 Abd El Hamied Ibrahim El Sayed1
Abd El Hamied Ibrahim El Sayed1 Mohamed T. Said
Mohamed T. Said Mohamed Salama
Mohamed Salama
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 26 January 2023
Sec. Aging and Public Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1068314
This article is part of the Research Topic Active and Healthy Aging and Quality of Life: Interventions and Outlook for the Future View all 53 articles
Introduction: Falling is a major health problem among old age persons and are the sixth cause of mortality and morbidity among them. Assessing the prevalence of falls among elderly in an Egyptian community and investigating its associated risk factors using the Arabic translation of the SHARE-Questionnaire.
Subjects and methods: This cross-sectional analytic study was a part of the pilot for AL-SEHA project. It included 289 old age people (50+ years age) residing in the study areas. The main project data were collected using the Arabic translation of the SHARE (Survey of Health, Aging, and Retirement in Europe) questionnaire. The original project data were collected by investigators from five universities, then uploaded to the internet server domain of the American University in Cairo (AUC) Social Research Center.
Results: The prevalence of falls was 11.07% (95% CI: 7.95–15.21). Falls were significantly more among 70 years or older (p < 0.001), unemployed or housewives (p = 0.026), have a family caregiver (p = 0.022), and home facilities for disability (p = 0.015). They had significantly higher rates of ischemic heart disease, hypertension, dyslipidemia, stroke, and diabetes mellitus. The most frequently reported problems were the fear of fall and dizziness (62.5%). The multivariate analysis identified the history of stroke and diabetes mellitus, the fear of fall and dizziness, and the total number of health problems and the score of difficulty in performing physical activities as significant independent predictors of fall occurrence. The history of stroke was the strongest risk factor (OR 33.49, CI: 3.45–325.40).
Discussion and recommendations: The prevalence of falls among old age persons in the studied community is not alarmingly high. It is highest among stroke patients. Community interventions and rehabilitation programs are recommended to train and educate old age people, especially those at risk such as stroke and diabetic patients, and those with dizziness to improve their physical fitness and reduce the fear of fall among them.
Falling is a common incident and a major health problem among old age persons. The World Health Organization (WHO) reports indicate that worldwide more than half-million falls with fatality occur yearly, mostly among persons 65 years age or older (1). Falls and consequent injuries and associated complications are the sixth cause of mortality and morbidity among elderly. They account for more than one-third of all deaths due to injuries and are a leading cause of related mortality among those 65 years or older in the United States. Moreover, approximately one-third of the old age persons 65 years or older and living in community dwellings experience one fall incident per year (2). The problem has deleterious consequences on fallers, their families, and the community at large (3).
Research addressing falls in old age attributes its high incidence to a combination of several intrinsic as well as extrinsic factors (4). Among the intrinsic risk factors identified are those related to old age persons' health status often associated with chronic diseases and polypharmacy, in addition to visual, auditory, and equilibrium problems, as well as the psychological disorders as the symptoms of depression. The extrinsic factors are mostly related to environmental hazards (5, 6).
Several environmental factors have been identified as risk factors underlying falls in the old age population (7). Among these are the slippery floors whether ceramic or old rugs, tripping obstacles, and poor lighting. Other factors include disordered furniture, ill-designed footsteps, broken stairs, and lack of handrails (8). Added to these are the lack of safety measures like grab rails, as well as first-aid and other indoor and outdoor environmental factors (9).
The fear of falling (FOF) has also been identified as an intrinsic factor of considerable importance in the incidence of falling among the elderly. Thus, it has been demonstrated that the prevalence of FOF is significantly higher among those old age persons who experienced falling in comparison with those with no history of falls. Moreover, those who fear falling tend to limit their physical activities and this in turn leads to reduction in their quality of life (10). Furthermore, research showed that the old persons 65 years or older with history of falls have a higher probability of falling again (2).
Falling and consequent injuries and complications among old age people constitute a major burden for them, their caregivers, the society, as well as the system of healthcare. The problem gains more importance with the demographic changes in Egypt with increasing numbers and proportion of elderly in the population. Thus, measuring the magnitude of the problem and identifying its underlying risk factors is of importance in mitigating such burden.
This study is a part of the pilot of the Egyptian aging study (AL-SEHA) which is the first of its type in Egypt. The current study aimed at assessing the prevalence of falls among elderly in an Egyptian community and investigating its associated risk factors using the SHARE-Questionnaire. The SHARE survey and its updated questionnaires can be accessed from this link: http://www.share-project.org/home0.html. The research questions are: (1) What is the prevalence of falls among Egyptian old age persons? and (2) What are the significant risk factors associated with these falls? The outcomes of this work should be advising policies to decrease the rate of falling among seniors through understanding of the current situation and risk factors in Egypt.
A cross-sectional analytic study was used where all dependent and independent variables are assessed at one and the same point in time.
The study is a part of a DAAD funded project (Aging in the East Mediteranean Region: Emage) which is piloting the Egyptian Longitudinal Aging Study (AL-SEHA).
Old age people (50+ years age) residing in the study areas constituted the sampling population for the study. The inclusion criteria were being able to communicate, and living independently at home, in rented accommodation, in a hostel, or in a retirement home. Those having a gross psychiatric disturbance were excluded. The sample consisted of 289 old age persons. This sample size was large enough to estimate an expected fall prevalence rate of 11% or higher with 4% absolute precision at 95% level of confidence and 80% power. A non-probability convenience sampling technique was used in recruiting participants according to the eligibility criteria.
The main project data were collected using the Arabic translated version of the SHARE (Survey of Health, Aging, and Retirement in Europe) questionnaire. It was validated by expertise from five Egyptian universities and the Social Research Center (SRC) American university Egypt. This is an extensive interview questionnaire developed by Mehrbrodt et al. (11). It consists of 16 sections covering respondent's personal and family information, health status and physical activity, mental abilities, mental health, health care, work and retirement, physical testing, relations with children, social support, finances, living conditions, family income, family assets, social activities, in addition to two sections for the data collector's views and information.
The original project data were collected by investigators from five universities who were trained in interviewing using the prepared SHARE form translated into Arabic. The sample of eligible old age persons was selected. The investigators in each governorate contacted the potential participants in their area, explained to them the aim of the study and the procedure of data collection. They were invited to participate after being informed about their rights. Those who gave their consent to participate were asked for the suitable time to conduct the interview. At the set time, the investigators visited participants at their homes. They were interviewed using the data collection form. The procedure of data collection lasted for about 1 month. Each investigator was assigned 15 old age person for interviewing. The collected data were then uploaded to the internet server domain of the American University in Cairo (AUC) Social Research Center.
In the present study, data pertaining to the old age persons residing in Beni Suef were extracted from the main project dataset. These data included parts of the personal and family information section such as age, gender, residence, education, etc.; parts of the health status and physical activity section as the history of chronic diseases, health problems, medication administration, vision, and hearing, etc.; mental abilities as recall; mental health as sleep problems; health care utilization; job; physical testing as grip; relations with children as caregiving; as well as the living conditions and facilities.
The data were extracted from the SPSS (Version 25) dataset. Bivariate analyses included chi-squared or Fisher exact tests for the comparison of categorical risk factors between faller and non-faller groups. Numeric data were compared using independent t-tests or Mann-Whitney tests as suitable. Multiple logistic linear regression with backward Wald method and ROC (Receiver Operator Curve) analysis were used to identify the independent risk factors of falling and model its risk. Statistical significance was considered at p < 0.05.
In a sample of 289 seniors, 32 reported fall incidents indicating a prevalence rate of 11.07% (95% CI: 7.95–15.21). Table 1 indicates that the old age people who experienced falls were significantly more among those aged 70 years or older (p < 0.001), unemployed or housewives (p = 0.026), have a family caregiver (p = 0.022), and home facilities for disability (p = 0.015). Their percentages also tended to be higher among females although the difference was not statistically significant (p = 0.170).

Table 1. Comparison of the demographics of old age persons with and without fall history.
As illustrated in Table 2, one-half of the old age persons in both groups were obese. Those in the fall group had significantly poorer visual acuity (p = 0.005) and hearing (p = 0.013), and less exercise frequency (p < 0.001). They also had lower recall rates for words (p = 0.028) with more depression (p = 0.002), use of antidepressants (p = 0.015), more sleep problems (p = 0.001), and hospital admission (p = 0.041). Their scores of difficulty in performing physical and daily life activities were higher (p < 0.001).
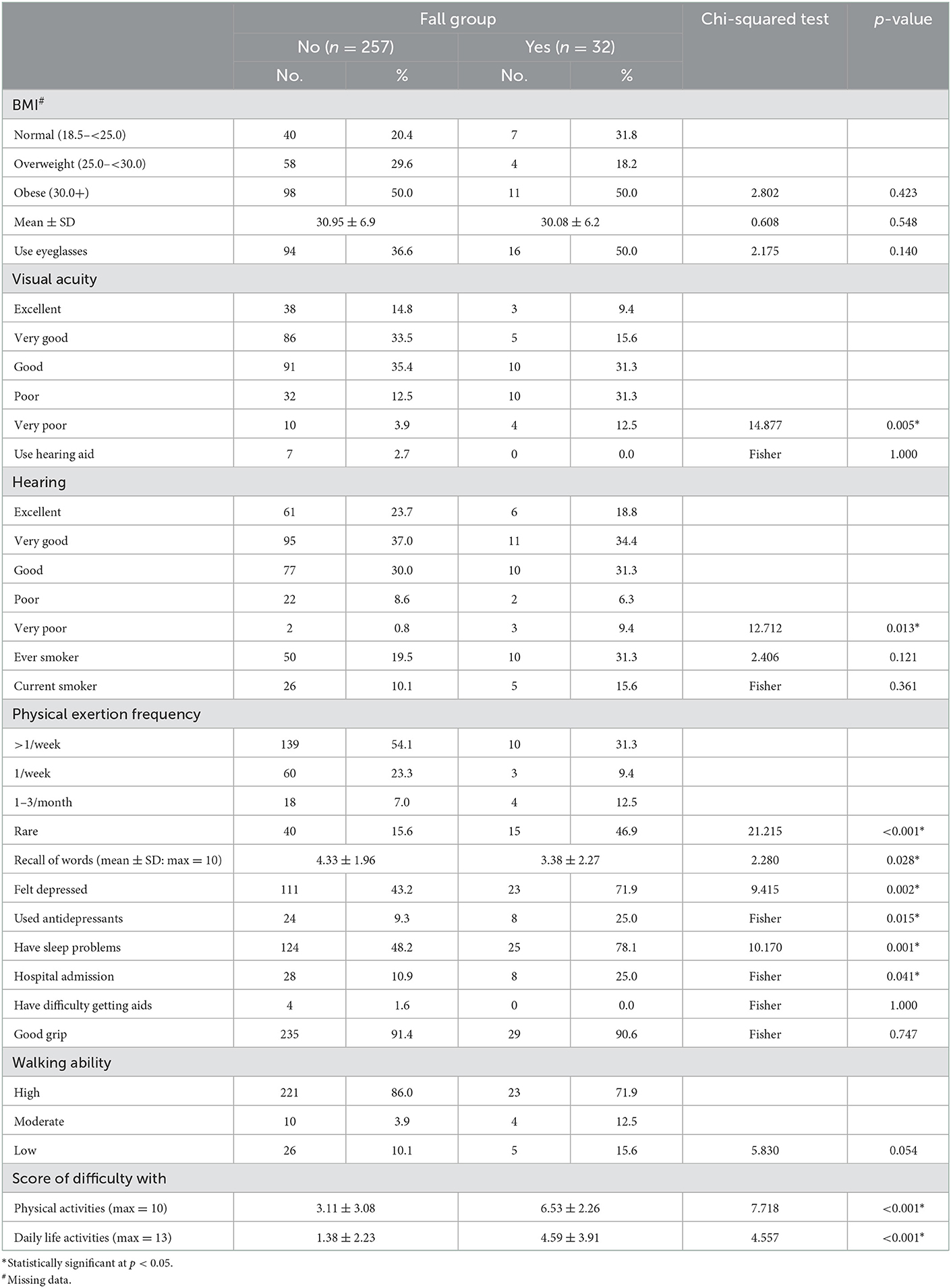
Table 2. Comparison of health status of old age persons with and without fall history.
Table 3 demonstrates that the old age persons in the fall group reported significantly higher rates of ischemic heart disease (p < 0.001), hypertension (p = 0.015), dyslipidemia (p = 0.042), stroke (p = 0.008), and diabetes mellitus (p < 0.001). They also had higher rates of osteoporosis (p = 0.031), cataract (p < 0.001), and arthritis (p < 0.001), in addition to more history of fracture hip (p = 0.016). Overall, the mean number of chronic diseases was higher among them (3.38 ± 1.77) compared with those in the no-fall group (1.74 ± 1.63), and the difference was statistically significant (p < 0.001).
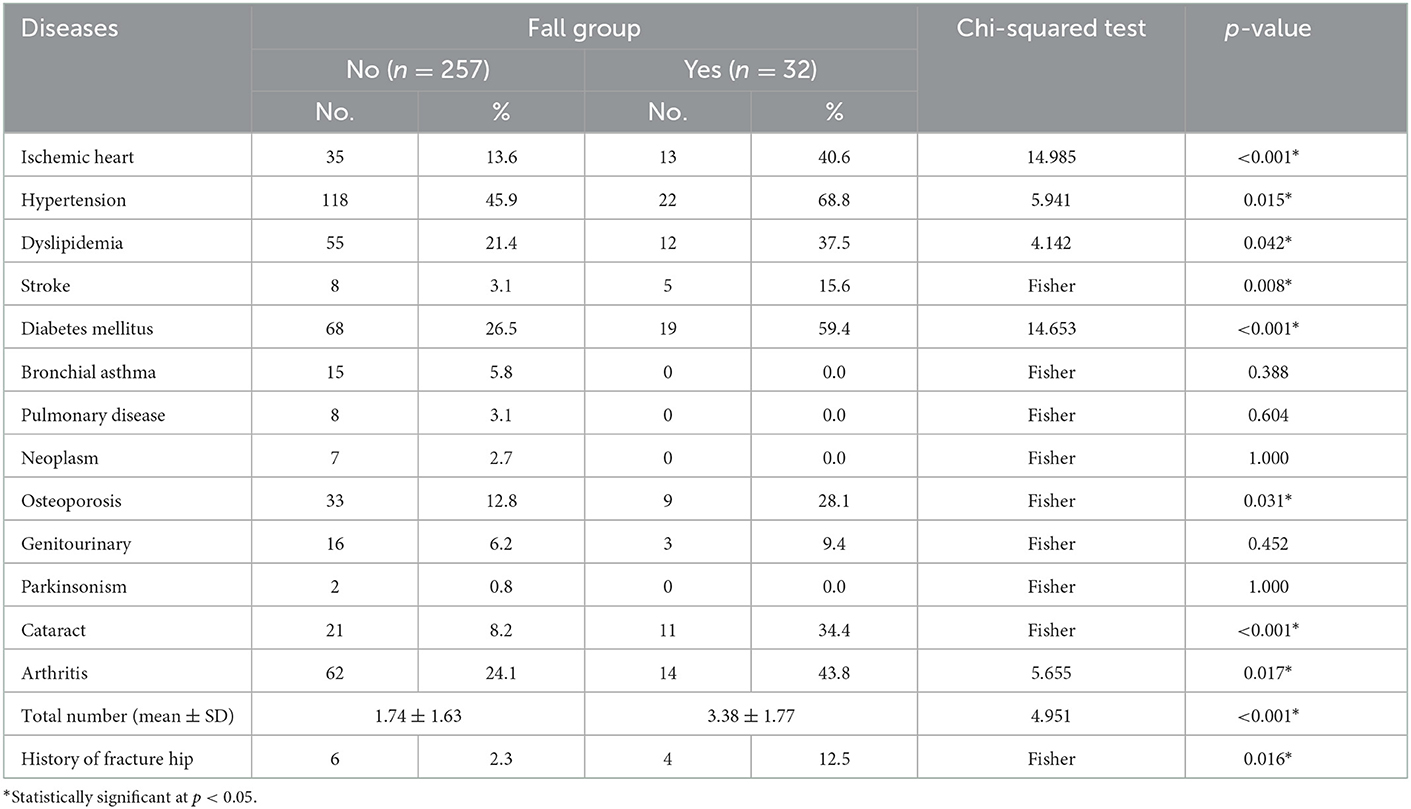
Table 3. Comparison of the prevalence of chronic diseases reported by old age persons with and without fall history.
Concerning the health problems reported by old age persons. Table 4 indicates statistically significantly higher percentages among those in the fall group in all types of problems. The only exception was that of recurrent cough (p = 0.080). The most frequently reported problems among them were the fear of fall and dizziness (62.5%), while the lowest were recurrent cough (15.6%) and incontinence of urine (21.9%). The table shows that all those in the fall group had at least one reported problem compared to 62.3% of those in the no-fall group (p < 0.001). Overall, the mean number of health problems was higher among those in the fall group (5.34 ± 1.81) compared with those in the no-fall group (1.39 ± 1.53), and the difference was statistically significant (p < 0.001).
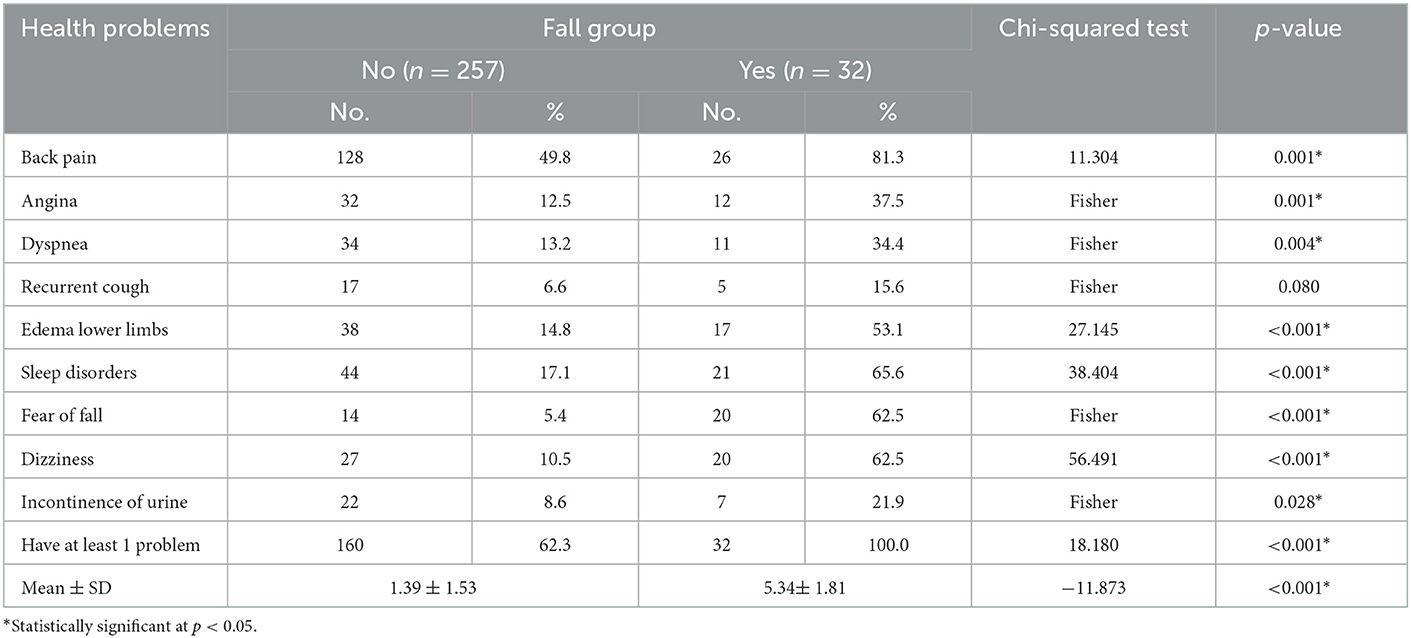
Table 4. Comparison of health problems reported by old age persons with and without fall history.
Similarly, the old age persons in the fall group had higher percentages of administration of almost all types of medications, reaching statistical significance regarding medications for IHD and other cardiac diseases (p = 0.001), diabetes (p < 0.001), arthritis (p = 0.010), analgesia (p = 0.005), and bronchitis (p = 0.035) as presented in Table 5. The table also indicates that all those in the fall group had at least one medication administered compared to 78.2% of those in the no-fall group (p = 0.003). Overall, the mean number of medications was higher among those in the fall group (4.00 ± 2.09) compared with those in the no-fall group (2.16 ± 1.96), and the difference was statistically significant (p < 0.001).
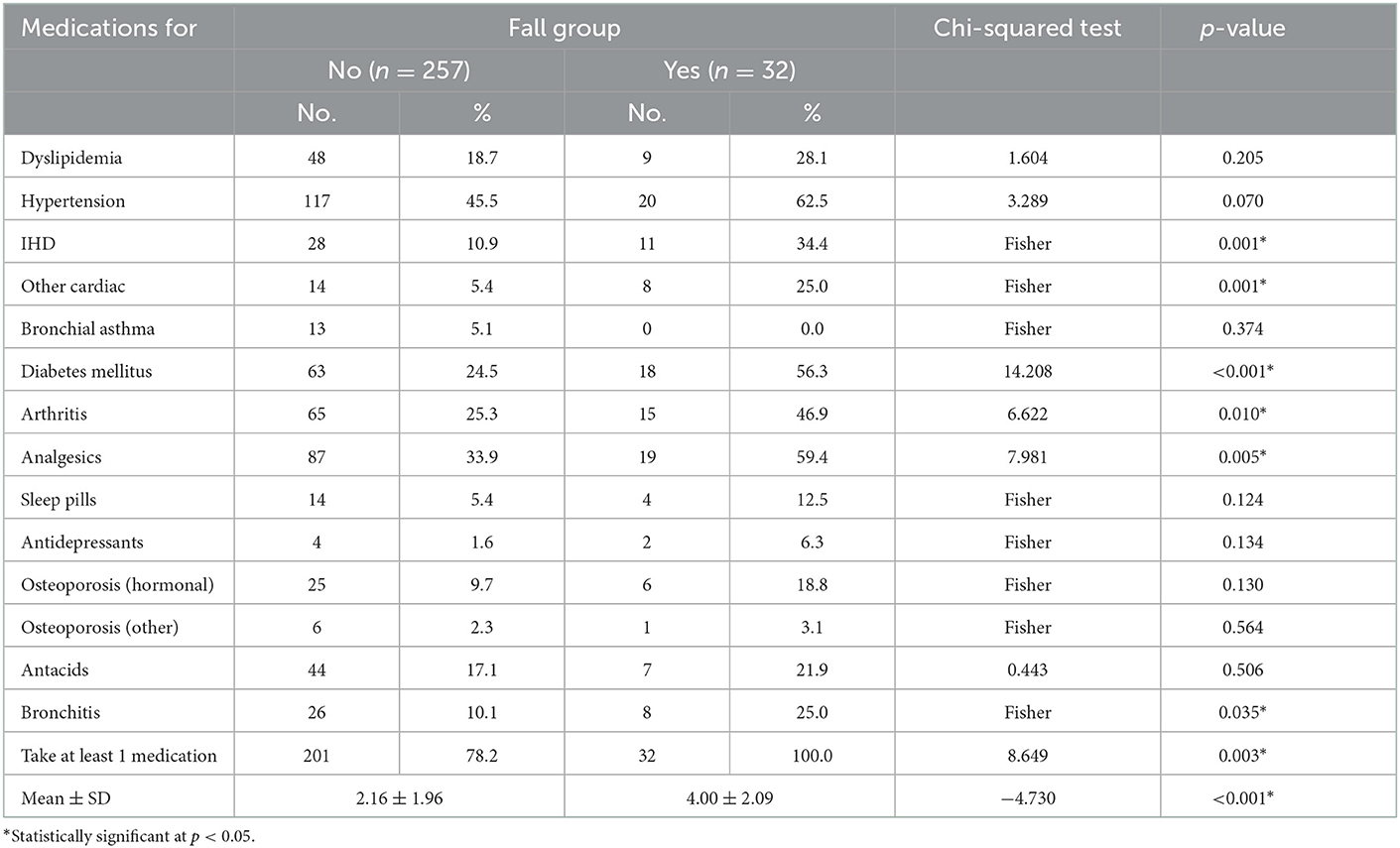
Table 5. Comparison of the administration of medications as reported by old age persons with and without fall history.
The multivariate analysis (Table 6) demonstrates that the statistically significant independent predictors of fall occurrence are the history of stroke and diabetes mellitus, the fear of fall and dizziness, in addition to the total number of health problems and the score of difficulty in performing physical activities. It is evident that the history of stroke is the strongest risk factor for falling, increasing its risk more than 33 folds (OR 33.49, CI: 3.45–325.40).
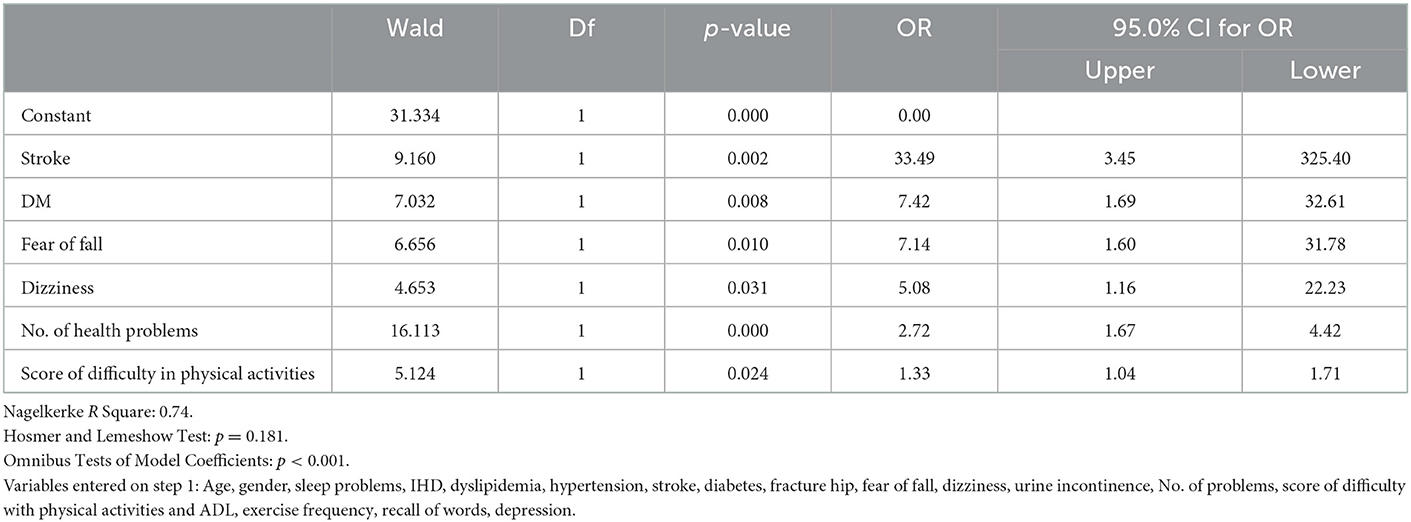
Table 6. Best fitting multiple logistic regression model for the occurrence of fall.
This study was aimed at assessing the prevalence of falls among elderly in an Egyptian community and investigating its associated risk factors using the SHARE-Questionnaire. The findings indicate a relatively high prevalence, with stroke being the most important risk factor underlying falls in this population.
According to the current study results, slightly more than one-tenth of the old age persons in the sample gave a positive history of previous fall incidents. This is quite a high rate that needs to be addressed carefully given its untoward consequences on the elderly person and his/her family, as well as the whole community and health care system. Nonetheless, the rate is still lower than that reported by Geetha et al. (12) in a study of fall risk in India who reported a rate 27.6%. This discrepancy might be due to that the Indian study was in a rural area, and the age of their participants was older in comparison with our study. Similarly, a study in China reported a prevalence rate of 20.65 among elderly persons living in rural and urban community dwellings (13). Their age group was also more than one decade older in comparison with the present study.
The bivariate analyses of the current study identified significant associations between certain old age persons' age, and being unemployed, retired, or housewife. Additionally, there was a trend of higher prevalence among women. In agreement with this, a study in New Zealand found significant associations with older age and female gender (14). On the same line, Guerreiro et al. (15) in a study in Spain demonstrated that female gender was a significant predictor of falls among old age people. However, the multivariate analysis could not confirm a significant independent role in the risk of falling.
Meanwhile, factors related to old age persons' health status and identified in bivariate analyses as having significant associations with the occurrence of falls were poor vision and hearing, lack of physical activity, sleep problems, inadequate recall, depression symptoms, and previous hospital admission. In addition, the difficulty in performing physical and daily life activities was a significant risk factor. These are all indicative of poorer health status that may lead to higher risk for accidents and injuries. They also reflect a low physical fitness leading to inability to prevent falling in case of stumbling or losing equilibrium. Similar associations between old age persons' falls and poor vision or hearing impairment (16, 17), sleep disorders (18), depression (19), and impaired recall and mental abilities (20) were previously reported.
Nevertheless, only the score of difficulty in performing physical activity was identified in the present study multivariate model as a significant independent risk factor of falling among old age persons. This would undoubtedly be due to that this score is the summative outcome of poor physical health. In congruence with this, several systematic reviews with meta-analyses provided a strong evidence of the positive effect of exercise training interventions in decreasing the risk of falling among old age people (21–23). Moreover, exercise interventions associated with lifestyle changes proved to have a high effectiveness in reducing the risk of falling in the elderly (24).
Concerning the health problems related to the occurrence of fall incidents among old age persons, the current study bivariate analyses demonstrated significant associations with their affection by certain chronic ailments such as ischemic heart disease, hypertension, dyslipidemia, stroke, and diabetes mellitus, as well as osteoporosis, cataract, arthritis, and history of fracture hip. These chronic conditions certainly have negative impacts on the elderly' physical and mental abilities, thereby increasing their risk of falling. In fact, the number of health problems was identified in the multivariate analyses as an independent significant positive predictor of the risk of falling. The findings are in agreement with a recent study in China that examined the relation between the number of chronic diseases and falling in the elderly population (25).
The multivariate analysis also identified stroke and diabetes mellitus as significant independent predictors of falling among old age persons. The influence of stroke is quite understandable given its negative impacts on the affected person's physical as well as mental abilities. In congruence with this, a study in Japan identified stroke as an independent predictor of the risk of falling among elderly (26). As for diabetes mellitus, it might increase the risk of falling due to associated neuropathy that may make the diabetic person more vulnerable to accidents and injuries. Moreover, diabetic patients may have impaired reactive balance to disequilibrium as demonstrated in a study in the United States, thus increasing their risk of falling (27).
The present study bivariate analyses also showed that the old age persons in the fall group reported significantly higher rates of almost all symptoms related to various chronic diseases. This again reflects their poor health status. However, the only symptom confirmed in the multivariate analysis was that of dizziness. This is quite conceivable given that it can lead to disequilibrium and the old age person is often unable to rapidly regain his/her equilibrium and his/her physical fitness and abilities cannot help in preventing falling. Similar significant relations between dizziness and the risk of falling among elderly were reported in studies in Sweden (28) and Greece (29).
The fear of fall (FOF) was also identified as a major factor affecting the occurrence of falls among the old age persons in the present study. Its role was evident both in bivariate and multivariate analyses. It may act through limiting the old person's physical activities, thus leading to low physical fitness and weak muscles, and may lead to frailty and even sarcopenia. In line with this, a study of elderly in Iran clarified that the fear of fall among them is associated with disturbance of their activities of daily living, with consequent negative impact on their quality of life (30). Furthermore, Qin et al. (31) in a study in China demonstrated a significant association between FOF and frailty among old age people.
The current study results revealed that the old age persons who experienced falling had higher rates of medication use compared with the non-fallers in the bivariate analyses. They also had higher rates of administration of polypharmacy. The influence of polypharmacy as a risk factor predicting falls in the old age people has been previously documented in the literature (32, 33). Yet, the effect of polypharmacy on the occurrence of fall was not confirmed in the current study multivariate analysis. This might be explained by that the effect of the disease itself as stroke or diabetes mellitus was more important than that of related medications.
The present study multivariate regression analysis produced a model that depends on the history of stroke and diabetes mellitus, the fear of fall and dizziness, the total number of health problems and the score of difficulty in performing physical activities. A similar model was developed by Gade et al. (28) in Denmark. The risk factors included in their model were old age person's level of education, feeling dizzy, alcohol intake, history of previous falls, perceived risk of falling, disabilities, and symptoms of depression. The differences with the present study model might be attributed to the differences in the study designs, where the Denmark study was a cohort one, in addition to the socio-demographic differences between the two studies such as the level of education and alcohol consumption. However, as highlighted by Seaman et al. (34), the development of predictive fall models for the elderly is still in “its infancy.” Thus, more research is needed.
Our study has some limitations that could jeopardize its generalizability to the whole Egyptian population. Firstly, the inclusion of participants in the fifth decade of age could make the study results not comparable to many old age studies. Secondly, the convenience sampling could have led to bias in the level of education, which might not reflect the true population figures. Lastly, the sample size was calculated using a relatively large margin of error, which might have led to a small sample size for a prevalence study; however, the sample size was large enough for the multivariate analysis.
The prevalence of falls among old age persons in the studied community is not alarmingly high, yet it could be reduced since the target should be “no-falls.” The risk is highest among stroke patients. The study recommends rehabilitation & community interventions to train and educate old age people, especially those at risk such as stroke and diabetic patients, and those with dizziness to improve their physical fitness and reduce the fear of fall among them. The developed prediction model needs to be validated through longitudinal studies.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by IRB of the American University in Cairo (IRB-AUC). The patients/participants provided their written informed consent to participate in this study.
AE, MS, OM, and AA: drafted the first version, conceptualized the idea, conducted data collection, and analysis. MS: funding, conceptualization, and final revision. All authors contributed to the article and approved the submitted version.
The present work has been supported by the German Academic Exchange Services (DAAD), through the funding program: Higher Education Dialogue with the Muslim World, project (Aging in the East Mediterranean Region: EMage), Pilot grant from Alzheimer's Association (AA), and the Global Brain Health Institute (GBHI).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. WHO: Falls. Available online at: https://www.who.int/news-room/fact-sheets/detail/falls (accessed January 17, 2023).
2. Kang GE, Naik AD, Ghanta RK, Rosengart TK, Najafi B. A wrist-worn sensor-derived frailty index based on an upper-extremity functional test in predicting functional mobility in older adults. Gerontology. (2021) 67:753–61. doi: 10.1159./000515078
3. Stina EK, Rizzuto D, Xu W, Calderón-Larrañaga A, Welmer AK. Predictors for functional decline after an injurious fall: a population-based cohort study. Aging Clin Exp Res. (2021) 33:2183–90. doi: 10.1007/s40520-020-01747-1
4. American Nurse Today. Health Com Media c2019. Assessing your patients' risks for falling. (2019). Available online at: https://www.americannursetoday.com/assessing-patients-risk-falling (accessed October 26, 2019).
5. Gale CR, Westbury LD, Cooper C, Dennison EM, Gale CR. Risk factors for incident falls in older men and women: the English longitudinal study of ageing. BMC Geriatr. (2018) 18:117. doi: 10.1186/s12877-018-0806-3
6. da Silva LP, Moreira NB, de Freitas PB, Pereira G, Rodacki AL. Gait parameters of older adults according to their fall history and functional capacity while walking at different speeds. Gerontology. (2021) 67:532–43. doi: 10.1159/000513601
7. Alex D, Khor HM, Chin AV, Hairi NN, Cumming RG, Othman S, et al. Factors associated with falls among urban-dwellers aged 55 years and over in the Malaysian elders longitudinal research (MELoR) study. Aging Public Health. (2020) 3:6238. doi: 10.3389./fpubh.2020.506238
8. Najafi B, Zhou H, Nguyen H. Gait test or no gait test: do we need walking assessment to determine physical frailty? Gerontology. (2019) 65:311–2. doi: 10.1159/000495984
9. Lee S. Falls associated with indoor and outdoor environmental hazards among community-dwelling older adults between men and women. BMC Geriatr. (2021) 21:547. doi: 10.1186/s12877-021-02499-x
10. Sitdhiraksa N, Piyamongkol P, Chaiyawat P, Chantanachai T, Ratta-Apha W, Sirikunchoat J, et al. Prevalence and factors associated with fear of falling in community-dwelling Thai elderly. Gerontology. (2021) 67:276–80. doi: 10.1159/000512858
11. Mehrbrodt T, Gruber S, Wagner M. Scales and multi-item indicators publication. (2019). Available at: https://www.researchgate.net/publication/323006860 (accessed March 31, 2017).
12. Geetha J, Sakthivadivel V, Gaur A. Assessment of fall risk in elderly rural population. Maedica. (2021) 16:609–14. doi: 10.26574/mae_dica.164.609
13. Chen X, Lin Z, Gao R, Yang Y, Li L. Prevalence and associated factors of falls among older adults between urban and rural areas of Shantou City, China. Int J Environ Res Public Health. (2021) 18:7050. doi: 10.3390/ijerph18137050
14. Abey-Nesbit R, Schluter PJ, Wilkinson TJ, Thwaites JH, Berry SD, Allore H, et al. Risk factors for injuries in New Zealand older adults with complex needs: a national population retrospective study. BMC Geriatr. (2021) 21:630. doi: 10.1186/s12877-021-02576-1
15. Guerreiro C, Botelho M, Fernández-Martínez E, Marreiros A, Pais S. Determining the profile of people with fall risk in community-living older people in algarve region: a cross-sectional, population-based study. Int J Environ Res Public Health. (2022) 19:2249. doi: 10.3390/ijerph19042249
16. Cai Y, Schrack JA, Wang HEJY, Wanigatunga AA, Agrawal Y, Urbanek JK, et al. Visual impairment and objectively measured physical activity in middle-aged and older adults. J Gerontol A Biol Sci Med Sci. (2021) 76:2194–203. doi: 10.1093/gerona/glab103
17. Mehta J, Czanner G, Harding S, Newsham D, Robinson J. Visual risk factors for falls in older adults: a case-control study. BMC Geriatr. (2022) 22:134. doi: 10.1186/s12877-022-02784-3
18. Han C, An J, Chan P. The influence of probable rapid eye movement sleep behavior disorder and sleep insufficiency on fall risk in a community-dwelling elderly population. BMC Geriatr. (2021) 21:606. doi: 10.1186/s12877-021-02513-2
19. van Poelgeest EP, Pronk AC, Rhebergen D, van der Velde N. Depression, antidepressants and fall risk: therapeutic dilemmas-a clinical review. Eur Geriatr Med. (2021) 12:585–96. doi: 10.1007/s41999-021-00475-7
20. Trevisan C, Ripamonti E, Grande G, Triolo F, Ek S, Maggi S, et al. The association between injurious falls and older adults' cognitive function: the role of depressive mood and physical performance. J Gerontol A Biol Sci Med Sci. (2021) 76:1699–706. doi: 10.1093/gerona/glab061
21. Dautzenberg L, Beglinger S, Tsokani S, Zevgiti S, Raijmann RCMA, Rodondi N, et al. Interventions for preventing falls and fall-related fractures in community-dwelling older adults: a systematic review and network meta-analysis. J Am Geriatr Soc69. (2021) 2973–84. doi: 10.1111/jgs.17375
22. Sun M, Min L, Xu N, Huang L, Li X. The effect of exercise intervention on reducing the fall risk in older adults: a meta-analysis of randomized controlled trials. Int J Environ Res Public Health. (2021) 18:12562. doi: 10.3390/ijerph182312562
23. Taylor J, Walsh S, Kwok W, Pinheiro MB, de Oliveira JS, Hassett L, et al. A scoping review of physical activity interventions for older adults. Int J Behav Nutr Phys Act. (2021) 18:82. doi: 10.1186/s12966-021-01140-9
24. Jansen CP, Nerz C, Labudek S, Gottschalk S, Kramer-Gmeiner F, Klenk J, et al. Lifestyle-integrated functional exercise to prevent falls and promote physical activity: results from the LiFE-is-LiFE randomized non-inferiority trial. Int J Behav Nutr Phys Act. (2021) 18:115. doi: 10.1186/s12966-021-01190-z
25. Tang S, Liu M, Yang T, Ye C, Gong Y, Yao L, et al. Association between falls in elderly and the number of chronic diseases and health-related behaviors based on CHARLS 2018: health status as a mediating variable. BMC Geriatr. (2022) 22:374. doi: 10.1186/s12877-022-03055-x
26. Yamashita T, Suzuki S, Inoue H, Akao M, Atarashi H, Ikeda T, et al. 2-year outcomes of more than 30 000 elderly patients with atrial fibrillation: results from the all Nippon AF in the elderly (ANAFIE) registry. Eur Heart J Qual Care Clin Outcomes. (2022) 8:202–13. doi: 10.1093/ehjqcco/qcab025
27. Rosenblatt NJ, Young J, Andersen R, Wu SC, Crews RT. Diabetes and reactive balance: quantifying stepping thresholds with a simple spring scale to measure fall-risk in ambulatory older adults. J Diabetes Sci Technol. (2021) 15:1352–60. doi: 10.1177/1932296820979970
28. Gade GV, Jørgensen MG, Ryg J, Masud T, Jakobsen LH, Andersen S, et al. Development of a multivariable prognostic PREdiction model for 1-year risk of FALLing in a cohort of community-dwelling older adults aged 75 years and above (PREFALL). BMC Geriatr. (2021) 21:402. doi: 10.1186/s12877-021-02346-z
29. Lytras D, Sykaras E, Iakovidis P, Kasimis K, Myrogiannis I, Kottaras A, et al. Recording of falls in elderly fallers in northern greece and evaluation of aging health-related factors and environmental safety associated with falls: a cross-sectional study. Occup Ther Int. (2022) 22:9292673. doi: 10.1155/2022/9292673
30. Zahedian-Nasab N, Jaberi A, Shirazi F, Kavousipor S. Effect of virtual reality exercises on balance and fall in elderly people with fall risk: a randomized controlled trial. BMC Geriatr. (2021) 21:509. doi: 10.1186/s12877-021-02462-w
31. Qin Y, Li J, McPhillips M, Lukkahatai N, Yu F, Li K, et al. Association of fear of falling with frailty in community-dwelling older adults: a cross-sectional study. Nurs Health Sci. (2021) 23:516–24. doi: 10.1111/nhs.12840
32. Abu Bakar AA, Abdul Kadir A, Idris NS, Mohd Nawi SN. Older adults with hypertension: prevalence of falls and their associated factors. Int J Environ Res Public Health. (2021) 18:8257. doi: 10.3390/ijerph18168257
33. Xue L, Boudreau RM, Donohue JM, Zgibor JC, Marcum ZA, Costacou T, et al. Persistent polypharmacy and fall injury risk: the health, aging, and body composition study. BMC Geriatr. (2021) 21:710. doi: 10.1186/s12877-021-02695-9
Keywords: risk factors, old age, Egyptian aging study, falls, AL-SEHA
Citation: El Sayed AEHI, Said MT, Mohsen O, Abozied AM and Salama M (2023) Falls and associated risk factors in a sample of old age population in Egyptian community. Front. Public Health 11:1068314. doi: 10.3389/fpubh.2023.1068314
Received: 12 October 2022; Accepted: 11 January 2023;
Published: 26 January 2023.
Edited by:
Yulan Lin, Fujian Medical University, ChinaReviewed by:
Karim Abu-Omar, University of Erlangen Nuremberg, GermanyCopyright © 2023 El Sayed, Said, Mohsen, Abozied and Salama. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohamed Salama,  TW9oYW1lZC1TYWxhbWFAYXVjZWd5cHQuZWR1; TW9oYW1lZC5zYWxhbWFAZ2JoaS5vcmc=
TW9oYW1lZC1TYWxhbWFAYXVjZWd5cHQuZWR1; TW9oYW1lZC5zYWxhbWFAZ2JoaS5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.