 Marie Cholley-Gomez
Marie Cholley-Gomez Steven Laujac1,3
Steven Laujac1,3 Cyrille Delpierre
Cyrille Delpierre Marion Carayol
Marion Carayol- 1IAPS Laboratory “Impact of Physical Activity on Health”, University of Toulon, Toulon, France
- 2ACTES Laboratory, University of Antilles, Pointe-à-Pitre, Guadeloupe
- 3Centre Hospitalier Intercommunal Toulon-La Seyne sur Mer, Hôpital Sainte Musse, Toulon, France
- 4EQUITY Team, CERPOP UMR 1295, Inserm-Université Toulouse III, Toulouse, France
Objectives: Preventive actions of sedentary behavior (SB) based on the socio-ecological model are needed among children and young adolescents. The aim of this systematic review is to ascertain the effectiveness of multilevel interventions (i.e., involving consideration of at least two interventional levels) in reducing sedentary time (ST) in children aged 5–12 years.
Methods: Adhering to PRISMA guidelines, a systematic literature search was conducted in three databases (PsyInfo, PubMed and ERIC) until July 2021.
Results: 30 trials met the eligibility criteria and were included. They showed acceptable (< 8, n = 18) and high (≥ 8, n = 12) methodological quality. Among studies targeting 2 (n = 2), 3 (n = 19) and 4 levels (n = 9), 1 (50%), 9 (47%) and 7 (78%) were effective and reported significant reduction of ST, respectively.
Conclusion: Interventions tend to be more effective when they involve 4 levels, using both agentic and structural strategies (targeting intrinsic determinants, in the organizational environment of the child). Findings underline the relevance of multilevel strategies to reduce ST in children, but also raise issues about operationalization of the socio-ecological perspective.
Systematic review registration: PROSPERO, identifier: CRD42020209653.
Introduction
Sedentary behavior in young populations: an increasing public health concern
Sedentary lifestyle or sedentary behavior (SB) refers to “any waking behavior characterized by an energy expenditure ≤1.5 metabolic equivalents (METs)” (1), such as reading, watching TV, or working on a computer. Among SB, “screen-related” SB (2) are particularly worrying this last decade. Indeed, Sedentary Time (ST) has been associated with poorer health outcomes in children (3, 4).
However, a significant part of children and young adolescents does not reach active lifestyle recommendations (5): SB (i.e., ≥4 h 30 min of daily sitting time) was identified in 76.8% of European adolescents in 2017 with no differences between girls and boys (6), and over the world, 81% of adolescents aged 11–17 years were insufficiently physically active in 2016 (7). In France, national surveys showed that screen-time increases with age: more than 50% of school-aged children (6–10 years) spent at least 3 h/day [ESTEBAN 2014–2016 survey, see Balicco et al., (8)]; and between 2007 and 2015 [Inca2, 2007, and Inca3, 2015, see Dubuisson et al. (9)], screen time was increased by 20 min on average.
The socio-ecological approach of sedentary behavior
There is a great demand in research for addressing public health issues by focusing on structural social determinants, particularly within the field of PA and sedentary lifestyle (10–14).
The socio-ecological model, based on the original work of McLeroy et al. (15) provides a useful comprehensive framework for this purpose. It marks a break with the cognitive behavioral-based approaches, by considering the social mechanisms of the production of health issues (16). The visual metaphor is a series of concentric circles representing different levels of influence on behavior. With a reciprocal determinism, each environmental level contains multiple types of environments (i.e., social, physical) and is in interaction with others.
Applied to the determinants of SB, this multifactorial approach states that these behaviors can be influenced by a multiplicity of levels, from the most proximal to the broader settings: intrapersonal [Psychological (e.g., self-esteem, attitudes toward SB) and physiological elements (e.g., capacities, health)], interpersonal [Social support of caregivers (parental rules, peers' behavior, encouragement from teachers…)], and organizational [Home; institution (care center, school): physical and social aspects (e.g., school wellness policy, garden equipment)] characteristics, and finally societal level including community Neighborhood, community environment (e.g., local associations) and public policies (Laws, national and local regulations (e.g., transport system, media, sports facilities in the city) (17).
The growing literature claiming for multilevel interventions assumed a larger effect on health outcomes, in comparison to single-level (intrapersonal) strategies but this argument suffers from limited empirical evidence (18–20).
Interventions targeting sedentary lifestyle in school-aged populations
Preventive actions of SB are more and more needed among children and young adolescents [WHO guidelines, (5)]. Studies evaluating these actions in children have been increasing these recent years, and several systematic reviews and/or meta-analyses were published this last decade. Overall, these studies highlight the high heterogeneity of trials and the difficulty to establish strong evidence regarding interventions for the promotion of a less sedentary lifestyle. However, promising strategies are mentioned such as behavior change interventions (21, 22), electronic TV monitoring devices or TV turn-off (13, 23). Family and high parental involvement is a crucial interventional strategy (22, 24, 25), and, when focusing on school environment and policy, studies showed that adequate and accessible facilities for PA, and that educational materials, pedagogic practices and standing desks in classroom are significant opportunities in reducing ST (13, 23, 26, 27).
Multi-component and mixed interventions, incorporating both behavioral and environmental components (27, 28) were also mentioned as promising.
To this day, no study has systematically examined the effectiveness of multilevel, socio-ecological-based, interventions on ST-SB only, depending on the types and number of levels targeted by the strategies used. A few reviews have investigated socio-ecological or multilevel interventions specifically but none has focused on the reduction of ST/SB: Mehtälä et al. (29) investigated socio-ecological-based interventions aiming to increase the level of young (2–6 years) children's PA; the review of Kellou et al. (30) aimed to analyze the effectiveness of interventions preventing overweight in youngsters by promoting PA; in a recent review, Bernal et al. (20) compared the effectiveness of school-based multi-component vs. mono-component interventions carried out to promote children's PA.
Therefore, the aim of the present review is to systematically summarize evidence regarding the effectiveness of socio-ecological model-based multilevel intervention strategies to reduce ST in children and young adolescents. It aims to answer the following research questions: are interventions using multilevel/socio-ecological framework and targeting SB effective to reduce ST in children? Are these interventions more effective when they target more levels? In addition, as previously mentioned, to reduce ST, family-based interventions could be more effective if they use a strong parental involvement as a key strategy and not just as a supervisory role. This has led us to consider, in this review, not only the settings or the levels of the intervention, but also the involvement or not, and the degree of involvement of caregivers or social support surrounding the child (e.g., parents, teachers): are these multilevel interventions more effective when they involve a stakeholder/level representative (e.g., teacher, parent) at a strong degree?
Methods
The present article reports a systematic review that has been conducted according to The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. The review aims and methods were registered on PROSPERO (registration nr CRD42020209653).
Systematic literature search and inclusion/exclusion criteria
Studies were included when they met the following PICOS criteria:
(i) P(Population): studies on healthy human subjects (i.e., no clinical population) that involve school-aged children (i.e., between 5 and 12 years-old) were included; studies with preschool < 5 years old and adolescents aged more than 12 were then excluded; studies involving only high-risk populations, defined as children or young adolescents being overweight with high risk of obesity, obese, or specific clinical populations (e.g., young with pathologies, e.g., cancer, or any disease) were excluded. Studies comparing normal weight children and obese children were included when results for the normal weight children were described separately.
(ii) I (Intervention): I (Intervention): intervention had to consider the reduction of ST, even if other health behaviors (e.g., nutrition habits, PA) could be mainly targeted; studies with interventions targeting at least two among the five levels of intervention according to the socio-ecological model of McLeroy et al. (15) (i.e., intra-, interpersonal, organizational, community-, society-based) were included;
(iii) C (Control), only studies with a control, or a comparison group (e.g., alternative intervention) were considered;
(iv) O (Outcome): studies had to report measures related to SB (e.g., TV viewing, computer-use, sitting-time); either objective (e.g., accelerometry) or reported (e.g., questionnaire) measures were considered.
(v) S (Study design): to be included, the study design had to test an intervention and to involve a comparative group. Randomized (or cluster randomized) studies were included but randomization was not mandatory. Studies performed in laboratory settings, studies without a control or comparative group, and cohort studies were excluded.
Searching process
An electronic database search of PubMed (MEDLINE), PsycInfo and ERIC has been performed through the end of July 2021 (data published from 2000 to the present days, July 2021) languages restricted to English and French. We decided to start selection in 2000 as there has been growing consideration regarding ST and SB, and more particularly for a wide range of “screen-time related behaviors” (2) in these last two decades. Studies targeting only TV-viewing or computer-use seem to not accurately reflect a growing reality for children and young adolescents. Indeed, in young populations, most of the ST is made up of modern screen items that arose in the 2,000 decade (e.g., computer/laptop, smartphone, tablet (31). We used a combination of keywords related to sedentary lifestyle and screen-related behavior, public health interventions, preventive actions, and socio-ecological model, multilevel strategies or studies targeting several environments.
Finally, the research algorithm was the following: (sedentar* OR screen* OR multimedia) AND (intervention* OR promot* OR prevent*) AND (multi* OR ecologic* OR environment* OR context*) NOT (disease* OR patholog*). Limiters were the following: age ranging from 5 to 12 years; the study design: comparative, controlled, multicenter studies were included; the languages English and French; and the period of publication, starting from 2000 to July 2021.
First, the first author MCG selected eligible studies based on the title and/or the abstract and assessed the inclusion criteria to determine preliminary eligibility of studies. Following the PRISMA guidelines, at this first step of the selection on abstract, the author applied the PICOS method to check if the data fit the following inclusion criteria.
Second, MCG and MC separately read the full text, using the inclusion PICOS criteria to assess the final inclusion of articles. Any discrepancies were discussed until consensus was reached. MCG and SL extracted relevant data including methodology, participants, outcomes, and results. The following data were extracted: concerning the methodology, population details (country of intervention, number of and age mean or range of participants in control and intervention group), duration of intervention, use and type of theoretical framework, main setting (e.g., school, home) of intervention, study timelines. Each level targeted were identify; for the intrapersonal level, type of strategies (i.e., informational vs. behavioral) was detailed; in the interpersonal level, the type and degree of involvement (“+” if strong, meaning being active, “-” if rated weak, meaning passive) of caregivers (e.g., teachers, parents) were indicated. At the organizational level, type of setting was mentioned (e.g., school, home) with, for each of them, an indication of the kind of environment components (i.e., Physical, P, Social, S) targeted. Finally, results on SB-ST were briefly reported.
These elements are documented below in the summary Table 2, and described in results.
SL, PD, and MC checked the salient data and the methodological quality of trials included. Any discrepancies were resolved by discussion.
Methodological quality
The methodological quality of each trial was examined using an 11-item scale derived from Cochrane collaboration's tools for assessing risk of bias in RCTs (81). This adapted scale, used by Gourlan et al. (82) in their review, assesses information of studies regarding (1) the eligibility criteria for participants; (2) the details of the intervention provided for each intervention level; (3) if the process of the intervention implementation was monitored; (4) the specific objective(s) of the study clearly mentioned; (5) the calculation technique used to determine the sample size was mentioned; (6) the method used to randomize participants [if randomization was used]; (7) the blinding to group assignment of assessors; (8) the participants flow; (9) the characteristics of the care providers performing the intervention; (10) the baseline data of participants are described for intervention and control groups; and (11) the number of participants included in each analysis is mentioned. All items were coded as “yes” (+), “no” (-) or “not applicable” (NA).
Results
Studies selection process
The literature search yielded a total of 6,166 publications: 1,821 in Pubmed, 1,590 in ERIC and 2,755 in PsychInfo. The searching and selection process is summarized in the flow chart presented below, Figure 1. After removing duplicates (n = 5,842) and checking eligibility of the studies, a total of 30 relevant studies were finally included in this systematic review (reported by 51 publications, including e.g., protocol, midway, follow-up publications).
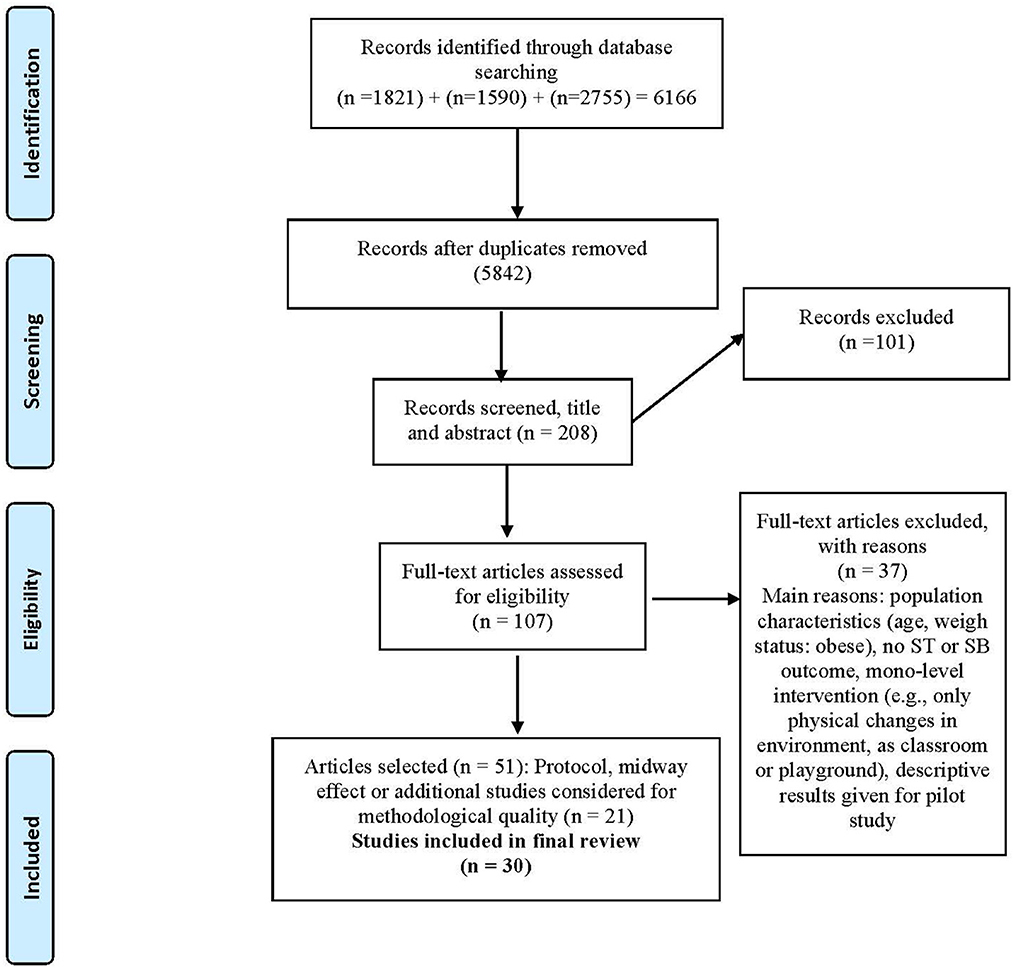
Figure 1. PRISMA flow diagram of the review (83).
Methodological quality
Briefly, based on the quality assessment form, most of the trials (n = 18 out of 30) demonstrated acceptable quality (i.e., rated under 8, on a total of 11 points), and 12 high quality (i.e., scoring ≥ 8). Concerning the criterion, the calculation technique used to determine the sample size of the trial was mentioned in less than half of the studies (n = 12 out of 30), and blinding to group assignment of assessors was mentioned in two trials only. Four studies were not randomized and among the others, 15 trials did not mention the method used to randomize participants. All studies clearly provided specific objectives, and most of them provided details of the intervention for each level (n = 28), participants' eligibility criteria (n = 21) and baseline characteristics (n = 29).
The following Table 1 summarizes the methodological quality assessment and reports the rate for each criterion and for each study selected.
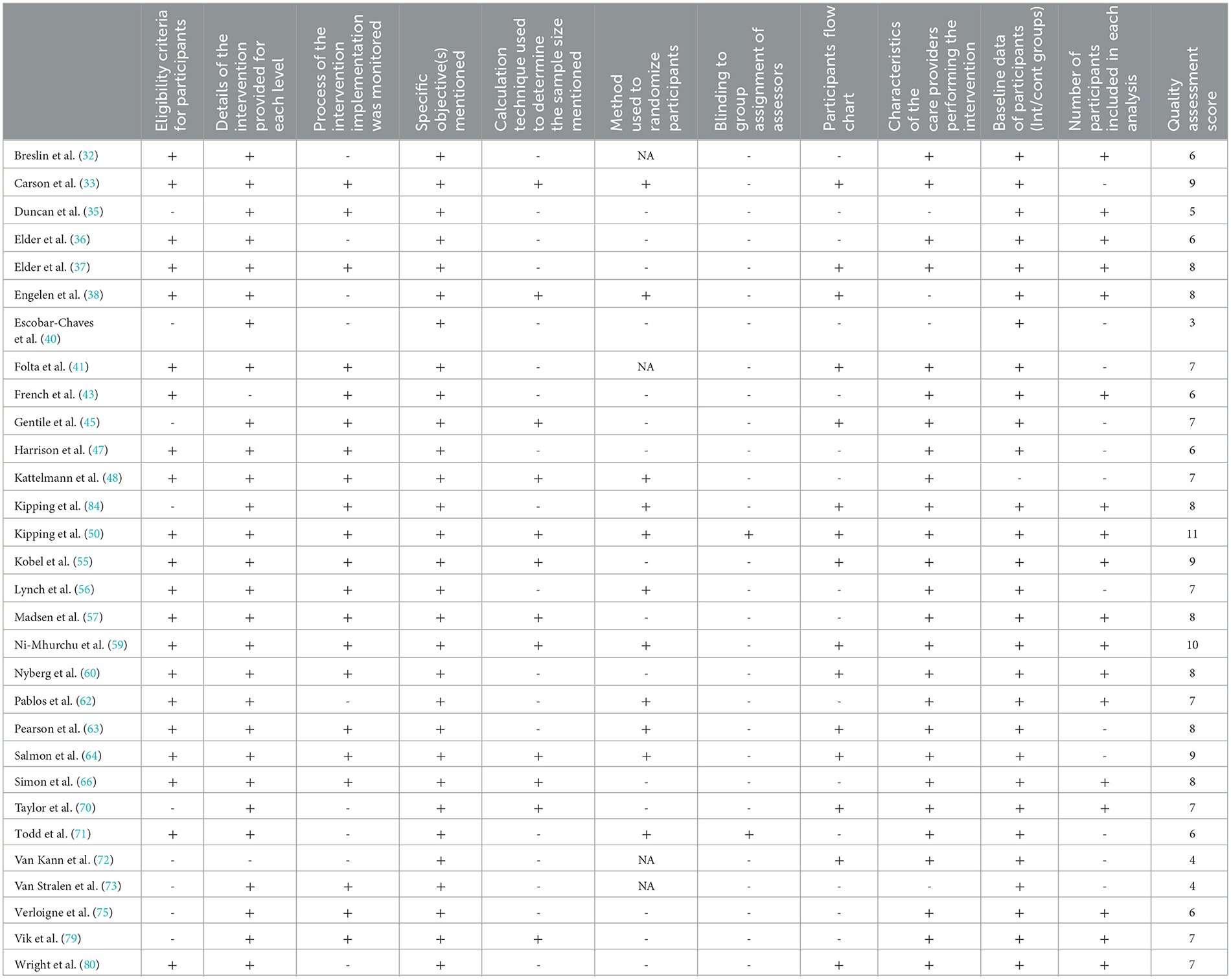
Table 1. Methodological quality assessment of interventions selected for the review (detail by criterion and global quality score).
Characteristics of trials included
The salient data are summarized in Table 2 with a description of the participants' characteristics and main details of the intervention (duration, settings, theoretical framework, assessment methods, main results on ST-SB, strategies by level targeted, degree of caregiver's involvement).

Table 2. Main characteristics of trials and strategies by levels targeted.
Briefly, the 30 trials were published between 2000 and 2020, in 2006 for the earliest and in 2020 for the most recent with 23 (77%) studies in the last decade. Eleven interventions were conducted in the USA, 15 took place in Europe (e.g., Poland, Sweden, France, Belgium), and 4 in New Zealand, or Australia. Populations from 10 trials were made up of low-income groups from deprived areas; one study (71) solely targeted boys. Baseline sample sizes ranged from 29 children in a pilot study (59), to 3,147 in a trial (79) involving young populations from five European countries. The duration of the delivered interventions ranged from 4 months in the pilot study of Lynch (2016) (56) to 30 months for the trial led by Wright (2013) (80).
Social-cognitive theories (of behavior change/motivation) (85, 86) and socio-ecological models (12, 15) are the most frequently theoretical backgrounds mentioned. However, most of the studies (N = 18) do not refer to the socio-ecological perspective, or any ecological anchoring, and six studies do not mention any theoretical background.
Among the 30 included studies, the main setting of intervention is school in 24 trials. More precisely, three studies targeted only the home environment, four interventions only the school environment, two studies involved home and community (city recreation center; participatory research) and almost half of the trials (N = 14) school and home. For the remaining studies (N = 7), interventions were implemented or involved both school, home and community (partnership with community stakeholders, e.g., medical staffs, community health workers, local municipalities, PA club educators, territorial and community agencies in charge of transportation infrastructures).
Reported outcomes included ST or SB for all of the studies, and in 28 (93%) trials, PA outcomes (e.g., steps, sport participation, MVPA) was measured as well; only two trials did not targeted PA: screen-time was assessed in addition to dietary variables, and beverage consumption and BMI (43, 63). Regarding sedentary assessment, 16 (53%) trials used only subjective assessment of ST-SB: 11 studies reported only self-declared assessment; parental/caregiver questionnaire only, and combined with self-reported measures, were respectively used in 4, and one (45) study; one trial (36) used observational data recorded by researchers. Objective assessment was used in 8 trials, that solely used a monitored or device-based method (e.g., pedometer, accelerometer). Finally, a combination of self-declared and device-based, and parent's and device-based assessments were reported in 3, and 2 studies, respectively.
Intervention components and strategies by level targeted
Table 2 summarizes the main characteristics of trials, and, for each targeted level, the type of strategy delivered. For the interpersonal level, we also considered the stakeholders/caregivers involved, and the strength of their participation.
Strategies used to deliver interventions can be described according to each socioecological model level.
Regarding the individual level (e.g., intrapersonal characteristics, such as attitudes, intrinsic motivation, skills), strategies were informational (e.g., passive: curriculum school program is designed to include health promotion and recommendation components about SB, energy-balance). Children sometimes received an educational program with key learning messages concerning various health determinants. Indeed, several interventions chose to include a multi-component strategy in delivering healthy messages: lessons and information could concern ST, PA, nutrition, or other health behaviors [e.g., (35, 48, 50)]. In this case, when the intervention aims to combine the messages on SB and physical activity with other health information, in an attempt to be more effective, it can be not easy to determine which component or part of the strategy was effective in reducing specifically ST, or an outcome isolated. Few studies (56, 72) mentioned informational determinants or knowledge in the intrapersonal level: e.g., delivering key learning messages (topics about weight, vegetables, recreational screen-time), presence of posters in the school. Cognitive components of strategies delivered could include goal setting to reduce electronic media, brainstorming, action-plan to achieve healthy behaviors or strategies to find alternative games and activities to replace SB. Mainly behavioral components were used in three interventions (36, 43, 70): e.g., active breaks bounce at the bell, playground activity challenge cards, training sessions, work with parents and children to limit screen-time. Most studies (N = 21) used a combination of informational and behavioral strategies (e.g., key learning messages during school lessons and a light active break; behavioral tools to modify behaviors and material and resources to identify healthy behaviors).
At the interpersonal level, one intervention component repeated in several designs of studies was the involvement of caregivers. Social support strategies were operationalized with the participation of parents, or other significant caregivers. The social circle, composed of people closed to the child, could be passively or actively involved: caregivers involved were mainly teachers and/or parents, but in some trials, school staff as principals, educators, health nurses, recreation center directors were also associated in the interpersonal level of intervention. Involvement was rated as “weak” (-) when passive: e.g., teachers who did not lead the lessons, but who were present during the intervention, who sent some information to the child's parents, who just received feedback from the research team who led the implementation. When their involvement was rated as strong (+), teachers could conduct the intervention, participate in material or tools development. Parents who took an active part in the intervention could attend workshops/meetings with their children, had activities or homework tasks to complete with children, or followed educational/motivational sessions with them. These study designs posit that having a supportive family environment can promote the targeted behavior change and be effective in reducing children's ST. Among studies (N = 27) targeting parents as social support (i.e., at the interpersonal level), 22 actively or strongly involved them, other studies targeted parents but with a more passive strategy (e.g., informational, as sending newsletters). In most studies (N = 20), implication of parents is linked with an involvement of school staff to target the entire social support of children (e.g., teachers, PE educators, nurses, educational staff in health promotion, recreational directors). This involvement is active in 17 trials.
At an environmental level (e.g., organizational, or institutional), almost half of the studies (N = 14) reported some physical components targeted: as for example, changes in the home or school physical environment (e.g., removing TV from the child's bedroom, install an electronic TV monitoring device, provide equipment and resources for physical activities, draw an asphalt line in the playground). Many studies were school-based [one was also recreational center based, (37)], some of them with a combination of school and home components strategies; few studies also included partnership with local municipalities, non-governmental partners, community stakeholders and external professionals (in the shape of collaborators in the field of nutrition, health staff, local community clinics, associations, municipal health employer, local sport clubs). Some actions were thus implemented outside of the initial institutional setting (e.g., steering committees with community members, afterschool sport leagues, sport competitions organized by sports clubs and local municipalities, event-specific activities in the community).
Few studies were community-based with a participatory research design (41, 45, 48, 80). In their intervention, Folta and others (2014) (41) targeted home and recreational centers, and the community environment by working with restaurants across the city to provide healthier options (e.g., offering more low-fat dairy products); the authors used a social ecological and systems approach, using community-based participatory research and involving community members in the development and implementation of the intervention. Kattelmann et al. (48) also used a similar design and formed steering committees composed of members of the research team, Expanded Food and Nutrition Education Program (EFNEP) staff, community members, and graduate students. Simon et al. (66) proposed, at the community level of their intervention, event-specific activities and established numerous partnerships (i.e., with medical staff, club educators, territorial and community agencies in charge of recreational areas and transportation infrastructures).
Effectiveness of interventions
Two studies targeted 2 levels (interpersonal and organizational), and all (100%) had high methodological quality (i.e., score equal to or higher than 8). Then, 19 studies targeting 3 levels (mainly intrapersonal, interpersonal and organizational), of which 14 (74%) had high methodological quality. Last, 9 trials used four-level strategies (i.e., intra-, interpersonal, organizational and community-based), of which 2 (22%) showed high quality, and 7 (78%) a lower quality score. No study achieved to target the macro-environment or public policies level (e.g., social and cultural norms via media, urban planning, transport system).
Effectiveness on sedentary outcomes was analyzed according to the number of levels targeted by the intervention, based on the socio-ecological model level stratification (see Figure 2). A trial was considered as effective when the study reported a significant impact of intervention on a sedentary measure at post- vs. pre-intervention; if several sedentary measures were reported and at least one showed a significant decrease of ST, the study was classified as effective.
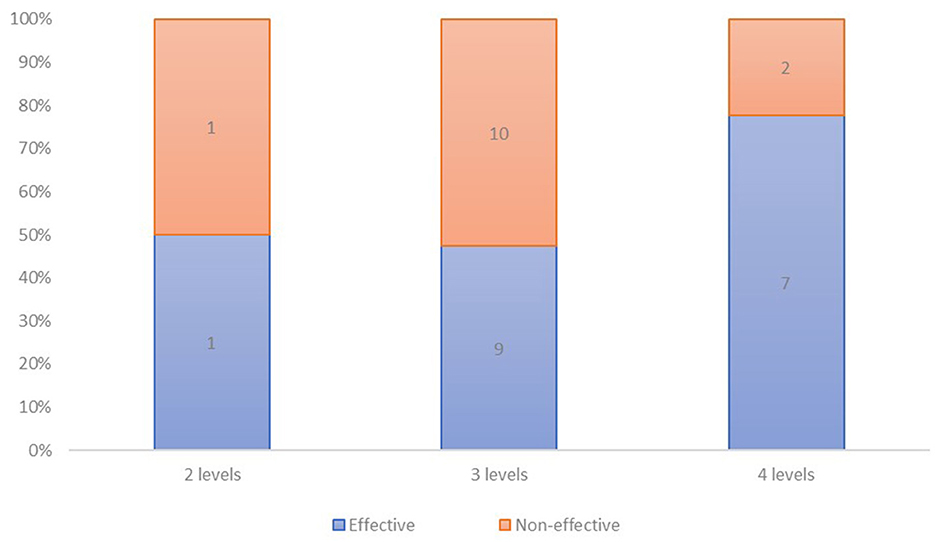
Figure 2. Number of interventions respectively reporting effectiveness and non-effectiveness on sedentary outcome, according to the number of levels targeted.
As shown in the Figure 2, 1 (50%) of studies targeting 2 levels, 9 (47%) that targeted 3 levels and 7 (78%) trials that targeted 4 levels of intervention, were effective in reducing ST-SB.
Table 3 summarizes, for each trial, the effectiveness according to the number and type of levels targeted and to the methodological quality score.
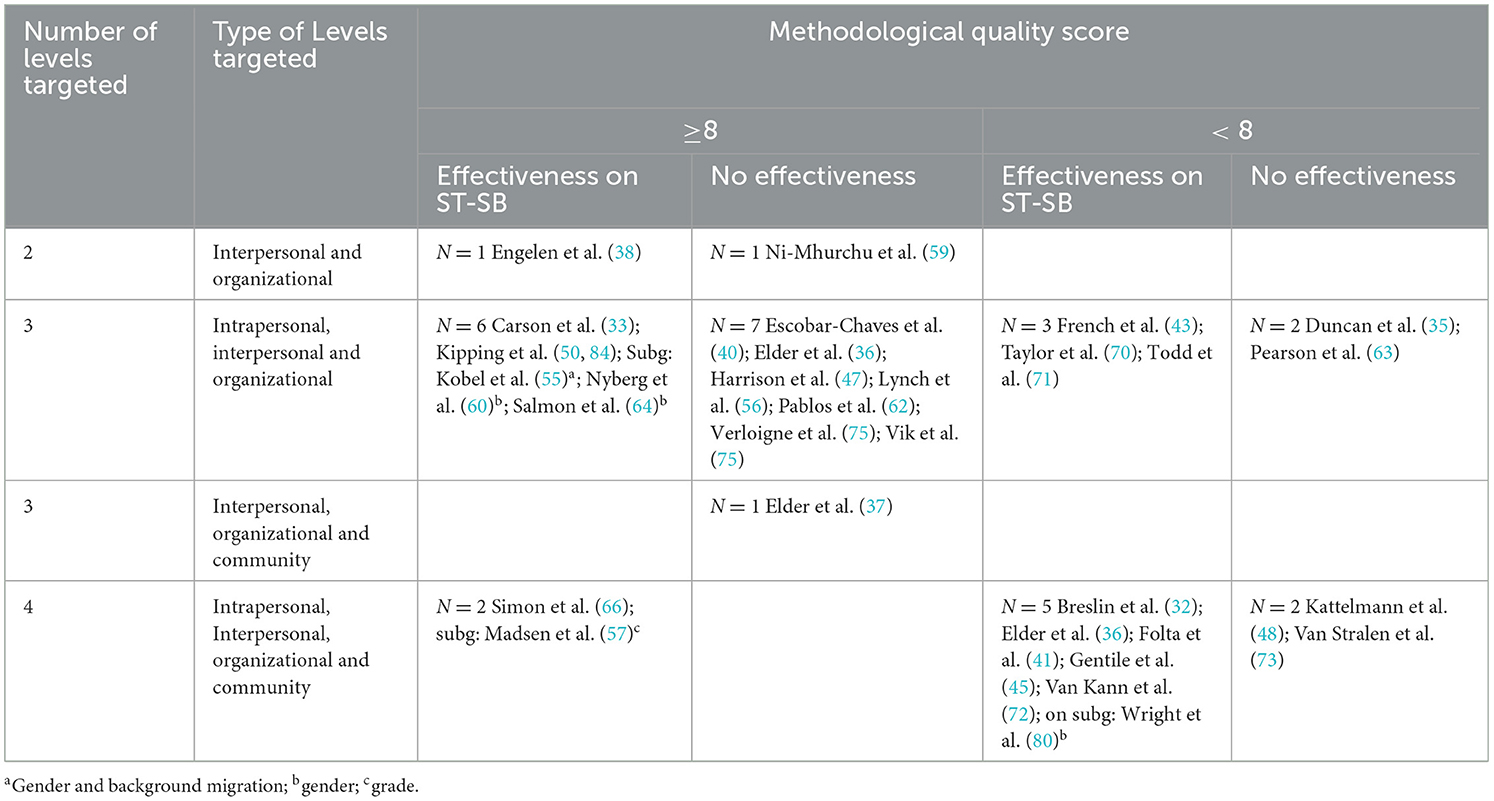
Table 3. Effectiveness on ST-SB of trials according to methodological quality score, number and type of interventional levels targeted (as defined by the socio-ecological model).
As presented in Table 2, among the trials that used a 2-levels based intervention, all (N = 2, 100%) having high methodological quality, 1 (50%) was effective in reducing ST-SB. Among the high (N = 14) and the acceptable (N = 5) quality studies of the 3-levels trials, 6 (43%) and 3 (60%) were effective, respectively. Lastly, among the 2 high-quality and the 7 lower quality score interventions that used a four-level strategy, 2 (100%), and 5 (71%) were effective, respectively.
Regarding high quality studies, 9 (50%) reported effectiveness on ST-SB, and among those, 1 included 2-level, 6 involved 3-level, and 2 presented 4-level based interventions. Regarding lower quality studies, 8 (67%) reported effectiveness on ST-SB, and among those, none included 2-level, 3 involved 3-level, and 5 presented 4-level based interventions.
The second aim of our review was to consider the involvement, and the degree of involvement of caregivers or social support close to the child (involvement is reported in Table 2). Involvement was considered as strong when the stakeholder had an active role (e.g., a teacher-lead intervention during school class), and weak when only passive (e.g., parent receiving a newsletter with information about ST). Among the 22 studies targeting parents as social support with a strong or active involvement, 10 (45%) were effective in reducing ST-SB; among the 5 studies that targeted parents with a more passive strategy, 4 (80%) have reported effectiveness; in 3 of these trials, teachers, community members and recreational centers directors were also, and strongly, involved. Above the 30 included interventions, implication of parents is often associated with an involvement of educational stakeholders (e.g., teachers, educators in health promotion, educational staff, recreational directors, nurses). Among the 17 effective trials that considered social support as an intervention strategy, 2 (12%) involved parents only; 3 (18%) involved educational stakeholders only and 11 (70%) involved both parents and caregivers from the educational environment, one involving parents and community stakeholders.
Finally, among the 21 studies involving educational stakeholders (e.g., teachers, educators in health promotion, educational staff, recreational directors, nurses) with a strong or active involvement, 13 (62%) were effective in reducing ST-SB; among the 5 studies that included weaker involvement of educational stakeholders, 1 (20%) has reported effectiveness.
Discussion
An important part of the scientific literature states that health behaviors linked with SB are influenced by intrapersonal factors, but also interpersonal and environmental determinants (11, 16, 17). Consequently, socio-ecological models and structural perspectives are drawing the attention of researchers (10, 13, 87). On a practical level, the combination of agentic and structural approach is operationalized by multi-level interventions that target multiple determinants, and use strategies at several levels of influence.
The purpose of this systematic review of the literature was to study and critically summarize controlled multilevel trials (i.e., targeting at least two levels of intervention) aiming to reduce SB (e.g., specific SB as TV-viewing, general ST), as primary or secondary outcome (e.g., it could first targeted PA) in young populations (children, from 5 to 12 years-old), and evaluate their effectiveness in relation to the number and the type of levels targeted (i.e., intrapersonal, interpersonal, organizational, and community), the methodological quality and the strategies (e.g., informational, behavioral, involving family and teachers) used in each level. To our knowledge, this is the first review that targets multilevel interventions specifically aiming for sedentary outcomes.
Main findings
Final review included 30 controlled studies (most of them were published in the last decade) that involve 2, 19, and 9 interventions targeting 2, 3, and 4 different levels, respectively. Most of the included studies showed a high methodological quality score. However, in line with previous findings (22, 23, 30), the characteristics of included studies were heterogeneous, regarding the duration of the intervention (pilot studies had a shorter duration), population characteristics (e.g., size, age range, socioeconomic profile), settings (e.g., home, recreational center, school), assessment methods of ST-SB (i.e., subjective, objective, a combination of both measures), interventional strategies raised, leading to a difficulty to draw clear conclusions regarding the strategies and components that could preferentially reduce ST in children. Very few studies targeted 2 levels of intervention, also resulting in difficulty to make strong conclusions and to allow meaningful comparisons between 2-levels trials and other multilevel (i.e., 3- and 4-levels) studies. Most of the included multi-level interventions targeted 3 levels, mainly intrapersonal factors, interpersonal or social support level and organizational level (e.g., school, home). As young populations usually spend most of their time at school, this institution is a critical and major setting of interventions. Some interventions involved the community level, but none included study has achieved to target the society level (macro-environment).
Regarding effectiveness to reduce SB in children, effectiveness was reported in 1 (50%), 9 (47%) and 7 (78%) interventions targeting 2, 3, and 4 levels, respectively. Results suggest that interventions could be more often effective when the strategies used are deployed along 4 levels. However, only two studies used a 2-level strategy, providing insufficient evidence to rigorously conclude, and more than 70% of the 3-level studies have a high quality, whereas the majority of 4-level trials (78%) has an acceptable methodological quality.
This review secondly aimed to consider the involvement of caregivers in the effectiveness of trials. Again, the low number of trials and the heterogeneity of the interventions does not allow to drive specific and clear conclusions and, therefore, to answer this question. However, it seems that an involvement of caregivers (parents but also educational stakeholders, teachers in particular) could be a relevant strategy, targeting the entire social support of children. This design is based on the assumption that having a supportive family environment can promote the targeted behavior change and be effective in reducing children's ST. In this study, results show that among effective trials that considered social support as an intervention strategy, most of them (70%) involved both parents and educational caregiver or community members and among the studies strongly involving educational stakeholders, 62% were effective in reducing ST-SB.
Results ultimately suggest that the key ingredients of a successful intervention may involve a combination of several components: (i) at the intrapersonal level, both behavioral (e.g., setting screen-time goals) and informational strategies (e.g., often in the regular curriculum of the child), (ii) at the interpersonal level, a supportive and highly involved social circle by including teachers and parents, (iii) at the organizational level, targeting several child's environments (school and home) and (iv) at a community level including stakeholders (e.g., partnership with local sport clubs, local municipalities).
Limitations and perspectives
Limitations of this work could be mentioned. First of all, a meta-analysis would have led to strongest conclusion. However, as previously raised, trials of very different nature met the inclusion criteria and were included and reviewed. Given the large heterogeneity in study design and intervention's characteristics, strong and relevant comparisons and analyses were difficult and it appeared that a meta-analysis was not relevant. This work also raised some methodological issues. The systemic approach proposed by the socio-ecological model is promising (10, 13), but also intimidating, integrating and conceptualizing different levels of the environment. Therefore, a challenge still remains in the operationalization of this model, such that socio-ecological is not a “buzzword” in public health (19), and in finding the methods for assessing the degree of integration of the socio-ecological model into research (87–89).
Future studies should analyze the impact of their intervention on ST-SB by specifying the type of SB (e.g., time spent reading, watching TV) and context (e.g., location or social situation). It is highly unlikely that a reduction in a specific SB will be directly replaced with PA; actually, it has a greater chance to be allocated to other SB (21, 22, 90).
When subjective assessments are used, different types of SB should be taken into account and lead to a comparison between different distinct behaviors (e.g., computer time vs. screen time) targeted by interventions (22). Domain-specific SB should be identified, with, as suggested by Owen et al. (13), a consideration of passive (e.g., TV viewing) vs. mentally active (e.g., reading, computer use) SB. Future trials should target other types of sedentary behavior, including non-screen-based measures, and consider the recent technological changes (3), given that this last decade, the use of small screens, as smartphones and tablets, is increasing in children.
In addition to the identification of domain-specific SB, there is a growing need to operationalize the distinction between passive (e.g., TV viewing) vs. mentally active (e.g., reading, computer use) SB (13). Moreover, the challenge of school-based interventions, even when they include home activities or home components in their strategies, is to reduce ST both at school and out of school. Another perspective thus concerns the need to interrupt ST during the whole day, as pointed out in the literature (30, 91, 92) and in the latest worldwide guidelines (5).
Targeting intrinsic levers in intervention strategies is important as only focusing on the environment of the child is not enough, considering that young people tend to select sedentary activities, even when physically active alternatives are available (22, 90, 93). On the other hand, targeting intrapersonal determinants to the detriment of the broader environment and of structural and political changes is an incomplete strategy. Future studies should use ecologic approach -e.g., targeting norms, physical components-, with a strong and active involvement of caregivers (social support) in the various environments (e.g., school staff, parents at home) of the child, in addition to curriculum or behavioral punctual strategies. Multilevel or socio-ecologic interventions should involve community level and the broader environment, as none included study has achieved to target the society level.
Conclusion
A paradigmatic shift is occurring in the literature, and interventions targeting health behaviors are more and more multi-level or socio-ecological based. To our knowledge, no study had systematically reviewed and assessed the effectiveness of multilevel controlled trials targeting ST-SB in young (5–12 years) populations. Our findings show that more than half of the included interventions based on socioecological model (i.e., multilevel) have reported effectiveness of children SB. Indeed, among included studies, effectiveness on children SB was reported in 50%, 47%, and 78% interventions targeting 2, 3, and 4 levels, respectively. Therefore, results suggest that interventions could be more often effective when the strategies used are deployed along 4 levels. In addition, it seems that targeting four different levels i.e., intrapersonal, interpersonal, organizational and community, tend to led to more successful interventions to reduce SB.
This review highlights the need for additional randomized controlled trials evaluating multilevel interventions targeting ST-SB in young populations. More studies designing and implementing multilevel interventions are needed to “address the gap between theory and practice” (19) and remove operational and empirical hurdles. In addition, more reviews and meta-analyses are required to clearly assess their effectiveness and the key strategies underlying their effectiveness. Also, a theoretical and methodological reflection to quantify the degree of integration of the socioecological model in studies has to be continued to correctly evaluate the socio-ecological perspective.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
MC-G selected eligible studies and assessed the inclusion criteria to determine preliminary eligibility of studies based on the title and/or the abstract. Following the PRISMA guidelines, MC-G applied the PICOS method to check if the data fit the following inclusion criteria. MC-G and MC separately read the full text, using the inclusion PICOS criteria to assess the final inclusion of articles. Any discrepancies were discussed until consensus was reached. MC-G and SL extracted relevant data including methodology, participants, outcomes, and results. CD brought his expertise to this work and ensured the overall review of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the French Institut National du Cancer (INCa project grant PREV19-021, INCA_14185).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Tremblay MS, Aubert S, Barnes JD, Saunders TJ, Carson V, Latimer-Cheung AE, et al. Sedentary behavior research network (SBRN) - terminology consensus project process and outcome. J Nutr Educ Behav. (2017) 14:75. doi: 10.1186/s12966-017-0525-8
2. He M, Piché L, Beynon C, Harris S. Screen-related sedentary behaviors: children's and parents' attitudes, motivations, and practices. J Nutr Educ Behav. (2010) 42:17–25. doi: 10.1016/j.jneb.2008.11.011
3. Tremblay MS, LeBlanc AG, Kho ME, Saunders TJ, Larouche R, Colley RC, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. J Nutr Educ Behav. (2011) 8:98. doi: 10.1186/1479-5868-8-98
4. Carson V, Hunter S, Kuzik N, Gray CE, Poitras VJ, Chaput JP, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Appl Physiol Nutr Metab. (2016) 41:S240–265. doi: 10.1139/apnm-2015-0630
5. Chaput JP, Willumsen J, Bull F, Chou R, Ekelund U, Firth J, et al. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5-17 years: summary of the evidence. Int J Behav Nutr Phys Act. (2020) 17:141. doi: 10.1186/s12966-020-01037-z
6. López-Fernández J, Lopez-Valenciano A, Mayo X, Liguori G, Lamb M, Copeland R, et al. No changes in adolescent's sedentary behaviour across Europe between 2002 and (2017). BMC Public Health. (2021) 21:3. doi: 10.1186/s12889-021-10860-3
7. Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolescent Health. (2020) 4:23–35. doi: 10.1016/S2352-4642(19)30323-2
8. Balicco A, Oleko A, Szego E, Boschat L, Deschamps V, Saoudi A, et al. Protocole Esteban : une Étude transversale de santé sur l'environnement, la biosurveillance, l'activité physique et la nutrition (2014–2016). Toxicologie Analytique et Clinique. (2017) 29:517–37. doi: 10.1016/j.toxac.2017.06.003
9. Dubuisson C, Dufour A, Carrillo S, Drouillet-Pinard P, Havard S, Volatier JL. The Third French Individual and National Food Consumption (INCA3) Survey 2014-2015: method, design and participation rate in the framework of a European harmonization process. Public Health Nutr. (2019) 22:584–600. doi: 10.1017/S1368980018002896
10. Richard L, Gauvin L, Raine K. Ecological models revisited: their uses and evolution in health promotion over two decades. Annu Rev Public Health. (2011) 32:307–26. doi: 10.1146/annurev-publhealth-031210-101141
11. Simon C, Kellou N, Dugas J, Platat C, Copin N, Schweitzer B, et al. A socio-ecological approach promoting physical activity and limiting sedentary behavior in adolescence showed weight benefits maintained 2.5 years after intervention cessation. Int J Obesity. (2014) 38:936–43. doi: 10.1038/ijo.2014.23
12. Sallis JF, Owen N. Ecological models of health behavior. In: Health Behavior: Theory, Research, and Practice, 5th ed. Hoboken, NJ, US: Jossey-Bass/Wiley. (2015) p. 43–64.
13. Owen N, Healy GN, Dempsey PC, Salmon J, Timperio A, Clark BK, et al. Sedentary behavior and public health: integrating the evidence and identifying potential solutions. Annu Rev Public Health. (2020) 41:265–87. doi: 10.1146/annurev-publhealth-040119-094201
14. Hu D, Zhou S, Crowley-McHattan ZJ, Liu Z. Factors that influence participation in physical activity in school-aged children and adolescents: a systematic review from the social ecological model perspective. Int J Environ Res Public Health 18 mars. (2021) 18:3147. doi: 10.3390/ijerph18063147
15. McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Q. (1988) 15:351–77. doi: 10.1177/109019818801500401
16. Wiltshire G, Lee J, Williams O. Understanding the reproduction of health inequalities: physical activity, social class and Bourdieu's habitus. Sport Educ Soc. (2019) 24:226–40. doi: 10.1080/13573322.2017.1367657
17. Sallis JF, Owen N, Fisher EB. Ecological models of health behavior. In: Health Behavior and Health Education: Theory Research and Practice 4th, ed. San Francisco, CA, US: Jossey-Bass. (2008) p. 465–85.
18. Lieberman L, Golden SD, Earp JAL. Structural approaches to health promotion: what do we need to know about policy and environmental change? Health Educ Behav. (2013) 40:520–5. doi: 10.1177/1090198113503342
19. Schölmerich VLN, Kawachi I. Translating the socio-ecological perspective into multilevel interventions: gaps between theory and practice. Health Educ Behav. (2016) 43:17–20. doi: 10.1177/1090198115605309
20. Bernal CMM, Lhuisset L, Fabre N, Bois J. Promotion de l'activité physique à l'école primaire : évaluation de l'efficacité des interventions uni-leviers et multi-leviers. Mov Sport Sci/Sci Mot. (2020) 110:49–78. doi: 10.1051/sm/2020022
21. Biddle SJ, O'Connell S, Braithwaite RE. Sedentary behaviour interventions in young people: a meta-analysis. Br J Sports Med. (2011) 45:937–42. doi: 10.1136/bjsports-2011-090205
22. Biddle SJH, Petrolini I, Pearson N. Interventions designed to reduce sedentary behaviours in young people: a review of reviews. Br J Sports Med. (2014) 48:182–6. doi: 10.1136/bjsports-2013-093078
23. Altenburg TM. Kist-van Holthe J, Chinapaw MJM. Effectiveness of intervention strategies exclusively targeting reductions in children's sedentary time: a systematic review of the literature. Int J Behav Nutr Phys Act. (2016) 13:65. doi: 10.1186/s12966-016-0387-5
24. Marsh S, Foley LS, Wilks DC, Maddison R. Family-based interventions for reducing sedentary time in youth: a systematic review of randomized controlled trials. Obes Rev. (2014) 15:117–33. doi: 10.1111/obr.12105
25. dos Santos PC, Barbosa Filho VC, da Silva JA, Bandeira A da S, Minatto G, da Silva KS. What works in sedentary behavior interventions for youth: a review of reviews. Adolescent Res Rev. (2019) 4:267–92. doi: 10.1007/s40894-018-0105-4
26. Morton KL, Atkin AJ, Corder K, Suhrcke M, van Sluijs EMF. The school environment and adolescent physical activity and sedentary behaviour: a mixed-studies systematic review. Obes Rev. (2016) 17:142–58. doi: 10.1111/obr.12352
27. Hegarty LM, Mair JL, Kirby K, Murtagh E, Murphy MH. School-based interventions to reduce sedentary behaviour in children: a systematic review. AIMS Public Health. (2016) 3:520–41. doi: 10.3934/publichealth.2016.3.520
28. Blackburn NE, Wilson JJ, McMullan II, Caserotti P, Giné-Garriga M, Wirth K, et al. The effectiveness and complexity of interventions targeting sedentary behaviour across the lifespan: a systematic review and meta-analysis. Int J Behav Nutr Phys Act déc. (2020) 17:53. doi: 10.1186/s12966-020-00957-0
29. Mehtälä MAK, Sääkslahti AK, Inkinen ME, Poskiparta MEH, A. socio-ecological approach to physical activity interventions in childcare: a systematic review. Int J Behav Nutr Phys Act. (2014) 11:22. doi: 10.1186/1479-5868-11-22
30. Kellou N, Sandalinas F, Copin N, Simon C. Prevention of unhealthy weight in children by promoting physical activity using a socio-ecological approach: what can we learn from intervention studies? Diabetes Metab. (2014) 40:258–71. doi: 10.1016/j.diabet.2014.01.002
31. Arundell L, Parker K, Timperio A, Salmon J, Veitch J. Home-based screen time behaviors amongst youth and their parents: familial typologies and their modifiable correlates. BMC Public Health. (2020) 20:1492. doi: 10.1186/s12889-020-09581-w
32. Breslin G, Brennan D, Rafferty R, Gallagher AM, Hanna D. The effect of a healthy lifestyle programme on 8–9 year olds from social disadvantage. Arch Dis Child. (2012) 97:618–24. doi: 10.1136/archdischild-2011-301108
33. Carson V, Salmon J, Arundell L, Ridgers ND, Cerin E, Brown H, et al. Examination of mid-intervention mediating effects on objectively assessed sedentary time among children in the Transform-Us! cluster-randomized controlled trial. Int J Behav Nutr Phys Act déc. (2013) 10:62. doi: 10.1186/1479-5868-10-62
34. Salmon J, Arundell L, Hume C, Brown H, Hesketh K, Dunstan DW, et al. A cluster-randomized controlled trial to reduce sedentary behavior and promote physical activity and health of 8-9 year olds: the transform-Us! study. BMC Public Health. (2011) 11:759. doi: 10.1186/1471-2458-11-759
35. Duncan S, McPhee JC, Schluter PJ, Zinn C, Smith R, Schofield G. Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study. Int J Behav Nutr Phys Act. (2011) 8:127. doi: 10.1186/1479-5868-8-127
36. Elder JP, McKenzie TL, Arredondo EM, Crespo NC, Ayala GX. Effects of a multi-pronged intervention on children's activity levels at recess: the aventuras para niños study. Adv Nutr. (2011) 2:171S−176S. doi: 10.3945/an.111.000380
37. Elder JP, Crespo NC, Corder K, Ayala GX, Slymen DJ, Lopez NV, et al. Childhood obesity prevention and control in city recreation centres and family homes: the MOVE/me Muevo project. Pediatric Obesity. (2014) 9:218–31. doi: 10.1111/j.2047-6310.2013.00164.x
38. Engelen L, Bundy AC, Naughton G, Simpson JM, Bauman A, Ragen J, et al. Increasing physical activity in young primary school children—it's child's play: A cluster randomised controlled trial. Prev Med. (2013) 56:319–25. doi: 10.1016/j.ypmed.2013.02.007
39. Bundy AC, Naughton G, Tranter P, Wyver S, Baur L, Schiller W, et al. The Sydney playground project: popping the bubblewrap–unleashing the power of play: a cluster randomized controlled trial of a primary school playground-based intervention aiming to increase children's physical activity and social skills. BMC Public Health. (2011) 11:680. doi: 10.1186/1471-2458-11-680
40. Escobar-Chaves SL, Markham CM, Addy RC, Greisinger A, Murray NG, Brehm B. The fun families study: intervention to reduce children's TV viewing. Obesity. (2010) 18:S99–101. doi: 10.1038/oby.2009.438
41. Folta SC, Kuder JF, Goldberg JP, Hyatt RR, Must A, Naumova EN, et al. Changes in diet and physical activity resulting from the Shape Up Somerville community intervention. BMC Pediatr. (2013) 13:157. doi: 10.1186/1471-2431-13-157
42. Economos CD, Hyatt RR, Goldberg JP, Must A, Naumova EN, Collins JJ, et al. A community intervention reduces BMI z-score in children: Shape Up Somerville first year results. Obesity (Silver Spring). (2007) 15:1325–36. doi: 10.1038/oby.2007.155
43. French SA, Sherwood NE, JaKa MM, Haapala JL, Ebbeling CB, Ludwig DS. Physical changes in the home environment to reduce television viewing and sugar-sweetened beverage consumption among 5- to 12-year-old children: a randomized pilot study: Home decrease TV and SSBs. Pediatric Obes. (2016) 11:e12–5. doi: 10.1111/ijpo.12067
44. French SA, Sherwood NE, Veblen-Mortenson S, Crain AL, JaKa MM, Mitchell NR, et al. Multicomponent obesity prevention intervention in low-income preschoolers: primary and subgroup analyses of the NET-works randomized clinical trial, 2012-2017. Am J Public Health. (2018) 108:1695–706. doi: 10.2105/AJPH.2018.304696
45. Gentile DA, Welk G, Eisenmann JC, Reimer RA, Walsh DA, Russell DW, et al. Evaluation of a multiple ecological level child obesity prevention program: Switch®what you do, view, and chew. BMC Med. (2009) 7:49. doi: 10.1186/1741-7015-7-49
46. Eisenmann JC, Gentile DA, Welk GJ, Callahan R, Strickland S, Walsh M, et al. SWITCH: rationale, design, and implementation of a community, school, and family-based intervention to modify behaviors related to childhood obesity. BMC Public Health. (2008) 8:223. doi: 10.1186/1471-2458-8-223
47. Harrison M, Burns CF, McGuinness M, Heslin J, Murphy NM. Influence of a health education intervention on physical activity and screen time in primary school children: ‘Switch Off–Get Active'. J Sci Med Sport. (2006) 9:388–94. doi: 10.1016/j.jsams.2006.06.012
48. Kattelmann KK, Meendering JR, Hofer EJ, Merfeld CM, Olfert MD, Hagedorn RL, et al. The iCook 4-H study: report on physical activity and sedentary time in youth participating in a multicomponent program promoting family cooking, eating, and playing together. J Nutr Educ Behav. mars (2019) 51:S30–40. doi: 10.1016/j.jneb.2018.09.002
49. Franzen-Castle L, Colby SE, Kattelmann KK, Olfert MD, Mathews DR, Yerxa K, et al. Development of the iCook 4-H curriculum for youth and adults: cooking, eating, and playing together for childhood obesity prevention. J Nutr Educ Behav. (2019) 51:S60–8. doi: 10.1016/j.jneb.2018.11.006
50. Kipping RR, Howe LD, Jago R, Campbell R, Wells S, Chittleborough CR, et al. Effect of intervention aimed at increasing physical activity, reducing sedentary behaviour, and increasing fruit and vegetable consumption in children: active for Life Year 5 (AFLY5) school based cluster randomised controlled trial. BMJ. (2014) 348:g3256–g3256. doi: 10.1136/bmj.g3256
51. Lawlor DA, Jago R, Noble SM, Chittleborough CR, Campbell R, Mytton J, et al. The active for life year 5 (AFLY5) school based cluster randomised controlled trial: study protocol for a randomized controlled trial. Trials. (2011) 12:181. doi: 10.1186/1745-6215-12-181
52. Lawlor DA, Peters TJ, Howe LD, Noble SM, Kipping RR, Jago R. The active for life year 5 (AFLY5) school-based cluster randomised controlled trial protocol: detailed statistical analysis plan. Trials. (2013) 14:234. doi: 10.1186/1745-6215-14-234
53. Dreyhaupt J, Koch B, Wirt T, Schreiber A, Brandstetter S, Kesztyüs D, et al. Evaluation of a health promotion program in children: Study protocol and design of the cluster-randomized Baden-Württemberg primary school study [DRKS-ID: DRKS00000494]. BMC Public Health. (2012) 12:157. doi: 10.1186/1471-2458-12-157
54. Anderson EL, Howe LD, Kipping RR, Campbell R, Jago R, Noble SM, et al. Long-term effects of the Active for Life Year 5 (AFLY5) school-based cluster-randomised controlled trial. BMJ Open. (2016) 6:e010957. doi: 10.1136/bmjopen-2015-010957
55. Kobel S, Wirt T, Schreiber A, Kesztyüs D, Kettner S, Erkelenz N, et al. Intervention effects of a school-based health promotion programme on obesity related behavioural outcomes. J Obesity. (2014) 2014:1–8. doi: 10.1155/2014/476230
56. Lynch BA, Gentile N, Maxson J, Quigg S, Swenson L, Kaufman T. Elementary school–based obesity intervention using an educational curriculum. J Prim Care Community Health. (2016) 7:265–71. doi: 10.1177/2150131916644888
57. Madsen K, Linchey J, Gerstein D, Ross M, Myers E, Brown K, et al. Energy balance 4 kids with play: results from a two-year cluster-randomized trial. Childhood Obes. (2015) 11:375–83. doi: 10.1089/chi.2015.0002
58. Myers EF, Gerstein DE, Foster J, Ross M, Brown K, Kennedy E, et al. Energy balance for kids with play: design and implementation of a multi-component school-based obesity prevention program. Child Obes. (2014) 10:251–9. doi: 10.1089/chi.2013.0075
59. Ni Mhurchu C, Roberts V, Maddison R, Dorey E, Jiang Y, Jull A, et al. Effect of electronic time monitors on children's television watching: Pilot trial of a home-based intervention. Prevent Med. (2009) 49:413–7. doi: 10.1016/j.ypmed.2009.09.003
60. Nyberg G, Sundblom E, Norman Å, Bohman B, Hagberg J, Elinder LS. Effectiveness of a universal parental support programme to promote healthy dietary habits and physical activity and to prevent overweight and obesity in 6-year-old children: the healthy school start study, a cluster-randomised controlled trial. PLoS ONE. (2015) 10:e0116876. doi: 10.1371/journal.pone.0116876
61. Nyberg G, Ekblom O, Marcus C. A 4-year cluster-randomised controlled intervention study on physical activity pattern and sedentary behaviour in children. Med Sci Sports. (2011) 43:24. doi: 10.1249/01.MSS.0000402741.12322.4e
62. Pablos A, Nebot V, Vañó-Vicent V, Ceca D, Elvira L. Effectiveness of a school-based program focusing on diet and health habits taught through physical exercise. Appl Physiol Nutr Metab. (2018) 43:331–7. doi: 10.1139/apnm-2017-0348
63. Pearson N, Biddle SJH, Griffiths P, Sherar LB, McGeorge S, Haycraft E. Reducing screen-time and unhealthy snacking in 9–11 year old children: the Kids FIRST pilot randomised controlled trial. BMC Public Health. (2020) 20:122. doi: 10.1186/s12889-020-8232-9
64. Salmon J, Jorna M, Hume C, Arundell L, Chahine N, Tienstra M, et al. A translational research intervention to reduce screen behaviours and promote physical activity among children: Switch-2-Activity. Health Promotion Int. (2011) 26:311.21.
65. Salmon J, Ball K, Hume C, Booth M, Crawford D. Outcomes of a group-randomized trial to prevent excess weight gain, reduce screen behaviours and promote physical activity in 10-year-old children: switch-play. Int J Obes (Lond). (2008) 32:601–12. doi: 10.1038/sj.ijo.0803805
66. Simon C, Schweitzer B, Triby E, Hausser F, Copin N, Kellou N, et al. Promouvoir l'activité physique, lutter contre la sédentarité et prévenir le surpoids chez l'adolescent, c'est possible : les leçons d'ICAPS. Cahiers de Nutrition et de Diététique. (2011) 46:130–6. doi: 10.1016/j.cnd.2011.03.003
67. Simon C, Schweitzer B, Oujaa M, Wagner A, Arveiler D, Triby E, et al. Successful overweight prevention in adolescents by increasing physical activity: a 4-year randomized controlled intervention. Int J Obes (Lond). (2008) 32:1489–98. doi: 10.1038/ijo.2008.99
68. Simon C, Wagner A, DiVita C, Rauscher E, Klein-Platat C, Arveiler D, et al. Intervention centred on adolescents' physical activity and sedentary behaviour (ICAPS): concept and 6-month results. Int J Obes Relat Metab Disord. (2004) 28:S96–103. doi: 10.1038/sj.ijo.0802812
69. Simon C, Wagner A, Platat C, Arveiler D, Schweitzer B, Schlienger JL, et al. ICAPS: a multilevel program to improve physical activity in adolescents. Diabetes Metab. (2006) 32:41–9. doi: 10.1016/S1262-3636(07)70245-8
70. Taylor S, Noonan R, Knowles Z, Owen M, McGrane B, Curry W, et al. Evaluation of a pilot school-based physical activity clustered randomised controlled trial—active schools: Skelmersdale. IJERPH. (2018) 15:1011. doi: 10.3390/ijerph15051011
71. Todd MK, Reis-Bergan MJ, Sidman CL, Flohr JA, Jameson-Walker K, Spicer-Bartolau T, et al. Effect of a family-based intervention on electronic media use and body composition among boys aged 8-−11 years: a pilot study. J Child Health Care. (2008) 12:344–58. doi: 10.1177/1367493508097404
72. Van Kann DHH, de Vries SI, Schipperijn J, de Vries NK, Jansen MWJ, Kremers SPJ. A multicomponent schoolyard intervention targeting children's recess physical activity and sedentary behavior: effects after one year. J Phys Act Health. (2016) 1–28. doi: 10.1123/jpah.2015-0702
73. van Stralen MM, de Meij J, te Velde SJ, van der Wal MF, van Mechelen W, Knol DL, et al. Mediators of the effect of the JUMP-in intervention on physical activity and sedentary behavior in Dutch primary schoolchildren from disadvantaged neighborhoods. Int J Behav Nutr Phys Act. (2012) 9:131. doi: 10.1186/1479-5868-9-131
74. De Meij JSB, Chinapaw MJM, Kremers SPJ, Van der Wal MF, Jurg ME, Van Mechelen W. Promoting physical activity in children: The stepwise development of the primary school-based JUMP-in intervention applying the RE-AIM evaluation framework. Br J Sports Med. (2010) 44:879–87. doi: 10.1136/bjsm.2008.053827
75. Verloigne M, Bere E, Van Lippevelde W, Maes L, Lien N, Vik FN, et al. The effect of the UP4FUN pilot intervention on objectively measured sedentary time and physical activity in 10–12 year old children in Belgium: the ENERGY-project. BMC Public Health. (2012) 12:805. doi: 10.1186/1471-2458-12-805
76. Verloigne M, Berntsen S, Ridgers ND, Cardon G, Chinapaw M, Altenburg T, et al. The UP4FUN intervention effect on breaking up sedentary time in 10- to 12-year-old belgian children: the ENERGY-project. Pediatr Exerc Sci. (2015) 27:234–42. doi: 10.1123/pes.2014-0039
77. Verloigne M, Ridgers ND, De Bourdeaudhuij I, Cardon G. Effect and process evaluation of implementing standing desks in primary and secondary schools in Belgium: a cluster-randomised controlled trial. Int J Behav Nutr Phys Act. (2018) 15:94. doi: 10.1186/s12966-018-0726-9
78. Van Lippevelde W, Bere E, Verloigne M, van Stralen MM, De Bourdeaudhuij I, Lien N, et al. The role of family-related factors in the effects of the UP4FUN school-based family-focused intervention targeting screen time in 10- to 12-year-old children: the ENERGY project. BMC Public Health. (2014) 14:857. doi: 10.1186/1471-2458-14-857
79. Vik FN, Lien N, Berntsen S, De Bourdeaudhuij I, Grillenberger M, Manios Y, et al. Evaluation of the UP4FUN intervention: a cluster randomized trial to reduce and break up sitting time in european 10-12-year-old children. PLoS ONE. (2015) 10:e0122612. doi: 10.1371/journal.pone.0122612
80. Wright K, Giger JN, Norris K, Suro Z. Impact of a nurse-directed, coordinated school health program to enhance physical activity behaviors and reduce body mass index among minority children: a parallel-group, randomized control trial. Int J Nurs Studies. (2013) 50:727–37. doi: 10.1016/j.ijnurstu.2012.09.004
81. Higgins JPT, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d5928–d5928. doi: 10.1136/bmj.d5928
82. Gourlan M, Bernard P, Bortolon C, Romain AJ, Lareyre O, Carayol M, et al. Efficacy of theory-based interventions to promote physical activity. A meta-analysis of randomised controlled trials. Health Psychol Rev. (2016) 10:50–66. doi: 10.1080/17437199.2014.981777
83. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
84. Kipping RR, Payne C, Lawlor DA. Randomised controlled trial adapting US school obesity prevention to England. Arch Dis Childhood. (2008) 93:469–73. doi: 10.1136/adc.2007.116970
85. Bandura A. Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ, US: Prentice-Hall, Inc. (1986).
86. Ryan RM, Deci EL. Self-determination theory and the role of basic psychological needs in personality and the organization of behavior. In: Handbook of personality: Theory and research, 3rd ed. New York, NY, US: The Guilford Press; (2008) p. 654–78.
87. Golden SD, Earp JAL. Social ecological approaches to individuals and their contexts: twenty years of health education and behavior health promotion interventions. Health Educ Behav. (2012) 39:364–72. doi: 10.1177/1090198111418634
88. Krieger N. Theories for social epidemiology in the 21st century: an ecosocial perspective. Int J Epidemiol. (2001) 30:668–77. doi: 10.1093/ije/30.4.668
89. Richards EL, Riner ME, Sands LP. A Social ecological approach of community efforts to promote physical activity and weight management. J Community Health Nurs. (2008) 25:179–92. doi: 10.1080/07370010802421145
90. Epstein LH, Roemmich JN, Saad FG, Handley EA. The value of sedentary alternatives influences child physical activity choice. Int J Behav Med. (2004) 11:236–42. doi: 10.1207/s15327558ijbm1104_7
91. Paing AC, McMillan KA, Kirk AF, Collier A, Hewitt A, Chastin SFM. The associations of sedentary time and breaks in sedentary time with 24-hour glycaemic control in type 2 diabetes. Prev Med Rep. (2018) 12:94–100. doi: 10.1016/j.pmedr.2018.09.002
92. Thivel D, Tremblay A, Genin PM, Panahi S, Rivière D, Duclos M. Physical activity, inactivity, and sedentary behaviors: definitions and implications in occupational health. Front Public Health. (2018) 6:288. doi: 10.3389/fpubh.2018.00288
Keywords: sedentary, intervention, prevention, socio-ecologic, multilevel
Citation: Cholley-Gomez M, Laujac S, Delpierre C and Carayol M (2023) Effectiveness of multilevel interventions based on socio-ecological model to decrease sedentary time in children: a systematic review of controlled studies. Front. Public Health 11:1106206. doi: 10.3389/fpubh.2023.1106206
Received: 23 November 2022; Accepted: 08 May 2023;
Published: 02 June 2023.
Edited by:
Mirko Brandes, Leibniz Institute for Prevention Research and Epidemiology - BIPS, GermanyReviewed by:
Sitong Chen, Victoria University, AustraliaBirgit Sperlich, Julius Maximilian University of Würzburg, Germany
Copyright © 2023 Cholley-Gomez, Laujac, Delpierre and Carayol. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marie Cholley-Gomez, bWFyaWUuY2hvbGxleWdvbWV6QGhvdG1haWwuZnI=