 Sarah Yeo1*
Sarah Yeo1* Yuae Park2
Yuae Park2 Deborah Jean McClelland3John Ehiri1Kacey Ernst4Priscilla Magrath1Halimatou Alaofè1
Deborah Jean McClelland3John Ehiri1Kacey Ernst4Priscilla Magrath1Halimatou Alaofè1- 1Department of Health Promotion Sciences, Mel and Enid Zuckerman College of Public Health, University of Arizona, Tucson, AZ, United States
- 2Department of Behavioral and Community Health Sciences, School of Public Health, University of Pittsburgh, Pittsburgh, PA, United States
- 3Arizona Health Sciences Library, University of Arizona, Tucson, AZ, United States
- 4Epidemiology and Biostatistics Department, Mel and Enid Zuckerman College of Public Health, University of Arizona, Tucson, AZ, United States
Background: Globally, refugee women continue to face higher maternity-related risks from preventable complications during pregnancy and childbirth, partly due to high health care costs, unfamiliarity with the healthcare system, language barriers, and discrimination. Nevertheless, there is still a paucity of literature that evaluates the available evidence in the US. This scoping review delineated the body of literature on maternal health among refugee women resettled in the US in order to identify knowledge gaps in the literature and highlight future research priorities and directions for maternal health promotion.
Methods: Electronic databases were searched in PubMed, CINAHL, PsycINFO, and EMBASE from inception through July 2021. We included all peer-reviewed study designs; qualitative, quantitative, and mixed method if they reported on refugee women's perinatal health experiences and outcomes in the US.
Results: A total of 2,288 records were identified, with 29 articles meeting the inclusion criteria. Refugee women tend to initiate prenatal care late and have fewer prenatal care visits compared to women born in the US. Some of them were reluctant to get obstetric interventions such as labor induction and cesarean delivery. Despite numerous risk factors, refugee women had generally better maternal health outcomes. Studies have also highlighted the importance of health care providers' cultural competency and sensitivity, as well as the potential role of community health workers as a bridge between refugee women and health care providers.
Conclusions: The scoping review emphasizes the need for early prenatal care initiation and more frequent prenatal care visits among refugee women. Furthermore, more needs to be done to mitigate resistance to obstetric interventions and mistrust. The mechanism by which healthy migrant effects occur could be better understood, allowing protective factors to be maintained throughout the resettlement and acculturation process. The scoping review identifies critical gaps in the literature, such as the underrepresentation of different ethnic groups of refugee women in refugee maternal studies in the US. Since this invisibility may indicate unspoken and unaddressed needs, more attention should be paid to underrepresented and understudied groups of refugee women in order to achieve health equity for all.
1. Introduction
Globally, persecution, conflict, violence, and human rights violations forced more than 26.6 million refugees to flee their home countries by the end of 2020 (1). Refugees tend to have higher health needs, limited access to health care, and poorer health outcomes. In addition, resettled refugees also experience challenges accessing health care in a host country due to high costs associated with care, limited health literacy, unfamiliarity with the new healthcare system, language barriers, inadequate health insurance, and racism and discrimination (2–6).
Refugee women, who account for nearly 47 percent of all those displaced across borders, are particularly vulnerable (1). Maternal health is adversely affected by a lack of housing, limited access to water and sanitation facilities, inadequate food and nutrition, and a lack of availability and accessibility of maternal healthcare services during forced displacement (7).
Migrant women, including refugee women, have higher maternal health risks than women in host countries, including gestational diabetes, stillbirth, low-birth-weight infants, early neonatal mortality, prenatal mortality, and preterm birth (8–10).
Refugee and migrant women have been found to attend fewer antenatal care appointments than their counterparts in host countries, despite the potential health risks (11). This is likely due to a variety of factors such as language barriers, cultural differences, transportation difficulties, financial constraints, and fear of discrimination (5, 11, 12). In the United States (US), research indicates that refugee and migrant women tend to postpone antenatal care visits more frequently than their domestic counterpart (11).
The US has welcomed refugees, resettling more than 3 million since the Refugee Act was passed in 1980 (13). Refugees admitted to the US are eligible for short-term health insurance known as Refugee Medical Assistance (RMA) for up to 8 months. Those who qualify for Medicaid may continue to receive benefits after the first 8 months (14). In addition, all refugees are entitled to a trained interpreter for medical visits. Health care providers receiving federal funds are mandated by Title VI of the 1964 Civil Rights Act to provide free interpretation services to those with limited English proficiency (15, 16).
Despite the resources available to admitted refugees, refugee health promotion programs in the US are often short-term, focusing on those who have been in the country for <2 years (17, 18). However, there is evidence that the refugees, the majority of whom had been in the country for more than 5 years, still had limited access to health care due to language barriers and a lack of insurance (19). Although the maternal health challenges experienced by refugee women resettled in the US are well-acknowledged, there remains a paucity of literature that critically summarizes available evidence. One study that synthesized systematic reviews conducted on perinatal health outcomes and care among refugees and asylum seekers identified 29 systematic reviews. Among these, no study focused solely on maternal health among refugees resettled in the US (9).
This scoping review was conducted to delineate the body of literature on maternal health among refugee populations resettled and living in the US. It sought to provide the magnitude, type, and nature of the studies through a thematic analysis, identify knowledge gaps in the literature, and highlight future research priorities for maternal health promotion among refugee women (20).
2. Methods
We included all peer-reviewed study designs, including qualitative, quantitative, and mixed methods. The definition of a refugee follows the one stipulated in the Immigration and Nationality Act (INA) “person who has experienced past persecution or has a well-founded fear of persecution on account of race, religion, nationality, membership in a particular social group, or political opinion” (13). The authors reviewed the papers based on the initial inclusion criteria, and as necessary, further details were added iteratively through consensus among the authors. More detailed inclusion criteria were as follows:
• Original research (excluding literature review, systematic review, scoping review, or policy guidelines)
• Studies that were conducted in the US
• Studies of maternal health care service utilization and maternal health outcomes among refugee women resettled in the US
• Topic is related to maternal care access and utilization among refugee women in the US
The studies were excluded if they were:
• Presentation abstracts without full texts
• Clinical reports
• Studies only related to gynecologic care, family planning, contraceptive care, or female genital mutilation
• Studies whose primary interests are infant or children without discussing maternal health, maternal health care access or utilization (studies that only examined child feeding or breastfeeding among refugee populations were excluded)
• Studies not directly related to pregnancy or maternal health although the population involves pregnant or postpartum refugee women (for example, HIV/AIDS, B hepatitis among pregnant refugee women)
• Studies without disaggregated data on refugee women.
The following electronic databases were searched with the assistance of a health science Librarian (DM): PubMed, CINAHL, PsycINFO, and EMBASE. The general concept areas searched were (1) refugee and (2) maternal. The search strategy was developed for each database including keywords and controlled vocabulary specific to the respective databases such as MeSH and Emtree. The databases were searched from inception through July 15, 2021. We did not apply any language or publication date restrictions to avoid potential bias associated with the restrictions (21, 22). The full search strategy is in Appendix.
After exporting the results from the searches, duplicates were removed using the function in EndNote. Then, the results were exported to Rayyan, a tool for systematic reviews (23). Two authors (SY and YP) independently screened the titles and abstracts of the records in Rayyan. The platform allows for blinded screening functionality so that one reviewer's decision would not influence the other reviewer. Throughout the review process, reviewers met on a regular basis to discuss the differences and reach a consensus. We intended to consult the other authors if any disagreements arose, but there were none.
The first author created a data extraction form to chart the results, which was validated through the screening process and modified as needed. After completing the form, two reviewers read the selected articles, entered the extracted data into the agreed form, and conducted a thematic analysis based on the form. The data were synthesized based on themes such as outcomes investigated and pregnancy period (prenatal, intrapartum, postpartum). Finally, we organized the studies and data by the identified themes, summarized the key findings, and discussed the implications.
We did not perform a quality assessment to exclude studies based on the results because the aim of this scoping review was to provide an overall picture of existing knowledge in relation to the topic of interest. The reporting followed the PRISMA guidelines.
3. Results
A total of 2,288 records were identified, with 29 articles meeting the inclusion criteria (Figure 1). Seventeen of the articles included were quantitative, 11 were qualitative, and one was a mixed method study. One-third of the studies included were on Somalis, and one-fifth were on Indochinese/Southeast Asians. Most studies were conducted in Minnesota, followed by New York and Ohio (Table 1).
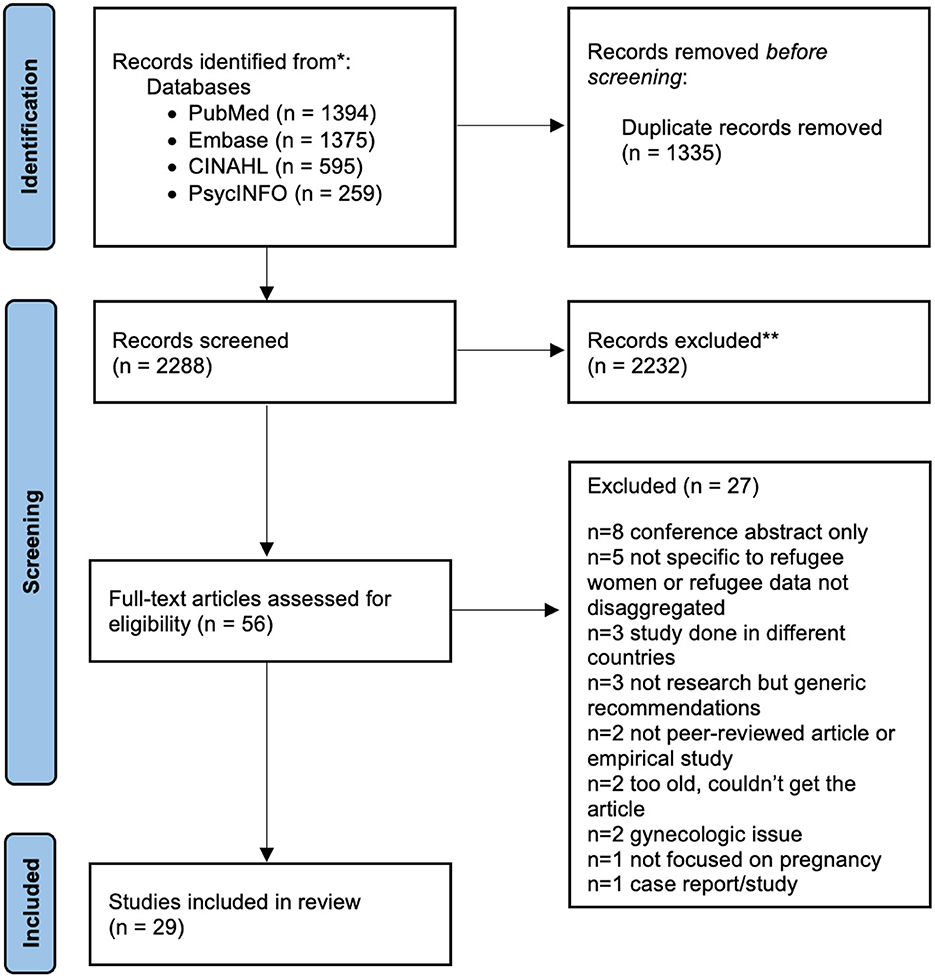
Figure 1. PRISMA flowchart of study selection.
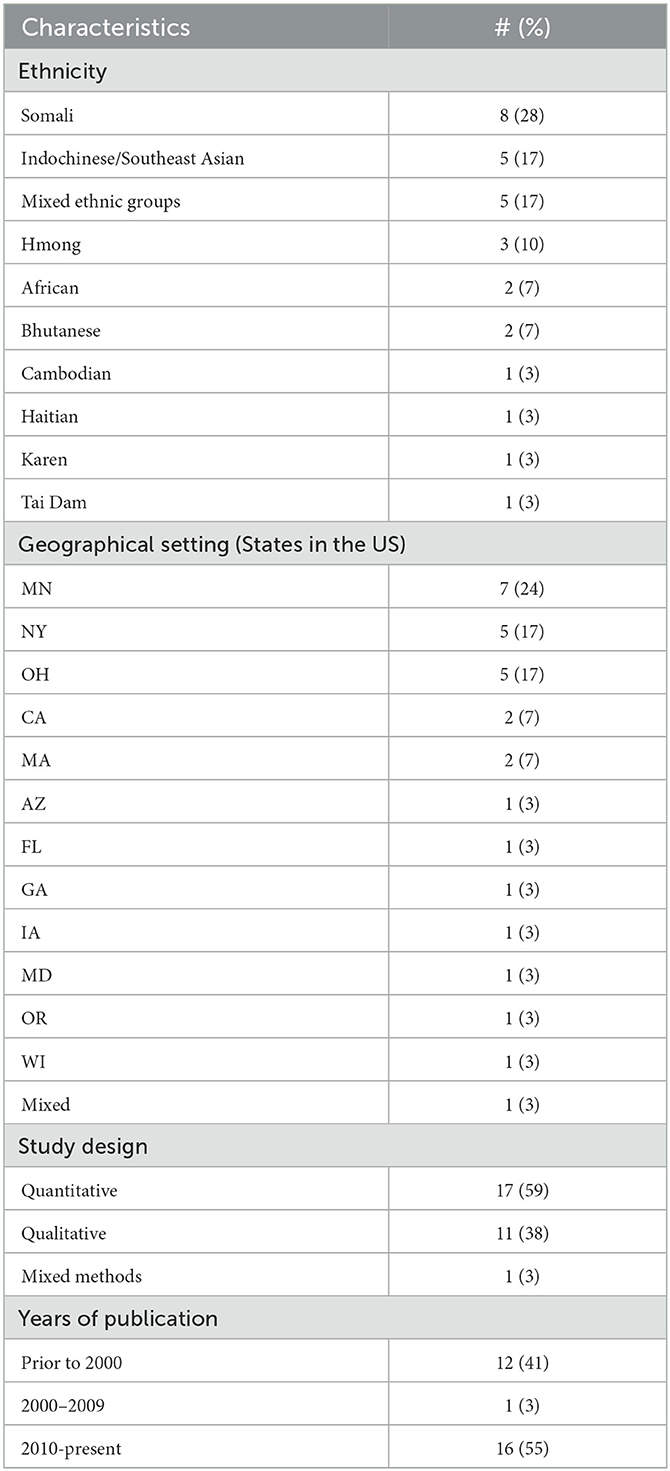
Table 1. Summary of the included papers.
To some extent, the studies on refugee maternal health appear to mirror the influx of refugees in the country caused by political turmoil and conflicts. As of 1981, in the aftermath of the Vietnam War and the fall of Saigon, ~500,000 refugees from the affected areas had fled to the US (24). Southeast Asians accounted for roughly one-third of annual deliveries in some of the US cities that received a high volume of refugees (25), and a small city with a total population of 97,000 at the time had ~16,000 Cambodian refugees (26). As a result, all studies published in the 1980's, with the exception of one, described maternal characteristics and outcomes, issues and cultural beliefs, values, and practices of Southeast Asians, and discussed challenges caused by new encounters with new immigrants and cultural and linguistic differences. The authors were mostly doctors and nurses who were grappling with the new challenges and most of the studies were conducted in the states that accepted a large number of refugees. The early 1990's were marked by the civil war in Somalia, and the US started resettling refugees from Somalia in 1990. Since then, Somali refugee arrivals have remained high with more than 100,000 refugees from Somalia during the last two decades (27). Out of all reviewed studies, eight studies, which is around 30%, were on Somali refugee women. Table 2 illustrates the overall characteristics of the included studies.
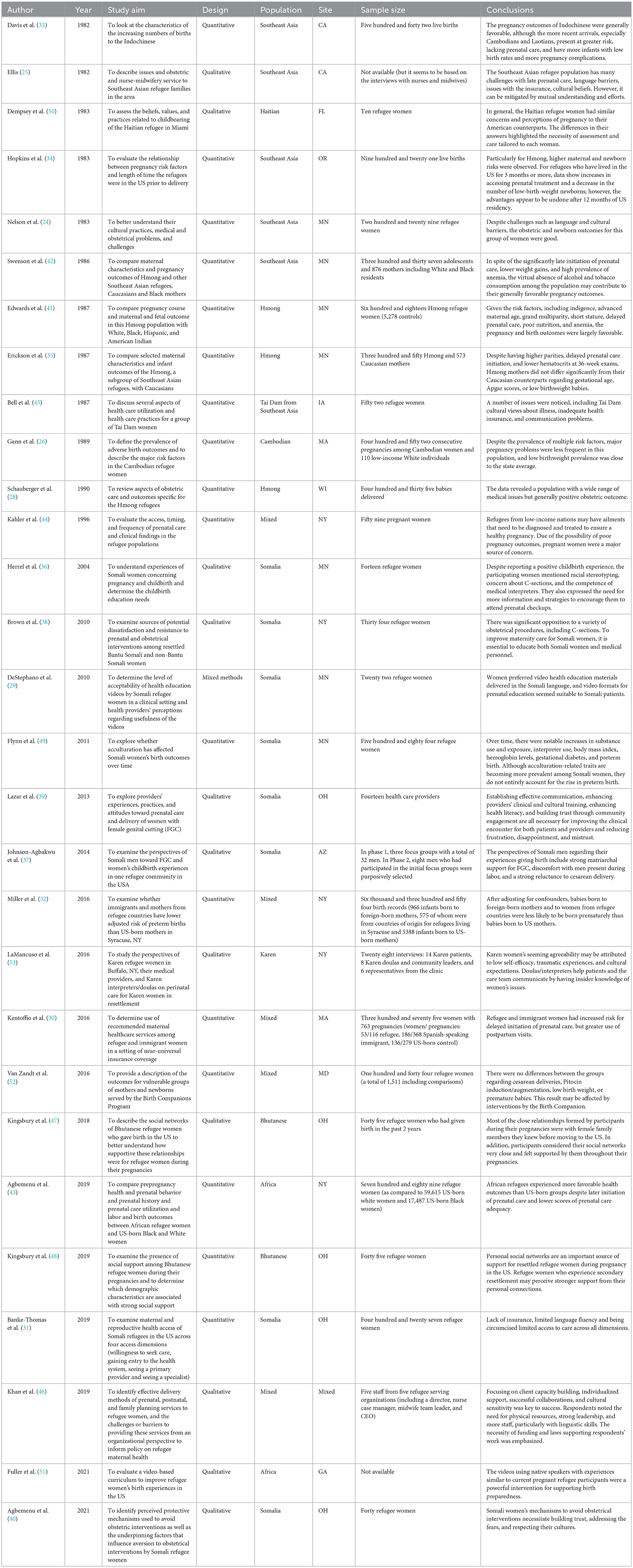
Table 2. Summary of included papers.
The following sections present a summary and critical appraisal of key findings of the included studies.
3.1. Maternal health care utilization
3.1.1. Prenatal care
Overall, refugee women tend to initiate prenatal care late and have fewer prenatal care visits than women born in the US (28–32). In the early 1980's, studies on Indochinese women consistently found that refugee women delayed seeking prenatal care. Many women delayed seeking prenatal care until the second or third trimester or did not seek prenatal care at all (25, 33, 34). One study on the Hmong refugee women noted a similar pattern with 16% refugee women beginning care in the first trimester, compared with 44% of the White women (35). A more recent study also indicated that 20.6% of refugee women had their first prenatal care visit after the first trimester, compared with 6% of women born in the US (30). The authors suggested that although women may recognize the importance of prenatal care visits, (36). refugee women may not be fond of visiting hospitals or perceive that a hospital is only for the sick (37). Or they may be reluctant to reveal their pregnancy and seek advice from elders rather than health care providers (37). According to one study, Hmong refugee women are reluctant to undergo procedures including pelvic exams, blood draws for testing, and the use of iron supplements since these practices violate their cultural traditions (35). These perceptions, preferences, and cultural norms all appeared to contribute to refugee women's delayed prenatal care visits.
3.1.2. Intrapartum
One theme that stood out in the scoping review was avoidance and resistance toward intrapartum interventions particularly among Somali women (36–40). and Southeast Asian women. The opposition seemed deeply rooted in the perception that health care providers prefer the interventions, such as induction and cesarean delivery, as “they were quicker, more convenient, or more lucrative” (39). Or Somali women considered the intervention to be the result of health care providers' ignorance of how to properly care for women with female genital cutting (FGC) (37). There were also studies on Southeast Asian refugee women that demonstrated their resistance to “unnatural” practices (24, 28, 35). They frequently held the view that cesarean birth and episiotomies were unnatural procedures with unfavorable outcomes. Some people believed that having a C-section is an indication of their female incapacity and a lasting physical disability (24).
3.1.3. Postpartum
A recent study comparing the use of prenatal and postpartum health services among refugee women and women born in the US found that refugees were more likely to have postpartum visits (73.3% and 54.8%, respectively) although the study does not elaborate on the reason (30).
3.2. Maternal health outcomes
3.2.1. Prenatal
Two studies reported that hypertension and preeclampsia were less likely to be observed among refugee women (28, 41). However, one study of Hmong women discovered that they were five times more likely to have experienced previous perinatal loss than women in the host country (41). Also, the other study speculated on the possibility of spontaneous miscarriages at home without seeking medical attention (28).
3.2.2. Intrapartum
Studies on Southeast Asian refugee women noted that the prevalence of cesarean delivery was significantly lower in refugee women compared to US-born mothers (24, 26, 28, 33, 41, 42). Also, fewer obstetric interventions such as induced labors and fetal monitoring were observed among Indochinese refugee women (42). African refugee women were less likely to experience cesarean delivery and induced delivery than US-born white and black mothers. The vaginal birth was 73.4% among refugee women as compared to 65.3% US-born white and 66.6% US-born black mothers) (43). Induced delivery occurred in 19.1% of refugees, 29.7% of US-born white mothers, and 25.6% of US-born black mothers (p < 0.001) (43). Another study, which looked at multiple ethnic groups of refugees, found the opposite. In this study, the aggregated refugee group had a higher prevalence of cesarean section (24.3%) than the US-born control (17.9%) or the other immigrant group (17.4%), though the difference was not statistically significant in the adjusted model (30).
3.2.3. Postpartum
Refugee women had generally better maternal health outcomes than US-born women despite risk factors such as delayed initiation of prenatal care, lower weight gains, poor nutritional status, psychosocial factors, high prevalence of infectious diseases, anemia, and short stature (26, 32, 33, 35, 41–43). One study found that Cambodian refugees had a lower prevalence of low birthweight infants, stillbirths, or major pregnancy complications than White low-income women in the state (26). A similar trend was observed in the study of Hmong refugee women. Despite risk factors such as high parity and delayed prenatal care, few low birthweight infants were born to Hmong mothers (35). Prematurity and perinatal mortality rates were also low (41). Another study on Indochinese refugee mothers noted that their low birthweight rates were slightly lower than the comparison (5.7% and 7.1%) and that their median birthweight (3,175 gm) is equivalent to that of mothers in the US. They also had a reduced infant mortality rate (33). A more recent study with mixed ethnic groups reported that refugees had a lower risk of preterm birth than US-born mothers, with an adjusted relative risk of 0.67 (95% CI 0.49–0.89) (32). Another study on African refugee women by Agbemenu et al. also found that African refugee women had fewer preterm births (p < 0.001), fewer low birth weight infants (p < 0.001), and higher rates of vaginal deliveries (p < 0.001) compared to their US counterparts (43). In one study of Indochinese women, the mean birth weight of the refugee women was 350 gm less than the mean for infants born to US-born mothers, but the mean was 3,200 gm, which was within the normal range (24). One study, however, concluded that prematurity was more common among the infants born to the Hmong refugees (8%) than the comparison (4%) (p < 0.01) (28).
3.3. Risk factors
The reviewed studies included different levels and domains of risk factors; biological factors such as maternal age, stature, nutritional levels, anemia, preexisting medical conditions, pre-pregnancy body mass index, behavioral risk factors in pregnancy such as smoking, drinking, and drug use, psychological factors, cultural factors, and social determinants of health such as insurance and socioeconomic status. Below is a summary of key themes identified from this review.
3.3.1. High prevalence of infectious disease
Infectious diseases were prevalent among refugee women who had resettled early in the 1980's (24, 25, 33). In a study with mixed ethnic groups, various infectious diseases were common among the women, including urinary tract infections (26% among African women and 14% among Central American women), monilial vaginitis (29% among African women and 29% among Central American women), tuberculosis (51% among African women, 41% among Central American women, 40% among Sri Lankan women) (44). Multiple parasitic infestation and hepatitis were also prevalent (24, 25, 33). However, a 1990 study of Hmong refugee women found that parasitic infections and hepatitis were less common than previously, indicating that many resettled refugee women in 1979–80 came from refugee camps with poor living conditions (28).
3.3.2. Anemia
Anemia was also common among refugee women, which could be attributed to chronic malnutrition, untreated hookworm infestation, or malaria (24, 26, 28, 42, 44). In a study conducted by Kahler et al. (44), a majority of refugee pregnant women had anemia ranging from 67% (women from Central America) to 88% (women from Africa).
3.3.3. Access to insurance
In two studies, almost one quarter of studied refugee women were not covered by any medical insurance (31, 45). In one study that examined reasons for postponing care among Somali refugees, 81% indicated that not having insurance coverage was a reason for postponing care (31). Also, it was noted that unapproved specialist care was a barrier to care in the same study. Those with health insurance, whether public or private, were more likely to seek care, enter the health system, experience less difficulty in meeting a primary care provider and a specialist compared to those without (31). Another study underscored the importance of having medical insurance for return visits after the initial visit (45).
3.3.4. Female genital circumcision
Compared to women without FGC, Somali refugee women with FGC were 50% less likely to seek medical care. Another factor was severity, with more severe FGC types being linked to lower motivation to seek care and higher access and entrance barriers to care (31, 39). The needs for training to provide “non-judgmental” and optimal care for women with FGC were noted. In one study that interviewed 14 health care providers who serve Somali refugee women, only one provider responded that she had received any type of formal training on the management of women with FGC prenatally and during labor and delivery (39).
3.3.5. Maternal age
Refugee women tend to have advanced maternal age compared to US-born women (26, 41). In a study conducted by Edwards et al., Hmong mothers were seven times more likely to have geriatric pregnancy than the comparison group (41).
3.3.6. Social determinants of health
According to a study, mothers of refugees had less years of education than mothers who were born in the US (11 years of education for the white and black mothers on average and 2 years for the Hmong and 5 years for other Southeast Asians) (42). Another study based on secondary analysis of birth records of mothers from “refugee countries” indicated that they were also more likely to have low socioeconomic status (32). One study on Tai Dam refugee women noted that they were likely to work as full-time housewives or work in a blue-collar job if employed (45). According to one recent study on Somali women, more than half of the surveyed women lived in households that were below the poverty line (31).
3.3.7. Dietary patterns during pregnancy
Southeast Asian refugee women reported two dietary patterns during pregnancy: restricting food intake and reluctance to take medications. Many Southeast women ate only once or twice a day because they were afraid of gaining too much weight and having a difficult delivery (25, 35). Additionally, some pregnant women were hesitant to take drugs like iron and vitamin supplements for concern that the baby could become too big (24, 35).
3.3.8. Language barriers
Many studies frequently mentioned language as a barrier to quality care. Women often had limited English proficiency regardless of length of stay in the US, and many women particularly from Southeast Asia in 1980's were illiterate in their native languages (24, 25, 31, 33, 41, 42, 44, 45). Even when interpretation services were available, women would not freely communicate with male interpreters, particularly during prenatal exams, labor, or delivery (24). Unfamiliar disease names and medical terminology added complexities (24). The quality and objectivity of the interpreters were also questioned at times (39).
3.3.9. Lack of medical records and documentation
Medical history including past pregnancy losses were not properly documented and other important information such as length of gestation, menstrual history, and the data of the last menstrual period was often not known (24).
3.3.10. Mistrust toward health care providers
Patients' mistrust of healthcare professionals was noted, especially among Somali patients (37, 39). The significant mistrust resulting from conflicting cultural norms and views seemed to stand in the way of effective patient-provider dialogue and high-quality care (37, 39).
3.3.11. Decision making
Another theme that came out in terms of maternal health among refugee women was decision making process. Health care decisions concerning refugee women's health were frequently made by the husband or head of the family, potentially due to patriarchal social norms, leading to frustration among providers who want direct communication with the women and her own autonomy (24, 39).
3.3.12. Political uncertainty
While the majority of the studies we analyzed discussed risk factors on a micro level, one research focused on political uncertainty, a risk factor on a macro level. According to Khan et al. (46) one of the difficulties in maintaining program stability was political unpredictability when they spoke with service providers who assist refugee women. Service providers commonly believed that the uncertainty posed a danger to the funding and sustainability of their programs because the number of refugees relocated is decided by a Presidential Executive Order each year and is frequently impacted by political climates.
3.3.13. Discrimination
One of the barriers was racial discrimination by healthcare professionals, according to research by Herrel et al. (36) on Somali refugee women.
3.4. Protective factors/enablers
3.4.1. Social support and network
As social support may influence maternal health, one study investigated the social networks of Bhutanese refugee women who had given birth in the US (47). The women's most important networks during pregnancy were their spouses, female family members, and friends (71.9%). The authors concluded that these “low-heterogeneity” connections are frequently important sources of information, advice, and support during the resettlement experience (47). Another study published the following year by the same authors reached a similar conclusion. Notably, women who relocated from one location in the US to another were almost five times more likely to report having a strong support network, with an odds ratio of 4.52 (95%CI 1.19–17.15) (48).
3.4.2. Low prevalence of smoking and drinking
Many studies found a low prevalence of smoking or drinking among refugee populations, pointing to a possible link between this and favorable maternal health outcomes despite adverse risk factors (26, 32, 35, 41, 42). In a study of Hmong refugee women in 1987, Hmong mothers did not use alcohol or smoke prior to or during their pregnancies, whereas 33.9% of Caucasian women used alcohol and 63.9% smoked (35). A similar trend was observed in a more recent study, though the figures were lower. When compared to refugee women, US-born mothers were also more likely to smoke during the first trimester (28.5% vs. 1.0%), use drugs (10.5% vs. 0.2%), and drink alcohol (1.4% vs. 0.3%) (32).
3.4.3. Acculturation
In one study, Somali refugee mothers were examined to see how acculturation affected birth outcomes including gestational age and infant birthweight. Acculturation was measured using factors such as the age of immigration, years spent in the US, percentage of life spent there, and use of an interpreter at prenatal checkups, and the study concluded that it was not linked to preterm birth or low birthweight of infants in the study (49).
3.5. Cultural issues concerning maternal health and services
3.5.1. Cultural norms and practices concerning pain
Culturally acceptable norms and practices during the intrapartum period may cause difficulties. For example, one study on Indochinese refugee women demonstrated how cultural norms relating to crying out in pain as shameful and pain tolerance as a virtue can make it difficult for health care providers to determine the delivery progression (25). This tendency was also observed in a study on Hmong women, which noted that because they are less likely to express pain and feelings during labor, special attention should be paid to subtle changes to assess progress (24).
3.5.2. Preference for female health care providers
Refugee women preferred female health care providers across cultures and regions (24, 42, 50).
3.5.3. Cultural practices and beliefs in relation to foods after delivery
Studies on Indochinese refugee women and Haitian refugee women noted cultural practices concerning foods for pregnant and postpartum women. For Indochinese postpartum women, only hot foods were allowed such as spicy tea or soup made with ginger root while prohibiting cold foods (25). The Haitian women also had to drink hot beverages such as hot milk or hot ginger tea during labor (50).
3.5.4. Women kept warm after delivery
Cultural practices to keep postpartum women warm were noted in studies on Indochinese refugee women and Haitian refugee women (25, 50). After birth, the Vietnamese, Mien, and Cambodian were traditionally placed near a fire. Postpartum Cambodian women would cover their heads with a towel. To meet the needs of the postpartum women, the midwives in the study provided them with a gown and blanket directly from the warmer (25). The results of the other study showed that Haitian moms made an effort to avoid cold foods and beverages after giving birth (50).
4. Recommendations
Recommendations suggested from the reviewed studies are epitomized in the following.
4.1. Cultural competency and sensitivity of health care providers
Several studies emphasized the importance of building cultural competency and sensitivity of health care providers. The authors argued that health care providers need to be better informed and taught on cultures, traditions, values, expectations and reluctance of refugee women to certain medical interventions such as cesarean delivery (36). Moreover, communication based on the cultural competency will help mitigate deep-rooted distrust between providers and patients and contribute to quality care for refugee women (38, 39).
4.2. Culturally appropriate health education program and materials
The needs for culturally appropriate health education programs and materials were also noted.
Community-based education programs that are collaboratively developed and incorporate both US practices and refugee women's perspectives and cultures could mitigate women's apprehension regarding obstetrical interventions and contribute to better maternal health outcomes (38). Also, given the high illiteracy or limited English proficiency among refugee women, culturally tailored visual materials in their languages, such as education video series, were suggested to facilitate better communication between providers and patients (29, 36, 51).
4.3. Community health educators as a bridge between refugee women and providers
Several studies have emphasized the importance of community health educators, community health workers, or “cultural health navigators” as a potential bridge between the US health care system and refugee women. The studies, whatever the workers were called, revealed similar expectations for their roles. They could disseminate information and alleviate women's fears concerning certain obstetrical interventions (38, 52). They could facilitate communication between providers and patients (37). They could coordinate, providing reminders for the appointments and helping women comply with the care (30). According to one study, trained doulas of the same ethnicity as refugee women could also serve as a role of interpreters and advocates who “translate the cultures,” bridging the communication gap (53).
4.4. Better communication between health care providers and patients
Given their unfavorable attitudes of obstetrical procedures, one study that included the viewpoints of healthcare professionals that serve Somali people highlighted the importance of increasing communication between professionals, patients, and their families during antenatal care (39). The authors also suggested soliciting feedback from the Somali community and engaging them in the decision-making process in order to improve community health literacy and demystify fears (39).
4.5. Interventions to promote prenatal care visits
Several interventions were proposed to increase prenatal care visits, including prenatal appointment reminder calls, transportation to the appointment, and childcare assistance (36).
4.6. Empowering refugee women
The importance of empowering women was mentioned so that they could understand their rights to health care, leading to better decision making and health outcomes (46).
4.7. The need for funding, personnel, and increased interpretation resources
In a study which involved service providers for refugee women, most respondents mentioned the need for more funding, personnel, and interpretation resources to improve service quality (46).
5. Discussion
This scoping review delineated the existing evidence base of perinatal health outcomes and maternal health care experiences among refugee populations in the US. Overall, refugee women had a variety of risk factors, including a high prevalence of infectious diseases, anemia, a lack of insurance, and language barriers, and they were likely to delay prenatal care initiation and had fewer prenatal care visits compared to women in the US. They were opposed to obstetric interventions such as labor induction and cesarean delivery. Despite risk factors and inadequate prenatal care, however, refugee women had better maternal health outcomes than US-born women. A number of studies have associated it to the low prevalence of smoking and drinking. Nonetheless, refugee maternal health necessitates a more nuanced understanding due to heterogeneity and underrepresentation, a lack of aggregation, and a lack of data at multiple levels and trajectories of health outcomes among refugee populations, as described below.
5.1. Geographically and ethnically disproportionate focus on the issue
Although the studies reflect the majority of the trends in terms of incoming refugees in the US, the results highlight an evidence gap in terms of refugee maternal health, as well as a geographically and ethnically disproportionate focus on the issue. Table 3 depicts the number of refugees resettled in the country over the last two decades. Even though a large number of refugees from Burma, Iraq, the Democratic Republic of the Congo, or Iran have resettled in the US during the period, little is known concerning their access to maternal health services or maternal health outcomes. There is also a scarcity of literature on the maternal health status of the approximately 500,000 refugees resettled from former Soviet Union countries between 1983 and 2004 after the collapse of the Soviet Union (54).
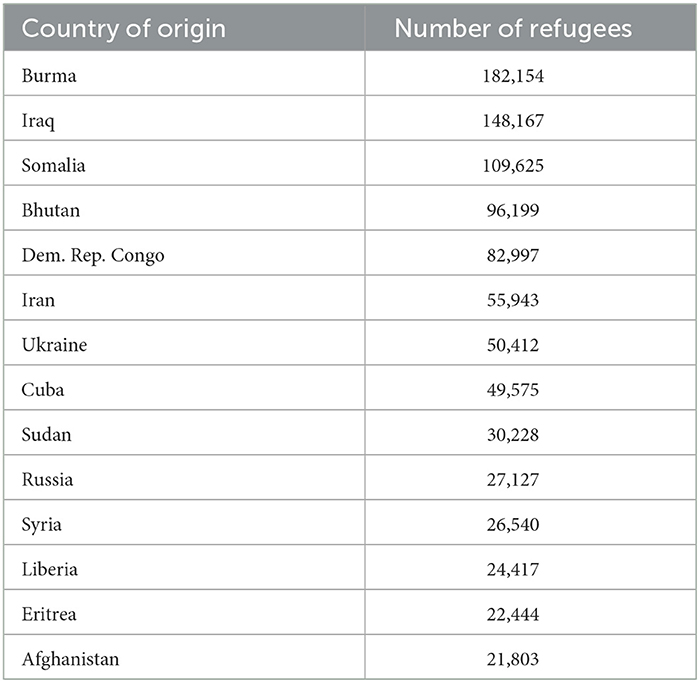
Table 3. The number of refugees resettled in the US (FY2001-FY2022) (27).
In terms of refugee maternal studies, some states were also underrepresented. According to recent data, five states received one-third of all refugees resettled in the US over the last decade: Texas (10%), California (9%), New York (6%), Michigan (5%), and Arizona (4%) (55). Despite the large number of refugees resettled in the states, no studies have been conducted on the maternal health of refugee women in Texas or Michigan, and the access to, utilization, or health outcomes of maternal health services in the states are largely unknown.
5.2. The need to recognize heterogeneity within a seemingly homogeneous group
Several studies focused on heterogeneity within a seemingly homogeneous group. Despite being grouped as “African refugees,” disparities were observed between groups of refugees from different African countries. In terms of highest level of education, English proficiency, and reported employment, resettling Congolese women and Somali women differed substantially (56). Indochinese refugees had varying levels of education, exposure to formal medical care and Western culture and different levels of maternal care utilization (24, 34). Furthermore, the Bantu Somali, although often lumped in with the rest of the Somali refugees, have distinct cultural, linguistic, and ethnic differences that set them apart from the rest of the Somali refugees (38). Different cultures, norms, pre-migratory experiences, and socioeconomic circumstances may result in varying levels of integration and acculturation, as well as access and utilization of maternal care services, satisfaction and trust in the health care system and health care providers. As a result, a greater emphasis should be placed on the subtle differences between seemingly homogeneous groups, such as refugee women or Somali refugees, and the various pathways through which each of them navigates health care systems and interacts with the system.
5.3. Disaggregated reporting
As previously stated, there is a great deal of heterogeneity among refugee women in general, and within a seemingly homogeneous group such as Somalia or Indochinese depending on ethnic groups. Different socioeconomic statuses, pre-migration experiences, pre-existing health conditions, living conditions prior to migration shape refugee women's perceptions and experiences in the US, and potentially lead to different maternal health outcomes. Furthermore, researchers must consider the possibility of a power dynamic among refugee communities, as well as pre-existing differences and disparities in access to resources and opportunities, all of which may influence health outcomes and create disparities. As a result, where possible, it may be useful to further disaggregate the ethnic groups, even within the commonly used category such as African refugees or Somali refugees.
5.4. Healthy migrant effects yet to be better understood
Despite the risk factors that refugee women in the US frequently face, favorable maternal health outcomes have been observed in many studies involving various ethnic groups in the scoping review (32, 41–43, 49). As previously stated, African refugees had fewer preterm births, fewer low birthweight infants, and higher rates of vaginal deliveries than white or black mothers born in the US (43). Despite risk factors such as advanced maternal age, late prenatal care initiation, poor nutrition, and anemia, the incidence of low birthweight infants and prematurity were not higher among Hmong refugee women than among US-born mothers (41). A similar pattern was observed in a more recent study of refugees from various ethnic groups. As previously mentioned, when compared to US mothers, refugee women had a lower risk of having preterm infants (ARR = 0.67, 95% CI = 0.49–0.89, p = 0.007) (32). Lower levels of alcohol and tobacco consumption were frequently mentioned as potential contributors to these healthy migrant effects although no empirical study investigated the potential hypothesis (28, 41, 42).
A number of studies documented “unhealthy acculturation” or “unhealthy assimilation” which could be characterized by the adoption of risky health behaviors such as drinking or smoking (57). For example, one study conducted in Sweden, one of the countries with the largest number of refugees per capita in Europe, revealed that smoking during pregnancy increases with duration of residence among migrants (58). Another study also concluded that the level of acculturation is associated with a higher smoking rate among Asian female adults in the US (59). Thus, determining whether the level of smoking or drinking, which are frequently attributed to the health migrant effects among refugee women, increases with length of residence and its influence on maternal health outcomes could be an important topic.
It may also be worthwhile to identify various factors that may contribute to generally favorable maternal health outcomes, such as dietary practices and health promotion practices among refugee women. Much is known about factors contributing to Mexican women's healthy migrant effects. Traditional dietary practices, lower levels of tobacco and alcohol consumption, stronger family support, and stronger religious beliefs and practices, for example, were found to be protective factors for favorable perinatal outcomes for Mexican women in one study (60). However, other than lower levels of smoking and drinking, potential protective factors for refugee women are largely unknown.
5.5. Resistance to obstetric interventions and its association with maternal health outcomes
Resistance to obstetric interventions such as C-sections and induced delivery, as well as refugee women's mistrust of the health care system and health care providers, has been well documented, particularly among Somali refugee women. Nevertheless, other from a few anecdotal cases reported by health care providers, there is little data on how the resistance affects maternal health outcomes (39).
It is inconclusive whether the prevalence of cesarean delivery is higher among refugee women than among US-born mothers although it is perceived as unacceptably high among Somali communities (37). Thus, more research may be required to determine the current status of obstetric interventions in comparison to mothers in the host country, as well as whether interventions for a specific group are higher than for any other group, and whether resistance to obstetric interventions is associated with adverse maternal health outcomes. As Somali women and men believe that obstetric interventions are the result of a lack of knowledge or training for women with FGC (37), lucrative motives, or rushing practices, more research on the current status, practices, and potential implications in collaboration with communities could help alleviate some of the misunderstanding and distrust.
5.6. Unspoken needs and concerns
According to one study in the scoping review, “gracious acceptance” or “unquestioning agreeability” among refugee women may not always translate into their satisfaction with health care, and there may be some unspoken needs and concerns due to refugee women's reluctance to voice a negative opinion and social hierarchy embedded in the doctor-patient relationship in a particular culture (53). They may be hesitant to ask questions due to lack of knowledge of their rights, and fear potentially associated with their traumatic experiences under dictatorship (53). To solicit their unspoken concerns and questions, it might be useful to get perspectives from others such as doulas or family members who may be able to reveal “insider knowledge” while equipping and empowering refugee women with knowledge and skills (53). For rich discussions with those with limited language proficiency and educational levels, different elicitation strategies, such as video elicitation prior to a focus group discussion, could also be used (37).
5.7. Maternal country of birth as a proxy for refugee status
In some studies, especially when using secondary data, maternal country of birth was frequently used as a proxy for refugee status (32, 43). In one study, women from Burundi, the Democratic Republic of the Congo, Eritrea, Rwanda, and Somalia were considered refugees (43). Despite the large number of refugees from those countries, not all migrants are refugees, and they include people of various socioeconomic backgrounds, language proficiency, perspectives, and values. The ways in which they navigate and experience the healthcare system may also differ, potentially leading to different health outcomes (9).
5.8. Neglected ethnic groups
Certain refugees are more visible than others. Some minorities may be overlooked despite pressing needs. For example, the US Census and many other demographic questions in many major studies classify people from the Middle East and North Africa, including refugee women from Iran, Iraq, Syria, or Afghanistan, as White individuals. However, the majority of people from these regions consider themselves to be an ethnic minority in the US (61). Invisibility and underrepresentation in studies and figures in reports frequently indicate ignorance about their status and needs, as well as a lack of funding or programs dedicated to the population. To compare the levels of need across ethnic groups, it may be necessary to include many, if not all, ethnic groups in studies. Furthermore, in large studies conducted at the state or national level, migration status, including “refugeeness,” could be included, or refugee women could be purposefully sampled in different assessments conducted to assess the health and wellbeing of women, mothers, caregivers, and children.
5.9. Macro-level factors not only micro-level factors
Although macro-level factors such as state-level policies and community-level resources influence maternal health care access and utilization and maternal health outcomes, a limited number of studies shed light on the levels and all the others only focused on the individual level factors. To fully comprehend the health disparities among immigrants, meso- and macro-level factors that cause and reproduce health disparities among immigrants must be better understood (62, 63). A variety of macro-level factors such as immigration policy, perceived discrimination, built environment, neighborhood ethnic composition, the discrepancy between origin and host environment cultures, housing, food supply, transportation, weather, and policy and available resources can be substantially influential for the health of refugees and should be part of the inquiry when studying the health of refugees.
5.10. Limitations
One limitation of this scoping review is that we did not include studies on general immigrants from countries that send many refugees to the US, such as Somalia, nor did we actively seek studies on immigrants from those countries or ethnic groups, such as the Hmong, for some reason. First, people from those countries may have different immigration statuses, and their experiences may differ from those of refugees. According to one observational study, migrant women with refugee backgrounds from African regions are at a higher risk of adverse pregnancy outcomes than migrant women without a refugee background although they are from the same regions (64). Furthermore, immigrant women are more likely to stay longer, and acculturation is strongly related to length of residence in a country and health outcomes (60). As a result, we concentrated our efforts on refugees rather than broadening our search to include other immigrant groups. Another limitation is that this scoping review did not include gray literature. Although there are some discussions in the form of gray literature published by refugee resettlement agencies or other organizations that serve the population, the goal of this scoping review was to delineate the scope and magnitude of the academic evidence bases and identify the evidence gap on maternal health among refugee women resettled in the US so that further research could be better informed. Finally, because we included all published studies, including studies from several decades ago, some characteristics described in studies from the 1980's or 1990's may not reflect current norms.
6. Conclusions
The scoping review emphasizes the critical need for early prenatal care initiation and more frequent prenatal care visits among refugee women. Sensitization and raising awareness to change their perceptions, as well as interventions such as reminder calls or transportation assistance, could help promote prenatal care visits and early initiation of prenatal care among refugee women in the US. Furthermore, more needs to be done to dispel some of the myths and reduce resistance to obstetric interventions and mistrust. Better communication and engagement of women and their families in decision-making could facilitate this. Despite numerous risk factors, refugee women have generally favorable maternal health outcomes. The mechanism by which healthy migrant effects occur could be better understood, allowing protective factors to be maintained throughout the resettlement and acculturation process. In addition, there were some inconsistencies in terms of utilization of maternal health care services and maternal health outcomes in the literature, which could be partly attributed to the high level of heterogeneity. Given the high level of heterogeneity in refugee populations, disaggregated values should be reported whenever possible. Finally, the scoping review identifies critical gaps in the literature, such as the underrepresentation of different ethnic groups of refugee women in refugee maternal studies in the US. Since this invisibility may indicate unspoken and unaddressed needs, more attention should be paid to underrepresented and understudied groups of refugee women in order to achieve health equity for all.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: All data generated or analyzed during this study are included in this published article. As the subject of analysis is published articles, and all of the articles are open to public, the articles can be easily searched and retrieved.
Author contributions
SY conceptualized and designed the study, screened the articles, synthesized the findings, and wrote the manuscript. As a co-reviewer, YP screened the articles and assisted with data analysis. DM provided feedback on the protocol, as well as assistance in developing search strategies and exporting the results. HA provided guidance for designing the protocol and search strategies and overall design. Throughout the process, JE, KE, and PM provided insightful comments and feedback. The final manuscript was read and approved by all authors.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1157098/full#supplementary-material
References
1. UNHCR Global Trends. Forced Displacement in 2020. UNHCR Global Trends. Available online at: https://www.unhcr.org/60b638e37/unhcr-global-trends-2020 (accessed March 9, 2022).
2. Yun K, Fuentes-Afflick E, Desai MM. Prevalence of chronic disease and insurance coverage among refugees in the United States. J Immigr Minor Health. (2012) 14:933–40. doi: 10.1007/s10903-012-9618-2
3. Lipson JG. Afghan refugee health: Some findings and suggestions. Qual Health Res. (1991) 1:349–69. doi: 10.1177/104973239100100305
4. Brouwer KC, Rodwell T. Assessment of Community Member Attitudes Towards Health Needs of Refugees in San Diego. UCSD. (2007). Available online at: https://www.sandiegocounty.gov/content/dam/sdc/hhsa/programs/phs/documents/RefugeeHealthAssessmentUCSD-2007.pdf (accessed May 6, 2022).
5. Morris MD, Popper ST, Rodwell TC, Brodine SK, Brouwer KC. Healthcare barriers of refugees post-resettlement. J Community Health. (2009) 34:529–38. doi: 10.1007/s10900-009-9175-3
6. Lebano A, Hamed S, Bradby H, Gil-Sameron A, Dura-Ferrandis E, Garces-Ferrer J, et al. Migrants' and refugees' health status and healthcare in Europe: A scoping literature review. BMC Public Health. (2020) 20:1039. doi: 10.1186/s12889-020-08749-8
7. Hirani SAA, Richter S. Maternal and child health during forced displacement. J Nurs Scholarsh. (2019) 51:252–61. doi: 10.1111/JNU.12460
8. Gissler M, Alexander S, Macfarlane A, Small R, Stray-Pedersen B, Zeitlin J, et al. Stillbirths and infant deaths among migrants in industrialized countries. Acta Obstetricia et Gynecologica. (2009) 88:134–48. doi: 10.1080/00016340802603805
9. Heslehurst N, Brown H, Pemu A, Coleman H, Rankin J. Perinatal health outcomes and care among asylum seekers and refugees: A systematic review of systematic reviews. BMC Med. (2018) 16:89. doi: 10.1186/s12916-018-1064-0
10. Liu C, Ahlberg M, Hjern A, Stephansson O. Perinatal health of refugee and asylum-seeking women in Sweden 2014-17: A register-based cohort study. Eur J Public Health. (2019) 29:1048–55. doi: 10.1093/eurpub/ckz120
11. World Health Organization. World Report on the Health of Refugees and Migrants. World Health Organization (2022). Available online at: https://www.who.int/publications/i/item/9789240054462 (accessed December 15, 2022).
12. Khanlou N, Haque N, Skinner A, Mantini A, Kurtz Landy C. Scoping review on maternal health among immigrant and refugee women in Canada: Prenatal, intrapartum, and postnatal care. J Pregnancy. (2017) 2017:8783294. doi: 10.1155/2017/8783294
13. Refugee Admissions – United States Department of State. Available online at: https://www.state.gov/refugee-admissions/ (accessed March 9, 2022).
14. U.S. Department of Health and Human Services, Office of Refugee Resettlement. Health Insurance. Available online at: https://www.acf.hhs.gov/orr/programs/refugees/health (accessed March 9, 2022).
15. U.S. Department of Health and Human Services, Office for Civil Rights. Guidance to Federal Financial Assistance Recipients Regarding Title VI and the Prohibition Against National Origin Discrimination Affecting Limited English Proficient Persons. Available online at: https://www.hhs.gov/civil-rights/for-individuals/special-topics/limited-english-proficiency/guidance-federal-financial-assistance-recipients-title-vi/index.html (accessed March 9, 2022).
16. Mishori R, Aleinikoff S. Primary Care for Refugees: Challenges and Opportunities, Vol 96. (2017). Available online at: http://www.wrapsnet.org/admissions-and-arrivals (accessed April 29, 2021).
17. Refugee Medical Assistance | Office of Refugee Resettlement | ACF. (2020). Available online at: https://www.acf.hhs.gov/orr/programs/cma/about (accessed April 18, 2020).
18. Refugee Health Promotion | Office of Refugee Resettlement | ACF. (2020). Available online at: https://www.acf.hhs.gov/orr/programs/preventive-health (accessed April 19, 2020).
19. Su D, Toure DM, Do K, Naw BS, Nlam L, Ern J. 2016 Refugee health needs assessment in Omaha, Nebraska. In: Vol 1. Posters and Presentations. Center for Reducing Health Disparities, University of Nebraska Medical Center (2017). Available online at: https://digitalcommons.unmc.edu/coph_pres/1 (accessed May 5, 2020).
20. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. (2018) 18:143. doi: 10.1186/s12874-018-0611-x
21. Egger M, Zellweger-Zähner T, Schneider M, Junker C, Lengeler C, Antes G. Language bias in randomised controlled trials published in English and German. Lancet. (1997) 350:326–9. doi: 10.1016/S0140-6736(97)02419-7
22. Song F, Eastwood AJ, Gilbody S, Duley L, Sutton AJ. Publication and related biases. Health Technol Assess (Rockv). (2000) 4. doi: 10.3310/hta4100
23. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. (2016) 5:1–10. doi: 10.1186/S13643-016-0384-4
24. Nelson C, Hewitt M. An indochinese refugee population in a nurse-midwife service. J Nurse Midwifery. (1983) 28:9–14. doi: 10.1016/0091-2182(83)90132-5
25. Ellis J. Southeast asian refugees and maternity care: The oakland experience. Birth. (1982) 9:191–4. doi: 10.1111/j.1523-536X.1982.tb01656.x
26. Gann P, Nghiem L, Warner S. Pregnancy characteristics and outcomes of Cambodian refugees. Am J Public Health. (1989) 79:1251–7. doi: 10.2105/AJPH.79.9.1251
27. Refugee Processing Center. (2020). Available online at: https://www.wrapsnet.org/ (accessed April 18, 2020).
28. Schauberger CW, Hammes B, Steingraeber PH. Obstetric care of a Southeast Asian refugee population in a midwestern community. J Perinatol. (1990) 10:280–24.
29. DeStephano CC, Flynn PM, Brost BC. Somali prenatal education video use in a United States obstetric clinic: A formative evaluation of acceptability. Patient Educ Couns. (2010) 81:137–41. doi: 10.1016/j.pec.2009.12.003
30. Kentoffio K, Berkowitz SA, Atlas SJ, Oo SA, Percac-Lima S. Use of maternal health services: comparing refugee, immigrant and US-born populations. Matern Child Health J. (2016) 20:2494–501. doi: 10.1007/s10995-016-2072-3
31. Banke-Thomas A, Agbemenu K, Johnson-Agbakwu C. Factors associated with access to maternal and reproductive health care among somali refugee women resettled in Ohio, United States: A cross-sectional survey. J Immigr Minor Health. (2019) 21:946–53. doi: 10.1007/s10903-018-0824-4
32. Miller LS, Robinson JA, Cibula DA. Healthy immigrant effect: Preterm births among immigrants and refugees in Syracuse, NY. Matern Child Health J. (2016) 20:484–93. doi: 10.1007/S10995-015-1846-3
33. Davis JM, Goldenring J, McChesney M, Medina A. Pregnancy outcomes of Indochinese refugees, Santa Clara County, California. Am J Public Health. (1982) 72:742–4. doi: 10.2105/AJPH.72.7.742
34. Hopkins DD, Clarke NG. Indochinese refugee fertility rates and pregnancy risk factors, Oregon. Am J Public Health. (1983) 73:1307–9. doi: 10.2105/AJPH.73.11.1307
35. Erickson D, Swenson I, Ehlinger E, Carlson G, Swaney S. Maternal and infant outcomes among Caucasians and Hmong refugees in Minneapolis, Minnesota. Hum Biol. (1987) 59:799–808.
36. Herrel N, Olevitch L, DuBois DK, Terry P, Throp D, Kind E, et al. Somali refugee women speak out about their needs for care during pregnancy and delivery. J Midwifery Womens Health. (2004) 49:345–9. doi: 10.1016/j.jmwh.2004.02.008
37. Johnson-Agbakwu CE, Helm T, Killawi A, Padela AI. Perceptions of obstetrical interventions and female genital cutting: Insights of men in a Somali refugee community. Ethn Health. (2014) 19:440–57. doi: 10.1080/13557858.2013.828829
38. Brown E, Carroll J, Fogarty C, Holt C. “They get a c-section ... they gonna die”: Somali women's fears of obstetrical interventions in the United States. J Transcult Nurs. (2010) 21:220–7. doi: 10.1177/1043659609358780
39. Lazar JN, Johnson-Agbakwu CE, Davis OI, Shipp MPL. Providers' perceptions of challenges in obstetrical care for somali women. Obstet Gynecol Int. (2013) 2013:1–12. doi: 10.1155/2013/149640
40. Agbemenu K, Banke-Thomas A, Ely G, Johnson-Agbakwu C. Avoiding obstetrical interventions among US-based Somali migrant women: A qualitative study. Ethn Health. (2021) 26:1082–97. doi: 10.1080/13557858.2019.1613519
41. Edwards LE, Rautio CJ, Hakanson EY. Pregnancy in hmong refugee women. Minnesota Med. (1987) 70:633–7. doi: 10.1016/0277-9536(94)00347-V
42. Swenson I, Erickson D, Ehlinger E, Swaney S, Carlson G. Birth weight, Apgar scores, labor and delivery complications and prenatal characteristics of Southeast Asian adolescents and older mothers. Adolescence. (1986) 21:711–22.
43. Agbemenu K, Auerbach S, Murshid NS, Shelton J, Amutah-Onukagha N. Reproductive health outcomes in african refugee women: A comparative study. J Womens Health. (2019) 28:785–93. doi: 10.1089/jwh.2018.7314
44. Kahler LR, Sobota CM, Hines CK, Griswold K. Pregnant women at risk: An evaluation of the health status of refugee women in buffalo, New York. Health Care Women Int. (1996) 17:15–23. doi: 10.1080/07399339609516216
45. Bell SE, Whiteford MB. Tai Dam health care practices: Asian refugee women in Iowa. Soc Sci Med. (1987) 24:317–25. doi: 10.1016/0277-9536(87)90150-X
46. Khan A, DeYoung SE. Maternal health services for refugee populations: Exploration of best practices. Glob Public Health. (2019) 14:362–74. doi: 10.1080/17441692.2018.1516796
47. Kingsbury DM, Bhatta MP, Castellani B, Khanal A, Jefferis E, Hallam JS. The personal social networks of resettled bhutanese refugees during pregnancy in the United States: A social network analysis. J Community Health. (2018) 43:1028–36. doi: 10.1007/s10900-018-0518-9
48. Kingsbury DM, Bhatta MP, Castellani B, Khanal A, Jefferis E, Hallam JS. Factors associated with the presence of strong social supports in bhutanese refugee women during pregnancy. J Immigr Minor Health. (2019) 21:837–43. doi: 10.1007/s10903-018-0790-x
49. Flynn PM, Foster EM, Brost BC. Indicators of acculturation related to somali refugee women's birth outcomes in Minnesota. J Immigr Minor Health. (2011) 13:224–31. doi: 10.1007/s10903-009-9289-9
50. Ann Dempsey P, Gesse T. The childbearing haitian refugee-cultural applications to clinical nursing. Public Health Rep. (1983) 98:261–7.
51. Fuller TJ, Leonard M, Cochran J, Hutchins RJ, Brioche R, Kitiabi H, et al. Collaborative development and implementation of a video-based curriculum expansion to improve refugee women's birth experiences in the United States. Health Promot Pract. (2021) 22:177–80. doi: 10.1177/1524839920915191
52. Van Zandt SE, Kim S, Erickson A. Nursing student birth doulas' influence on the childbearing outcomes of vulnerable populations. J Community Health Nurs. (2016) 33:128–8. doi: 10.1080/07370016.2016.1191869
53. LaMancuso K, Goldman RE, Nothnagle M. “Can i ask that?”: perspectives on perinatal care after resettlement among karen refugee women, medical providers, and community-based doulas. J Immigr Minor Health. (2016) 18:428–35. doi: 10.1007/s10903-015-0172-6
54. Singer A, Wilson JH. From “There” to “Here”: Refugee Resettlement in Metropolitan America. The Brookings Institution (2006).
55. Monin K, Batalova J, Lai T. Refugees and Asylees in the United States. Migration Policy Institute (2021). Available online at: https://www.migrationpolicy.org/article/refugees-and-asylees-united-states-2021 (accessed June 21, 2022).
56. Mehta PK, Saia K, Mody D, Crosby SS, Raj A, Maru S, et al. Learning from UJAMBO: Perspectives on gynecologic care in african immigrant and refugee women in Boston, Massachusetts. J Immigr Minor Health. (2018) 20:380–7. doi: 10.1007/S10903-017-0659-4
57. Antecol H, Bedard K. Unhealthy assimilation: Why do immigrants converge to American health status levels? Demography. (2006) 43:337–60. doi: 10.1353/DEM.2006.0011
58. Klöfvermark J, Hjern A, Juárez SP. Acculturation or unequal assimilation? Smoking during pregnancy and duration of residence among migrants in Sweden. SSM Popul Health. (2019) 8:100416. doi: 10.1016/J.SSMPH.2019.100416
59. Ma GX. Acculturation and smoking behavior in Asian-American populations. Health Educ Res. (2004) 19:615–25. doi: 10.1093/her/cyg070
60. Callister LC, Birkhead A. Acculturation and perinatal outcomes in mexican immigrant childbearing women. J Perinat Neonatal Nurs. (2002) 16:22–38. doi: 10.1097/00005237-200212000-00005
61. Awad GH, Hashem H, Nguyen H. Identity and ethnic/racial self-labeling among americans of arab or middle eastern and north african descent. Identity. (2021) 21:115–30. doi: 10.1080/15283488.2021.1883277
62. Thurston WE, Vissandjée B. An ecological model for understanding culture as a determinant of women's health. Crit Public Health. (2005) 15:229–42. doi: 10.1080/09581590500372121
63. Viruell-Fuentes EA, Miranda PY, Abdulrahim S. More than culture: Structural racism, intersectionality theory, and immigrant health. Soc Sci Med. (2012) 75:2099–106. doi: 10.1016/j.socscimed.2011.12.037
Keywords: refugee, prenatal care, maternal care, maternal health, United States, refugee health, host country, perinatal care
Citation: Yeo S, Park Y, McClelland DJ, Ehiri J, Ernst K, Magrath P and Alaofè H (2023) A scoping review of maternal health among resettled refugee women in the United States. Front. Public Health 11:1157098. doi: 10.3389/fpubh.2023.1157098
Received: 13 February 2023; Accepted: 05 April 2023;
Published: 09 May 2023.
Edited by:
Georgi Iskrov, Plovdiv Medical University, BulgariaReviewed by:
Eleonora Hristova-Atanasova, Medical University of Plovdiv, BulgariaAndrew Adewale Alola, Inland Norway University of Applied Sciences, Norway
Copyright © 2023 Yeo, Park, McClelland, Ehiri, Ernst, Magrath and Alaofè. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sarah Yeo, c3llb0Bhcml6b25hLmVkdQ==