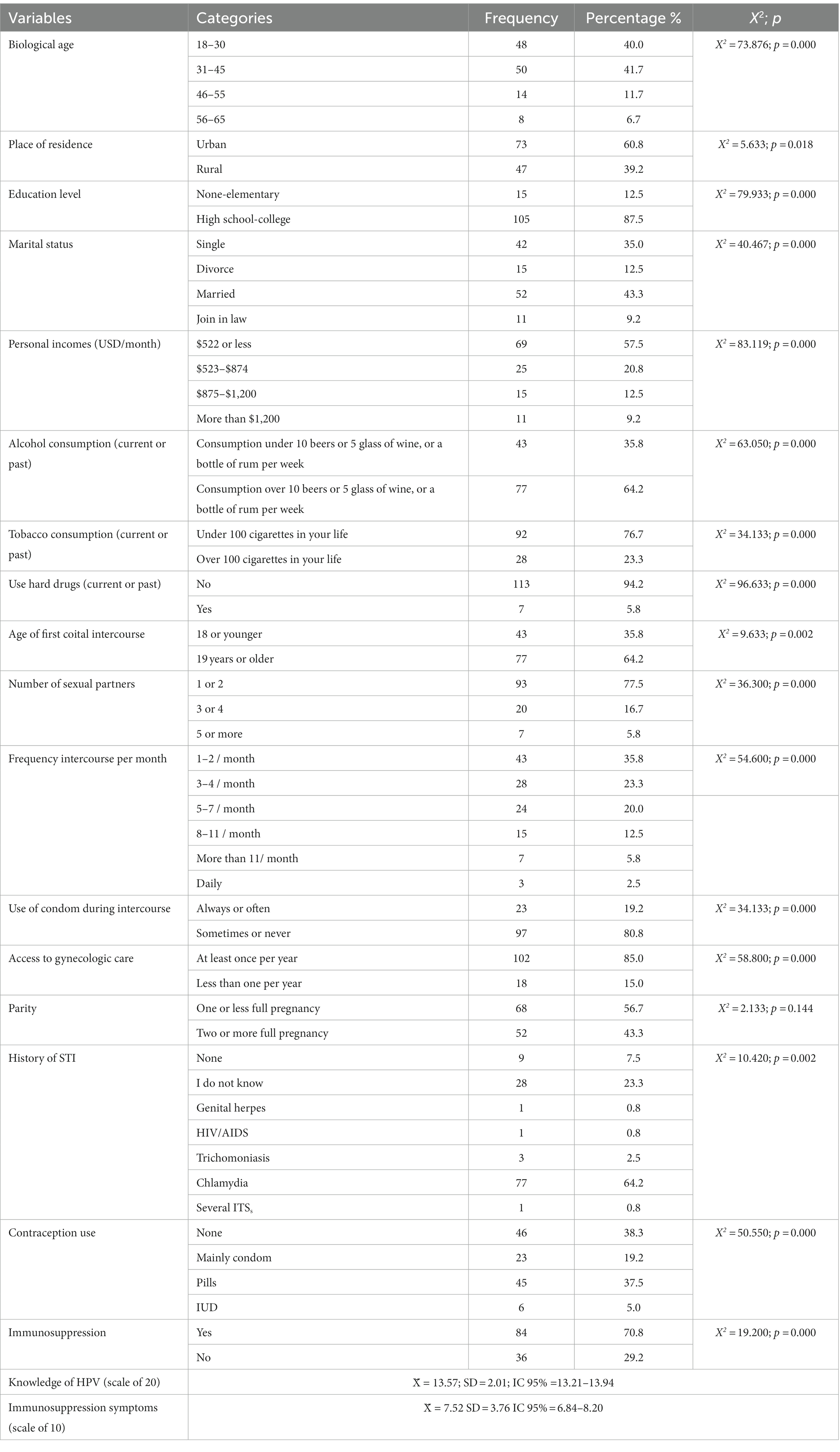
Table 1. Sociodemographic variables of women in Cuenca-Ecuador, 2019 N = 120.
The average age of participants was 35.6 years old (+/− 10.9). Most patients were between 31–45 years (41.7%), and 18–30 years (40.0% of patients) followed by ages 46–55 (11.7%) and 56–65 (6.6%) (X2 = 73.876; p = 0.000). The place of residence was predominantly urban (60.8%) over rural areas (39.2%) (X2 = 5.633; p = 0.018). Must participants had a secondary or university level of education (87.5%; X2 = 79.933; p = 0.000). Additional demographics revealed that 78.3% of the sample had incomes below $875 USD (X2 = 83.119; p = 0.000) 64.2% consumed alcohol regularly (X2 = 63.050; p = 0.000), 23.3% of participants had a current or past consumption of tobacco (X2 = 34.133; p = 0.000), and only 5.8% of participants have consumed hard drugs (X2 = 93.633; p = 0.000).
Most participants (52.5%) had a partner (43.3% married, 9.2% common law). The remaining 47.5% were either single (35.0%) or divorced (12.50%) (X2 = 40.467; p = 0.000). For a majority of the sample, the first instance of coitarche occurred at age 19 years or older (64.2%) (X2 = 9.633; p = 0.002). The number of sexual partners per month varied throughout the participants with 77.5% indicating they have had 1–2 sexual partners, 16.7% between 3–4 partners, and 5.8% 5 or more partners (X2 = 36.300; p = 0.000). 59.1% of sample patients reported a frequency of 1–4 sexual relations per month (X2 = 54.600; p = 0.000).
Frequency of condom use in sexual intercourse was in low proportion (19.2%) compared to women that never or sometimes use condoms in coital (80.8%) (X2 = 34.133; p = 0.000). 42.5% of the participants were currently using oral contraceptives or intrauterine devices and 38.3% did not use any contraceptive method (X2 = 50.550; p = 0.000). The majority of women had given birth to one or no children (56.7%) and 43.3% were multiparous (X2 = 2.133; p = 0.144). 69.2% of participants reported having a history of STIs (besides HPV) as opposed to 7.5% never having contracted an STI. It should be noted that 23.3% were unaware of their STI history (X2 = 10.420; p = 0.002).
The access to gynecological health care had high occurrence with 85.0% of the sample population having at least one appointment per year, and the remaining participants (15.0%) having less than one appointment per year (X2 = 58.800; p = 0.000). Clinical immunosuppression was found in 70.8% of the women (X2 = 19.200; p = 0.000).
The sample population had an average level of knowledge on HPV of 13.6 +/− 2.0 (95% CI 13.2–13.9) on a scale of 20. There were significant differences in knowledge according to the level of education (U = 425.5; p = 0.004). Background knowledge on HPV was higher for the group with high school-college education compared to elementary-no education. No differences in knowledge were found due to age (U = 1442.0; p = 0.150) or marital status (U = 1450.0; p = 0.122).
The frequency of infection according to HPV strain is shown in Figure 2A. Of the total sample population, 65.0% were identified as HPV positive with 49.1% of the population identified to be infected with high-risk HPV. For the group of patients with HPV, 75.6% of infections corresponded to a high-risk genotype and 74.3% of the patients were identified to have coinfections with multiple HPV strains (48.3% of total sample population). Some coinfected women presented up to 8 different genotypes.
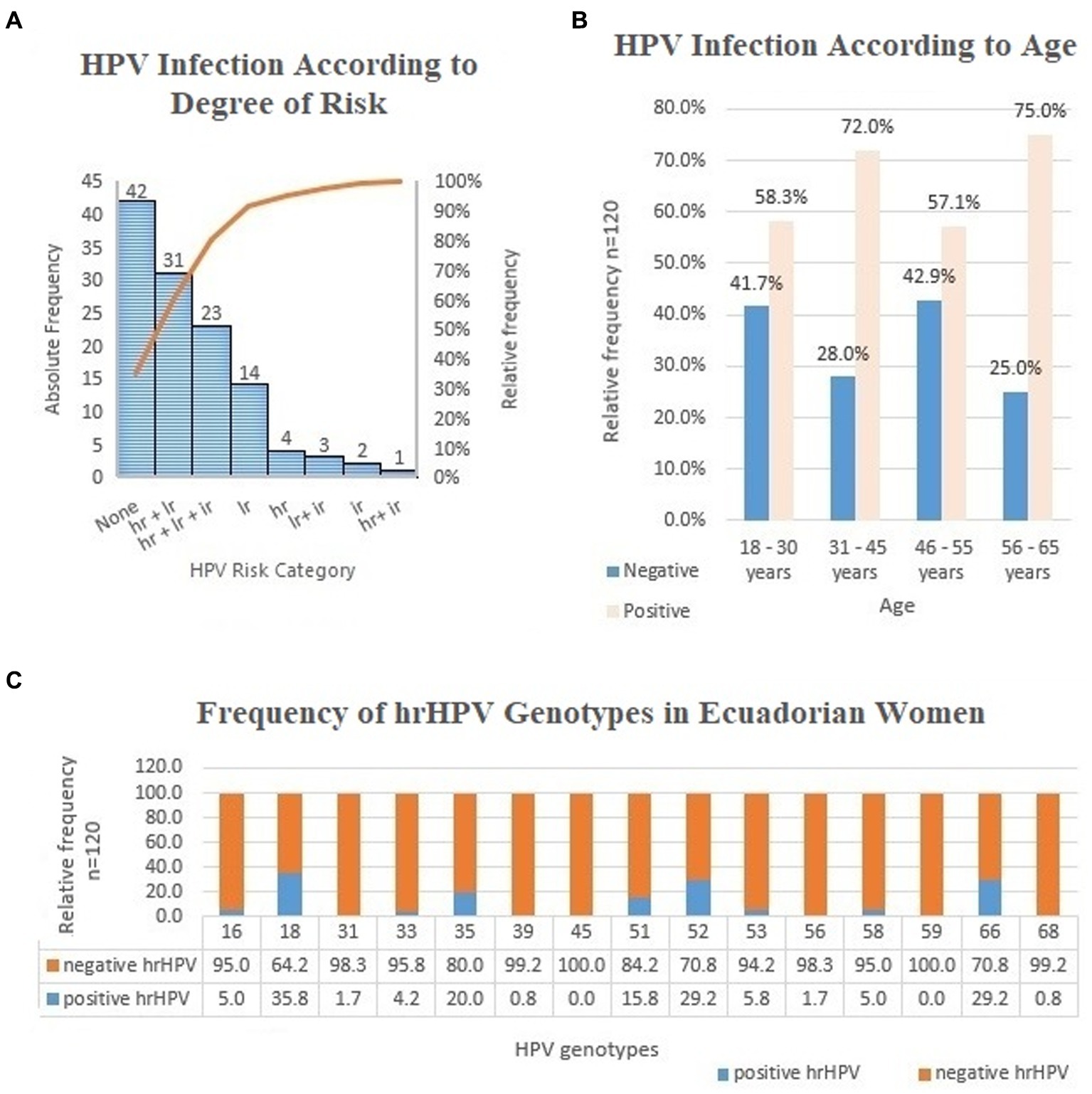
Figure 2. (A) Frequency analysis of HPV infection in women according to degree of risk, Cuenca, Ecuador; 2019. n=120 lr (low risk)-HPV 6, 11, 42, 43, 44, 81 (CP8304). ir (undetermined risk)-HPV 26, 34, 40, 54, 55, 57, 61, 67, 69, 70, 71, 72, 73, 82, 83, 84. hr (high risk)-HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68. (B) Frequency analysis of HPV infection in women according to age; Cuenca, Ecuador; 2019. n=120. (C) Frequency analysis of hr HPV genotypes in women; Cuenca, Ecuador; 2019. n=120.
Even though the groups of women aged 56–65 and 31–45 years old had a higher proportion of HPV infections (Figure 2B), the Z test comparison for proportion was unable to establish significant differences between age groups (p > 0.050). There was no association between age groups and HPV infection (X2 = 2.746; p = 0.432).
The frequency distribution of the hrHPV strains is shown in Figure 2C. The most frequent genotype was hrHPV 18, followed by genotypes 52, 66, 35, and 51 (X2 = 7.234; p = 0.041). HPV 16 had a low frequency of infection in the group studied.
3.2. Modeling of HPV infection
The correlation analysis showed a moderate association between HPV infection and certain biological, sociodemographic, sexual and reproductive health variables. Table 2 shows the statistics for each of these associations.
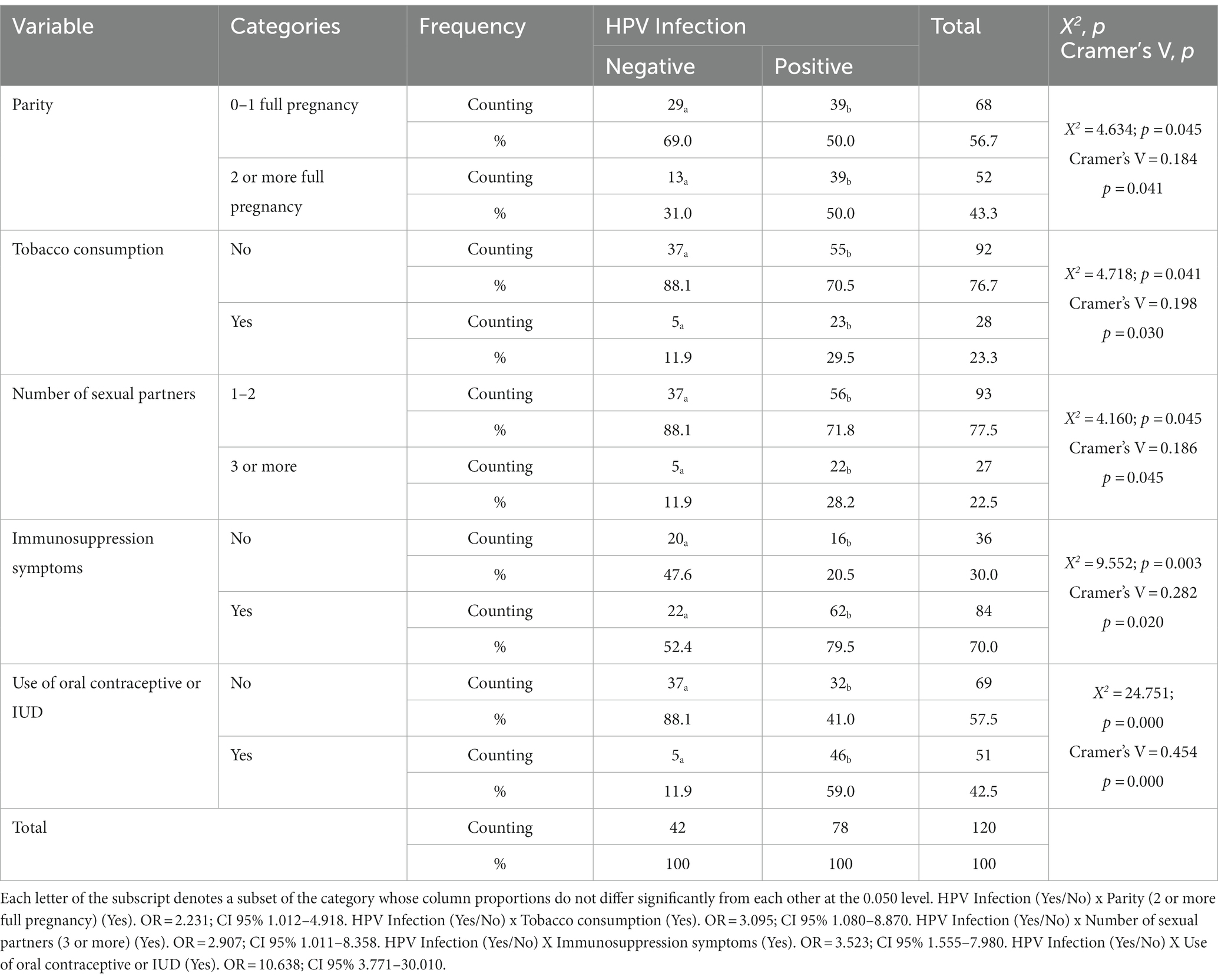
Table 2. HPV infection according to Parity, Tobacco consumption, Number of sexual partners, Contraception and Immunosuppression symptoms in women from Cuenca Ecuador, 2019.
While overall no association was found between HPV infection and condom use, when accounting for marital status, participants who were single or in common law unions, condom use was associated with lower infectivity (Fisher’s X2 = 5.852; p = 0.026; V Cramer = − 0.293; p = 0.016). For married women, this association was not found (X2 = 1.231; p = 0.412).
The remaining variables included: the age at which the participant became sexually active (X2 = 3,234; p = 0.357), knowledge about HPV (X2 = 0.261; p = 0.610), gynecological medical care (X2 = 0.141; p = 0.708), place of residence (X2 = 0.369; p = 0.562), education level (X2 = 0.188; p = 0.664), alcohol consumption (X2 = 0.669; p = 0.413), age groups (X2 = 2.033; p = 0.362), previous STIs (X2 = 1.553; p = 0.276), frequency of sexual intercourse (X2 = 0.701; p = 0.441), and marital status (X2 = 1.528; p = 0.250). These were not associated with HPV infection in the sample studied.
Binary logistic regression confirmed an association between parity, immunosuppression symptoms, use of oral contraceptives/IUDs, and positive HPV infection. The rest of the variables were excluded due to their low statistical significance (p > 0.050) or low predictive power with a non-significant OR. No confounding or interaction variables were found. The characteristics of the model obtained by binary logistic regression are shown in Table 3.

Table 3. Explanatory model of HPV infection through health and sociodemographic variables.
The model has significant values of Hosmer Lemeshow test (X2 = 6.698; fg = 4; p = 0.845), diagnostic power of 81.7%, a high sensitivity of 89.5% and an acceptable specificity of 73.8%. This model makes it possible to explain up to 42.9% of the variance of the infection with HPV according to the Nagelkerke coefficient of Determination (R2 = 0.429). Even though the model is not comprehensively adequate, select variables have been viewed as possible explanations for HPV infection. This model attempts to rule out tobacco use and number of sexual partners as significant explanations of infection according to their respective OR values.
The equation that describes HPV infection probability is as follows:
4. Discussion
The World Health Organization (WHO) reports more than 1 million new sexually transmitted infections each day (5). The frequency of infection among women is found to be higher in Latin America (16%) than more developed areas, such as North America (4.7%) (2). The most prevalent viral types contributing to cervical cancer burden in Latin America are HPV 16, 18, 31, 58, 33, 45, and 52 in decreasing frequency.
In Ecuador, there is no epidemiological study about HPV infection within the country in its entirety. For instance, ENSANUT’s 2019 report (National Survey for Health and Nutrition) does not contain information about HPV infection. Neither exists a national program to test HPV infection, even when deaths for UCC increased to 902 women in the country in 2019 (19).
A 2016 study found that in a cohort of 164 Ecuadorian women, 86% tested positive for HPV. Out of those who were tested positive, the most common strains found were HPV 16 at 42% and HPV 58 at 31%. HPV18 was only detected in 3% of the samples (20). Comparatively in Ecuador, prevalence by strain contributing to invasive cervical cancer ranks HPV 16, 58, 52, 31, 59, 39 in decreasing frequency (21). Another study carried out in Cañar, a region of the Ecuadorian highlands, confirms a shift in infection patterns towards hrHPV 31, 58, 59, and 66 in around 20% of the infected women (22). A study conducted in the city of Guayaquil between 2015–2018 in 800 participants from the Ecuadorian coast found a high percentage of infection by non 16–18 HPV strains in men and women (51.38%) (23). The same change of HPV patron infection is shown in Cuenca where the most prevalent HPV strains were 58, 51, 31, 52 and 53 (24).
A systematic review published in 2021 identified the main results of the HPV investigations in the country in the last 7 years (25, 26). These articles have a few differences with the present investigation: an increase in hrHPV 18 and hrHPV31 infections, and a low level of hrHPV-16. Other systematic reviews also show heterogeneity in the circulating strains according to the country’s region. In the 2021 report from the HPV Information Center, HPV strains 16 (38%), 58 (28%), 52 (12%), and 31 (10%) were found to be the most frequent strains in Ecuadorian women with invasive cervical cancer by histology. Notably, HPV18 was not listed in the top ten most frequent strains (21). These findings highlight high rates of infection in the Ecuadorian highlands region. Results were heterogeneous in populations, sampling, and HPV identification techniques. Differences in current studies hinder a thorough comparison needed to achieve agreement and generalizability for HPV trends in Ecuador.
The presence of different strains infecting women according to the geographic region in Ecuador may be related to population characteristics (biological, cultural, and social) which suggest differences in susceptibility to HPV infection. Biological characteristics of the host, such as immune status, trophic predisposition to the virus, and favorable vaginal biome could promote a greater viral infection.
Although infection with HPV is a high-frequency phenomenon, viral clearance occurs in 80–90% of infected women (27). One of the main factors in blocking or eliminating infection is the functioning of the host’s immune system. Immunological status of the patient is relevant in the infection and persistence of HPV (28). Investigations have found a protective humoral response against the L1 and L2 proteins present in the viral capsid and the presence of non-neutralizing antibodies against the early phase proteins E6 and E7 (29). Other factors related to the persistence of the infection are the APOBEC3A proteins, which act as antiviral protection mechanisms through epigenetic mechanisms (30). It suggests that innate defense could be a relevant mechanism to destroy virus infection of mucosal (31). Vaccination against HPV has also been able to generate protection against infection in numerous populations (32), confirming the role of the immune system in preventing or eliminating HPV infection (28). Currently, there are no scientific reports that establish the efficacy and type of immune response after HPV vaccination in Ecuador.
The substantial differences in the circulating genotypes in the south highlands of Ecuador and a possible change in the patterns of infection with HPV suggest a specific approach in diagnostic research, prevention, and treatment (33, 34). Non-cytology-based approaches to diagnosis could have high efficacy in low-resource settings and can decrease the prevalence of pre-cervical cancer lesions (35). A national program for HPV infection diagnosis could unify the diverse diagnostic methods used in clinical laboratories of the country, and generate more reliable data for decision-making in HPV strategy.
The age distribution of HPV infection did not show a classical “U” shape view like in several Latin-American countries (Brazil, Costa Rica, México, and Chile) (36). In these countries, HPV infection was more widespread in older women. Conversely, our study found that young women less than 30 years old had a similar proportion of HPV infection to the group of 31–45 years old. This fact suggests different patterns of population infection, differential effectiveness of vaccination campaigns realized in 2014 (38), or a possible bias due to the small sample for investigation.
The role of risky sexual behavior as a determinant of STIs has been validated by numerous investigations (37–41). Unlike reports in the literature (42), our study shows that the age of first coitarche and the number of sexual partners is not associated with STIs.
There is also a lack of overall correlation between condom use and HPV infection. This finding may be related to the inconsistent use of condoms in married women who are infected by marital and extramarital sex, which is identified by Calatrava et al. in other populations of women infected with STIs (37).
Although tobacco use potentiates the appearance of cervical cancer in women infected with hrHPV (11), the effect on HPV infection is not well understood. Epidemiological research made by Utami et al. fails to prove the statistical association between HPV infection and tobacco use in cross-sectional research (43). HPV could be a synergic or potentiating factor for HPV infection. Subsequent investigations could shed light on the effect of tobacco use and HPV infection by controlling the level and frequency of tobacco consumption in a prospective cohort’s design.
Hormonal contraception and HPV infection have been found to induce the progression of UCC (44). Estrogens that can be found within these contraceptives are associated with the development of UCC in conjunction with hrHPV. However, other studies have found no significant association between hormonal contraception and cervical cancer when controlling for HPV infection (45) or are inconclusive about HPV infection risk (46).
Previous research has corroborated an association between the use of estrogenic oral contraceptives and hrHPV infection. The influence of female hormones on HPV infection is not well understood, but the effect has recently been suggested. Estrogens induce the expression of the polysaccharide layer present in the basement membrane of the cervical epithelium of animal models (47, 48). Researchers describe that the mechanism of entry of HPV into cells occurs through the binding of the viral L1 protein (49) to proteoglycans (heparan sulfate) (50) present in the basement membrane of the epithelium of animal models. Estrogen receptor knockout mice have shown protection against viral infection of the reproductive system (51). Recent research has also found an association between estrogenic oral contraceptives and hrHPV infectivity (52). Hormonal estrogen contraception could enhance the entrance of HPV through the high level of heparan sulfate in the epithelial cell surface (53).
Although previous epidemiological studies documented parity as a risk factor for cervical cancer, the reported strength of association is variable and inconsistent. Several investigations revealed a connection between parity, HPV infection, and CCU (54). These studies suggest that a high rate of cervical abnormalities during pregnancy is conducive to cervical lesions and make epithelial cells more susceptible to HPV infection. The main problem is determining the parity cut-off due to differing values between studies.
4.1. Study limitations
Interpretations of the discussed findings should consider the tested demographic in relation to sampling method and sociocultural characteristics. The extrapolation of results must be assessed carefully in different contexts. While utilizing the random selection method, there was potential for bias in sampling. Participants who came for healthcare services at the facility expressed interest in research participation, and this may introduce potential bias with its convenience.
Sample size and cultural diversity of participants was considered a limitation of this study. We acknowledge that the results represent a small-scale sample of the sexually active female population of the Ecuadorian highlands. Further studies should be carried out to increase external validity. We suggest continuing with different multicentric studies to substantiate diagnostic value within a large and diverse group of women in regions of Ecuador.
The survey method can also be considered a limitation based on the participant’s ability to answer accurately. To achieve reliable data, a comfortable environment must be established to maintain confidence in doctor-patient disclosure. Although a relationship was found between HPV and immunosuppression symptoms, it is inaccurate to draw a correlation based on our study due to the reliability of the survey method and absence of molecular testing. These clinical implications could also be confounded by participants, resulting in a source of perception bias. We suggest that our method should be validated further through pilot testing in populations under study.
5. Conclusion
The predominant strains of HPV among Ecuadorian women are diverse. The risk of HPV infection is a complex phenomenon where biological and psychosocial variables are integrated into a model. HPV pre-screening in populations with limited access to health services, low socioeconomic status, and negative sociocultural beliefs about STIs could use surveys as a step before screening for HPV infections. The diagnostic value of the model should be tested further in multicenter studies all over Ecuador.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://ucacueedu-my.sharepoint.com/:f:/g/personal/jbaculima_ucacue_edu_ec/ElO4GinuTYpIqSv39NWCDI8B4d_LBdfiiruxKz4W2mU1pw?e=5KZNNhAccesionkey:Investigacion.BF.
Ethics statement
The studies involving human participants were reviewed and approved by Human Research Ethics Committee UCACUE. The patients/participants provided their written informed consent to participate in this study.
Author contributions
CR: research design, survey design and validation, biospecimen processing, and data processing and statistical analysis. YH: research design, survey design and validation, and data processing and statistical analysis. DA: research design and data processing and statistical analysis. ZS and LM: data processing and statistical analysis, biospecimen collection, and sociodemographic data collection. EC, LG, and MM: survey design and validation, biospecimen processing, and sociodemographic data collection. MS: biospecimen collection and sociodemographic data collection. JB: data processing and statistical analysis. All authors contributed to the article and approved the submitted version.
Funding
Funding was received from UCACUE (Grant UCACUE-DIPVP-2018-165-OF).
Acknowledgments
The authors would like to thank UCACUE for institutional support for data collection and the respective authorizations for the research. To Katherine Stadler and Robert Lewis for chart designs and language edition of the article.
Conflict of interest
CR and JB were employed by Diagnostic Department, MEDsan, Inc., Saint Petersburg, FL, United States.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. OMS, (2021). Infecciones de transmisión sexual. Available at: https://www.who.int/es/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis) (accessed June 15, 2021).
2. Chan, CK, Aimagambetova, G, Ukybassova, T, Kongrtay, K, and Azizan, A. Human papillomavirus infection and cervical Cancer: epidemiology, screening, and vaccination—review of current perspectives. J Oncol. (2019, 2019) 2019:3257939–11. doi: 10.1155/2019/3257939
3. Mena, M, Taberna, M, Monfil, L, Arbyn, M, de Sanjosé, S, Bosch, FX, et al. Might Oral human papillomavirus (HPV) infection in healthy individuals explain differences in HPV-attributable fractions in oropharyngeal Cancer? A systematic review and Meta-analysis. J Infect Dis. (2019) 219:1574–85. doi: 10.1093/infdis/jiy715
4. Gargano, J., Meites, E., Watson, M., Unger, E., and Markowitz, L., (2021). HPV-vaccine preventable diseases surveillance manual|CDC. Available at: https://www.cdc.gov/vaccines/pubs/surv-manual/chpt05-hpv.html
5. World Health Organization, (2020). Papilomavirus humanos (PVH) y cáncer cervicouterino. Available at: https://www.who.int/es/news-room/fact-sheets/detail/human-papillomavirus-(hpv)-and-cervical-cancer (Accessed March 8, 2021).
6. Nogueira-Rodrigues, A. HPV vaccination in Latin America: global challenges and feasible solutions. Am Soc Clin Oncol Educ Book. (2019) 39:e45–52. doi: 10.1200/EDBK_249695
7. Monteiro, JC, Souza, R, Sousa, C, Silva, L, da Silva, A, Gomes, S, et al. Prevalence of high risk HPV in HIV-infected women from Belém, Pará, Amazon region of Brazil: a cross-sectional study. Front Public Health. (2021) 9:649152. doi: 10.3389/fpubh.2021.649152
8. Osazuwa, N, Boakye, E, Rohde, R, Ganesh, R, Moiyadi, A, Hussaini, A, et al. Understanding of risk factors for the human papillomavirus (HPV) infection based on gender and race. Sci Rep. (2019) 9:297. doi: 10.1038/s41598-018-36638-z
9. Yang, J, Wang, W, Wang, Z, Wang, Z, Wang, Y, Wang, J, et al. Prevalence, genotype distribution and risk factors of cervical HPV infection in Yangqu, China: a population-based survey of 10086 women. Hum Vaccin Immunother. (2020) 16:1645–52. doi: 10.1080/21645515.2019.1689743
10. Li, M, Yang, Q-F, Cao, Q, Tang, J, Gao, Y, Zhi, M, et al. High-risk human papillomavirus infection and cervical neoplasm in female inflammatory bowel disease patients: a cross-sectional study. Gastroenterol Rep. (2019) 7:338–44. doi: 10.1093/gastro/goy053
11. Baskaran, K, Kumar, PK, Santha, K, and Sivakamasundari, I. Cofactors and their association with Cancer of the uterine cervix in women infected with high-risk human papillomavirus in South India. Asian Pac J Cancer Prev. (2019) 20:3415–9. doi: 10.31557/APJCP.2019.20.11.3415
12. Riaz, L, Manazir, S, Jawed, F, Arshad Ali, S, and Riaz, R. Knowledge, perception, and prevention practices related to human papillomavirus-based cervical Cancer and its socioeconomic correlates among women in Karachi, Pakistan. Cureus. (2018) 12:e7183. doi: 10.7759/cureus.7183
13. Ngoma, M, and Autier, P. Cancer prevention: cervical cancer. Ecancermedicalscience. (2019) 13:952. doi: 10.3332/ecancer.2019.952
14. Rivera, A, Eduardo, P, Moreno, A, Espinosa, E, Arreaga, C, Karool, E, et al. Estudios sobre el virus del papiloma humano (VPH) en el Ecuador, parte I. Revista INSPILIP. (2018) 2:22. doi: 10.31790/inspilip.v2i1.39.g44
15. Ministerio de Salud Pública. Manual de procedimientos del Subsistema de Vigilancia Epidemiológica alerta acción SIVE–ALERTA. 2nd ed. Quito-Ecuador: MSP (2014).
16. Campoverde, EJ, and Guaillazaca, LJ. Propiedades métricas de un cuestionario para evaluar el riesgo de infección con virus de papiloma humano (Tesis de Grado). Ecuador: Universidad Católica de Cuenca (2020).
17. Reed, P, Vile, R, Osborne, LA, Romano, M, and Truzoli, R. Problematic internet usage and immune function. PLoS One. (2015) 10:e0134538. doi: 10.1371/journal.pone.0134538
18. Company, BD, (2021). BD SurePath™ liquid-based pap test. Available at: https://www.bd.com/en-us/offerings/capabilities/cervical-cancer-screening/cervical-sample-collection/surepath-liquid-based-pap-test (Accessed December 20, 2021).
19. Serrano, M, Pozo, M, Medina, D, Viteri, JJ, Lombeida, E, Moreno, L, et al. Encuesta Nacional de Salud y Nutrición 2018 (Informe Técnico), Encuesta Nacional de Salud y Nutrición. Dirección de Innovación en Métricas y Metodologías. Quito-Ecuador: MSP (2019).
20. Mejía, L, Muñoz, D, Trueba, G, Tinoco, L, and Zapata, S. Prevalence of human papillomavirus types in cervical cancerous and precancerous lesions of Ecuadorian women. J Med Virol. (2016) 88:144–52. doi: 10.1002/jmv.24310
21. Bruni, LBRL, Barrionuevo-Rosas, L, Albero, G, Serrano, B, Mena, M, Gómez, D, et al. Human papillomavirus and related diseases report (summary report). ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). Costa Rica: (2019) Available at: https://hpvcentre.net/statistics/reports/XWX.pdf.
22. Carrión, JI, Soto, Y, and Pupo, M. Infección por virus del papiloma humano en mujeres del Cantón Cañar, Ecuador. Rev Cubana Med Trop. (2020) 72 Available at: http://scielo.sld.cu/scielo.php?script=sci_abstract&pid=S0375-07602020000100006&lng=es&nrm=iso&tlng=es
23. García, G, Mendoza, M, Burgos-Galárraga, R, Ollague, K, Vargas, C, and Ruiz, J. Frequency and distribution of HPV genotypes in 800 genital samples of Ecuadorian men and women from the City of Guayaquil. Rev Inst Med Trop São Paulo. (2019) 61:e41. doi: 10.1590/S1678-9946201961041
24. Vega, B, Neira, V, Ortíz Segarra, J, Maldonado Rengel, R, López, D, Orellana, M, et al. Role of self-sampling for cervical Cancer screening: diagnostic test properties of three tests for the diagnosis of HPV in rural communities of Cuenca, Ecuador. Int J Environ Res Public Health. (2022) 19:4619. doi: 10.3390/ijerph19084619
25. Falcón, D, and Carrero, Y. Situación actual de la infección por Virus del Papiloma Humano (VPH) asociado a lesiones cervicales en mujeres del Ecuador. Revisión sistemática. Kasmera. (2021) 49:e49133050. doi: 10.5281/zenodo.4587242
26. Yuxi, JR, and Gallegos, SH. Prevalencia de serotipos del virus de papiloma humano en mujeres de Ecuador. Revista Vive. (2021) 4:262–87. doi: 10.33996/revistavive.v4i11.93
27. Rosa, MI, Fachel, JMG, Rosa, DD, Medeiros, LR, Igansi, CN, and Bozzetti, MC. Persistence and clearance of human papillomavirus infection: a prospective cohort study. Am J Obstet Gynecol. (2008) 199:617.e1–7. doi: 10.1016/j.ajog.2008.06.033
28. Paaso, A, Jaakola, A, Syrjänen, S, and Louvanto, K. From HPV infection to lesion progression: the role of HLA alleles and host immunity. ACY. (2019) 63:148–58. doi: 10.1159/000494985
29. Gutierrez, L, Salazar, DA, Pedroza, A, Chihu, L, Rodriguez, AN, Maldonado, M, et al. Humoral immune response against human papillomavirus as source of biomarkers for the prediction and detection of cervical Cancer. Viral Immunol. (2016) 29:83–94. doi: 10.1089/vim.2015.0087
30. Warren, CJ, Westrich, JA, Doorslaer, KV, and Pyeon, D. Roles of APOBEC3a and APOBEC3b in human papillomavirus infection and disease progression. Viruses. (2017) 9:233. doi: 10.3390/v9080233
31. Milewska, A, Kindler, E, Vkovski, P, Zeglen, S, Ochman, M, Thiel, V, et al. APOBEC3-mediated restriction of RNA virus replication. Sci Rep. (2018) 8:5960. doi: 10.1038/s41598-018-24448-2
32. Pattyn, J, Van Keer, S, Tjalma, W, Matheeussen, V, Van Damme, P, and Vorsters, A. Infection and vaccine-induced HPV-specific antibodies in cervicovaginal secretions. A review of the literature. Papillomavirus Res. (2019) 8:100185. doi: 10.1016/j.pvr.2019.100185
33. Elbasha, EH, and Galvani, AP. Vaccination against multiple HPV types. Math Biosci. (2005) 197:88–117. doi: 10.1016/j.mbs.2005.05.004
34. Sinchi, PST, Torres, ZKS, Martin, LE, Hinostroza, KAA, Espinosa, HM, and Heredia, FRC. Genotipos del virus del papiloma humano en neoplasias intraepiteliales tipo III; Cuenca-Ecuador, 2013-2017. Kasmera. (2019) 47:95–101. doi: 10.5281/zenodo.3521760
35. Denny, L, Kuhn, L, De Souza, M, Pollack, AE, Dupree, W, and Wright, TC. Screen-and-treat approaches for cervical cancer prevention in low-resource settings: a randomized controlled trial. JAMA. (2005) 294:2173–81. doi: 10.1001/jama.294.17.2173
36. Sichero, L, Picconi, MA, Villa, LL, Sichero, L, Picconi, MA, and Villa, LL. The contribution of Latin American research to HPV epidemiology and natural history knowledge. Braz J Med Biol Res. (2020) 53:e9560. doi: 10.1590/1414-431x20199560
37. Calatrava, M, López, C, and de Irala, J. Factores de riesgo relacionados con la salud sexual en los jóvenes europeos. Med Clin (Barc). (2012) 138:534–40. doi: 10.1016/j.medcli.2011.07.020
38. PAHO.org. [citado el 22 de mayo de 2023]. (2017). Available at: https://paho.org/hq/dmdocuments/2017/Inmunizaciones-EPI-InternationalEvaluation-ECU-2017-s.pdf
39. Lazarus, JV, Sihvonen, H, Laukamm, U, Wong, F, and Liljestrand, J. Systematic review of interventions to prevent spread of sexually transmitted infections, including HIV, among young people in Europe. Croat Med J. (2010) 51:74–84. doi: 10.3325/cmj.2010.51.74
40. Pérez-Morente, MÁ, Cano-Romero, E, Sánchez, MT, Castro-López, E, and Jiménez-Bautista, F. Factores de riesgo relacionados con las infecciones de transmisión sexual. Rev Esp Salud Pública. (2017) 91:e1–e67. Available at: https://www.mscbs.gob.es/biblioPublic/publicaciones/recursos_propios/resp/revista_cdrom/VOL91/O_BREVE/RS91C_APM.pdf
41. Wendland, EM, Horvath, JDC, Kops, NL, Bessel, M, Caierão, J, Hohenberger, GF, et al. Sexual behavior across the transition to adulthood and sexually transmitted infections. Medicine (Baltimore). (2018) 97:e11758. doi: 10.1097/MD.0000000000011758
42. Domínguez, SR, Trujillo, T, Aguilar, K, and Hernández, M. Infección por el virus del papiloma humano en adolescentes y adultas jóvenes. Rev Cuba Obstet Ginecol. (2018) 44:1–13. Available at: http://scielo.sld.cu/scielo.php?script=sci_abstract&pid=S0138-600X2018000100017&lng=es&nrm=iso&tlng=es
43. Utami, TW, Kusuma, F, Winarto, H, Anggraeni, TD, Peters, AAW, Spaans, V, et al. Tobacco use and its association with HPV infection in normal uterine cervix: a study from a sustainable development goals perspective. Tob Induc Dis. (2021) 19:1–7. doi: 10.18332/tid/140093
44. Volpato, L, Siqueira, I, Nunes, R, and Piovezan, A. Association between hormonal contraception and injuries induced by human papillomavirus in the uterine cervix. Rev Bras Ginecol Obstet. (2018) 40:196–202. doi: 10.1055/s-0038-1642603
45. Anastasiou, E, McCarthy, K, Gollub, E, Ralph, L, Wijgert, J, and Jones, H. The relationship between hormonal contraception and cervical/Cancer controlling for human papillomavirus infection: a systematic review. Contraception. (2022) 107:1–9. doi: 10.1016/j.contraception.2021.10.018 Dysplasia
46. McCarthy, K, Gollub, E, Ralph, L, van de Wijgert, J, and Jones, H. Hormonal contraceptives and the Acquisition of Sexually Transmitted Infections: an updated systematic review. Sex Transm Dis. (2019) 46:290–6. doi: 10.1097/OLQ.0000000000000975
47. Johnson, KM, Kines, RC, Roberts, JN, Lowy, DR, Schiller, JT, and Day, PM. Role of Heparan sulfate in attachment to and infection of the murine female genital tract by human papillomavirus. J Virol. (2009) 83:2067–74. doi: 10.1128/JVI.02190-08
48. Richards, KF, Bienkowska-Haba, M, Dasgupta, J, Chen, XS, and Sapp, M. Multiple Heparan sulfate binding site engagements are required for the infectious entry of human papillomavirus type 16. J Virol. (2013) 87:11426–37. doi: 10.1128/JVI.01721-13
49. Kumar, A, Jacob, T, Abban, CY, and Meneses, PI. Intermediate heparan sulfate binding during HPV 16 infection in HaCaTs. Am J Ther. (2014) 21:331–42. doi: 10.1097/MJT.0000000000000054
50. Ozbun, MA. Extracellular events impacting human papillomavirus infections: epithelial wounding to cell signaling involved in virus entry. Papillomavirus Res. (2019) 7:188–92. doi: 10.1016/j.pvr.2019.04.009
51. Nanjappa, MK, Medrano, TI, Mesa, AM, Ortega, MT, Caldo, PD, Mao, J, et al. Mice lacking membrane estrogen receptor 1 are protected from reproductive pathologies resulting from developmental estrogen exposure. Biol Reprod. (2019) 101:392–404. doi: 10.1093/biolre/ioz090
52. Torres, K, Ruiz, I, Madrid, V, Chavez, M, and Richardson, V. High risk HPV infection prevalence and associated cofactors: a population-based study in female ISSSTE beneficiaries attending the HPV screening and early detection of cervical cancer program. BMC Cancer. (2019) 19:1205. doi: 10.1186/s12885-019-6388-4
53. Morris, JE, Potter, SW, and Gaza-Bulseco, G. Estradiol induces an accumulation of free heparan sulfate glycosaminoglycan chains in uterine epithelium. Endocrinology. (1988) 122:242–53. doi: 10.1210/endo-122-1-242
54. Tekalegn, KB, Aseffa, T, Gezahegn, H, and Kene, C. High parity is associated with increased risk of cervical cancer: systematic review and meta-analysis of case-control studies. Womens Health. (2022) 18:17455065221075904. doi: 10.1177/17455065221075904
55. HPV Vaccine|CDC, (2021). About HPV Vaccines. Available at: https://www.cdc.gov/vaccines/vpd/hpv/hcp/vaccines.html (Accessed December 16, 2021).
56. Ministerio de Salud Pública-Viceministerio de Gobernanza y Vigilancia de la Salud, Subsecretaria Nacional8de Vigilancia de la Salud Pública, Dirección Nacional de Estrategias de Prevención y Control Ecuador, (2015). Protocolos con evidencia para la deteccion oportuna del cancer de cuello uterino. Available at: https://www.studocu.com/ec/document/universidad-central-del-ecuador/ginecologia-y-obstetricia/protocolo-de-cancer-cervico-uterino/44513814
Keywords: HPV, cervical cancer, sexually transmitted infection, risk factors, genotypes
Citation: Roman C, Andrade D, Hernández Y, Salazar ZK, Espinosa L, Campoverde E, Guallaizaca L, Merchán M, Sarmiento M and Brenner J (2023) Biological, demographic, and health factors associated with HPV infection in Ecuadorian women. Front. Public Health. 11:1158270. doi: 10.3389/fpubh.2023.1158270
Edited by:
Antoinette Van Der Kuyl, University of Amsterdam, NetherlandsReviewed by:
Xinyue Hu, Nanchang University, ChinaArnaud John Kombe Kombe, Agricultural Research Service (USDA), United States
Chinmay Kumar Panda, Chittaranjan National Cancer Institute (CNCI), India
Copyright © 2023 Roman, Andrade, Hernández, Salazar, Espinosa, Campoverde, Guallaizaca, Merchán, Sarmiento and Brenner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diego Andrade, ZGFuZHJhZGVAdWNhY3VlLmVkdS5lYw==