
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 27 March 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1108465
 Ishita Gupta1*
Ishita Gupta1* Shivani A. Patel2,3,4Dimple Kondal1Michael Goodman4
Shivani A. Patel2,3,4Dimple Kondal1Michael Goodman4 Sailesh Mohan1,5,6Mohammed K. Ali2,3,4,7Nikhil Tandon8K. M. Venkat Narayan3,4†Dorairaj Prabhakaran1,4,5,9Krithiga Shridhar1,5
Sailesh Mohan1,5,6Mohammed K. Ali2,3,4,7Nikhil Tandon8K. M. Venkat Narayan3,4†Dorairaj Prabhakaran1,4,5,9Krithiga Shridhar1,5Background: Studies have highlighted a possible influence of gingival and periodontal disease (PD) on COVID-19 risk and severity. However, the evidence is based on hospital-based studies and community-level data are sparse.
Objectives: We described the epidemiological pattern of SARS-CoV-2 infection in Delhi and evaluated the associations of gingival and PD with incident COVID-19 disease in a regionally representative urban Indian population.
Methods: In a prospective study nested within the Centre for Cardiometabolic Risk Reduction in South-Asia (CARRS) study, participants with clinical gingival and periodontal status available at baseline (2014–16) (n = 1,727) were approached between October 2021 to March 2022. Information on COVID-19 incidence, testing, management, severity was collected as per the WHO case criteria along with COVID-19 vaccination status. Absolute incidence of COVID-19 disease was computed by age, sex, and oral health. Differences in rates were tested using log-rank test. Poisson regression models were used to evaluate independent associations between gingival and PD and incidence of COVID-19, adjusted for socio-demographic and behavioral factors, presence of comorbidity, and medication use.
Results: Among 1,727 participants, the mean age was 44.0 years, 45.7% were men, 84.5% participants had baseline gingival or PD and 89.4% participants had received at least one dose of COVID-19 vaccine. Overall, 35% (n = 606) participants were tested for COVID-19 and 24% (n = 146/606) tested positive. As per the WHO criteria total number of cases was 210, constituting 12% of the total population. The age and sex-specific rates of COVID-19 were higher among men and older participants, but women aged >60 years had higher rates than men of same age. The incidence rate did not differ significantly between those having gingival or PD and healthy periodontium (19.1 vs. 16.5/1,000 person-years) and there was no difference in risk of COVID-19 by baseline oral disease status.
Conclusion: Gingival and PD were not associated with increased risk of COVID-19.
COVID-19 disease caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-COV-2) has accounted for over 598 million cases and more than 6 million deaths across the world since first reported in 2020 (1). With more than 44 million test-confirmed cases and over five hundred thousand deaths, India is among the most affected countries worldwide (2). While most infected people have mild symptoms and recover at home, over 15% require specialized treatment such as hospitalization, intensive care, and oxygen supplementation due to severity, acute respiratory distress syndrome, and other conditions (3). Several factors influence the disease progression, which include but are not restricted to old age and comorbid conditions such as obesity, hypertension, diabetes, cardiovascular diseases (4–11).
An understudied dimension of COVID-19 risk is oral health. Studies have highlighted shared risk factors between oral and chronic diseases and COVID-19 infection and thus a possible influence of poor oral hygiene, gingival, and periodontal diseases on the risk of COVID-19 infection (12, 13) and its severity (14–19). Gingival disease (GD), characterized by poor oral hygiene and plaque biofilm harboring oral microbial pathogens deposited on dental and tissue surfaces of the oral cavity, clinically manifests as episodes of acute inflammatory changes and bleeding from gums that may be transient or persistent in nature (20). Periodontal disease (PD) is a complex, multicausal chronic inflammatory disorder leading to the destruction of soft tissues and bone surrounding the teeth (21). According to the Global Burden of Disease Study, severe PD is the 11th most prevalent condition worldwide (affecting ~10.8% people) (22–24), with prevalence ranging between 30–90% in India (25).
Cross-sectional (12, 14, 16–19) and prospective (13, 15) observational studies report, over three-fold increase in severity of COVID-19 infection (and death) among persons with poor oral health or PD. However, they are limited by either sample size, lack of community level prospective data, or clinically ascertained oral health status. Therefore, we prospectively followed a regionally representative community-based population in New Delhi, a geographic region that experienced one of the highest incidence and severity of COVID-19 both in India and globally (1, 26). We utilized baseline clinical information on gingival and periodontal health to evaluate its association with incident COVID-19 and its severity.
This was a prospective observational analysis of the Centre for Cardiometabolic Risk Reduction in South-Asia (CARRS) study. CARRS is a community-based longitudinal health assessment of 30,000 adult participants in New Delhi and Chennai, India and in Karachi, Pakistan across two urban representative cohorts initiated in 2010 and 2014, respectively (27, 28). Annual follow-ups comprise of a comprehensive questionnaire along with physical measurements and 8-h fasting blood sample collection at alternate follow-ups from men and non-pregnant women aged ≥ 20 years residing in the study areas.
From the 4,725 CARRS cohort-2 members in New Delhi, a random sub-set of 2,045 participants were enrolled in the Oral Health Study (OHS) between October 2014 and December 2016 (N = 2,045). They responded to the World Health Organization’s (WHO) Oral Health Assessment questionnaire and underwent detailed clinical oral examination (29). The field interviewers followed-up the OHS participants between October 2021 to March 2022 to complete telephone interviews and collect information on the history of COVID-19 and its severity. Except for those who refused, each participant was contacted five times over telephone at different times and days of the week. Participants who did not respond to phone calls were contacted by the study team through household visits to confirm loss to follow-up. Interviews were conducted by trained research staff who were blinded to the exposure status of participants.
• Participants of the CARRS cohort residing in New Delhi
• Men and women (≥20 y) with baseline information on oral health status
• Participants who agreed to participate in the follow-up study with informed consent.
• Men and women (≥20 y) without baseline information on oral health status
• Participants who refused to participate in the follow-up study.
• Participants who were not contacted after multiple attempts over both phone (five times) and household visit (twice) during the study.
The study was conducted according to the Declaration of Helsinki and was approved by Institutional Ethics Committee of the Centre for Chronic Disease Control, New Delhi (CCDC-IEC_13_2021). Informed consent was obtained from all participants before administering the questionnaire.
Gingival and periodontal health status was ascertained at baseline by qualified and trained dentists who attended calibration workshops for assessment and interpretation of oral indices. The details are published elsewhere (29, 30) with an overview presented in Table 1.

Table 1. Exposure and outcome assessment.
Outcome assessment (Table 1) was done as per the WHO COVID-19 case criteria (3, 31) based on self-reported COVID-19 history and severity. COVID-19 deaths were ascertained through verbal autopsy with next of kin (28). Participants were also asked about COVID-19 testing, care received, and vaccination status (with number of doses).
Data on participant demographic characteristics (age, sex, monthly household income, education, and employment status), lifestyle factors (ever use of tobacco/alcohol, vigorous to moderate physical activity at work or leisure, type of diet), comorbidities (diabetes, hypertension, hyperlipidaemia, overweight/obesity, cancer, kidney disease, heart diseases, stroke), and medication history for chronic diseases were collected using interviewer-administered questionnaires. Plasma fasting blood glucose (Hexokinase), systolic and diastolic blood pressure (automated Omron HEM-7080) and anthropometric measurements (Tanita BC-418, Seca-213 Portable Stadiometer) were also available (28, 29).
Baseline characteristics of the study participants were summarized by calculating percentages for categorical data and means and standard deviations (SD) for continuous variables. The differences in proportions and means between those reporting COVID-19 and those with no history of COVID-19 were compared using chi-square or t-test, respectively. Overall and stratum-specific (by age, sex, and exposure status) incidence rates of COVID-19 were calculated and differences in rates across groups was evaluated using log-rank test. Incidence rates (IR) with 95% confidence intervals (CI) were computed over the time from baseline to final available follow-up, censored for participants lost to follow-up. Person-years were estimated from the date of enrolment to the time of COVID-19 diagnosis or the last date of visit or death, whichever was documented earlier.
Multivariable Poisson regression models were used to evaluate independent associations between GD and PD and incidence of COVID-19 with results expressed as adjusted incidence rate ratios (IRR) and the corresponding 95% CI, comparing with those without GD or PD. The covariates of interest in these models included age in years (20–40/41–60/>60 age categories), sex (men/women), education status (up to secondary school/graduation and above), employment status (employed/unemployed), monthly household income in INR (≤30,000/>30,000), alcohol and tobacco consumption (yes/no), vigorous to moderate physical activity (yes/no), diet (vegetarian/non-vegetarian), presence of comorbidities mentioned above (yes/no), and any regular medication intake (yes/no). Robust standard error models were utilized to account for household clustering in our study population. The analysis was performed using STATA statistical package (StataCorp. 2011. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP).
Among 2,045 participants with information on baseline (2016–18) gingival and periodontal health status, 84.5% (N = 1,727) responded to the follow-up survey from October 2021 to March 2022 (Supplementary Figure S1) either by telephone (52.7%) or during a household visit (47.3%). Demographic characteristics of respondents and non-respondents were similar (Supplementary Table S1). However, a greater proportion of respondents had graduate or above level of education (27.3% vs. 18.6%) and comorbidities (89.7% vs. 85.5%) compared to non-respondents. Respondents were also less likely to be tobacco users (21.3% vs. 31.1%,) compared to non-respondents.
Table 2 summarizes the baseline characteristics of study participants (n = 1,727) included in the final analysis (mean (±SD) age in years: 44.0 (±12.8); 45.7% men). Less than a third (27.3%) had graduate or above level of education, 13.7% had no formal education and more than half (55.2%) were currently unemployed. A fifth of participants were tobacco and/or alcohol users with less than a half (48.1%) doing moderate to vigorous physical activity at work or leisure and half (50.2%) were vegetarian. Nearly 90% participants had at least one comorbidity at baseline and 89.4% participants had received at least one dose of COVID-19 vaccine at the time of survey. Of the 1,727 participants who responded, 896 (51.9%) had GD, 555 (32.1%) had PD, and 276 (16%) presented with apparently healthy gingiva and periodontium at baseline.
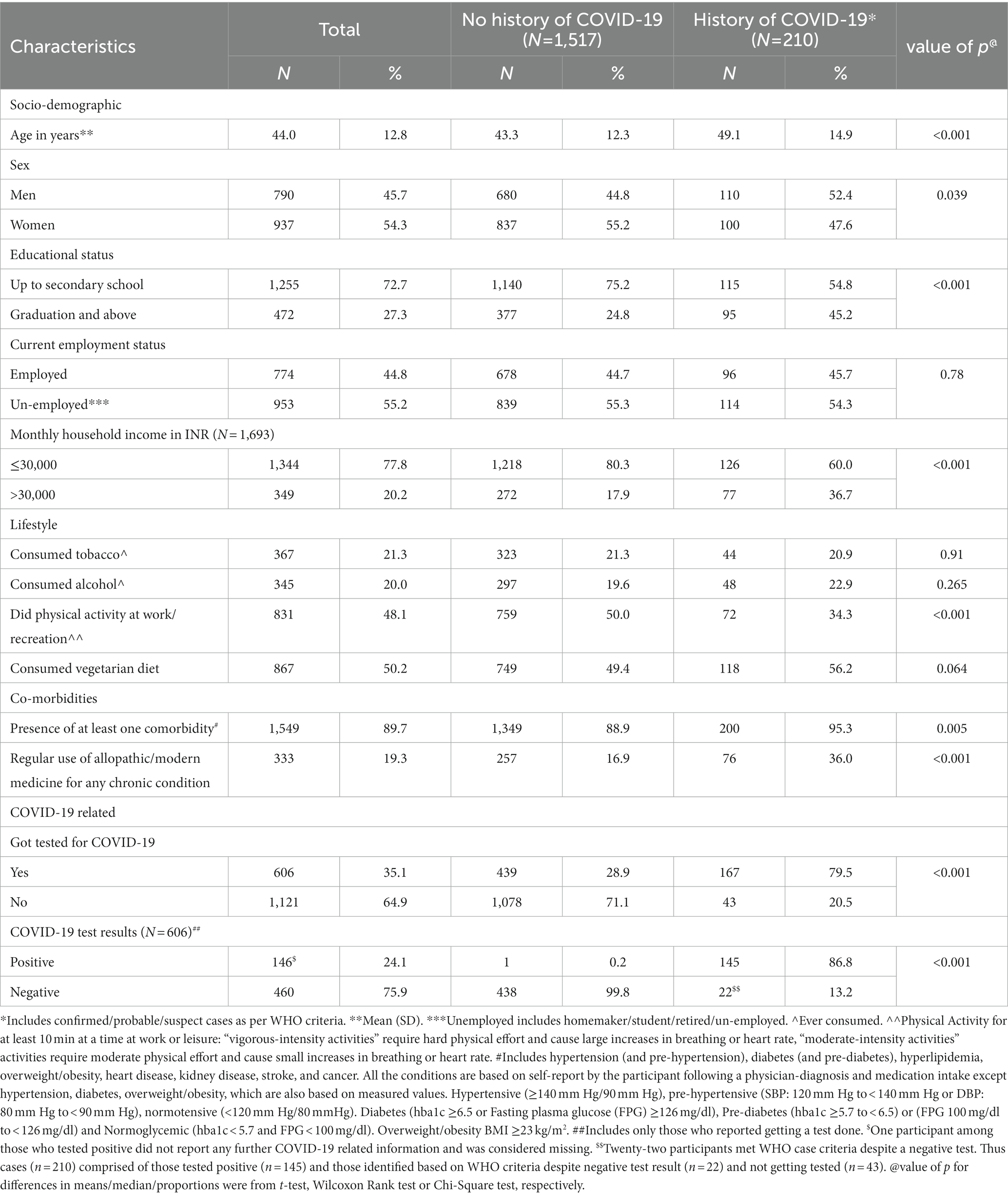
Table 2. Baseline characteristics (2016–2018) of study participants (N = 1,727) by history of COVID-19 at follow-up (2021–2022).
A total of 606 participants (35.1%) reported getting tested for COVID-19, and of those 146 (24.1%) tested positive (out of which one participant was considered missing due to missing other relevant COVID-19 information). We classified our study participants for COVID-19 as per the WHO case criteria (Table 1): 210 (12.2%) participants with COVID-19 included 169 (80.5%) confirmed cases, 33 (15.7%) suspected cases and 8 (3.8%) probable cases. Among COVID-19 cases, one episode (77.6%) and mild infection (82.9%) were common wherein about 70% experienced three or more symptoms and less than a 10% required additional support in terms of oxygen/assisted ventilation. Comparison of baseline characteristics (Table 2), by differences in means, revealed that participants with COVID-19 were older in age compared to those who did not have COVID-19 (mean (±SD) 49.1 (±14.9) vs. 43.3 (±12.3) years). By differences in proportion, men (52.4% vs. 47.6%) with lower education status (54.8% vs. 45.2%), household income (60% vs. 36.7%) and comorbidities (95.3% vs. 4.7%) were more likely to be cases compared to their counterparts.
The overall incidence rate of COVID-19 was 18.64/1,000 person-years (95% CI: 16.3–21.3/1,000 person-years) (Table 3). Men reported greater overall incidence rates compared to women (21.4; 95% CI: 17.8–25.9 vs. 16.3; 95% CI: 13.4–19.8/1,000 person-years, p: 0.034). The incidence rates increased significantly with age [20–40 years: 13.6 (95% CI: 10.7–17.2)], 41–60 years: 18.6 [95% CI: 15.1–22.8), >60 years: 38.1 (95% CI: 28.9–50.3)/1,000 person-years, p < 0.001]. A similar pattern was observed when incidence rates were estimated for confirmed cases only (N = 169). Men of age-group 20–40 years had higher incidence rates compared to women that narrowed in 40–60 years and disappeared in the >60 years group 38.4 [(95% CI: 24.8–59.5)/1,000 person-years in women vs. 37.9 (95% CI: 26.5–54.2)/1,000 person-years in men]. However, among confirmed cases, men reported higher incidence rates than women in the same age group throughout. Additionally, the incidence rates did not differ significantly between those having GD/PD and healthy periodontium [19.1 (95% CI:16.5–22.1) vs. 16.5 (95% CI:11.5–23.6)/1,000 person-years, p: 0.394)].
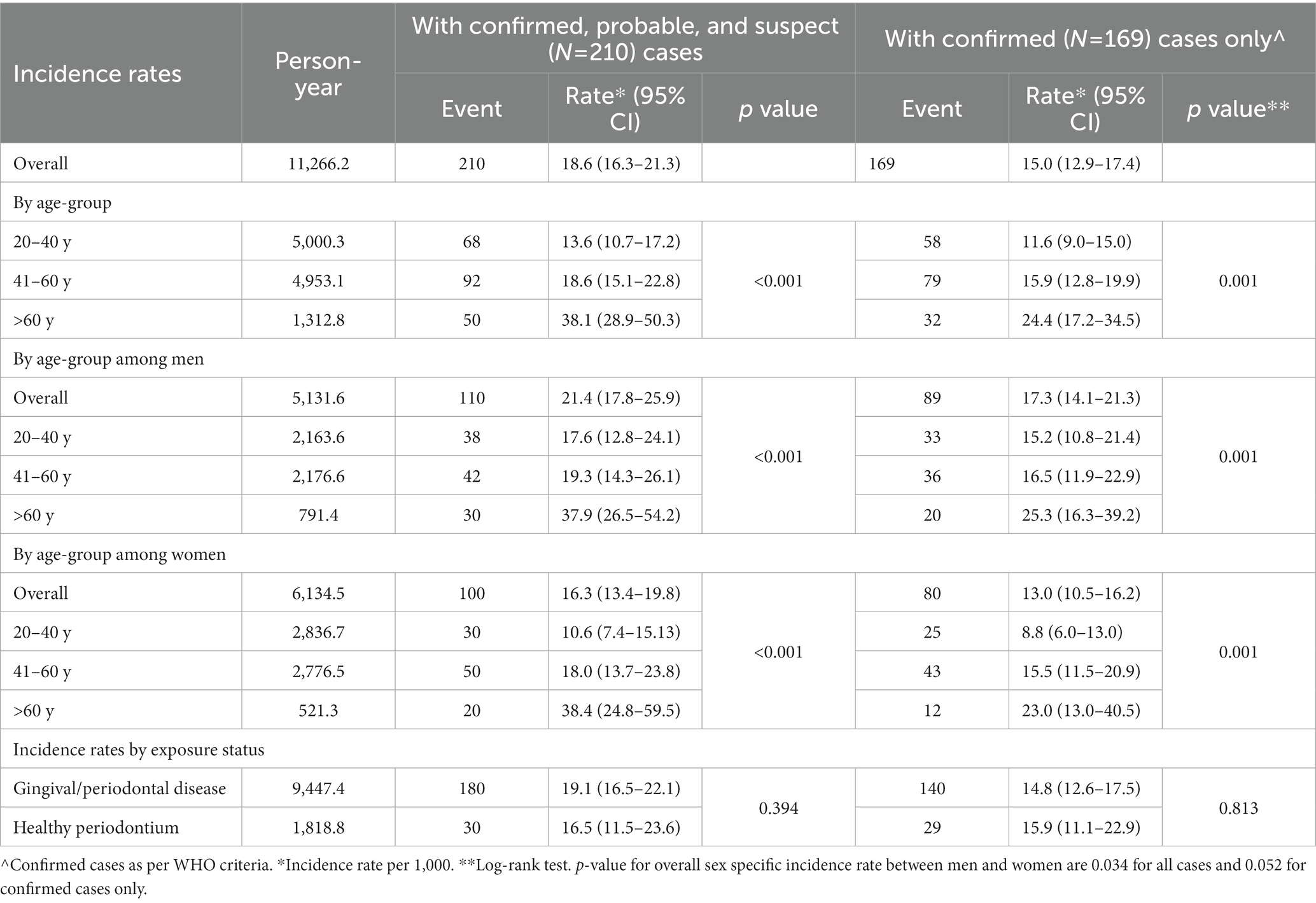
Table 3. COVID-19 incidence rates (per 1,000) by age, gender, and exposure status (N = 1,727).
Unadjusted and adjusted IRR (95% CI) for the association between baseline oral disease status of study participants and COVID-19 incidence is presented in Table 4. The crude IRR (95% CI) of risk of COVID-19 was 1.16 (95% CI: 0.80–1.67) among those with baseline oral disease compared to those without any oral disease. On adjusting for all known important confounders and/or competing exposures with inverse probability weighting, no association was found between baseline oral disease and incidence of COVID-19 among the study participants (IRR: 1.05, 95% CI: 0.72–1.52). The findings remained unchanged when analyzed for GD and PD separately or confirmed cases only. Due to small outcome numbers, we limited our explorations to bivariate differences in proportions of GD and PD with COVID-19 severity and did not find any significant difference (Supplementary Figure S2).
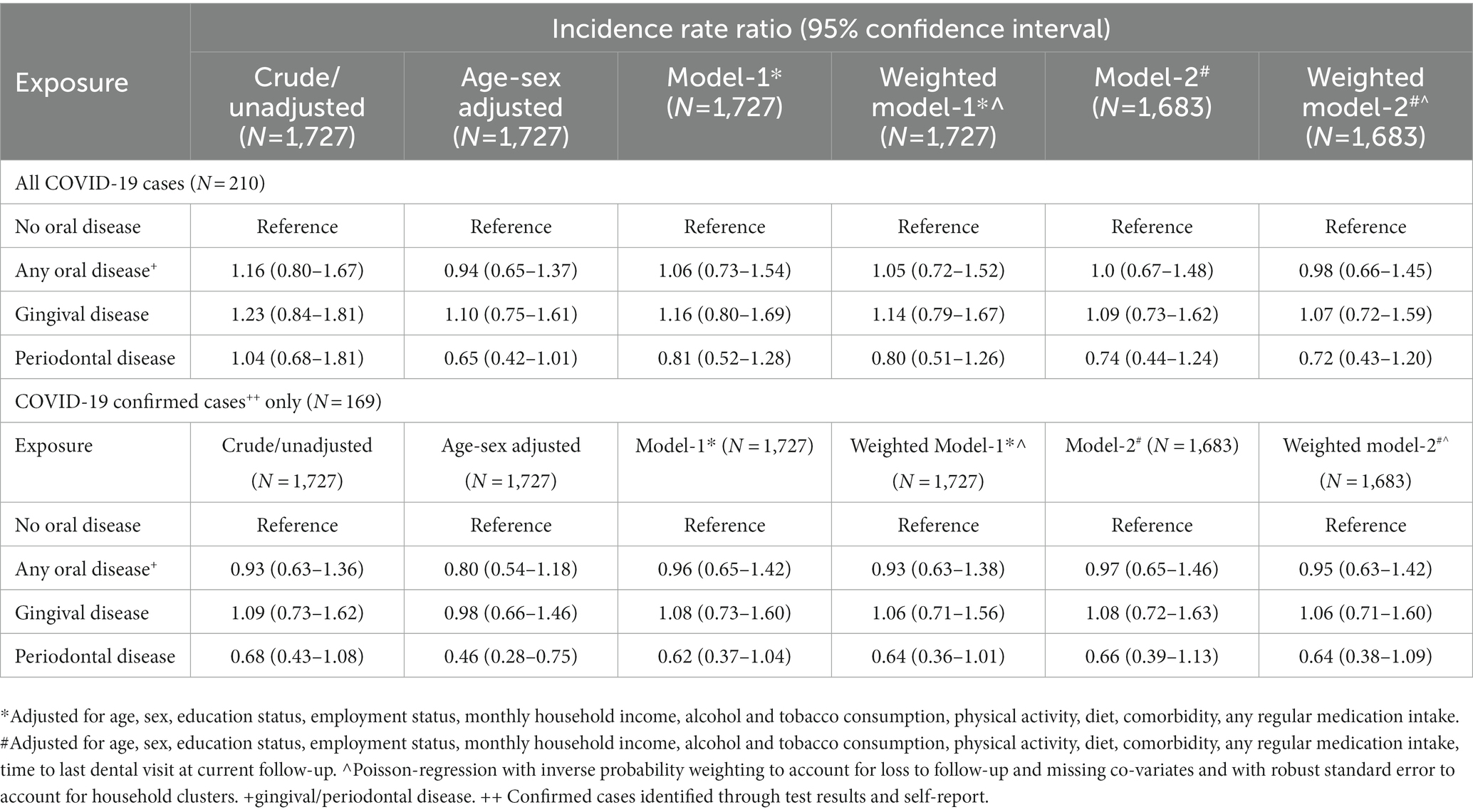
Table 4. Unadjusted and adjusted incidence rate ratio for the association of COVID-19 incidence with baseline oral disease of study participants aged ≥20 years.
In this study of a representative urban Indian population in New Delhi, diagnosed COVID-19 disease (as per WHO COVID-19 case criteria based on self-reported COVID-19 history and severity) was observed among 12% of participants with an overall incidence rate of 18.6/1,000 person-years. The overall incidence rate was higher among men than women and age-specific incidence rates were significantly higher with older age among both men and women. However, our study findings do not support the hypothesis that poor oral health is associated with increased risk of COVID-19.
The proportion of new cases observed in a sub-population of CARRS is similar to that reported by Larvin et al., (13) from participants across United Kingdom, another country with a high cumulative case load (23,840,513) and COVID-19 deaths (2,07,375) comparable to India (1). Although the COVID-19 cases reported in our study included those assessed using the WHO’s clinical and epidemiological criteria, among those tested for COVID-19, an overall 24% test positivity was observed which also corresponds to a high-test positivity rate (> 20%) as reported in several regions of India including New Delhi in April, 2021 during the peak of second wave (32).
The incidence rates observed in our study are consistent with those reported in other countries and settings (6, 10, 11, 33). It is noteworthy that the differences in incidence rates among men and women narrowed with advancing age and older women (>60 years) tended to have higher incidence rates than men of the same age; an observation previously reported elsewhere (34). Though early epidemiological studies reported lower risk of COVID-19 in women (33, 35), the gender differences reduced with the subsequent waves of the pandemic (36, 37).
Our finding on the association between baseline oral disease and risk of COVID-19 was in disagreement with the results of an earlier study by Anand and colleagues (in India) who reported significantly increased risk of COVID-19 infection with gingivitis, and severe periodontitis (12). This could be due to the differences in study design (case–control vs. prospective) and settings (hospital-based vs. community). On balance, the existing literature suggests that while severity of COVID-19 infection may be positively associated with oral health indicators including PD (14–19), the occurrence of COVID-19 may be unrelated to oral health (13). One of the largest available studies, examined retrospective UK Biobank data on oral health status from 13,253 adults and also reported no association between poor oral health (loose teeth or painful, bleeding gums) and risk of COVID-19 infection. Nevertheless, the observed results might have also been affected by systematic error, such as uncontrolled confounding or insufficient statistical power to detect precise associations due to the high prevalence of GD and PD at baseline in our study population and shared yet competing risk factors such as age and comorbid conditions. Due to the small sample size, we were limited in our ability to test the association between baseline oral disease and severity of COVID-19, however, crude analysis revealed no significant difference. The UK study reported a 70% increased risk of death due to COVID-19 among participants with painful or bleeding gums (indicating the severity) compared to the control group (13). It also worth noting that the association with “bleeding or painful gums” may be different from the association with “loose teeth”; however, a more in-depth understanding of this difference will require further evaluations.
Other studies focusing on COVID-19 severity or complications such as assisted ventilation, intensive care admission and deaths report 3 to 36 times higher odds of any COVID-19 complication among periodontally compromised individuals (14–16, 18, 19, 38) compared to those with healthy periodontium. Despite reporting statistically significant results, the wide confidence intervals indicate low precision due to small sample size. Other limitations of these studies include convenience sampling, relative paucity of prospective data, lack of data from clinical oral examinations, and limited information on recent access to oral care (Supplementary Table S2, 12–19, 39–43). Additionally, only one of the previous studies had a representative population-based sample (13) and sample for most studies comprised of COVID-19 positive cases to explore the association with severity rather than risk (14–19).
A plausible biological explanation for the association of GD and PD with COVID-19 risk and severity is the increase in the expression of viral adhesion receptors such as ACE2 on the mucosa of oral cavity, galectin-3 (44–48) and transmembrane protease serin 2 (TMPRSS2), on oral epithelium which is necessary for activation of the SARS-CoV-2 S-protein to bind with host cells and increase its infectivity (49, 50). Additionally, oral bacterial dysbiosis, defined as shift from healthy microbiome toward pathogenic gram-negative anaerobic genera (51), associated with PD may lead to bacterial co-infection through aspirated gingival crevicular fluid thereby initiating inflammatory changes including “cytokine storm” (52, 53).
Ours is one of the largest population-based studies with a prospective design from a low- and middle-income setting to quantify the association between GD/PD and COVID-19 risk in one of the worst affected regions. New Delhi reported 2,002,772 cases with over 26,500 deaths (26) as on September 2022. Additional strengths of our study include the objective clinical assessment data on oral health status (for exposure) and a comprehensive questionnaire administered directly to the participants or household members (for deceased participants) to gather COVID-19 information (outcomes). Use of the WHO COVID-19 case criteria based on self-reported COVID-19 history and severity (31) addresses the concerns of low testing rates during the peak waves of the pandemic (6).
An important limitation of our study was the inability to consider the time-dependent nature of the main exposure, i.e., changes in GD or PD status during follow-up. We attempted to partly account for this by adjusting for access to oral care during this time-period. Although, this could have missed those who newly developed oral disease during the recent period and did not access care, this was unlikely to have influenced our findings as a small proportion of participants presented with apparently healthy gingiva and periodontium at baseline. As the outcome was self-reported, there was a likelihood of recall bias in reporting details of COVID-19 infection, symptoms, and management. However, respondents tend to remember such uncommon/severe events in recent past. Another limitation due to the prospective nature of the study is the loss to follow-up, especially given the migration of people during the pandemic. However, the loss to follow-up was just over 15% and baseline characteristics of respondents with those lost to follow-up did not differ largely.
In summary, although we did not find an association between poor gingival/periodontal health and increased risk of COVID-19, our study provides insights into the epidemiological pattern of COVID-19 at a community level. Studies, such as ours provide an opportunity to explore novel links between oral health and systemic conditions enabling a better understanding of the disease pathways and strategies to manage them (54) and to prospectively follow participants and assess immediate and delayed complications (55).
The datasets presented in this article are not readily available because of privacy issues. Requests to access the datasets should be directed to the Indian principal investigator of the CARRS study (DP at ZHByYWJoYWthcmFuQGNjZGNpbmRpYS5vcmc=).
The studies involving human participants were reviewed and approved by Institutional Ethics Committee-Centre for Chronic Disease Control, New Delhi, India. The ethics committee waived the requirement of written informed consent for participation.
IG and KS contributed to conceptualization, project administration, data curation, analysis, interpretation, writing, and reviewing the manuscript. DK did the formal analysis and interpretation, reviewing and editing of manuscript. SP, MG, SM, MA, NT, KN, and DP contributed to conceptualization and reviewing and editing of manuscript. All authors contributed to the article and approved the submitted version.
The work was supported by the Cardiometabolic Risk Reduction in South Asia Surveillance Study was funded in part by the National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health (NIH), Department of Health and Human Services [Contract no. HHSN268200900026C] and the United Health Group (Minneapolis, MN, USA). Research reported in this publication is a sub-study of the CARRS study supported by the National Heart, Lung, And Blood Institute of the National Institutes of Health under Award Number P01HL154996. Several members of the research team were/are supported by the Fogarty International Center (FIC) and the Eunice Kennedy Shriver National Institute of Child Health & Human Development, NIH through Grant Number 1 D43 HD065249, FIC at the NIH under Award Number D43TW009135 and NIH, National Cancer Institute grant number P20CA210298-01. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
This sub-study was coordinated by CoE-CARRS (Center of Excellence-Center for Cardiometabolic Risk Reduction in South Asia) based at the Public Health Foundation of India (PHFI), New Delhi, India in collaboration with the Centre for Chronic Disease Control (CCDC), New Delhi, Emory University, Atlanta, USA, All India Institute of Medical Sciences (AIIMS), New Delhi, Madras Diabetes Research Foundation (MDRF), Chennai, India and Aga Khan University, Karachi, Pakistan. We would like to thank all participants for their time and valuable insights and the field team of CARRS-Study for assistance with approaching the participants and collecting data.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1108465/full#supplementary-material
CARRS, Centre for Cardiometabolic Risk Reduction in South-Asia Study; GD, Gingival Disease; IRR, Incidence Rate Ratio; OHS, Oral Health Study; PD, Periodontal Disease; SARS-COV-2, Severe Acute Respiratory Syndrome Coronavirus-2; SD, Standard Deviation; WHO, World Health Organization.
1. Johns Hopkins University and Medicine Coronovirus Resource Centre. (2021). COVID-19 Dashboard. Available at: https://coronavirus.jhu.edu/map.html (Accessed September 30, 2022)
2. World Health Organisation. (2021). WHO COVID-19 dashboard. Available at: https://covid19.who.int/ (Accessed September 30, 2022)
3. Government of India. (2022). Ministry of Health and Family Welfare. Available at: https://www.mohfw.gov.in/ (Accessed October 1, 2022)
4. Holt, H, Talaei, M, Greenig, M, Zenner, D, Symons, J, Relton, C, et al. Risk factors for developing COVID-19: a population-based longitudinal study (COVIDENCE UK). Thorax. (2022) 77:900–12. doi: 10.1136/thoraxjnl-2021-217487
5. Pfützner, A, Lazzara, M, and Jantz, J. Why do people with diabetes have a high risk for severe COVID-19 disease?-a dental hypothesis and possible prevention strategy. J Diabetes Sci Technol. (2020) 14:769–71. doi: 10.1177/1932296820930287
6. Laxminarayan, R, Chandra Mohan, B, Vinay, TG, Arjun Kumar, KV, Wahl, B, and Lewnard, JA. SARS-CoV-2 infection and mortality during the first epidemic wave in Madurai, South India: a prospective, active surveillance study. Lancet Infect Dis. (2021) 21:1665–76. doi: 10.1016/S1473-3099(21)00393-5
7. Barman Roy, D, Gupta, V, Tomar, S, Gupta, G, Biswas, A, Ranjan, P, et al. Epidemiology and risk factors of COVID-19-related mortality. Cureus. (2021) 13:e20072. doi: 10.7759/cureus.20072
8. Centers fror Disease Control and Prevention (CDC). COVID-19. Available at: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (Accessed October 1, 2022)
9. Grasselli, G, Zangrillo, A, Zanella, A, Antonelli, M, Cabrini, L, Castelli, A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA. (2020) 323:1574. doi: 10.1001/jama.2020.5394
10. Zhang, X, Tan, Y, Ling, Y, Lu, G, Liu, F, Yi, Z, et al. Viral and host factors related to the clinical outcome of COVID-19. Nature. (2020) 583:437–40. doi: 10.1038/s41586-020-2355-0
11. Gallo Marin, B, Aghagoli, G, Lavine, K, Yang, L, Siff, EJ, Chiang, SS, et al. Predictors of COVID-19 severity: a literature review. Rev Med Virol. (2021) 31:1–10. doi: 10.1002/rmv.2146
12. Anand, PS, Jadhav, P, Kamath, KP, Kumar, SR, Vijayalaxmi, S, and Anil, S. A case-control study on the association between periodontitis and coronavirus disease (COVID-19). J Periodontol. (2022) 93:584–90. doi: 10.1002/JPER.21-0272
13. Larvin, H, Wilmott, S, Wu, J, and Kang, J. The impact of periodontal disease on hospital admission and mortality during COVID-19 pandemic. Front Med. (2020) 7:1–7. doi: 10.3389/fmed.2020.604980
14. Alnomay, N, Alolayan, L, Aljohani, R, Almashouf, R, and Alharbi, G. Association between periodontitis and COVID-19 severity in a tertiary hospital: a retrospective cohort study. Saudi Dent J. (2022) 34:623–8. doi: 10.1016/j.sdentj.2022.07.001
15. Costa, CA, Vilela, ACS, Oliveira, SA, Gomes, TD, Andrade, AAC, Leles, CR, et al. Poor oral health status and adverse COVID-19 outcomes: a preliminary study in hospitalized patients. J Periodontol. (2022) 93:1889–901. doi: 10.1002/JPER.21-0624
16. Mishra, S, Gupta, V, Rahman, W, Gazala, MP, and Anil, S. Association between periodontitis and COVID-19 based on severity scores of HRCT chest scans. Dent J. (2022) 10:106. doi: 10.3390/dj10060106
17. Gupta, S, Mohindra, R, Singla, M, Khera, S, Sahni, V, Kanta, P, et al. The clinical association between periodontitis and COVID-19. Clin Oral Invest. (2022) 26:1361–74. doi: 10.1007/s00784-021-04111-3
18. Said, KN, Al-Momani, AM, Almaseeh, JA, Marouf, N, Shatta, A, Al-Abdulla, J, et al. Association of periodontal therapy, with inflammatory biomarkers and complications in COVID-19 patients: a case control study. Clin Oral Investig. (2022) 26:6721–32. doi: 10.1007/s00784-022-04631-6
19. Marouf, N, Cai, W, Said, KN, Daas, H, Diab, H, Chinta, VR, et al. Association between periodontitis and severity of COVID-19 infection: a case–control study. J Clin Periodontol. (2021) 48:483–91. doi: 10.1111/jcpe.13435
20. Page, RC. Gingivitis*. J Clin Periodontol. (1986) 13:345–55. doi: 10.1111/j.1600-051X.1986.tb01471.x
21. Loos, BG, and Van Dyke, TE. The role of inflammation and genetics in periodontal disease. Periodontol 2000. (2020) 83:26–39. doi: 10.1111/prd.12297
22. Frencken, JE, Sharma, P, Stenhouse, L, Green, D, and Laverty, DDT. Global epidemiology of dentalcaries and severe periodontitis–a comprehensive review. J Clin Periodontol. (2017) 44:S94–S105. doi: 10.1111/jcpe.12677
23. Vos, T, Abajobir, AA, Abate, KH, Abbafati, C, Abbas, KM, Abd-Allah, F, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet. (2017 Sep) 390:1211–59. doi: 10.1016/S0140-6736(17)32154-2
24. Bernabe, E, Marcenes, W, Hernandez, CR, Bailey, J, Abreu, LG, Alipour, V, et al. Global, regional, and National Levels and trends in burden of Oral conditions from 1990 to 2017: a systematic analysis for the global burden of disease 2017 study. J Dent Res. (2020) 99:362–73. doi: 10.1177/0022034520908533
25. Shewale, AH, Gattani, DR, Bhatia, N, Mahajan, R, and Saravanan, SP. Prevalence of periodontal disease in the general population of India-a systematic review. J Clin Diagn Res. (2016) 10:ZE04–9. doi: 10.7860/JCDR/2016/17958.7962
26. Government of Delhi Department of Information & Publicity. Delhi fights Corona. Available at: https://delhifightscorona.in/ (Accessed September 30, 2022)
27. Nair, M, Ali, MK, Ajay, VS, Shivashankar, R, Mohan, V, Pradeepa, R, et al. CARRS surveillance study: design and methods to assess burdens from multiple perspectives. BMC Public Health. (2012) 12:701. doi: 10.1186/1471-2458-12-701
28. Kondal, D, Patel, SA, Ali, MK, Mohan, D, Rautela, G, Gujral, UP, et al. Cohort profile: the center for cArdiometabolic risk reduction in South Asia (CARRS). Int J Epidemiol. (2022) 51:e358–71. doi: 10.1093/ije/dyac014
29. Rawal, I, Ghosh, S, Hameed, SS, Shivashankar, R, Ajay, VS, Patel, SA, et al. Association between poor oral health and diabetes among Indian adult population: potential for integration with NCDs. BMC Oral Health. (2019) 19:191. doi: 10.1186/s12903-019-0884-4
30. Page, RC, and Eke, PI. Case definitions for use in population-based surveillance of periodontitis. J Periodontol. (2007) 78:1387–99. doi: 10.1902/jop.2007.060264
31. WHO. (2022). Public health surveillance for COVID-19. Available at: https://www.who.int/publications/i/item/who-2019-nCoV-surveillanceguidance-2020.8
32. Ritchie, Hannah, Mathieu, Edouard, Rodés-Guirao, Lucas, Appel, Cameron, Giattino, Charlie, Ortiz-Ospina, Esteban, et al. (2020). Coronavirus pandemic (COVID-19). Available at: https://ourworldindata.org/coronavirus (Accessed October 3, 2022)
33. Chen, N, Zhou, M, Dong, X, Qu, J, Gong, F, Han, Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet (London, England). (2020) 395:507–13. doi: 10.1016/S0140-6736(20)30211-7
34. O’Brien, J, Du, KY, and Peng, C. Incidence, clinical features, and outcomes of COVID-19 in Canada: impact of sex and age. J Ovarian Res. (2020) 13:137. doi: 10.1186/s13048-020-00734-4
35. Mazumder, A, Arora, M, Bharadiya, V, Berry, P, Agarwal, M, Behera, P, et al. SARS-CoV-2 epidemic in India: epidemiological features and in silico analysis of the effect of interventions. F1000Res. (2020) 9:315. doi: 10.12688/f1000research.23496.2
36. Global Health. (2020). 50/50. Available at: https://globalhealth5050.org/covid19/age-and-sex-data/ (Accessed 2022 September 29)
37. World Health Organization. (2020). World Health Organization. Coronavirus disease (COVID-19) situation report–198.
38. Shamsoddin, E. Is periodontitis associated with the severity of COVID-19? Evid Based Dent. (2021) 22:66–8. doi: 10.1038/s41432-021-0179-x
39. Kamel, AHM, Basuoni, A, Salem, ZA, and Abubakr, N. The impact of oral health status on COVID-19 severity, recovery period and C-reactive protein values. Br Dent J. (2021) 1–7. doi: 10.1038/s41415-021-2656-1
40. Gardelis, P, Zekeridou, A, Suh, N, Le Terrier, C, Stavropoulos, A, and Giannopoulou, C. A pilot clinical and radiographic study on the association between periodontitis and serious COVID-19 infection. Clin Exp Dent Res. (2022) 8:1021–7. doi: 10.1002/cre2.610
41. Kaur, A, Sandhu, HS, Sarwal, A, Bhagat, S, Dodwad, R, Singh, G, et al. Assessment of correlation of COVID-19 infection and periodontitis- a comparative study. J Fam Med Prim care. (2022) 11:1913–7. doi: 10.4103/jfmpc.jfmpc_1978_21
42. Katz, J, Yue, S, and Xue, W. Dental diseases are associated with increased odds ratio for coronavirus disease 19. Oral Dis. (2022) 28:991–3. doi: 10.1111/odi.13653
43. Wang, Y, Deng, H, Pan, Y, Jin, L, Hu, R, Lu, Y, et al. Periodontal disease increases the host susceptibility to COVID-19 and its severity: a Mendelian randomization study. J Transl Med. (2021) 19:528. doi: 10.1186/s12967-021-03198-2
44. Badran, Z, Gaudin, A, Struillou, X, Amador, G, and Soueidan, A. Periodontal pockets: a potential reservoir for SARS-CoV-2? Med Hypotheses. (2020) 143:109907. doi: 10.1016/j.mehy.2020.109907
45. Xu, H, Zhong, L, Deng, J, Peng, J, Dan, H, Zeng, X, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci. (2020) 12:8. doi: 10.1038/s41368-020-0074-x
46. Takahashi, Y, Watanabe, N, Kamio, N, Kobayashi, R, Iinuma, T, and Imai, K. Aspiration of periodontopathic bacteria due to poor oral hygiene potentially contributes to the aggravation of COVID-19. J Oral Sci. (2020) 63:1–3. doi: 10.2334/josnusd.20-0388
47. Bertolini, M, Pita, A, Koo, S, Cardenas, A, and Meethil, A. Periodontal disease in the COVID-19 era: potential reservoir and increased risk for SARS-CoV-2. Pesqui Bras Odontopediatria Clin Integr. (2020) 20:162. doi: 10.1590/pboci.2020.162
48. Kara, C, Çelen, K, Dede, FÖ, Gökmenoğlu, C, and Kara, NB. Is periodontal disease a risk factor for developing severe Covid-19 infection? The potential role of Galectin-3. Exp Biol Med (Maywood). (2020) 245:1425–7. doi: 10.1177/1535370220953771
49. Sakaguchi, W, Kubota, N, Shimizu, T, Saruta, J, Fuchida, S, Kawata, A, et al. Existence of SARS-CoV-2 entry molecules in the Oral cavity. Int J Mol Sci. (2020) 21:6000. doi: 10.3390/ijms21176000
50. Hoffmann, M, Kleine-Weber, H, Schroeder, S, Krüger, N, Herrler, T, Erichsen, S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. (2020) 181:e8:271–80. doi: 10.1016/j.cell.2020.02.052
51. Kilian, M, Chapple, ILC, Hannig, M, Marsh, PD, Meuric, V, Pedersen, AML, et al. The oral microbiome – an update for oral healthcare professionals. Br Dent J. (2016) 221:657–66. doi: 10.1038/sj.bdj.2016.865
52. Hayata, M, Watanabe, N, Tamura, M, Kamio, N, Tanaka, H, Nodomi, K, et al. The Periodontopathic bacterium fusobacterium nucleatum induced Proinflammatory cytokine production by human respiratory epithelial cell lines and in the lower respiratory organs in mice. Cell Physiol Biochem. (2019) 53:49–61. doi: 10.33594/000000120
53. Sahni, V, and Gupta, S. COVID-19 & periodontitis: the cytokine connection. Med Hypotheses. (2020) 144:109908. doi: 10.1016/j.mehy.2020.109908
54. Khanji, MY, Aung, N, Chahal, CAA, and Petersen, SE. COVID-19 and the UK biobank-opportunities and challenges for research and collaboration with other large population studies. Front Cardiovasc Med. (2020) 7:156. doi: 10.3389/fcvm.2020.00156
55. World Health Organization. (2021). A clinical case definition of post COVID-19 condition by a Delphi consensus. Geneva. 1–27. Available at: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (Accessed October 1, 2022).
Keywords: SARS-CoV-2, COVID-19, periodontal disease, gingival disease, oral health
Citation: Gupta I, Patel SA, Kondal D, Goodman M, Mohan S, Ali MK, Tandon N, Narayan KMV, Prabhakaran D and Shridhar K (2023) Epidemiological pattern of COVID-19 and its association with periodontal health in an urban Indian cohort. Front. Public Health. 11:1108465. doi: 10.3389/fpubh.2023.1108465
Edited by:
João Botelho, Egas Moniz Interdisciplinary Research Center, PortugalReviewed by:
Sanjay Pandey, All India Institute of Medical Sciences (Patna), IndiaCopyright © 2023 Gupta, Patel, Kondal, Goodman, Mohan, Ali, Tandon, Narayan, Prabhakaran and Shridhar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ishita Gupta, aXNoaXRhQGNjZGNpbmRpYS5vcmc=
†ORCID: K. M. Venkat Narayan, https://orcid.org/0000-0001-8621-5405
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.