 Mizanur Rahman
Mizanur Rahman Kanta Jamil
Kanta Jamil Quamrun Nahar
Quamrun Nahar Nitai Chakraborty1
Nitai Chakraborty1 M. Moinuddin Haider
M. Moinuddin Haider Shusmita Khan
Shusmita Khan
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 03 April 2023
Sec. Life-Course Epidemiology and Social Inequalities in Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1125056
This article is part of the Research Topic Adolescent Sexual and Reproductive Health Challenges in Low-Income Settings View all 8 articles
Background: Intimate partner violence (IPV), and especially intimate partner physical violence (IPPV), perpetrated by husbands, and within adolescence marriage are pervasive in Bangladesh. Younger women are more vulnerable to IPPV.
Objectives: We examined factors associated with IPPV experienced by married adolescents ages 15–19 and tested four hypotheses: (1) adolescent girls married to relatively older husbands, (2) adolescents living in extended families with parents or parents-in-law, (3) adolescents who are minimally controlled by husbands, and (4) adolescents who have a child after marriage are protective of IPPV.
Methods: We analyzed IPPV data from 1,846 married girls ages 15–19 obtained from a national adolescent survey conducted in 2019–20. IPPV is defined as the respondent having physical violence perpetrated by her husband at least once in the last 12 months. We implemented logistic regression models to test our hypotheses.
Results: Sixteen percent of married adolescent girls experienced IPPV. Girls living with parents-in-law or parents had adjusted odds ratio (AOR) of 0.56 (p < 0.001) of IPPV compared to those girls who lived with husband alone. Girls with husbands ages 21–25 years and 26 years or older had AORs of 0.45 (p < 0.001) and 0.33 (p < 0.001) of IPPV compared to those girls with their husband ages 20 and younger. Married adolescent girls who did not own a mobile phone (an indicator of spousal power dynamics) had an AOR of 1.39 (p < 0.05) compared to those girls who had a phone. IPPV risk increases with an increased duration of marriage for those with no living children (p < 0.001) but not for those with at least one living child; the risk was higher among those who had a child within the 1st year of marriage than those who had not yet had a child. At a duration of 4 years and longer, IPPV risk was higher among those with no living children than those with children.
Discussion: Findings related to those living with parents-in-law or parents, girls married to relatively older boys/men, having the ability to communicate with outside world, and having a child are protective of IPPV in Bangladesh are new, to our knowledge. Strictly adhering to the law that requires men waiting until the age of 21 to marry can reduce married girls' risk of IPPV. Raising girls' legal marriage age can minimize adolescents' IPPV and other health risks associated with adolescent childbearing.
Four types of intimate partner violence (IPV)—physical violence, sexual violence, stalking, and psychological aggression—are identified by the Centers for Disease Control and Prevention (1). IPV is one of the most common forms of violence against women and includes physical, sexual, and emotional abuse and controlling behaviors by an intimate partner (2). IPV is pervasive across countries, especially in those with traditional economies (2). Such violence has short- and long-term negative effects on women's health and wellbeing with varying degrees and magnitude (1). For example, morbidity and mortality of under-five children were significantly higher among women who experienced IPV than those women who did not (3, 4) and major depressive disorder was significantly higher among married adolescent IPPV victims than those who did not face IPPV (5).
Bangladesh is a country with a moderate to high level of IPV (2, 6). Younger women are more vulnerable to IPV (2, 7–11), and the country is among the top three with high incidence of adolescent marriages (Statcompiler). Six in ten women are married by age 18 and about three in ten women begin their childbearing in their teenage period (12). Child marriage or marriage before age 18 has been positively associated with IPV in Bangladesh, India, Nepal, and Pakistan (13–17).
In this paper, we examine the factors associated with IPPV experienced by married adolescents ages 15–19. We use data from a nationally representative survey of adolescents conducted in 2019–20. We concentrate on factors involving household living arrangement, partner (husband-wife) demography, partner control, and onset of childbearing after marriage. All these factors are likely to play important roles at the onset of their life-time partnership development immediately after marriage.
In this paper, the term “intimate partner” refers to husband and wife; living together as intimate partner is uncommon and not typically allowed as a societal norm in Bangladesh. At the outset, we review the reported reasons behind IPV in Bangladesh. We then review various aspects of marriage formation processes, demography of intimate partners, living arrangement after marriage, and expectations of the newlywed female partner from the husband and other household members. We then develop hypotheses on how some selected factors can lead to intimate partner violence. A schematic diagram is shown to show the associations between factors and IPPV (Figure 1).
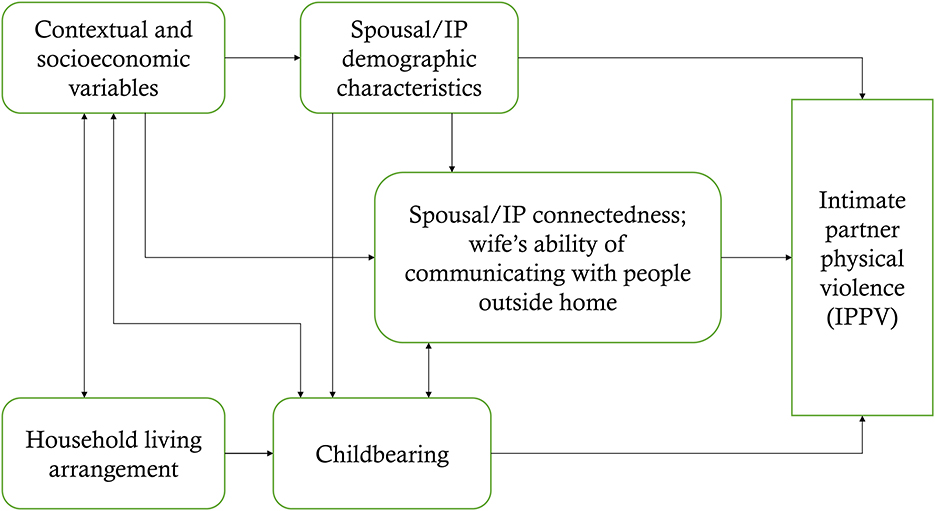
Figure 1. Association of spousal/intimate partners' (IP) demographic characteristics, household living arrangement, childbearing, and partner control with IPV.
Various reasons from more serious to day-to-day routine issues are reported as reasons behind the physical violence that are perpetrated by the husband against his wife. Lack of or inability of dowry payment (15, 18–23) and related familial conflict (24) are more serious and important factors. Other common causes of IPV include:
• A husband's controlling attitude, his sense of superiority over his wife, or his perceived and proclaimed legitimacy over his wife and related behavior (21, 25–27).
• A wife's lack of interest in sex or refusing sex at a time upon the husband's demand (28).
• An argument between a wife and her husband.
• If a wife questions her husband in day-to-day matters.
• If a wife leaves the home without letting her husband or other family member know (28–30).
• If a wife does not meet her husband's expectations in household chores (i.e., negligence of children or meals are not properly prepared) (7, 15).
• Not conforming to wearing a veil or other expected behavior (29).
• The inability to become pregnant (28).
Other family members such as in-laws (usually mother- or/and sisters-in-law) can also instigate IPV (7). However, the role of in-laws in IPV has likely minimized over time with increased education and women's greater participation in income earning (27). In Bangladesh, married women agreed that wife-beating is justified for the following reasons: argument with husband, neglecting children, going outside home without permission of husband, refusing sex when asked by husband, and burning of food (31).
Marriage is typically arranged by parents or grandparents, family members, and relatives (32). No or limited chance exists for potential marital partners of knowing each other although this norm is changing, especially in urban areas. Partner selection by the spouses, if any, usually occurs among relatively older people, especially those with more education. Partners are now given a chance to formally meet for a few hours immediately prior to the wedding, if desired. However, there are few cases of adolescent marriage that take place following love affair, initially without the knowledge of parents and family members and eventually family accept the couples as married.
Most couples receive gifts from the bride's family in cash, in kind, or both. Negotiated gifts from bride's family to the groom's family is known as a dowry and is a common practice, especially within low-income households. The dowry is given at the time of wedding or before, but the payment can be deferred partially or in full for months or years after the wedding.
As mentioned above, teenage marriage is the cultural norm in Bangladesh, especially in rural areas, but it is still common in urban areas. Husbands are, on average, almost 8 years older than their wives (12, 32). According to the 2017–18 BDHS, 32 and 46% married women ages 15–49 had husbands 10 or more years older and 5–9 years older, respectively. Only 20% had husbands who were less than 5 years older and less than 1% had husbands their same age or younger. Data shows that the age gap between partners is gradually declining over time (Statcompiler). According to the 2019–20 BAHWS, age distribution of husbands of married adolescents was as follows: less than 10% were 20 years or younger, 46% were 21–25 years old, and 44% were older than 25 (12).
The bride moves to the household of the groom after marriage, but in rare cases the couples in Bangladesh begin their family life as a standalone, nuclear family. Some siblings living in the groom's home may be married and have children. There may be grandparents there too, along with grandparents' other married or unmarried children (married children may have their children), extending the household structure further. More than one in four families is a three-generation family according to the recent BDHS 2017–18 (12).
Some brides temporarily live with their parents, a trend increasing with the international migration of males who work in the Middle East and other countries. One in four married adolescents ages 15–19 reported that husbands live elsewhere (12). In the case of a migrant husband, the bride is likely to continue to live with her parents and her husband will visit her once every year or two. In a few cases, a groom moves to his in-laws' household, meaning the bride will live with her parents.
In the 2019–20 BAHWS, one in three married adolescent girls reported that she lives only with her husband, and not with any parents-in-law or parents (30). Married adolescent girls who live in non-nuclear households live with her husband's mother- and/or father-in-law or her own parents. Those who live with in-laws may also have sister- and/or brother in-laws in the house.
Household chores, cooking, cleaning, caring for children, and caring for older adults (if the household has such person[s]) are all carried out by the wife in Bangladesh. A husband rarely participates in these activities. The expectation is that these activities will be completed efficiently and timely. Additionally, a wife is expected to adhere to the advice and/or directions of the in-laws if she lives with them.
The male partner (a husband in Bangladesh) is mainly the perpetrator of IPV, and his age is an important factor associated with that IPV. Partners of adolescents (ages 15–19) are likely to be young men (30). Youths or adolescents are likely to be impulsive in their behavior and thus are more likely to be prone to violent behavior. Relatively younger males (or youth males) may react more aggressively to situations than their relatively older counterparts merely because of the age. The United Nations defines youths as those ages 15–24.
Thus, we hypothesize that adolescent girls who are married to youth males are more likely to encounter more violent attitudes and behavior than those who are married to males ages 25 and older.
IPV incidence can vary within household living arrangements. The following scenarios may be considered in terms of the link between the living arrangement and IPV:
1. When an argument or other situation arises within a nuclear family (where only the spouses live), there is no mediator who can help to calm or pacify the episode and/or intervene.
2. If a couple lives with other family member(s) and an argument or an incidence that may lead to physical violence occurs, it can worsen if one or more members seem to support either of the spouses. In-laws, especially, mothers-in-law, can worsen the situation when spouses argue and this can increase the risk of IPV.
3. In contrast, there may be no incidence of IPV if a family member mediates the argument between the spouses.
Considering these scenarios, living in an extended family may be protective or harmful in terms of IPV. However, as we will see below, ideological shifts around women's roles are occurring. These are, over time, associated with social and economic transformations that lower the risk of IPV. A recent study indicates that mothers-in-law are now more tolerant about daughters-in-law, especially for those daughters-in-law who participate in income earning (33). It is therefore possible that mothers-in-law can help ease the situation and minimize the chance of IPV.
In Pakistan, support from family members was negatively associated with IPV (34). Married adolescent girls living with her parent(s) are likely to benefit from a parent moderating or intervening in an event that could lead to IPV. Schuler et al. (27) observed that with increased economic collaboration between husbands and wives, the power and importance of mothers-in-law is fast diminishing. Education is becoming more common among the current generation of brides and as husbands become more dependent on their wives' economic contributions, more egalitarian attitudes are growing.
Social isolation is a risk factor of IPV across societies (35). Living in nuclear households may increase social isolation as those who live in extended households are more likely to receive social/familial support to avoid IPV. Stoff et al. (35) found in Bangladesh that women who maintain natal family contact at least six times a year were more likely protected from psychological IPV. When they contact their natal family more than ten times a year, she is ten times more protected from the likelihood that she will be a victim of sexual IPV. Instrumental social support can also be negatively associated with psychological, sexual, and physical violence (35). This is when a bride has someone outside the home but in the village who will be willing to provide financial or other support if needed. It is also possible that community members can intervene when IPV occurs (36). Social support acted as a protective buffer against spousal physical violence (22).
In this study, we hypothesize that a married adolescent girl living with some family members, especially parent(s)-in-law or parent(s), experiences a different risk of IPV than one living alone with her husband.
In the Bangladesh patriarchal society, husbands have a controlling attitude toward their wives. In fact, daughters grow up under the “guardianship” of the father and through a marriage the guardianship is transferred to the husband. Wives are exposed to the risk of IPV through this controlling mechanism (21). A husband's controlling behavior is a strong predictor for domestic violence in India (37).
Partner control may be influenced by two behaviors—wife-husband connectedness and wife having a power of some kind. Wife-husband connectedness may be a condition under which the wife is less likely to be controlled by the husband if the partners are connected. A wife may be classified as connected if she feels that she enjoys spending time with husband and she talks with husband about very personal things always or most of the time. Therefore, connectedness may be treated as a proxy for controlling the wife by the husband. Negotiating as a power/skill by the wife can lessen the controlling power of the husband.
A wife may acquire empowerment from her own personality asset (e.g., negotiation) or wealth which may help lessen the controlling strength of the husband. For example, if the wife earns money through a job, she may also participate in microfinance or receive remittances from parents or relatives. This empowerment of the wife, however, may be negatively or positively associated with IPV. Women who work for money were less likely to experience IPV in Bangladesh (9, 20). Such earning is a source of empowerment which helps reduce the burden of IPV (36). Hadi (38, 39) maintained that women's productive roles through participation in credit programs and making financial contributions to their families not only improved women's positions in their households but also significantly reduced domestic violence.
However, women's participation in microfinance for earning was not associated with higher level of IPV (8). Women who meaningfully contributed to the family income through earnings were more likely to be experiencing violence (18). Women who were more equal with their husbands in their family relationships by participating in decision making increased their exposure to IPV by membership in microfinance programs (37). Women who make decisions about household purchases were more likely to experience physical abuse by their husbands (9, 40).
A relatively new idea of women's exit options from abusive marriages such as separation of marriage or divorce, which is more becoming common and recognized by the community, as indicated by Schuler and Nazneen (36). This is also a source of women's empowerment. Schuler et al. (33) observed that men's attitude of controlling their wives are changing and commented: Men's growing acceptance of egalitarian gender norms and their self-reported decreased engagement in IPV are driven largely by pragmatic self-interest: their desire to improve their economic status and fear of negative consequences of IPV.
Another vital source of empowerment of a married girl may be her ability to communicate with people outside home seeking advice, suggestions, or even help in crisis. Access to a mobile phone, for example, may serve this purpose, and such access may be realized through her own earnings or remittances from natal family or relatives or from her husband. This is also a source of empowerment which may help protect a wife from IPV perpetrated by her husband.
We hypothesize that spousal control is associated with IPV, i.e., a husband who fully controls his wife is more likely to practice IPV than a husband who does not control or minimally controls. The effect of control is minimized when (a) husband and wife are connected, i.e., spouses have a sense of togetherness, and (b) wife is empowered with her ability to communicate with people outside home owing to some resources owned by her.
Bangladesh is an early-childbearing society, as indicated above, three in ten women begin childbearing during adolescent ages. Parents in laws, family members, and relatives encourage the newlywed couples to have a child early after marriage at whichever age the marriage takes place. It is the social norm, there is even a pressure for newlyweds in favor of early childbearing and proving their ability of childbearing (41). Young male adults working abroad is common in Bangladesh, and Gipson and Hindin (41) observed in the communities with male migration observed that having a child may be one way to cement the bond between the husband and wife before he leaves for the country for work, meaning the encouragement of childbearing immediately after marriage.
Many young newly married girls/women fear that they may become childless or may not be able to bear a child with passage of time which is bolstered by their natal and marital family members (32). The family wants to see that the wife has given birth to a child. This has probably been derived from the perception that exists in subsistence and agricultural economies that children are beneficial to family earning and that children can join the workforce at an early age. It is also expected that a son will be born and will reach adulthood before the father reaches old age or dies so the son can take of the family.
Pressures come from in-laws to have a child immediately after marriage in India (42). The decision to have a child after marriage is largely influenced by in-laws and husbands—a woman's choice of low importance in Bangladesh (43). Delaying the first birth after marriage can cause rumors of infertility, bring shame upon the family, and in some cases lead the husband's family to seek another wife for their son (44). Additionally, social stigma for childless women, emigration of husbands, and the belief that using modern contraceptives prior to the birth of the first child results in infertility also inhibits couples from delaying their first pregnancy. It should be mentioned that there has been a rapid demographic transition in Bangladesh wherein fertility declined from over 6.0 births per woman to 2.3 births and life expectancy has declined from about 50 years to over 70 years in the last 40 years, the perceived benefit of early childbearing seems to remain in the older generation.
The young newly married women, e.g., adolescents ages 15–19 want to delay their childbearing and the family members encourage or sometimes pressurize newly married ones to have a child earliest possible time. While the women may pursue the delay, her spouse may support family members' view of early childbearing and demand the wife to have a child, and if there is disagreement the husband may become violent. In India, IPV was associated with the intention of delaying the first birth (45).
Therefore, we hypothesize that delaying of childbearing is associated with IPV among adolescents in Bangladesh.
Data for this study come from the nationally representative Bangladesh Adolescent Health and Wellbeing Survey 2019–20 (30) [The survey details are given in NIPORT (30), including the questionnaires.]. The age limit for adolescents in this survey was 15–19 years. The survey was based on a two-stage stratified sample of households, which involved sampling of primary sampling units (PSU), and sampling of households. At the first stage, PSUs were randomly selected from each stratum according to probability proportional to size of the number of households. PSUs were randomly and equally divided into Type 1 and Type 2 PSUs, and information on physical violence was collected from Type 2 PSUs. At the second stage, 67,093 households were selected from where 7,800 unmarried female adolescents, 4,926 ever-married female adolescents (2,904 in Type 1 and 2,022 in Type 2), and 5,523 unmarried male adolescents were selected for interview. The response rate for married adolescent sample was 97.2%. Data were collected on paper and pencil through face-to-face interviews at the home of the respondents by using a structured questionnaire. Our sample come from Type 2 PSUs and thus Type 2 questionnaire, and the respondents were 2,022 married adolescents.
All target adolescents in the selected households were included in the survey. However, if there were more than one adolescent in a household, the module that has questions on violence was not implemented. This was done on a consideration that multiple sample adolescents from the same household may feel embarrassed of the reportable incident(s) that occurred in the past 12 months with a fear that other respondent(s) would know about it. Only 3.3% of sample households had multiple adolescents. For our analysis we excluded 200 married adolescents whose husband resided outside home and did not visit home in past 12 months.
Our analysis considers appropriate sampling weights calculated based on the complex sampling design of the BAHWS 2019–20, and our sample consisted of 1,822 (weighted n = 1,846) married adolescent girls ages 15–19.
Table 1 shows the variables and measurements of factors and outcome used in this analysis.
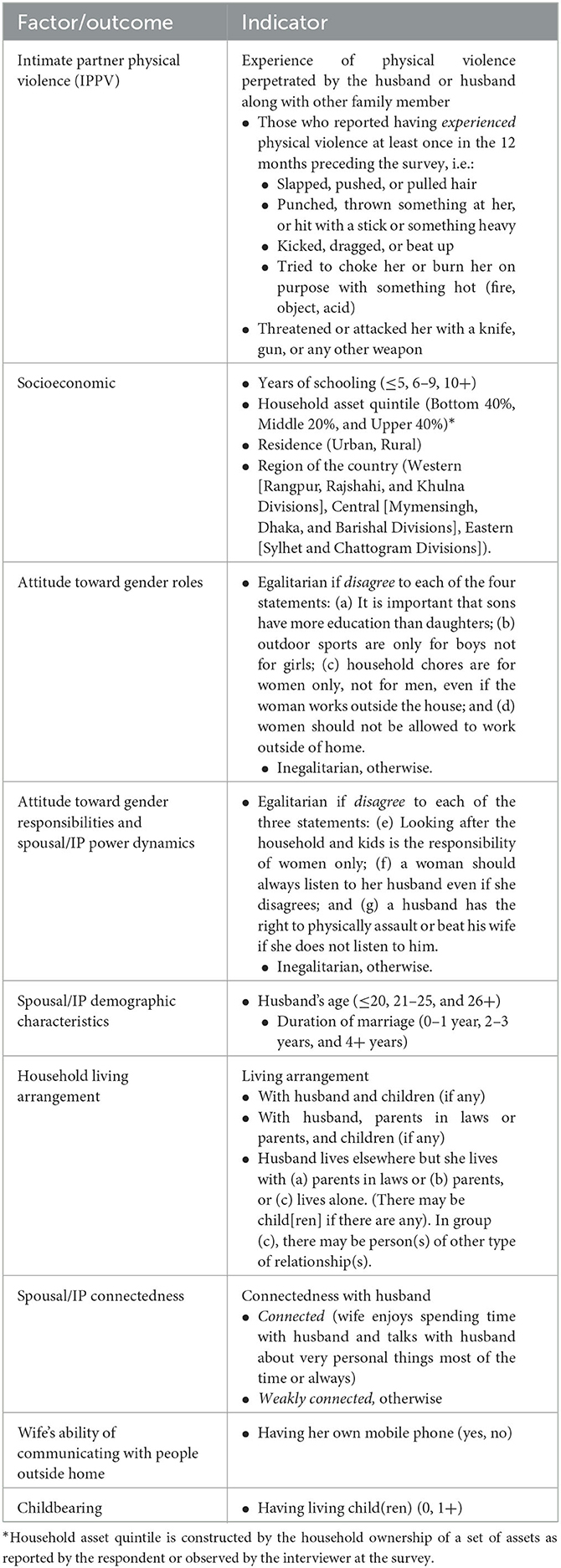
Table 1. Indicators and measurement of factors and outcome.
The 2019–20 BAHWS had five questions on the nature of physical violence experienced by married adolescents, see the first row in Table 1. If such violence was perpetrated by her husband at least once in the past 12 months of the survey is treated as IPPV. Answering Yes to at least one of the questions is defined as an outcome of IPPV and coded as 1, and otherwise as 0.
Husband's age is categorized as ≤ 20, 21–25, and 26+ and ≤ 20 category is treated as the reference category in the logistic regression. Duration of marriage is divided in to three groups: ≤ 1 year, 2–3 years, and 4+ years and the 1st year of marriage is treated as reference category.
We consider three categories of living arrangements: (a) with husband (and children, if any), (b) with husband and parents-in-law or parents and children if any, and (c) husband lives elsewhere but wife lives with parents-in-law or parents and children, if any. In group (c), there may be person(s) of other type of relationship(s). The category (a) here is treated as the reference category in the logistics regression.
We use two variables to capture the effect of spousal control: respondent's connectedness with her husband and respondent having her own mobile phone. On the married girl's connectedness with her husband, we assume that a married girl who has a feeling of connectedness with her husband, she is less likely to be fully controlled by her husband. A wife possessing a phone and using it is likely due to indicate two characteristics: (1) she can communicate with people outside home and (2) she has power, economic or otherwise, acquired either by her own earning, through inheritance of resources from relatives, or through negotiation with the husband. Such characteristics can soften or minimize a husband's controlling attitude and/or actual control over his wife.
The childbearing indicator is dichotomized as having at least one living child at the time of survey (coded as 1) and no living child is coded as zero.
We also include the following variables (see Table 1 for definitions):
• Years of schooling in three categories— ≤ 5 years (reference category), 6–9 years, and 10+ years.
• Attitude toward gender roles—Inegalitarian (reference category) and egalitarian.
• Attitude toward gender responsibilities and power dynamics in the family—Inegalitarian (reference category) and egalitarian.
• Household asset quintiles—Bottom 40% (reference category), middle 20%, and upper 40%.
• Region of the country—Western (reference category), Central, and Eastern.
• Residence—Urban (reference category) and Rural.
It is possible that IPPV is influenced by husband's education, husband's smoking or drinking habits, or respondent's parental education but the BAHWS 2019–20 did not collect information on those, neither did we have adolescents' information on religion.
We estimate the effects of various variables on IPPV in logistic regression model. The independent variables included in the regression model to represent the factors indicated in the conceptual framework. We did not use stepwise procedure to include or exclude the variables. We checked for multicollinearity between independent variables and none of the tests required to exclude any independent variables. For example, the mean Variance Inflation Factor (VIF) was 1.3 (and maximum limit was 1.76) which is much less than 10, the acceptable limit. We used STATA version 17. There were only seven records (0.38%) with missing values in two variables, and the STATA exclude those records that has a missing value.
Table 2 shows the distribution of 1,846 married adolescent girls according to categories of factors considered in the analysis. About one in four is an urban resident; about two in five are each from Western and Central regions; and about two in five from the upper 40% and about one in three from the bottom 40%. About one in four had no or less than 6 years of schooling, about half had 6 to 9 years of schooling, and about one in four had ten or more years of schooling. About two in five married girls had egalitarian attitudes toward gender roles (see Table 1) and about one in three had egalitarian attitudes toward gender responsibilities and spousal power dynamics.
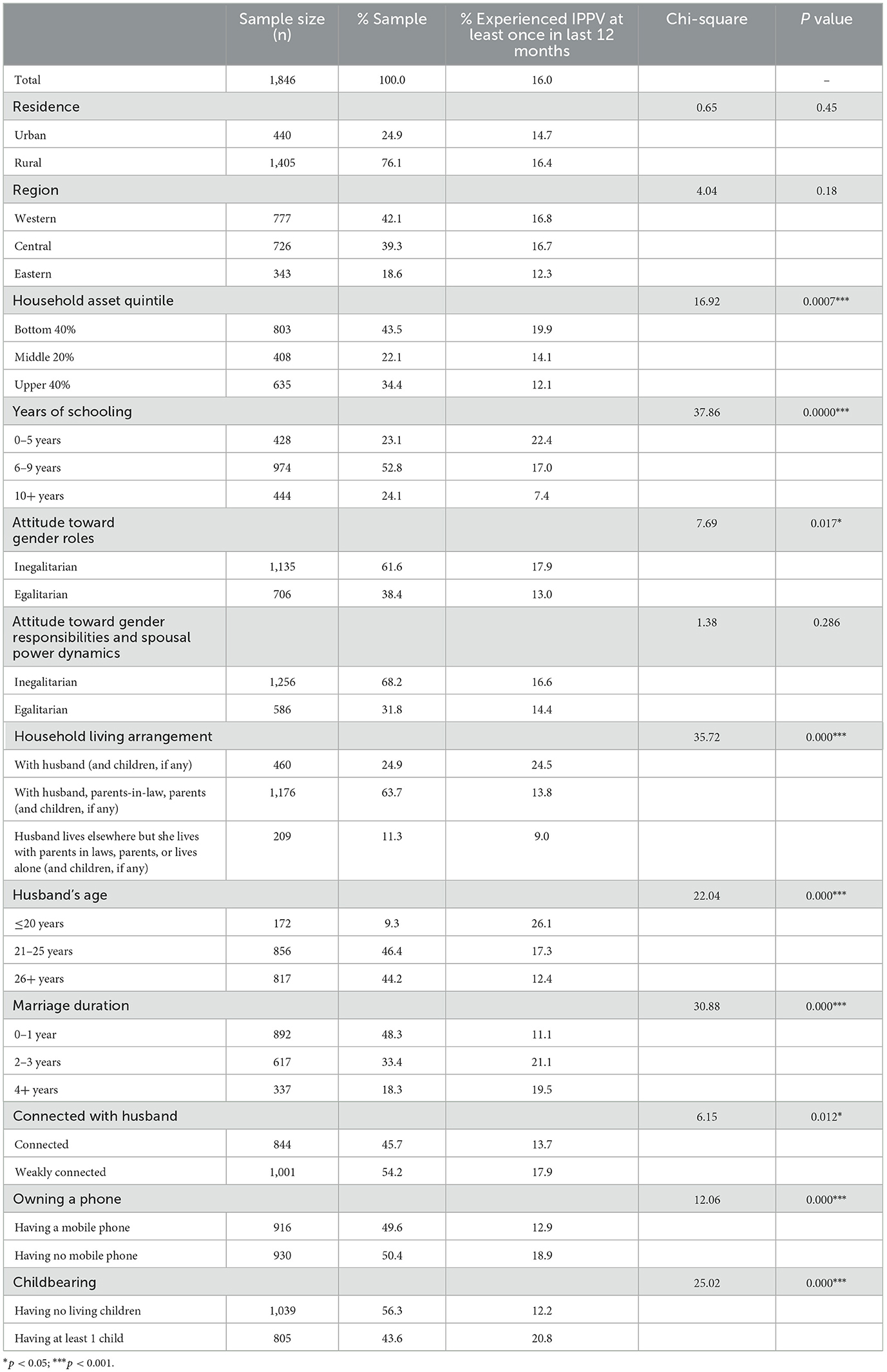
Table 2. Description of sample of currently married adolescents ages 15–19 who are exposed to IPPV, Bangladesh Adolescents Health and Wellbeing Survey 2019–20.
About one in four married girls lived alone with husband (including own children if any), about two in three lived in extended family with husband and at least one parent or parent-in-law, and about one in ten lived without husband but with at least one parent or parent-in-law.
While the girls were ages 15–19, 9, 46, and 44% of their husband were 20 or below, 21–25, and 26 and higher years of age, respectively (Table 2). Nearly half (48%) were married for less than 2 years, one third (33%) for 2–3 years, and about one in five (18%) were married for 4 or more years.
Slightly less than half of married girls were “connected” with their husband, measured by the indicator “enjoy spending time with husband and can talk with husband about very personal things most of the time or always” (Tables 1, 2). Also, half of the girls had their own mobile phone.
Regarding childbearing, 44% of married girls had at least one surviving child (Table 2).
Table 2 (Column 4) shows the prevalence of IPPV according to their characteristics. Sixteen percent of married girls reported that they experienced IPPV at least once in the past 12 months. IPPV was similar for rural and urban areas; it was slightly lower, not significantly, in the Eastern region than other regions; about 20% girls in the bottom 40% households experienced IPPV compared to 12% in the upper 40% households, the difference is significant (p < 0.001). IPPV substantially decreases with education, from 22% among girls with no or below 6 years of schooling to 17% among girls with 6–9 years of schooling to only 7% among those with 10 or more years of schooling (p < 0.001).
Girls with inegalitarian attitude toward gender roles had an IPPV rate of 18% compared to 13% among egalitarian (p < 0.05). IPPV differential in terms of attitude toward gender responsibilities and spousal power dynamics was similar between the inegalitarian and egalitarian groups (17 vs. 14%, not significant).
IPPV is strongly associated with living arrangement (p < 0.001); 25% girls living with husband alone (i.e., nuclear family) experienced IPPV compared to 14% among those who lived with husband and parents-in-law, or parents. Those girls who lived without her husband (i.e., her husband lived elsewhere but visited home sometimes) but with in-laws or parents have significantly lower IPPV rate of 9% than other groups.
IPPV risk significantly decreases from 26% among those whose husband was 20 years old or younger to 17% among those whose husband were 21–25 years old to only 12% among those with husband of 26 years or older (p < 0.001). The risk increases with the duration of marriage (11% among those with 0–1 year of duration vs. about 20% among those with higher duration [p < 0.001]).
IPPV risk is moderately associated with girls' “connectedness” with their husbands (p < 0.05)−14 vs. 18% for the connected and weakly connected groups, respectively. Not having a mobile phone exposes girls to IPPV as it was 19% among those who did not have a phone compared to 13% among those who had a phone (p < 0.001).
IPPV rate was 21% among married girls without a living child compared to only 12% among those who had at least one living child (P < 0.001).
We modeled IPPV risk associated with factors under consideration by using logistic regression (Table 3). We considered contextual and socioeconomic factors such as rural-urban residence, geographical region, household asset quintiles, girls' education, and two variables capturing girls' attitudes toward gender roles. The model includes spousal demographic characteristics (husband age and marital duration), spousal connectedness and the girl's ownership of a mobile phone, household living arrangement, and a childbearing (measured as having at least one living child) indicator. We included the interaction term “living children x marriage duration.” Adjusted odds ratios (AOR) are shown in Table 3.

Table 3. Binary logistic regression-based unadjusted odds ratios (OR) and adjusted odds ratios (AOR) of IPPV among currently married adolescents ages 15–19, Bangladesh Adolescents Health and Wellbeing Survey 2019–20.
AOR of IPPV is 0.45 and 0.33, respectively, for girls whose husband were ages 21–25 and 26 or more years old compared to girls with husband younger than 21 (p < 0.001) (Table 3). These findings demonstrate that girls with husbands ages 21–25 and 26 or higher have 55% ([1.00–0.45] × 100) and 67% ([1.00–0.33] × 100) lower odds of IPV than their counterpart girls with husbands younger than 21. Thus, we find that adolescent girls marrying relatively older husband provide a IPPV protective effect, and our hypothesis is supported.
Table 3 shows that adolescent girls who lived with their parents-in-law or parents have an AOR of 0.56 (p < 0.01), meaning that the odds of their IPPV are 44% lower than those girls who live with her husband alone or within a nuclear family. Thus, living with in-laws or parents provide a protective effect on IPPV, and a support for our hypothesis. Girls who live with in-laws or parents, but without their husbands, have even lower odds of IPPV, i.e., 56% ([1.00–0.44] × 100) lower than girls who live with alone with their husbands or in nuclear families. These lower odds reflect the effect of infrequent exposure to IPPV as the husband lived elsewhere and visited the wife and family occasionally.
Spousal connectedness is not associated with IPPV as indicated by the non-significant AOR related to the category “weakly connected,” although it was significant in the bivariate association. Owning a mobile phone is significantly associated with the risk of experiencing IPPV as AOR of not owning one is 1.39 and is statistically significant (p < 0.05).
Our measure of childbearing is whether a girl has at least one living child (Table 2). Our hypothesis is that a girl who survives having a child is less likely to experience IPPV risk than her counterpart without a child. Having a living child is associated with marriage duration which is associated with IPPV as shown in bivariate findings (Table 2). We include an interaction between marriage duration and the childbearing indicator in Table 3.
Significant interaction occurs between having a child and the duration of marriage (Table 3). Figure 2 shows three distinct effects:
• IPPV risk for girls who did not a have living child increases from 11% during year 0–1 to 17% during years 2–3 to 29% after 4 or more years of marriage.
• IPPV risk is higher among those who have a child immediately after marriage (0–1 year) than those who have not yet have a child (18 vs. 11%).
• IPPV risk for girls with a child is about similar for the years of marriage duration.
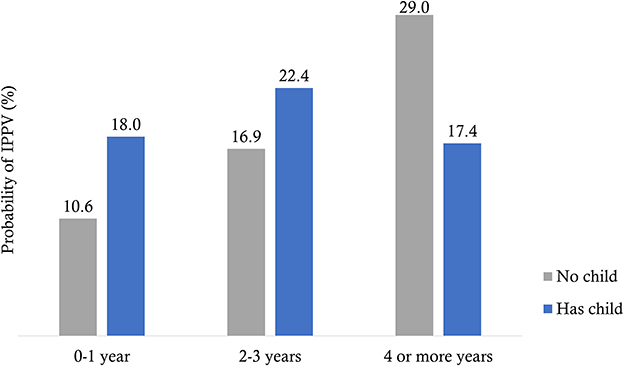
Figure 2. Predicted probability of IPPV based on model interaction between marriage duration and having a child.
We found that the longer girls wait to have a child the higher the risk of IPPV, and thus, our hypothesis is supported.
Rural-urban residence and region were not significantly associated with IPPV in the bivariate analysis (Table 2) nor in the multivariate regression (Table 3). Household asset quintiles and girls' years of schooling were significantly associated with IPPV in bivariate analysis but only years of schooling is significantly associated with IPPV in the multivariate regression (p < 0.01). IPPV risk is significantly lower among girls who have 10 or more years of schooling than others. Among the two factors influencing attitudes toward gender roles, none were significantly associated with IPPV according to the regression models.
We analyzed intimate partner physical violence data from 1,846 married adolescent girls ages 15–19 based on the nationally representative adolescents survey conducted in 2019–20. We tested four hypotheses—adolescent girls married to husbands ages 25 and older, adolescents living in extended families with parents-in-law or parents, adolescents who are minimally controlled by their husbands, and adolescents who have a child immediately after marriage are protective of IPPV in Bangladesh. We find support in favor of each of the hypotheses. The findings are new, to our knowledge, except for that on the association between spousal control and IPPV.
The finding that girls married to husbands beyond the age of youthhood, i.e., 25 years or older, are protective of IPPV is like that of Adebowale (46) in Nigeria which indicates that women married to relatively older husband (measured by age difference between husband and wife) have lower likelihood of IPV in general and IPPV and emotional violence, but not true for sexual violence. Our finding implies that strictly adhering to the Bangladesh law that requires men marrying at 21 or later can reduce married girls' risk of IPPV. Increase in males' ages at marriage will benefit adolescent girls from the risk of IPV as well as through their reduced likelihood of adolescence marriage, and men should be encouraged to marry girls who are 20 or older or at least 18 years old girls as required by law.
We find that married adolescents living with parents-in-law or parent(s) helps reduce IPPV. Various studies and anecdotes indicate that living with in-laws, especially mother-in-law, is a risk of IPPV, but Schuler et al. (33) observed that there has been ideological change among in-laws wherein they believe that daughters-in-law need to be treated with dignity and respect. This is because of social and economic development and their daughter-in-law's increased economic role in families. Our finding is consistent with the notion of changed attitudes toward compromised behavior of husbands in terms of IPPV.
As Bangladesh is in transition from a traditional to contemporary economy, it is still expected that newlywed couples will begin their lives in extended family settings and then move toward nuclear ones. Our findings show that 25% married adolescents live in nuclear families, 64% with parents-in-law or parent(s), and 11% with parents-in-law or parent(s) but the husband lives elsewhere (usually for work). One reason young couples live in a nuclear family is when one of the spouses' (mostly the husband's) workplace is distant from the husband's natal home. Some young girls work in the non-agricultural sector (e.g., garment factories) and their husbands may accompany her to live in city areas. The proportion of this nuclear living arrangement is probably increasing because of the growing economic activities of the non-agricultural sector, and thus, likely increases IPPV risk for young married women.
A husband's control of his wife is a source of IPPV, but this control is moderated or lessened when his wife has some power. This can mean having a phone that enables her to communicate with the outside world. Owning a phone may also be related to her economic power, helping reduce the burden of IPPV. We argue that ownership of a mobile phone is possible through a wife's income earnings or through remittance obtained from relatives or even from her husband. However, the literature suggests, as we show in our conceptual framework, that income earning can have both negative and positive effect on IPV in Bangladesh (18, 36, 38–40). The negative association of having a phone and IPPV is likely to work through social isolation and IPV hypothesis as well as instrumental social support and IPV hypothesis (35). The social isolation hypothesis asserts that those women who communicate with natal or other kins or relatives more frequently are less likely to experience IPV and the instrumental social support hypothesis claims that those women who have someone in the same or neighboring communities willing to provide support are less likely to face IPV. In Bangladesh, instrumental support is available even at the local government level through the newly enacted Domestic Violence (Prevention and Protection) Act 2020 (7). Phone calls can be a vehicle of communication to satisfy these hypotheses and thus likely reduce IPPV. IPPV is likely to decline over time with economic growth, which is occurring rapidly in Bangladesh, that benefits women in owning mobile phone.
We did not find any significant association between spousal connectedness and IPPV. Our argument was that connectedness between spouses would reduce the feeling of husband's control over his wife and thus lower IPPV. One reason why we did not find significant association between connectedness and IPPV may be that the indicator we used is not an appropriate measure of connectedness. It is also possible that IPPV itself has a negative effect on connectedness in that a wife experiencing IPPV does not feel close to her husband. Without closeness, a wife may not share personal ideas with her husband, and thusly there is no significant association between connectedness and IPPV.
Childbearing is strongly associated with IPPV, specifically in that IPPV continues to increase with marriage duration if the wife does not have a living child. In contrast, having a living child puts a married girl at a moderate risk of IPPV in the early years of marriage but it does not increase with marriage duration. This finding is consistent with the common belief that the family, including the in-laws, and the society in general expect that a child should be born immediately after marriage as observed by previous researchers (41, 42). If that does not happen the married girl is at the risk for IPPV.
This finding is disturbing because childbearing during adolescence is harmful for both maternal and infant/child health. Healthcare providers recommend avoiding having a birth before age 20. Adolescent girls are in a quandary and those who desire to follow the health advice intend to use contraception. But pressures come from in-laws and family against contraceptive use at this time of her life, and, in some cases the husband joins the family against contraceptive use. This situation may lead to violence against the girl.
We are in a dilemma; should we recommend delaying childbearing after age 20 as recommended by public health practitioners? If we do, the adherent girls will be at increased risk of IPPV. Also, a significant portion of married adolescent girls who had a birth reported that they wanted to have the birth later, as shown in our companion study (5). Adolescent girls who wanted to have the birth later had 1.30 times higher risk of major depressive disorder than those who wanted the birth earlier.
We will still recommend waiting to have children after the age of 20. Following our recommendation of raising the age at marriage, we reiterate that an increase in age at marriage will minimize or even eliminate the chance of adolescent childbearing and thus reduce maternal and child health risks and the risk of IPV. However, there is only a slow increase in age at marriage—it has increased from 15.3 years in 1993 to 17.5 years in 2017, roughly a year per decade. A germane question is how can we accelerate the pace of increasing age at marriage? An obvious solution to this is keeping girls in school for 12 years of education. Although there has been a praiseworthy improvement in education in Bangladesh, only 34%, or one in three, married women aged 20–24 had 10 or more years of schooling in 2017–18. In many countries it is required that young people complete 12 years of schooling (i.e., high school graduation) and by that time they are usually 18 years old or over. Providing girls with high school or higher education also helps nation building and thus facilitating social and economic development. Girls from families that cannot afford this may be given scholarships. Cost-benefit analysis will likely show this is a noble option, and future research should be conducted in this area.
An important limitation of this study is that we analyzed cross-sectional IPPV data of quantitative nature from an adolescent health and wellbeing survey which did not have more in-depth information on issues related to IPPV. We only identified factors affecting IPPV but do not know the exact mechanisms of how these factors caused IPPV. We exercise caution that we measure association but not cause-and-effect relationships between various factors and IPPV. Further research particularly of qualitative nature can help better understand such mechanisms of IPPV among married adolescents. There is dearth of qualitative studies of IPV in Bangladesh, e.g., 6 in his review mentioned that there were 17 quantitative studies, 11 jointly quantitative and qualitative, and only 3 qualitative studies.
To conclude, married adolescent girls living with parents-in-law or parents, girls married to relatively older boys/men, having a power of communicating with outside world, and having a child immediately after marriage are protective of IPPV in Bangladesh. Strictly adhering to the law that requires men to marry at 21 or older can reduce married girls' risk of IPPV. Raising girls' age at marriage can minimize adolescents' IPPV and other health risks associated with adolescent childbearing.
Publicly available datasets were analyzed in this study. This data can be found here: https://dataverse.unc.edu/dataset.xhtml;jsessionid=2041ade5046836520c1117daa52b?persistentId=doi%3A10.15139%2FS3%2FDVEI9A&version=&q=&fileTypeGroupFacet=%22Tabular+Data%22&fileAccess=&fileTag=&fileSortField=&fileSortOrder=.
The studies involving human participants were reviewed and approved by icddr,b ERC. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
MR and KJ conceptualized the study and designed the analysis. NC and MMH performed the statistical analysis. MR drafted the manuscript. SK provided support in literature review and in writing part of the discussion. KJ, MMH, QN, and SK reviewed the manuscript. All authors reviewed, contributed to finalization of the manuscript, and approved the final version of the article.
This publication was produced with the support of the United States Agency for International Development (USAID) under the terms of USAID's Research for Decision Makers (RDM) Activity cooperative agreement no. AID-388-A-17-00006 and of Data for Impact (D4I) associate award no. 7200AA18LA00008. Data source for this publication is the Bangladesh Health and Wellbeing Survey 2019-20 (BAHWS 2019-20) funded by the US Agency for International Development (USAID) through the MEASURE Evaluation Project, Data for Impact (D4I) Project and Research for Decision-Makers (RDM) Activity (GR: 154601546). Additional funding was provided by the Foreign, Commonwealth and Development Office (FCDO) and by the Government of Bangladesh. The BAHWS 2019-20 was implemented under the authority of the National Institute of Population Research and Training (NIPORT) of the Government of the People's Republic of Bangladesh. The BAHWS 2019-20 data were collected and processed by Human Development Research Center (HDRC).
The authors are grateful to Anadil Alam from icddr,b who facilitated the research team's activities and Kaiser Mahmud who helped in the initial data analysis. Nurul Alam from icddr,b and Md. Mahabubur Rahman from icddr, b/D4I provided helpful comments. The authors would also like to thank Sian Curtis and Gabriela Escudero from D4I for their careful review of the publication and Katie Kosma from the Knowledge Management (KM) team of D4I for providing editing support of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Center for Disease Control and Prevention. Fast Facts: Preventing Intimate Partner Violence. (2010). Available online at: https://www.cdc.gov/violenceprevention/intimatepartnerviolence/fastfact.html (accessed October 3, 2022).
2. World Health Organization. Violence Against Women. (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/violence-against-women (accessed March 22, 2023).
3. Silverman JG, Decker MR, Gupta J, Kapur N, Raj A, Naveed RT. Maternal experiences of intimate partner violence and child morbidity in Bangladesh: Evidence from a national bangladeshi sample. Arch Pediatr Adolesc Med. (2009) 163:700–5. doi: 10.1001/archpediatrics.2009.115
4. Hossain MA, Sumi NS, Haque ME, Bari W. Consequences of intimate partner violence against women on under-five child mortality in Bangladesh. J Interpers Violence. (2014) 291402–1417. doi: 10.1177/0886260513507140
5. Haider MM, Jamil K, Ahsan KZ. Mental Health of Marries Adolescents Following Pregnancy Outcome in Bangladesh. Dhaka (2023).
6. Yount KM, Crandall AA, Cheong YF, Osypuk TL, Bates LM, Naveed RT, et al. Child marriage and intimate partner violence in rural Bangladesh: A longitudinal multilevel analysis. Demography. (2016) 53:1821–52. doi: 10.1007/s13524-016-0520-8
7. Khan AR. Domestic violence against women in bangladesh: a review of the literature and the gaps to fill-in by future interventions. Khazar J Humanit Soc Sci. (2015) 18:57–81. doi: 10.5782/2223-2621.2015.18.3.57
8. Murshid NS, Akincigil A, Zippay A. Microfinance participation and domestic violence in Bangladesh: results from a nationally representative survey. J Interper Violence. (2016) 31:1579–96. doi: 10.1177/0886260515569065
9. Rahman M, Hoque MA, Makinoda S. Intimate partner violence against women: is women empowerment a reducing factor? A study from a national bangladeshi sample. J Fam Viol. (2011) 26:411–20. doi: 10.1007/s10896-011-9375-3
10. Sambisa W, Angeles G, Lance PM, Naved RT, Thornton J. Prevalence and correlates of physical spousal violence against women in slum and nonslum areas of urban Bangladesh. J Interpers Violence. (2011) 26:2592–618. doi: 10.1177/0886260510388282
11. Islam R, Alam R, Islam R. Factors Affecting Physical Violence against Women in Bangladesh. Int J Adv Multidisc Soc Sci. (2015) 1:1–6. doi: 10.5923/j.jamss.20150101.01
12. National National Institute of Population Research and Training (NIPORT) and ICF. Bangladesh Demographic and Health Survey 2017–18. Dhaka, Bangladesh, and Rockville, Maryland, USA: NIPORT and ICF. (2020).
13. Nasrullah M, Zakar R, Zakar MZ. Child marriage and its associations with controlling behaviors and spousal violence against adolescent and young women in Pakistan. J Adolesc Health. (2014) 55:804–9. doi: 10.1016/j.jadohealth.2014.06.013
14. Oshiro A, Poudyal AK, Poudel KC, Jimba M, Hokama T. Intimate partner violence among general and urban poor populations in Kathmandu, Nepal. J Interpers Violence. (2011) 26:2073–92. doi: 10.1177/0886260510372944
15. Rahman M, Hoque A, Mostofa G, Makinoda S. Association between adolescent marriage and intimate partner violence: A study of young adult women in Bangladesh. Asia-Pacific J Public Health. (2014) 26:160–8. doi: 10.1177/1010539511423301
16. Raj A, Saggurti N, Lawrence D, Balaiah D, Silverman JG. Association between adolescent marriage and marital violence among young adult women in India. Int J Gynecol Obstetr. (2010) 110:35–9. doi: 10.1016/j.ijgo.2010.01.022
17. Speizer IS, Pearson E. Association between early marriage and intimate partner violence in India: A focus on youth from Bihar and Rajastha. J Interpers Violence. (2011) 26:1963–81. doi: 10.1177/0886260510372947
18. Bates LM, Schuler SR, Islam F, Islam K. Socioeconomic factors and processes associated with domestic violence in rural Bangladesh. Int Fam Plan Perspect. (2004) 30:190–9. doi: 10.1363/3019004
19. Khan ME, Rob U, Hossain SM. Violence against women and its impact on women's lives-some observations from Bangladesh. J Fam Welf. (2000) 46:12–24.
20. Naved RT, Persson LA. Factors associated with spousal physical violence against women in Bangladesh. Stud Fam Plann. (2005) 36:289–300. doi: 10.1111/j.1728-4465.2005.00071.x
21. Naved RT. Sexual Violence Towards Married Women in Bangladesh. Arch Sex Behav. (2013) 42:595–602. doi: 10.1007/s10508-012-0045-1
22. Jeyaseelan L, Kumar S, Neelakantan N, Peedicayil A, Pillai R, Duvvury N. Physical spousal violence against women in India: Some risk factors. J Biosoc Sci. (2007) 39:657–670. doi: 10.1017/S0021932007001836
23. Naved RT, Persson LA. Dowry and spousal physical violence against women in Bangladesh. J Fam Issues. (2010) 31:830–56. doi: 10.1177/0192513X09357554
24. Khan ME, Aeron A. Prevalence, nature and determinants of violence against women in Bangladesh. J Fam Welf. (2006) 52:33–51.
25. Fattah KN, Camellia S. Gender norms and beliefs, and men's violence against women in rural Bangladesh. J Interpers Violence. (2017) 35:771–93. doi: 10.1177/0886260517690875
26. Dalai K, Lindqvist K. A National study of the prevalence and correlates of domestic violence among women in India. Asia-Pacific J Public Health. (2012) 24:265–277. doi: 10.1177/1010539510384499
27. Schuler SR, Lenzi R, Nazneen S, Bates LM. Perceived decline in intimate partner violence against women in Bangladesh: qualitative evidence. Stud Family Plann. (2013) 44:243–257. doi: 10.1111/j.1728-4465.2013.00356.x
28. Hossain MM, Abdulla F, Rahman A, Khan HTA. Prevalence and determinants of wife-beating in Bangladesh: evidence from a nationwide survey. BMC Psychiatry. (2022) 22:9. doi: 10.1186/s12888-021-03652-x
29. Bhuiya A, Sharmin T, Hanifi SMA. Nature of domestic violence against women in a rural area of Bangladesh: implication for preventive interventions. J Health, Populat Nutr. (2003) 21:48–54.
30. National National Institute of Population Research and Training (NIPORT) International Centre for Diarrhoeal Disease Research Bangladesh (icddr b) and Data for Impact. Bangladesh Adolescent Health and Wellbeing Survey 2019–20: Final Report. Dhaka, Bangladesh, and Chapel Hill, NC, USA: NIPORT, icddr,b, and Data for Impact. (2021).
31. Rashid M, Kader M, Perera NK, Sharma A. Wife beating: A population-based study in Bangladesh. Violence Gender. (2014) 1:170–175. doi: 10.1089/vio.2014.0015
32. Schuler SR, Bates LM, Islam F, Islam K. The timing of marriage and childbearing among rural families in Bangladesh: Choosing between competing risks. Soc Sci Med. (2006) 62:2826–37. doi: 10.1016/j.socscimed.2005.11.004
33. Schuler SR, Lenzi R, Badal SH, Nazneen S. Men's perspectives on women's empowerment and intimate partner violence in rural Bangladesh. Culture, Health Sexual. (2018) 20:113–27. doi: 10.1080/13691058.2017.1332391
34. Richardson RA, Haight SC, Hagaman A, Sikander S, Joanna M, Lisa MB. Social support and intimate partner violence in rural Pakistan: A longitudinal investigation of the bi-directional relationship. SSM - Population Health. (2022) 19:101173. doi: 10.1016/j.ssmph.2022.101173
35. Stoff LW, Bates LM, Schuler SR, Renner LM, Erickson DJ, Osypuk TL. Intimate partner violence and social connection among married women in rural Bangladesh. J Epidemiol Community Health. (2021) 75:1202–7. doi: 10.1136/jech-2020-214843
36. Schuler SR, Nazneen S. Does intimate partner violence decline as women's empowerment becomes normative? Perspectives of bangladeshi women. World Dev. (2018) 101:284–92. doi: 10.1016/j.worlddev.2017.09.005
37. Dalal K, Dahlström Ö, Timpka T. Interactions between microfinance programmes and non-economic empowerment of women associated with intimate partner violence in Bangladesh: A cross-sectional study. BMJ Open. (2013) 3:e002941. doi: 10.1136/bmjopen-2013-002941
38. Hadi A. Women's productive role and marital violence in Bangladesh. J Fam Violence. (2005) 20:181–9. doi: 10.1007/s10896-005-3654-9
39. Hadi A. Prevalence and correlates of the risk of marital sexual violence in Bangladesh. J Interpers Violence. (2000) 15:787–805. doi: 10.1177/088626000015008001
40. Akhter R, Wilson JK. Using an ecological framework to understand men's reasons for spousal abuse: An investigation of the Bangladesh Demographic and Health Survey 2007. J Fam Viol. (2016) 31:27–38. doi: 10.1007/s10896-015-9741-7
41. Gipson JD, Hindin MJ. ‘Marriage means having children and forming your family' so what is the need of discussion?' Communication and negotiation of childbearing preferences among Bangladeshi couples. Culture, Health and Sexuality. (2007) 9:185–98. doi: 10.1080/13691050601065933
42. Dixit A, Bhan N, Benmarhnia T, Reed E, Kiene SM, Silverman J, et al. The association between early in marriage fertility pressure from in-laws' and family planning behaviors, among married adolescent girls in Bihar and Uttar Pradesh, India. Reprod Health. (2021) 18:60. doi: 10.1186/s12978-021-01116-9
43. Chowdhury SA, Talukdar A, Naveed RT. Young women's decision-making regarding timing of first conception in Dhaka slums. In: 7th Asia Pacific Conference on Reproductive and Sexual Health and Right. (2014) 21.
44. Henry EG, Lehnertz NB, Alam A, Ali NA, Williams EK, Rahman SM, et al. Sociocultural factors perpetuating the practices of early marriage and childbirth in Sylhet District, Bangladesh. Int Health. (2015) 7:212–217. doi: 10.1093/inthealth/ihu074
45. Ibarra-Nava I, Choudhry V, Agardh A. Desire to delay the first childbirth among young, married women in India: a cross-sectional study based on national survey data. BMC Public Health. (2020) 20:350. doi: 10.1186/s12889-020-8402-9
Keywords: intimate partner violence, intimate partner physical violence, adolescence marriage, living arrangement, spousal control
Citation: Rahman M, Jamil K, Nahar Q, Chakraborty N, Haider MM and Khan S (2023) Factors that provide protection against intimate partner physical violence among married adolescents in Bangladesh. Front. Public Health 11:1125056. doi: 10.3389/fpubh.2023.1125056
Received: 15 December 2022; Accepted: 24 February 2023;
Published: 03 April 2023.
Edited by:
Omid Dadras, University of Bergen, NorwayReviewed by:
Natarajan Gopalan, Central University of Tamil Nadu, IndiaCopyright © 2023 Rahman, Jamil, Nahar, Chakraborty, Haider and Khan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mizanur Rahman, cmFobWFubUBlbWFpbC51bmMuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.