 Temple Kahilu Mumba1
Temple Kahilu Mumba1 Mark Divall
Mark Divall Kelvin Mwangilwa
Kelvin Mwangilwa
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 20 September 2023
Sec. Public Health Policy
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1103133
Background: Coronavirus disease 2019 (SARS-CoV-2) was declared a global pandemic by WHO after it spreads quickly around the world from its source city in Wuhan. Africa has some of the lowest documented SARS-CoV-2 incidences globally, with over 9 million confirmed cases as of December 2022. This may be due to efficient mitigation, outbreak response, or demographic traits. Surveillance capability may have suffered as nations changed funding, regulations, and testing plans. Therefore, this study was to document the prevalence of SARS-CoV-2, its characteristics, and the socio-economic characteristics in the two mining districts of Solwezi and Kalumbila of Zambia.
Methods: Between 28 March and 26 April 2021, a cross-sectional cluster-sample survey of households in two mining districts of Zambia was conducted. Twenty standard enumeration areas (SEAs) were randomly selected in Kansanshi (17 SEA) and Kalumbila (3 SEA) from a total of 67 SEA that encompass the two mines. Members of households aged <5 years were not eligible to participate in the survey. All participants that consented to participate in the interview were also asked to consent to test for SARS-CoV-2 infection using a rapid diagnostic test (RDT), which tested for recent infection and past exposure to the virus (IgM and IgG, respectively).
Result: Out of the total sample of 3,047 that were present for the interview, 622 of them agreed to test for COVID-19. Of the total that tested for SARS-CoV-2, 2.6% were IgM positive while 9.0% were IgG positive. Despite the above results, 1,586 participants that agreed to the interview indicated a low self-risk assessment of getting COVID-19 (46.5%) or someone (45.5%). On the public health measures, participants who did handwashing more than usual (65.0%), not hand sanitizing more than usual (69.0%), not disinfecting surfaces in their households than usual (87.5%), not avoiding drinking from bars or nightclubs (90.6%), and not wearing a mask when out in public places (71.1%). In the logistic multivariable model, participants with age 24 years and above (AOR = 2.94; 95% CI = 1.10, 7.81) and having experienced symptoms of SARS-CoV-2 (AOR = 2.60; 95% CI: 1.33, 5.05) had a significant effect on testing positive for SARS-CoV-2.
Conclusion: Although the results showed that active COVID-19 prevalence in Solwezi and Kalumbila communities surrounding the two mines was low, exposure to infection was five times high. Government and mining firms should continue to sensitize the community members on the preventive measures of COVID-19 and continue with community testing so that all those positive but without symptoms can self-isolate and those with symptoms and sick can be admitted to the hospital.
SARS-CoV-2 was declared a global pandemic on 11th March 2020 by WHO. On 16th July 2023, the world recorded 767 million positives and 6.9 million deaths. During the same period, Zambia recorded 347,022 cases of COVID-19 with 4,062 deaths (1). The North-Western province was identified as one of the hotspots of the pandemic in Zambia, with 6,073 cases being recorded during the same period. Solwezi and Kalumbila districts contributed 3,076 cases and 854 cases, respectively, to the total number of cases reported in the North-Western province. Further SARS-CoV-2 effects differ significantly across various social, political, and geographic contexts (2).
Early COVID-19 forecasts suggested a sizable morbidity and mortality burden in Africa due to COVID-19. However, with over 9 million verified cases as of December 2022, Africa has some of the lowest known incidences of COVID-19 in the entire world (3). It is yet unknown, though, whether this is due to effective mitigation, outbreak response, or demographic characteristics. As nations altered their funding, national legislation, and testing strategies in response to the COVID-19 pandemic, surveillance capability may have decreased. Currently, Africa has far lower death rates than other regions, which is sometimes attributed, among other things, to the continent's youthful population (4), but in the majority of African countries, community transmission is currently accelerating (5). Although the epidemic is spreading most swiftly in South Africa, where there are the most cases, the bulk of COVID-19-related deaths in Africa have occurred in Egypt. Even if testing and case data in Africa are not as complete as those in other areas of the world, the pandemic's impact on economies and health systems cannot be denied. Aside from Ghana and Nigeria, other countries that have suffered greatly include Algeria, Morocco, and Morocco (6).
The virus was mainly spread between people during close contact, often via small droplets produced by coughing, sneezing, or talking (7). Other people got infected by touching contaminated surfaces and then touching their faces (8). To prevent COVID-19 transmission, the Zambian government, such as most governments around the world, instituted preventive measures such as masking up when in public, social distancing, maintaining personal hygiene by washing hands or hand sanitizing, closing high spreader places, and stopping high spreader events. Other public health measures instituted included the closure of schools and higher learning institutions, restriction of public gatherings, requiring all restaurants to operate only on take away and delivery basis, and closure of all bars, nightclubs, cinemas, gyms, casinos, banks, mines, government and private institutions, schools and universities both private/government, and all international flights to land and depart from Kenneth Kaunda International Airport in Lusaka (9). Zambia is a land-linked country with ten provinces, and all the provinces reported case of COVID-19 by 16th of July 2023. The North-Western province is in the North-Western part of Zambia and has two mining districts (Kalumbila and Solwezi). The measures were also implemented in the two mining districts of Solwezi and Kalumbila in North-Western province of Zambia. Furthermore, supportive interventions were implemented to mitigate the COVID-19 socio-economic and mental health shocks among the miners and their families.
As COVID-19 is a new disease, many knowledge gaps exist on the magnitude of spread among the community members, especially that most of them were asymptomatic (10), its virulence, and infective dosage (11). Questions also remain unanswered surrounding its symptom manifestation, which so far range from mild to severe, particularly, the role of subclinical infections in person-to-person transmission and if persons with subclinical presentation can transmit to other individuals (12). During interventions of public health measures, different health promotion mechanisms were used and it is important to document the most effective methods and if people were adhering to the preventive measures instituted by the government. Mental health effects of COVID-19 on the miners and theirs need to be documented.
A study conducted in July 2020 in Kabwe, Livingstone, Lusaka, Nakonde, Ndola, and Solwezi districts showed a high prevalence of acute SARS-CoV-2 infection in the community but a low prevalence of antibodies among participants, meaning there had been few previous infections (13). However, that study was not representative of the entire country as the six districts were purposefully selected. Additionally, among confirmed cases in Zambia, most have been reported from Lusaka District (Zambia National Public Health Institute, 2020) (13). However, the completed prevalence study from six districts indicated equivalent SARS-CoV-2 burden, suggesting a potential reporting bias resulting from more tests being performed in Lusaka District compared to elsewhere in Zambia. Prevalence surveys that measure the distribution of SARS-CoV-2 in the population are important tools to address this bias from uneven distribution of testing in Zambia, and SARS-CoV-2 prevalence survey will better help assess the extent and nature of a reporting bias (14).
While this is important for policy decision-making, nationally, health and wellness program had an interest in understanding disease transmission in its wider community in Solwezi and Kalumbila to determine the effectiveness of controls and demographic spread in the mining areas. This was to support the evidence for better workplace controls and understanding of behaviors and practices to better inform education and communication programs. Ultimately, First Quantum Minerals (FQM) supported the desire for zero harm for improving health and wellness in its communities. Therefore, this study aims to document the prevalence of COVID-19, its characteristics, and the socio-economic characteristics in the two districts of Solwezi and Kalumbila of Zambia. The benefit of the study was that knowing the determinants of the community burden of COVID-19 would help put up specific interventions aimed at improving service delivery eventually improving the management of COVID-19 in Zambia and future similar outbreaks.
The COVID-19 seroprevalence survey was a cross-sectional study, and a similar method has been used elsewhere (10, 13, 15). In this study, 800 households with an estimated 3,045 persons in communities in the Solwezi and Kalumbila districts of North-Western province were involved.
The COVID-19 prevalence survey included the following populations in Solwezi and Kalumbila districts: the miners and their dependents. The study participants were recruited through the household survey of communities surrounding the mines, with a population of 203,799 in the Solwezi district and 127,604 in the Kalumbila district. A household listing of selected standard enumeration areas (SEAs) was conducted, and 40 households per SEA were randomly selected. All persons in the selected SEA aged >5 years were eligible for the survey, which gave an estimated sample size of 3,200 persons.
A two-stage sampling methodology was used to recruit participants for the household survey.
The primary sampling unit (PSU) was the standard enumeration area (SEA) that was selected using probability proportional to size (PPS) of the SEAs. A total of 20 SEAs were randomly selected from the 2010 Census of Population and Housing sampling frame (16). The sampling frame in the targeted areas of Solwezi and Kalumbila districts has 61 SEA, and it details the estimated total number of households and the estimated population per SEA. Each SEA has a cartographical map that shows the boundaries, which do not overlap, and the main landmarks. In this study, Kamitaka township, Kimalamba, Trident town, Northern Resettlement, Kisasa, Kansanshi golf estate, and Kimasala were the communities considered for enumeration as they are areas where mine workers live with their dependents.
The sampling process began by stratifying areas around the two mines that are Kansanshi in the Solwezi district and Kalumbila in the Kalumbila district into SEAs. The SEAs were further stratified by rural–urban areas. Sampling weights for each SEA were calculated, taking into consideration that each SEA has a different sampling probability of selecting a household. In the second stage of sampling, we used systematic random selection to select a fixed number of 40 households in each selected SEA. Using the household listing software, the survey team listed all households in the selected SEA and randomly selected 40 households. A total of 800 residential households were selected for the survey. In each selected household, all eligible household members (aged ≥ 5 years) who gave consent were interviewed. The target sample was 3,200 persons for the survey.
The following was used as the criteria for recruiting participants in the study: All participants living in the selected households in each selected SEA provide informed consent/assent to participate in the study and consent to drawing blood specimens and/or being swabbed.
All participants who already tested for COVID-19 and had a positive result were excluded.
The field team comprised data collectors and phlebotomists. These data collectors and phlebotomists (blood collectors) were fluent in the local languages (Kaonde, Lunda, and Luvale) and understand the culture of the communities. They were trained in research ethics (17), data collection questionnaire implementation, biosafety, quality assurance, and correct use of PPE and worked under the supervision of a team leader. The phlebotomists were furthermore oriented on the best practice of finger prick and capillary tests. Data collectors and supervisors were trained on how to complete the questionnaire on the tablet. Additionally, the field teams were equipped with Infection Prevention and Control (IPC) and safety handling practices. Data quality was also controlled by close supervision, data cleaning and editing, and cross-checking of the completeness of the questionnaires. The questionnaire was pre-tested in similar settings which were not part of the study area, and the necessary modifications were made on some items of the questionnaire.
On completion of the questionnaire, the participant was referred to the phlebotomist for a finger prick to test for COVID-19 using RDT antigen per standard procedures defined by the manufacturer of the rapid detection kits (Onsite Rapid Test®) (18–20). The samples were analyzed following the manufacturer's instructions with the result recorded on a laboratory form and entered into the tablet. All tests were performed according to the manufacturer's instructions and approved survey standard operating procedures (SOPs). SOPs were adhered to during the entire survey period, including procedures for testing, biosafety, and waste disposal (18).
A standardized COVID-19 questionnaire was used to collect information on demographic data (age, sex, occupation); household socio-economic situation; knowledge attitudes and practices toward COVID-19; and comorbidities and healthcare seeking.
After consenting, a face-to-face interview was conducted in a local language with all eligible members of the household using a tablet device. The exceptions were children under 5 years who were not subjected to a questionnaire. The data manager checked for completeness of the COVID-19 questionnaire on the chosen electronic platform during and at the end of each day. These data were loaded on a database that links to the questionnaire.
A standard finger prick blood sampling method was used to obtain a capillary blood sample from consenting participants. This was performed using universal protection and according to best practices (21). All blood samples were analyzed in the field, and the results were available within 15 min as SARS-CoV-2 rapid diagnostic tests were used. The result was recorded with one of the following outcomes if the participant was exposed to the virus and got infected or was negative (21). The results of the test were shared with the participant or the parent/legal guardian immediately. Privacy provision was ensured when the results were shared. With participants that tested positive for the RDT test whether IgG or IgM, we checked whether they are exhibiting any symptoms (9). For those with symptoms, a team was put on standby to go and test them using the PCR test, and if the PCR test became positive, then national guidelines were followed (22). All medical wastes were collected in biohazardous bags and incinerated at the ZEMA-approved incinerator at Kansanshi mine.
A rapid diagnostic test (RDT) was selected for the survey to address numerous logistical challenges (Onsite Rapid Test, CTK Biotech, USA). The test is reported to have a 97% sensitivity and 97.8% specificity when compared to PCR samples and the RDT test kits (23).
Ethics approval was granted for the study by the University of Zambia, Biomedical Research Ethics Committee (UNZABREC: REF. NO. 1660/2021). The data sets did not have participants' names but had an identification number, and hence, anonymity and confidentiality were guaranteed.
As previously described, survey data were entered directly onto a tablet during the interview. Data from the tablet were removed from the device when transferred to the central database. Data entry checks were put in place during the interview to prevent illogical data values. Interview data were password-protected on encrypted tablets and were stored in central databases on encrypted, password-protected computers at the study sites. All data and survey results were kept confidential and stored in a safe place. Paper data containing household, locator, and identifying data were kept separate from the interview data in a secure locked cabinet, in locked offices. The Public Health Coordinator at Zambia National Public Health Institute was responsible for making sure that all documents are properly secured. Hard copies of consent forms will be kept for 5 years beyond the end of the study and then destroyed. All ethics procedures were also followed using international ethical guidelines (17).
Data were cleaned containing age, sex, and occupation; household socio-economic situation; knowledge attitudes and practices toward COVID-19; and comorbidities and healthcare-seeking behaviors, with a total of 1, 586 participants. Prior to analysis, the data were weighted by primary sampling unit, stratum, and sample weight to ensure the survey's representativeness. Descriptive statistics were performed to observe the characteristics of the variables (numbers and percentages were reported as the variables were categorical). To account for the complex multistage sampling design and the clustered nature of the data, survey analysis approaches were used. Since the conditions for a chi-squared test were met, associations between categorical variables were evaluated using the chi-squared test of independence. The vce (cluster comp) syntax in the Stata version 15 command was used to take into consideration the complex multistage sampling design and the clustered nature of the data.
The primary statistical analysis used univariable and multivariable logistic regression to determine the factors that predicted SARS-CoV-2 infections among the mining community. Multiple logistic regression was used to select variables influencing SARS-CoV-2 using an investigator-led stepwise regression procedure. The final multiple regression model's variables were chosen by first running the multiple logistic regression command with all of the predictor variables and then removing one by one the predictor variables with the highest p-values from the model until only those predictor variables that best predicted the outcome remained in the model. Finally, based on Akaike's information criterion and Bayesian information criterion (AIC and BIC) for the competing models, the best-fit model was chosen. The model that had the lowest AIC and BIC values in comparison with other models was picked. The 95% confidence intervals (CIs) for the crude odds ratio (cOR) and adjusted odds ratio (aOR) were shown. A p-value of 0.05 was regarded as significant. STATA 15 (STATA Corp.) was used to analyze the data.
Out of 622 respondents, 9.0% tested positive for IgG and 2.6% for IgM, with more positive responses in the Solwezi district. The study examines respondents' knowledge levels and self-risk assessment of COVID-19 symptoms in Zambia. Most respondents believe that close contact with infected individuals can lead to infection, with only 2.3% having no knowledge of COVID-19 transmission. Most respondents assessed their self-risk as no chance (27.4%), very small chance (19.1%), and medium chance (27.1%), with no differences between Solwezi and Kalumbila districts. Respondents trusted information on COVID-19 from healthcare providers, with 56.2% trusting the Ministry of Health website. Participants with age 24 years and above as well as having experienced symptoms of SARS-CoV-2 had a significant effect on testing positive for SARS-CoV-2.
The targeted sample for the survey was 3,200 persons in Solwezi (2,720) and Kalumbila (480) districts. During the listing of households in the selected enumeration areas, 802 households were successfully listed out of the target of 800 households, that is, 160 in Kalumbila and 642 in Solwezi (Kansanshi). In the listed households, 3,047 persons were successfully listed, which made 95% of the target sample. However, during the actual survey, only 53% (1, 586) of the persons listed were present for the interview, that is, 294 (19%) in Kalumbila and 1, 294 (81%) in Solwezi (Figure 1).
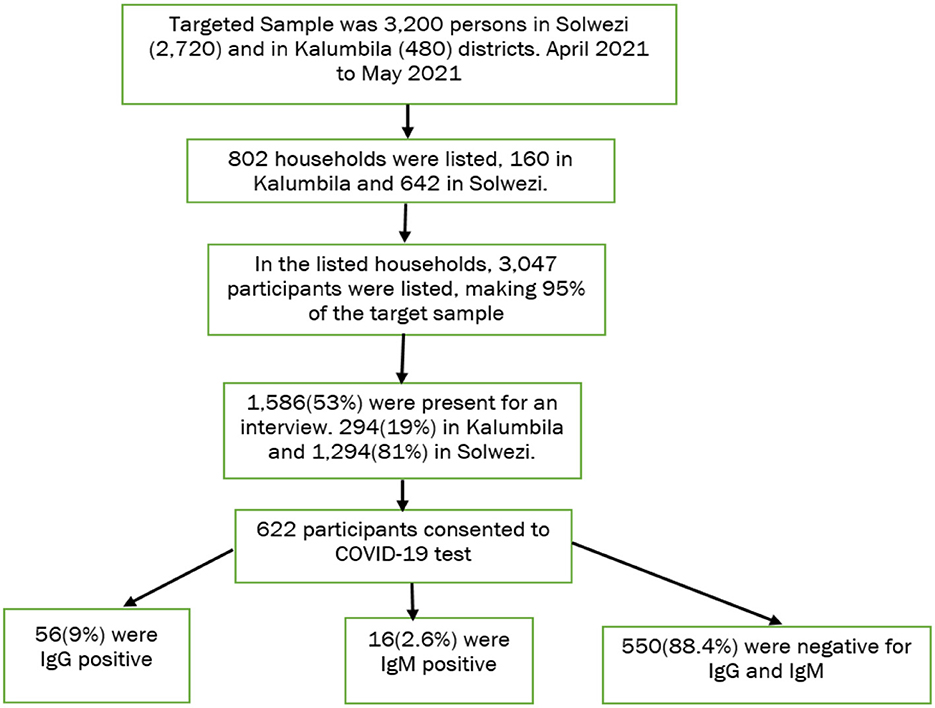
Figure 1. Flow chart of the sampling process and enumerated participants.
Table 1 reveals that the median age of the respondents was 26 years (IQR, 6–48). More females than males responded to the interview. In terms of marital status, the majority of those interviewed were married/cohabiting (55.9%). A large number of respondents interviewed had secondary education (46.2%). At the household level, 37.4% of the household heads had not changed their employment status after the COVID-19 outbreak. However, 15.9% of the respondents had reduced hours of work, while 13.0% of the participates were working from home and 9.3% had lost their jobs.
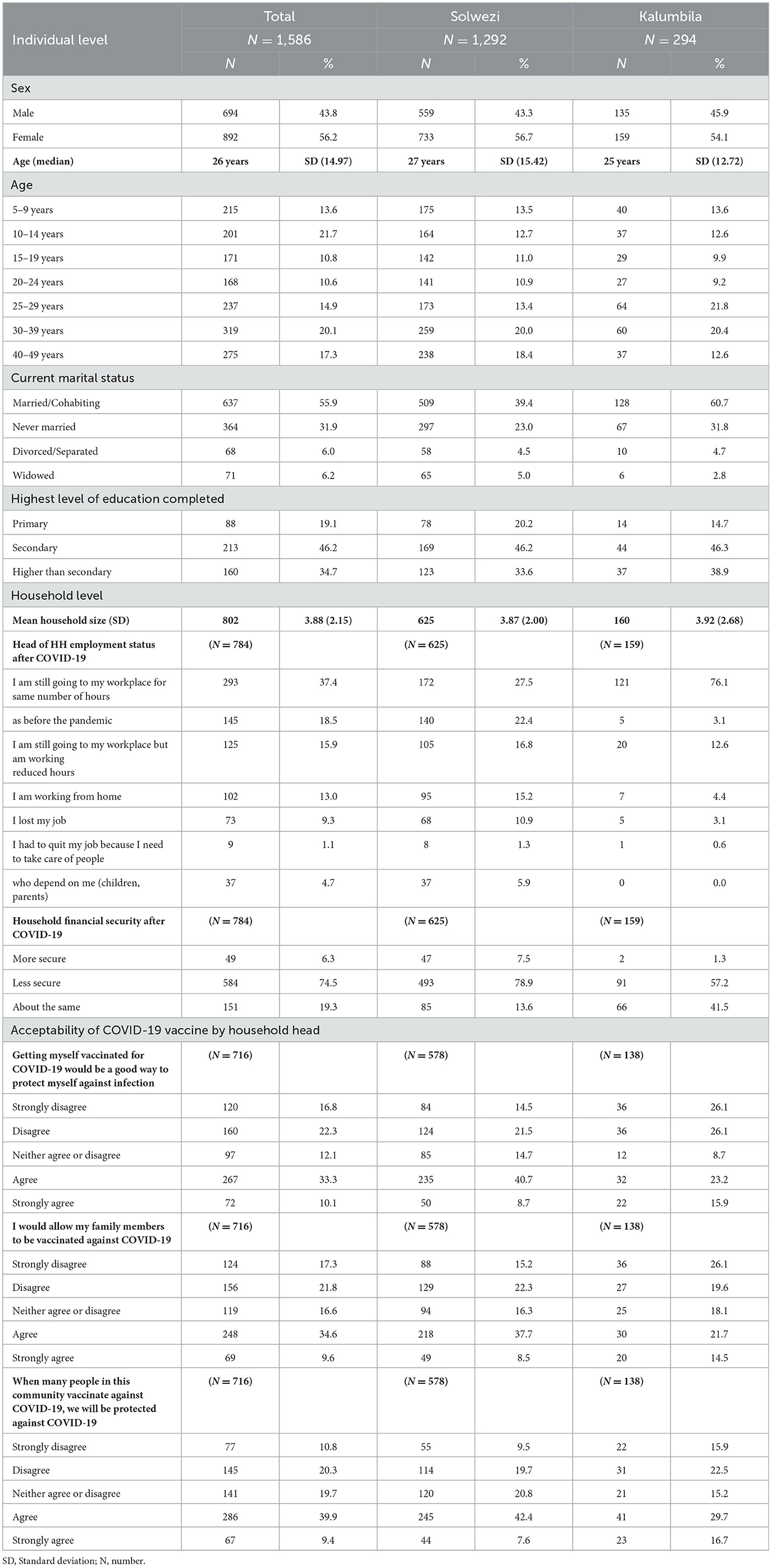
Table 1. Demographic characteristics and vaccine acceptability.
On household financial security that is the monthly income level of the household after the COVID-19, 74.5% of households that participated in the survey were less financially secure. However, little more respondents in the Kalumbila district indicated that their financial position had not changed, and this percentage was higher than that indicated by Solwezi district participants.
On the acceptability of the COVID-19 vaccine, almost half of the household heads agreed to get the vaccine and to allow their family members to get the vaccine. These household heads agreed that if many people in their community get vaccinated against COVID-19, the communities will be protected against COVID-19. However, ~39.1% of the household heads did not accept to get the vaccine. This non-acceptance of the vaccine was more in the Kalumbila district than the Solwezi district.
Table 2 reveals the COVID-19 experience of the respondents. When asked whether the respondents had experienced any symptoms of COVID-19 from 1 March 2020 and in the last 2 weeks, most of them reported that they had not. However, only 26.0% of the respondents had ever tested for COVID-19 (i.e., 23.4% in the Solwezi district and 37.8% in the Kalumbila district).
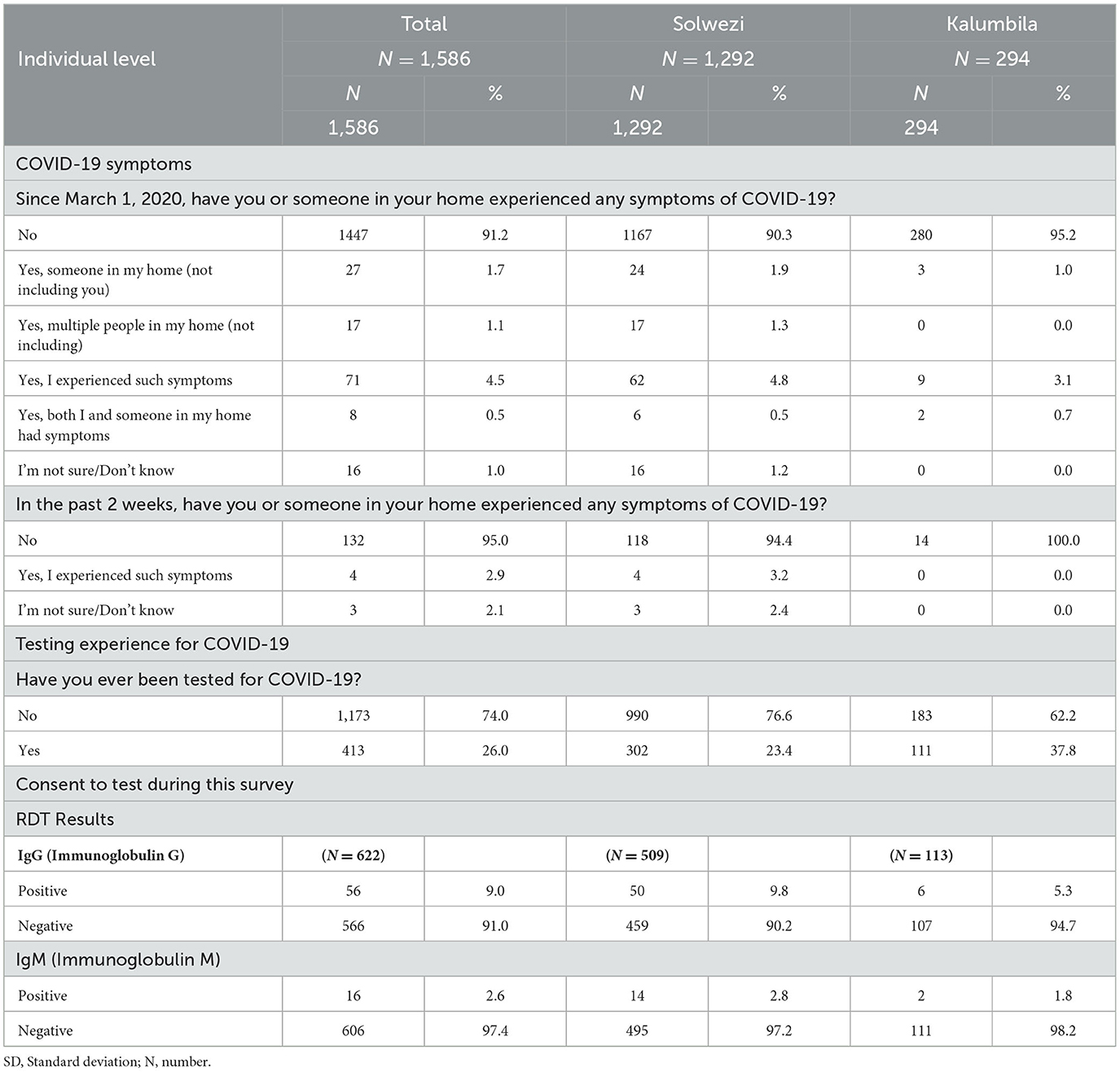
Table 2. COVID-19 characteristics.
A total of 622 respondents consented to take a test for COVID-19 in this study. Of the total that tested for COVID-19, 9.0% were found positive for IgG (past infection) and 2.6% were found positive for IgM (recent infection). More positive respondents were found in the Solwezi district compared to the Kalumbila district.
Table 3 highlights the knowledge levels of respondents to COVID-19 and how they assess their self-risk. A few of the respondents were able to indicate the symptoms of COVID-19, and these were limited to those that were commonly mentioned in Zambia. Some differences in knowledge levels of knowing symptoms were observed among the respondents in the Solwezi and Kalumbila districts.
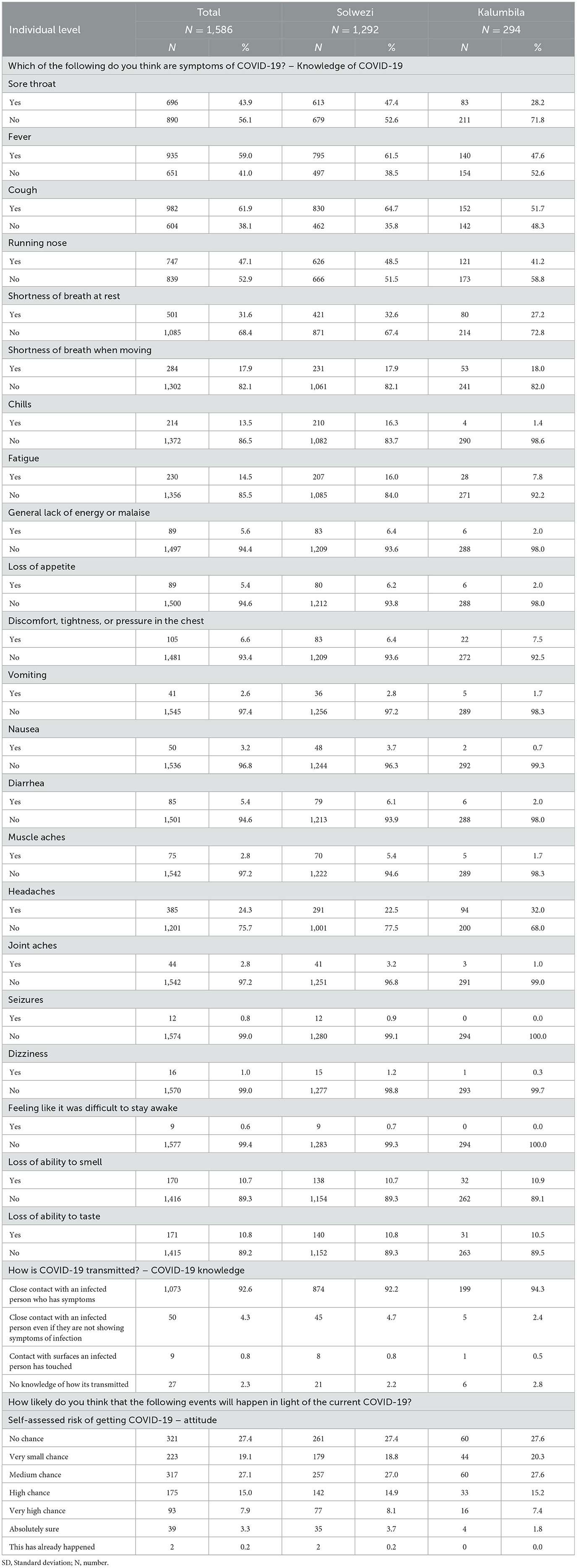
Table 3. COVID-19 knowledge and attitudes of COVID-19.
Otherwise, many of them stated that they did not know the symptoms of COVID-19. When the participants were asked how one could get COVID-19, the majority felt it was through coming into contact with a COVID-19 patient with symptoms. However, only 2.3% of the respondents had no knowledge of how COVID-19 was transmitted. There were no observed differences between Solwezi and Kalumbila districts.
When the respondents were asked to gauge their risk of getting COVID-19, most of them assessed their self-risk to no chance (27.4%), very small chance (19.1%), and medium chance (27.1%). Even for this variable, the differences between Solwezi and Kalumbila districts were small.
Respondents were asked to gauge their trusted sources of information for COVID-19, as shown in Table 4. Most respondents indicated that they trusted information of COVID-19 from Doctors or other healthcare providers, with 56.2% of them responding that they completely trusted this source. Other sources of information completely trusted by respondents included the official Ministry of Health website (47.3%), the Press conference by the Minister of Health (46.8%), the Provincial or District Health Offices (46.5%), the World Health Organization (44.0%), the local media (42.1%), and the CDC (36.3%).
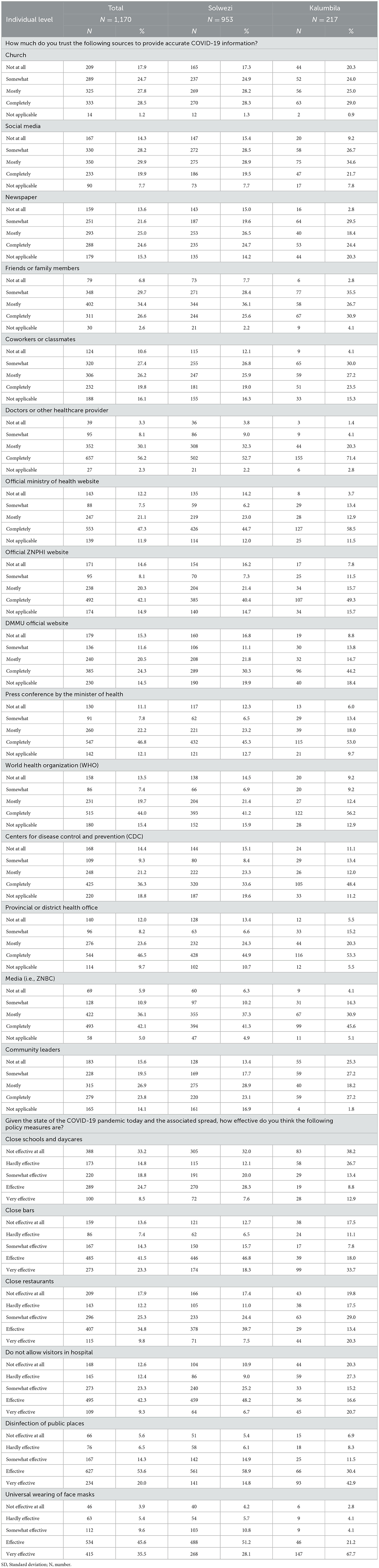
Table 4. COVID-19 trusted sources for COVID-19 information and effectiveness of prevention measures.
Furthermore, the respondents were asked how effective the policy measures were to control COVID-19 spread. Most respondents stated that disinfection of public places (53.6%), universal wearing of face masks (45.6%), not allowing visitors in hospitals (42.3%), closing bars (41.5%), and closing restaurants (34.8%) were indicated as the most effective measures of controlling COVID-19.
In Table 5, respondents were asked whether they have made lifestyle changes to prevent COVID-19 infection, and the majority of them indicated that they are practicing social distancing, staying at home more, hand washing more than usual, hand sanitizing more than usual, and wearing face masks when out in public. However, some respondents indicated that they are not adhering to the following: cleaning their houses more than usual, disinfecting surfaces in their households more than usual, avoiding or canceling domestics travel, avoiding or canceling international travel, eating from restaurants, and drinking from bars or nightclubs.
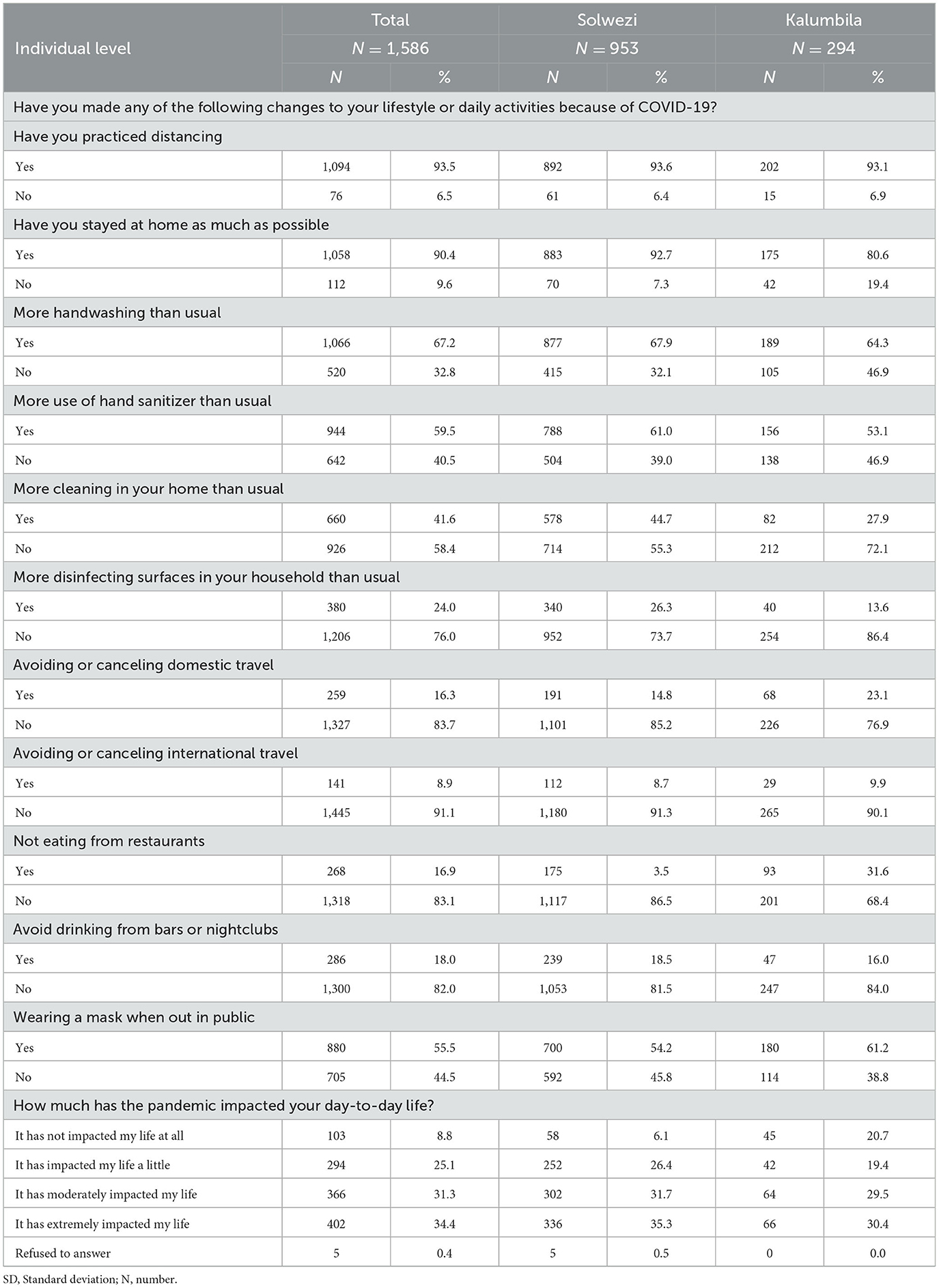
Table 5. Lifestyle or daily activities change during COVID-19.
When asked whether COVID-19 has had an impact on the respondent's day-to-day life, 34.4% of them indicated that COVID-19 has had an extreme impact on their life, whereas 8.8% of the respondents revealed that COVID-19 has had no impact on their lives.
The chi-square test was done to determine associations between categorical variables and COVID-19 infection. Table 6 shows the results between participant socio-demographic characteristics and COVID-19 infections as determined by Pearson's chi-square test of independence. Female participants had higher COVID-19 positive results (8.2%) (49/594) than male participants (5.4%) (32/594). Nonetheless, there was no significant difference in COVID-19 positive test results of males and females (p = 0.110). The study further showed that participants who were in Solwezi tested positive for COVID-19 (49/594) (8.3%) compared to those that were in Kalumbila. There was a significant difference in the positivity of the test done in Kalumbila and those in Solwezi as evidenced by the p-value (p = 0.043). The results, however, showed no significant difference in those participants who have tested for COVID-19 before the survey was conducted and those who tested when the survey was conducted (p = 0.145).
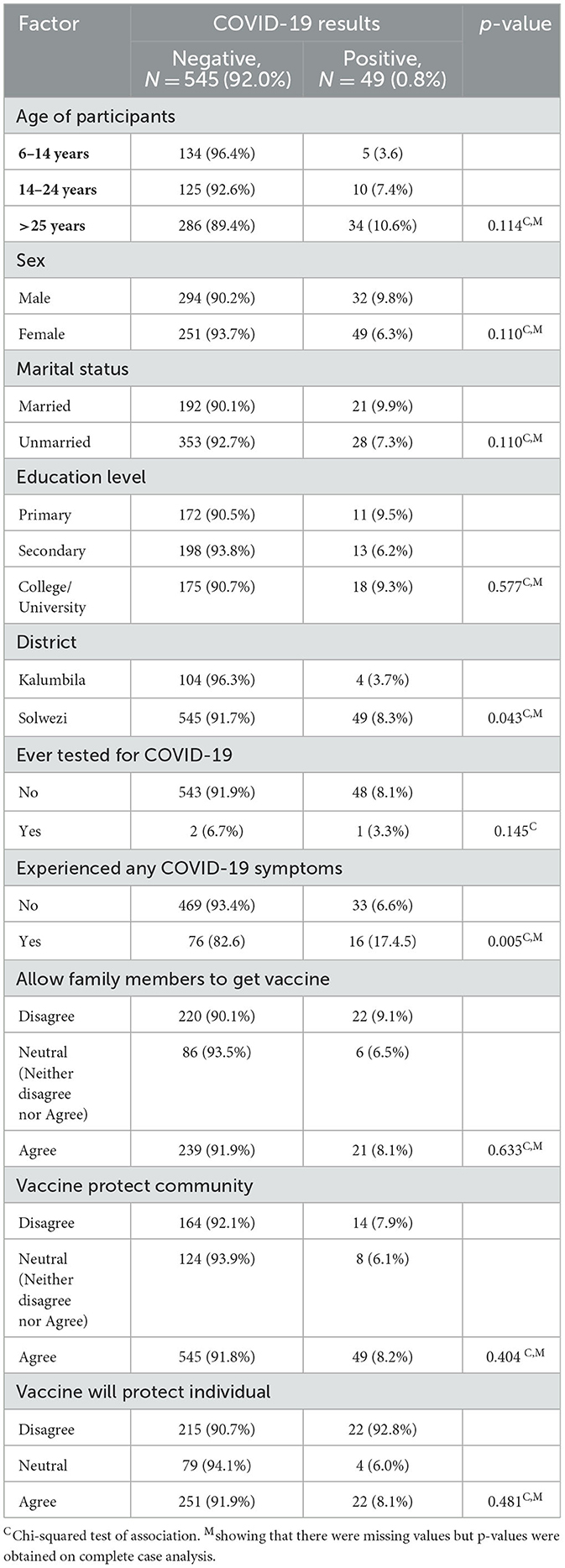
Table 6. Cross-tabulation of the predictors of COVID-19 infection.
There was no evidence of a difference in testing positive for COVID-19 between age groups, whether one was married or not, whether attained a certain level of education or not, whether the participant will allow a family member to have a vaccine or not, whether the participants disagreed or agreed that COVID-19 vaccine will protect the community, and whether the participants will disagree or agree that COVID-19 vaccine will protect individuals. However, there was a significant difference in who did not experience COVID-19 compared to those that did experience as evidenced by the p-value (p = 0.006).
A logistic regression was performed to examine the predictors of the prevalence of COVID-19 participants of 5 years and above. The significance level was set at a p < 0.05 at 95% confidence interval.
The results of univariate analysis, that is, crude odds ratios (cOR) in Table 7, show that participants in Kalumbila, that is, participants who lived in Solwezi mining community had 2.7 times the odds of testing positive for COVID-19 compared to participants who lived in Kalumbila mining community (cOR = 2.65; 95% CI: 1.00, 7.01), participants whose age, that is, age above 24 years had 3.2 times the odds of being testing positive for COVID-19 compared to participants who age was between 6 and 14 years (cOR = 3.19, 95% CI: 1.01, 10.05), and also participants who had or their family member had experienced COVID-19 symptoms before had 3.0 times the odds of testing positive for COVID-19 compared to those who never experienced COVID-19 symptoms before the study was done (cOR = 2.99, 95% CI: 1.50, 5.96), and participants marital status (cOR = 0.73; 95% CI: 0.30, 1.77), sex of participant (cOR = 0.62; 95% CI: 0.33, 1.15) and educational level, secondary (cOR = 0.63; 95% CI: 0.20, 2.07) university/college (cOR = 0.98; 95% CI: 0.42, 2.28) compared to primary level had no statistically significant association with testing positive for COVID-19.
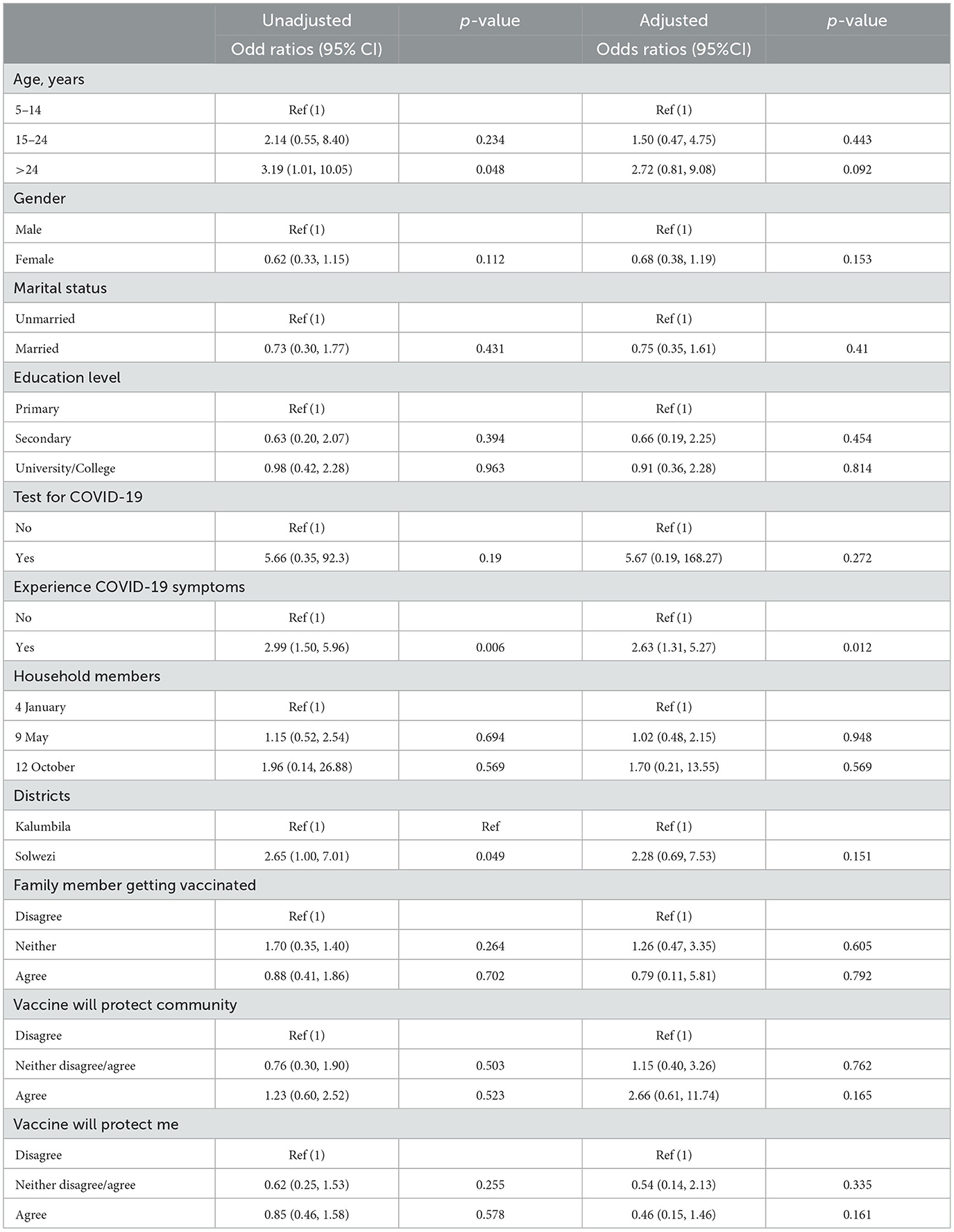
Table 7. Logistic regression adjusted and unadjusted.
On the other hand, participants who had a COVID-19 test before the study (cOR = 5.66; 95% CI: 0.35, 92.3), household members 5 to 9 (cOR = 1.15; 95% CI: 0.52, 2.54), household members 10 to 12 (cOR = 1.96; 95% CI: 0.14, 26.88) compared to those with 1–4 household members, whether the household members would be allowed to receive the vaccine by household head, neither disagree nor agree (cOR = 1.70; 95% CI: 0.35, 1.40), agree (cOR = 0.88; 95% CI: 0.41, 1.86), will you accept the vaccine as an individual, neither or agree (cOR = 0.62; 95% CI: 0.25, 1.53), agree (cOR = 0.85; 95% CI: 0.46, 1.58), and will the vaccine protect the community, neither disagree nor agree (cOR = 0.76; 95% CI: 0.30, 1.90), agree (cOR = 1.23; 95% CI: 0.60, 2.52) had no statistically significant association with testing positive for COVID-19.
Table 8 shows the final multivariable analysis model arrived that fit the data well. Multiple regression was done in order to control for possible confounding. An investigator-led stepwise regression was used to arrive at the model. This implies running the multiple logistic regression command with all the predictor variables in the first stage and then removing variables with the highest p-values one by one from the model until we remained with a model that best explained the data (parsimonious model). The multivariable analysis model contains six explanatory variables: participants' age, sex, whether the participant tested for COVID-19 before the study or not, whether the participants experienced symptoms of COVID-19 or not, whether participants agreed, disagreed, or neither disagreed nor agreed that vaccinating the community would protect them from COVID-19, and whether an individual getting the vaccine would protect them from COVID-19 as the best predictors of being found COVID-19 positive. Although participants sex, whether the participant tested for COVID-19 before the study or did not, whether participants agreed, disagreed, or neither disagreed nor agreed that vaccinating the community would protect them from COVID-19, and whether an individual getting the vaccine would protect them from COVID-19 were not statistically significant, the variables were left in the model due to prior knowledge from other studies which consistently showed that they could be used to perfectly predict one being found positive.
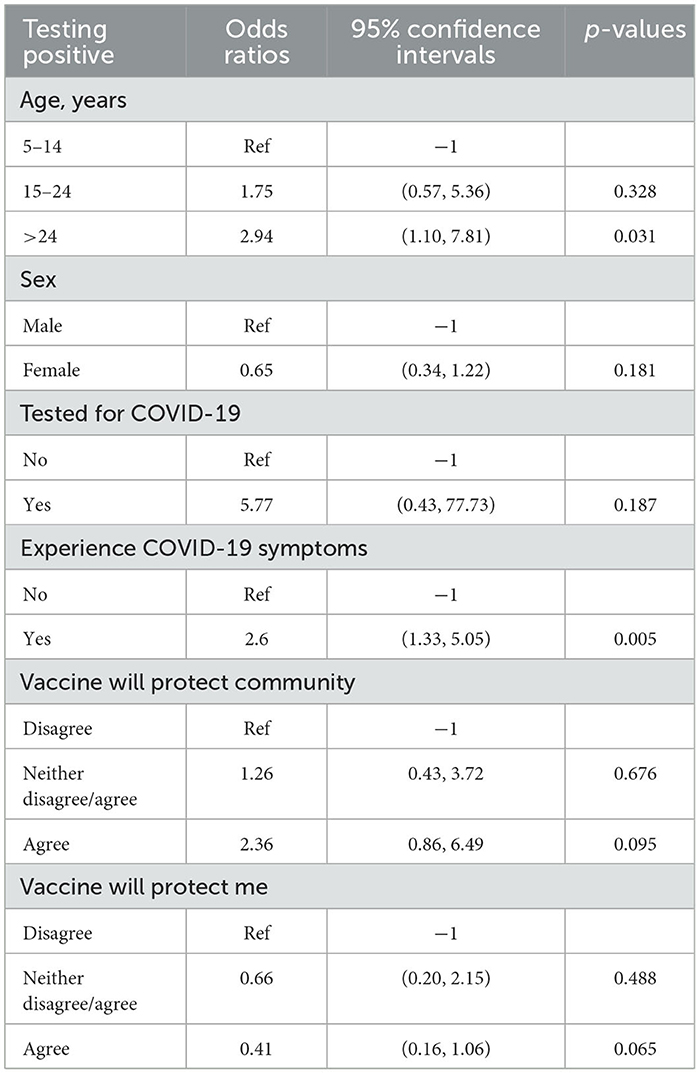
Table 8. Multivariable analysis.
As shown in Table 8, age and having experienced symptoms of COVID-19 before the study were significantly associated with being found positive for COVID-19. The effect of experiencing COVID−19 symptoms, that is, whether the participant had experienced symptoms before the study, was 2.6 times more likely to be infected (AOR = 2.60; 95% CI: 1.33, 5.05) compared to participants who did not have any COVID-19 symptoms before the study, holding constant the effect of other predictors in the model. The other predictor was age, participants with age >24 years were 1.5 times more likely to be positive for COVID−19 (AOR =2.94; 95% CI = 1.10, 7.81) compared to other age categories holding constant the effects of other predictors in the model. However, sex (AOR = 0.65; 95% CI: 0.34, 1.22), and whether they tested for COVID-19 before the study or not (AOR = 5.77; 95% CI: 0.43, 77.73), whether the vaccine will protect the community, neither disagree nor agree (AOR = 1.26; 95% CI: 0.43, 3.72), agree (AOR = 2.36; 95% CI: 0.86, 6.49) compared to those who disagree. Whether the vaccine will protect the individual, neither disagree nor agree (AOR = 0.66; 95% CI: 0.20, 2.15), agree (AOR = 0.41; 95% CI: 0.16, 1.06) compared to participants who disagreed had no statistically significant association with healthcare-seeking behaviors controlling for the effect of other predictors in the model.
The study aimed at understanding disease transmission in its wider community in Solwezi and Kalumbila to determine the effectiveness of controls and the demographic spread of COVID-19. The results have shown that the prevalence of COVID-19 in the two mining towns of Solwezi and Kalumbila was 9.0% for previous infections and 2.6% for active cases. The findings are not different from what was reported in six districts of Zambia, which showed that 5–11% of the population was infected, while previous infections were ~8.2% (13). In contrast, a study done in Jakarta (24) found a much higher prevalence of 15.7% compared to our finding, which was the same period this survey was conducted, with the highest infection rates occurring in March 2020 (26.3%), followed by January 2021 (23.9%) and February 2021 (21.8%).
The study has shown that older age groups were more likely to be found with SARS-CoV-2. This is not a different study done in Zambia that found that age youngest age group, 15 to 19 years, had the lowest seroprevalence of SARS-CoV-2 (25). The findings have been demonstrated elsewhere that combined measure's pooled SARS-CoV-2 prevalence rose with age (13). Another study found that the only age groups where SARS-CoV-2 transmission has persisted with reproduction numbers (transmission rates) continuously over one are people aged 20 and above (26).
Furthermore, the study has shown that the results have also revealed that the knowledge of COVID-19 was limited to the general public provided during sensitization in most of the communities and hence increasing infections. It has been demonstrated elsewhere (27) that greater awareness and attitude toward COVID-19 prevention methods can reduce transmission rates and enhance public health results. This is in line with the findings of another study (28) that found that little was known about the general Zambian population's views and awareness about COVID-19 preventative efforts.
This study has further established that strong preventative and control measures undertaken by local governments such as the use of mask and hand washing in every public area are mostly responsible for reductions in infections among community members and the prevalence of COVID-19 was still high. A study done in Zambia (28) found that despite the awareness of COVID-19 preventative measures being high, people's opinions about these measures were unfavorable and may have an impact on people adherence to COVID-19 measures. Another study argues that adherence to COVID-19 preventive measures was correlated with occupation and knowledge (29). With the problem of adherence to public health measures because of false information which has presented difficulties in Zambia's fight against COVID-19, continuous public education and sensitization on COVID-19 and the value of vaccinations are required. Vaccines boost immune function and help the body fight against infectious invaders (30). Vaccines are highly successful at containing disease outbreaks, according to the available data (31). Similar research has demonstrated the high efficacy and safety of COVID-19 vaccinations (31–33).
The study has demonstrated that most of the information that is trusted about COVID-19 is from the health providers and generally from the Ministry of Health as well as WHO and Center for Disease Control (CDC). The findings in this study are in line with the findings from other studies (34), which observed that willingness to participate in contact tracing was positively correlated with trust in information from public health organizations, even though these organizations were not always the primary providers of information regarding COVID-19. In contrast, a study (35) found that when it comes to knowledge regarding COVID-19 vaccinations, doctors have more faith in official government sources and their employers than do nurses, pharmacists, and advanced practice providers (35).
Furthermore, the study demonstrated that COVID-19 had a negative impact on the two communities in terms of financial insecurity (monthly income) and job losses. According to a study (36), it was found that 24% of respondents lost their jobs or income and had reduced hours of work due to the COVID-19 pandemic. In contrast with our findings, another study (37) found that the need for specialized skills in the logistics and healthcare industries was expanded. Furthermore, there is evidence of a rise in job openings incorporating remote working conditions (37).
The study further demonstrates that vaccine acceptability is mixed with some agreeing to taking the vaccine and recommending it to their family members and other persons in their communities, whereas other persons totally refused to accept the COVID-19 vaccine. This is in line with what has been reported elsewhere (38) that the acceptance rate of the COVID-19 vaccination was just 37.4% due to hesitance. In contrast to our finding, a study done in Japan (39) found that participants who had received the seasonal influenza vaccination had higher acceptance rates for the COVID-19 vaccine. Another study found that participants were more inclined to take the COVID-19 shots because they thought that vaccines are typically safe and if they were prepared to pay for them once they became available (38). However, in line with this study finding, participants who were working and older than 35 years were less likely to receive the COVID-19 vaccinations (40). Additionally, individuals who distrusted all sources of information about COVID-19 vaccinations and those who thought there was a conspiracy behind the disease were less likely to accept the vaccine (38).
The study has highlighted gaps, such as a lack of adherence to COVID-19 preventive measures, as a result of a lack of knowledge and misinformation on vaccine uptake. Therefore, this is a good opportunity for the Ministry of Health and other partners in Zambia to work together to put up the right message and to sensitize the community to the importance of the vaccine as it stimulates the immune system and aids in the fight against infectious agents. A random sample of the population was used in our study. This study further highlights the mixed feeling about the vaccine uptake from participants in the mining communities. It has also demonstrated that it is important to strengthen the level of knowledge about COVID-19 among community members by emphasizing good practices as it can help reduce the disease burden among workers who work for the mining community. Very few studies have been done with a focus on the prevalence of COVID-19 in mining communities.
This study is not free from limitations mainly resulting from being a cross-sectional study, and it can only provide information at one point in time. As such, it is not possible to draw firm conclusions on the evolution of the pandemic in the two communities. Despite the robust sampling process that was used to select SEA and households, the results reported in this study are limited to the two mining communities. The target household size estimated for the study was four persons. During the listing of households, the number of persons per household was almost the target size. However, during the actual survey, the number of household members available per household was less. The less members per household could have biased the findings of the study, especially if those that were not available had different attributes from those present.
The prevalence of COVID-19 in the mining towns for previous infections and active cases was similar to previous studies done in Zambia. Older age groups and being symptomatic were associated with COVID-19 infection. The study has shown that the knowledge of COVID-19 was limited to the general public provided during sensitization in the mining communities, leading to increased infections. Greater awareness and attitudes toward COVID-19 prevention methods can reduce transmission rates and enhance public health results. Local governments' strong preventative and control measures, such as mask use and hand washing in public areas, could reduce infections among community members. Many community members were probably asymptomatic and, as such, gauged themselves as having a low risk of getting infected with COVID-19. This resulted in most community members not adhering to public health preventive measures. The government and partners should continue to sensitize the community members on the preventive measures of COVID-19 in spite of not being adhere to and continue with community testing so that all those positive but without symptoms can self-isolate and those with symptoms and who are sick can be admitted to the hospital. There should also be a campaign in promoting vaccine uptake among community members.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by University of Zambia, Biomedical Research Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Conceived, composed the manuscript, the manuscript was rewritten, updated, and improved by TM, KMe, NK, MD, and KMw. The essay was co-written by all the authors, who also gave their approval to the final draft. All authors contributed to the article and approved the submitted version.
KMe and MD were employed by First Quantum Minerals Limited.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Chipimo PJ, Barradas DT, Kayeyi N, Zulu PM, Muzala K, Mazaba ML, et al. First 100 persons with COVID-19—Zambia, March 18–April 28, 2020. Morbid Mortal Wkly Rep. (2020) 69:1547. doi: 10.15585/mmwr.mm6942a5
2. Anyanwu OA, Naumova EN, Chomitz VR, Zhang FF, Chui K, Kartasurya MI, et al. The effects of the COVID-19 Pandemic on nutrition, health and environment in Indonesia: a qualitative investigation of perspectives from multi-disciplinary experts. Int J Environ Res Pub Health. (2022) 19:11575. doi: 10.3390/ijerph191811575
3. World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard With Vaccination Data | WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. Geneva: World Health Organization, 1–5 (2021).
4. Africa CDC. Coronavirus Disease 2019 (COVID-19) – Africa CDC,” Africa CDC Dashboard. Addis Ababa: CDC (2021).
5. Oosthuizen M, Cilliers J, Pooe TK, Alexander K, Moyer JD. Impact of COVID-19 in Africa: a scenario analysis to 2030. ISS Africa Rep. (2020) 2020:1–40. doi: 10.2139/ssrn.3660866
6. Ozili P. COVID-19 in Africa: socio-economic impact, policy response and opportunities. Int J Sociol Soc Policy. (2020) 42:177–200. doi: 10.1108/IJSSP-05-2020-0171
7. Zhang N, Chen W, Chan PT, Yen HL, Tang JWT, Li Y. Close contact behavior in indoor environment and transmission of respiratory infection. Indoor Air. (2020) 30:645–61. doi: 10.1111/ina.12673
8. Nicas M, Best D. A study quantifying the hand-to-face contact rate and its potential application to predicting respiratory tract infection. J Occup Environ Hyg. (2008) 5:347–52. doi: 10.1080/15459620802003896
9. Quashie PK, Mutungi JK, Dzabeng F, Oduro-Mensah D, Opurum PC, Tapela K, et al. Trends of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antibody prevalence in selected regions across Ghana. Wellcome Open Res. (2021) 6:173. doi: 10.12688/wellcomeopenres.16890.1
10. Helliwell JA, Bolton WS, Burke JR, Tiernan JP, Jayne DG, Chapman SJ. Global academic response to COVID-19: cross-sectional study. Learned Pub. (2020) 33:385–93. doi: 10.1002/leap.1317
11. Salian VS, Wright JA, Vedell PT, Nair S, Li C, Kandimalla M, et al. COVID-19 transmission, current treatment, and future therapeutic strategies. Mol Pharm. (2021) 18:754–71. doi: 10.1021/acs.molpharmaceut.0c00608
12. Nakamoto I, Zhang J. Modeling the underestimation of COVID-19 infection. Results Phys. (2021) 25:104271. doi: 10.1016/j.rinp.2021.104271
13. Mulenga LB, Hines JZ, Fwoloshi S, Chirwa L, Siwingwa M, Yingst S, et al. Prevalence of SARS-CoV-2 in six districts in Zambia in July, 2020: a cross-sectional cluster sample survey. The Lancet Global Health. (2021) 9:e773–81. doi: 10.1016/S2214-109X(21)00053-X
14. Rostami A, Sepidarkish M, Fazlzadeh A, Mokdad AH, Sattarnezhad A, Esfandyari S, et al. Update on SARS-CoV-2 seroprevalence: regional and worldwide. Clin Microbiol Inf. (2021) 27:1762–71. doi: 10.1016/j.cmi.2021.09.019
15. World Health Organization. Eastern Mediterranean health journal. East Med Health J. (2022) 28:635–701. doi: 10.26719/2022.28.9.701
16. Eide AH, Loeb M. Living Conditions Among People With Activity Limitations in Zambia. A National Representative Study. SINTEF Rapport (2006).
17. Council for International Organizations of Medical Sciences. International Ethical Guidelines for Health-Related Research Involving Humans. International Ethical Guidelines for Health-Related Research Involving Humans. Geneva: Council for International Organizations of Medical Sciences (2017).
18. Centers for Disease Control and Prevention. CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel. Atlanta, GA: Centers for Disease Control and Prevention (2020).
19. Hungerford J, Wu WH. Comparison study of three rapid test kits for histamine in fish: BiooScientific MaxSignal enzymatic assay, Neogen Veratox ELISA, and the Neogen Reveal Histamine Screening test. Food Control. (2012) 25:448–57. doi: 10.1016/j.foodcont.2011.11.007
20. Food and Drug Administration. Emergency Use Authorization. Silver Spring, MD: Food and Drug Administration (2022).
21. Cohen KW, Linderman SL, Moodie Z, Czartoski J, Lai L, Mantus G, et al. Longitudinal analysis shows durable and broad immune memory after SARS-CoV-2 infection with persisting antibody responses and memory B and T cells. Cell Rep Med. (2021) 2:100354. doi: 10.1016/j.xcrm.2021.100354
22. Bajwa SJS, Sarna R, Bawa C, Mehdiratta L. Peri-operative and critical care concerns in coronavirus pandemic. Indian J Anaesth. (2020) 64:267. doi: 10.4103/ija.IJA_272_20
23. Boelaert M, Verdonck K, Menten J, Sunyoto T, van Griensven J, Chappuis F, et al. Rapid tests for the diagnosis of visceral leishmaniasis in patients with suspected disease. Cochrane Database Syst. Rev. (2014) 2014:CD009135 doi: 10.1002/14651858.CD009135.pub2
24. Setiadi W, Rozi IE, Safari D, Daningrat WOD, Johar E, Yohan B. Prevalence and epidemiological characteristics of COVID-19 after one year of pandemic in Jakarta and neighbouring areas, Indonesia: a single center study. PLoS ONE. (2022) 17:e0268241. doi: 10.1371/journal.pone.0268241
25. Shanaube K, Schaap A, Klinkenberg E, Floyd S, Bwalya J, Cheeba M, et al. SARS-CoV-2 seroprevalence and associated risk factors in periurban Zambia: a population-based study. Int J Inf Dis. (2022) 118:256–63. doi: 10.1016/j.ijid.2022.03.021
26. Monod M, Blenkinsop A, Xi X, Hebert D, Bershan S, Tietze S. Age groups that sustain resurging COVID-19 epidemics in the United States. Science. (2021) 371:eabe8372. doi: 10.1126/science.abe8372
27. Rehman R, Jawed S, Ali R, Noreen K, Baig M, Baig J. COVID-19 pandemic awareness, attitudes, and practices among the Pakistani general public. Front Pub Health. (2021) 9:588537. doi: 10.3389/fpubh.2021.588537
28. Mudenda S, Botha M, Mukosha M, Daka V, Chileshe M, Mwila K, et al. Knowledge and attitudes towards COVID-19 prevention measures among residents of Lusaka district in Zambia. Aquademia. (2022) 6:ep22005. doi: 10.21601/aquademia/12210
29. Abeya SG, Barkesa SB, Sadi CG, Gemeda DD, Muleta FY, Tolera AF, et al. Adherence to COVID-19 preventive measures and associated factors in Oromia regional state of Ethiopia. PLoS ONE. (2021) 16:e0257373. doi: 10.1371/journal.pone.0257373
30. Omer SB, Salmon DA, Orenstein WA, Dehart MP, Halsey N. Vaccine refusal, mandatory immunization, and the risks of vaccine-preventable diseases. N Eng J Med. (2009) 360:1981–8. doi: 10.1056/NEJMsa0806477
31. Mudenda S, Chileshe M, Mukosha M, Hikaambo CNA, Banda M, Kampamba M, et al. Zambia's response to the COVID-19 pandemic: exploring lessons, challenges and implications for future policies and strategies. Pharmacol Pharm. (2022) 13:11–33. doi: 10.4236/pp.2022.131002
32. Ngwewondo A, Nkengazong L, Ambe LA, Ebogo JT, Mba FM, Goni HO, et al. Knowledge, attitudes, practices of/towards COVID 19 preventive measures and symptoms: a cross-sectional study during the exponential rise of the outbreak in Cameroon. PLoS Negl Trop Dis. (2020) 14:e0008700. doi: 10.1371/journal.pntd.0008700
33. Chacón FR, Doval JM, Rodríguez VI, Quintero A, Mendoza DL, Mejía MD, et al. Knowledge, attitudes, and practices related to COVID-19 among patients at Hospital Universitario de Caracas triage tent: a cross-sectional study. Biomédica. (2021) 41:48. doi: 10.7705/biomedica.5808
34. Amara PS, Platt JE, Raj M, Nong P. Learning about COVID-19: sources of information, public trust, and contact tracing during the pandemic. BMC Public Health. (2022) 22:1348. doi: 10.1186/s12889-022-13731-7
35. Brauer E, Choi K, Chang J, Luo Y, Lewin B, Munoz-Plaza C, et al. Health care providers' trusted sources for information about COVID-19 vaccines: mixed methods study. JMIR Infodemiology. (2021) 1:e33330. doi: 10.2196/33330
36. Despard MR, Grinstein-Weiss M, Chun Y, Roll S. COVID-19 Job and Income Loss Leading to More Hunger and Financial Hardship. Washington, DC: Brookings Institution (2020).
37. Organisation for Economic Co-operation and Development. An Assessment of the Impact of COVID-19 on Job and Skills Demand Using Online Job Vacancy Data. London: OECD Publishing (2020).
38. El-Elimat T, AbuAlSamen MM, Almomani BA, Al-Sawalha NA, Alali FQ. Acceptance and attitudes toward COVID-19 vaccines: a cross-sectional study from Jordan. PLoS ONE. (2021) 16:e0250555. doi: 10.1371/journal.pone.0250555
39. Ishimaru T, Okawara M, Ando H, Hino A, Nagata T, Tateishi S. Gender differences in the determinants of willingness to get the COVID-19 vaccine among the working-age population in Japan. Hum Vacc Immunother. (2021) 17:3975–81. doi: 10.1080/21645515.2021.1947098
Keywords: COVID-19, prevalence survey, cluster, vaccine uptake, community sensitization
Citation: Mumba TK, Merwe KVD, Divall M, Mwangilwa K and Kayeyi N (2023) Seroprevalence survey of SARS-CoV-2, community behaviors, and practices in Kansanshi and Kalumbila mining towns. Front. Public Health 11:1103133. doi: 10.3389/fpubh.2023.1103133
Received: 24 November 2022; Accepted: 07 August 2023;
Published: 20 September 2023.
Edited by:
Oyelola A. Adegboye, Charles Darwin University, AustraliaReviewed by:
Steward Mudenda, University of Zambia, ZambiaCopyright © 2023 Mumba, Merwe, Divall, Mwangilwa and Kayeyi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kelvin Mwangilwa, a2VsdmlucGV0ZXJzakBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.