 Daniela Andrea Paira1,2
Daniela Andrea Paira1,2 José Javier Olmedo3Carolina Olivera1,2
José Javier Olmedo3Carolina Olivera1,2 Andrea Daniela Tissera4
Andrea Daniela Tissera4 Rosa Isabel Molina4
Rosa Isabel Molina4 Virginia Elena Rivero1,2
Virginia Elena Rivero1,2 Rubén Darío Motrich1,2*†
Rubén Darío Motrich1,2*† Héctor Alex Saka1,2*†
Héctor Alex Saka1,2*†- 1Centro de Investigaciones en Bioquímica Clínica e Inmunología (CIBICI), CONICET, Córdoba, Argentina
- 2Departamento de Bioquímica Clínica, Facultad de Ciencias Químicas, Universidad Nacional de Córdoba, Córdoba, Argentina
- 3Fundación Urológica Córdoba para la Docencia e Investigación Médica (FUCDIM), Córdoba, Argentina
- 4Laboratorio de Andrología y Reproducción (LAR), Córdoba, Argentina
Chlamydia trachomatis is an obligate intracellular pathogen and the leading bacterial cause of sexually transmitted infections worldwide. Chlamydia trachomatis genovars L1–L3 are responsible for lymphogranuloma venereum (LGV), an invasive sexually transmitted disease endemic in tropical and subtropical regions of Africa, South America, the Caribbean, India and South East Asia. The typical signs and symptoms of C. trachomatis LGV urogenital infections in men include herpetiform ulcers, inguinal buboes, and/or lymphadenopathies. Since 2003, endemic cases of proctitis and proctocolitis caused by C. trachomatis LGV emerged in Europe, mainly in HIV-positive men who have sex with men (MSM). Scarce data have been reported about unusual clinical presentations of C. trachomatis LGV urogenital infections. Herein, we report a case of a 36-year-old heterosexual, HIV-negative male declaring he did not have sex with men or trans women, who presented to the Urology and Andrology outpatient clinic of a healthcare center from Cordoba, Argentina, with intermittent testicular pain over the preceding 6 months. Doppler ultrasound indicated right epididymitis and funiculitis. Out of 17 sexually transmitted infections (STIs) investigated, a positive result was obtained only for C. trachomatis. Also, semen analysis revealed oligoasthenozoospermia, reduced sperm viability as well as increased sperm DNA fragmentation and necrosis, together with augmented reactive oxygen species (ROS) levels and the presence of anti-sperm IgG autoantibodies. In this context, doxycycline 100 mg/12 h for 45 days was prescribed. A post-treatment control documented microbiological cure along with resolution of clinical signs and symptoms and improved semen quality. Strikingly, sequencing of the ompA gene revealed C. trachomatis LGV L2 as the causative uropathogen. Remarkably, the patient did not present the typical signs and symptoms of LGV. Instead, the infection associated with chronic testicular pain, semen inflammation and markedly reduced sperm quality. To our knowledge, this is the first reported evidence of chronic epididymitis due to C. trachomatis LGV L2 infection in an HIV-negative heterosexual man. These findings constitute important and valuable information for researchers and practitioners and highlight that C. trachomatis LGV-L2 should be considered as putative etiologic agent of chronic epididymitis, even in the absence of the typical LGV signs and symptoms.
Introduction
Chlamydia trachomatis is an obligate intracellular bacterium and the etiologic agent of a range of oculo-genital infections representing a huge burden to public health. Based on the variable domains of the major outer membrane protein (MOMP), this bacterium can be sub-classified into genovars A to L. This classification is epidemiologically relevant since different genovars are associated to specific diseases. Genovars A–C are the causative agents of endemic trachoma, a chronic infection of the eye's conjunctiva and the leading cause of infectious blindness (1–3). Genovars D–K are the most frequent bacterial cause of sexually transmitted infections (STI) worldwide, with urethritis and cervicitis being the main clinical presentations in males and females, respectively (1, 3, 4). Noteworthy, more than 50% of C. trachomatis genital infections caused by genovars D–K have been estimated to be asymptomatic and long-lasting, producing repeated cycles of tissue damage and scarring that can ultimately result in pelvic inflammatory disease, ectopic pregnancy and irreversible infertility in women (3, 5, 6). On the other hand, C. trachomatis genovars L1, L2, L3, and its subvariants are responsible for lymphogranuloma venereum (LGV), a relatively infrequent and invasive sexually transmitted disease (3, 7). Most LGV cases occur in endemic, tropical and subtropical regions of Africa, South America and the Caribbean, India and South East Asia (8).
The classical manifestations of LGV involve three consecutive stages. The first stage occurs up to a month upon infection and may present with symptoms of urethritis, cervicitis, proctitis or it can even be asymptomatic. This stage implies the formation of a primary lesion at the site of inoculation, usually a papule or small herpetiform ulcer that heals spontaneously in a few days. In the second stage, which develops days to weeks upon the resolution of the primary lesion, the bacteria disseminate via the lymphatics and proliferate within lymph nodes and surrounding tissues close to the inoculation site causing inflammation, lymphadenopathy, systemic symptoms and typically the formation of inguinal buboes that may rupture and spontaneously drain to the outside. If left untreated, LGV may progress to a third stage of the disease characterized by a chronic granulomatous inflammatory process leading to severe and frequently irreversible complications in the genital and anorectal tracts, including fibrosis, stenosis, strictures, lymphedema, elephantiasis, and ulceration of the external genitalia both in men and women (3, 9).
In 2003, endemic cases of LGV proctitis and proctocolitis were reported in Europe, clearly associated to HIV-positive men who have sex with men (MSM) (10, 11). Since then, similar LGV cases have been increasingly reported mainly in the MSM community of metropolitan areas in Europe, the USA, Canada and Australia (12–16). Interestingly, the ongoing epidemics of LGV in developed countries displays particular epidemiologic features, including a strong association to MSM and HIV co-infection, proctitis sometimes mimicking Crohn's disease symptoms as the main clinical finding, a significant proportion of asymptomatic cases likely contributing to LGV transmission and, surprisingly, a markedly increased proportion of anorectal compared to genital infections (17–21).
Herein, we report, to our knowledge, the first case of chronic epididymitis due to C. trachomatis LGV-L2 infection in an HIV-negative, heterosexual man without the typical signs and symptoms of LGV.
Case description
A 36-year-old male presented to a Urology and Andrology outpatient clinic of a healthcare center from Cordoba, Argentina, in July 2018 referring signs and symptoms of epididymo-orchitis (Figure 1). He is a heterosexual male, married to a woman, declaring not to have had sex with men or trans women, who was also seeking care for couple's primary infertility (attributed to his wife anovulation). The patient complained of intermittent pain and discomfort in the testicles over the last 6 months. His height and weight were 178 cm and 75 kg, respectively, indicating a normal body mass index (BMI: 23.7). Physical examination revealed intense pain on scrotum palpation (particularly in the right epididymis), tender and swollen right epididymis, slightly increased size of the right testicle and enlargement of the right spermatic cord. Blood pressure, heart rate, breathe sounds on auscultation, body temperature and the remainder of the routine physical examinations were normal. The patient's medical record revealed a history of varicocele surgery 1 year earlier (July 2017) (Figure 1). In this context, chronic epididymo-orchitis was considered as a presumptive diagnosis and a series of imaging and laboratory studies were indicated.
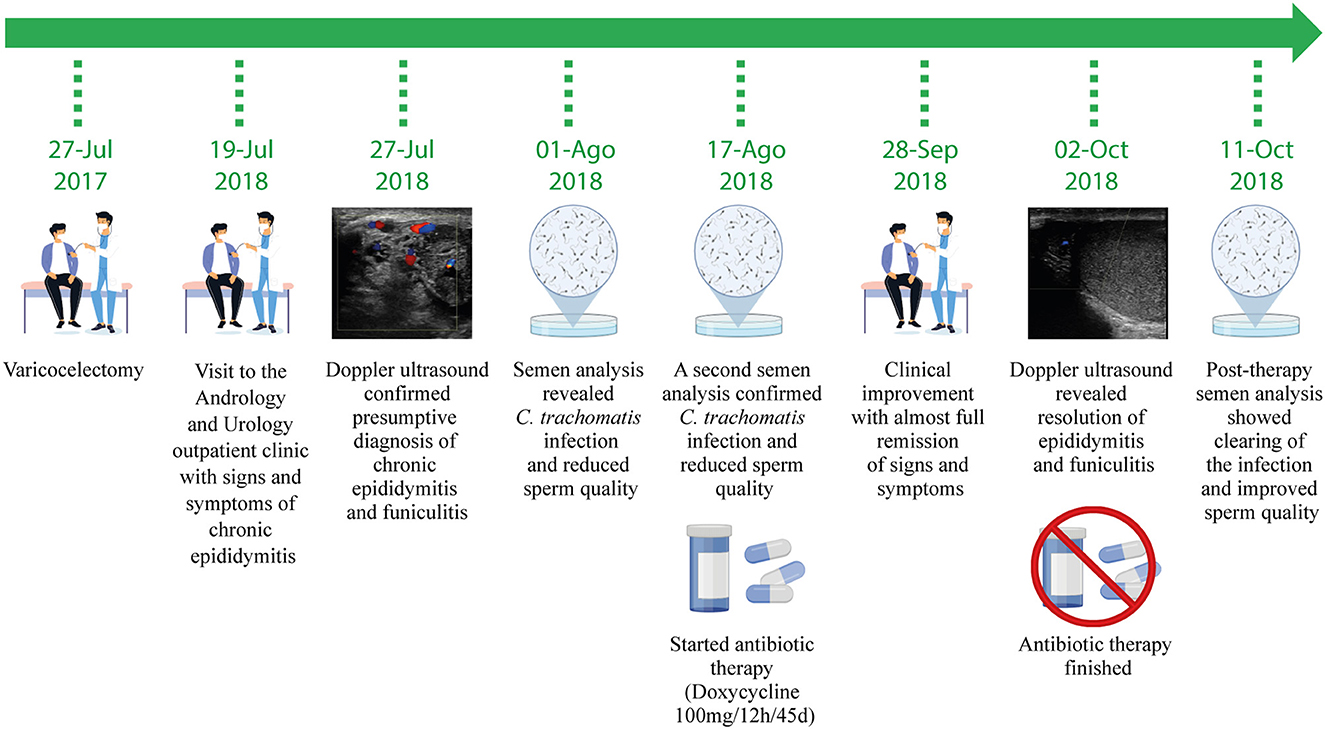
Figure 1. Timeline of the clinical evolution, diagnostic studies, pathogen identification, therapy and outcome of the patient case study.
Diagnostic assessment
A Doppler ultrasound showed hyperechogenicity, augmented size and hypervascularization of the cephalic region of the right epididymis. Moreover, hypervascularization extended to the fatty spermatic cord was observed. These findings were consistent with focal epididymitis and funiculitis (Figures 2A, B). Neither apparent abnormalities nor lesions were observed in the left epididymis and in both testicles.
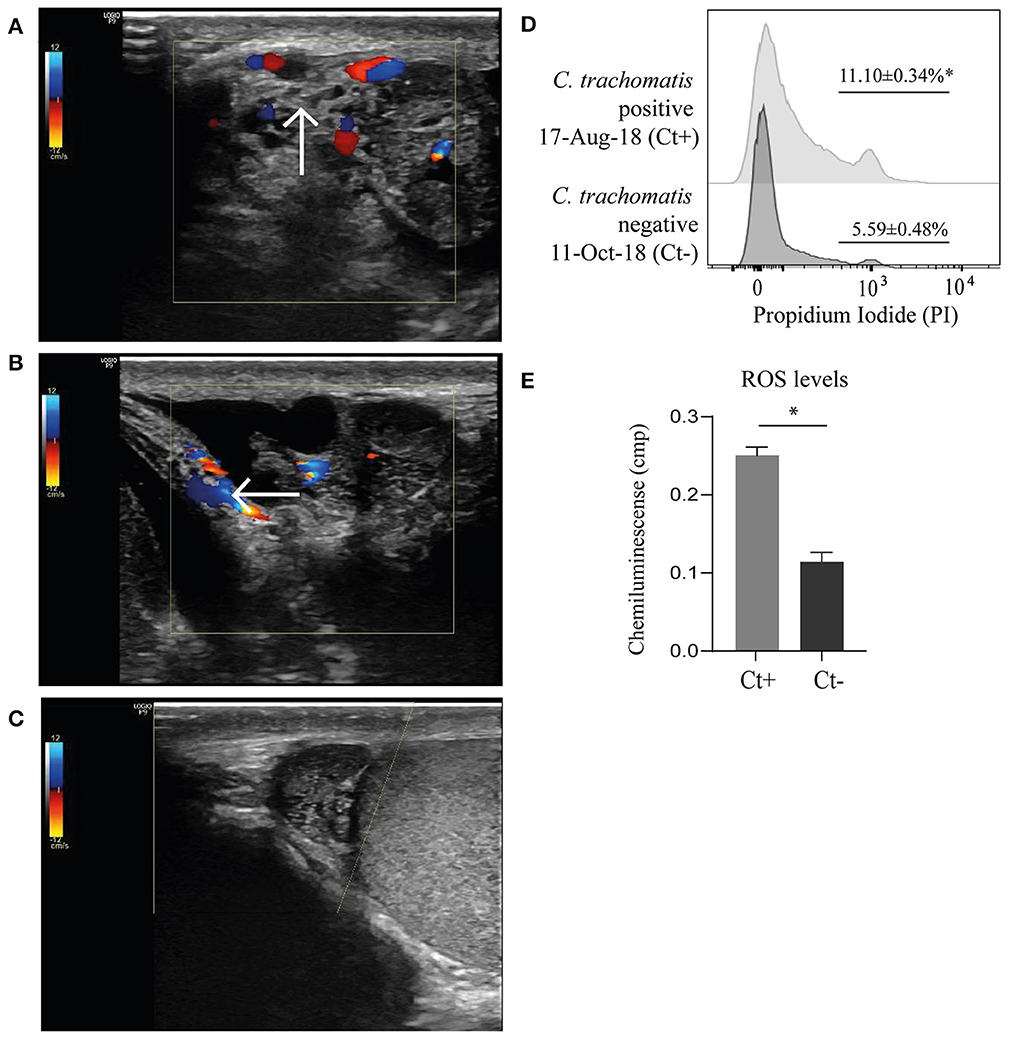
Figure 2. Testicular color Doppler ultrasounds showing hyperechogenicity and enlarged right epididymis with markedly increased vascularity that extended to the fatty spermatic cord compatible with epididymitis (A) and funiculitis (B) at patient admission (indicated with arrows), and almost complete resolution of tissue changes after antibiotic therapy and infection clearing (C). Assessment of sperm viability by flow cytometry using propidium iodide staining as previously described (22) (D). Representative histograms depicting frequencies of necrotic spermatozoa (propidium iodide-positive) within the spermatozoa population gated on FSC vs. SSC plots. Data were collected on FACS-CANTO II flow cytometer (BD Biosciences, San Diego, USA) and analyzed using FlowJo software (version 7.6.2). Proper compensation using Fluorescence Minus One (FMO) controls were used. Quantification of reactive oxygen species (ROS) level in seminal plasma by chemiluminescence using luminol (Sigma-Aldrich, St. Louis, USA) was carried out according to the WHO laboratory manual for the examination and processing of human semen (23) (E). Measurements were made with use of a Berthold luminometer (model LKB 953; Wallac Inc., Gaithersburg, USA). Results are expressed as percentages (%) or counted photons per minute (cpm). Experiments were performed in triplicates. Data are shown as mean ± SD. Mann–Whitney test; *p<0.05.
On August 1st 2018, the patient provided a semen sample (obtained by masturbation) and a panel of 17 sexually transmitted infections (STIs) including Human Immunodeficiency Virus, C. trachomatis, Ureaplasma urealyticum, Mycoplasma hominis, Mycoplasma genitalium, Herpes Simplex Virus type 1 and 2, Human Papilloma Virus, Trichomonas vaginalis, Treponema pallidum, Neisseria gonorrhoeae, Escherichia coli, Pseudomonas spp., Streptococcus spp., Staphylococcus spp., Corynebacterium spp. and Candida spp. were investigated by either PCR or culture as previously described (24). The specific primers used are detailed in Supplementary Table 1. As shown in Table 1, a positive result was obtained for C. trachomatis infection while all the other pathogens were negative. The urogenital infection by C. trachomatis was later confirmed on August 17th 2018 in an independent sample (Table 1, Supplementary Figure 1, Figure 1).
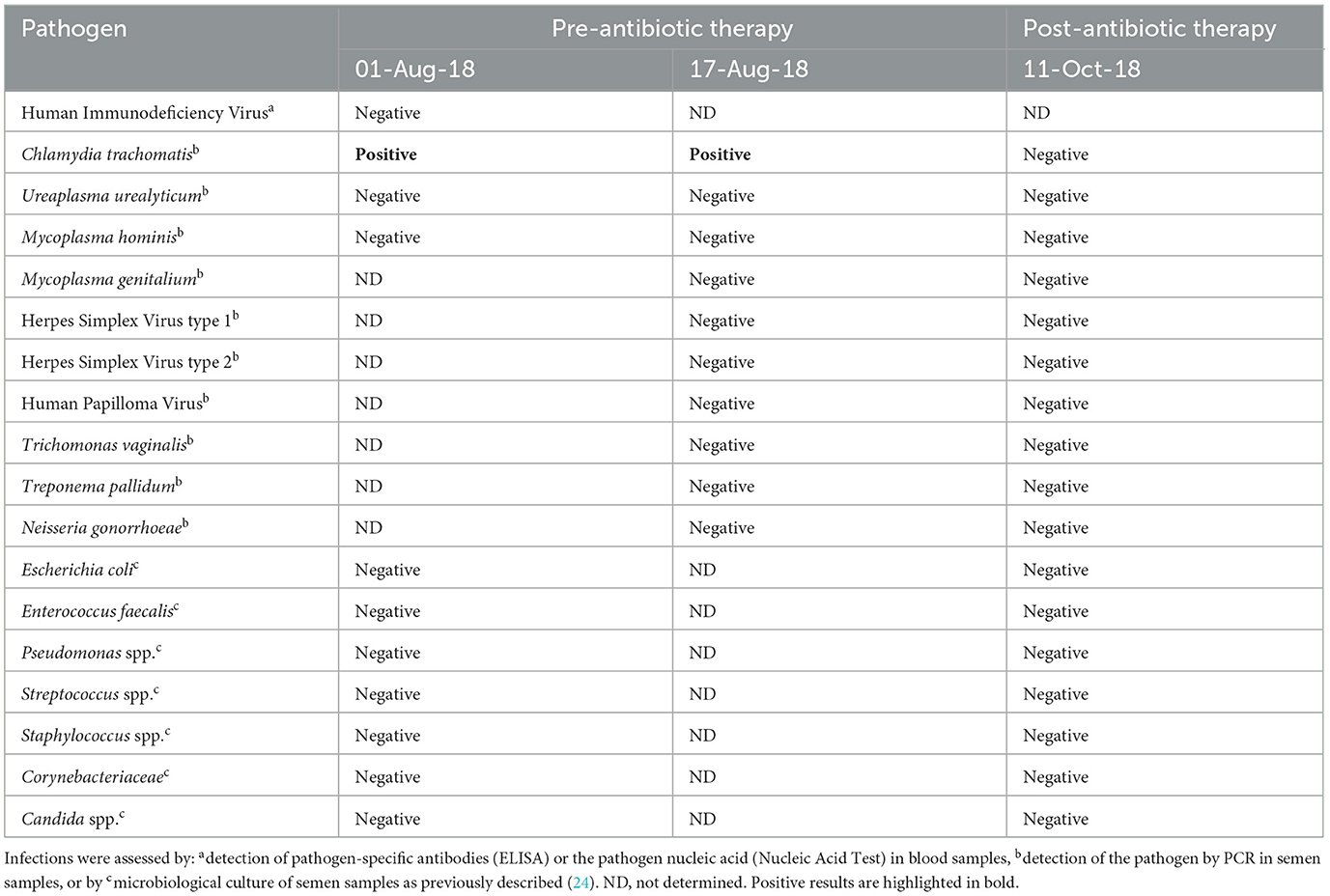
Table 1. Assessment of STI.
In addition, semen analysis revealed oligoasthenozoospermia (decreased levels of sperm concentration and motility), reduced sperm viability together with increased sperm DNA fragmentation and the presence of anti-sperm IgG autoantibodies (Table 2). All these findings allowed the diagnosis of chronic epididymitis due to C. trachomatis infection and a treatment with doxycycline 100 mg/12 h for 45 days was prescribed (Figure 1). In this context, the patient's wife, who was asymptomatic, was immediately prescribed the proper antibiotic treatment as recommended (3, 25).
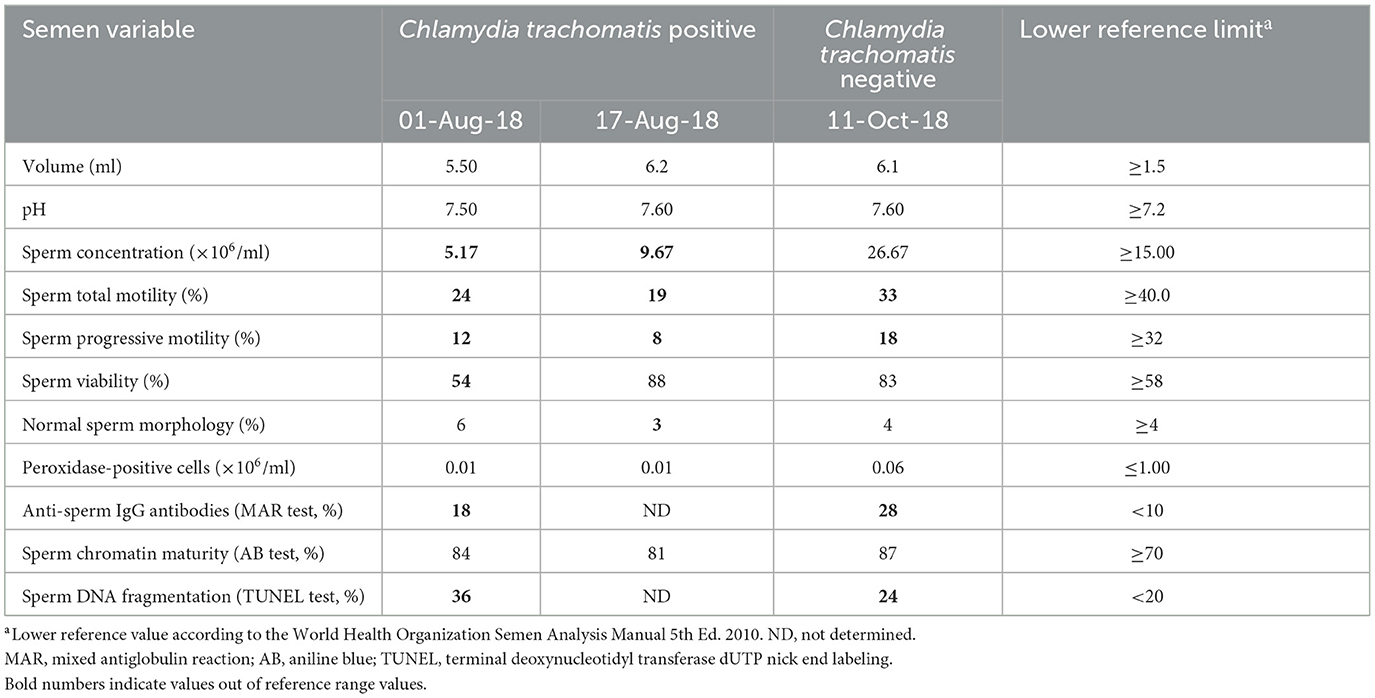
Table 2. Semen quality.
Once the antimicrobial treatment was completed, the patient reported complete resolution of clinical signs and symptoms. A post-treatment Doppler ultrasound showed scarce to absent hypervascularization and slightly increased size and echogenicity of the right epididymitis, findings that were compatible with sequelae of focal chronic epididymitis (Figure 2C). In addition, no signs of inflammation in the right spermatic cord indicated resolution of the funiculitis (Figure 2C). In order to document microbiological cure after treatment, the patient provided a new semen sample on October 11th 2018, which was subjected to infection screening. Negative results were obtained for C. trachomatis as well as for all the other pathogens investigated indicating resolution of the infection (Table 1, Supplementary Figure 1, Figure 1). The same results were observed after testing the patient's wife.
Interestingly, a new semen analysis revealed an overall improvement of sperm quality after antimicrobial treatment as shown by increased sperm concentration, viability and motility (Table 2). In addition, levels of reactive oxygen species (ROS) in seminal plasma and necrosis of spermatozoa were evaluated. Moreover, the resolution of the infection associated with significant reductions in ROS and sperm necrosis levels (Figures 2D, E).
In the framework of an ongoing molecular epidemiology study, the identification of the genotype of the C. trachomatis strain detected in the patient was performed. For that, sequencing of the MOMP gene (ompA) as well as high-resolution genotyping by multilocus sequence typing (MLST) according to the Uppsala scheme were carried out as previously described (26–28). Both, the complete sequence of ompA and the MLST allelic profile were successfully obtained. Unexpectedly, the MLST allelic profile showed an exact match with C. trachomatis sequence type 141 (ST141). Moreover, the ompA gene sequence obtained was 100% identical to that of C. trachomatis genovar L2, confirming that the strain detected was C. trachomatis LGV L2 (Supplementary Figure 2 and Supplementary Table 2).
Overall, these results indicate that C. trachomatis LGV-L2 was identified as the cause of chronic epididymitis in an HIV-negative, heterosexual patient presenting without the typical LGV signs and symptoms.
Discussion
The epididymis is an important male accessory sex organ where sperm motility and fertilization ability develop. Epididymitis is an inflammation of the epididymis that can be caused by infectious or non-infectious agents and a common cause of male infertility (29). Due to lack of large and comprehensive studies, the exact global prevalence of epididymitis is currently unclear (30). However, it is likely low considering that around 600,000 cases/year occur in the USA (31). Reported data in different settings have shown that epididymitis accounts for 0.69%−1.5% of men presenting to urology outpatient visits (30–32). In line with this, several studies stated a prevalence of epididymitis ranging from 25 to 65 per 10,000 person/year [(33) and references therein].
Although epididymitis can occur in men of any age, the majority of epididymitis cases occur in men aged 20–39 and they are most often associated with STIs (34). In sexually active men younger than 40 years old, C. trachomatis and N. gonorrhoeae are the most frequent causes of epididymitis (30, 35, 36). However, it is worth mentioning that chlamydial epididymitis usually arises as a complication of ascending urethritis caused by non-LGV C. trachomatis genovars (D–K) and mostly presents as an acute episode. In fact, LGV genovars (L1–L3) have not been so far associated to epididymitis (37, 38).
Herein, we report a case of a patient with chronic epididymitis due to C. trachomatis LGV-L2 infection associated with oligoasthenozoospermia, necrozoospermia, and increased sperm DNA fragmentation and ROS levels in seminal plasma that significantly improved after antimicrobial treatment and microbiological cure. To the best of our knowledge, this is the first report of C. trachomatis LGV-L2 as a causative agent of epididymitis. More unusual, it was in fact a case of chronic epididymitis since signs and symptoms lasted for more than 3 months. Noteworthy, due to its low prevalence, there is very scarce reported data and standardized guidelines for chronic epididymitis clinical management and therapy (32, 39–41).
It is well-known that there is a connection between male infertility and epididymitis/epididymo-orchitis resulting from ascending STIs (42). Inflammatory processes in the epididymis may lead to alterations in sperm count, motility and several sperm functions. In fact, reported evidence indicates that men with epididymitis usually present with impaired semen quality. It has been shown that acute epididymitis associates with reduced sperm concentration, motility and viability (43). The latter could be consequence of pathogen-induced damage and/or inflammation that in turn may result in epididymal dysfunction, tissue scarring and obstruction (29, 44). The drop in sperm concentration observed during the acute phase of epididymitis is usually reversible; however, persistent azoospermia was observed in ~10% of patients and oligozoospermia in another 30% (42, 43). Besides, and in agreement with our data, chronic epididymitis may also result in reduced sperm concentration and motility (45). Interestingly, oligozoospermia has been previously reported during chlamydial epididymitis, whereas no evidence indicates long-term impairment of future fertility (31, 46). Moreover, in most cases of chronic epididymitis, the number of leukocytes in the ejaculate is below the threshold of leukocytospermia in spite of ongoing local inflammation revealed by increased levels of seminal inflammatory cytokines and/or ROS. The latter may in turn impair sperm quality parameters, induce sperm DNA fragmentation and affect several important sperm functions (45). In addition, positive effects of antinflammatory/antibiotic treatment on semen quality have been reported (45). In agreement, it is reasonable to postulate that C. trachomatis LGV-L2 chronic infection in the epididymis and the induced local inflammation may be triggering direct or indirect damage to sperm cells, which is supported by the higher levels of ROS in semen, and necrosis and DNA fragmentation in spermatozoa presented by the patient under study prior to antimicrobial treatment and microbiological cure.
Interestingly, the patient also presented anti-sperm IgG autoantibodies. Strikingly, rather than ameliorating, anti-sperm IgG levels increased after antibiotic treatment and microbiological cure of the infection. These results are in line with previous reports pointing out to an association between epididymitis and anti-sperm autoantibodies. Reported data indicates that 27% of patients with acute epididymitis increased the titers of anti-sperm antibodies 3 years after recovery. Moreover, 15% of patients with acute epididymitis developed anti-sperm antibodies de novo (43, 47). Physiologically, the epididymal immune balance must be set and maintained toward spermatozoa. The epididymis has a blood-epididymis barrier (BEB) that creates a suitable immune-privileged environment for sperm maturation preventing autoimmune responses against antigenic postpubertal germ cells (48, 49). Infection and inflammation can damage the BEB thus resulting in loss of the immune privilege, which could lead to autoimmunity against sperm antigens (50, 51).
Remarkably, the patient presented with chronic epididymitis but without the typical signs and symptoms of C. trachomatis LGV urogenital infections such as inguinal papules or buboes, herpetiform ulcers and/or lymphadenopathy. The causality of the patient's condition related to C. trachomatis LGV infection is strongly supported by resolution of clinical signs and symptoms along with microbiological cure after anti-chlamydial antibiotic therapy was implemented. This finding highlights the importance of considering C. trachomatis LGV among other common STIs when diagnosing male urogenital infections even in the absence of the typical clinical presentation of LGV. Indeed, atypical clinical presentations of C. trachomatis LGV infections have already been reported (14, 52, 53).
As mentioned above, we did not find any previous report of epididymitis caused by C. trachomatis LGV genovars pointing out to the novelty of this communication. Interestingly, the detection of this case concurred in time with the re-emergence of endemic cases of urogenital infections caused by C. trachomatis LGV in our country after decades (54). Noteworthy, between September 2017 and July 2018, 33 confirmed cases of C. trachomatis LGV (mainly L2b genovar) infections were detected in the region. All these infections were detected in MSM, 90% of them HIV-positive, presenting with proctitis as the dominant clinical manifestation (55). Clearly, these emergent cases of C. trachomatis LGV infection recently reported in the region share similar epidemiological features with those detected in Europe, Australia and North America, as opposed to the case presented herein.
In summary, this case highlights the importance of considering C. trachomatis genovars LGV as a putative cause of epididymitis, even in the absence of the typical LGV signs and symptoms. The findings presented herein delivers important data for researchers as well as clinically useful information for physicians and microbiologists to improve diagnosis and prevent infection transmission and its associated complications. Moreover, our data warrant further molecular epidemiological investigations to elucidate the precise role of C. trachomatis LGV genovars in male urogenital infections.
Patient perspective
The patient has remained stable and with no further evident complications after adhering to the treatment proposed and clearing the infection. He was satisfied with the improvement in the clinical condition and regularly attends to periodic controls.
Data availability statement
The original contributions presented in this work are included in the article/Supplementary material. Further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving human participants were reviewed and approved by Institutional Review Board of the Hospital Nacional de Clínicas, Universidad Nacional de Córdoba (RePIS #3512). The patients/participants provided their written informed consent to participate in this study. Written informed consent to participate in this study was provided by the patient for the publication of any potentially identifiable images or data included in this article.
Author contributions
RDM and HAS: conceptualization, funding acquisition, resources, supervision, data analysis and curation, writing, and editing of the manuscript. DAP: data acquisition, formal analysis, validation, writing, and editing of the manuscript. JJO: patient care, data acquisition, formal analysis, and validation. CO, ADT, and RIM: methodology and data acquisition. VER: writing and editing of the manuscript. All authors significantly contributed to the article and approved the submitted version.
Funding
DAP is recipient of a doctoral fellowship from CONICET at CIBICI-CONICET. RDM and HAS are Professors at the Departamento de Bioquímica Clínica, Facultad de Ciencias Químicas, Universidad Nacional de Córdoba, Argentina. RDM and HAS are Independent Investigators at CIBICI-CONICET. This work was supported by the Agencia Nacional de Promoción Científica y Tecnológica (ANPCyT-FONCyT, grants PICT 2019-2451 and 2018-3004), CONICET (grants PIP 11220200103254CO, PGD 22920160100116CO, and P-UE 22920160100116CO), and Secretaría de Ciencia y Tecnología de la Universidad Nacional de Córdoba (Secyt-UNC).
Acknowledgments
We thank Paula Abadie and Pilar Crespo for technical assistance.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1129166/full#supplementary-material
Abbreviations
LGV, lymphogranuloma venereum; HIV, human immunodeficiency virus; STI, sexually transmitted infection; MOMP, major outer membrane protein; MSM, men who have sex with men; BMI, body mass index; IgG, immunoglobulin G; DNA, deoxyribonucleic acid; ROS, reactive oxygen species; MLST, multilocus sequence typing; ompA, outer membrane protein A; BEB, blood-epididymis barrier; PCR, polymerase chain reaction; CTP, cryptic plasmid; cmp, counted photons per minute; ELISA, enzyme-linked immunosorbent assay.
References
1. Elwell C, Mirrashidi K, Engel J. Chlamydia cell biology and pathogenesis. Nat Rev Microbiol. (2016) 14:385–400. doi: 10.1038/nrmicro.2016.30
2. Zambrano AI, Sharma S, Crowley K, Dize L, Munoz BE, Mishra SK, et al. The World Health Organization recommendations for trachoma surveillance, experience in nepal and added benefit of testing for antibodies to Chlamydia trachomatis pgp3 protein: NESTS Study. PLoS Negl Trop Dis. (2016) 10:e0005003. doi: 10.1371/journal.pntd.0005003
3. Bennett JE, Dolin R, Mandell GL, Blaser MJ, Douglas RG. Chlamydia trachomatis (trachoma and urogenital infections). In: BE Battegier, M Tan, editors. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 9th ed. Philadelphia, PA: Elsevier (2020). 2301–19.
4. Newman L, Rowley J, Vander Hoorn S, Wijesooriya NS, Unemo M, Low N, et al. Global estimates of the prevalence and incidence of four curable sexually transmitted infections in 2012 based on systematic review and global reporting. PLoS ONE. (2015) 10:e0143304. doi: 10.1371/journal.pone.0143304
5. Stamm WE. Chlamydia trachomatis infections: progress and problems. J Infect Dis. (1999) 179(Suppl 2):S380–3. doi: 10.1086/513844
6. Panzetta ME, Valdivia RH, Saka HA. Chlamydia persistence: a survival strategy to evade antimicrobial effects in-vitro and in-vivo. Front Microbiol. (2018) 9:3101. doi: 10.3389/fmicb.2018.03101
7. Stoner BP, Cohen SE. Lymphogranuloma venereum 2015: clinical presentation, diagnosis, and treatment. Clin Infect Dis. (2015) 61(Suppl 8):S865–73. doi: 10.1093/cid/civ756
8. de Vries HJC, de Barbeyrac B, de Vrieze NHN, Viset JD, White JA, Vall-Mayans M, et al. 2019 European guideline on the management of lymphogranuloma venereum. J Eur Acad Dermatol Venereol. (2019) 33:1821–8. doi: 10.1111/jdv.15729
9. White JA. Manifestations and management of lymphogranuloma venereum. Curr Opin Infect Dis. (2009) 22:57–66. doi: 10.1097/QCO.0b013e328320a8ae
10. Centers for Disease Control and Prevention (CDC). Lymphogranuloma venereum among men who have sex with men–Netherlands, 2003-2004. MMWR Morb Mortal Wkly Rep. (2004) 53:985–8.
11. Spaargaren J, Fennema HS, Morre SA, de Vries HJ, Coutinho RA. New lymphogranuloma venereum Chlamydia trachomatis variant, Amsterdam. Emerg Infect Dis. (2005) 11:1090–2. doi: 10.3201/eid1111.050821
12. Pathela P, Blank S, Schillinger JA. Lymphogranuloma venereum: old pathogen, new story. Curr Infect Dis Rep. (2007) 9:143–50. doi: 10.1007/s11908-007-0010-7
13. de Voux A, Kent JB, Macomber K, Krzanowski K, Jackson D, Starr T, et al. Notes from the field: cluster of lymphogranuloma venereum cases among men who have sex with men - Michigan, August 2015-April 2016. MMWR Morb Mortal Wkly Rep. (2016) 65:920–1. doi: 10.15585/mmwr.mm6534a6
14. de Vries HJC. Lymphoganuloma venereum in the Western world, 15 years after its re-emergence: new perspectives and research priorities. Curr Opin Infect Dis. (2019) 32:43–50. doi: 10.1097/QCO.0000000000000519
15. Martinez-Garcia L, Rodriguez-Dominguez M, Lejarraga C, Rodriguez-Jimenez MC, Gonzalez-Alba JM, Puerta T, et al. The silent epidemic of lymphogranuloma venereum inside the COVID-19 pandemic in Madrid, Spain, March 2020 to February 2021. Euro Surveill. (2021) 26:2100422. doi: 10.2807/1560-7917.ES.2021.26.18.2100422
16. Smolarczyk K, Mlynarczyk-Bonikowska B, Majewski S, Rudnicka E, Unemo M, Fiedor P. Lymphogranuloma venereum: an emerging problem in Poland. Postepy Dermatol Alergol. (2022) 39:587–93. doi: 10.5114/ada.2020.101466
17. Tinmouth J, Rachlis A, Wesson T, Hsieh E. Lymphogranuloma venereum in North America: case reports and an update for gastroenterologists. Clin Gastroenterol Hepatol. (2006) 4:469–73. doi: 10.1016/j.cgh.2005.12.006
18. de Vries HJC. The enigma of lymphogranuloma venereum spread in men who have sex with men: does ano-oral transmission plays a role? Sex Transm Dis. (2016) 43:420–2. doi: 10.1097/OLQ.0000000000000466
19. Saxon C, Hughes G, Ison C, Group ULC-F. Asymptomatic lymphogranuloma venereum in men who have sex with men, United Kingdom. Emerg Infect Dis. (2016) 22:112–6. doi: 10.3201/EID2201.141867
20. de Vrieze NHN, Versteeg B, Bruisten SM, van Rooijen MS, van der Helm JJ, de Vries HJC. Low prevalence of urethral lymphogranuloma venereum infections among men who have sex with men: a prospective observational study, sexually transmitted infection clinic in Amsterdam, the Netherlands. Sex Transm Dis. (2017) 44:547–50. doi: 10.1097/OLQ.0000000000000657
21. Hughes Y, Chen MY, Fairley CK, Hocking JS, Williamson D, Ong JJ, et al. Universal lymphogranuloma venereum (LGV) testing of rectal chlamydia in men who have sex with men and detection of asymptomatic LGV. Sex Transm Infect. (2022) 98:582–5. doi: 10.1136/sextrans-2021-055368
22. Motrich RD, Breser ML, Molina RI, Tissera A, Olmedo JJ, Rivero VE. Patients with chronic prostatitis/chronic pelvic pain syndrome show T helper type 1 (Th1) and Th17 self-reactive immune responses specific to prostate and seminal antigens and diminished semen quality. BJU Int. (2020) 126:379–87. doi: 10.1111/bju.15117
23. World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen. 5th ed. World Health Organization (2010). Available online at: https://apps.who.int/iris/handle/10665/44261
24. Paira DA, Olivera C, Tissera AD, Molina RI, Olmedo JJ, Rivero VE, et al. Ureaplasma urealyticum and Mycoplasma hominis urogenital infections associate with semen inflammation and decreased sperm quality. J Leukoc Biol. (2023) 113:18–26. doi: 10.1093/jleuko/qiac006
25. CDC Sexually Transmitted Infections Treatment Guidelines 2021. Centers for Disease Control and Prevention (CDC), U.S. Department of Health and Human Services. (2021). Available online at: https://www.cdc.gov/std/treatment-guidelines/lgv.htm (accessed December 18, 2022).
26. Klint M, Fuxelius HH, Goldkuhl RR, Skarin H, Rutemark C, Andersson SG, et al. High-resolution genotyping of Chlamydia trachomatis strains by multilocus sequence analysis. J Clin Microbiol. (2007) 45:1410–4. doi: 10.1128/JCM.02301-06
27. Bom RJ, Christerson L, Schim van der Loeff MF, Coutinho RA, Herrmann B, Bruisten SM. Evaluation of high-resolution typing methods for Chlamydia trachomatis in samples from heterosexual couples. J Clin Microbiol. (2011) 49:2844–53. doi: 10.1128/JCM.00128-11
28. Bom RJ, van der Helm JJ, Schim van der Loeff MF, van Rooijen MS, Heijman T, Matser A, et al. Distinct transmission networks of Chlamydia trachomatis in men who have sex with men and heterosexual adults in Amsterdam, The Netherlands. PLoS ONE. (2013) 8:e53869. doi: 10.1371/journal.pone.0053869
29. Zhao H, Yu C, He C, Mei C, Liao A, Huang D. The immune characteristics of the epididymis and the immune pathway of the epididymitis caused by different pathogens. Front Immunol. (2020) 11:2115. doi: 10.3389/fimmu.2020.02115
31. Trojian TH, Lishnak TS, Heiman D. Epididymitis and orchitis: an overview. Am Fam Physician. (2009) 79:583–7.
32. Tracy CR, Steers WD, Costabile R. Diagnosis and management of epididymitis. Urol Clin North Am. (2008) 35:101–8. vii. doi: 10.1016/j.ucl.2007.09.013
33. Çek M, Sturdza L, Pilatz A. Acute and chronic epididymitis. Eur Urol Suppl. (2017) 16:124–31. doi: 10.1016/j.eursup.2017.01.003
34. Fijak M, Pilatz A, Hedger MP, Nicolas N, Bhushan S, Michel V, et al. Infectious, inflammatory and 'autoimmune' male factor infertility: how do rodent models inform clinical practice? Hum Reprod Update. (2018) 24:416–41. doi: 10.1093/humupd/dmy009
36. Sivaraj V, Ahamed A, Artykov R, Menon-Johansson A. Epididymitis and its aetiologies in a central London sexual health clinic. Int J STD AIDS. (2021) 32:96–9. doi: 10.1177/0956462420963879
37. ECDC European Centre for Disease Prevention and Control. Sexually transmitted Infections in Europe 2013. Stockholm (2015). Available online at: https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/sexual-transmitted-infections-europe-surveillance-report-2013.pdf (accessed December 18, 2022).
38. Workowski KA, Bolan GA, Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. (2015) 64(RR-03):1–137.
39. Nickel JC, Teichman JM, Gregoire M, Clark J, Downey J. Prevalence, diagnosis, characterization, and treatment of prostatitis, interstitial cystitis, and epididymitis in outpatient urological practice: the Canadian PIE Study. Urology. (2005) 66:935–40. doi: 10.1016/j.urology.2005.05.007
40. Michel V, Pilatz A, Hedger MP, Meinhardt A. Epididymitis: revelations at the convergence of clinical and basic sciences. Asian J Androl. (2015) 17:756–63. doi: 10.4103/1008-682X.155770
41. Medscape. Epididymitis Treatment and Management. Ching, CB (2022). Available online at: https://emedicine.medscape.com/article/436154-treatment (accessed December 5, 2022).
42. Schuppe HC, Pilatz A, Hossain H, Diemer T, Wagenlehner F, Weidner W. Urogenital infection as a risk factor for male infertility. Dtsch Arztebl Int. (2017) 114:339–46. doi: 10.3238/arztebl.2017.0339
43. Rusz A, Pilatz A, Wagenlehner F, Linn T, Diemer T, Schuppe HC, et al. Influence of urogenital infections and inflammation on semen quality and male fertility. World J Urol. (2012) 30:23–30. doi: 10.1007/s00345-011-0726-8
44. Stammler A, Hau T, Bhushan S, Meinhardt A, Jonigk D, Lippmann T, et al. Epididymitis: ascending infection restricted by segmental boundaries. Hum Reprod. (2015) 30:1557–65. doi: 10.1093/humrep/dev112
45. Haidl G, Allam JP, Schuppe HC. Chronic epididymitis: impact on semen parameters and therapeutic options. Andrologia. (2008) 40:92–6. doi: 10.1111/j.1439-0272.2007.00819.x
46. Berger RE, Alexander ER, Harnisch JP, Paulsen CA, Monda GD, Ansell J, et al. Etiology, manifestations and therapy of acute epididymitis: prospective study of 50 cases. J Urol. (1979) 121:750–4. doi: 10.1016/S0022-5347(17)56978-5
47. Ingerslev HJ, Walter S, Andersen JT, Brandenhoff P, Eldrup J, Geerdsen JP, et al. A prospective study of antisperm antibody development in acute epididymitis. J Urol. (1986) 136:162–4. doi: 10.1016/S0022-5347(17)44764-1
48. Mital P, Hinton BT, Dufour JM. The blood-testis and blood-epididymis barriers are more than just their tight junctions. Biol Reprod. (2011) 84:851–8. doi: 10.1095/biolreprod.110.087452
49. Cyr DG, Dufresne J, Gregory M. Cellular junctions in the epididymis, a critical parameter for understanding male reproductive toxicology. Reprod Toxicol. (2018) 81:207–19. doi: 10.1016/j.reprotox.2018.08.013
50. Dube E, Cyr DG. The blood-epididymis barrier and human male fertility. Adv Exp Med Biol. (2012) 763:218–36. doi: 10.1007/978-1-4614-4711-5_11
51. Smith TB, Cortez-Retamozo V, Grigoryeva LS, Hill E, Pittet MJ, Da Silva N. Mononuclear phagocytes rapidly clear apoptotic epithelial cells in the proximal epididymis. Andrology. (2014) 2:755–62. doi: 10.1111/j.2047-2927.2014.00251.x
52. Monetti MS, Molina RA, Estofan P, Frutos MC, Kiguen AX, Venezuela RF, et al. Distribution of Chlamydia trachomatis genotypes in infertile patients of Córdoba, Argentina. Int J Virol Mol Biol. (2013) 2:1–6. doi: 10.5923/j.ijvmb.20130201.01
53. Kiguen AX, Marrama M, Ruiz S, Estofan P, Venezuela RF, Mosmann JP, et al. Prevalence, risk factors and molecular characterization of Chlamydia trachomatis in pregnant women from Cordoba, Argentina: a prospective study. PLoS ONE. (2019) 14:e0217245. doi: 10.1371/journal.pone.0217245
54. Lopez LS, La Rosa L, Entrocassi AC, Caffarena D, Santos B, Fermepin MR. Rectal lymphogranuloma venereum, Buenos Aires, Argentina. Emerg Infect Dis. (2019) 25:598–9. doi: 10.3201/eid2503.180600
55. MSAL Ministerio de Salud Presidencia de la Nación. ALERTA EPIDEMIOLOGICA: Casos de linfogranuloma venéreo (LGV) en Argentina. (2018). Available online at: https://www.argentina.gob.ar/sites/default/files/alerta_linfogranuloma_venereo_se332018.pdf (accessed December 18, 2022).
Keywords: sexually transmitted infections, Chlamydia trachomatis, epididymitis, semen, case report
Citation: Paira DA, Olmedo JJ, Olivera C, Tissera AD, Molina RI, Rivero VE, Motrich RD and Saka HA (2023) Chronic epididymitis due to Chlamydia trachomatis LGV-L2 in an HIV-negative heterosexual patient: a case report. Front. Public Health 11:1129166. doi: 10.3389/fpubh.2023.1129166
Received: 21 December 2022; Accepted: 05 April 2023;
Published: 09 May 2023.
Edited by:
Nathlee Abbai, University of KwaZulu-Natal, South AfricaReviewed by:
Khine Swe Swe Han, National Health Laboratory Service (NHLS), South AfricaEi Aung, Melbourne Sexual Health Centre (MSHC), Australia
Copyright © 2023 Paira, Olmedo, Olivera, Tissera, Molina, Rivero, Motrich and Saka. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rubén Darío Motrich, cm1vdHJpY2hAdW5jLmVkdS5hcg==; Héctor Alex Saka, YWxleC5zYWthQHVuYy5lZHUuYXI=
†These authors have contributed equally to this work and share senior authorship