
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Public Health, 29 March 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1143468
This article is part of the Research TopicSARS-CoV-2: Virology, Epidemiology, Diagnosis, Pathogenesis, and ControlView all 24 articles
 Zitong Zhang1
Zitong Zhang1 Yifeng Chen1
Yifeng Chen1 Qingyu Li1
Qingyu Li1 Yan Yang1Jiake Chen1Yan Lin1Zhihong Xiao1Marie Ma2
Yan Yang1Jiake Chen1Yan Lin1Zhihong Xiao1Marie Ma2 Chuancheng Wu1Baoying Liu1Rongxian Xu1
Chuancheng Wu1Baoying Liu1Rongxian Xu1 Jianjun Xiang1
*
Jianjun Xiang1
*
Previous studies investigating the characteristics of imported cases were mostly limited to a certain province/city or a specific sub-group during a certain period with a small sample size, which may not provide an overall picture of the characteristics of imported cases. In this scoping literature review, we comprehensively synthesized the epidemiological characteristics of overseas imported COVID-19 cases into China by retrieving six literature databases, with aims to provide implications for more targeted control, prevention, and medical treatment of this disease. After dropping duplicates and reviewing titles, abstracts, and full-texts, 50 articles were included in the review finally, including 26 (52%) articles in English and 24 (48%) articles in Chinese. According to the type of data sources, the 50 studies were divided into three categories: 13 (26%) articles using data sourced from the Chinese Infectious Diseases Online Reporting System, 15 (30%) articles using data from the websites of national/local health departments, and 22 (44%) articles using hospital admission data. Most of the overseas imported COVID-19 cases were young and middle-aged Chinese students and businessmen returning from the United States, Europe, and some neighboring countries. Airport routine health screening measures could not identify COVID-cases effectively, although scheduled multiple nucleic acid tests were required before boarding. Almost all imported cases were identified during the hotel quarantine period. Although a large proportion of imported cases were asymptomatic or with mild symptoms in the published literature, they may be due to participant selection bias. The exact proportion of asymptomatic cases may need to be further investigated especially through population-based large-scale studies.
Since the first case of COVID-19 was identified in late-December in Wuhan, Hubei Province of central China, the epidemic spread rapidly and was declared a global pandemic by WHO on 11 March 2020 (1). COVID-19 is one of the most widespread epidemics in human history, not only posing a huge threat to the health of vulnerable populations (e.g., older adults) but also severely impacting global economic development (2). Looking back at China’s tremendous efforts in fighting against COVID-19 in the past 3 years, the whole process could be roughly divided into four stages (3). The first stage is the formation of the COVID-19 epicenter in Wuhan and its spread to other provinces from 31st December 2019 to 29th February 2020; The second stage lasted from 1st to 21st March 2020, characterized with the containment of COVID-19 outbreaks and the number of cases was reduced to less than 10 in most provinces; The third stage is the sporadic outbreak mostly triggered by overseas imported cases from March 2021 to June 2022. In this stage, the priority of precautionary measures has gradually shifted from domestic infected cases to overseas imported cases. To prevent overseas imported cases, since 29th March 2022 Civil Aviation Administration of China introduced the “Five-One” policy to limit the number of international flights, namely each airline can only operate one flight per week to travel to and out of China (4). Moreover, a flight would be suspended for 1–2 weeks when confirmed cases accounted for a certain percentage (e.g., 4%) of inbound passengers. The duration of hotel/home quarantine for incoming passengers was updated correspondingly (Figure 1), according to the domestic and international COVID-19 epidemic situations. The fourth stage is the relaxation of strict COVID-19 restrictions (e.g., case tracing) since 7th December 2022. COVID-19 was initially classified as a B-category notifiable infectious disease in China but managed under A-category protocols. From 8th January 2023, control measures against COVID-19 have been downgraded from A-category to B-category (5).
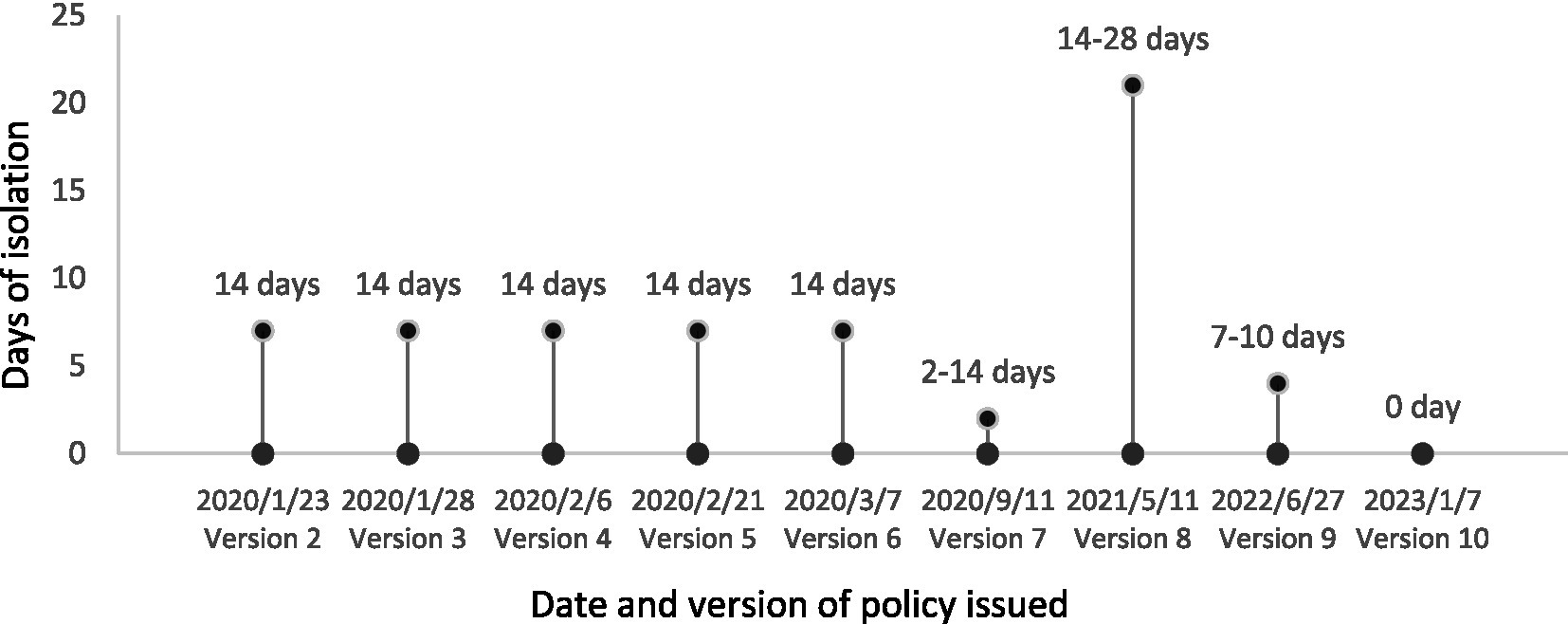
Figure 1. Duration of mandatory hotel/home quarantine for incoming passengers according to the 2nd–9th editions of the COVID-19 prevention and control guidelines.
The infectivity and virulence of SARS-CoV-2 evolve rapidly, and the corresponding prevention guidelines have been updated to the 10th edition in China (6). Under the new policy, the control strategy has shifted from the hard-line “zero-COVID” measures such as strict lockdown and large-scale all-staff COVID-19 testing to co-exist with the virus. The current priorities include the protection and medical treatment of infected vulnerable populations, increasing the vaccination rate of older adults, strengthening surveillance, and optimizing border control. International flights are anticipated to restore gradually. The duration of hotel quarantine has been reduced from at least 2–3 weeks in a certain period to 5 days in November 2022. From 8th January 2023, quarantine requirements on inbound travelers have been canceled. Overseas imported cases into China are likely to increase in the following several months because of the relaxed international travel restrictions (e.g., the cancelation of hotel quarantine), which may burden the already overloaded healthcare system, especially in the under-developed rural areas.
Most of previous studies focused on the spatial and temporal distribution of overseas imported COVID-19 cases, and they were published at an early stage with a small sample size (7, 8). In this scoping literature review, we aimed to comprehensively synthesize the epidemiological characteristics of overseas imported COVID-19 cases into China, to provide implications for more targeted control, prevention, and medical treatment of this disease.
Articles involving epidemiological characteristics of overseas imported COVID-19 cases into China were searched using the combination of keywords: imported COVID-19 AND (China OR mainland China OR Taiwan OR Hongkong OR Macao), including studies published from the time of database creation to November 10, 2022. Literature databases used for this review included PubMed, Embase, and Scopus. Three Chinese literature databases, China National Knowledge Infrastructure (CNKI), Wanfang, and Weipu, were also retrieved to avoid language bias, as the Ministry of Science and Technology of China released a notice on 29 January 2020 to encourage Chinese researchers to publish COVID-19 related studies in domestic journals (9). The initial search results were imported into an Endnote library. Duplicate records were removed using the EndNote function of “find duplicates.” Appropriate peer-reviewed studies were identified by a three-step process (Figure 2): screening titles, reviewing abstracts of articles that were difficult to judge by screening their titles, and reviewing the full-texts. Studies were independently appraised by two investigators (ZZH and JX). Where consensus could not be reached, there was a group discussion to determine the final articles included for reviewing. Reference lists and similar articles recommended by PubMed were also scanned for additional articles not previously identified. The ‘Google Scholar’ and ‘Baidu Scholar’ search engines were also used to retrieve relevant literature.
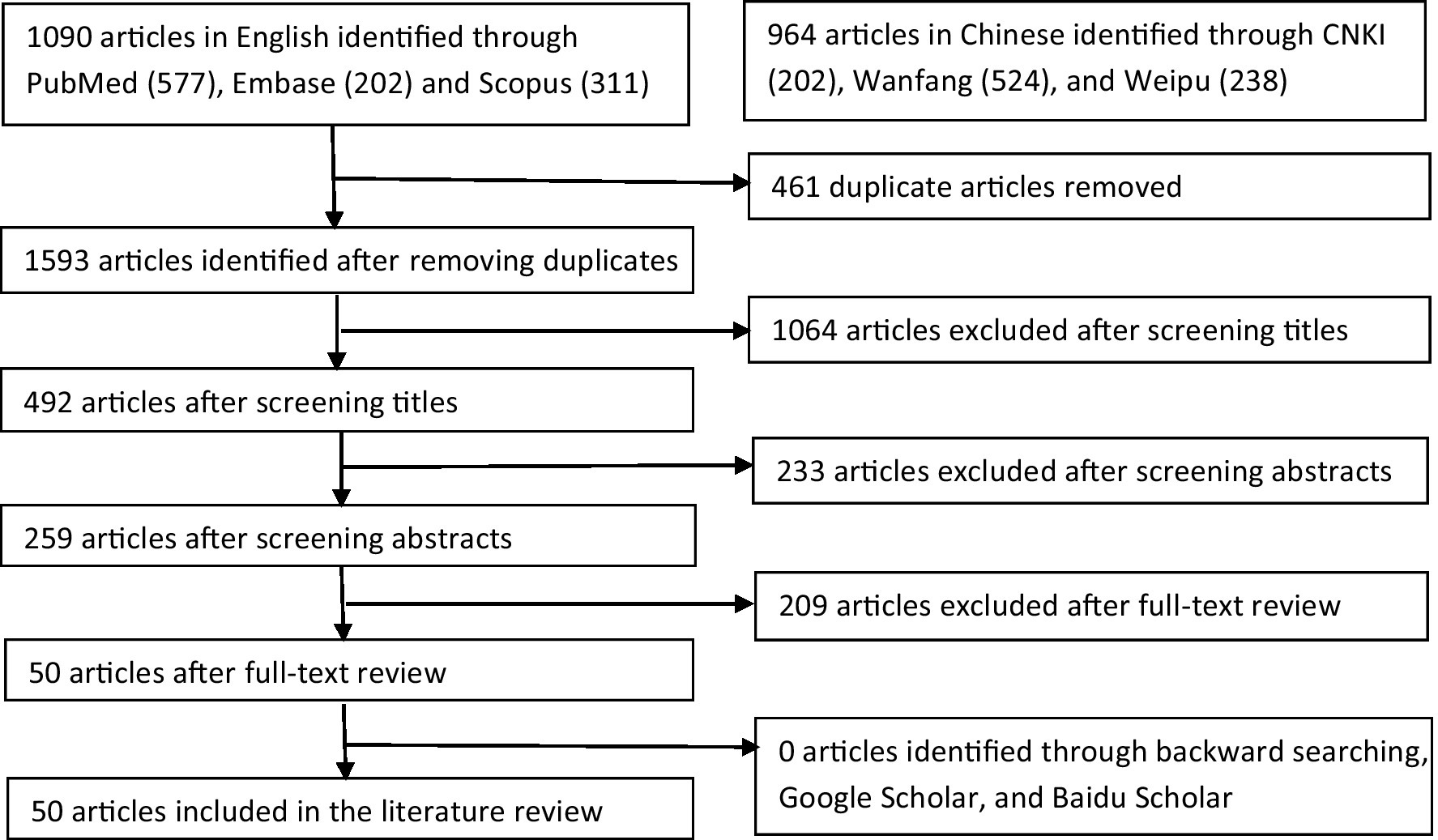
Figure 2. Flow chart of literature search process.
This scoping review of overseas imported cases includes articles from three data sources: China Infectious Disease Reporting System, national/local health department websites, and hospital inpatient data. Due to the different emphases of the source data, we divided the collected literature data into three tables to facilitate the statistics of useful information.
The studies selected in this review met the following criteria:
• Investigated the epidemiological characteristics of overseas imported COVID-19 cased into China.
• Peer-reviewed studies published from database inception to 10 November 2022.
• Conference abstracts, letters, editorials, field investigations, reports and unrefereed preprints on medRxiv and bioRxiv were excluded.
Figure 1 shows the process of selection of articles for inclusion in the review. An initial search generated 2054 articles, with 53.1% being published in English and the rest in Chinese. After dropping duplicates and reviewing titles, abstracts, and full-texts, 50 articles were finally included in the review, including 26 (52%) articles in English and 24 (48%) articles in Chinese. According to the type of data sources, the 50 studies were divided into three categories: 13 (26%) articles using data sourced from the Chinese Infectious Diseases Online Reporting System, 15 (30%) articles using data from the websites of national/local health departments, and 22 (44%) articles using hospital admission data. They were summarized in Tables 1–3, respectively.
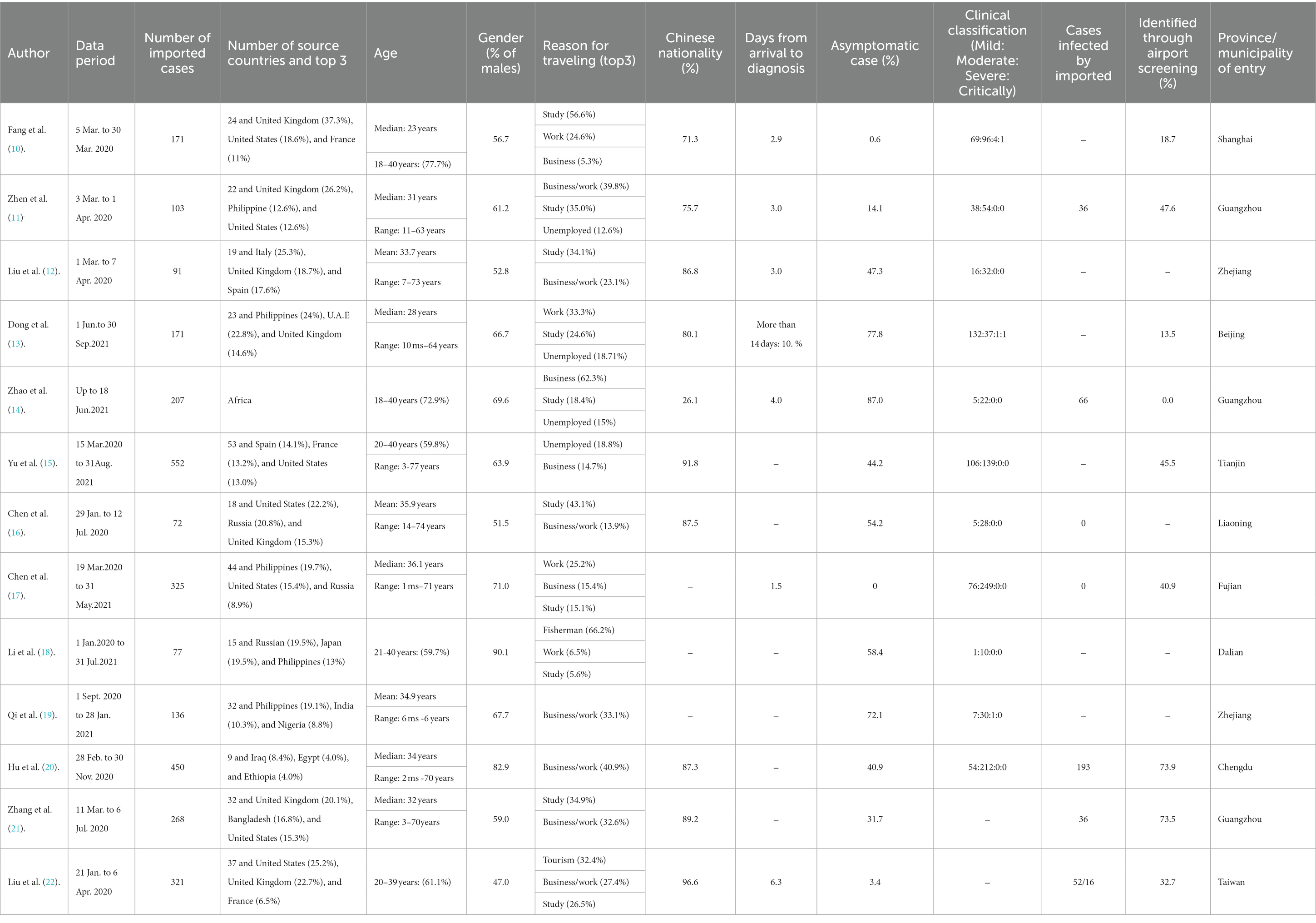
Table 1. Summary of 13 studies using data sourced from the Chinese Infectious Diseases Reporting System.
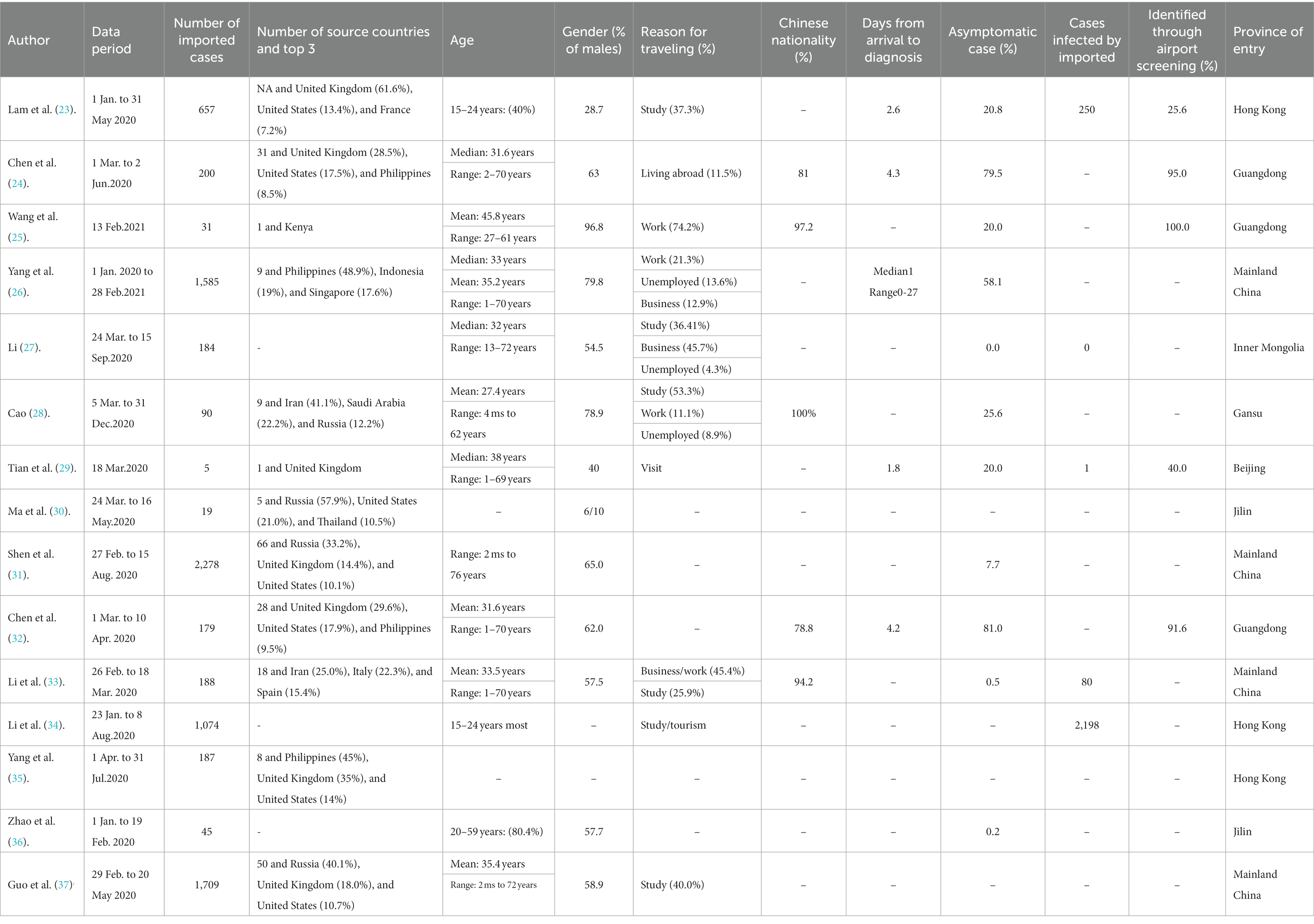
Table 2. Summary of 15 studies using data sourced from the websites of national/local health departments.
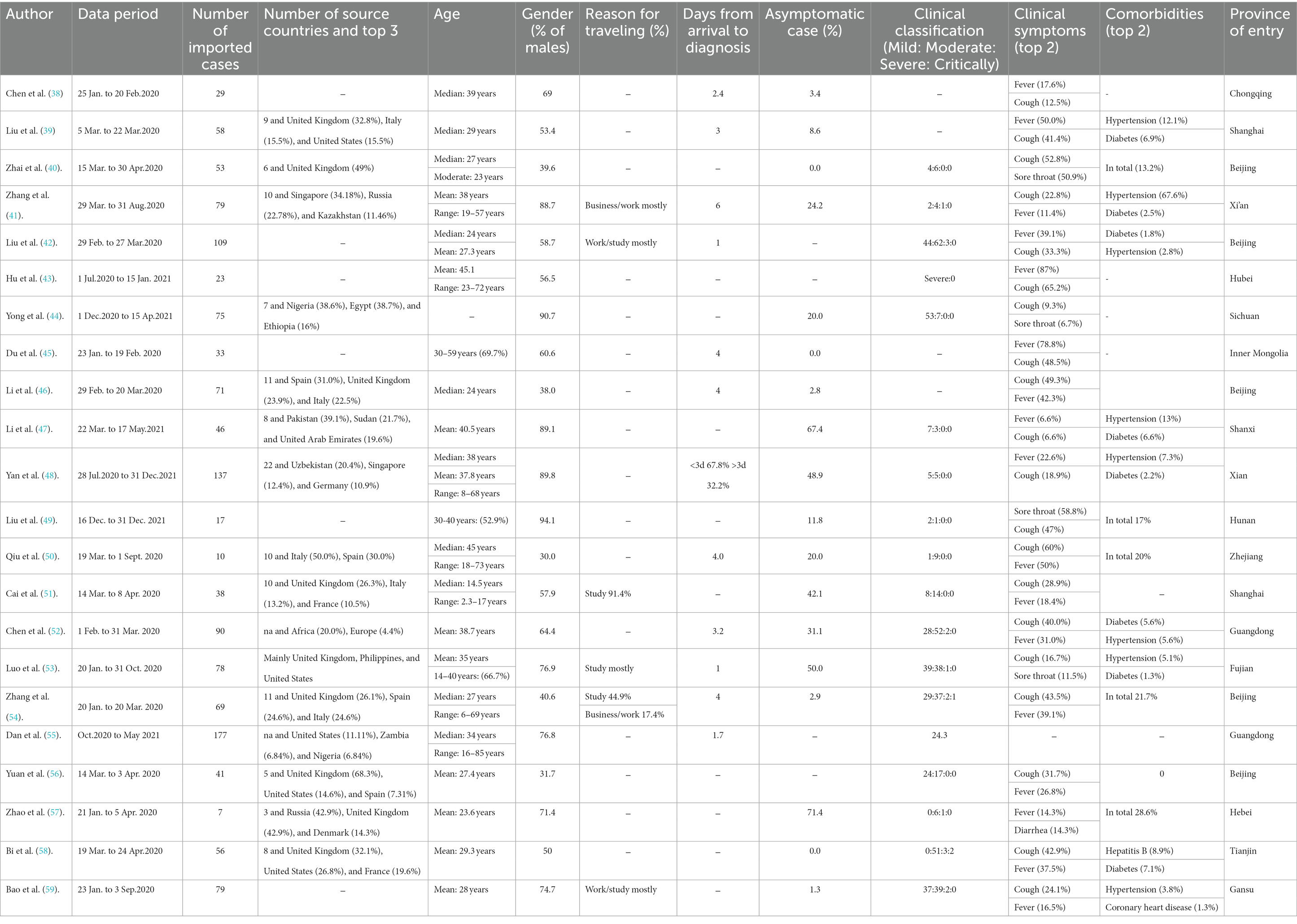
Table 3. Summary of 22 studies using hospital admission data.
Table 1 summarized the key characteristics of 13 articles analyzing imported cases reported through the online Chinese Infectious Diseases Reporting System (CIDRS). The number of source countries ranged from 5 to 53 and the most frequent top-three countries were United States, United Kingdom, and Philippines. The ranges of median and mean ages were 23–36 and 34–36 years, respectively. Most imported cases were males, with the proportion reaching as high as 90.1%. Study, work, and business were the most frequent reasons for traveling. The vast majority of cases were Chinese citizens (71.3–96.6%). The number of days from entry to diagnosis ranged from 1.5 to 6.3, while it should be noted that there was a special case taking 14 days to be diagnosed. The proportion of asymptomatic cases varied largely from zero to 87%. The proportion of cases identified through airport health screening measures ranged from zero to 74%.
Table 2 showed the characteristics of 15 articles analyzing COVID-19 cases sourced from the websites of national or local health departments. Basically, the characteristics of imported cases in Table 2 were similar with that in Table 1 in the aspects of reasons for traveling and days from entry to diagnosis, because COVID-19 data released on the official websites were also sourced from the CIDRS. By contrast, characteristics of imported cases based on hospital admission data (Table 3) were slightly different with cases sourced from the CIDRSA and governmental websites in Tables 1, 2. The number of source countries reached 177 by May 2021. Moreover, they were relatively more diverse compared to that in Tables 1, 2. The proportion of asymptomatic cases ranged from zero to 71.4%, which was lower than that in Tables 1, 2. The most frequent clinical symptoms of imported cases were fever, coughing, and sore throat, with the highest percentages reaching 87, 65, and 51%, respectively. The most common comorbidities were hypertension and diabetes.
Imported COVID-19 cases are an important source triggering local sporadic outbreaks. One imported case could reportedly result in more than 2,000 infections in a short period of time. Thus, strict border control measures had been taken by the government to reduce the risk, such as scheduled multiple nucleic acid tests before boarding, a “Five-One” flight policy, closed-loop management, and hotel quarantine. Previous studies investigating the characteristics of imported cases were mostly limited to a certain province/city or a specific sub-group during a certain period, which may not provide an overall picture of the characteristics of imported cases. In this study, we comprehensively reviewed the epidemiological characteristics of overseas imported COVID-19 cases into China, retrieving six literature databases. Findings of this literature review may not only provide evidence for the development of current control measures against COVID-19 but also facilitate the management of imported cases.
We found that the importing countries were mainly high-income countries (e.g., United States and United Kingdom) or neighboring countries (e.g., Russia and Malaysia) with close trade links with China. United States and United Kingdom are the top two destinations for Chinese students. In 2021, many overseas Chinese students were selected to return to China due to the following reasons. First, many western countries abandoned case tracking, early detection, and case isolation and selected coexistence with the virus, leading to the surge of COVID-19 related morbidity and mortality (60). By contrast, China took a strict zero-case policy at that time and the epidemic was well-contained. Second, some universities transferred to online teaching temporarily to avoid campus outbreaks. Third, evidence has shown that the well-being of Chinese international students deteriorated in the early stage of COVID-19 pandemic. Over the debate of COVID-19 origin, a high prevalence of mental health issues (e.g., depression, anxiety, and feeling of discrimination) was observed among them (61, 62). In addition, work and business activities were also the most common reasons for traveling to China, while most incoming travelers were Chinese nationals. International air flights are the major way for imported cases (63), however, some travelers sought to enter via land or port when most international flights were suspended at the early stage of the global pandemic. For example, most cases imported from Russia were through land border ports, especially the Suifen River Estuary in Mudanjiang city. The proportion of male travelers was higher than their female counterparts. Our result is supported by the findings of a global study of population mobility networks (61), which utilized the characteristics of travelers and geographical factors to predict the COVID-19 cross-border transmission.
According to the level of severity, COVID-19 was initially divided into four types: mild, moderate, severe, and critical cases. However, published literature shows that many infections of COVID-19 are asymptomatic (64). It has been reported that viral loads of asymptomatic patients were similar with those of symptomatic individuals (65), suggesting that asymptomatic patients have a similar capacity in infectivity for transmission. The potential transmission of asymptomatic infections poses a significant challenge to the control and prevention of COVID-19. Two prerequisites must be met for the diagnosis of asymptomatic COVID-19 infection: the absence of self-perceived or clinically recognizable symptoms; and a positive reverse transcription-PCR (RT-PCR) test. In this review, the proportion of asymptomatic cases was highly variable with a range from 0 to 87%. Not only in the imported cases, a highly varied proportion of asymptomatic infections was also reported in the general population (8). This may be due to participant selection bias. For example, in this review we found the average proportion of asymptomatic infections based on hospital admission data (22%) was lower than the proportion based on data sourced from CDC (41%) and the websites of local health departments (26%). Most of the imported cases were young and middle-aged who were less likely to have clinical manifestations than the vulnerable sub-groups (e.g., children, pregnant women, and older adults with chronic diseases). Moreover, symptomatic cases may opt to postpone their trips. Relative fewer cases from low- and middle-income countries due to the soaring airfares and the limited number of flights may also contribute to the participant selection bias. Another factor associated with clinical manifestations was the course of disease. Evidence has shown that the proportion of asymptomatic infections ranged from approximately 20–75% at initial testing, however, only 4% remained asymptomatic throughout the disease finally (66). In addition, vaccination status, the type of vaccines, and virus strain also affect the presentation of clinical symptoms. The exact proportion of asymptomatic cases needs to be further investigated especially through population-based large-scale studies.
We observed a high heterogeneity in sample size, patients’ age, COVID-19 symptoms, and comorbidities, although most of the included studies were conducted in China. Fever and coughing were the most common symptoms. Regarding comorbidities for patients with COVID-19, the highest severity factors were hypertension, diabetes, obesity, chronic obstructive pulmonary disease, and cardiovascular disease. This is consistent with a recent literature review focused on the general population (8). Pustahija et al. found there were no significant differences between travel-associated cases and cases identified in the general population in terms of the epidemiological and clinical characteristics in Serbia (67). Another study from Bolivia found similar epidemiological characteristics of imported COVID-19 cases with this study (68). It should be noted that the differences between studies in symptoms and comorbidities cannot be compared directly without taking demographical factors, virus strain, healthcare systems, selection criteria, the course of disease, and border control measures into account.
In response to the COVID-19 pandemic, many countries have imposed international travel restrictions to prevent the importation of COVID-19 cases. In this review, we found the proportion of imported cases identified by airport health screening measures varied considerably from zero to 100% with an average of 49.9%, indicating that entry screening alone may not detect imported cases effectively at borders. Although more than 90% of COVID-19 patients had a fever, body temperature might not be an adequate screening method as it may miss travelers in the incubation period or travelers concealing fever during travel (69). Despite the ineffectiveness of entry screening measures, travel restrictions may delay the transmission of COVID-19 between countries and have concomitant positive effects such as discoursing the travel of ill persons and raising the awareness of infectious disease control (63, 70). In this review, the number of days from entry to diagnosis ranged from 1.5 to 6.3 days. To prevent the importation of COVID-19 cases, 1–3 weeks’ hotel quarantine was mandatorily required by the Chinese government for all incoming passengers before 8th January 2023. Moreover, multiple RT-PCT tests were required before boarding and during the quarantine period to minimize the risk of importation as much as possible. However, it should be noted that quarantine hotels are not designed with infection control and there is a risk of within hotel transmission between guests and/or staff. It has been estimated that 8–11 per 1,000 cases identified during hotel quarantine may be infected by another unlinked case during quarantine (71). Therefore, its impact on the characteristics of imported cases should be minimal.
To maintain international personnel and economic exchanges, quarantine strategies have been adjusted timely according to the infectivity, virulence, and incubation period of different variants. A recent systematic review suggested that the incubation periods of Alpha, Beta, Delta, and Omicron variants were 5.0, 4.5, 4.4, and 3.4 days, respectively (72). With the shortening of the incubation periods of new variants, the quarantine period has been reduced accordingly. Now hotel quarantine requirements on inbound travelers are no longer required. Nevertheless, negative RT-PCR test 48 h before departure and online self-declaration of health status are still in place to prevent importation. These targeted measures significantly reduced the importation of COVID-10 cases into China and the pressure on the healthcare system (73). China will keep monitoring the characteristics of imported cases to adjust prevention policies to lessen the impact on economic and social development.
Most of the overseas imported COVID-19 cases were young and middle-aged Chinese students and businessmen returning from the United States, Europe, and some neighboring countries. Airport routine health screening measures could not identify COVID-cases effectively although scheduled multiple nucleic acid tests were required before boarding. Almost all imported cases were identified during the hotel quarantine period. Although a large proportion of imported cases were asymptomatic or with mild symptoms in the published literature, they may be due to participant selection bias. The exact proportion of asymptomatic cases needs to be further investigated especially through population-based large-scale studies.
JX, RX, BL, and ZZ conceived the review. ZZ, JX, YC, QL, YY, JC, YL, and ZX participated in the literature search and selection. ZZ and JX drafted the manuscript and made the tables. ZZ, MM, CW, BL, RX, and JX revised the manuscript. All authors contributed to the article and approved the submitted version.
This study was supported by the 2019 Minjiang Scholar Start-up Research Fund of Fujian Province.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Health Organization (WHO) . WHO director-General's opening remarks at the media briefing on COVID-19. (2020) Available at: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (Accessed January 10, 2023).
2. Verschuur, J, Koks, EE, and Hall, JW. Global economic impacts of COVID-19 lockdown measures stand out in high-frequency shipping data. PLoS One. (2021) 16:e0248818. doi: 10.1371/journal.pone.0248818
3. Chen, L, Cai, J, Lin, Q, Xiang, B, and Ren, T. Imported COVID-19 cases pose new challenges for China. J Inf Secur. (2020) 80:e43–4. doi: 10.1016/j.jinf.2020.03.048
4. Central People's Government of the People's Republic of China (2020). Notice on further reduction of international flights to China during the period of COVID-19 pandemic. Available at: http://www.gov.cn/zhengce/zhengceku/2020-03/27/content_5496232.htm (Accessed January 10, 2023).
5. National Health Commission of the People's Republic of China (2023). Notice on further optimizing and implementing the prevention and control measures of COVID-19 epidemic. Available at: http://www.nhc.gov.cn/xcs/zhengcwj/202212/8278e7a7aee34e5bb378f0e0fc94e0f0.shtml (Accessed January 10, 2023).
6. National Health Commission of the People's Republic of China Notice on further optimizing and implementing the prevention and control measures of COVID-19 epidemic. (2022) Available at: http://www.nhc.gov.cn/xcs/zhengcwj/202212/8278e7a7aee34e5bb378f0e0fc94e0f0.shtml (Accessed February 25, 2023).
7. Hâncean, MG, Slavinec, M, and Perc, M. The impact of human mobility networks on the global spread of COVID-19. J Complex Netw. (2020) 8:1–14. doi: 10.1093/comnet/cnaa041
8. Ferreira-Santos, D, Maranhão, P, and Monteiro-Soares, M. Identifying common baseline clinical features of COVID-19: a scoping review. BMJ Open. (2020) 10:e041079. doi: 10.1136/bmjopen-2020-041079
9. Ministry of Science and Technology of the People's Republic of China (2023). The Ministry of Science and Technology advocates that researchers should bravely shoulder heavy responsibilities, devote all their efforts to scientific and technological research tasks, and write papers on the front line of fighting against the epidemic. Available at: https://www.most.gov.cn/kjbgz/202001/t20200129_151264.html (Accessed January 10, 2023).
10. Fang, QW, Gong, XH, Xiao, WJ, Jin, BH, Yu, X, Cui, P, et al. Epidemiological characteristics and measures of prevention and control of imported COVID-19 cases in early phase in Shanghai. Chin J Epidemiol. (2020) 41:2034–9. doi: 10.3760/cma.j.cn112338-20200413-00566
11. Zhen, RN, Huang, Y, Li, YL, Zhou, S, Chen, YY, Qin, FJ, et al. Epidemiological characteristics of imported COVID-19 cases in Guangzhou. Chin J Epidemiol. (2020) 41:1786–90. doi: 10.3760/cma.j.cn112338-20200413-00569
12. Liu, BY, Qi, XH, Jiang, M, and Wang, Z. Epidemiological characteristics of imported COVID-19 cases from abroad to Zhejiang Province. Prev Med. (2020) 32:550–4. doi: 10.19485/j.cnki.issn2096-5087.2020.06.003
13. Dong, SB, Wang, XL, Zhao, H, Wang, Y, Liu, BW, Liu, YH, et al. Epidemiological characteristics of imported COVID-19 cases in Beijing. Chin J Epidemiol. (2022) 43:478–82. doi: 10.3760/cma.j.cn112338-20211213-00975
14. Zhao, WH, Ma, Y, Wang, H, Li, K, Dong, H, Liu, WH, et al. Epidemiological characteristics of three local epidemics of COVID-19 in Guangzhou. Chin J Epidemiol. (2021) 42:2088–95. doi: 10.3760/cma.j.cn112338-20210728-00592
15. Yu, JB, Wang, YM, Yu, H, Zhang, JW, Zhou, PH, Zhou, P, et al. Epidemiological characteristics of imported COVID-19 cases in Tianjin. Chin J Epidemiol. (2021) 42:2082–7. doi: 10.3760/cma.j.cn112338-20210816-00647
16. Chen, T, Na, J, Tian, J, Liu, R, Wang, ZJ, Yang, XL, et al. Epidemiological characteristics analysis of imported cases of novel coronavirus pneumonia in Liaoning Province and effectiveness evaluation of prevention and control measures. Chin J Public Health. (2021) 37:307–10. doi: 10.11847/zgggws1132464
17. Chen, GM, Lan, MF, Xie, JF, Ou, JM, and Zheng, GC. Analysis on the characteristics of confirmed cases of COVID-19 imported from outside Fujian Province. Chin Prevent Med. (2021) 22:736–40. doi: 10.16506/j.1009-6639.2021.10.002
18. Li, YT, Fan, YJ, and Han, CX. Epidemiological characteristics of imported and local COVID-19 cases in Dalian City. J Community Med. (2022) 20:426–9. doi: 10.19790/j.cnki.JCM.2022.08.03
19. Qi, XH, Liu, BY, Wang, Z, and Zhang, RJ. Characteristics of imported COVID-19 cases in Zhejiang Province. Prev Med. (2021) 33:541–4. doi: 10.19485/j.cnki.issn2096-5087.2021.06.001
20. Hu, M, Yue, Y, Du, XB, Fan, SF, Chen, H, Zhou, R, et al. Analysis of epidemiological characteristics of imported COVID-19 patients in Chengdu, Sichuan Province. Dis Surv. (2021) 36:587–92. doi: 10.3784/jbjc.202102160069
21. Zhang, ZB, Li, L, Qin, PZ, Li, K, Huang, Y, Luo, L, et al. Countries of origin of imported COVID-19 cases into China and measures to prevent onward transmission. J Travel Med. (2020) 27:1–12. doi: 10.1093/jtm/taaa139
22. Liu, JY, Chen, TJ, and Hwang, SJ. Analysis of imported cases of COVID-19 in Taiwan: a Nationwide study. Int J Environ Res Public Health. (2020) 17:1–12. doi: 10.3390/ijerph17093311
23. Lam, HY, Lam, TS, Wong, CH, Lam, WH, Leung, CME, Au, KWA, et al. The epidemiology of COVID-19 cases and the successful containment strategy in Hong Kong-January to may 2020. Int J Infect Dis. (2020) 98:51–8. doi: 10.1016/j.ijid.2020.06.057
24. Chen, H, Shi, L, Zhang, Y, Wang, X, and Sun, G. Epidemiological characteristics and core containment measures of imported COVID-19 cases from abroad in early phase in Guangdong. Chin Risk Manag Health Policy. (2021) 14:3955–63. doi: 10.2147/RMHP.S317910
25. Wang, H, Zhang, ZZ, Li, YG, Li, WP, Long, JL, Chen, ZQ, et al. Investigation of a cluster of COVID-19 cases imported through inbound air flight. Dis Surv. (2022) 37:850–4. doi: 10.3784/jbjc.202107070386
26. Yang, D, Chen, QL, Wang, Z, Chen, N, and Zhu, MT. Epidemiological characteristics of imported cases of COVID-19 from Association of Southeast Asian Nations countries to China. Dis Surv. (2021) 36:561–5. doi: 10.3784/jbjc202105120259
27. Li, X. Epidemiological and genetic characteristics of novel coronavirus pneumonia in Inner Mongolia in 2020. Inner Mongolia Medical University. (2021).
28. Cao, LJ . Study on epidemiology and control strategies of foreign-imported COVID-19 in Gansu Province: Lanzhou University. (2021).
29. Tian, LL, Qian, C, Xin, RL, Yi, JL, Ren, YX, Lin, CY, et al. Epidemiological investigation, diagnosis and treatment of a family cluster of imported novel coronavirus pneumonia. Capit J Public Health. (2020) 14:132–6. doi: 10.16760/j.cnki.sdggws.2020.03.006
30. Ma, YY, and Li, LJ. Epidemiological characteristics of COVID-19 in Jilin Province. J Dali Univ. (2020) 5:7–11. doi: 10.3969/j.issn.2096-2266.2020.08.002
31. Shen, SR, Ma, ZC, Xu, YL, Gao, Y, and Chen, XF. Epidemic impact of overseas-imported COVID-19 infected cases on China. J Zhejiang Norm Univ. (2021) 44:197–205. doi: 10.16218/j.issn.1001-5051.2021.02.011
32. Cheng, L, and Xu, H. Interval between entry of mainland China and diagnosis in imported COVID-19 cases and factors contributing to delayed diagnosis in Guangdong Province. J South Med Univ. (2020) 40:741–5. doi: 10.12122/j.issn.1673-4254.2020.05.21
33. Li, ZH, Wang, J, Huang, JY, Lu, JH, and Guo, ZM. Epidemiological characteristics of imported cases of COVID⁃19 from outside China in early stage. J Trop Med. (2020) 20:1093–7.
34. Li, C, Zhao, S, Tang, B, Zhu, Y, Ran, J, Li, X, et al. Estimating the instantaneous asymptomatic proportion with a simple approach: exemplified with the publicly available COVID-19 surveillance data in Hong Kong. Front Public Health. (2021) 9:1–6. doi: 10.3389/fpubh.2021.604455
35. Yang, B, Tsang, TK, Wong, JY, He, Y, Gao, H, Ho, F, et al. The differential importation risks of COVID-19 from inbound travellers and the feasibility of targeted travel controls: a case study in Hong Kong. Lancet Reg Health West Pac. (2021) 13:100184–9. doi: 10.1016/j.lanwpc.2021.100184
36. Zhao, Q, Wang, Y, Yang, M, Li, M, Zhao, Z, Lu, X, et al. Evaluating the effectiveness of measures to control the novel coronavirus disease 2019 in Jilin Province, China. BMC Infect Dis. (2021) 21:245. doi: 10.1186/s12879-021-05936-9
37. Guo, XY, Guo, WW, Li, P, Chen, FY, Shen, MW, Zeng, LX, et al. Epidemiological characteristics of imported COVID-19 cases from abroad in mainland China. Chin J Public Health. (2020) 36:1763–6. doi: 10.11847/zgggws1131945
38. Chen, P, Zhang, Y, Wen, Y, Guo, J, Jia, J, Ma, Y, et al. Epidemiological and clinical characteristics of 136 cases of COVID-19 in Chongqing. J Formos Med Assoc. (2020) 119:1180–4. doi: 10.1016/j.jfma.2020.04.019
39. Liu, XH, Lu, SH, Chen, J, Xia, L, Yang, ZG, Charles, S, et al. Clinical characteristics of foreign-imported COVID-19 cases in Shanghai, China. Emerg Microbes Infect. (2020) 9:1230–2. doi: 10.1080/22221751.2020.1766383
40. Zhai, W, Luo, Z, Zheng, Y, Dong, D, Wu, E, Wang, Z, et al. Moderate vs. mild cases of overseas-imported COVID-19 in Beijing: a retrospective cohort study. Sci Rep. (2021) 11:6483. doi: 10.1038/s41598-021-85869-0
41. Zhang, L, Liu, M, Li, J, Li, X, Cheng, L, Ji, Y, et al. Clinical characteristics of foreign-imported COVID-19 cases in Xi'an, China. Int J Gen Med. (2021) 14:2069–78. doi: 10.2147/IJGM.S315159
42. Liu, JH, Chang, YF, Ma, SF, and Wang, LH. Comparative study on the clinical characteristics of local cases of COVID-19 and imported cases from abroad: a retrospective cohort study. Medicine. (2021) 100:e26933. doi: 10.1097/MD.0000000000026933
43. Hu, YL, and Ding, T. Clinical characteristics of COVID-19 patients in Xiaogan, China: comparison between recent imported cases and earlier local cases. Am J Transl Res. (2021) 13:12724–33.
44. Yue, Y, Liang, X, Mao, Y, Hu, M, Han, DL, Su, LY, et al. Influence of SARS-CoV-2 vaccination on the epidemiological and clinical characteristics of imported COVID-19 cases in Chengdu. Chin J Epidemiol. (2021) 42:1365–70. doi: 10.3760/cma.j.cn112338-20210330-00261
45. Du, S, Lu, H, Su, Y, Wang, X, Bi, S, Wu, J, et al. Epidemiological characteristics of COVID-19 under government-mandated control measures during January-February 2020 in Inner Mongolia. China Jpn J Infect Dis. (2022) 75:361–7. doi: 10.7883/yoken.JJID.2021.274
46. Li, L, Ma, CJ, Chang, YF, Yang, SY, Tang, YX, and Wang, LH. The characteristics of overseas imported COVID-19 cases and the effectiveness of screening strategies in Beijing. BMC Infect Dis. (2022) 22:59. doi: 10.1186/s12879-021-06998-5
47. Li, J, Jiang, N, Zeng, QL, Zhang, Y, He, X, Chu, Y, et al. The epidemiological, clinical features and outcomes of imported Chinese COVID-19 patients following inactivated vaccines injection. Infect Drug Resist. (2022) 15:2115–25. doi: 10.2147/IDR.S356460
48. Yan, Y, Yang, L, Li, X, Hao, J, Wang, B, Wang, D, et al. Clinical characteristics in patients with redetected positive RNA test after recovery from foreign-imported COVID-19 cases in Xi'an, China. Infect Drug Resist. (2022) 15:3295–307. doi: 10.2147/IDR.S371088
49. Liu, X, Chen, M, Zhou, Z, Chen, D, Mo, J, and Liu, J. Epidemiological characteristics of 17 imported patients infected with SARS-CoV-2 omicron variant. J Cent South Univ. (2022) 47:344. doi: 10.11817/j.issn.1672-7347.2022.220040
50. Qiu, CC, Liu, XJ, Liu, SD, Zhou, YY, Wu, ZX, and Shi, ZC. Clinical characteristics of 10 cases of imported novel coronavirus pneumonia in Wenzhou area. Mod Pract Med. (2020) 32:1038–40. doi: 10.3969/j.issn.1671-0800.2020.09.007
51. Cai, JH, Xia, AM, Wang, XS, Zeng, W, Wang, JL, Tian, H, et al. 38 imported pediatric cases of SARS-CoV-2 infection from abroad in Shanghai: a case series report. Chin J Evid Pediatr. (2020) 15:206–9. doi: 10.3969/j.issn.1673-5501.2020.03.009
52. Chen, M, Zhou, YM, Peng, H, Wu, PL, and Mo, XN. Clinical characteristics of imported COVID-19 patients after inoculating inactivated vaccine. Chin J Infect Control. (2021) 20:586–91. doi: 10.12138/j.issn.1671-9638.20211352
53. Luo, W, Lin, YH, Wu, DH, Yao, XY, Lu, F, and Wang, ZX. Comparative analysis of characteristics of imported cases from abroad and local cases infected with COVID-19 in Xiamen. Int J Resp. (2021) 41:591–6. doi: 10.3760/cma.j.cn131368-20200624-00540
54. Zhang, SJ, Wang, XK, Xu, YL, Song, R, Wang, L, Song, MH, et al. Epidemiological and clinical characteristics of 69 cases with imported corona virus disease 2019. Chin J Infect Dis. (2020) 38:690–5. doi: 10.3760/cma.j.cn311365-20200331-00440
55. Liang, D, Wang, T, Li, JJ, Guan, DW, Zhang, GT, Liang, YF, et al. Genomic epidemiology of imported cases of COVID-19 in Guangdong Province, China, October 2020 - may 2021. Biomed Environ Sci. (2022) 35:393–401. doi: 10.3967/bes2022.055
56. Yuan, Q, Ma, JJ, Wang, ZF, Fu, YB, Zuo, JP, Feng, YH, et al. Clinical features and TCM (traditional Chinese medicine) syndromes distribution of 41 patients with COVID-19 imported from abroad in Beijing. World Chin Med. (2020) 15:2008–10. doi: 10.3969/j.issn.1673-7202.2020.13.031
57. Zhao, L, Qin, H, Dai, EH, Wang, YL, Xu, ZG, Shi, XH, et al. Clinical characteristics of overseas imported and local COVID-19 cases in Hebei Province. Chin Gen Med. (2020) 23:4425–9. doi: 10.12114/j.issn.1007-9572.2020.00.596
58. Bi, YF, Tian, Y, Zhang, WF, Su, LS, Zhao, GY, Sun, HY, et al. Analysis of TCM (traditional Chinese medicine) syndromes of 56 imported cases of novel coronavirus pneumonia. Tianjin J Trad Chin Med. (2021) 38:1098–101. doi: 10.11656/j.issn.1672-1519.2021.09.03
59. Bao, HR, Li, XP, Liu, JX, Ma, BY, Wang, HY, Wen, XJ, et al. Clinical characteristics of imported and local COVID-19 cases in Gansu. Med J West China. (2022) 34:1193–8. doi: 10.3969/j.issn.1672-3511.2022.08.019
60. de Souza, L, Castro, MC, Hage Carmo, E, and Polidoro, M. The global failure of facing the pandemic. Glob Health Action. (2022) 15:2124645. doi: 10.1080/16549716.2022.2124645
61. Amoah, PA, and Mok, EWC. COVID-19 and well-being of non-local students: implications for international higher education governance. High Educ Policy. (2022) 35:651–72. doi: 10.1057/s41307-022-00270-4
62. Lin, C, Tong, Y, Bai, Y, Zhao, Z, Quan, W, Liu, Z, et al. Prevalence and correlates of depression and anxiety among Chinese international students in US colleges during the COVID-19 pandemic: a cross-sectional study. PLoS One. (2022) 17:e0267081. doi: 10.1371/journal.pone.0267081
63. Mouchtouri, VA, Christoforidou, EP, An der Heiden, M, Menel Lemos, C, Fanos, M, Rexroth, U, et al. Exit and entry screening practices for infectious diseases among travelers at points of entry: looking for evidence on public health impact. Int J Environ Res Public Health. (2019) 16:1–53. doi: 10.3390/ijerph16234638
64. Gao, Z, Xu, Y, Sun, C, Wang, X, Guo, Y, Qiu, S, et al. A systematic review of asymptomatic infections with COVID-19. J Microbiol Immunol Infect. (2021) 54:12–6. doi: 10.1016/j.jmii.2020.05.001
65. Zou, L, Ruan, F, Huang, M, Liang, L, Huang, H, Hong, Z, et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med. (2020) 382:1177–9. doi: 10.1056/NEJMc2001737
66. You, Y, Yang, X, Hung, D, Yang, Q, Wu, T, and Deng, M. Asymptomatic COVID-19 infection: diagnosis, transmission, population characteristics. BMJ Support Palliat Care. (2021) 11:bmjspcare-2020-002813–8. doi: 10.1136/bmjspcare-2020-002813
67. Pustahija, T, Ristic, M, Medic, S, Vukovic, V, Strbac, M, Rajcevic, S, et al. Epidemiological characteristics of COVID-19 travel-associated cases in Vojvodina, Serbia, during 2020. PLoS One. (2021) 16:e0261840. doi: 10.1371/journal.pone.0261840
68. Escalera-Antezana, JP, Lizon-Ferrufino, NF, Maldonado-Alanoca, A, Alarcon-De-la-Vega, G, Alvarado-Arnez, LE, Balderrama-Saavedra, MA, et al. Clinical features of the first cases and a cluster of coronavirus disease 2019 (COVID-19) in Bolivia imported from Italy and Spain. Travel Med Infect Dis. (2020) 35:101653. doi: 10.1016/j.tmaid.2020.101653
69. Bwire, GM, and Paulo, LS. Coronavirus disease-2019: is fever an adequate screening for the returning travelers? Trop Med Health. (2020) 48:14. doi: 10.1186/s41182-020-00201-2
70. Adekunle, A, Meehan, M, Rojas-Alvarez, D, Trauer, J, and McBryde, E. Delaying the COVID-19 epidemic in Australia: evaluating the effectiveness of international travel bans. Aust N Z J Public Health. (2020) 44:257–9. doi: 10.1111/1753-6405.13016
71. Adam, DC, Martin-Sanchez, M, Gu, H, Yang, B, Lin, Y, Wu, P, et al. Risk of within-hotel transmission of SARS-CoV-2 during on-arrival quarantine in Hong Kong: an epidemiological and phylogenomic investigation. Lancet Reg Health West Pac. (2023) 1–11. doi: 10.1016/j.lanwpc.2022.100678
72. Wu, Y, Kang, L, Guo, Z, Liu, J, Liu, M, and Liang, W. Incubation period of COVID-19 caused by unique SARS-CoV-2 strains: a systematic review and meta-analysis. JAMA Netw Open. (2022) 5:e2228008. doi: 10.1001/jamanetworkopen.2022.28008
Keywords: imported, COVID-19, epidemiological characteristics, review, China
Citation: Zhang Z, Chen Y, Li Q, Yang Y, Chen J, Lin Y, Xiao Z, Ma M, Wu C, Liu B, Xu R and Xiang J (2023) Epidemiological characteristics of overseas imported COVID-19 cases into China: A scoping literature review. Front. Public Health. 11:1143468. doi: 10.3389/fpubh.2023.1143468
Edited by:
Severino Jefferson Ribeiro da Silva, University of Toronto, CanadaReviewed by:
Jifang Zhou, China Pharmaceutical University, ChinaCopyright © 2023 Zhang, Chen, Li, Yang, Chen, Lin, Xiao, Ma, Wu, Liu, Xu and Xiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianjun Xiang, amlhbmp1bi54aWFuZ0Bmam11LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.