 Caroline Figueira Pereira
Caroline Figueira Pereira Divane de Vargas1
Divane de Vargas1- 1Mental Health and Psychiatric Nursing, School of Nursing, University of São Paulo, São Paulo, Brazil
- 2School of Nursing, University of North Carolina at Chapel Hill, Chapel Hill, NC, United States
Background: The comorbidity of anxiety and drug use disorders complicates treatment prognosis, and one of the greatest challenges is to address the environmental and behavioral factors involved. The aim of this study was to describe the uses of intervention mapping in the design of a theory and evidence-based complex intervention to develop skills around the management of anxiety for cocaine users in outpatient addiction treatment.
Methods: The six steps of the intervention mapping approach, which are needs assessment, creation of matrices of performance objectives, selection of methods and practical strategies, program development, adoption and implementation, and evaluation were applied to develop the Interpersonal Theory of nursing to Anxiety management in people with Substance Use Disorders (ITASUD) intervention. The theory used for the conceptual model was interpersonal relations theory. All theory-based methods and practical applications were developed at the individual level, acting in behavioral, interpersonal, organizational and community environments.
Results: The intervention mapping provided a broad overview of the problem and outcome expectations. The ITASUD intervention consists of five consecutive sessions of 110-min targeting individual determinants of anxiety (knowledge, triggers, relief behaviors, self-efficacy and relations), delivered by a trained nurse using Peplau's concepts of interpersonal relations. Intervention Mapping is a multi-step process that incorporates theory, evidence, and stakeholder perspectives to ensure that implementation strategies effectively address key determinants of change.
Conclusions: The intervention mapping approach increases the effectiveness of the intervention since the matrices provide a broad view of all factors that affect the problem and facilitate replication through transparency of the determinants, methods, and applications used. ITASUD addresses all factors that play an important role in substance use disorders based on a theoretical basis, which provides the translation of evidence from research into effective practice, policy, and public health improvements.
Background
The comorbidity of anxiety with drug use disorders has been investigated by several researchers (1), and a strong association has been shown. This association complicates treatment prognosis and increases services utilization and health care costs, generating a global issue. The main challenges are to address both anxiety and substance use disorders by identifying the relationship between them and the environmental and behavioral factors involved.
Anxiety is one of the most prevalent health problems worldwide, generating health care costs, a high burden of disease, and implications associated with untreated illness that affect health, economic, and social sectors (2). According to the World Health Organization (3), the consequences of anxiety disorders occupy the 6th position in the ranks of contributors to global disability. Clinical reviews have shown that the presence of an anxiety disorder is a risk factor for the development of mood disorders and substance abuse (1, 2) and is highly comorbid with other mental disorders (4, 5).
Research has shown a 14.9% increase since 2005 in the number of people living with anxiety (6), and 21% of that estimated number is in the region of the Americas (3). In Brazil, the prevalence of anxiety disorders is 9.3% (3) of the population, and another factor that has been shown to be related to this prevalence is the increase in cocaine users in the country. Currently, cocaine is the most commonly used stimulant in Brazil. One explanation is that Brazil is the largest cocaine market in South America, because of its geographic position (neighboring the world's largest cocaine producers—Peru, Colombia and Bolivia), and leader in the cocaine trafficked from South America to Africa, Europe and Africa (6). A previous study (7) showed that the prevalence of cocaine users in the country is ~3.2 million people. This high prevalence occasioned an increase in cocaine users arriving in emergency care, resulting in Brazilian cocaine users arriving in emergency care at three times higher rates than elsewhere in the world (8, 9). This high demand in emergency care demonstrates that it is necessary to optimize treatment in specialized facilities for people with substance use disorders to avoid this high demand in emergency care.
The major challenge with this population is keeping them in specialized treatment, as high levels of anxiety are the main cause for relapse and withdrawal from treatment. One of the keys for keeping this population in treatment is to treat the anxiety experienced by cocaine users. This article presents the development of an implementation intervention called the Interpersonal Theory of nursing to Anxiety management in people with Substance Use Disorders (ITASUD) that can be incorporated into daily health care programs in early intervention focusing on the management of anxiety in cocaine users with a focus on the steps of the intervention mapping (IM) approach. These steps of IM are guided by theory, evidence, and input from relevant stakeholders perspectives to improve the effectiveness and ensure that implementation strategies effectively address key determinants of change (10, 11). Since, according to studies (12, 13), the implementation strategies often were poorly conceived, with incongruence between strategies and determinants, and the effect is variable and tends to be small to moderate; it remains unclear how determinants should be identified, decisions should be made on which determinants are most important to address, and strategies should be selected to address the important determinants (13). This signals a need for more rigorous processes and methods to guide these key steps of implementation strategy selection and tailoring (10–14).
Peplau's theory
The Peplau's theory provides the concepts that guide in the establishment of a strategic communication with clients by using an observational, experiential, and reflexive approach in structured and unstructured interactions. A central driver of the interpersonal relationship process developed by Peplau is anxiety, which, if strategically approached, can be a key to clients' health problems (15). Anxiety is defined by Peplau as a tension that generates energy transformation, this energy transformation generates physiological and behavioral answers. The main way to work with the tension of anxiety is to learn how to be aware of it and enact strategies that keep the level of anxiety in the mild to moderate range, which allows it to power productive growth. However, the tension of anxiety is often neglected in the interpersonal relationship due to the lack of theoretical knowledge and research addressing anxiety, mainly in the treatment of individuals with substance use disorders. The use of psychoactive substances is a kind of relief behavior used to decrease anxiety, and it can be transformed into a pattern of behavior that changes the self-system. Therefore, to treat people with substance disorders, it is necessary to treat the anxiety felt by them, because it is this anxiety that leads to the initiation of psychoactive substances and that plays an important role in relapse, and to keep patients in treatment.
Method
The methodology used to develop the intervention was the systematic IM (16) development process. IM is a framework consistent with the Medical Research Council (17) guidance on developing complex interventions and has been used to develop intervention programs for many health behaviors (18–23) because it employs an ecological approach that considers environmental influences on behavior and develops methods and strategies to address them (18).
IM is very useful because it specifies processes for integrating theoretical constructs and evidence-based literature for the purposeful development of an intervention through a description of a logical planning process. IM is a six-step process that is structured and sequenced as follows: (1) needs assessment (logic model of the problem); (2) creation of matrices of performance objectives (logic model of change); (3) selection of theory-based methods and practical strategies (program design); (4) program development; (5) adoption and implementation; and (6) evaluation.
Step 1: Needs assessment
The aim of step 1 is to develop the logic model of the problem, which allows for the programming of goals for the intervention related to health and quality of life. The logic model in the present study was based on the combination of a comprehensive understanding of the problem through Peplau's theory, empirical data about the factors that contribute to the problem, and experiential information about the problem. In addition, this step focuses on the description of the intervention context (population, setting and community).
Step 2: Creation of matrices of performance objectives
Step 2 of IM involves the following: (1) developing a statement of expected outcomes related to behavior and the environment, and developing performance objectives related to those behavioral and environmental outcomes; (2) identifying selected determinants related to the behavioral and environmental outcomes; and (3) constructing matrices of change objectives and creating the logic model of change.
The main aim of this step is the development of the logic model of change, which represents pathways of the intervention that act from behavioral and environmental perspectives through the connections between determinants and change objectives, performance objectives, desired outcomes, and improved quality of life in relation to the health problem of anxiety.
Step 3: Selection of theory-based methods and practical strategies
Step 3 is to generate program themes, components, scope and sequence. To accomplish this aim, we chose Peplau's theory as a conceptual model and method and selected evidence-based methods to reach change objectives. We also used published guidance on the intervention mapping approach (16) to choose some methods based on the definition and parameter of each method.
Step 4: Program development
Guided by the matrices, the team started to refine program structure and organization, prepare plans for program materials, and develop specific messages, materials and protocols. The change objectives were converted into practical applications using a range of evidence-based research. At the end of this step, the definitive intervention content and materials were created based on relevant additions made through the team discussion.
Step 5: Adoption and implementation
The aim of the program implementation plan was to determine the balance between what was planned and what could be implemented in the real world through the identification of potential users (adopters, implementers and maintainers) and the context in which the users are inserted, resulting in a better implementation design. Additionally, an intervention manual was adapted to increase the chances of adoption, implementation and sustainability.
Step 6: Evaluation
After step 5, adoption and implementation, this program was evaluated through operational definitions of feasibility, such as acceptability, demand, practicality, and adaptation (24).
The qualitative data were analyzed using thematic analysis described by Braun and Clarke (25) for identify, analyze, and reporting patterns within data. The phases of thematic analysis were: (1) familiarizing with the data—transcription of the data, reading and re-reading the data, noting down initial ideas; (2) generate initial codes—coding interesting features of the data across the entire data set, collating data relevant to each code; (3) searching for themes—collating codes into potential themes, gathering all data relevant to each potential theme; (4) reviewing themes—checking if the themes work in relation to the coded extracts and the entire data set, generating a thematic “map” of the analysis; (5) defining and naming themes—generating clear definitions and names for each theme; (6) producing the report—final analysis of selected extracts.
Although the feasibility study is a component of step 6, the evaluation of this intervention program is not within the scope of the current paper; the feasibility study will be only briefly discussed in the Results and Discussion sections.
Theoretical approach
According to IM, it is important to use a theory and evidence to specify determinants and behavioral and environmental factors that are related to the health problem that the intervention intends to address. The present intervention used Peplau's Interpersonal Theory of Nursing (ITN) (15) as the conceptual model, and we selected some methods associated with other theories to achieve certain intervention outcomes based on empirical findings. The ITN is a middle-range theory used for nursing in psychotherapeutic intervention, and we used some concepts from that theory as determinants of anxiety, such as knowledge, triggers, relief behaviors, self-efficacy and relations.
Results
Intervention development
Step 1: Needs assessment
The priority population is adult male cocaine users (age > 18 years) with anxiety who are residents in Brazil and undergoing treatment in specialized outpatient health facilities. We are focusing on male cocaine users due to the higher prevalence of crack use by adults, especially among young males (26–30), and because we understand that there are differences between the sexes in brain chemistry, physiology and the way that they tend to deal with stress and anxiety (1). In Brazil, cocaine users have been identified as a major health and social problem owing to the increase in users presenting at health facilities and the increase in illegal activities affecting urban security (30).
Based on the theoretical explanation provided by Peplau's theory (15), cocaine use is a kind of relief behavior used to decrease anxiety, and it can be transformed into a pattern of behavior that changes the self-system. Therefore, to treat cocaine users, it is necessary to treat the anxiety felt by cocaine users, because it is this anxiety that led to the initiation of cocaine use and that plays an important role in relapse, and to keep patients in treatment.
We developed a logic model of the problem to connect all behavioral and environmental factors that play an important role in anxiety, including its determinants and its consequences on quality of life (Figure 1).
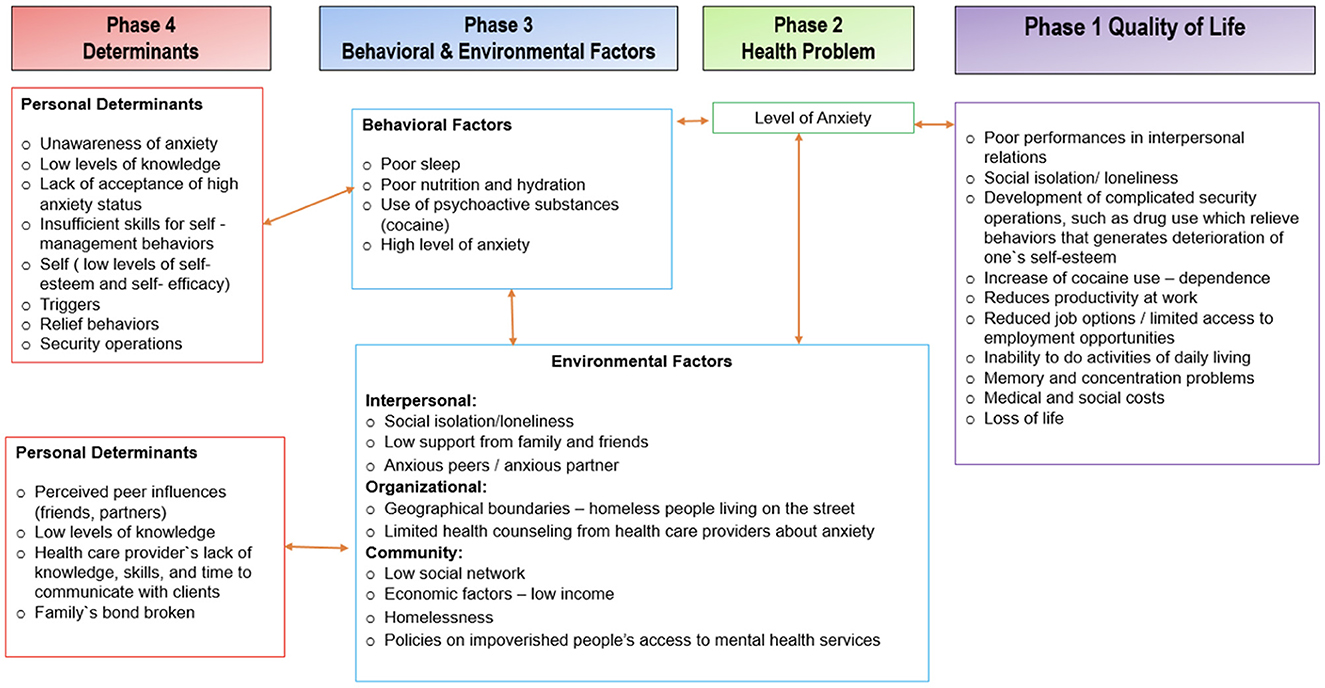
Figure 1. Logic model of problem.
Step 2: Creation of matrices of performance objectives
To achieve the first step of step 2, we worked from the needs assessment and an integrated theoretical framework to specify behaviors and environmental conditions that the program would promote using the logic model of the problem (Figure 1) as a guide to develop desired behavioral and environmental outcomes and then create performance objectives for each behavioral and environmental outcome (Figure 2).
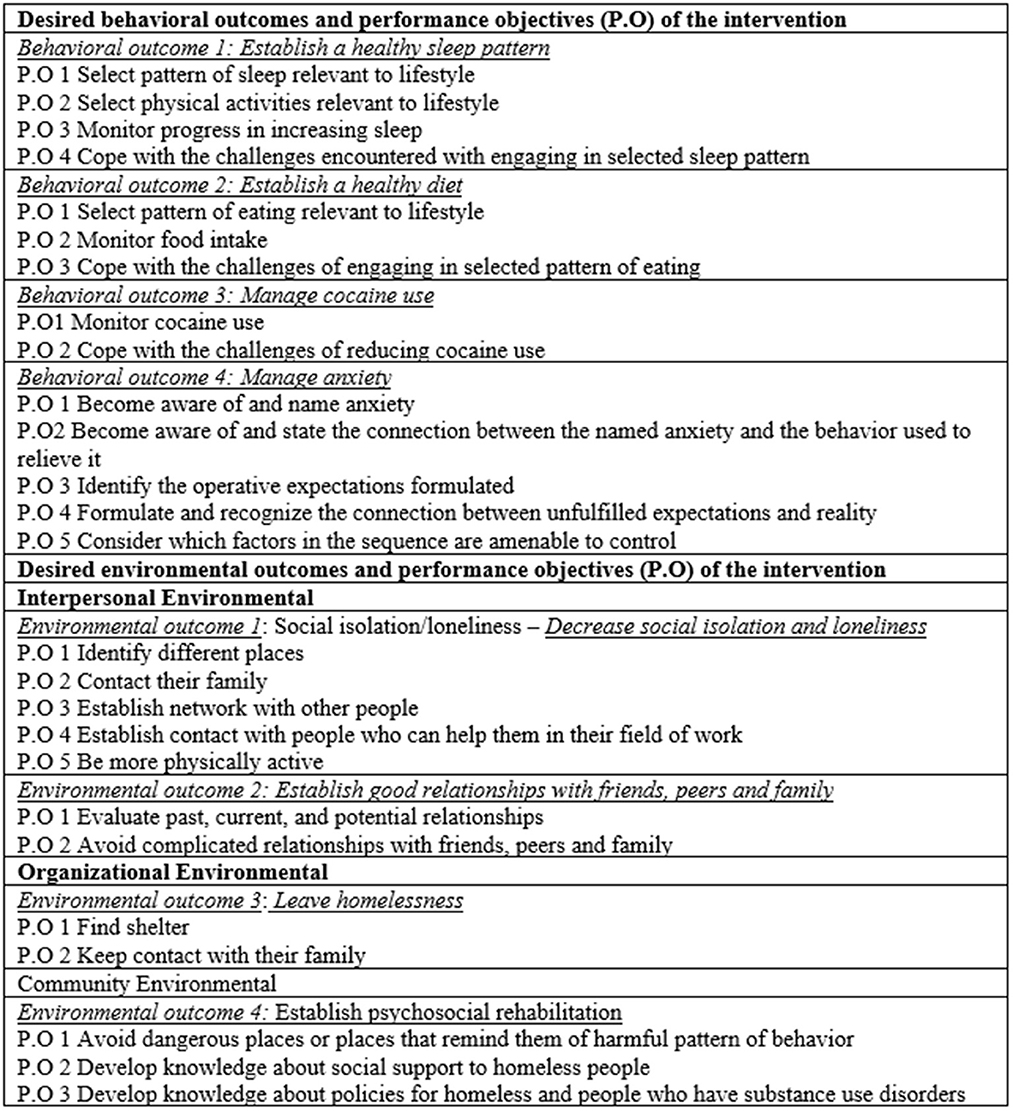
Figure 2. Expected outcomes for behavioral and environmental outcomes.
The determinants (knowledge, triggers, relief behaviors, self-efficacy, and relations) were developed by adapting Peplau's concepts from a behavioral and environmental perspective (31). The first step of this adaptation was to choose some of Peplau's concepts that are related to anxiety and substance abusers to develop relational propositions among them.
Finally, we integrated the behavioral and environmental outcomes with performance objectives and determinants. The first thing that we developed was the logic model of change (Figure 3), and through this model, we constructed the matrices of change objectives based on each behavioral and environmental outcome (Table 1). For example, the behavioral outcome “establish a healthy sleep pattern” has four determinants (knowledge, triggers, relief behaviors, and self-efficacy), and for each determinant, we wrote a performance outcome (specific outcome) that would be expected to occur as a result of the intervention.
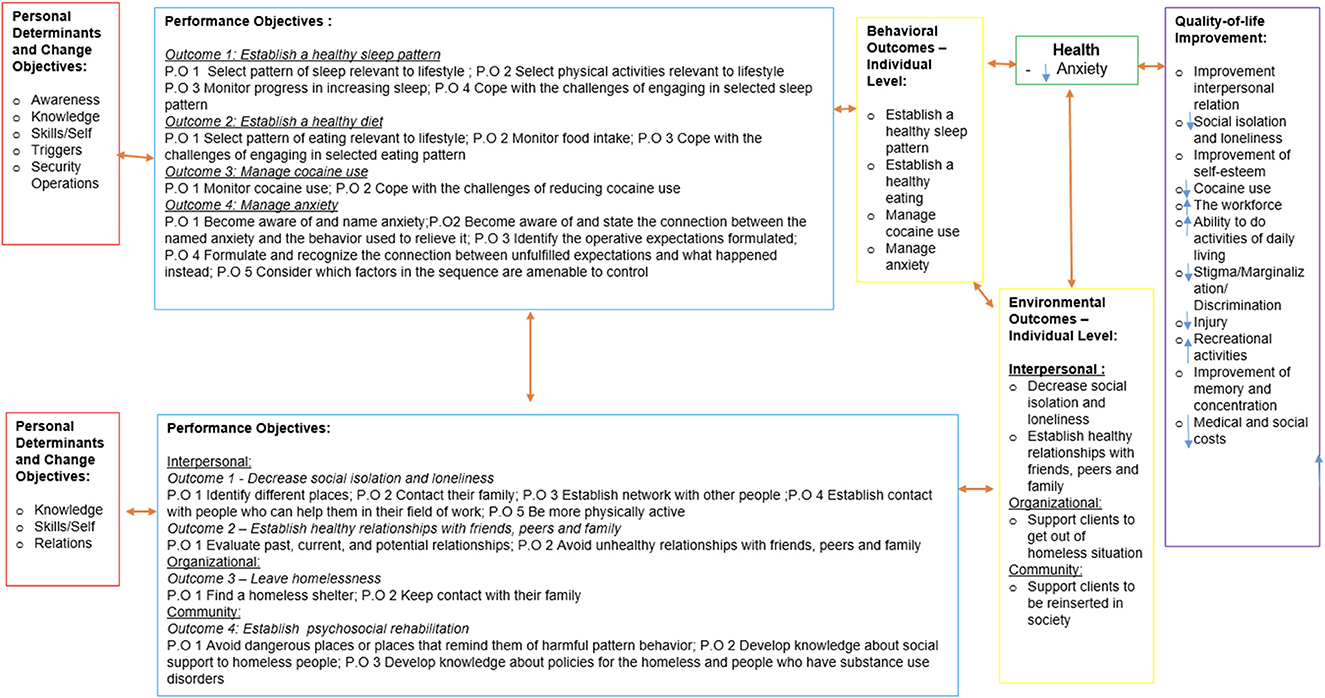
Figure 3. Logic model of change.
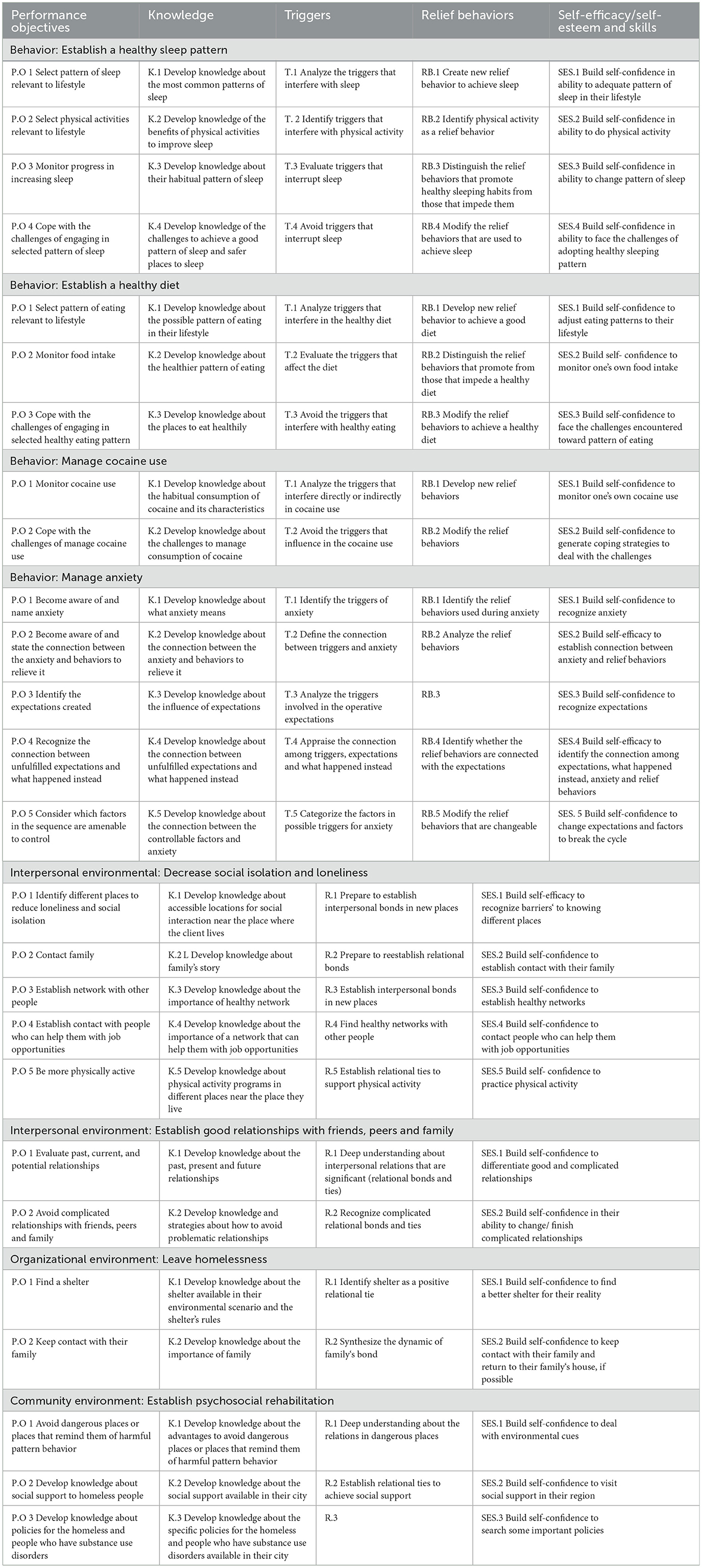
Table 1. Matrices construction of change objectives.
Step 3: Selection of theory-based methods and practical strategies
The first task was to organize all the change objectives created in step 2 (Table 1) together with the performance objectives, according to the determinants which they were associated. The second task was to match change objectives with specific determinants and methods selected. In the third task, the team started to propose applications, that is, strategies to operationalize the delivery of these methods, for each change objective (Supplementary File 1, Step 3).
Step 4: Program development—ITASUD
The selected theories that we used to develop the intervention were behavioral cognitive theory (BCT) (32), Peplau's theory (15), social cognitive theory (33), the trans-theoretical model (34), goal-setting theory (35), theories of information processing, the precaution adoption process model (36), self-affirmation theory (37), theories of automatic, impulsive and habitual behavior (38), attribution theory and relapse prevention theory (39), theories of goal-directed behavior (40), theories of social networks and social support (41), and theories of self-regulation (42). Consensus regarding the theories, methods, and applications was built for final agreement based on the adaptations needed for the intervention prototype structure to provide and equip cocaine users with the tools to manage anxiety in specialized outpatient health facilities.
The program ITASUD (Interpersonal Theory of nursing to Anxiety management in people with Substance Use Disorders) was designed for individual sessions (nurse-client) based on the phases of interpersonal relations proposed by Peplau (orientation, work and resolution) during five consecutive sessions delivered by a trained nurse using Peplau's concepts of interpersonal relationships. The first session would last 30 min, and the subsequent sessions would last 20 min. We chose this duration of time because in Brazil, according to public health minister (43), nurses need to attend three clients in a period of 60 min. However, the first session is scheduled for longer than the others because this session consists of two phases of interpersonal relationships (orientation and work).
The prototype of the intervention manual was guided by the matrices and the ideas about the methods and strategies that make possible the construction of specific messages and the overall content of each program component. During the intervention manual phase, we used the matrices developed during phase 3 and included the structure of each appointment; that is, we thought about the order of the target behavioral and environmental outcomes and the time and material used. All material used, such as notebooks, guidelines, and images, was designed to be appropriate for individuals with low literacy skills and was produced in English and Portuguese.
Step 5: Adoption and implementation of ITASUD
The outcomes of the program were divided into behavioral—to establish a healthy sleep pattern, to establish healthy eating, to manage anxiety, and to manage cocaine use—and environmental outcomes—to decrease social isolation, to have healthy relationships, to get out of homeless situations, and to be reinserted into society. However, these behavioral and environmental outcomes were developed at the individual level. During the outcome development, the reality of the population (homeless people and cocaine/crack users) and how this reality could affect the program were considered. The authors structured the intervention sessions as self-contained due to the potential high rate of dropout. We thought that in this specific population, the client could come to the first session and may not return for the other sessions, and therefore, the minimal dose will be one appointment and the maximum dose will be five appointments.
Step 6: ITASUD evaluation
To evaluate the intervention manual, we conducted a focus group with nurses who worked in a health facility to deeply understand their conceptions about the intervention plan to equip cocaine users to manage anxiety through specific questions that addressed each operational definition of feasibility through a guideline to conduct the focus group (Supplementary File 2).
The focus group was composed of seven nurses who worked in a specialized outpatient health facility in São Paulo. The nurses who participated were composed by four women (57.14%) and three man (42.85%); the majority were married (n = 5; 71.42%), white (n = 6; 85.71%), and to practice a religion (n = 5; 71.42%). We used thematic analysis to investigate the themes (25). Twelve themes related to feasibility adaptation were generated (n = 5; different world, environmental factor as the most important, relation between behavior and environmental factors, food, and specialized outpatient health facilities' focus on the anxiety), demand (n = 3; intoxication level, exclusion criteria, and clients who use crack/cocaine), acceptability (n = 1; answering the scale), and practicability (n = 3; worries about applying the intervention, placing the appointment, and adequate time in the work day).
The most frequent theme was related to adaptation of the intervention to the specificity of the particular population being studied (homeless, illiterate, vulnerable) and the factors that could influence the acceptance of the intervention to decrease the rate of treatment withdrawal. The nurses' opinions were mixed about the scale application in the first and last appointments, mainly because of the large number of scales; some nurses said that once the patient accepted participation in the intervention, they would answer the scales regardless of the number, but other nurses said that the intervention involves too many scales to ask a patient who presents with a high level of anxiety to answer. All nurses considered it important to change the order in which the environmental and behavioral factors that affect anxiety were addressed approached. They suggested approaching environmental situations first and then the behavioral factors, and they suggested taking out two of the identified behavioral factors, sleeping and eating patterns, because of the homeless situation of the participants in the intervention.
In relation to practicability, they raised issues such as the times for the appointment and the complexity of the intervention manual; in particular, all nurses agreed that 20 min to address all the issues related to anxiety in each appointment could be insufficient. The main theme related to demand was intoxication status because the health facility is an outpatient facility, and it is difficult for patients to remain abstinent, mainly at the onset of treatment. After the focus group, the team altered the intervention manual to improve the intervention feasibility for this particular health care facility scenario.
We described above some data from feasibility studies related to the development of the intervention, mainly the intervention manual, to achieve step six. The participants' recruitment process of the feasibility trial was by convenience sampling, totalizing 39 participants in the feasibility trial, what is considered enough for a feasibility study (44). The data was analyzed by the use of the linear mixed effects model to assess the changes in the level of anxiety after the intervention. The feasibility trial indicated that ITASUD appears to be feasible and support the design of a powered larger trial to evaluate the effectiveness of the ITASUD (45).
Discussion
This study describes the development of an intervention to equip cocaine users with strategies to manage anxiety through the IM approach. There is limited literature about the phases of the development of complex interventions, mainly in this theme that includes comorbidities (anxiety and cocaine use). One of the explanations for this sparse literature is that the development of complex interventions is a considerable challenge for researchers, mainly because it is very difficult to identify all the factors that play an important role in the health problem of interest and to present all the steps of a new intervention in such a way that the readers can understand the entire process undertaken to develop the intervention protocol.
IM is based on the creation of matrices to show all the steps in the development of the intervention. The process of creating these matrices is very time consuming but helps the authors of all components during the brainstorming to see the relationships between the determinants, change objectives, performance objectives, and behavioral and environmental outcomes that affect the health problem being studied. In addition, this methodological process assists in the development of the theoretical framework of the intervention, which is necessary for the identification of mediators and moderators of the intervention that will play an important role in the success and failure of any particular intervention.
The needs assessment produced during this study was fundamental to identify the barriers to accessing cocaine users and services based on the logic related to this population of outpatients, such as high rates of dropping out, undocumented status, and environmental factors that directly affect the level of anxiety. IM is a powerful methodological tool that facilitates the comprehensive examination of these environmental factors using an ecological perspective instead of acting only on behavioral factors. We followed all the steps of IM using a mix of quantitative and qualitative methods to achieve a more comprehensive intervention manual that incorporates resources that affect the majority of the identified barriers to accomplish the desired outcomes of the intervention.
The overall structure of the program was adapted to the particular patient population based on the stakeholders' experiences. The structure of the intervention was adapted such that environmental factors are addressed in the 4th appointment rather than the 5th appointment, and this change was taken to enhance clients' acceptability: as demonstrated in the focus group, all nurses said that the environmental factors were the factors that the clients liked to talk about, which would affect each individual's level of anxiety. Additionally, we removed two behavioral factors, sleeping and eating, that we identified as important factors in increasing anxiety, but during the focus group, all nurses identified these factors as difficult topics to broach with the clients, as the majority of them were homeless. The intervention will be applied over five consecutive days, 20 min for each appointment, while taking into consideration the high dropout rates of these clients in the outpatient service.
Conclusion
This study will provide valuable guidance for future researchers, health agencies, and health care professionals who are interested in reproducing this systematic approach to developing a complex intervention, once there is limited literature about the phases of the development of complex interventions. The program has already been implemented in the feasibility study, and demonstrate to be feasible. Additionally, ITASUD can be generalizable to other settings around the world into daily care programs.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was obtained from the Institutional Review Board of the School of Nursing, University of São Paulo (CAEE number: 86848418.4.0000.5392) and the Municipal Health Secretary of São Paulo (CAEE number: 86848418.4.3001.0086). The patients/participants provided their written informed consent to participate in this study.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1124295/full#supplementary-material
References
1. Remes O, Brayne C, Van der Linde R, Lafortune L. A systematic review of reviews on the prevalence of anxiety disorders in adult populations. Brain Behav. (2016) 6:e00497. doi: 10.1002/brb3.497
2. Fatseas M, Serre F, Swendsen J, Auriacombe M. Effects of anxiety and mood disorders on craving and substance use among patients with substance use disorder: an ecological momentary assessment study. Drug Alcohol Depend. (2018) 187:242–8. doi: 10.1016/j.drugalcdep.2018.03.008
3. World Health Organization. Depression and Other Common Mental Disorders Global Health Estimates. Geneva (2017).
4. Welsh JW, Knight JR, Hou SSY, Malowney M, Schram P, Sherritt L, et al. Association between substance use diagnoses and psychiatric disorders in an adolescent and young adult clinic-based population. J Adolesc Health. (2017) 60:648–52. doi: 10.1016/j.jadohealth.2016.12.018
5. Hosseini S, Oremus M. The effect of age of initiation of cannabis use on psychosis, depression, and anxiety among youth under 25 years. Can J Psychiatry. (2019) 64:304–12. doi: 10.1177/0706743718809339
6. Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. (2016) 388:1545–602. doi: 10.1016/S0140-6736(16)31678-6
7. World Drug Report. United Nations Publication. (2020). Available online at: https://wdr.unodc.org/wdr2020 (accessed September 10, 2020).
8. Abdalla RR, Madruga CS, Ribeiro M, Pinsky I, Caetano R, Laranjeira R. Prevalence of cocaine use in Brazil: data from the II Brazilian national alcohol and drugs survey (BNADS). Addict Behav. (2014) 39:297–301. doi: 10.1016/j.addbeh.2013.10.019
9. Global Drug Survey,. The Global Drug Survey 2015 Findings. (2015). Available online at: https://www.globaldrugsurvey.com/the-global-drug-survey-2015-findings (accessed September 10, 2020).
10. Chambers DA, Azrin ST. Partnership: a fundamental component of dissemination and implementation research. Psychiatr Serv. (2013) 64:509–11. doi: 10.1176/appi.ps.201300032
11. Powell BJ, Beidas RS, Lewis CC, Aarons GA, McMillen JC, Proctor EK, et al. Methods to improve the selection and tailoring of implementation strategies. J Behav Health Serv Res. (2015) 44:177–94. doi: 10.1007/s11414-015-9475-6
12. Colquhoun HL, Squires JE, Kolehmainen N, Grimshaw JM. Methods for designing interventions to change healthcare professionals' behaviour: a systematic review. Implement Sci. (2017) 12:1–11. doi: 10.1186/s13012-017-0560-5
13. Bosch M, van der Weijden T, Wensing M, Grol R. Tailoring quality improvement interventions to identified barriers: a multiple case analysis. J Eval Clin Pract. (2007) 13:161–8. doi: 10.1111/j.1365-2753.2006.00660.x
14. Baker R, Comosso-Stefinovic J, Gillies C, Shaw EJ, Cheater F, Flottorp S, et al. Tailored interventions to address determinants of practice. Cochrane Database Syst Rev. (2015) 4:1–118. doi: 10.1002/14651858.CD005470.pub3
15. Peplau HE. Interpersonal Relations in Nursing : A Conceptual Frame of Reference for Psychodynamic Nursing. New York, NY: Springer (1991).
16. Eldredge LKB, Markham CM, Ruiter RA, Fernández ME, Kok G, Parcel GS. Planning Health Promotion Programs: An Intervention Mapping Approach. California: John Wiley & Sons (2016).
17. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. (2008) 337:1655. doi: 10.1136/bmj.a1655
18. Bartholomew LK, Parcel GS, Kok G. Intervention mapping: a process for developing theory and evidence-based health education programs. Health Educ Behav. (1998) 25:545–63. doi: 10.1177/109019819802500502
19. Van Empelen P, Kok G, Schaalma HP, Bartholomew LK. An AIDS risk reduction program for dutch drug users: an intervention mapping approach to planning. Health Promot Pract. (2003) 4:402–12. doi: 10.1177/1524839903255421
20. Fernández ME, Gonzales A, Tortolero-Luna G, Partida S, Bartholomew LK. Using intervention mapping to develop a breast and cervical cancer screening program for hispanic farmworkers: cultivando la salud. Health Promot Pract. (2005) 6:394–404. doi: 10.1177/1524839905278810
21. Munir F, Kalawsky K, Wallis DJ, Donaldson-Feilder E. Using intervention mapping to develop a work-related guidance tool for those affected by cancer. BMC Public Health. (2013) 13:6. doi: 10.1186/1471-2458-13-6
22. Hurley DA, Murphy LC, Hayes D, Hall AM, Toomey E, McDonough SM, et al. Using intervention mapping to develop a theory-driven, group-based complex intervention to support self-management of osteoarthritis and low back pain (SOLAS). Implement Sci. (2015) 11:56. doi: 10.1186/s13012-016-0418-2
23. Powell BJ, Haley AD, Patel SV, Amaya-Jackson L, Glienke B, Blythe M, et al. Improving the implementation and sustainment of evidence-based practices in community mental health organizations: a study protocol for a matched-pair cluster randomized pilot study of the Collaborative Organizational Approach to Selecting and Tailoring Implementation Strategies (COAST-IS). Implement Sci Commun. (2020) 1:1–13. doi: 10.1186/s43058-020-00009-5
24. Eldridge SM, Lancaster GA, Campbell MJ, Thabane L, Hopewell S, Coleman CL, et al. Defining feasibility and pilot studies in preparation for randomised controlled trials: development of a conceptual framework. PLoS ONE. (2016) 11:e0150205. doi: 10.1371/journal.pone.0150205
25. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
26. Zeferino MT, Fermo VC, Fialho MB, Bastos FI. Similarities and differences in crack cocaine use patterns in Santa Catarina, Brazil: Capital vs. Midwest. Cienc Saude Coletiva. (2017) 22:97–106. doi: 10.1590/1413-81232017221.18342016
27. Garcia EL, Zacharias DG, Sontag J. (Re)Conhecendo o perfil do usuário de crack de Santa Cruz do Sul. Barbarói. (2012) 36:83–95.
28. Zeferino MT, Fermo VC, Fialho MB, Kenthi A, Bastos FI. Crack cocaine use scene in the capital of the state of Santa Catarina/Brazil: the (in) visibility of users. Texto Contexto Enfermagem. (2019) 28. doi: 10.1590/1980-265x-tce-2017-0460
29. Vernaglia TVC, Vieira RADMS, Cruz MS. Crack cocaine users living on the streets–gender characteristics. Cien Saude Colet. (2015) 20:1851–9. doi: 10.1590/1413-81232015206.11562014
30. Toledo L, Cano I, Bastos L, Bertoni N, Bastos FI. Criminal justice involvement of crack cocaine users in the city of Rio de Janeiro and Greater Metropolitan Area: implications for public health and the public security agenda. Int J Drug Policy. (2017) 49:65–72. doi: 10.1016/j.drugpo.2017.07.034
31. Beeber LS, Canuso R, Emory S. Instrumental inputs: moving the interpersonal theory of nursing into practice. ANS Adv Nurs Sci. (2004) 27:275–86. doi: 10.1097/00012272-200410000-00004
32. Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. (2013) 46:81–95. doi: 10.1007/s12160-013-9486-6
33. Bandura A. Social cognitive theory: an agentic perspective. Asian J Soc Psychol. (2002) 52:1–26. doi: 10.1016/B0-08-043076-7/01340-1
34. Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. Am J Health Promot. (1997) 12:38–48. doi: 10.4278/0890-1171-12.1.38
35. Latham GP, Locke EA. Goal setting research. Eur Psychol. (2007) 12:290–300. doi: 10.1027/1016-9040.12.4.290
36. Glanz K, Rimer BK, Viswanath K. Health Behavior and Health Education. California: Jossey-Bass (2008).
37. Sherman DK. Self-affirmation: understanding the effects. Soc Personal Psychol Compass. (2013) 7:834–45. doi: 10.1111/spc3.12072
38. Wood W, Neal DT. A new look at habits and the habit-goal interface. Psychol Rev. (2007) 114:843. doi: 10.1037/0033-295X.114.4.843
39. Marlatt GA, Donovan DM. Relapse Prevention: Maintenance Strategies in the Treatment of Addictive Behaviors. New York, NY: Guilford Press (2005).
40. Hofmann W, Friese M, Wiers RW. Impulsive versus reflective influences on health behavior: a theoretical framework and empirical review. Health Psychol Rev. (2008) 2:111–37. doi: 10.1080/17437190802617668
41. Glanz K, Rimer BK, Viswanath K. Health Behavior: Theory, Research, and Practice. California: John Wiley & Sons (2015).
42. Creer TL. Self-management of chronic illness. In: Handbook of Self-regulation. California: Academic Press (2000).
43. Brasil and Ministério da Saúde. Portaria n° 1101/GM, de 12 de junho de 2002. Brasilia: Diário Oficial da União (2002).
44. Mailhot T, Goulet MH, Maheu-Cadotte MA, Fontaine G, Lequin P, Lavoie, et al. Methodological reporting in feasibility studies: a descriptive review of the nursing intervention research literature. J Res Nurs. (2020). 25:460–72. doi: 10.1177/1744987119883404
Keywords: intervention mapping, anxiety, Peplau's theory, substance use disorders, evidence-based interventions, anxiety management
Citation: Pereira CF, Vargas Dd and Beeber LS (2023) An anxiety management intervention for people with substance use disorders (ITASUD): An intervention mapping approach based on Peplau's theory. Front. Public Health 11:1124295. doi: 10.3389/fpubh.2023.1124295
Received: 15 December 2022; Accepted: 30 January 2023;
Published: 21 February 2023.
Edited by:
Jaya Kumar, National University of Malaysia, MalaysiaReviewed by:
Mohd Azizuddin Amir Shariffuddin, Clinical Research Centre Hospital Kuala Lumpur (CRC HKL), MalaysiaRashidi Mohamed, National University of Malaysia, Malaysia
Copyright © 2023 Pereira, Vargas and Beeber. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Caroline Figueira Pereira,  cGVyZWlyYWNmQHVzcC5icg==
cGVyZWlyYWNmQHVzcC5icg==