 Fangfang Shou
Fangfang Shou Jing Wang
Jing Wang Steven Laureys
Steven Laureys Lijuan Cheng
Lijuan Cheng Wangshan Huang1
Wangshan Huang1
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Public Health , 30 March 2023
Sec. Family Medicine and Primary Care
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1071008
This article is part of the Research Topic Advances in Physical and Psychosocial Telecare: Promises and Pitfalls View all 5 articles
Background: The significant lack of rehabilitation prognostic data is the main reason that affects the treatment decision-making and ethical issues of patients with disorders of consciousness (DoC). Currently, the clinic's consciousness assessment tools cannot satisfy DoC patients' follow-up needs.
Objective: The purpose of this study is to construct a sensitive, professional, and simple telephone follow-up scale for DoC patients to follow up on the prognosis, especially the recovery of consciousness, of prolonged DoC patients transferred to community hospitals or at home.
Methods: This study is to adopt expert consultation to construct and to verify the validity and feasibility of the scale on-site.
Conclusion: At present, there is a strong demand for portable, accurate, and easily operated scales. It is helpful to improve the rehabilitation data of prolonged DoC patients and provide more basis for their treatment and rehabilitation.
With the progress of medical technology and the development of artificial feeding, more and more patients with Disorders of Consciousness (DoC) have survived. Among the broad classification of DoC (1), three main conscious levels have been clinically identified according to behavioral criteria: Coma, Unresponsive Wakefulness Syndrome (UWS) or Vegetative State (VS), and Minimally Conscious State (MCS) (2). Coma Recovery Scale-Revised (CRS-R) is considered as the gold standard for consciousness assessment (3, 4) and the primary method for consciousness follow-up. CRS-R includes auditory, visual, motor, oral, communication and arousal (5, 6). Such patients can be divided into coma, UWS/VS, MCS-, MCS+, and Emergence from the Minimally Conscious State (EMCS) according to their behaviors (7). However, CRS-R operation is conducted face-to-face, which is time-consuming. Furthermore, due to the fluctuation of awakening and the effect of drugs, it is difficult to accurately identify the patient of consciousness in a one-time behavioral assessment. Studies have shown that repeated CRS-R assessments can reduce misdiagnosis (8). However, for community hospitals and home-based patients, implementing behavioral assessment is difficult due to transportation and time cost, especially for low-income families or assessors.
In the past decades, telephone follow-up was increasingly utilized in various fields. In the medical area, it has been variously used for patient compliance and continuity of care after patient discharged (9–14). Telephone follow-up can comprehensively assess patients' state of consciousness and provide remote health education for patients and their family members. Therefore, a highly targeted and feasible telephone follow-up scale is urgently needed.
Telephone service is an innovative expansion of the traditional “face-to-face” medical service, which is timelier and more flexible, more personalized, and more convenient to operate (15). Patients can communicate with healthcare workers anytime and anywhere through cell phones or other mobile platforms. Medical staffs can use the telephone to follow up, inform patients and exchange pictures and images sent by patients for preliminary diagnosis and medical guidance, which can overcome the time and space limitations of medical services (16). Telephone follow-up is to guide and supervise patients' condition and recovery status and psychological status via telephone. The purpose is to enable patients to continue to receive health education and medical services even after discharged. This service can effectively extend the care in-hospital to out-of-hospital. In addition, for DoC patients, the telephone program allows not only voice communication but also video assessment, which can keep abreast of the prognosis status and disease progression of DoC patients and improve patients' self-management ability, thus reducing the hospitalization rate and mortality rate of related diseases.
This study aims to construct a telephone follow-up scale more suitable for DoC patients. The scale is constructed using the currently verified consciousness indicators [vision pursuit (2), auditory localization (17), reproducible response to command, automatic motor response (18), localization to harmful stimuli (19) and olfactory stimulus response (20, 21)] observed by the patients' family members. The telephone consultant will make a consciousness diagnosis according to the information provided by the patient's family members.
This study is divided into two stages (see Figures 1, 2).
Stage 1: To develop the telephone follow-up scale for consciousness recovery.
Stage 2: To verify the accuracy and validity of the telephone follow-up scale for patients with DoC.
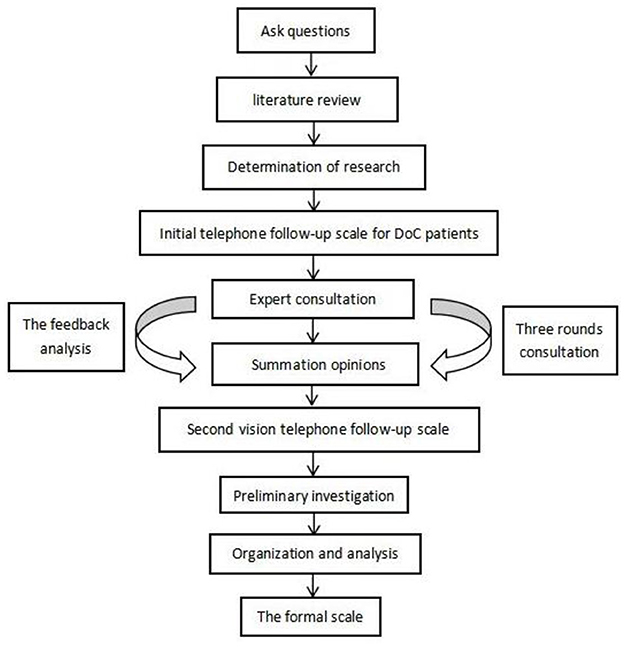
Figure 1. Flow chart of scale development.
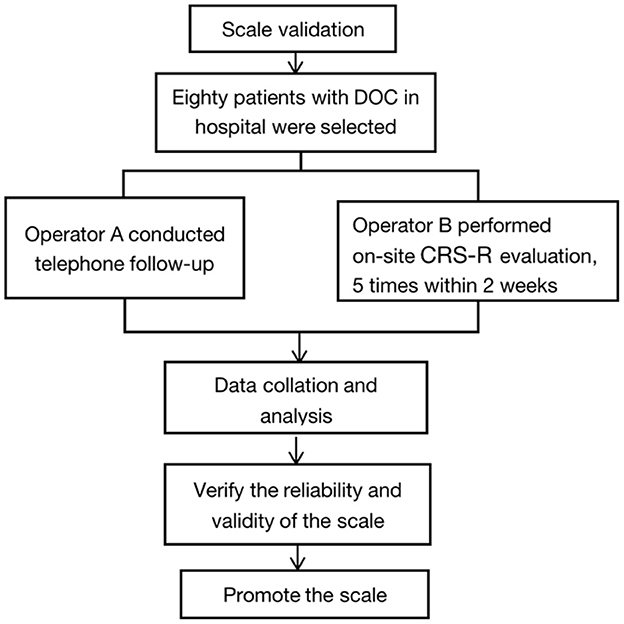
Figure 2. Flow chart of scale validation.
The team members are divided into two groups. One is the study group, consisting of professionally trained researchers and clinicians. The other is the expert group, consisting of researchers and clinicians, doctors, and professional statisticians with over 10 years of experience in DoC research.
DoC telephone follow-up scale will be used to investigate the prognosis and recovery in eight points: awakening, vision, hearing, communication, movement, touch or pain sensation, smell or taste, emotional response, and functional recovery.
The draft of the telephone follow-up scale was developed based on published literature, DoC field-related guidelines, and clinical scales.
The first round was done face-to-face and email communication with the expert group. Firstly, we will briefly introduce the purpose and significance of this study and invite experts to answer the questionnaires, which are divided into two parts: The first part is the preliminary framework of the telephone follow-up program for DoC patients' consciousness recovery (see Appendix 1). The second part is the questionnaire of experts (see Appendix 2). In the questionnaire, experts will score the importance, accuracy, and operability of all indicators of scale items, write corresponding scores in the blanks, and put forward suggestions for modification. And the opinion collation, induction, and statistics.
The language will be revised according to the items determined in the first round. The revised scale and opinions will be fed back to the expert group for the second round of expert consultation. The main content of the second round includes re-evaluation of the selected items and the understanding from patient's family members on such items. The expert opinions of this round will be sorted out, summarized, counted, and fed back again.
The scale will be revised according to the second round of expert feedback. The opinions were synthesized and fed back to the expert group for the third round of expert consultation. After feedback, a study group discussion was conducted to form a second vision telephone follow-up scale.
The pre-survey sample size will be 10–20% of the total sample size. Ten patients will be selected for a pre-test of the telephone follow-up scale at the hospital. The main investigation content includes whether the family members can understand the entry. The result will be used to revise the final version of the telephone follow-up scale. According to the telephone follow-up scale's pre-survey results, the final version of the telephone follow-up scale will be revised.
The formula is “N = [number of variables × (5–10) * (1–15%)]”. According to the Kendall sample size calculation method, the sample size should be 5–10 times the number of independent variables, and a 15% missing rate should be set.
Inclusion criteria: (1) Patients with brain injury for over 28 days. (2) Age between 18 years old and 65 years old. (3) No sedatives administered within 15 days. (4) No fever, infection, or other symptoms occurred within 15 days. (5) The agreement from patients' families on participation in the study with signed informed consent.
Exclusion criteria: (1) The patient has documented dysfunction resulting from developmental psychosis or neurological disease. (2) Patients with untreated epilepsy. (3) Untreated cerebral edema. (4) The patient's vital signs are unstable.
Inclusion criteria: (1) Undertaking primary care of the patients. (2) Age over 18 years. (3) Caregiving time over 3 hours per day. (4) Agree to participate in the study and sign an informed consent form.
Exclusion criteria: (1) Caregivers with cognitive or psychiatric disorders who cannot communicate properly. (2) Those who refused to participate in this study or withdrew during the experimental study.
The primary caregivers of DoC patients are first trained on the scale. The main content of the training includes observation indicators and operation specifications. Family members of discharged patients will receive operation videos to guide their observations. Once the family observed the target behavior, a video was taken and sent to researcher A. After 2 weeks, Investigator A followed up with the patients by telephone or video and diagnosed their consciousness. Investigator B assessed patients face-to-face using CRS-R, the behavioral gold standard.
The project evaluation criteria mainly refer to the CRS-R evaluation criteria for MCS and EMCS. In CRS-R evaluation, functional communication and object use can be diagnosed as EMCS. Reproducible movement to command and object recognition is MCS+. Visual pursuit, automatic motor response and pain localization as MCS-. These behaviors can be observed frequently (more than three times), occasionally or none. Only frequently observed behaviors are rated. For occasionally observed behaviors, the patients will be further observed by their families. The follow up is going to be carried out in every 2 weeks until the patient recovers from EMCS or dies.
The telephone follow-up scale was designed to effectively assess the recovery of DoC patients without the presence of a professional for the face-to-face assessment. Therefore, the diagnosis of consciousness is not based on the total score of the scale but on whether patients show repeatable conscious behavior.
The actual and average use time of telephone follow-up and the satisfaction of patients' family members will be collected.
SPSS 27.0 statistical software will be used for statistical analysis: Calculate Cronbach's α coefficient and half-fold reliability of each dimension and total amount table. Cronbach's α > 0.65 is normal. Cronbach's α > 0.85 is good.
20 of the 80 patients will be selected for evaluation 2 weeks later, and the retest correlation coefficient r will be calculated, ranging from 0 to 1. The closer r is to 1, the higher the retest reliability is.
Five experts in the field of DoC will be invited to evaluate the content validity I-CVI for each item. When the value of I-CVI reached more than 0.78, the research tool is considered to have good content validity.
Cohen Weighted Kappa (22) will be used to assess the correlation between CRS-R and the telephone follow-up scale.
Exploratory factor analysis is performed using principal component analysis and variance maximization orthogonal rotation method. If the cumulative explanation of common factors in the scale is > 50% variation, the number of common factors is consistent with the theoretical hypothesis. The loading value of each item on the corresponding common factors is high (> 0.4), and the loading value on other common factors is low, which can be considered that the scale has good structural validity.
Electrophysiological and imaging methods cannot be used as long-term follow-up tools for DoC patients due to their high cost, complexity, and contraindications. Therefore, behavioral scales remain the most basic assessment tool and have irreplaceable clinical value (23). The CRS-R is currently the most widely used clinical assessment (24) and follow-up tool (25). However, the disadvantage is that it is time-consuming and requires face-to-face evaluation by medical personnel. In addition, evaluating CRS-R in rehabilitation hospitals, community hospitals, and home-based patients is more complicated and time-consuming. In addition, there are currently Glasgow coma scale (GCS) (26), Full outline unresponsive (FOUR) (27), Wessex head injury matrix (WHIM) (28), Sensory modality assessment and rehabilitation technique (SMART) (29), Western neuro sensory stimulation profile (WNSSP) (30) and Disorder of consciousness scale (DOCS) (31) in the field of DoC. Unfortunately, these scales are designed for awareness professionals and cannot meet the needs of family assessment.
Telephone follow-up is a purposeful interactive link between medical staff, patients, and their families using electronic information tools. Implementing a resource-saving follow-up form is easy to promote patients' recovery. Constructing a professional, simple, and feasible Telephone follow-up scale is the key to the effective follow-up implementation. Wannez et al. found in 282 patients with MCS in the behavior of the diagnosis, limiting CRS-R evaluation to the five most observed items (i.e., fixation, visual pursuit, reproducible response to command, automatic motor response, and localization to harmful stimuli) detected in 99% of MCS patients. If clinicians have only limited time to evaluate patients with DoC, we recommend that at least these five items of CRS-R be evaluated.
It has been reported that visual pursuit is very important in distinguishing MCS from VS patients, and the re-emergence of visual pursuit seems to be an early behavioral marker of patients' recovery from VS to MCS (10). This result was also confirmed in 2020. Martens et al. found that visual pursuit was the most common initial sign in their study of consciousness recovery in 79 patients with severe brain injury (18). In 2020, Carriere et al. conducted a multimodal analysis on patients with auditory localization, suggesting that auditory localization is a sign of MCS (17). Previous studies found that compared with VS, MCS patients had a robust perception of pain (32). The Nociception Coma Scale–Revised (NCS-R) was used to study the pain behavior for DoC patients (33), and it was found that patients' response to pain stimuli can effectively evaluate the state of consciousness for DoC patients (19).
Autonomic movement is a conscious behavior that we often observe. For example, DoC patient may scratch bedcovers, the nasal tube or catheter, and the body. These behaviors are triggered when the elementary sensory cortex detects an object touch or an external (e.g., object entering the visual field) stimulus. Neural signals are then sent downstream to the association cortex for further sensory encoding (e.g., what object is this) eventually reaching the motor cortex, which initiates specific motor sequences associated with the triggering stimulus (e.g., grasping the object).These processing steps indicate that awareness of self and environment must be preserved for such behaviors to be performed (18). Individual studies were confirmed in a study by Rem et al. who conducted an autonomous movement study in patients who had a stroke and found that patients who could cross their legs while sitting had significantly better post-injury recovery (34). Using these validated sensitive indicators as the main indicators of the telephone follow-up scale for DoC patients may increase the effectiveness of telephone follow-up.
Many recent studies have shown that the involvement of family members (35, 36) and home environment can enhance patients' awareness of behavioral performances. Due to the familiarity of patients' preference (37), patients' families can adopt more personalized stimulation. The deeper participation of family caregivers, the more observed subtle changes from patients. These cannot be replaced by medical staffs, so we should give full play to the role of patient's family members in the evaluation, to reduce the misdiagnosis rate of behavior evaluation.
In addition, communication by telephone also strengthens the link between patients and medical staff. It also has a guiding role in rehabilitating patients at home and in the community. A 2021 study on traumatic brain injury by Sebastiaan et al. found consistency in GOS-E test results for face-to-face, and telephone extensions (38). It indicated that telephone assessment was an effective alternative to face-to-face where this was not feasible. In addition, the telephone scale form is also convenient to use in the hospital environment. Using a telephone scale for follow-up can save time and timely understand the recovery status of patients.
A limitation of this study is that we included only behavioral indicators that have been proven repeatedly, while some promising new indicators that are being promoted, such as auditory localization (17); habituation of auditory startle reflex (39); spontaneous eye blinking (40); resistance to eye-opening; olfactory stimulation (20) still needs to be verified in larger samples and multi-center environments, so it is not included. In addition, being sensitive, simple, and easy to operate for family members is a very important goal of the telephone follow-up scale.
Currently, most patients are in an environment with insufficient medical resources. Through telephone communication with patients' family members, patients' subtle changes can be timelier understood, and health guidance can be given to them. In this study, observing patients' family members and diagnosing professional evaluators will be used to enhance the objectivity of consciousness assessment.
The studies involving human participants were reviewed and approved by the Hangzhou Normal University (No. 2022044). The patients/participants provided their written informed consent to participate in this study.
FS and JW conceived and designed the study. FS wrote the protocol and manuscript. WH and LC participated in the discussion of the study protocol. HD and SL substantially contributed to study supervision. All authors contributed to the article and approved the submitted version.
This work was supported by the National Natural Science Foundation of China (Grant no. 81920108023).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1071008/full#supplementary-material
1. Bruno MA, Vanhaudenhuyse A, Thibaut A, Moonen G, Laureys S. From unresponsive wakefulness to minimally conscious PLUS and functional locked-in syndromes: recent advances in our understanding of disorders of consciousness. J Neurol. (2011) 258:1373–84. doi: 10.1007/s00415-011-6114-x
2. Giacino JT, Ashwal S, Childs N, Cranford R, Jennett B, Katz DI, et al. The minimally conscious state: definition and diagnostic criteria. Neurology. (2002) 58:349–53. doi: 10.1212/WNL.58.3.349
3. Giacino JT, Schnakers C, Rodriguez-Moreno D, Kalmar K, Schiff N, Hirsch J. Behavioral assessment in patients with disorders of consciousness: gold standard or fool's gold? Prog Brain Res. (2009) 177:33–48. doi: 10.1016/S0079-6123(09)17704-X
4. Seel RT, Sherer M, Whyte J, Katz DI, Giacino JT, Rosenbaum AM, et al. Assessment scales for disorders of consciousness: evidence-based recommendations for clinical practice and research. Arch Phys Med Rehabil. (2010) 91:1795–813. doi: 10.1016/j.apmr.2010.07.218
5. Giacino JT, Kalmar K, Whyte J. The JFK Coma Recovery Scale-Revised: measurement characteristics and diagnostic utility. Arch Phys Med Rehabil. (2004) 85:2020–9. doi: 10.1016/j.apmr.2004.02.033
6. Di H, He M, Zhang Y, Cheng L, Wang F, Nie Y, et al. Chinese translation of the Coma recovery scale-revised. Brain Inj. (2017) 31:363–5. doi: 10.1080/02699052.2016.1255780
7. Zhang Y, Wang J, Schnakers C, He M, Luo H, Cheng L, et al. Validation of the Chinese version of the coma recovery scale-revised (CRS-R). Brain Inj. (2019) 33:529–33. doi: 10.1080/02699052.2019.1566832
8. Wannez S, Heine L, Thonnard M, Gosseries O, Laureys S. The repetition of behavioral assessments in diagnosis of disorders of consciousness. Ann Neurol. (2017) 81:883–9. doi: 10.1002/ana.24962
9. Zou B, Li X, Huang X, Xiong D, Liu Y. Telephone follow-up design and practice for advanced cancer pain patients. J Cancer Educ. (2020) 35:751–9. doi: 10.1007/s13187-019-01523-4
10. Bakker WJ, Roos MM, Kerkman T, Burgmans JPJ. Experience with the PINQ-PHONE telephone questionnaire for detection of recurrences after endoscopic inguinal hernia repair. Hernia. (2019) 23:685–91. doi: 10.1007/s10029-019-01909-9
11. Kuprasertkul A, Christie AL, Zimmern P, A. standardized telephone interview with validated questionnaires for very long-term evaluation of women lost to follow-up after a stress urinary incontinence procedure. Low Urin Tract Symptoms. (2021) 13:366–71. doi: 10.1111/luts.12378
12. Danko KJ, Dahabreh IJ, Ivers NM, Moher D, Grimshaw JM. Contacting authors by telephone increased response proportions compared with emailing: results of a randomized study. J Clin Epidemiol. (2019) 115:150–9. doi: 10.1016/j.jclinepi.2019.05.027
13. Thakkar J, Kurup R, Laba TL, Santo K, Thiagalingam A, Rodgers A, et al. Mobile telephone text messaging for medication adherence in chronic disease: a meta-analysis. JAMA Intern Med. (2016) 176:340–9. doi: 10.1001/jamainternmed.2015.7667
14. Xin Y, Li X, Du J, Cheng J, Yi C, Mao H. Efficacy of telephone follow-up in children tonsillectomy with day surgery. Indian J Pediatr. (2019) 86:263–6. doi: 10.1007/s12098-018-2813-y
15. Rochette C, Michallet AS, Malartre-Sapienza S, Rodier S. Telephone follow-up of oncology patients: the contribution of the nurse specialist for a Service-Dominant Logic in hospital. BMC Health Serv Res. (2021) 21:580. doi: 10.1186/s12913-021-06552-8
16. Qiao J, Liu X, Shan Y. Research progress of telephone follow-up in continuing care of discharged patients. J Nurs Sci. (2012) 27:95–7. doi: 10.3969/j.isn.1672-5921.2009.12.002
17. Carrière M, Cassol H, Aubinet C, Panda R, Thibaut A, Larroque SK, et al. Auditory localization should be considered as a sign of minimally conscious state based on multimodal findings. Brain Commun. (2020) 2:fcaa195. doi: 10.1093/braincomms/fcaa195
18. Martens G, Bodien Y, Sheau K, Christoforou A, Giacino JT. Which behaviours are first to emerge during recovery of consciousness after severe brain injury? Ann Phys Rehabil Med. (2020) 63:263–9. doi: 10.1016/j.rehab.2019.10.004
19. Cortese MD, Arcuri F, Nemirovsky IE, Lucca LF, Tonin P, Soddu A, et al. Nociceptive response is a possible marker of evolution in the level of consciousness in unresponsive wakefulness syndrome patients. Front Neurosci. (2021) 15:771505. doi: 10.3389/fnins.2021.771505
20. Wang J, Zhang S, Liu W, Zhang Y, Hu Z, Sun Z, et al. Olfactory stimulation and the diagnosis of patients with disorders of consciousness: a double-blind, randomized clinical trial. Front Neurosci. (2022) 16:712891. doi: 10.3389/fnins.2022.712891
21. Arzi A, Rozenkrantz L, Gorodisky L, Rozenkrantz D, Holtzman Y, Ravia A, et al. Olfactory sniffing signals consciousness in unresponsive patients with brain injuries. Nature. (2020) 581:428–33. doi: 10.1038/s41586-020-2245-5
22. Vetter TR, Schober P. Agreement analysis: what he said, she said vs. you said. Anesth Analg. (2018) 126:2123–8. doi: 10.1213/ANE.0000000000002924
23. Gao D, Su Y, Zhang Y, Wang L, Gao R, Zhao J, et al. Prognostic prediction of acute stroke patients with disturbance of consciousness by different coma scales. Chin J Cerebrovasc Dis. (2009) 6:620–5. doi: 10.3870/hlxz.2012.20.095
24. Wang J, Hu X, Hu Z, Sun Z, Laureys S, Di H. The misdiagnosis of prolonged disorders of consciousness by a clinical consensus compared with repeated coma-recovery scale-revised assessment. BMC Neurol. (2020) 20:343. doi: 10.1186/s12883-020-01924-9
25. Wang F, He Y, Qu J, Xie Q, Lin Q, Ni X, et al. Enhancing clinical communication assessments using an audiovisual BCI for patients with disorders of consciousness. J Neural Eng. (2017) 14:046024. doi: 10.1088/1741-2552/aa6c31
26. Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale Lancet. (1974) 2:81–4. doi: 10.1016/S0140-6736(74)91639-0
27. Wijdicks EF, Bamlet WR, Maramattom BV, Manno EM, McClelland RL. Validation of a new coma scale: the FOUR score. Ann Neurol. (2005) 58:585–93. doi: 10.1002/ana.20611
28. Shiel A, Horn SA, Wilson BA, Watson MJ, Campbell MJ, McLellan DL. The Wessex Head Injury Matrix (WHIM) main scale: a preliminary report on a scale to assess and monitor patient recovery after severe head injury. Clin Rehabil. (2000) 14:408–16. doi: 10.1191/0269215500cr326oa
29. Wilson SL, Gill-Thwaites H. Early indication of emergence from vegetative state derived from assessments with the SMART—a preliminary report. Brain Inj. (2000) 14:319–31. doi: 10.1080/026990500120619
30. Ansell BJ, Keenan JE. The Western Neuro Sensory Stimulation Profile: a tool for assessing slow-to-recover head-injured patients. Arch Phys Med Rehabil. (1989) 70:104–8. doi: 10.1037/t28459-000
31. Pape TL, Tang C, Guernon A, Lundgren S, Blahnik M, Wei Y, et al. Predictive value of the disorders of consciousness scale (DOCS). Pmr. (2009) 1:152–61. doi: 10.1016/j.pmrj.2008.11.002
32. Pistoia F, Sacco S, Sarà M, Carolei A. The perception of pain and its management in disorders of consciousness. Curr Pain Headache Rep. (2013) 17:374. doi: 10.1007/s11916-013-0374-3
33. Wang J, Di H, Hua W, Cheng L, Xia Z, Hu Z, et al. A study of the reliability and validity of the Chinese version of the nociception coma scale-revised. Clin Rehabil. (2020) 34:1112–21. doi: 10.1177/0269215520927445
34. Rémi J, Pfefferkorn T, Owens RL, Schankin C, Dehning S, Birnbaum T, et al. The crossed leg sign indicates a favorable outcome after severe stroke. Neurology. (2011) 77:1453–6. doi: 10.1212/WNL.0b013e318232abe4
35. Sattin D, Giovannetti AM, Ciaraffa F, Covelli V, Bersano A, Nigri A, et al. Assessment of patients with disorder of consciousness: do different Coma Recovery Scale scoring correlate with different settings? J Neurol. (2014) 261:2378–86. doi: 10.1007/s00415-014-7478-5
36. Formisano R, Contrada M, Aloisi M, Ferri G, Schiattone S, Iosa M, et al. Nociception Coma Scale with personalized painful stimulation vs. standard stimulus in non-communicative patients with disorders of consciousness. Neuropsychol Rehabil. (2020) 30:1893–904. doi: 10.1080/09602011.2019.1614464
37. Sattin D, Magnani FG, Cacciatore M, Leonardi M. Towards a new assessment tool for caregivers of patients with disorders of consciousness: the social and family evaluation scale (SAFE). Brain Sci. (2022) 12:323. doi: 10.3390/brainsci12030323
38. Bossers SM, van der Naalt J, Jacobs B, Schwarte LA, Verheul R, Schober P. Face-to-face vs. telephonic extended glasgow outcome score testing after traumatic brain injury. J Head Trauma Rehabil. (2021) 36:E134–e8. doi: 10.1097/HTR.0000000000000622
39. Hermann B, Salah AB, Perlbarg V, Valente M, Pyatigorskaya N, Habert MO, et al. Habituation of auditory startle reflex is a new sign of minimally conscious state. Brain. (2020) 143:2154–72. doi: 10.1093/brain/awaa159
Keywords: disorders of consciousness, prognosis, follow-up tool, telephone follow-up, diagnosis
Citation: Shou F, Wang J, Laureys S, Cheng L, Huang W and Di H (2023) Study protocol: Developing telephone follow-up scale for patients with disorders of consciousness. Front. Public Health 11:1071008. doi: 10.3389/fpubh.2023.1071008
Received: 15 October 2022; Accepted: 06 March 2023;
Published: 30 March 2023.
Edited by:
Błazej Cieślik, Jan Długosz University, PolandReviewed by:
Guoyi Gao, Shanghai General Hospital, ChinaCopyright © 2023 Shou, Wang, Laureys, Cheng, Huang and Di. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Haibo Di, aGFpYm9kaUBoem51LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.