 Elshaday Bekele Werke1*
Elshaday Bekele Werke1* Zewdu Shewangizaw Weret2
Zewdu Shewangizaw Weret2- 1Department of Public Health, School of Public Health, College of Medicine and Health Science, Dilla University, Dilla, Ethiopia
- 2Department of Psychiatry, Menelk II Medical and Health Science College, Kotebe University of Education, Addis Ababa, Ethiopia
Background: By its very nature, the nursing profession involves a lot of stress. Working in this field includes interacting with individuals who are already under a great deal of stress. Workplace stress affects the quality of services provided and also causes staff burnout, departure, and absenteeism.
Objective: This study is to determine occupational stress and associated factors among nurses working at public hospitals, Addis Ababa, Ethiopia, 2022.
Materials and methods: An institutional based cross sectional study was conducted among 422 nurses working at public hospitals from March 1 to April 1/2022. Simple random sampling technique was used to select public hospitals. The calculated sample size was allocated proportionally to each hospital based on the number of nurses. Finally, systematic sampling method was used to approach the study participants. The data was collected by using a self-administered structured questionnaire (Expanded Nursing Stress Scale). The collected data was entered by Epi-data version 3.1 and analyzed by SPSS version 23. Descriptive analysis such as frequency distribution and measure of central tendency and variability (mean and standard deviation) was computed to describe variables of the study. Binary logistic regression was used to assess associations between dependent and independent variables. The degree of associations was interpreted using odds ratio (OR) and 95% confidence interval (CI) and statically significance at value of p < 0.05. The result was presented using text, tables, and graphs.
Result: The study finding showed that 198 (47.8%) of nurses were occupationally stressful. Factors significantly associated with occupational stress among nurses were having children (no: AOR = 0.46, 95% CI: 0.22, 0.96) and work shift (rotating: AOR = 2.89, 95% CI: 1.87, 4.45).
Conclusion: In this study, job stress affected over half of the nurses. The presence of children and respondents’ work shifts were personal characteristics that were significantly linked to job stress. Therefore based on this result the government policy makers, different stakeholders and hospitals need to collaborate to reduce nurses job related stress.
1. Introduction
A common way to define stress is as a feeling of being overburdened, wound up tight, tense, and concerned (1). It is a disruptive condition that develops in reaction to harmful effects from the internal or external settings (2).
Occupational stress is defined by the National Institute for Occupational Safety and Health (NIOSH) as “the negative physical and emotional reactions that occur when the requirements of the job do not match the worker’s talents, resources, or needs” (3). Occupational stress is sometimes referred to as job stress and/or work-related stress (WRS) in an organizational environment. In organizations, both phrases are frequently used interchangeably, but their meanings are the same (4).
One of the most significant sources of occupational stress is the workplace (5). Stress at work is a topic that psychologists, counselors, and employers are all quite concerned about (6).
In general, nursing is seen as a difficult and stressful career (7). Numerous studies have shown that working in nursing is stressful, which can have an adverse effect on one’s physical and mental health as well as their professional performance (8).
Occupational stress can have a number of detrimental effects on both the individual and the company. Poor physical and mental health as well as organizational costs was documented at the individual and organizational levels (9). Additionally, stress has a cost in terms of one’s health, wellbeing, and job satisfaction. It also has a cost for companies in terms of absenteeism and turnover, which may have an effect on the standard of patient care (10).
In organizations, stress has become a bigger issue over time (11). Stress varies in intensity depending on the circumstance and the person, and if it is not well managed, it can prevent people and organizations from reaching their objectives. The consequences of stress on medical workers, and nurses in particular, have drawn a lot of attention (12). Due to the nature of their occupation and the system in which they operate, nurses are perceived to be under more stress than the majority of individuals (13). The first of 40 stressful professions identified by the National Association of Safety Professionals is nursing (14).
In any healthcare facility, nurses make up the majority of the workforce and play a crucial role in patient care. Nurses provide direct care, and providing care is an interpersonal activity characterized by expert nursing, interpersonal sensitivity, and close connections, as well as by effective communication and the use of professional knowledge and abilities. Nursing staff members are occasionally asked to work lengthy hours without getting enough rest (15, 16). Consequently, the nursing profession is highly stressful. Furthermore, the occupation requires interacting with individuals who are under a great deal of stress themselves. Patients can occasionally be challenging, scared, or angry, and nurses may find themselves responding with an increasing irritation and anger that may result in quitting the profession (17, 18).
The major causes of stress among nurses at work include working shifts, long hours, a lack of control, poor relationships with coworkers, low pay, and unfavorable working conditions (19).
According to research, nurses who experience high levels of job-related stress and physical and mental health issues are more likely to quit their jobs, clash with coworkers, experience intense displacement, suffer from poor health and be unable to complete tasks, exhibit vulnerabilities in professional communication, and, as a result, provide lower-quality care and become dissatisfied with their careers. The influence could also have detrimental effects on patient care, such as medication errors and inadequate care for those receiving it (20).
Depending on research carried out in several nations, stress in particular in the nursing profession has been a significant global issue. A research conducted among staff members of a health authority in the United Kingdom revealed that nurses are under the most pressure out of all medical professionals (21). According to a research done in India, 87.4% of Indian nurses reported feeling stressed (22). Based on a research done in the Greater Accra Region of Ghana, the number of hours that nurses work, their financial situation, and patient deaths are all sources of stress (23).
In comparison to other African nations, Ethiopia has one of the lowest ratios of health personnel to population. One healthcare professional was assigned to every 4,050 people, according to a report from the World Health Organization. Resources shortages, macroeconomic problems, and governmental factors are the causes of Ethiopia’s human resource crisis (24, 25). However, the final report of the Health Sector Development Program (HSDP) IV in Ethiopia indicated that there was a lack of nursing staff on a national level, with a nurse to population ratio of 1:3,870 (26). In Ethiopia, a study conducted in the Jima Zone in the southwest of the country revealed an average total job-related stress level of 58.46 ± 12.62, while in the East Gojjam Zone Public hospitals in the northwest, 57.3% of nurses reported experiencing occupational stress (15, 18).
The recent acceleration in the rate of COVID-19’s spread resulted in a heavy workload, physical exhaustion, a high risk of infection, and ethical conflicts regarding decisions about which patients should be given priority. These factors led to significant psychological stress in healthcare professionals. Given that they spend more time with COVID-19 patients than any other healthcare provider, nurses are disproportionately impacted by the pandemic (27, 28).
The findings of this study will provide information on the prevalence and associated factors of occupational stress to nurses, hospital managers, and health policymakers. It also help health care institutions; particularly hospitals to recognize factors related to stress & help them to take corrective measures in attempt to create conducive environment and to improve the health status of their employees as well as efficiency and quality of care. In addition to this the data gathered will aid in the development of appropriate interventions for stress reduction strategies and programs. Furthermore, this research will create knowledge that may be used as input for future research in the same field.
Although study on the topic of work-related stress among nurses in developed countries has been documented, there is currently little data backed by studies conducted in developing nations, such as Ethiopia. Thus, this study determines the prevalence of stress among nurses in the study area as well as its contributing elements.
2. Materials and methods
2.1. Study setting and design
This study was conducted in Addis Ababa which is the capital city of Ethiopia. It is located at the center of the country with an estimated area of 527 square kilometers (29). Currently, Addis Ababa has 12 state run and more than 40 private hospitals (29). Five public hospitals namely, Menelik II, St. Paul, St. Peter, Yekatit 12 and Zewditu memorial hospitals was included in this study. The study was done from March 1 to April 1/2022. Institution based cross sectional study was conducted.
2.2. Source population and study population
The source population was nurses who were working at public hospitals of Addis Ababa and the study population was nurses who were working at selected public hospitals of Addis Ababa.
2.3. Inclusion criteria and exclusion criteria
Nurses who had experience of working for at least 6 months at public hospitals were included whereas nurses who were ill or on leave (annual, maternal, or sick) during data collection period were excluded.
2.4. Sample size and sampling technique
A single population proportion calculation was used to get the sample size. The previous research’s 49.2% prevalence rate of occupational stress is used to compute the sample size (30). Five hospitals were selected by simple random sampling technique. The calculated sample size was allocated proportionally to each hospital based on the number of nurses. Finally, simple random sampling method was used to approach the study participants.
2.5. Data collection tools
Data was collected using self-administered structured questionnaire. There are three sections in the questionnaire. Socio-demographic information, working place data, and Modified Expanded Nursing Stress Scale make up Parts 1 through 3. An instrument for measuring work-related stress is the Expanded Nursing Stress Scale (31). The ENSS measures occupational stress by using 54 items over eight subscales. The response options on the ENSS questionnaire, which is often created using a likert scale format, typically suggest that stress levels are (1 = never stressful, 2 = occasionally stressful, 3 = frequently stressful, and 4 = always stressful). The responder agreed that the scenario was stressful to a greater extent the higher the score. An overall chronbach’s alpha score of 0.9 indicates that the instrument is reliable (31).
2.6. Data collection procedure
Five BSc nurses one for each hospital as data collector and two BSc nurses as supervisor working outside the selected hospitals was recruited. On the day of data collection, the data collectors explained the purpose of the study to the participants before data collection. Then self-administered structure questioner was distributed by giving appropriate instruction to assist respondents how to fill the questions. The study was done from March 1 to April 1/2022.
2.7. Data quality control
A pre-test was conducted using 5% of the sample size among nurses working at Ras Desta Damtew hospital 2 weeks prior to data collection and necessary amendment was made. To ensure quality of data training was given for data collectors and supervisors on data collection tool and data collection procedure. Data completeness was checked by data collectors and principal investigator.
2.8. Data processing and analysis
Data was coded, cleaned and entered to Epi-data version 3.1 and exported to Statistical Package for Social Science (SPSS) version 23 for analysis. Descriptive analysis such as frequency distribution and measure of central tendency and variability (mean and standard deviation) was computed to describe variables of the study. Binary logistic regression was used to assess associations between dependent and independent variables. The degree of associations was interpreted using odds ratio (OR) and 95% confidence interval (CI) and statically significance at value of p < 0.05. The result was presented using text, tables, and graphs.
3. Results
3.1. Socio demographic characteristics of the respondents
This study had a response rate of 414 (98.1%). In all, 178 (43%) men and 236 (57%) women took part in the study. The respondents’ average age was 27.85 ± 4.28 years. According to this study, 350 (84.5%) of individuals had a BSc degree. Nurses with 5 to 10 years of professional experience made up more than 50% of the participants. Additionally, 179 (43.2%) respondents had children, while 190 (45.9%) respondents were married (Table 1).

Table 1. Socio-demographic characteristics of nurses working at public hospitals of Addis Ababa, Ethiopia, 2022 (N = 414).
3.2. Work place characteristics of the respondents
Majority of participants 239 (57.7%) reported working shift of them were rotating. Most of participants 250 (60.4%) had a daily work schedule of no more than 8 h (Table 2).
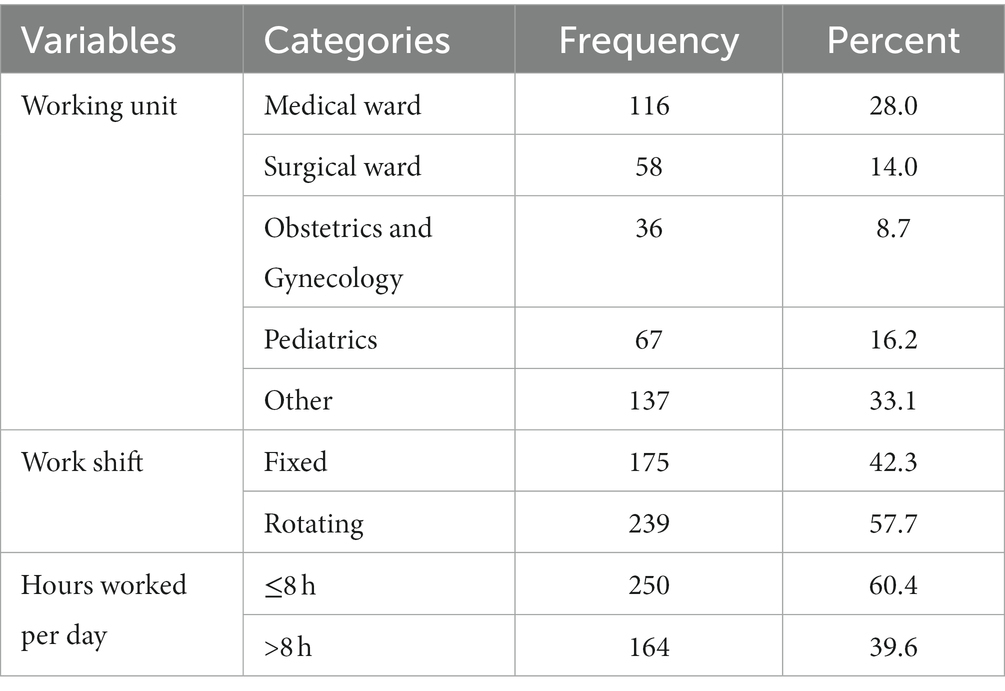
Table 2. Work place characteristics of nurses working at public hospitals of Addis Ababa, Ethiopia, 2022 (N = 414).
3.3. Prevalence of occupational stress among nurses
In order to assess the prevalence of occupational stress, participants who scored below the mean value were labeled as “Not stressed,” while those who scored the mean value or higher were categorized as “Stressed.” As a result, 198 (47.8%) of nurses reported having occupational stress (Figure 1).
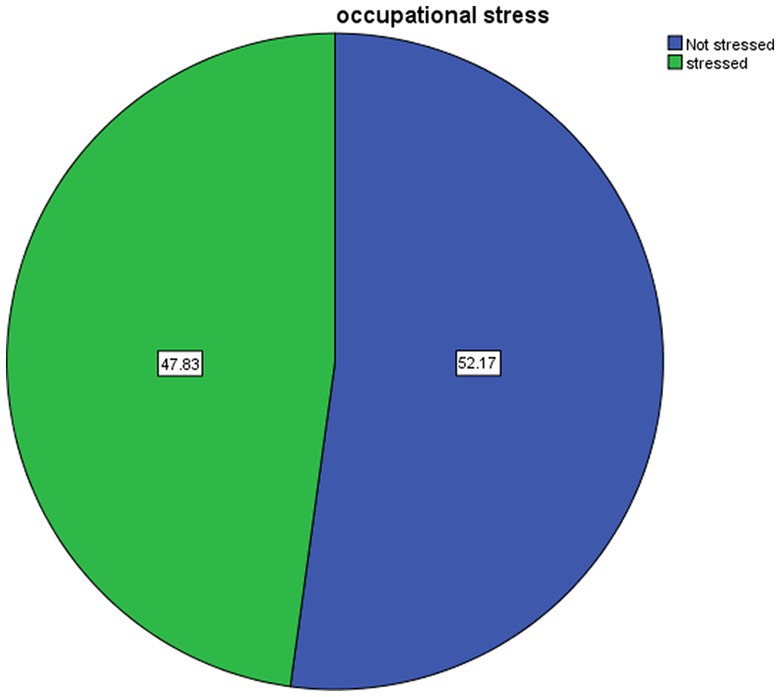
Figure 1. Prevalence of occupational stress among nurses working at Addis Ababa public hospitals, Ethiopia, 2022.
The mean score of the occupational stress subscales was computed. According to this research, the least stressful aspects of nurses’ jobs were problems with peers while the most stressful aspects were death and dying, uncertainty about treatment, and conflict with physician (Table 3).
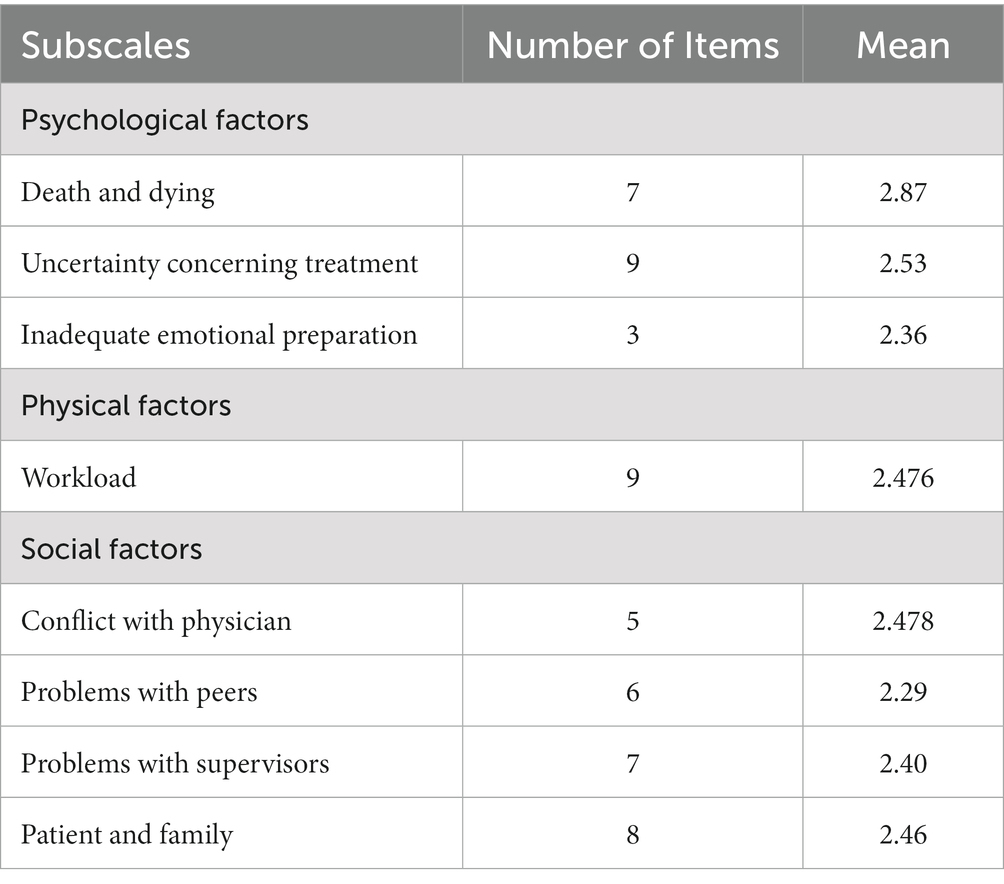
Table 3. Mean score of response of nurse to ENSS in Addis Ababa public hospitals, Ethiopia, 2022 (N = 414).
3.4. Factors associated with occupational stress
The relationship between the independent variables and the dependent variable was examined using binary logistic regression. The multivariate analysis included all independent variables with p-values less than 0.25 in the bivariate analysis, and p-values less than 0.05 in multiple logistic regressions were regarded as significant. The results of the multivariate analysis showed that working shifts and having children were both strongly related to job stress.
According to the findings, nurses without children were 54% less anxious than nurses with children (AOR: 0.46, 95% CI: 0.22, 0.96). Working rotating shifts increased respondents’ risk of occupational stress by 2.8 times compared to working fixed shifts (AOR = 2.89, 95% CI: 1.87, 4.45) (Tables 4, 5).
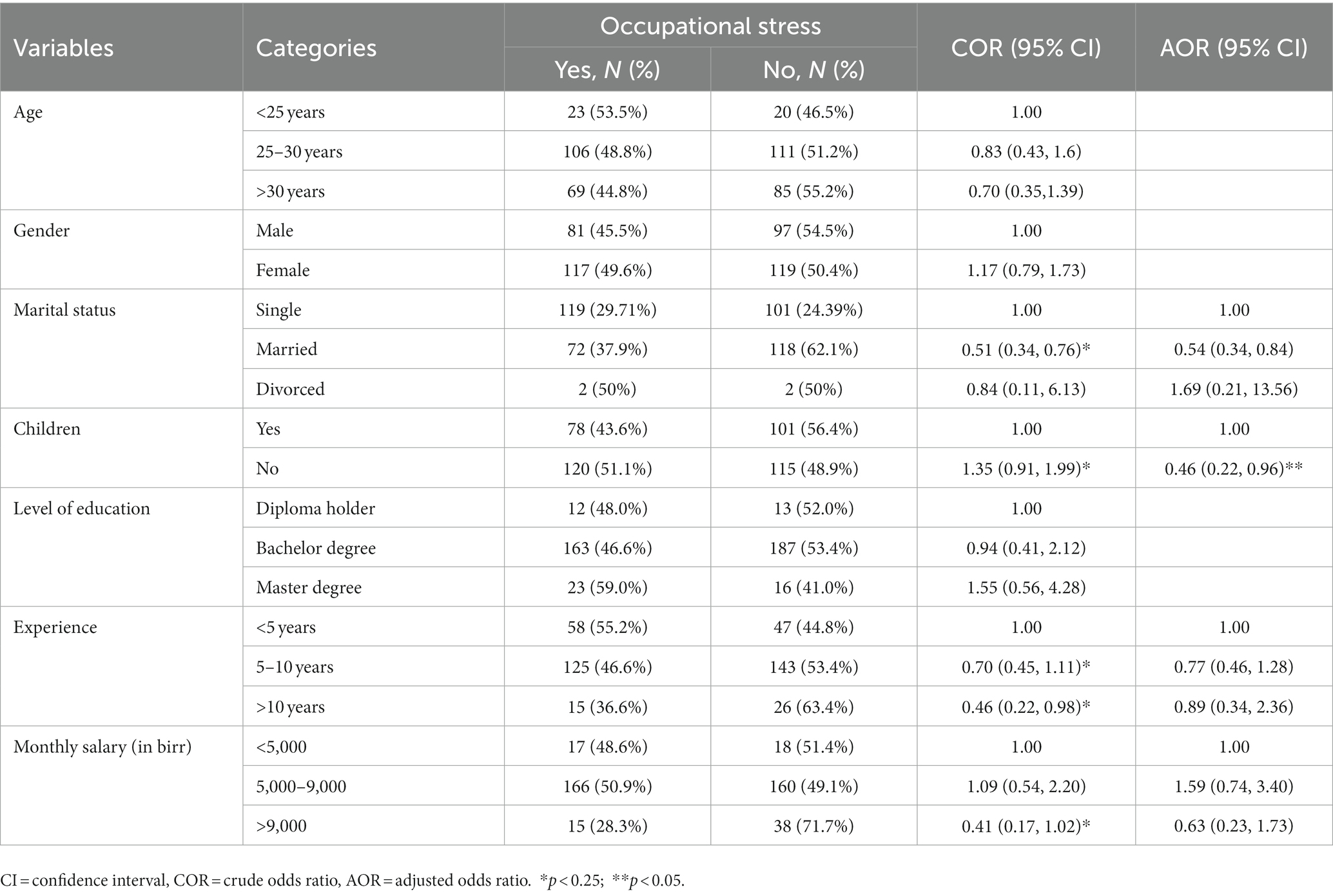
Table 4. Socio demographic results of bivariate and multivariate binary logistic regression of factors associated with occupational stress among nurses working at public hospitals of Addis Ababa, Ethiopia, 2022 (N = 414).
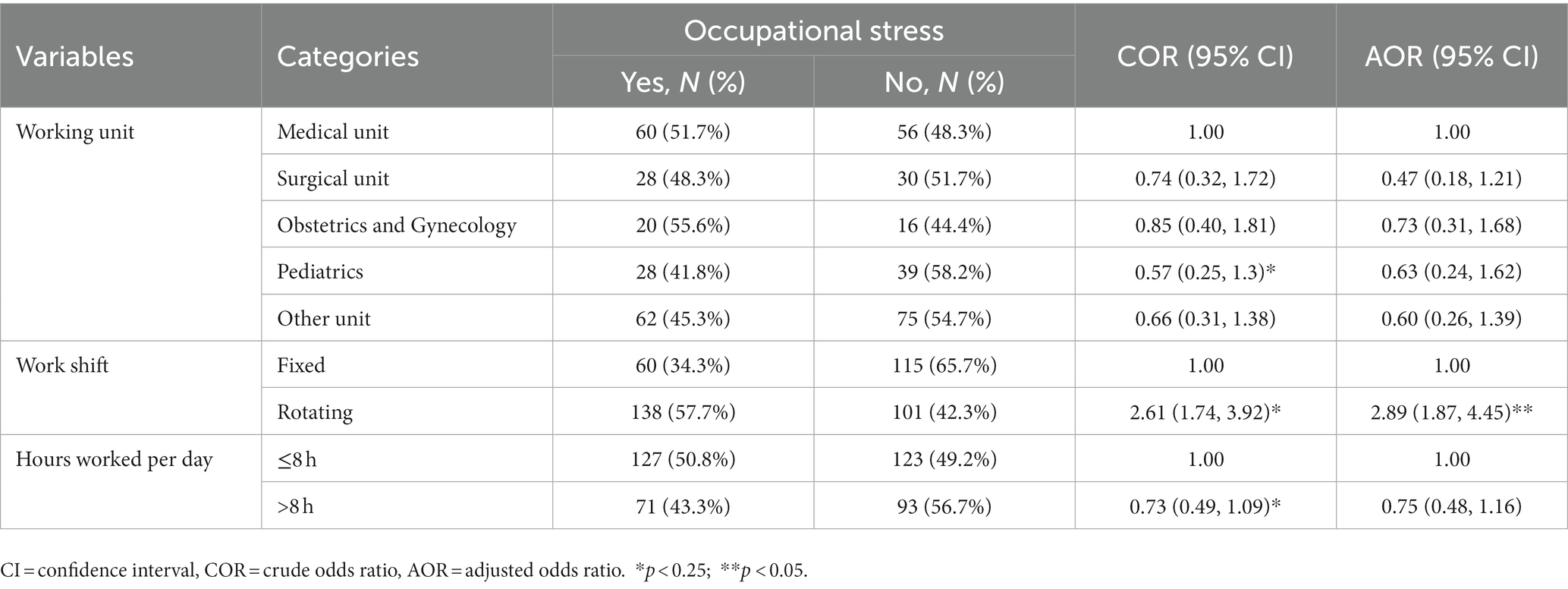
Table 5. Work place results of bivariate and multivariate binary logistic regression of factors associated with occupational stress among nurses working at public hospitals of Addis Ababa, Ethiopia, 2022 (N = 414).
4. Discussion
The prevalence of occupational stress among nurses was found to be 47.8% in this study, which is higher than the studies conducted in Isfahan, Iran, which found that the prevalence of stress was 34.9% (32) and Addis Ababa, Ethiopia, which found that the prevalence of occupational stress among nurses was 37.8% (33). The difference could be a result of the different tools used and the sample size, but another explanation could be that Isfahan, Iran, had stronger occupational health and safety practices implemented.
However, the results of this study are less significant than those of earlier research done in Delhi, which found that 87.4% of nurses experienced job-related stress, and in Jima Zone South West Ethiopia, which found that the average level of job-related stress was 58.46 ± 12.62 (15, 34). When compared to the study conducted in Jima, this may be related to sample size, however in Delhi, the discrepancy may be caused by study tools and the study location.
According to this study, the four main sources of stress for nurses are “death and dying,” “uncertainty regarding patient treatment,” “conflict with physician,” and “work load.” The biggest source of stress, in respondent’s opinions, was death and dying. The current study found that dealing with death and dying situations is a significant source of stress, which is consistent with studies conducted in Sudan, where dealing with death and dying situations had the highest mean scores of ENSS, mean = 2.23, Standard deviation = 0.56, and in Jima, where the highest stressful condition that nurses rated as always stressful was the death and dying of a patient with 62.94%, followed by uncertainty regarding patient treatment with 57.72% (15, 35). The study participants’ cultural and humanitarian sympathy may be the cause of their emotional problems with relation to the patient’s death or dying.
Uncertainty regarding the treatment subscale was the second cause of work-related stress in this study. Similar findings were found in a research conducted among 135 ICU nurses at the Children’s University Hospital at El-Shatby (Egypt), which demonstrated “death and dying” followed, by uncertainty concerning the treatment (36). This could be as a result of a lack of knowledge, experience, or expertise in dealing with unforeseen and challenging issues.
The third source of stress had a mean score of 2.47 and was conflict with physician subscale. Conflict with physician was identified as a source of work-related stress in studies conducted in Spain, which is consistent with this finding (37). This may be due to a lack of relationships, communication, and cooperation.
Many of socio-demographic and workplace factors in this study had no statistically significant relationships with overall occupational stress. This may be the tool’s strongest attribute. In multivariate logistic regression, the only significant predictors of occupational stress were having children and working a shift.
According to this study, there is a significant association between having children and workplace stress. Nurses who did not have children reported being 54% less stressed than those who did (AOR: 0.46, 95% CI: 0.22, 0.96). This may be because raising children increases the workload for these nurses. This study is in line with one done in Kampala, Uganda, which found that nurses in Ugandan hospitals deal with a fair amount of occupational stress. Additionally, the findings revealed that nurses without children experienced much less occupational stress than those with children (38).
A significant relationship between work shift and stress at work was also discovered in this study; rotating shift nurses reported higher levels of stress than fixed shift nurses (AOR = 2.89, 95% CI: 1.87, 4.45). This result was in line with a study conducted in Addis Ababa, which found that nurses working rotational shifts experienced higher levels of stress than those working fixed shifts (39). Additionally, this result was consistent with study conducted in Egypt that found the work shift was the strongest predictor of nurses’ stress (36) and that revealed nurses working the rotating shift were more stressed than those who worked the morning shift (40).
5. Limitations of the study
Since stress is mainly subjective and psychological, the qualitative approach would provide rich and meaningful information about the nurses’ experiences with stress and related concepts.
6. Conclusion
In this study, about half of the nurses reported experiencing occupational stress. The presence of children and respondents’ work shifts were personal characteristics that were significantly linked to job stress. The biggest drivers of work-related stress for nurses were death and dying, treatment uncertainty, conflict with physician, and problem with peers.
According to these findings, Ministry of Health and Addis Ababa Health Bureau and Nursing stake holders should collaborate to design stress management programs for nurses that include the proactive identification and evaluation of stressors in work areas. All hospitals and nursing administrators must take responsibility for the health and well-being of their staff by reducing stressful situations. They should reschedule shifts and recruit adequate nurses, decreasing workloads. Furthermore, support systems such as counseling services and self-help groups should be made available to nurses.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical clearance was obtained from Addis Ababa Health Bureau before data collection. Supportive letter was obtained from Kotebe University of Education, Menelik II College of Medical and Health Science. Oral consent was obtained from each study participants during data collection. Right was given to study participants to refuse, stop, or withdraw from the interview at any time. Confidentiality was maintained throughout the study.
Author contributions
EW wrote the proposal, participated in data collection, analyzed the data, wrote the manuscript, and approved the manuscript for publication. ZW reviewed and approved the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
First, we would like to thank the hospitals where the study conducted. In addition to this our heartfelt thanks goes to data collectors, supervisors, and participants. Furthermore, we would like to extend our deepest gratitude to our friends and families for their unconditional love and support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AOR, Adjusted odd ratio; CI, Confidence Interval; COR, Crude odd ratio; COVID-19, Coronavirus disease 2019; ENSS, Expanded nursing stress scale; HSDP, Health sector development program; ICU, Intensive care unit; NIOSH, National institute for occupational safety and health; OR, Odd ratio; SPSS, Statistical package of social sciences; SD, Standard deviation; WRS, Work related stress.
References
1. Australian Psychological Association (2013). APS-EQIP-information sheets-stress. https://psychology.org.au/getmedia/2054e564-49e7-4b6a-beba-e6f6e156d1ca/2013-aps-annual-report.pdf
2. Smeltzer, SC, Bare, BG, Hinkle, JL, and Cheever, KH. (2010). Homeostasis, Stress, and Adaptation. Brunner & Suddarth’s textbook of medical-surgical nursing. 12 Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 78–95.
3. Centers for Diseases Control Prevention (2008). Exposur to stress: occupational hazards in hospitals. National Institute for Occupational Safety and Health.
4. AbuAIRub, RF. Job stress, job performance, and social support among hospital nurses. J Nurs Scholarsh. (2004) 36:73–8. doi: 10.1111/j.1547-5069.2004.04016.x
5. Moustaka, E, and Constantinidis, T. Sources and effects of work-related stress in nursing. Health Sci J. (2010) 4:210–6.
7. Rogers, B. Occupational and environmental health nursing: Concepts and practice. Elsevier Health Sciences. (2003).
8. Al-Hawajreh, KM. (2013). Exploring the relationship between occupational stress and organizational commitment among nurses in selected jordanian hospitals. Dirasat: Administrative Sciences. 40: 127–43.
9. Hui, W, Chi, T-S, and Li Chen, LW. Occupational stress among hospital nurses : cross-sectional survey. J Adv Nurs. (2010) 66:627–34. doi: 10.1111/j.1365-2648.2009.05203.x
10. Beheshtifar, M, and Nazarian, R. Role of occupational stress in organizations. Interdiscip J Contemp Res Bus. (2013) 4:648–57.
11. Bashir, U. Impact of stress on employees job performance. A study on banking sector of Pakistan. IJMS. (2010) 2:122–6. doi: 10.5539/ijms.v2n1p122
12. Gupta, S. (2016). Why America’s nurses are burning out. Stress and fatigue top the list of on-the-job health concerns. So what can be done? Everyday Health. Available at: https://www.everydayhealth.com/news/why
13. Burke, M. Managing work-related stress in the district nursing workplace. Br J Commun Nurs. (2013) 18:535–8. doi: 10.12968/bjcn.2013.18.11.535
14. Mojdeh, S, Sabet, B, Doosti Irani, M, Hajian, E, and Malbousizadeh, M. Relationship of nurse’s stress with environmental-occupational factors. Iran J Nurs Midwifery Res. (2008) 13: 5–9.
15. Dagget, T, Molla, A, and Belachew, T. Job related stress among nurses working in Jimma zone public hospitals, South West Ethiopia: a cross sectional study. BMC Nurs. (2016) 15:1–10. doi: 10.1186/s12912-0160158-2
16. Sarafis, P, Rousaki, E, Tsounis, A, Malliarou, M, Lahana, L, and Bamidis, P. The impact of occupational stress on nurses’ caring behaviors and their health related quality of life. BMC Nurs. (2016) 15:56–9. doi: 10.1186/s12912-016-0178-y
17. Mccarthy, VJC, Power, S, and Greiner, BA. (2018). Perceived occupational stress in nurses working in. Oxfordjournals Available at: https://academic.oup.com/occmed/articleabstract/60/8/604/1607289 [Accessed October 1, 2010].
18. Kassa, DH, Afenigus, AD, Meteku, BT, Mengisitie, BL, and Telila, BD. Assessment of occupational stress and associated factors among nurses in East Gojjam Zone Public Hospitals Northwest Ethiopia, 2016. Sci Publ Gr. (2017) 6:43–8. doi: 10.11648/j.cmr.20170602.13
19. Toh, SG, Ang, E, and Devi, MK. Systematic review on the relationship between the nursing shortage and job satisfaction, stress and burnout levels among nurses in oncology/haematology settings. Int J Evid Based Healthc. (2012) 10:126–41. doi: 10.1111/j.1744-1609.2012.00271.x
20. Valiei, S, Rezaei, M, and Rezaei, K. The relationship between personality characteristics and Nursing occupational stress. Iran J Psychiatr Nurs. (2013) 3:27–34.
21. Executive, S. (2017). Work-related stress, depression or anxiety statistics in Great Britain 2017. Available at: www.hse.gov.uk/statistics/.
22. Mohite, N, Shinde, M, and Gulavani, A. Occupational stress among nurses working at selected tertiary care hospitals. Int J Sci Res. (2014) 3:999–1005.
23. Kyreaa, A. Causes of stress among nurses in the Greater Accra region. Int J Res Soc Sci. (2014) 3:3–4.
24. Asegid, A, Belachew, T, and Yimam, E. Factors influencing job satisfaction and anticipated turnover among nurses in Sidama zone public health facilities. South Ethiopia Nurs Res Pract. (2014) 2014:1–26. doi: 10.1155/2014/909768
25. Dr. Janice Rider Ellis rn phd anef ms (n.d.). Celia love hart. 344Nursing in Today’s world, 10 Edition.
26. FDR (2014). Health FDR of EM of, 2014/15 H. Health sector developmental program. Available at: http:www.google.com.
27. Liu, Z, Han, B, Jiang, R, Huang, Y, Ma, C, Wen, J, et al. Mental health status of doctors and nurses during COVID-19 epidemics in China. BMC Psychiatry. (2020) 20:2–9. doi: 10.1186/s12888-020-02838-z
28. Pappa, S, Ntella, V, Giannakas, T, Giannakoulis, VG, Papoutsi, E, and Katsaounou, P. Prevalence of depression, anxiety, and insomnia among health care workers during COVID-19 pandemic: a systematic review and meta-analysis. Brian Behav Immun. (2020) 88:901–7. doi: 10.1016/j.bbi.2020.05.026
29. Projected population of Ethiopia (2019). https://worldpopulationreview.com/countries/ethiopia-population
30. Amsalu, N. Assessment of job related stress and its peredictors among nurses working in government hospitals of west Shoa zone. Ethiopia: Oromia Region (2018).
31. French, SLR, Walters, V, and Eyles, J. An empirical evaluation of an expanded nursing, stress scale. J Nurs Manag. (2000) 8:161–78. doi: 10.1891/1061-3749.8.2.161
32. Mosadeghrad, AM. Occupational stress and turnover intention: implications for nursing management. Int J Health Policy Manag. (2013) 1:169–76. doi: 10.15171/ijhpm.2013.30
33. Zewdu, S. Alemu AWork-related stress and associated factors among nurses working in public hospitals of Addis Ababa, Ethiopia: a. Research Gate. (2016) 62:326–32. doi: 10.3928/21650799-20140708-02
34. Bhatia, N, Kishore, J, Anand, T, and Jiloha, RC. Occupational stress amongst nurses from two tertiary care hospitals in Delhi occupational stress amongst nurses from two tertiary care hospitals in Delhi. Theatr Res Int. (2014) 2010:731–8. doi: 10.4066/AMJ.2010.289
35. Mojdeh, S, Sabet, B, Irani, MD, Hajian, E, and Malbousizadeh, M. Relationship between nurse’s stress and environmental - occupational factors. Iranian Journal of Nursing and Midwifery Research. (2008) 13.
36. Mohamed, F, Gaafar, Y, and Abd, AW. Pediatric nurses stresses in intensive care units and its related factors. J Am Sci. (2011) 7:304–15.
37. Oo, A, Osamudiamen, OS, and Ojo, AA. Occupational stress management among nurses in selected hospital in Benin city, Edo state, Nigeria. Pelagia Res Libr. (2013) 3:473–81.
38. Nabirye, RC, Brown, KC, Pryor, ER, and Maples, EH. Occupational stress, job satisfaction and job performance among hospital nurses in Kampala. Uganda J Nurs Manag. (2011) 19:760–8. doi: 10.1111/j.1365-2834.2011.01240.x
39. Salilih, SZ, and Abajobir, AA. Work-related stress and associated factors among nurses working in public hospitals of Addis Ababa, Ethiopia: a cross-sectional study. Workplace Health Safe. (2014) 62:326–32. doi: 10.1177/216507991406200803
Keywords: occupational stress, nurses, public hospitals, Addis Ababa, Ethiopia
Citation: Werke EB and Weret ZS (2023) Occupational stress and associated factors among nurses working at public hospitals of Addis Ababa, Ethiopia, 2022; A hospital based cross-sectional study. Front. Public Health. 11:1147086. doi: 10.3389/fpubh.2023.1147086
Edited by:
Majed Alamri, University of Hafr Al Batin, Saudi ArabiaReviewed by:
Deepak Chandran, Amrita Vishwa Vidyapeetham University, IndiaAmir Jalali, Substance Abuse Prevention Research Center and Sleep Disorders Research Center and Kermanshah University of Medical Sciences, Iran
Copyright © 2023 Werke and Weret. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elshaday Bekele Werke, ZWxzaGFkYXlidzFAZ21haWwuY29t