
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 16 February 2023
Sec. Public Mental Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1134032
 Semira Defar1
Semira Defar1 Yacob Abraham2
Yacob Abraham2 Yared Reta2
Yared Reta2 Bedilu Deribe2
Bedilu Deribe2 Meskerem Jisso3
Meskerem Jisso3 Tomas Yeheyis2Kurabachew Mengistu Kebede4
Tomas Yeheyis2Kurabachew Mengistu Kebede4 Bereket Beyene2
Bereket Beyene2 Mohammed Ayalew2*
Mohammed Ayalew2*Background: People with mental illness (PWMI) have declining health related quality of life (HRQoL), which is frequently equivalent to or greater than that of medical disorders. Although, HRQoL is rapidly being recognized as an essential treatment outcome indicator in modern psychiatry, research on the identification and significance of factors impacting QoL in PWMI is still in its early stages.
Objective: The aim of this study was to identify predictors of HRQoL among people with mental illness who underwent outpatient follow-up in Sidama region, southern Ethiopia.
Methods: We conducted a multicenter, cross-sectional study from April-1, to May-30, 2022. A total of 412 participants took part in the study, using an interviewer-administered structured questionnaire. The HRQoL was measured using the 12-item Short-Form Health Survey-Version 2 (SF-12v2) scale. To describe different variables, descriptive statistics were employed. To find independent HRQoL predictors, we used multivariable linear regression analysis. P-value of <0.05 were declared statistically significant at 95% confidence interval (CI).
Result: Out of 412 participants, nearly two-third 261 (63.3%) were male and nearly half 203 (49.3%) were diagnosed as schizophrenia. HRQoL was positively associated with social support (β = 0.321) and being single (β = 2.680). Conversely, functional disability (β = −0.545), being a student (β = −4.645) and jobless (β = −3.279) by occupation, and being diagnosed with depression (β = −2.839) were negatively impacted HRQoL among PWMI.
Conclusion: HRQoL of people with mental disorders in this study was significantly associated to social support, marital status, occupation, diagnosis and level of functional disability. Therefore, the mental health care system should develop HRQoL promoting measures that enhance PWMI functioning, social support and employment.
Mental illness (MI) is a term used to describe a range of mental health disorders characterized by mental, behavioral, or emotional impairments that have a significant impact on the functionality, major life activities, and quality of life of those suffering from the condition (1). Globally, the rise in overall morbidity and disability is mostly fueled by mental disorders (2, 3). Overtaking its other primary causes, such as non-communicable diseases and injuries, psychiatric disorders account for one-third (32.4%) of the years lived with disability burden (4). Depression, anxiety disorders, schizophrenia, and bipolar disorder are the most frequent mental disorders that lead to years lived with disability (YLDs) (5).
Mental illness is the most prevalent non-communicable disease in Ethiopia. Indeed, mental illness accounted for 11% of the total disease burden in a primarily rural area of Ethiopia, with schizophrenia and depression ranking among the top 10 highest burdens (6). According to a recent systematic review and meta-analysis, the prevalence of common mental illness is 21.6% in the general population and 36.4% in patients with co-morbid conditions (7). Rapidly spreading communicable diseases (like HIV and TB), non-communicable chronic diseases, unintended teenage pregnancies, malnutrition, and insecurity, including violence, may be intertwined with the rapidly rising pattern of these mental health issues in the country (7). Patients with severe mental illnesses have a lower quality of life than the general population (8), because their mental illness makes it harder for them to accomplish many of their daily tasks, reducing their level of independence and resulting low self-confidence and self-esteem.
Quality of life (QoL) and health-related quality of life (HRQoL) are terms that are frequently used interchangeably (9). QoL refers to an individual's subjective wellbeing in relation to their health, psychological condition, beliefs, interpersonal relationships, and relationship to significant environmental conditions such as living condition, security, accessibility to medical care, opportunity for recreation, and facilities (10). Furthermore, HRQoL is defined as a person's perceived wellbeing in physical, mental, and social domains of health, as well as how well they function in their daily lives (11). HRQoL is an important disease indicator in health care HRQoL can also be utilized to examine disease severity, treatment outcomes, client satisfaction with health care, effectiveness of healthcare, patients' overall wellbeing, and the expense of a specific intervention (12).
In recent years, QoL has been recognized as an important measure of disease impact among PWMI (8), and it has been shown to be considerably impaired in these individuals (13). Improving the HRQoL of PWMI in the community has also become an important public health agenda. Integration of social, psychological, and medical care is required to improve HRQoL (14, 15). PWMI have declining HRQOL, which is frequently equivalent to or greater than that of medical disorders (16). This has a substantial impact on treatment adherence, relapse rates, ability to engage in and/or enjoy social and vocational activities, future prospects, and medical issues (17).
A decline in HRQoL in individuals with mental illness has been demonstrated in several studies to be clinically significant. Socio-demographic variables like age, sex, marital status, living condition (18, 19), and low level of education (20) explained the variation in HRQoL in PWMI. Clinical factors such as being depressed, having positive and negative symptoms in schizophrenia, poor social support (21) and greater disability (20) predicted poor HRQoL in PWMI. Social support has been shown to boost self-esteem, coping abilities, and resilience while also minimizing stigma (22). A recent study also revealed that severity of symptoms, duration of treatment and number of hospitalization determines HRQoL among patients with schizophrenia and depression (23). Likewise, recent studies in Ethiopia elicited that age of onset of illness, perceived stigma, medication compliance, substance use, and comorbid medical illness are significantly impacted HRQoL among PWMI (24–26).
Severe mental illnesses may cause functional disability (27–30), that can significantly interfere with daily life activities, negatively impact health outcomes, and have a significant impact on patients QoL. The HRQoL of people with mental illness may be negatively impacted by functional restrictions brought on by a disability associated with mental illness (31).
Although, HRQoL is rapidly being recognized as an essential outcome in modern psychiatry, research on the relative impact of the co-occurrence of mental disorders is still in its early stages. The identification and significance of factors impacting HRQoL in PWMI is of special relevance because HRQoL is more frequently used as a patient-related outcome in research. Thus, the current study would look at the quality of life of those suffering from PWMI in southern Ethiopia. The purpose of this study was to fill the gap in the local literature by investigating the potential of accessible variables, specifically demographic and clinical parameters, and disability due to mental illness to predict HRQoL in patients with mental illness.
Institution based cross sectional study was conducted between April-1, and May-30, 2022 among patients with mental illnesses in selected hospitals in Sidama national regional state (Hawassa university comprehensive specialized hospital, Adare general hospital, and Yirgalem general hospital).
Four hundred and twelve participants were consecutively recruited from psychiatry outpatient clinics at the three selected hospitals in Sidama regional state, southern Ethiopia. Three hospitals (one specialized tertiary and two general hospitals) were chosen to provide outpatient services to those suffering from mental illnesses in the region and adjoining regions of the southern Nation Nationalities and People Region and Oromia. Eligibility requirements included a clinical diagnosis of mental disorders, being 18 or older, and being in a stable mental condition at the time of examination. To assess the current intensity of symptoms, the Clinical Global Impression Severity (CGI-S) Scale with a seven-point scale was utilized. The CGI-S scale spans from 1 (normal) to 7 (very unwell) (32). Patients with a CGI-S score of 6 or higher were excluded from the study because the intensity of their symptoms may prevent them from responding appropriately.
The data were collected using an interviewer-administered structured questionnaire. The questionnaire contains sociodemographic factors, clinical related factors, social support, disability related items, and health related HRQoL items. Some of the clinical factors such as clinical diagnosis, duration of illness, substance use history, and comorbidities were obtained from the patient's chart. Clinical diagnosis of mental disorders were made by psychiatrists, psychiatry nurses, and senior or expert mental health professionals based on the Diagnostic Statistical Manual for Mental Disorders-5 (DSM-5) diagnostic criteria.
Level of social support among patients with mental illness was assessed using the 3-item Oslo social support scale (OSSS) and the scores range from 3 to 14. It is categorized as poor [3–8], moderate [9–11], and strong [12–14] social support (33), and a higher score indicates better social support. In the previous study (24), it had a good internal consistency (Cronbach's alpha) of 0.93, and in the current study, it had an acceptable Cronbach's alpha of 0.75.
The World Health Organization Disability Assessment Schedule (WHODAS-2.0) 12-item version was used to assess functional disability. The WHODAS is a cross-cultural measure of a person's activity limitations and social restrictions in the last 30 days that is not condition specific (34). A number of research have established the WHODAS's psychometric properties (35, 36). The WHODAS has also been developed and validated in a variety of languages and cultures, including rural Ethiopia (37). In the current study, it had a very good Cronbach's alpha of 0.94.
To assess quality of life (QoL), the 12-item Short-Form Health Survey-Version 2 (SF-12v2) scale was used. It was designed to assess multidimensional elements of physical and mental health in the general population as well as people suffering from chronic conditions such as mental disorders, and a higher score indicates better self-reported QoL (38). The scale has eight (physical role, physical functioning, general health, body pain, social functioning, vitality, mental health, and emotional role) subdomains. Furthermore, two general scores were computed: the physical health component summary (PHCS) and the mental health component summary (MHCS), with higher score indicating greater QoL (39). Thus, SF-12 appears to be a reliable psychometric instrument for assessing HRQoL in PWMI (40). It has been validated and developed in varieties of settings and cultures with good psychometric properties (41–46). It had a very good Cronbach's alpha of 0.92 in the current study.
Collected data were entered to Epi-data version 3.1 and exported to SPSS version 24 for windows for analysis. Descriptive statistics such as frequency, percentage, mean, standard deviation, and median were used to describe different variables. Assumptions such as normality, lack of multi-collinearity among explanatory variables, presence of linearity relationship, independence and homoscedasticity of the errors were checked. Simple and multivariable linear regression were done to identify independent predictors of QoL among patients with mental illness. P-value of < 0.05 were declared statistically significant at 95% confidence interval (CI).
A total of 412 participants involved in the study. Nearly two-third 261 (63.3%) participants were male. About one-third 147 (35.7%) participants were at age group 18–27 years, 215 (52.2%) were single and 245 (59.5%) were protestant by religion (Table 1).
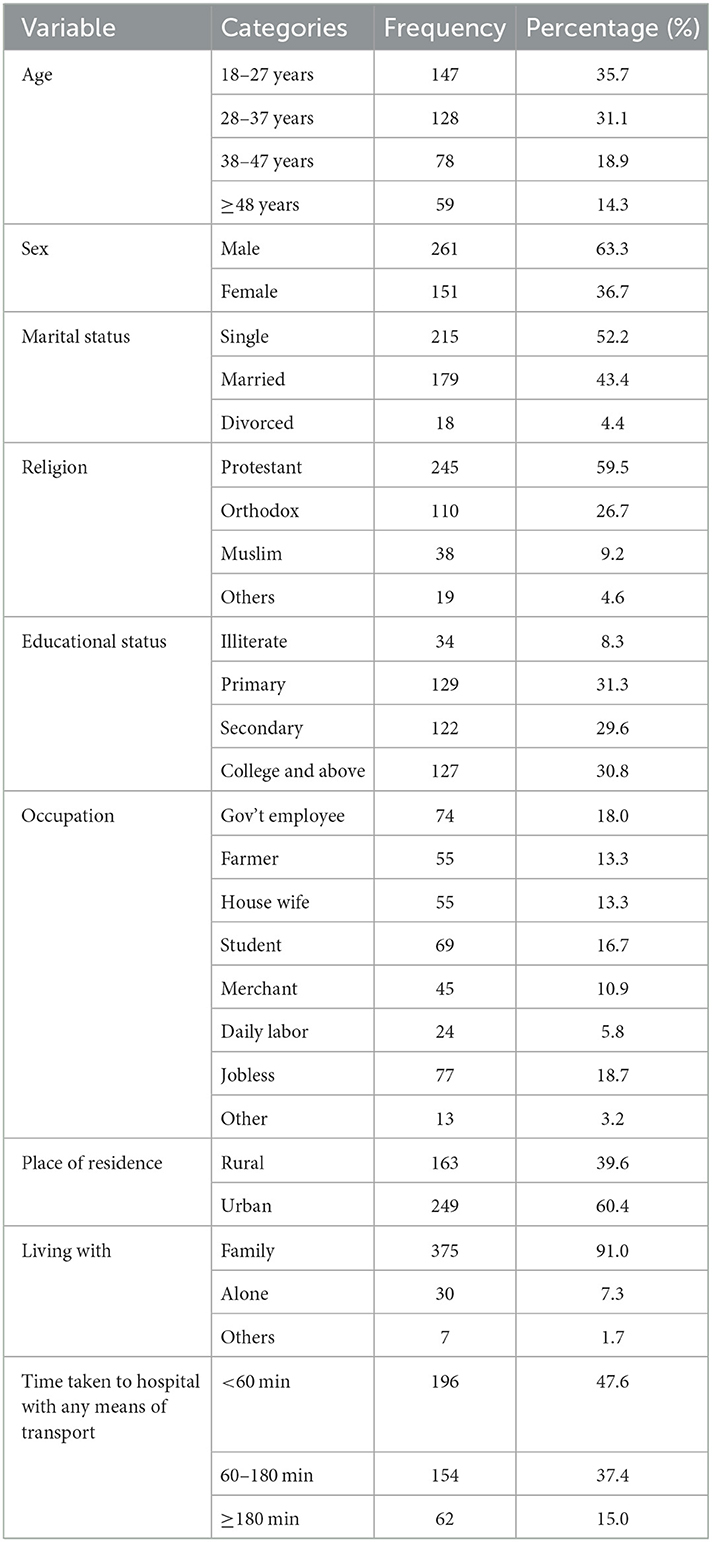
Table 1. Socio-demographic characteristics of study participants to HRQoL among people with mental illness in Sidama region, south Ethiopia, 2022 (n = 412).
Among the 412 participants, 161 (39.1%) reported the onset of their illness between the ages of 21 and 30 years. Furthermore, 158 (38.3%) had been ill for 1 year or less, about half 219 (53.2%) had a history of suicidal ideation, 120 (29.1%) had a lifetime history of substance use, and nearly half 203 (49.3%) were diagnosed with schizophrenia, as shown in Table 2.
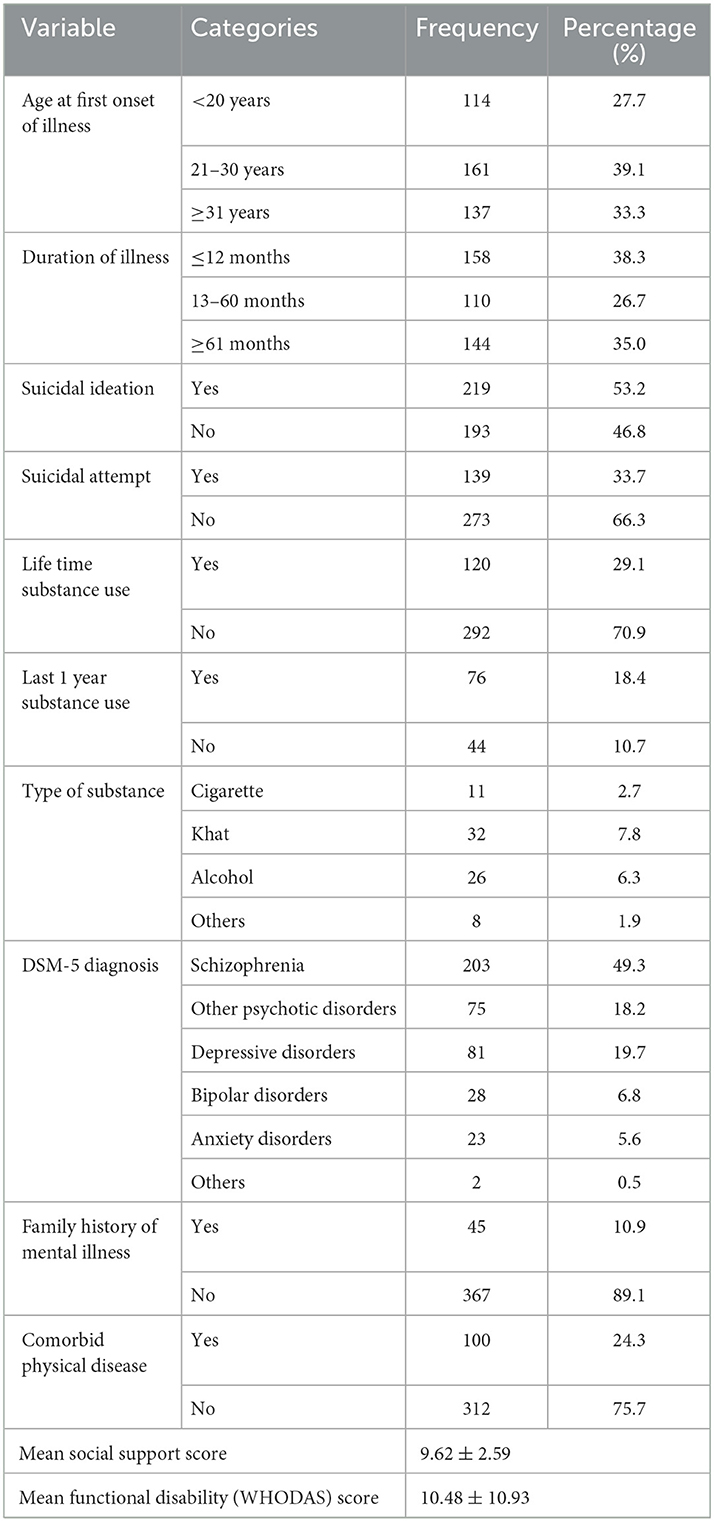
Table 2. Clinical characteristics of study participants to health related quality of life among people with mental illness in Sidama region, south Ethiopia, 2022 (n = 412).
The mean score of overall SF-12 (Health related quality of life) was 38.54 ± 10.33. Whereas, the mean physical health component and mental health component score were found to be 17.15 ± 4.37 and 21.38 ± 6.63, respectively as shown in Table 3.
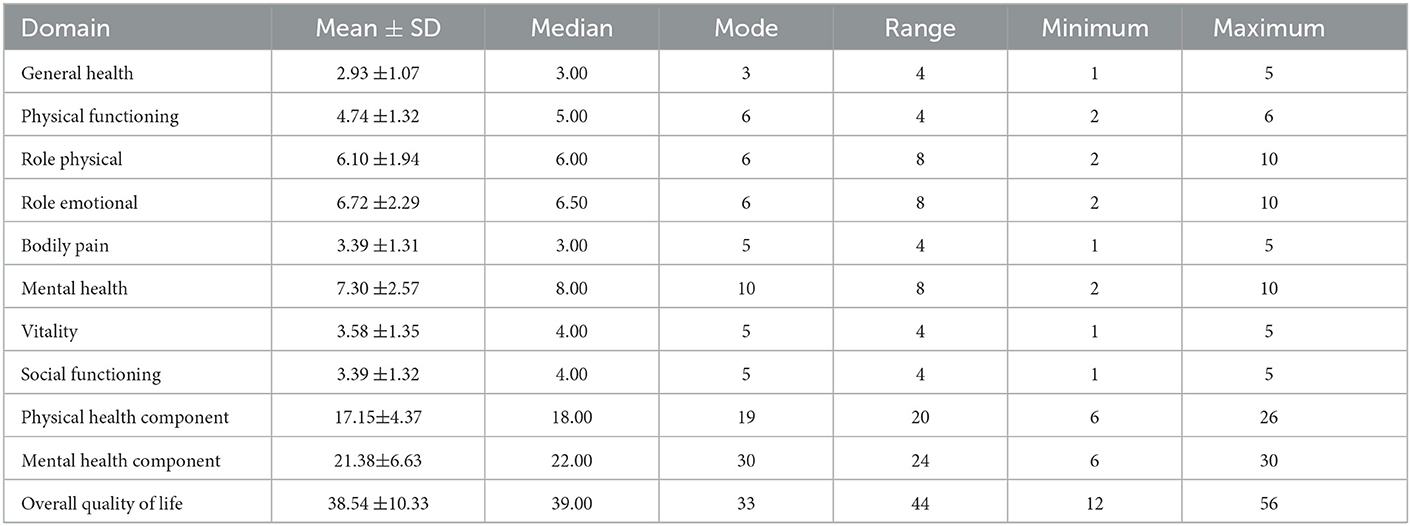
Table 3. Descriptive statistics of domains of health related quality of life among people with mental illness in Sidama region, south Ethiopia, 2022 (n = 412).
After controlling for confounding variables, we identified five independently significant predictors for HRQoL among PWMI. Those PWMI who had high social support scale score were better HRQoL (β = 0.321; 95% CI = 0.003, 0.639; p = 0.048). Functional disability (WHODAS-score) had significant negative impact on HRQoL among PWMI (β = −0.545; 95% CI = −0.620, −0.470; p = < 0.001). PWMI who were single had better HRQoL as compared to married individuals (β = 2.680; 95% CI = 0.571, 4.789; p = 0.013). Patients who were student (β = −4.645; 95% CI = −7.865, −1.424; p = < 0.001) and jobless (β = −3.279; 95% CI = −6.193, −0.365; p = 0.028) by occupation had lower HRQoL scores as compared to employed patients. In addition, patients with depression were lower HRQoL score as compared to patients with schizophrenia (β = −2.839; 95% CI = −5.110, −0.568; p = 0.014) as described in Table 4.
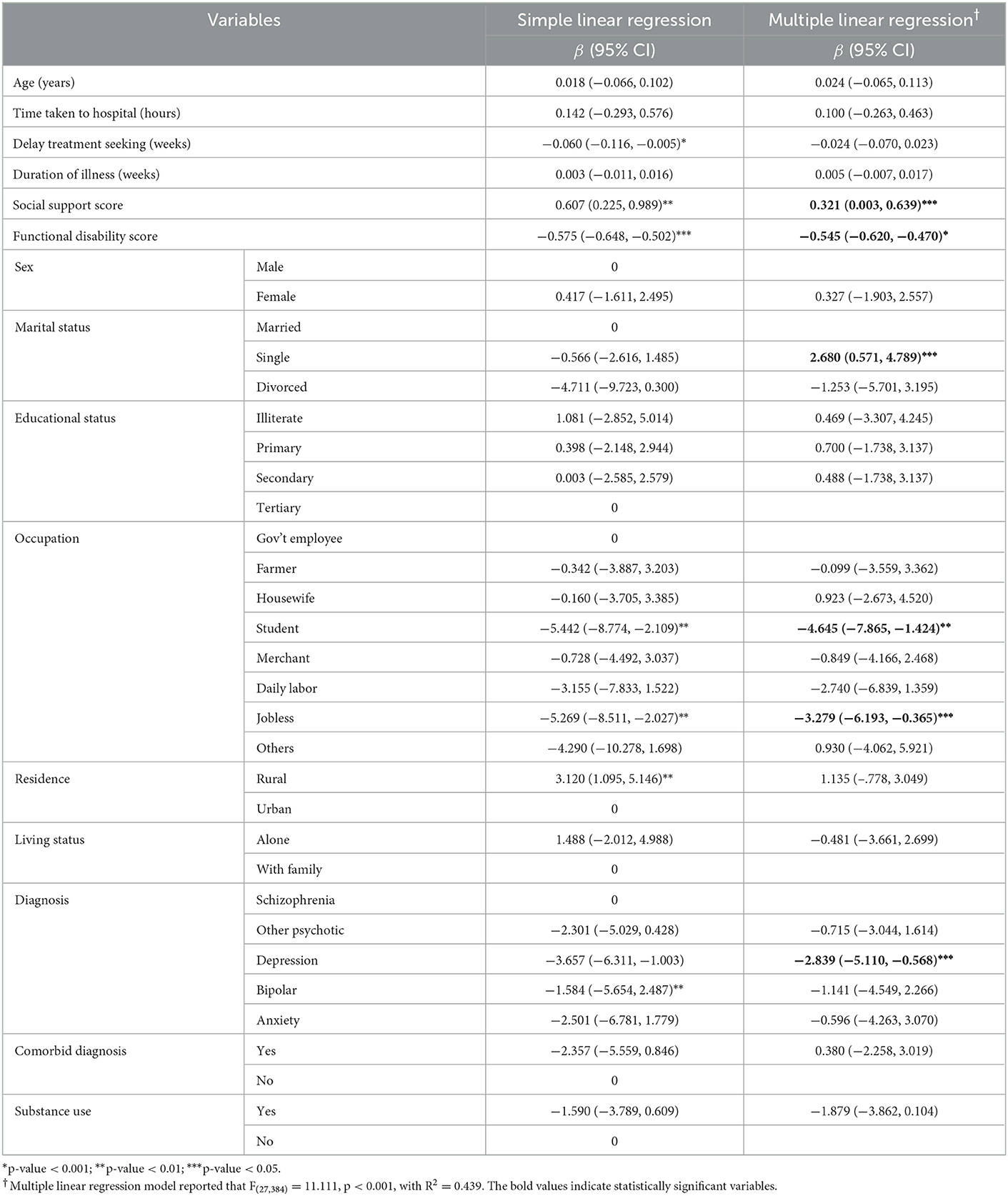
Table 4. Simple and multiple linear regression for health related quality of life among patients with mental illness in Sidama regional state, southern Ethiopia, 2022 (n = 412).
We evaluated all patients with a diagnosis of mental disorders who attended follow-up at public hospitals in Sidama National Regional State in the current study. Taking into account the variety of mental illness outcomes (47, 48), sociodemographic, general clinical characteristics and functional impairment, as well as health related quality of life, were evaluated in order to confirm the association between these variables and health related quality of life. Hence, good social support and being single was positively associated with QoL, however, functional disability, being student and jobless by occupation, and diagnosed with depression were negatively affect HRQoL in PWMI.
Regarding the association of social support and QoL, we found a statistically significant association between OSSS and HRQoL. In the current study, a higher social support score among those with mental illness is a significant positive predictor of a greater HRQoL. This finding is supported by other studies done in Ethiopia (24) and other parts of the world (49–52). Cohen et al., discovered that the absence of loneliness and consistent social interactions predicted subjective wellbeing in people with severe mental illness such as schizophrenia (53). Poor social support is associated with depression and non-compliance to treatment (54, 55). On other hand, adequate social support has been shown to boost resilience, coping mechanisms, self-esteem, lowering stigma and improving life satisfaction (22, 56). As a result, social support may increase HRQoL by buffering stress, lowering depression, and boosting the adaption process (57).
Similar to previous studies (58, 59), in this study, the HRQoL of people with mental illness was negatively associated to their level of functioning/disability status, which might be represented in low employment rates and social interactions. Researchers have discovered that a worse HRQoL is connected with the incapacity to perform functional life tasks, such as activities of daily living such as bathing, dressing and instrumental activities of daily living like driving, budgeting (31, 60). Disability associated with mental illness can cause impairments, limitations, and restrictions to activities and participation in relation to the environment which may compromise HRQoL (59). This suggests that HRQoL and functioning can be employed as essential parameters in the creation of mental healthcare strategies, health condition monitoring, and social reintegration of these persons, hence helping the introduction of new assisted living facilities and enhancing the existing one. Furthermore, finding the consequences of the condition is important for choosing more effective treatments and determining the best strategies for public resource allocation. The functioning assessment and limitations of the person with mental disorders play a vital role in this process (61).
We found out that being single increases HRQoL scores as compared to married PWMI. Similar findings in earlier study reported that single women and single participants 30–39 years old had higher HRQoL (62). The fact that being married increases societal burdens such as shouldering family responsibilities could explain why single PWMI had greater HRQoL in our study. As a result, married individuals may have a negative perspective of their HRQoL, such as feeling like a burden to their families, failing to care for children or other family members, and failing to appropriately handle duty. Furthermore, problems among married people are related to the partner, such as challenging marital intimacy and commonality, restructuring of familial and partnership responsibilities, and reinterpretation of mutual life plans (63). However, other reports also indicated that being married predicts better HRQoL (64). That is, those who have a partner are more likely to express their emotions, daily experiences, and thoughts, as well as receive enough social support, resulting in a good outlook on life.
In this study we found that students and jobless patients have lower HRQoL score than the employed patients. Similarly, other studies have found that employed patients have higher HRQoL scores than those who are unemployed (65–68). This could be explained by higher self-esteem among patients with employment, which has been described as a moderating factor between employment and HRQoL, as well as having a larger social network as a result of employment (69, 70). Moreover, the relationship between employment status and HRQoL in our study may be due to differences in income because employed patients had higher source of income while students and unemployed patients may not have had enough income to cover their basic needs.
We also found that patients diagnosed with depression have decreased HRQoL than patients with schizophrenia. Similarly, depression has been identified as a critical predictor of subjective HRQoL in prior studies (68, 71, 72). Also, low HRQoL has been associated to depression among outpatients in Spanish and French studies (73, 74). This is due to the fact that patients suffering from psychosis were unaware of their condition and social milieu. Individuals with depression, on the other hand, have symptoms such as anhedonia, depressed mood, pessimistic outlook, decreased motivation and energy level, and are thus more likely to report poor HRQoL than patients with schizophrenia (75). Therefore, the possibility that depressed individuals may have unfavorable perceptions of their circumstances, could have a detrimental impact on how they perceive their HRQoL.
The following limitations should be kept in mind in this study. Firstly, this study only used cross-sectional data. Therefore, no causal relationships could be identified. Secondly, HRQoL and disability were self-reported, which might be prone to social desirability bias. Thirdly, some clinical factors like treatment adherence, adverse drug reactions, and the types of medications the participants had taken were not addressed in this study. Lastly, our results might only apply to people who are actively engaged in treatment. Thus, the results of this research may not accurately reflect the experiences of PWMI who do not actively involved in modern psychiatry care. Therefore, additional research is required to confirm and broaden the findings in various individuals with mental disorders, including those PWMI outside the formal mental healthcare system.
In conclusion, the HRQoL of people with mental disorders in this study was significantly associated to their social support, marital status, occupation, diagnosis and level of disability due to their mental illness. Taking into account all of these variables, the mental health care system should develop HRQoL promoting measures that enhance PWMI functioning, social support and employment.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Hawassa University, College of Medicine and Health Sciences, Institutional Review Board (IRB) with reference number: IRB/030/14. The participants provided their written informed consent to participate in this study. This study complies with the Declaration of Helsinki.
SD, MA, BD, YA, YR, and MJ participated in the conception and designed the study and involved in the data collection. SD, MA, YA, TY, KK, BB, and MJ did the analysis of the study. SD, MA, and MJ prepared the manuscript for publication. BD, YA, YR, TY, KK, and BB critically reviewed the manuscript. All authors read and approved the final manuscript.
This study was financially supported by Hawassa University.
We would like to thank Hawassa University for providing fund to conduct this study. Our heartfelt gratitude also goes to the data collectors and participants for their valuable contributions to the study process.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
CGI-S, Clinical Global Impression Severity; CI, Confidence interval; MHCS, Mental Health Component Summary; PHCS, Physical health component summary; PWMI, People with mental illness; QoL, Quality of life; SF-12, Short-Form Health Survey-12; WHODAS, World Health Organization Disability Assessment Schedule.
1. World Health Organization (WHO). Mental Health Action Plan 2013–2020. World Health Organization [Internet] (2013). Available online at: https://apps.who.int/iris/handle/10665/89966
2. Prince M, Patel V, Saxena S, Maj M, Maselko J, Phillips MR, et al. No health without mental health. Lancet. (2007) 370:859–77. doi: 10.1016/S0140-6736(07)61238-0
3. Alonso J, Chatterji S, He Y. The Burdens of Mental Disorders: Global Perspectives From the WHO World Mental Health Surveys. Cambridge: Cambridge University Press (2013).
4. Vigo D, Thornicroft G, Atun R. Estimating the true global burden of mental illness. Lancet Psychiatry. (2016) 3:171–8. doi: 10.1016/S2215-0366(15)00505-2
5. Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet. (2015) 386:743–800. doi: 10.1016/S0140-6736(15)60692-4
6. Fekadu A, Thornicroft G. Global mental health: Perspectives from Ethiopia. Glob Heal Action. (2014) 7:25447. doi: 10.3402/gha.v7.25447
7. Kassa GM, Abajobir AA. Prevalence of common mental illnesses in Ethiopia: A systematic review and meta-analysis. Neurol Psychiatry Brain Res. (2018) 30:74–85. doi: 10.1016/j.npbr.2018.06.001
8. Berghöfer A, Martin L, Hense S, Weinmann S, Roll S. Quality of life in patients with severe mental illness: A cross-sectional survey in an integrated outpatient health care model. Qual Life Res. (2020) 29:2073–87. doi: 10.1007/s11136-020-02470-0
9. Karimi M, Brazier J. Health, health-related quality of life, and quality of life: What is the difference? Pharmacoeconomics. (2016) 34:645–9. doi: 10.1007/s40273-016-0389-9
10. World Health Organization. Promoting Mental Health: Concepts, Emerging Evidence, Practice (Summary Report). Geneva: WHO (2004).
11. Hays RD, Reeve BB. Measurement and modeling of health-related quality of life. In:J Killewo, HK Heggenhougen, , editor, Epidemiology and Demography in Public Health. San Diego, CA: Academic Press (2010). p. 195–205.
12. Kaso A, Agero G, Hurisa Z, Kaso T, Ewune HA, Hailu A. Evaluation of health-related quality of life of COVID-19 patients: A hospital-based study in South Central Ethiopia. Heal Qual Life Outcomes. (2021) 19:268. doi: 10.1186/s12955-021-01900-y
13. Evans S, Banerjee S, Leese M, Huxley P. The impact of mental illness on quality of life: A comparison of severe mental illness, common mental disorder and healthy population samples. Qual Life Res. (2007) 16:17–29. doi: 10.1007/s11136-006-9002-6
14. CDC. Health-Related Quality of Life (HRQOL). Centers for Disease Control and Prevention. (2019). Available online at: https://www.cdc.gov/hrqol/concept.htm (accessed January 23, 2023).
15. Nakamura H, Watanabe N, Matsushima E. Structural equation model of factors related to quality of life for community-dwelling schizophrenic patients in Japan. Int J Ment Health Syst. (2014) 8:1–12. doi: 10.1186/1752-4458-8-32
16. Bonicatto S, Dew M, Zaratiegui R, Lorenzo L, Pecina P. Adult outpatients with depression: Worse quality of life than in other chronic medical diseases in Argentina. Soc Sci Med. (2001) 52:911–9. doi: 10.1016/S0277-9536(00)00192-1
17. Papakostas GI, Petersen T, Mahal Y, Mischoulon D, Nierenberg AA, Fava M. Quality of life assessments in major depressive disorder: A review of the literature. Gener Hosp Psychiatry. (2004) 26:13–7. doi: 10.1016/j.genhosppsych.2003.07.004
18. Trompenaars FJ, Masthoff ED, Van Heck GL, De Vries J, Hodiamont PP. Relationships between social functioning and quality of life in a population of Dutch adult psychiatric outpatients. Int J Soc Psychiatry. (2007) 53:36–47. doi: 10.1177/0020764006074281
19. Berlim MT, McGirr A, Fleck MP. Can sociodemographic and clinical variables predict the quality of life of outpatients with major depression? Psychiatry Res. (2008) 160:364–71. doi: 10.1016/j.psychres.2007.07.024
20. Ruggeri M, Nosè M, Bonetto C, Cristofalo D, Lasalvia A, Salvi G, et al. Changes and predictors of change in objective and subjective quality of life: Multiwave follow-up study in community psychiatric practice. Br J Psychiatry. (2005) 187:121–30. doi: 10.1192/bjp.187.2.121
21. Wang XQ, Petrini MA, Morisky DE. Predictors of quality of life among Chinese people with schizophrenia. Neuropsychiatr Dis Treat. (2015) 11:1371–9. doi: 10.1111/nhs.12286
22. Hardy SE, Concato J, Gill TM. Resilience of community-dwelling older persons. J Am Geriatr Soc. (2004) 52:257–62. doi: 10.1111/j.1532-5415.2004.52065.x
23. Choo CC, Chew PKH, Ho CS, Ho RC. Quality of life in patients with a major mental disorder in Singapore. Front Psychiatry. (2019) 10:1–7. doi: 10.3389/fpsyt.2018.00727
24. Shumye S, Amare T, Derajew H, Endris M, Molla W, Mengistu N. Perceived quality of life and associated factors among patients with severe mental illness in Ethiopia: A cross-sectional study. BMC Psychol. (2021) 9:1–8. doi: 10.1186/s40359-021-00664-w
25. Desalegn D, Girma S, Abdeta T. Quality of life and its association with current substance use, medication non-adherence and clinical factors of people with schizophrenia in Southwest Ethiopia: A hospital-based cross-sectional study. Health Qual Life Outcomes. (2020) 18:1–10. doi: 10.1186/s12955-020-01340-0
26. Desalegn D, Girma S, Tessema W, Yeshigeta E, Kebeta T. Quality of life and associated factors among patients with schizophrenia attending follow-up treatment at Jimma Medical Center, Southwest Ethiopia: A cross-sectional study. Psychiatry J. (2020) 2020:1–7. doi: 10.1155/2020/4065082
27. Zhigang Xie R. Catherine L, Striley NMM. Association of functional disability with mental health services use and perceived unmet needs for mental health care among adults with serious mental illness. J Affect Disord. (2022) 299:449–55. doi: 10.1016/j.jad.2021.12.040
28. Tesfaye E, Kassaw C, Agenagnew L. Functional disability in patients with mood disorders at St Paul's Hospital Psychiatry Clinic, Addis Ababa, Ethiopia, 2019. Patient Relat Outcome Meas. (2021) 12:181–9. doi: 10.2147/PROM.S295680
29. Habtamu K, Medhin G, Selamu M, Tirfessa K, Hanlon C, Fekadu A. Functional impairment among people diagnosed with depression in primary healthcare in rural Ethiopia: A comparative cross-sectional study. Int J Ment Health Syst. (2019) 13:1–12. doi: 10.1186/s13033-019-0305-8
30. Isaacson D, Mueller JL, Article R. Impairment in role functioning in mental and chronic medical disorders in the United States: Results from the national comorbidity survey replication. Mol Psychiatry. (2009) 14:728–37. doi: 10.1038/mp.2008.13
31. Sánchez J, Rosenthal DA, Tansey TN, Frain MP, Bezyak JL. Predicting quality of life in adults with severe mental illness: Extending the international classification of functioning disability, and health. Rehabil Psychol. (2016) 61:19–31. doi: 10.1037/rep0000059
32. Haro JM, Kamath SA, Ochoa S, Novick D, Rele K, Fargas A, et al. The clinical global ImpressionSchizophrenia scale: A simple instrument to measure the diversity of symptoms present in schizophrenia. Acta Psychiatr Scand. (2003) 1073:16–2. doi: 10.1034/j.1600-0447.107.s416.5.x
33. Hege B, Odd Steffen Dalgard EB. The importance of social support in the associations between psychological distress and somatic health problems and socio-economic factors among older adults living at home : A cross sectional study. BMC Geriatr. (2012) 12:27. doi: 10.1186/1471-2318-12-27
34. Silva C, Coleta I, Silva AG, Amaro A, Alvarelhão J, Queirós A, Rocha N. Adaptation and validation of WHODAS 20 in patients with musculoskeletal pain. Rev Saúde Pública. (2013) 47:1–6. doi: 10.1590/S0034-8910.2013047004374
35. Downing NR, Kim J-I, Williams JK, Long JD, Mills JA, Paulsen JS. WHODAS 20 in prodromal Huntington disease: measures of functioning in neuropsychiatric disease. Eur J Hum Genet. (2014) 22:958–63. doi: 10.1038/ejhg.2013.275
36. Gold LH. DSM-5 and the assessment of functioning: The World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0). J Am Acad Psychiatry Law. (2014) 42:173–81.
37. Habtamu K, Alem A, Medhin G, Fekadu A, Dewey M, Prince M, et al. Validation of the World Health Organization Disability Assessment Schedule in people with severe mental disorders in rural Ethiopia. Health Qual Life Outcomes. (2017) 15:1–11. doi: 10.1186/s12955-017-0647-3
38. Ware JE Jr, Kosinski M, Keller SD. A 12-item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med Care. (1996) 34:220–33. doi: 10.1097/00005650-199603000-00003
39. Ramírez-Vélez R, Agredo-Zuñiga RA, Jerez-Valderrama AM. The reliability of preliminary normative values from the short form health survey (SF-12) questionnaire regarding Colombian adults. Rev Salud Pública. (2010) 12:807–19.
40. Salyers MP, Bosworth HB, Swanson JW, Lamb-Pagone J, Osher FC. Reliability and validity of the SF-12 health survey among people with severe mental illness. Med Care. (2000) 38:1141–50. doi: 10.1097/00005650-200011000-00008
41. Gandhi SK, Warren Salmon J, Zhao SZ, Lambert BL, Gore PR, Conrad K. Psychometric evaluation of the 12-Item Short-Form Health Survey (SF-12) in osteoarthritis and rheumatoid arthritis clinical trials. Clin Ther. (2001) 23:1080–98. doi: 10.1016/S0149-2918(01)80093-X
42. Damásio BF, Andrade TF, Koller SH. Psychometric properties of the Brazilian 12-item short-form health survey version 2 (SF-12v2). Paideia. (2015) 25:29–37. doi: 10.1590/1982-43272560201505
43. Ibrahim AA, Akindele MO, Ganiyu SO, Kaka B, Abdullahi BB, Sulaiman SK, et al. The Hausa 12-item short-form health survey (SF-12): Translation, cross-cultural adaptation and validation in mixed urban and rural Nigerian populations with chronic low back pain. PLoS ONE. (2020) 15:1–19. doi: 10.1371/journal.pone.0232223
44. Haddad C, Sacre H, Obeid S, Salameh P, Hallit S. Validation of the Arabic version of the “12-item short-form health survey” (SF-12) in a sample of Lebanese adults. Arch Public Heal. (2021) 79:1–8. doi: 10.1186/s13690-021-00579-3
45. Huo T, Guo Y, Shenkman E, Muller K. Assessing the reliability of the short form 12 (SF-12) health survey in adults with mental health conditions: A report from the wellness incentive and navigation (WIN) study. Health Qual Life Outcomes. (2018) 16:1–8. doi: 10.1186/s12955-018-0858-2
46. Shou J, Ren L, Wang H, Yan F, Cao X, Wang H, et al. Reliability and validity of 12-item Short-Form health survey (SF-12) for the health status of Chinese community elderly population in Xujiahui district of Shanghai. Aging Clin Exp Res. (2016) 28:339–46. doi: 10.1007/s40520-015-0401-9
47. Vaingankar JA, Chong SA, Abdin E, Siva Kumar FD, Chua BY, Sambasivam R, et al. Understanding the relationships between mental disorders, self-reported health outcomes and positive mental health: Findings from a national survey. Health Qual Life Outcomes. (2020) 18:1–10. doi: 10.1186/s12955-020-01308-0
48. Barbalat G, Van Den Bergh D, Kossakowski JJ. Outcome measurement in mental health services: Insights from symptom networks. BMC Psychiatry. (2019) 19:1–9. doi: 10.1186/s12888-019-2175-7
49. Xiang Y-T, Hou Y-Z, Yan F, Dixon LB, Ungvari GS, Dickerson F, et al. Quality of life in community-dwelling patients with schizophrenia in China. J Nerv Ment Dis. (2012) 200:584–7. doi: 10.1097/NMD.0b013e31825bfc71
50. Ribas AC, Lam CS. Social support and quality of life among Latinos with mental illness. J Nerv Ment Dis. (2010) 198:137–43. doi: 10.1097/NMD.0b013e3181cc522d
51. Kuehner C, Beuger C. Determinants of subjective quality of life in depressed patients: The role of self-esteem, response styles, and social support. J Affect Disord. (2005) 86:205–13. doi: 10.1016/j.jad.2005.01.014
52. Chung L, Pan A-W, Hsiung PC. Quality of life for patients with major depression in Taiwan: A model-based study of predictive factors. Psychiatry Res. (2009) 168:153–62. doi: 10.1016/j.psychres.2008.04.003
53. Cohen CI, Talavera N. Predictors of subjective well-being among older, community-dwelling persons with schizophrenia. Am J Geriatr Psychiatry. (1997) 5:145–55. doi: 10.1097/00019442-199721520-00007
54. Suttajit S, Pilakanta S. Prevalence of and factors associated with depression in patients with schizophrenia in Thailand: A post-hoc analysis. Chiang Mai Med J. (2011) 50:115–21. Available online at: https://thaiscience.info/Journals/Article/CMMJ/10886618.pdf
55. Suttajit S, Punpuing S, Jirapramukpitak T, Tangchonlatip K, Darawuttimaprakorn N, Stewart R, et al. Impairment, disability, social support and depression among older parents in rural Thailand. Psychol Med. (2010) 40:1711–21. doi: 10.1017/S003329170999208X
56. Clinton M, Lunney P, Edwards H, Weir D, Barr J. Perceived social support and community adaptation in schizophrenia. J Adv Nurs. (1998) 27:955–65. doi: 10.1046/j.1365-2648.1998.t01-1-00573.x
57. Caron J, Lecomte Y, Stip E, Renaud S. Predictors of quality of life in schizophrenia. Community Ment Heal J. (2005) 41:399–417. doi: 10.1007/s10597-005-5077-8
58. Gowda GS, Komal S, Sanjay TN, Mishra S, Kumar CN, Math SB. Sociodemographic, legal, and clinical profiles of female forensic inpatients in Karnataka: A retrospective study. Indian J Psychol Med. (2019) 41:138–43. doi: 10.4103/IJPSYM.IJPSYM_152_18
59. Mayer RCF, Alves MR, Yamauti SM, Silva MT, Lopes LC. Quality of life and functioning of people with mental disorders who underwent deinstitutionalization using assisted living facilities: A cross-sectional study. Front Psychol. (2021) 12:1–11. doi: 10.3389/fpsyg.2021.622973
60. Norman RMG, Malla AK, McLean T, Voruganti LPN, Cortese L, McIntosh E, et al. The relationship of symptoms and level of functioning in schizophrenia to general wellbeing and the Quality of Life Scale. Acta Psychiatr Scand. (2000) 102:303–9. doi: 10.1034/j.1600-0447.2000.102004303.x
61. Silveira C, Parpinelli MA, Pacagnella RC, de Camargo RS, Costa ML, Zanardi DM, et al. Cross-cultural adaptation of the World Health Organization Disability Assessment Schedule (WHODAS 20) into Portuguese. Rev Assoc Med Bras. (2013) 59:234–40. doi: 10.1016/S2255-4823(13)70462-4
62. Han KT, Park EC, Kim JH, Kim SJ, Park S. Is marital status associated with quality of life? Health Qual Life Outcomes. (2014) 12:1–10. doi: 10.1186/s12955-014-0109-0
63. Jungbauer J. Living with a schizophrenic patient: A comparative study of burden as it affects parents and spouses. Psychiatry. (2002) 65:110–23. doi: 10.1521/psyc.65.2.110.19930
64. Gutiérrez-Vega M, Esparza-Del Villar OA, Carrillo-Saucedo IC, Montañez-Alvarado P. The possible protective effect of marital status in quality of life among elders in a US-Mexico Border City Community. Ment Health J. (2018) 54:480–4. doi: 10.1007/s10597-017-0166-z
65. Hsiao CY, Hsieh MH, Tseng CJ, Chien SH, Chang CC. Quality of life of individuals with schizophrenia living in the community: Relationship to socio-demographic, clinical and psychosocial characteristics. J Clin Nurs. (2012) 21:2367–76. doi: 10.1111/j.1365-2702.2012.04067.x
66. Alonso J, Croudace T, Brown J, Gasquet I, Knapp MR, Suárez D, et al. Health-related quality of life (HRQL) and continuous antipsychotic treatment: 3-year results from the Schizophrenia Health Outcomes (SOHO) study. Value Heal. (2009) 12:536–43. doi: 10.1111/j.1524-4733.2008.00495.x
67. Haro JM, Novick D, Perrin E, Bertsch J, Knapp M. Symp- tomatic remission and patient quality of life in an observational study of schizophrenia: Is there a relationship? Psychiatry Res. (2014) 15:163–9. doi: 10.1016/j.psychres.2014.07.034
68. Arraras JI, Ibañez B, Basterra I, Pereda N, Martin M, Iribarren S. Determinants of Quality of Life in Spanish outpatients with schizophrenia spectrum disorders. Eur J Psychiatry. (2018) 32:113–21. doi: 10.1016/j.ejpsy.2017.11.001
69. Tan XW, Shahwan S, Satghare P, Chua BY, Verma S, Tang C, et al. Trends in subjective quality of life among patients with first episode psychosis—A 1 year longitudinal study. Front Psychiatry. (2019) 10:1–10. doi: 10.3389/fpsyt.2019.00053
70. Caron J, Mercier C, Diaz P, Martin A. Socio-demographic and clinical predictors of quality of life in patients with schizophrenia or schizo-affective disorder. Psychiatry Res. (2005) 137:203–13. doi: 10.1016/j.psychres.2005.07.002
71. Strauss GP, Sandt AR, Catalano LT, Allen DN. Negative symptoms and depression predict lower psychological well- being in individuals with schizophrenia. Compr Psychiatry. (2012) 53:1137–44. doi: 10.1016/j.comppsych.2012.05.009
72. Fleury MJ, Grenier G, Bamvita JM, Tremblay J, Schmitz N, Caron J. Predictors of quality of life in a longitudinal study of users with severe mental disorders. Heal Qual Life Outcomes. (2013) 11:92. doi: 10.1186/1477-7525-11-92
73. Yamauchi K, Aki H, Tomotake M, Iga J, Numata S, Motoki I, et al. Predictors of subjective and objective quality of life in outpatients with schizophrenia. Psychiatry Clin Neurosci. (2008) 62:404–11. doi: 10.1111/j.1440-1819.2008.01818.x
74. Maurino J, Sanjúan J, Haro JM, Díez T, Ballesteros J. Impact of depressive symptoms on subjective well-being: The importance of patient-reported outcomes in schizophrenia. Patient Prefer Adherence. (2011) 5:471–4. doi: 10.2147/PPA.S24479
Keywords: health related quality of life, functional disability, predictors, mental illness, SF-12
Citation: Defar S, Abraham Y, Reta Y, Deribe B, Jisso M, Yeheyis T, Kebede KM, Beyene B and Ayalew M (2023) Health related quality of life among people with mental illness: The role of socio-clinical characteristics and level of functional disability. Front. Public Health 11:1134032. doi: 10.3389/fpubh.2023.1134032
Received: 29 December 2022; Accepted: 30 January 2023;
Published: 16 February 2023.
Edited by:
S. M. Yasir Arafat, Enam Medical College, BangladeshReviewed by:
Anitha Jeyagurunathan, Institute of Mental Health, SingaporeCopyright © 2023 Defar, Abraham, Reta, Deribe, Jisso, Yeheyis, Kebede, Beyene and Ayalew. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohammed Ayalew,  bWFtZWF5YWxlQGdtYWlsLmNvbQ==
bWFtZWF5YWxlQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.