 Shan Qiao
Shan Qiao Sara Wilcox
Sara Wilcox Bankole Olatosi
Bankole Olatosi Xiaoming Li
Xiaoming Li
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Public Health , 02 June 2023
Sec. Public Mental Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1156717
This article is part of the Research Topic Community Series in Mental Illness, Culture, and Society: Dealing with the COVID-19 Pandemic, Volume VI View all 10 articles
Despite the aggregated burdens and challenges experienced by rural Black women during the COVID-19 pandemic, many likely also demonstrated strength and resilience to overcome challenges. A mixed methodology and a community-based participatory approach will be used to collect multilevel data on challenges, responses, resilience, and lessons during the pandemic from Black women, community health workers, and community leaders in rural areas in South Carolina (SC). Specifically, the unique circumstances and lived experiences of rural Black women during the COVID-19 pandemic will be documented to understand their needs regarding effective management of social, physical, and mental health challenges through focus group discussions and in-depth interviews with Black women, community health workers, and local community leaders recruited from rural SC communities. Barriers, facilitators, and potential impacts of multilevel resilience development will be identified through a survey administered among rural Black women recruited from 11 rural counties (with one as site for a pilot testing of the questionnaire). A report for public health practice will be developed, including recommended strategies to optimize health systems' emergency preparedness and responses through triangulation of qualitative and quantitative data from multiple sources. Findings in the proposed study will provide valuable references in terms of addressing social determinants of health factor challenges during the pandemic, fostering resilience, and informing evidence-based decision-making for policymakers. The study will contribute to the development of public health emergency preparedness plans, which can promote the resilience of women, their families, and local communities as well as optimize effective preparedness and response of health systems for rural Black women and their families during infectious disease outbreaks and other public health emergencies.
Existing literature suggests that women are more likely to bear the brunt of socioeconomic and health consequences of the pandemic due to the compounded effect of pre-existing gender inequity, their social role as caregivers, work-life conflicts, increased domestic violence, and limited access to healthcare services in the context of COVID-19 (1–4). Unpaid caregiving during the pandemic has imposed a disproportionate burden on women who are often the primary caregivers for children and older adults (5). Lack of paid leave, family caregiving responsibilities, and traditional gender roles have placed additional strains on work-life conflicts (6, 7). When social isolation and distancing practices are being enforced in a pandemic, the risk of violence against women increases (8, 9). The pandemic also has impacted the availability and utilization of women's healthcare services such as sexual and reproductive health services and preventive care such as mammography screening (10, 11). Mental health issues for women related to financial and other stressors are also evident during the pandemic (12). Furthermore, national polls indicate that women are more likely than men to report negative mental health effects from worrying about COVID-19 (13, 14).
Black women from rural households in southern states are especially vulnerable, given the existing disparities in social determinants of health (SDOH), health infrastructure, and access to healthcare resources (15–18). The disproportionate effects of COVID-19 among racial/ethnic minority groups were present from the beginning of the pandemic (19). Counties with large Black populations experienced greater case, mortality, and progression rates of the disease than counties with small Black populations (20). Analysis of data from the COVID Tracking Project highlighted that the national COVID-19-related mortality rate for Black people was 2.4 times higher than that of White people (21). The COVID-19 pandemic further elevated social disparities. Black people were more likely than White people to experience job or wage loss because of the pandemic (44 and 38%, respectively) (22) and experienced higher levels of food insufficiency and rent or mortgage defaults relative to other racial and ethnic groups as well (23). In addition, the southern United States is a region in which structural racism and oppression have resulted in poor health infrastructure, limited access to care (e.g., lack of health insurance and geographic maldistribution of healthcare services) (24), and biased and suboptimal care (25, 26).
Despite the aggregated burdens and challenges experienced by rural Black women during the pandemic, it is likely that many have also demonstrated strength and resilience to overcome challenges and manage critical resources for themselves and their families (27, 28). Resilience refers to the capacity to which individuals are able to respond to stress-induced challenges and burdens (29). Within the literature over the past few decades, there has been a shift to consider resilience not only as an individual trait but, from the ecologic perspective, an bidirectional interaction between individuals and their environment (30). Thus, resilience can now be understood as a multidimensional, responsive, and dynamic process across the life span (31). Resilience can be cultivated through a series of protective factors such as social support, self-efficacy, positive self-perception, and an optimistic perspective of the future (32–34). The extant literature demonstrates the essential role of protective factors in aiding in the bolstering and maintenance of resilience within the individual, community, and the institutional levels of the socioecological model in times of crisis including public emergencies (35–39). Several recent studies particularly examined the resilience model for older people in the context of COVID-19 pandemic (40, 41).
Resilience can play a significant role in the coping and responses to the pandemic (42, 43). However, empirical data are especially limited regarding the needs and challenges among Black women in rural areas, how they successfully cope with SDOH challenges during the pandemic, and the facilitators of resilience from multiple levels (e.g., family, community, policy) (14, 44–46). Furthermore, there are limited data on first-hand evidence from front-line health workers and key stakeholders in rural areas such as community health workers and community leaders who are rooted in local communities, serve women in rural areas through connecting local neighborhood and external resources, and can provide insights and recommendations to public health policy and practice (47).
To address these gaps, a mixed-methods exploratory study will be conducted to collect multilevel data on challenges, responses, and resilience among rural Black women during the pandemic. A community-based participatory approach will be used to engage Black women, community health workers, and community leaders in South Carolina (SC), a state with 27% of its population being Black and 33.7% of its population living in rural areas (48). The advanced understanding of the resilience process and facilitators and barriers of resilience for women will contribute to optimizing emergency preparedness and response for special needs and challenges identified for Black women from rural areas and their families (42).
SC is a largely rural state (48), currently ranked the 42nd overall healthiest state, 49th for cost of care, and 32nd for access to care in the nation (49). A majority of counties in SC (45 of 46) are designated as Health Professional Shortage Areas (50, 51). SC also ranked at the bottom for various health outcome indicators in 2019: 49th in infectious diseases, 41st in maternal mortality, and 39th in infant mortality (52). According to the most recent American Community Survey, White people account for 63.7% of the whole population, followed by Black people (27.03%), and Hispanics or Latinos (6%). In SC, racial disparities exist in many healthcare outcomes such as breast cancer (53, 54), stroke (55), maternal health (56, 57), and cervical cancer (58, 59). Considering SC's poor health ranking, striking disparities in many health outcomes, racially diverse population, and historical Southern context, SC has an appropriate environment to explore and understand lived experiences of Black women living in rural areas facing SDOH challenges during the pandemic. The study will be conducted in 11 rural counties (out of totally 46 counties in SC) in which Black people account for over 30% of the total population. These counties have been heavily hit by COVID-19. The participants of the study are adults with a large range of age in order to explore the lived experiences across life course.
The research team will closely work with community-based organization and community health workers on the study design and implementation. Our main local partner is the South Carolina Community Health Worker Association (SCCHWA), a community-based organization made up of community health workers and their supporters in SC. It provides a forum for networking and sharing of strategies and resources as well as a foundation for education and training of community health workers. The SCCHWA has implemented numerous health promotion education projects with local partners across SC, including the multilevel COVID-19 vaccination promotion project among Black communities with collaboration from our team. With the assistance of the SCCHWA, a CAB will be assembled to include Black women, community leaders, government officers, healthcare providers and community health workers. The CAB members will either live in or serve people in the local communities or have strong connections with rural communities. The CAB will meet every 2 months to provide advice regarding community engagement, study protocol development, and research implementation and dissemination.
The proposed mixed methodology study consists of three main specific research phases in term of study design. Phase 1 is qualitative research via focus group discussions (FGDs) and in-depth interviews with Black women, community health workers and community leaders in rural areas. Phase 2 is quantitative research including the adaption of assessment tools and implementation of a survey among Black women from the research sites. Phase 3 includes data triangulation and report writing. A community charrette approach (60) will be applied in report revision and finalization to empower local partners.
FGDs will be conducted with Black women, community health workers, and local community leaders recruited from various rural SC communities to document the unique circumstances and lived experiences of rural Black women during the COVID-19 pandemic and to understand their needs regarding effective management of social, physical, and mental health challenges.
FGD is selected to collect qualitative data for Aim 1 since it is a time-efficient and interactive approach to conduct need assessments among diverse subgroups (61). With the assistance of SCCHWA and the CAB, participants will be purposely recruited from the study sites including Black women (n−15), community health workers serving rural communities (n−10), and local community leaders (n−10) to conduct 3 FGDs. The Black women will include young adults (18–34 years of age), middle-aged adults (35–59 years of age), and older adults (≥60 years of age) given that COVID-19 may impose different challenges for women at different age. COVID-19 infection history of women and their families will also be considered to maximize the focus group representativity. Community health workers will include the ones staying short in the local communities (<3 years) and staying long (≥ 3 years). Community leaders may include people from churches, non-government organizations, grassroot organizations, or other trusted messengers in local communities with covering both health-related organizations and non-health-related organizations. Potential eligible participants will be identified through local community health workers in study sites (for Black women), SCCHWA staff (for community health workers), or recommendation by the CAB (for community leaders). Research staff at SCCHWA will conduct outreach and recruit the participants, highlighting that the FGDs are confidential.
To ensure that FGD participants have sufficient time and opportunities to express their opinions and share their experiences, the research team will hold relatively small FGDs with 5–6 participants per group. The group discussion guidelines will be drafted by the research team and then be reviewed and discussed by our local partners and the CAB to ensure that the questions are meaningful in local contexts and asked in appropriate way/language. The FGDs will be facilitated by experienced SCCHWA project staff, but research staff_will attend all of the FGDs as backups and for assistance. The main topics of the FGDs may include: (1) lived experiences in response to the COVID-19 pandemic, including COVID-19 prevention, testing, and treatment and health seeking; (2) challenges with various health and social aspects during the pandemic; (3) impacts of COVID-19 on physical health, mental health, family relationships, social networks, and socioeconomic conditions; (4) needs and available resources to address multiple challenges, especially SDOH challenges; and (5) unmet needs and additional resources they need to deal with the evolving pandemic and life recoveries. To avoid research burden of the participants, the research team will select relevant topics and tailor the questions to different groups. For example, for Black women participants, the questions will focus on their own experiences; for community leaders, the topics will also include their observations of the whole communities; and for community health workers, the discussion will focus on lessons in bridging communities and healthcare systems, reflections on organizational responses, and suggestions toward capacity building as public health front-line workers. The FGDs will last about 1 h and be held in a private conference room at the SCCHWA site offices. Considering the transportation cost and burden for participants, online FGDs via an Internet conference (e.g., Team, Zoom meetings) will also be prepared for, depending on local logistics as well as suggestions and preferences of the participants.
In-depth interviews will be conducted with Black women, community health workers, and community leaders recruited across the communities to explore effective strategies that women use in coping with various challenges in the pandemic and identify barriers to and facilitators of multiple resilience. Given that people will apply various coping strategies and demonstrated different types of resilience, in-depth interviews will be an appropriate approach to collecting qualitative data regarding our specific research aims, which will offer opportunities for one-on-one, in-depth conversations with minimum influence of others on the interviewee.
Following a similar study protocol as used in the FGDs, the research team will purposely recruit about 20 Black women living in rural areas, 10 community health workers, and 10 local community leaders for in-depth interviews. A “saturation” approach will be applied in the interviews, whereby respondents will be interviewed until a point that no significant new data are anticipated from additional interviews. Data saturation will be assessed after ~60% of the interviews have been conducted with each group of participants.
Separate interview guides will be developed for Black women, community health workers, and community leaders. Semi-structured qualitative interview guides will be created with significant input and guidance from the local CAB. The interview guides will be grounded in phenomenological and constructivist frameworks, which provide a general structure for discussion but require participants to provide their own conceptualizations of terms and phrases based on their life experiences. The interview with Black women will document their lived experiences and various coping strategies in response to SDOH challenges during the pandemic; identify components of multilevel resilience, interactions of different resilience, and barriers and facilitators for resilience; and needs, expectations, and suggestions for health systems' emergency responses tailored to their needs. Interviews with community health workers and community leaders will focus on community resilience and institutional/organizational resilience observed and experiences during the pandemic, local resources, community connections, and their reflections and insights on optimizing emergency response strategies in healthcare systems and local communities. Additional topics will be added as appropriate and as indicated by the CAB and findings from the FGDs. With appropriate consent, the interviews will be audio-recorded. Interviewers will take field notes during the interviews to serve as a complementary data source. The field notes will include interviewees' non-verbal responses and interviewers' observations or impressions regarding the conditions of the interviews. Each interview will take 1 h led by a trained interviewer in a private room. Online interview will be conducted if preferred by the participants.
The analysis of both FGD and in-depth interview data will be guided by grounded theory (62) in order to obtain key themes based on data itself rather than preexisting opinions. This inductive approach helps prevent preconceived notions from interfering with the data collection and analysis (62). In keeping with the grounded theory principles, data analysis will run concurrently alongside data generation. Transcription and coding will take place after the first three interviews for each group. The line-by-line open coding will sensitize us to the range of potential meanings in the data and identify themes. Axial coding will be used to elucidate relationships between themes and subthemes along with their properties and dimensions. Memo writing and diagramming will be used to develop themes and relationships between themes. Research staff will independently code all of the transcripts. Any coding disagreements will be resolved through discussions. Representative quotes will be selected verbatim to illustrate key findings. Data analysis will be conducted through the software NVivo 12. The project coordinator and research staff at SCCHWA and CAB members will also contribute to result interpretation and findings dissemination.
The findings from qualitative research in Phase 1 will be used to inform the cultural adaptation of assessment tools in Phase 2 and data triangulation and report development in Phase 3. Specifically, the measurement instruments and existing scales will be adapted regarding resilience, coping, and other psychosocial wellbeing outcomes in the local context. The results of the qualitative studies will advance our understanding of the social and cultural environment that surrounds Black women, their families, and community health workers, and thus assist us in measurement selection and adaptation. Reports will be developed on needs assessment and strategy recommendations based on the rich qualitative evidence. For example, the materials of lived experiences and challenges of Black women, community health workers, and other key stakeholders in rural communities as they have faced this public health crisis will inform potential interventions and policymaking in fostering resilience and readiness for public health emergencies among rural communities and healthcare systems. Specific scenarios and examples needed in the intervention will also be developed by extracting the qualitative data and/or citing representative quotes. From the perspective of the community-based research, our local partner will be engaged in each step of the study design and data collection and analysis, which will empower community health workers and increase their ownership of this project, and thus further strengthen the academic-community trust and collaboration.
After discussion with our local partner SCCHWA, a cluster sampling approach will be used to recruit ~200 Black women living in rural areas in SC. Specifically, the research team will select 11 counties (with one county as the site for pilot testing) in SC as our study sites. About 20 Black women in each site will be recruited. With the coordination of research staff at SCCHWA, community health workers serving the rural communities in the study sites will recruit potential participants for the survey through disseminating project flyers at community activity centers, community clinics, grocery stores, and public libraries. Inclusion criteria include: (1) Black females; (2) at least 18 years of age; (3) living in the study site since the COVID-19 outbreak; and (4) not concurrently participating in any health promotion intervention. A half-day project training workshop will be conducted for the local research team (mainly composed of community health workers) in terms of study protocol, data collection, and research ethics. The trained research staff (survey interviewers) will confirm the eligibility of the participants; explain the study design, including the purpose, procedure, risk and benefit, and confidentiality issues; and invite them to participate. All who agree to participate will provide written informed consent.
Survey interviewers (local community health workers who receive project training) will administer the survey to participants via Tablets. The Tablet will display and read (with a real human voice, utilizing a headset) the survey questionnaire in a private room (e.g., community health worker's office) in local counties where the participants are recruited. By using this method, the research team will not only ensure the privacy and quality of the data collection, but also ensure that varying degrees of literacy do not affect the individual's ability to understand the items. Clarifications or assistance (with the Tablet) will be provided on site by the interviewers as needed. It is estimated that the survey will take about 30 min. Participants will be instructed to take a short break (~5 min) after every 15 min as needed.
In the survey, basic screening will be conducted to avoid logic errors in completing the questionnaire. The project PI and local partner will take the responsibility of data quality control and monitoring during the data collection by randomly selecting and reviewing first five finished questionnaires and data record from each site. The questions and feedback will be provided to the research staff in a timely way through daily supervision by SCCHWA and regular meeting and monitoring by the USC research team.
The key measurements in this study are composed of primary outcomes, secondary outcomes, and individual background measures (to be collected through the survey questionnaire); and contextual measures (to be extracted from publicly available datasets). Most of the demographic and psychosocial and health behavior measurements used for Black women participants in this study are field-tested and validated in previous studies and have been shown to be reliable and valid. The measures will be further modified based on the specific aims of this study, qualitative study findings, and literature on resilience, coping strategies, mental health in the context of COVID-19. The final draft of all measures will be reviewed by the CAB and will be pilot-tested among 15 Black women recruited from pilot-testing site to obtain participants' perspectives on the clarity, cultural sensitivity, and appropriateness of relevant measures.
Primary outcomes will be mental health symptoms measured by standardized self-reported scales with good psychometric characteristics (e.g., validity and reliability) in previous studies: (1) depression, measured Patient Health Questionnaire-9 (PHQ-9) (63). One recent literature review suggests solid evidence supporting the validity of the PHQ-9 as a unidimensional measure of depression. Used in major depressive disorder (MDD) screening with a cut-point of 11, its sensitivity was 95% and specificity was 88.3% (PPV 51.4%, NPV 48.6%) (64); (2) anxiety measured by Generalized Anxiety disorder-7 (GAD-7) (65). Confirmatory factor analyses suggest the 1-dimensional structure of the GAD-7 and its factorial invariance for gender and age. GAD-7 shows high reliability across gender and age groups (α = 0.89). Intercorrelations with the depression and the Rosenberg Self-Esteem Scale were r = 0.64 (P < 0.001) and r = −0.43 (P < 0.001), respectively (66). (3) Post-traumatic stress disorders, PTSD, measured by (PC-PTSD-5) (67). The PC-PTSD-5 is modified based on Primary Care PTSD screen (PC-PTSD) to reflect the new Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria for PTSD. The PC-PTSD-5 demonstrated excellent diagnostic accuracy (AUC = 0.941; 95 % C.I.: 0.912–0.969) (68); and (4) domestic violence measured by a four-item scale that asks respondents how often their partner physically Hurt, Insulted, Threatened with harm, and Screamed at them. These four items make the acronym HITS (69). This is a short domestic violence screening tool widely used in a family practice setting. The sensitivity ranged from 30 to 100% and specificity ranged from 86 to 99%. The reliability is generally good (α ranged from 0.61 to 0.8) (70).
Secondary outcomes will include multiple resilience and their resources: (1) individual resilience of Black women, for example, personal resilience strengths (71), coping strategies (72), self-concept (73); (2) family factors, for example, quality of relationship (74), and healthcare system factors, such as perceived acceptance and trust from healthcare facilities; (3) community resilience, for example, perceived social support (75); and (4) institutional resilience, for example, organizational resilience (an organization's ability to anticipate issues ahead of time and develop a plan for handling identified problems) (76).
Individual background measures are basic sociodemographic variables, including: (1) age; (2) educational level; (3) marriage status; (4) household income; (5) health insurance; (6) employment; and (7) COVID-19 infection history, long COVID symptoms, or caregiving experience for family members or neighbors infected by COVID-19, if any.
Contextual characteristics variables include aggregated county-level measures at the structural level, community level, and institutional level (Table 1): (1) Structural level: SDOH obtained from the American Community Survey (ACS) (77); (2) Community level: social capital data from an existing dataset from the county-level Social Capital Index Project in the US (78), behavioral and environmental risk exposure data obtained from Behavioral Risk Factor Surveillance System (BRFSS) and County Health Rankings & Roadmaps Program (CHRRP); and (3) Institutional level: health infrastructure data can be retrieved from Area Health Resources File (AHRF), including health professions capacity [primary care physicians (PCP) per 100,000 population, population to PCP ratio] and distance to health facilities. All the aggregated data are county-level measures so we control the cluster effect of various counties in the analysis.
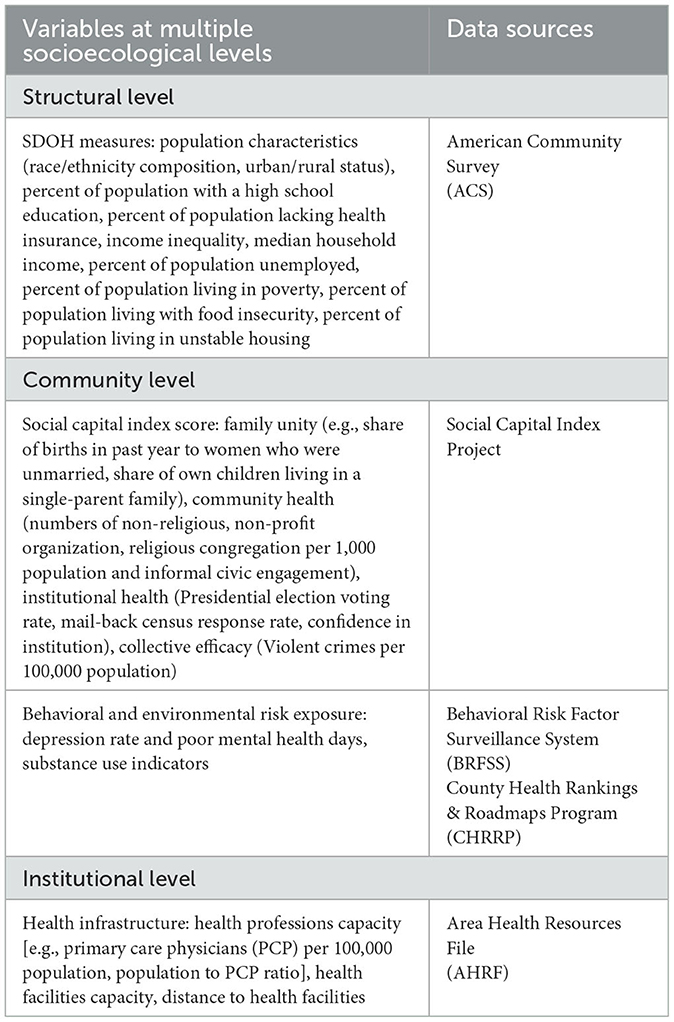
Table 1. Contextual characteristics variables and their data sources.
Given the preliminary nature of this work and the small sample size dictated by time and budget limitations of the 1-year research mechanism, quantitative analyses will focus on obtaining estimates of mental health outcomes and multilevel resilience among Black women living in rural areas and characteristics associated with these outcomes, for use in design of a larger study. Therefore, the specific analysis plan includes (1) Participant characteristics will be presented using counts and percentages for categorical variables and means and standard deviations or medians and inter-quartile ranges (IQR) for continuous variables; (2) Descriptive statistics will be used to evaluate distributions of the measures; (3) Psychometric characteristics of scales will be evaluated using Cronbach's alpha and factor analysis, then compared to published scale psychometrics in Black women if possible. The temporal stability of scales will also be investigated to ensure reliability. These approaches will help assess the utility of the instruments used for future analyses and research in this subpopulation; (4) Exploration and estimation of the associations between primary outcomes (mental health and domestic violence) and secondary outcomes (multilevel resilience), for which correlation analysis and ANOVA for continuous variables will be conducted; and (5) Potential cofounders (e.g., sociodemographic factors) will be evaluated for associations with outcomes using Wilcoxon rank sum or independent-sample t-tests, Spearman or Pearson correlations, and chi-square tests as appropriate. Multivariable analyses will be used to adjust for sociodemographic and other potential covariates (including aggregated county-level contextual characteristics). Cluster effect will be adjusted too in the regression analysis.
Since the proposed study is not a clinical trial or longitudinal study, it is not designed or powered to determine the overall intervention effect nor the causal relation between key variables. It is hard to calculate the power and appropriate sample size due to lack of information of key indicators. However, according to rule of thumb of the minimum sample sizes in absolute Ns, any N > 200 sample offers adequate statistical power for data analysis (79, 80). Therefore, the sample size of 200 in our quantitative study is still acceptable and the preliminary data analysis will help to provide some insights into the promise of a potential resilience-based intervention to inform a future RCT.
Different types of data will be synthesized and triangulated in different forms and from multiple sources, including inputs from our governmental and community partners and the CAB, findings from the qualitative research and quantitative research, published peer-reviewed and gray literature, conference presentations, government reports, and unpublished data. The data triangulation activities will engage various community and health organization stakeholders (e.g., through local data sharing and interpretation forums). The main results/themes will be cataloged using data-plotting worksheets to identify areas of convergence (“syntheses”) or divergence of the study findings from different sources of data (81). For issues with significant divergence from multiple data sources, the CAB and other key stakeholders will be consulted with for further clarification and interpretation. For results that remain inconclusive, the research team will generate research questions or hypotheses for future research.
With assistance from SCCHWA and CAB, the University of South Carolina (USC) research team will draft the final report on policy recommendations based on the outputs of data triangulation. Generally, five key issues will be covered in the policy recommendation report: (1) Risk and vulnerability including the key challenges, especially SDOH challenges among Black women in rural communities during the COVID-19 pandemic and their unique needs in healthcare access and mental health intervention; (2) Resilience including the manifestations of multilevel resilience (individual-, community-, institutional-level) extracted from participants' lived experiences and their coping strategies. (3) Resources including available resources for Black women and community health workers in local communities in response to public health emergencies as well as the types of resources they need but that are not yet available to optimize emergency responses; (4) Community connectedness. Rural communities could be connected with each other and shared resources through statewide health organizations such as SCCHWA. The practice will be discussed regarding resource sharing and collaborations across communities but within a common healthcare system; and (5) Planning and procedures. Recommendations will be provided about how to improve preparedness and readiness in response to public health emergencies through highlighting the take-home messages for policymakers in healthcare systems. The report will be tailored for community health workers as part of toolkit of their resilience development to optimize emergency preparedness and responses in research translation phase.
The report draft will be adapted and finalized through a community charrette among the CAB members. As a community engagement strategy recommended by the National Minority AIDS Council, a charrette is a collaborative planning process that purposefully brings together the expertise of community and academic research partners in order to strengthen partnerships, engage stakeholders, and make decisions regarding translational research (82). Since the launch of the charrette model in 2009 [i.e., originating from a clinical translational science award (CTSA) initiative], this process has been used successfully to launch community-engaged research initiatives across the clinical-translation spectrum (82, 83). This approach can help address specific community problems and provide a context for integrating design and scientific inquiries with local community knowledge (84).
The community charrette will be held in a USC or SCCHWA conference room to assure privacy or conducted in a Zoom platform using the “breakout discussion room” function, depending on the logistics and the COVID-19 situation at the time. CAB members will receive the report draft 2 weeks prior to the charrette and be required to review and provide feedback on its content and structure. The charrette will begin with a review of the charrette goals and an explanation of the procedures for the day. Participants (about 10–15) will be divided into groups of 3–4, and members of the research team will co-lead each of the small group discussions. Each group will discuss the same set of questions that are based on the charrette objective (e.g., feedback on each chapter, strengths and weakness, additional content, etc.), and a co-leader will record the primary points on poster paper. After completing small group discussions, the full group will re-convene, and a representative from each group will present their findings; other members will ask questions and points of clarification, and additional information will be added to the poster paper if needed. The poster paper notes become the primary data source. Field notes will be taken during the course of the charrette by two research staff, with observational and interpretive elements. At the end of the charrette, the CAB will engage in a process of critical reflection regarding the group and develop combined reflection notes based on these conversations.
The report will be further revised and finalized based on the data/notes collected from the community charrette among the CAB members. The USC research team will lead the revision and hold multiple meetings of research staff (from both USC and SCCHWA) when necessary. An iterative process will be used with interactive strategies similar to the community charrettes, whereby poster paper notes become new primary data sources, along with field notes taken during the course of each meeting.
The COVID-19 challenges, responses, and resilience among Black women and their families in rural communities in southern states are critical issues for addressing health disparities and improving population wellness. Aiming to explore lived experience and resilience resources among Black women in rural areas, our study has several strengths in terms of theories, data integration, and research approach. First, the integration of multilevel resilience emphasized in the proposed study will address potential limitations or even hazards of an “individual resilience only” approach (e.g., lack of cultural reflection regarding individualism, victim blaming) and inform effective strategies to equip Black women in rural areas with supportive systems from their communities for boosting resilience. Second, the multiple sources of data collected from key stakeholders (e.g., Black women, community leaders, and community health workers) will delineate a full picture regarding individual, institutional, and social/cultural factors influencing the manifestations and effects of different resilience in the context of the southern states. Our final recommendation report based on data triangulation will inform a comprehensive, concrete, and evidence-based strategies and/or interventions tailored for Black women living in rural areas. Finally, the application of community-based participatory approach will contribute to research/operational capacity-building to paraprofessionals and local health organizations, which will, in turn, enhance resilience, increase access to care, improve public health emergency response, and address the healthcare needs of underserved subpopulations and communities affected by COVID-19 (including long COVID).
This study also has some limitations. First, the participants recruited in the study may not be representative for all the Black women in SC given not all of them can access to the recruitment flyers or have the time to receive the interview or finish the survey questionnaire. With the assistance of the community health workers rooted in the local communities, the research team will advertise our project recruitment via multiple channels and optimize their social network in reaching out the “hidden” group. Second, it is difficult to avoid bias in data collection. For example, the recall bias and socially desirable bias may occur in our in-depth interviews and self-report-based survey. Therefore, the insights and advice from the CAB through each step of the research development, implementation, and interpretation of the findings is critical and helpful. Third, the study sites are not randomly selected from all the Black rural counties in SC with a relatively small sample size. Therefore, the findings may not be generalized to the SC and beyond. Further studies with a larger sample size using random sampling are needed to improve the external validity of the resilience study among Black women in rural areas. Last, the study will not recruit Black men in rural counties therefore there is no “control group” in data analysis. This study design is based on the research aims with a focus on Black women's lived experiences. Future studies can investigate and compare the challenges and resilience by gender.
Despite these limitations, this study will have strong and sustainable public health implications in terms of improving emergency responses and informing capacity-building strategies. Through reviewing our reports, the health officers will get a comprehensive picture of the lived experience, vulnerability and resilience of rural Black women, their families, and local communities; obtain solid, multi-level, and multi-type evidence of the common challenges and typical situations Black women and their families have to face in public health crisis; and develop effective strategies and plans for resource allocations to increase the preparedness of the whole health system for future local or national emergencies.
Identifying potential resilience resources in local communities that may mitigate negative impacts of COVID-19 pandemic will inform capacity building within rural healthcare system. The findings of this proposed study will assist the state agencies and health systems in their efforts in assessing, integrating, and fostering multilevel resilience resources, particularly at the institutional and community levels. In the future, the research team will work with SCCHWA and key stakeholders through a series of meetings and workshops to finalize the assessment tools and develop training materials beyond the toolkit to assist with institutional resilience development and improvement within community health workers. Through long-term ownership by SCCHWA of the assessment instruments and training package, the resilience development will be sustained and incorporated into the capacity building efforts in response to public health emergency now and in the future.
The data collection, analysis, and interpretation will strengthen our collaboration with SCCHWA and other key stakeholders in rural communities. The dissemination of findings will further enhance the academic-government partnership in response to COVID-19 and future public health emergencies and address unique health needs among rural Black women and their families. The key stakeholders will be encouraged to share their lessons and experiences from front-line practice and give insights into their expectations and recommendations so that the research team can collectively develop plans and strategies for building a resilient health system.
In conclusion, findings in the proposed study will provide valuable references in terms of addressing SDOH challenges during the pandemic, fostering resilience, and informing evidence-based decision-making for policymakers. The study will contribute to the development of public health emergency preparedness plans, which can promote the resilience of women, their families, and local communities as well as optimize effective preparedness and response of health systems for rural Black women and their families during infectious disease outbreaks and other public health emergencies.
The studies involving human participants were reviewed and approved by the Institutional Review Boards at the University of South Carolina (Pro00123957). Informed consent will be provided by participants in the focus group discussions, in-depth interviews, and survey. All methods will be conducted in accordance with relevant guidelines and regulations. The patients/participants provided their written informed consent to participate in this study.
SQ and XL conceptualized and designed the study. SQ wrote the first draft. SW and XL participated in reviewing and editing the original proposal. BO reached out and engaged local partners and community organization. SQ and SW secured the funding. All authors critically reviewed and edited the manuscript. All authors contributed to the article and approved the submitted version.
The current study was funded by Centers of Disease Control and Prevention (Grant# 3U48 DP006401-04S7).
The authors thank the engagement of South Carolina Community Health Worker Association in the current study, especially the constructive feedback from Ms. Donna Mack and Ms. Lynda Guess.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. King T, Hewitt B, Crammond B, Sutherland G, Maheen H, Kavanagh A. Reordering gender systems: can COVID-19 lead to improved gender equality and health? Lancet. (2020) 396:80–1. doi: 10.1016/S0140-6736(20)31418-5
2. Fisher AN, Ryan MK. Gender inequalities during COVID-19. Group Process Interg Relati. (2021) 24:237–45. doi: 10.1177/1368430220984248
3. Wenham C, Smith J, Davies SE, Feng H, Grépin KA, Harman S, et al. Women are most affected by pandemics—lessons from past outbreaks. Nature. (2020) 583:194–8. doi: 10.1038/d41586-020-02006-z
4. United Nations. Policy Brief: The Impact of COVID-19 on Women (2020). Available online at: https://www.unwomen.org/sites/default/files/Headquarters/Attachments/Sections/Library/Publications/2020/Policy-brief-The-impact-of-COVID-19-on-women-en.pdf (accessed February 20, 2023).
5. Hupkau C, Petrongolo B. Work, care and gender during the Covid-19 crisis. Fisc Stud. (2020) 41:623–51. doi: 10.1111/1475-5890.12245
6. Schieman S, Badawy PJ, Milkie A, Bierman M. A work-life conflict during the COVID-19 pandemic. Socius. (2021) 7:2378023120982856. doi: 10.1177/2378023120982856
7. Del Boca D, Oggero N, Profeta P, Rossi M. Women's and men's work, housework and childcare, before and during COVID-19. Rev Econ Househ. (2020) 18:1001–17. doi: 10.1007/s11150-020-09502-1
8. Malik S, Naeem K. Impact of COVID-19 Pandemic on Women: Health, Livelihoods & Domestic Violence. Sustainable Development Policy Institute (2020). Available online at: htp://hdl.handle.net/11540/11907 (accessed February 20, 2023).
9. Mojahed A, Brym S, Hense H, Grafe B, Helfferich C, Lindert J, et al. Rapid review on the associations of social and geographical isolation and intimate partner violence: Implications for the ongoing CoViD-19 pandemic. Front Psychiatry. (2021) 12:486. doi: 10.3389/fpsyt.2021.578150
10. Sprague BL, Lowry KP, Miglioretti DL, Alsheik N, Bowles EJ, Tosteson AN, et al. Changes in mammography use by women's characteristics during the first 5 months of the COVID-19 pandemic. J Natl Cancer Inst. (2021) 113:1161–7. doi: 10.1093/jnci/djab045
11. Song H, Bergman A, Chen AT, Ellis D, David G, Friedman AB, et al. Disruptions in preventive care: mammograms during the COVID-19 pandemic. Health Serv Res. (2021) 56:95–101. doi: 10.1111/1475-6773.13596
12. Thayer ZM, Gildner TE. COVID-19-related financial stress associated with higher likelihood of depression among pregnant women living in the United States. Am J Hum Biol. (2021) 33:e23508. doi: 10.1002/ajhb.23508
13. Frederiksen B, Gomez I, Salganicoff A, Ranji U. Coronavirus: A Look at Gender Differences in Awareness Actions. San Francisco, CA: Kaiser Famiy Foundation-Women's Health Policy (2020). Available online at: https://www.kff.org/womens-health-policy/issue-brief/coronavirus-a-look-at-gender-differences-in-awareness-and-actions (accessed March 2, 2023).
14. Lauren BN, Silver ER, Faye AS, Rogers AM, Woo-Baidal JA, Ozanne EM, et al. Predictors of households at risk for food insecurity in the United States during the COVID-19 pandemic. Public Health Nutr. (2021) 24:3929–36. doi: 10.1017/S1368980021000355
15. Bowleg L. We're not all in this together: On COVID-19, intersectionality, and structural inequality. Am. J. Public Health. (2020) 110:917. doi: 10.2105/AJPH.2020.305766
16. Chandler R, Guillaume D, Parker AG, Mack A, Hamilton J, Dorsey J, et al. The impact of COVID-19 among Black women: evaluating perspectives and sources of information. Ethn Health. (2021) 26:80–93. doi: 10.1080/13557858.2020.1841120
17. Adesogan O, Lavner JA, Carter SE, Beach SRH. COVID-19 stress and the health of black Americans in the rural south. Clin Psychol Sci. (2022) 10:1111–28. doi: 10.1177/21677026211049379
18. Brooks JM, Patton C, Maroukel S, Perez AM, Levanda L. The differential impact of COVID-19 on mental health: implications of ethnicity, sexual orientation, and disability status in the United States. Front Psychol. (2022) 13:902094. doi: 10.3389/fpsyg.2022.902094
19. Khanijahani A, Tomassoni L. Socioeconomic and racial segregation and COVID-19: concentrated disadvantage and Black Concentration in Association with COVID-19 Deaths in the USA. J Racial Ethn Health Disparities. (2022) 9:367–75. doi: 10.1007/s40615-021-00965-1
20. Zephyrin L, Radley DC, Getachew Y, Baumgartner JC, Schneider EC. COVID-19 More Prevalent, Deadlier in U.S. Counties With Higher Black Populations: The Commonwealth Fund (2020). Available online at: https://www.commonwealthfundorg/blog/2020/covid-19-more-prevalent-deadlier-us-counties-higher-blackpopulations (accessed February 20, 2023).
21. The COVID Tracking Project. COVID-19 is Affecting Black, Indigenous, Latinx, and Other People of Color the Most: The COVID Tracking Project at the Atlantic. (2020). Available online at: https://covidtracking.com/race (accessed February 12, 2023).
22. Lopez MH, Rainie L, Budiman A. Financial Health Impacts of COVID-19 Vary Widely by Race Ethnicity. Washington, DC: Pew Research Center (2020). Available online at: https://www.pewresearch.org/short-reads/2020/05/05/financial-and-health-impacts-of-covid-19-vary-widely-by-race-and-ethnicity/ (accessed March 3, 2023).
23. Chakrabarti S, Hamlet LC, Kaminsky J, Subramanian S. Association of human mobility restrictions and race/ethnicity–based, sex-based, and income-based factors with inequities in well-being during the COVID-19 pandemic in the United States. JAMA Netw Open. (2021) 4:e217373. doi: 10.1001/jamanetworkopen.2021.7373
24. Moore JX, Langston ME, George V, Coughlin SS. Epidemiology of the 2020 pandemic of COVID-19 in the state of Georgia: inadequate critical care resources and impact after 7 weeks of community spread. J Am Coll Emerg Phys Open. (2020) 1:527–32. doi: 10.1002/emp2.12127
25. Tan SB, deSouza P, Raifman M. Structural racism and COVID-19 in the USA: a county-level empirical analysis. J Racial Ethn Health Disparities. (2022) 9:236–46. doi: 10.1007/s40615-020-00948-8
26. Krouse HJ. COVID-19 and the widening gap in health inequity. Otolaryngol Head Neck Surg. (2020) 163:65–6. doi: 10.1177/0194599820926463
27. Killgore WD, Taylor EC, Cloonan SA, Dailey NS. Psychological resilience during the COVID-19 lockdown. Psychiatry Res. (2020) 291:113216. doi: 10.1016/j.psychres.2020.113216
28. Walsh F. Loss and resilience in the time of COVID-19: meaning making, hope, and transcendence. Fam Process. (2020) 59:898–911. doi: 10.1111/famp.12588
29. Dulin AJ, Dale SK, Earnshaw VA, Fava JL, Mugavero MJ, Napravnik S, et al. Resilience and HIV: a review of the definition and study of resilience. AIDS Care. (2018) 30:S6–17. doi: 10.1080/09540121.2018.1515470
30. American Psychological Association Task Task Force on Resilience Strength in Black Children Adolescents. Resilience in African American Children and Adolescents: A Vision for Optimal Development. Washington, DC: American Psychological Association (2008). Available online at: htp://www.apa.org/pi/cyf/resilience.html (accessed March 1, 2023).
31. Infurna FJ. Utilizing principles of life-span developmental psychology to study the complexities of resilience across the adult life span. Gerontologist. (2021) 61:807–18. doi: 10.1093/geront/gnab086
32. Earnshaw VA, Lang SM, Lippitt M, Jin H, Chaudoir SR, HIV. stigma and physical health symptoms: do social support, adaptive coping, and/or identity centrality act as resilience resources? AIDS Behav. (2015) 19:41–9. doi: 10.1007/s10461-014-0758-3
33. Dale SK, Safren SA. Resilience takes a village: Black women utilize support from their community to foster resilience against multiple adversities. AIDS Care. (2018) 30:S18–26. doi: 10.1080/09540121.2018.1503225
34. Catabay CJ, Stockman JK, Campbell JC, Tsuyuki K. Perceived stress and mental health: the mediating roles of social support and resilience among black women exposed to sexual violence. J Affect Disord. (2019) 259:143–9. doi: 10.1016/j.jad.2019.08.037
35. Bonanno GA. Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events? Am Psychol. (2004) 59:20. doi: 10.1037/0003-066X.59.1.20
36. Bonanno GA, Brewin CR, Kaniasty K, Greca AML. Weighing the costs of disaster: consequences, risks, and resilience in individuals, families, and communities. Psychol Sci Public Int. (2010) 11:1–49. doi: 10.1177/1529100610387086
37. Bonanno GA, Ho SM, Chan JC, Kwong RS, Cheung CK, Wong CP, et al. Psychological resilience and dysfunction among hospitalized survivors of the SARS epidemic in Hong Kong: a latent class approach. Health Psychol. (2008) 27:659. doi: 10.1037/0278-6133.27.5.659
38. Cheng C, Lau H-PB, Chan M-PS. Coping flexibility and psychological adjustment to stressful life changes: a meta-analytic review. Psychol Bull. (2014) 140:1582. doi: 10.1037/a0037913
39. Galatzer-Levy IR, Huang SH, Bonanno GA. Trajectories of resilience and dysfunction following potential trauma: a review and statistical evaluation. Clin Psychol Rev. (2018) 63:41–55. doi: 10.1016/j.cpr.2018.05.008
40. Vannini P, Gagliardi GP, Kuppe M, Dossett ML, Donovan NJ, Gatchel JR, et al. Stress, resilience, and coping strategies in a sample of community-dwelling older adults during COVID-19. J Psychiatr Res. (2021) 138:176–85. doi: 10.1016/j.jpsychires.2021.03.050
41. Wister A, Klasa K, Linkov I. A unified model of resilience and aging: applications to COVID-19. Front Public Health. (2022) 10:865459. doi: 10.3389/fpubh.2022.865459
42. Chen S, Bonanno GA. Psychological adjustment during the global outbreak of COVID-19: a resilience perspective. Psychol Trauma. (2020) 12:S51. doi: 10.1037/tra0000685
43. Zhang J, Yang Z, Wang X, Li J, Dong L, Wang F, et al. The relationship between resilience, anxiety and depression among patients with mild symptoms of COVID-19 in China: a cross-sectional study. J Clin Nurs. (2020) 29:4020–9. doi: 10.1111/jocn.15425
44. Shockley KM, Clark MA, Dodd H, King EB. Work-family strategies during COVID-19: examining gender dynamics among dual-earner couples with young children. J Appl Psychol. (2021) 106:15. doi: 10.1037/apl0000857
45. Lin TK, Law R, Beaman J, Foster DG. The impact of the COVID-19 pandemic on economic security and pregnancy intentions among people at risk of pregnancy. Contraception. (2021) 103:380–5. doi: 10.1016/j.contraception.2021.02.001
46. Goodsmith N, Ijadi-Maghsoodi R, Melendez RM, Dossett EC. Addressing the urgent housing needs of vulnerable women in the era of COVID-19: the Los Angeles County experience. Psychiatr Serv. (2021) 72:349–52. doi: 10.1176/appi.ps.202000318
47. Allen S, Julian Z, Coyne-Beasley T, Erwin PC, Fletcher FE. COVID-19's impact on women: a stakeholder-engagement approach to increase public awareness through virtual town halls. J Public Health Manag Pract. (2020) 26:534–8. doi: 10.1097/PHH.0000000000001249
48. South Carolina Revenue Fiscal Affairs Office. Urban and Rural Population (2010). Available online at: https://rfa.sc.gov/data-research/populationdemographics/census-state-data-center/urban-and-rural-population-2010 (accessed December 12, 2022).
49. Osby L,. South Carolina Ranked 8th Worst in Nation for Health Care: Cost Access Are Issues. The Greenville News (2018). Available online at: https://www.greenvilleonline.com/story/news/2018/08/07/sc-8th-worst-nation-health-care-costand-access-issues/921780002/ (accessed December 12, 2022).
50. US News. South Carolina Rankings Facts (2020). Available online at: https://www.usnews.com/news/best-states/south-carolina (accessed December 12, 2022).
51. South Carolina Department of Health Environment Control. An Epidemiologic Profile of HIV and AIDS in South Carolina (2019). South Carolina. Available online at: https://scdhec.gov/sites/default/files/media/document/2019-Epi-Profile.pdf
52. United Health Foundation. America's Health Rankings Analysis of America's Health Rankings Composite Measure. South Carolina: AmericasHealthRankings.org. (2020). Available online at: https://assets.americashealthrankings.org/app/uploads/ahr-annual-report-2020.pdf
53. Heiney SP, Truman S, Babatunde OA, Felder TM, Eberth JM, Crouch E, et al. Racial and geographic disparities in endocrine therapy adherence among younger breast cancer survivors. Am J Clin Oncol. (2020) 43:504–9. doi: 10.1097/COC.0000000000000696
54. Cunningham JE, Butler WM. Racial disparities in female breast cancer in South Carolina: clinical evidence for a biological basis. Breast Cancer Res Treat. (2004) 88:161–76. doi: 10.1007/s10549-004-0592-9
55. Feng W, Nietert PJ, Adams RJ. Influence of age on racial disparities in stroke admission rates, hospital charges, and outcomes in South Carolina. Stroke. (2009) 40:3096–101. doi: 10.1161/STROKEAHA.109.554535
56. Fleischer NL, Abshire C, Margerison CE, Nitcheva D, Smith MG. The South Carolina multigenerational linked birth dataset: developing social mobility measures across generations to understand racial/ethnic disparities in adverse birth outcomes in the US South. Matern Child Health J. (2019) 23:787–801. doi: 10.1007/s10995-018-02695-z
57. Wende ME, Liu J, Mclain AC, Wilcox S. Gestational weight gain disparities in South Carolina: temporal trends, 2004-2015. Paediatr Perinat Epidemiol. (2021) 35:37–46. doi: 10.1111/ppe.12706
58. Vengaloor Thomas T, Gandhi S, Bhanat E, Krishna K, Robinson W, Ridgway M, et al. An analysis of the racial disparities among cervical cancer patients treated at an Academic Medical Center in the Southeastern United States. Cureus. (2021) 13:e13296. doi: 10.7759/cureus.13296
59. Adams SA, Fleming A, Brandt HM, Hurley D, Bolick-Aldrich S, Bond SM, et al. Racial disparities in cervical cancer mortality in an African American European American cohort in South Carolina. J South Carolina Med Assoc (1975). (2009) 105:237–44.
60. Sutton SE, Kemp SP. Integrating social science and design inquiry through interdisciplinary design charrettes: an approach to participatory community problem solving. Am J Community Psychol. (2006) 38:51–62. doi: 10.1007/s10464-006-9065-0
62. Corbin J, Strauss A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 3rd ed. Los Angeles, CA: Sage Publications Inc. (2008) p. 358. doi: 10.4135/9781452230153
63. Kroenke K, Spitzer RL, Williams JB, Löwe B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiatry. (2010) 32:345–59. doi: 10.1016/j.genhosppsych.2010.03.006
64. Patrick S, Connick P. Psychometric properties of the PHQ-9 depression scale in people with multiple sclerosis: a systematic review. PLoS ONE. (2019) 14:e0197943. doi: 10.1371/journal.pone.0197943
65. Spitzer RL, Kroenke K, Williams JB, Löwe B, A. brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
66. Löwe B, Decker O, Müller S, Brähler E, Schellberg D, Herzog W, et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. (2008) 46:266–74. doi: 10.1097/MLR.0b013e318160d093
67. Prins A, Bovin M, Kimerling R, Kaloupek D, Marx B, Pless Kaiser A, et al. The primary care PTSD screen for DSM-5 (PC-PTSD-5). Natl Cent PTSD. (2015) 5:1–3.
68. Prins A, Bovin MJ, Smolenski DJ, Marx BP, Kimerling R, Jenkins-Guarnieri MA, et al. The primary care PTSD screen for DSM-5 (PC-PTSD-5): development and evaluation within a veteran primary care sample. J Gen Intern Med. (2016) 31:1206–11. doi: 10.1007/s11606-016-3703-5
69. Sherin KM, Sinacore JM Li X-Q, Zitter RE, Shakil A, HITS. a short domestic violence screening tool for use in a family practice setting. Fam Med. (1998) 30:508–12.
70. Rabin RF, Jennings JM, Campbell JC, Bair-Merritt MH. Intimate partner violence screening tools: a systematic review. Am J Prev Med. (2009) 36:439–45. e4. doi: 10.1016/j.amepre.2009.01.024
71. Connor KM, Davidson JR. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress Anxiety. (2003) 18:76–82. doi: 10.1002/da.10113
72. Carver CS. You want to measure coping but your protocol'too long: consider the brief cope. Int J Behav Med. (1997) 4:92–100. doi: 10.1207/s15327558ijbm0401_6
73. Marsh HW, Richards GE. Tennessee Self Concept Scale: reliability, internal structure, and construct validity. J Pers Soc Psychol. (1988) 55:612. doi: 10.1037/0022-3514.55.4.612
74. Qiao S, Li X, Zhou Y, Shen Z, Tang Z. Interpersonal factors associated with HIV partner disclosure among HIV-infected people in China. AIDS Care. (2016) 28:37–43. doi: 10.1080/09540121.2016.1146397
75. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. (1988) 52:30–41. doi: 10.1207/s15327752jpa5201_2
76. Barasa E, Mbau R, Gilson L. What is resilience and how can it be nurtured? A systematic review of empirical literature on organizational resilience. Int J Health Policy Manag. (2018) 7:491. doi: 10.15171/ijhpm.2018.06
77. United States Census Bureau. American Community Survey (ACS) (2017). Available online at: https://census.gov/programs-surveys/acs/news/data-releases.html#.html (accessed January 25, 2018).
78. United States Congress Joint Economic Committee. The Geography of Social Capital in America (2018). Available online at: https://www.jec.senate.gov/public/index.cfm/republicans/2018/4/the-geography-of-social-capital-in-america (accessed December 12, 2022).
79. Hoe SL. Issues and procedures in adopting structural equation modelling technique. J Quant Methods. (2008) 3:76.
80. Kyriazos TA. Applied psychometrics: sample size and sample power considerations in factor analysis (EFA, CFA) and SEM in general. Psychology. (2018) 9:2207. doi: 10.4236/psych.2018.98126
81. Rutherford GW, McFarland W, Spindler H, White K, Patel SV, Aberle-Grasse J, et al. Public health triangulation: approach and application to synthesizing data to understand national and local HIV epidemics. BMC Public Health. (2010) 10:1–10. doi: 10.1186/1471-2458-10-447
82. Samuel CA, Lightfoot AF, Schaal J, Yongue C, Black K, Ellis K, et al. Establishing new community-based participatory research partnerships using the community-based participatory research Charrette model: lessons from the Cancer health accountability for managing pain and symptoms study. Progr Commun Health Partners. (2018) 12:89–99. doi: 10.1353/cpr.2018.0010
83. Black KZ, Hardy CY, De Marco M, Ammerman AS, Corbie-Smith G, Council B, et al. Beyond incentives for involvement to compensation for consultants: increasing equity in CBPR approaches. Progr n Commun Health Partners. (2013) 7:263. doi: 10.1353/cpr.2013.0040
Keywords: COIVD-19, Black or African American, women, rural health, psychological resilience, community-based participatory research
Citation: Qiao S, Wilcox S, Olatosi B and Li X (2023) COVID-19 challenges, responses, and resilience among rural Black women: a study protocol. Front. Public Health 11:1156717. doi: 10.3389/fpubh.2023.1156717
Received: 01 February 2023; Accepted: 12 May 2023;
Published: 02 June 2023.
Edited by:
Mohammadreza Shalbafan, Iran University of Medical Sciences, IranReviewed by:
Monica Georgiana Brinzac, Babeş-Bolyai University, RomaniaCopyright © 2023 Qiao, Wilcox, Olatosi and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shan Qiao, c2hhbnFpYW9AbWFpbGJveC5zYy5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.