
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 02 February 2023
Sec. Family Medicine and Primary Care
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1058828
This article is part of the Research Topic New Trends in Type 2 Diabetes Diagnosis and Management in Primary Care View all 14 articles
 Ana María Salinas Martínez1,2*
Ana María Salinas Martínez1,2* Angélica Gabriela Juárez Montes1
Angélica Gabriela Juárez Montes1 Yesenia Ramírez Morado3
Yesenia Ramírez Morado3 Hid Felizardo Cordero Franco2
Hid Felizardo Cordero Franco2 Francisco Javier Guzmán de la Garza2,4
Francisco Javier Guzmán de la Garza2,4 Luis Carlos Hernández Oyervides3
Luis Carlos Hernández Oyervides3 Georgina Mayela Núñez Rocha1
Georgina Mayela Núñez Rocha1Introduction: Information on treatment expectations in diabetes is scarce for Mexican and Latino populations. We determined idealistic, realistic, and unrealistic expectations for metformin, insulin, and glyburide in primary care. We also explored the association between sociodemographic attributes, time since diagnosis, and expectations.
Methods: This was a cross-sectional study conducted during 2020–2022 in governmental primary care centers. We consecutively included persons with type 2 diabetes aged 30–70 years under pharmacological medication (n = 907). Questions were developed using information relevant to expectation constructs. Data were collected by interview. We used descriptive statistics, a test of the difference between two proportions, and multivariate ordinal logistic regression.
Results: A high percentage of participants would like to have fewer daily pills/injections or the option of temporarily stopping their medication. Realistic expectations ranged from 47% to 70%, and unrealistic expectations from 31 to 65%. More insulin users wished they could take a temporary break (p < 0.05) or would like to be able to change the route of administration (p < 0.001) than metformin users. More persons with diabetes on insulin expected realistic expectations compared to those on metformin or glyburide (p ≤ 0.01). Being able to interrupt medication upon reaching the glucose goal was higher in combined therapy users (p < 0.001).
Conclusion: Time since diagnosis, place of residence, sex, and diabetes education were factors associated to expectations. Management of expectations must be reinforced in primary care persons with type 2 diabetes undergoing pharmacological medication.
Diabetes is a chronic condition characterized by high blood glucose levels, which, if left untreated, leads to heart, vascular, eye, kidney, and nerve complications. There are two main types of diabetes: type 2 and type 1. The first is initially due to insulin resistance that progresses to loss of adequate insulin secretion by b-cells. Type 1 is an insulin-dependent diabetes, in which the pancreas produces little or no insulin by itself due to autoimmune b-cell destruction (1, 2). Type 2 diabetes is the most common type accounting for over 90% of all diabetes cases worldwide. An estimated 537 million adults aged 20–79 years were living with diabetes in 2021 (10.5% prevalence); 50.5 million in the North America and Caribbean region (14.0% prevalence) and 32.5 million in the South and Central America region (9.5% prevalence). Mexico is among the top 10 countries for diabetes, with 14.1 million people affected (15% prevalence) (2). Regular physical activity, a healthy diet, and a healthy body weight are key factors that must be promoted by public and private health institutions since they are the foundation of type 2 diabetes management. If the adoption of healthy habits does not achieve optimal glucose levels, pharmacotherapy should be initiated. Metformin is one of the first-choice oral medications. If a single diabetes-specific medication does not work, a range of combination therapy options are available (sulfonylureas, thiazolidinediones, and alpha glucosidase inhibitors, among others). Additionally, insulin injections may be needed to reach glycemic goals (3, 4). From 25 to 90% of persons with type 2 diabetes do not take medication as prescribed (5). Differences in managing diabetes expectations between the diabetes care team and persons living with diabetes lead to inconsistencies in taking medication because those who notice no benfit may stop taking them (6). Meeting expectations is important because the individual may think medication does not work (7), and dissatisfied persons are less likely to follow the medication plan or to take an active role in their care (8). The loss of continuity in taking the medication will, in turn, decrease therapeutic efficacy, with consequences on target glucose levels (9–11), hospitalization (5, 10), mortality (5, 12), and high costs (10, 13). Therefore, awareness of personal expectations is essential for healthcare professionals, health managers, and health policymakers.
An expectation refers to the anticipation of the occurrence of a specific outcome. It is a type of belief or perception of a future event. The theory of expectations in psychology maintains that they are the product of a cognitive process dependent on experience and social learning (14, 15). The individual compares what is anticipated with what is received and confirms or modifies his/her expectations. He/she also compares results with other individuals, medications, and health conditions (7, 16). There are structural (e.g., tablet shape and color) and process (e.g., medication procedure) expectations. For instance, an injectable medication may be anticipated to be more effective than an oral one, or a medicine prescribed by a cardiologist may be anticipated to be more effective than one prescribed by a general practitioner (15). Expectations can be idealistic (what the person wants or prefers if given the choice), unrealistic (myth or fantasy), or realistic (predictive). Moreover, realistic expectations can be positive (e.g., symptom relief, hospitalization prevention, goal achievement) or negative (e.g., adverse effect experience) (7, 14, 15, 17). The literature on realistic expectations show 70% of persons living with diabetes on oral medication anticipate the benefit of achieving target glucose levels and only 11.7% expect a reduction in the risk of complications (18). One study found that only one-fifth of persons with diabetes expected to take glucose-lowering agents for the rest of their lives (19). Moennig et al. (20) found that 42% of insulin users expected an improvement in glucose, and fulfillment of this expectation was the main cause of uninterrupted use. Naegeli et al. (21) documented a higher percentage of insulin users anticipate achieving optimal glucose levels (61%). Notably, 58% had their expectations exceeded and 29% their expectations fulfilled. On the other hand, the following erroneous expectations have been reported: being able to stop the medication when reaching the glucose goal, anticipating diabetes cure, and expecting freedom to eat while taking the medicine (18, 19, 22–26). The study of expectations in diabetes is worthwhile because persons living with diabetes with positive outcome expectations are more likely to benefit from diabetes management than those with negative outcome expectations (27), while idealistic expectations or misperceptions seem to have the opposite effect on health outcomes (15).
Personal expectations may vary according to ethnic origin, age, sex, socioeconomic status, schooling, diabetes education, time since diagnosis, and diabetes severity (14, 22, 28). However, information on expectations and associated factors in persons with diabetes is practically non-existent in Mexican or Latino populations (24). The objective of this study was to determine the idealistic, realistic, and unrealistic expectations of pharmacological medication (metformin, insulin, and glyburide) among persons with type 2 diabetes in primary care. We also explored the association between sociodemographic attributes (sex, schooling, place of residence, education in diabetes), time since diagnosis, and expectations.
This was a cross-sectional study conducted from October 2020 to March 2022. We consecutively included persons with type 2 diabetes between 30 and 70 years old under pharmacological therapy. Those with current pregnancy or history of blindness, hemodialysis, peritoneal dialysis, lower-extremity amputation, and heart surgery were excluded (to limit persons with advanced diabetes severity among whom expectations might differ from those of persons with mild or no complications). The participants were approached in waiting rooms of primary care centers of a governmental health institution in the metropolitan area of Monterrey (the third-largest urban area of the country, with a population density of 3,523 inhabitants/km2) and one primary care center in a suburban area located in Linares (population density of 33.7 inhabitants/km2), Mexico. The prevalence of idealistic, realistic, and unrealistic expectations was taken as the parameter (p) for estimating the sample size. A minimum sample size of 385 individuals with diabetes was required considering p = 50% with a 95% confidence level and a precision of 5%. However, the total sample size was 907; 507 participants from the urban area and 400 participants from the suburban area. The protocol was approved by the Local Committees of Ethics and Health Research (No. 2020-1909-062, 2021-1909-101, and 20-FASPYN-SA-22.TP). Informed consent was provided by all the participants. Anonymity was always preserved, and the confidentiality of the data was ensured.
Three types of expectations were studied: idealistic, realistic, and unrealistic; and the anticipation of a future event was the common definition. Idealistic expectations focused on management preferences, realistic expectations on perceived medication efficacy, and unrealistic expectations on incorrectly perceived therapeutic benefits. Expectation items were subject to content validity evaluation. A group of experts (three medical doctors and two public health specialists) assessed and approved by consensus the pertinence and relevance of the questions. Special attention was paid to avoiding ambiguity and technical vocabulary. Pre-test and pilot tests were carried out to verify clarity and ease of understanding. The internal consistency results are provided below.
Measurement was based on what the person with diabetes preferred if given the choice. Questions were developed using information relevant to idealistic expectation constructs (14, 15). Three items were included: (1) If you had the option, you would like to take fewer pills or receive fewer applications of insulin per day (in those who took more than one tablet or received more than one application per day); (2) You would like to be able to change the route of administration from oral to injectable, or vice versa; and (3) You wish you could take a temporary break from the medication. In persons treated with metformin, a fourth item on preference for a smaller tablet size was also included. The response options were on a Likert scale (−1 = No, 0 = Indifferent, 1 = Yes). The questions were specific to the medication being received, so an individual on metformin answered the questions about metformin. If someone was on two medications, for example, metformin and insulin, he/she answered the metformin and insulin questions separately (metformin: n = 725, Cronbach's Alpha = 0.97; insulin: n = 352, Cronbach's Alpha = 0.94; glyburide: n = 180, Cronbach's Alpha = 0.68). For the analysis of association, an index was constructed to summarize the idealistic expectations domain. The negative and indifferent responses were regrouped and coded as 0; the positive response remained as 1. Responses were then summed and categorized into null, low, and moderate-high depending on the number of idealistic expectations 0, 1, and 2–3, respectively.
Measurement was based on the perception of true medication benefits. Six items adapted from other authors (7, 18) were used: (1) How much do you expect the medicine will bring blood sugar down to a normal range; (2) Eliminate symptoms of hyperglycemia; (3) Prevent or delay foot amputations; (4) Prevent or delay the need for dialysis; (5) Prevent or delay vision loss; and (6) Reduce the need for hospitalization. The response options were on a Likert scale (1= Null, 4= Very much). Cronbach's Alpha was as follows: Metformin = 0.92, insulin = 0.90, and glyburide: = 0.90. For the analysis of association, an index was constructed to summarize the realistic expectations domain. The “null”, “a little”, and “moderately” responses were regrouped and coded as 0; the “very much” response was recoded as 1. Responses were then summed and categorized into null, low, moderate, and high depending on the number of realistic expectations 0, 1–2, 3–4, and 5–6, respectively.
Measurement was based on misperception of medication benefits. Four items adapted from other authors (22–25) were used: (1) How much do you expect the medicine will cure your diabetes; (2) Allow you to stop treatment when reaching your glucose goal; (3) Allow freedom to eat; and (4) Allow you to have no complications despite medication. The response options were on a Likert scale (1=Null, 4= Very much). The questions were generic; for example, a person treated with metformin and insulin answered the section without distinguishing between medications (n = 907, Cronbach's Alpha = 0.66). For the analysis of association, an index was constructed to summarize the unrealistic expectations domain. The “a little”, “moderately”, and “very much” responses were regrouped and coded as 1; the “null” response was recoded as 0. Responses were then summed and categorized into null, low, and moderate-high depending on the number of unrealistic expectations 0, 1, and 2–4, respectively.
Sociodemographic attributes (sex, age, marital status, schooling, occupation, place of residence), diabetes education in the last year (yes, no), time since diagnosis (years), and frequency of medical visits for diabetes management (monthly, every 2 months, other) were included. Comorbidities (hypertension, dyslipidemia, other) (yes, no), hospitalization due to diabetes in the past year (yes, no); and last glucose result (mg/dL) (self-report) were also considered. Data were collected through a face-to-face interview lasting approximately 15 min. Two postgraduate students (Family Medicine and Master of Sciences in Public Health) and two medical interns participated. All were supervised by the principal investigator. Participants with incorrect expectations were given the correct information at the end of the survey. Those with idealistic expectations were instructed to express their preferences to their doctor at the next visit, so that they could jointly analyze the possibility of satisfying them.
Means and standard deviations were used to describe continuous variables, and percentages to describe categorical variables. The z test for the difference between two proportions was used for comparing the frequency of expectations by type of medication. The chi-square test (univariate analysis) and ordinal logistic regression (multivariate analysis) were employed for analyzing the association between factors under study and expectations; the sociodemographic attributes and time since diagnosis were considered the independent variables; the idealistic, realistic, or unrealistic expectations index constituted the dependent variable; and the comorbidity and frequency of medical visits for diabetes management were the control variables. Odds ratios (OR) and 95% confidence intervals (CI) were estimated for quantifying the strength of the association between associated factors and expectations.
The mean age was 55.7 ± 10.6, and the mean time since diabetes diagnosis was 9.9 ± 7.9 years. Most of the participants were female and married or with a partner. More than 80% had routine monthly medical visits for diabetes management. Table 1 shows in detail the sociodemographic and comorbidity profile of the study population.
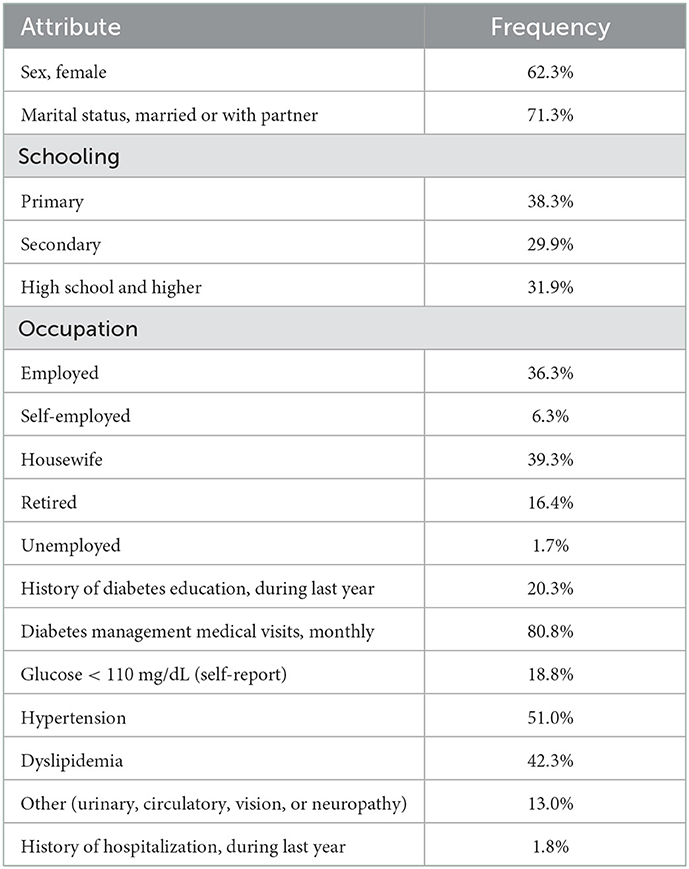
Table 1. Sociodemographic and comorbidity profile (n = 907).
A high percentage of participants on metformin would like the pill size to be smaller (77.8%). About 90% would like fewer pills/injections per day. More insulin users wished they could take a temporary break or would like to change the route of administration (Figure 1). Suburban residence, ≥ 3 years since diagnosis, and female sex increased the odds of higher metformin idealistic expectations. Place of residence was also associated to glyburide idealistic expectations and time since diagnosis with those of insulin (Table 2).
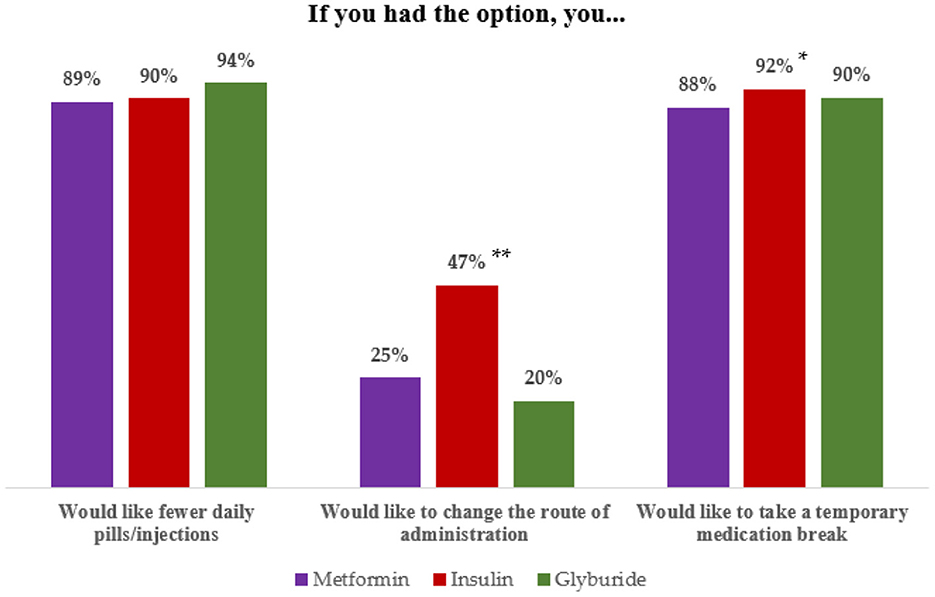
Figure 1. Idealistic expectations according to type of medication. Information at the bottom of the figure: z test for the difference between two proportions p values: *<0.05, Insulin > Metformin, **<0.001, Insulin > Metformin and glyburide.
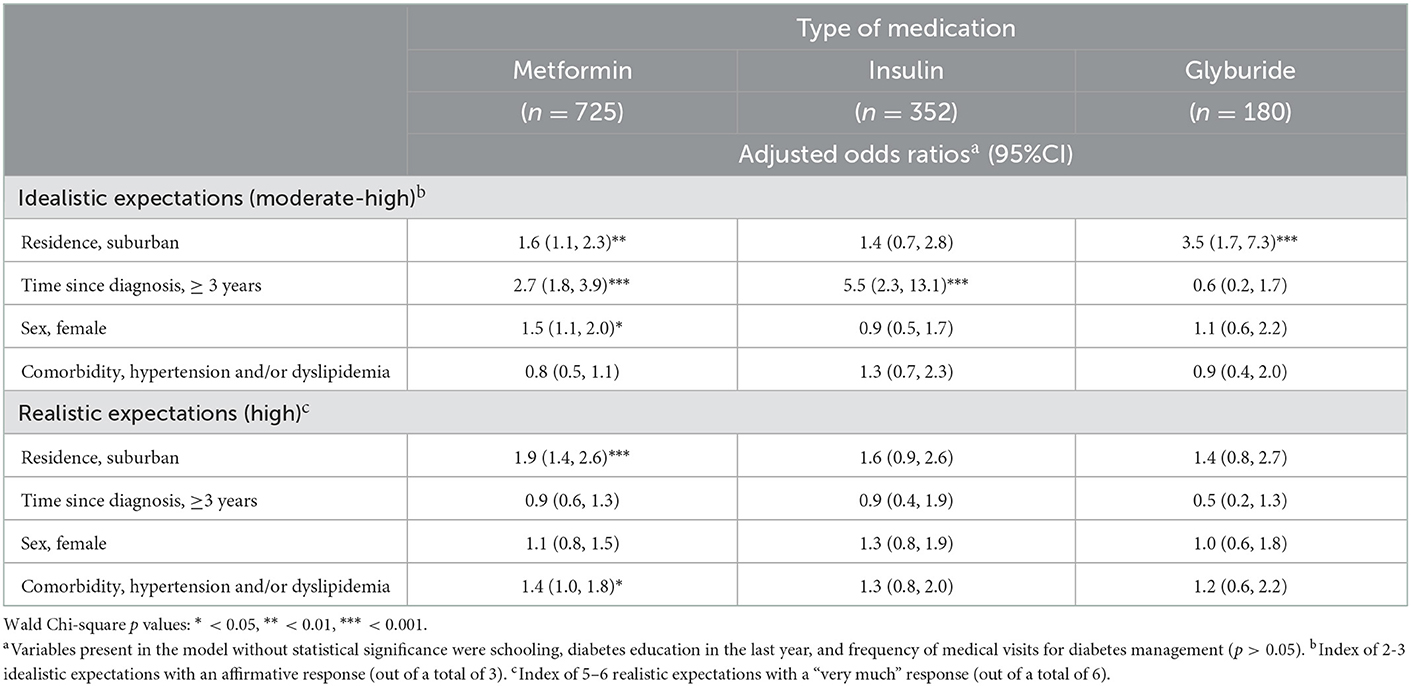
Table 2. Multivariate ordinal regression analyses of factors associated to idealistic and realistic expectations.
Between 47 and 70% of participants had realistic expectations; insulin users had more realistic expectations than metformin users (Table 3). Suburban residence and having hypertension and/or dyslipidemia increased the odds of higher metformin realistic expectations (Table 2).
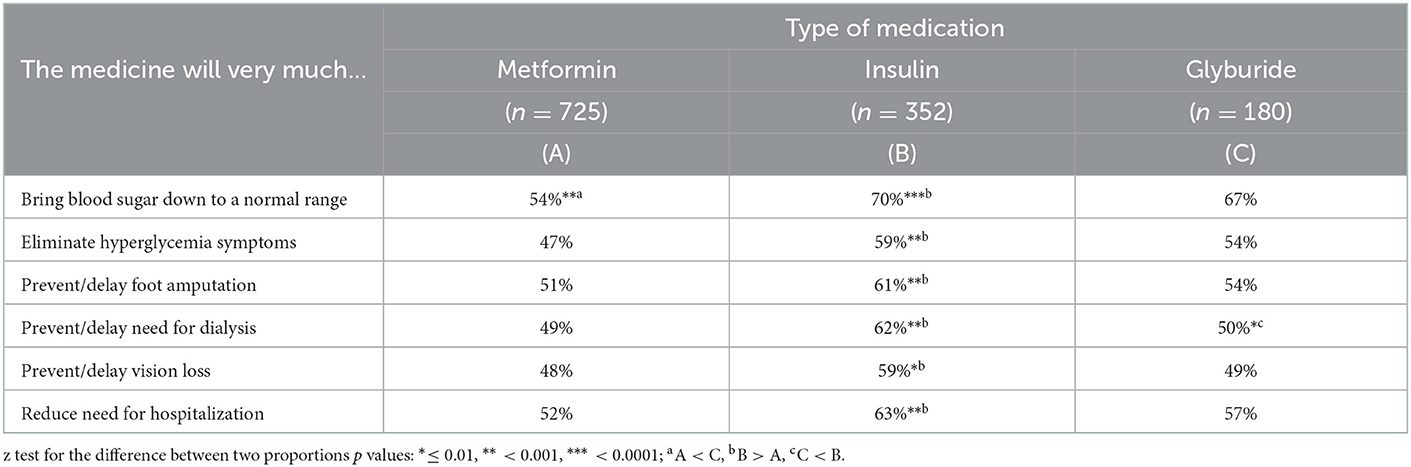
Table 3. Realistic expectations according to type of medication.
The most frequent unrealistic expectation was anticipating complications despite the medication (64.8%). It was followed by expecting interruption of medication upon reaching the glucose goal (55.0%), freedom to eat (39.1%), and diabetes cure (30.7%). Combined therapy users had a higher expectation of being able to discontinue the medication upon reaching the glucose goal (Table 4). Suburban residence increased 1.98 times (95%CI 1.47, 2.68) the odds of higher unrealistic expectations while diabetes education in the last year decreased them (OR 0.62, 95% CI 0.44, 0.87); after adjustment for type of medication, sex, schooling, time since diagnosis, comorbidity, and frequency of medical visits for diabetes management.
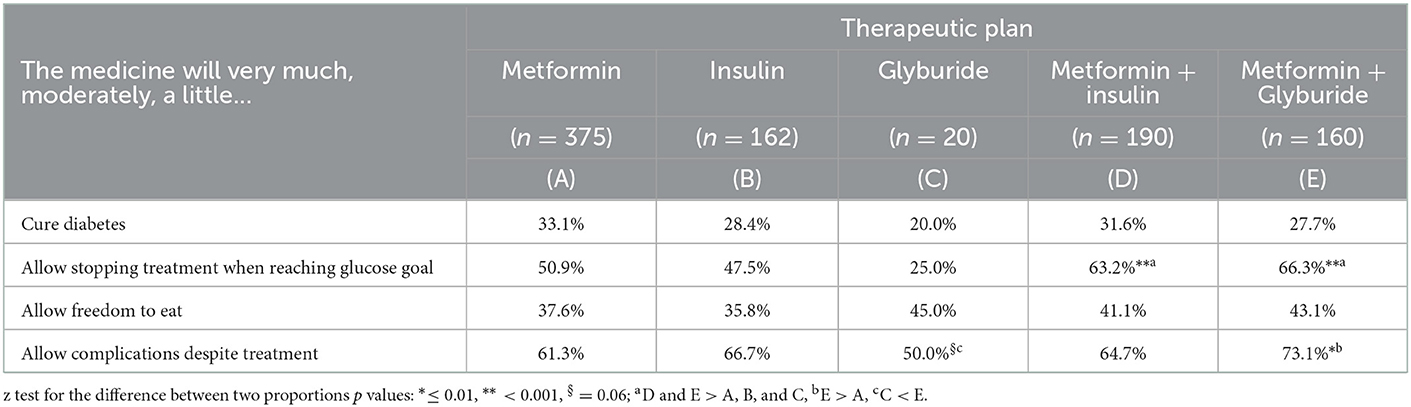
Table 4. Unrealistic expectations according to therapeutic plan.
We determined idealistic, realistic, and unrealistic expectations about metformin, insulin, and glyburide in persons with type 2 diabetes in primary care. We found several expectation differences by type of medication. Almost half of the people on insulin would like to be able to switch to oral administration compared to one-fourth on metformin who would like the opposite, indicating that personal preferences should not be taken for granted. Boye et al. (29) evidenced 25.5% of persons with diabetes had switched from preferring oral to injectable medication after learning about the product specifications (daily oral semaglutide vs. once-weekly injectable dulaglutide). We also identified 8 out of 10 participants on metformin would like the size of the pill to be smaller and a high percentage would like fewer daily pills/injections or a temporary break from the medication. Fairchild et al. (19) documented 78% of adults in primary care did not expect to take oral medications for life. Idealistic expectations must be discussed with the person living with diabetes because the ideal may not be feasible. And personal preferences, shared decision making, and mutual agreement for changes should be encouraged.
There were more real benefits perceived with insulin than metformin. Laferton et al. (15) also showed an injectable medication was expected to be more effective than an oral one. Reduction of glucose to a target level was the number one most expected benefit, 7 out of 10 insulin participants anticipated this result, higher than 42 and 61% reported by multinational studies (20, 21). In contrast, 5 out of 10 metformin users expected this benefit, a result lower than that documented in primary care of 70% (18). Differences in findings emphasize the importance of identifying expectations in different populations. Correspondence between the diabetes care team members and the person with diabetes is essential since it may contribute to non-taking the medication by failing to explain benefits and side effects adequately (30). Realistic expectations must be reinforced, since the greater the perception of effectiveness, the greater the medication taking (31, 32). Furthermore, a low efficacy perception has been associated with higher levels of HbA1c (33).
More than half of the respondents anticipated complications would occur despite treatment or that they could stop the medication when the glucose goal was reached. In Saudi Arabia, these were also the most common unrealistic expectations (89 and 66.5%, respectively) (22). Analysis by type of therapeutic plan showed combined therapy users expected more to discontinue the medication upon reaching the glucose goal. One-third anticipated diabetes would be cured over time with no differences by medication scheme. The frequency of this erroneous expectation has been wide-ranging (11.7–65%) (19, 23–26) and some authors such as Mann et al. (25) have reported insulin users are less likely to believe in diabetes cure. Additionally, over a third of participants expected they could eat anything while taking the medication. Literature reports vary from 23 to 49.1% (23, 24, 26). Food freedom means always eating what you want in the amount you want. Freedom might be an exception, but not the rule. Medical nutrition therapy plays an integral role in diabetes management that considers maintaining the pleasure of eating by providing flexibility with healthy food choices, while limiting unnecessary and unhealthy ones. The American Diabetes Association advises people with diabetes to minimize the consumption of foods with added sugar and refined grains. It also emphasizes the consumption of polyunsaturated fats and limits the serving size of nutrient-dense foods for favoring a healthy body weight and achieving glucose and lipid goals (34). Certainly, knowledge and beliefs about medications should be attended to. Health educators and decision makers should keep in mind that outcome expectations and self-care behaviors are correlated (35, 36), and that unrealistic expectations constitute barriers to effective diabetes management. Clearly, the insertion of effective health communication strategies is urgently needed to neutralize misconceptions, such as the diabetes cure, and to reinforce true facts.
We explored the association between several factors and expectations, ≥3 years since diagnosis increased the odds of higher metformin and insulin idealistic expectations indicating need for matching correct information over time. Time since diagnosis was not associated to unrealistic expectations, which differed from other studies that have shown greater misperceptions with <5 (26) or between 5 and 15 years with diabetes (22). This lack of consistency requires further research. Being female increased the odds of metformin idealistic expectations, but not those of erroneous expectations. Other authors have identified women tend to have higher misconceptions (22, 26). Suburban residence was another associated factor. It augmented the odds of metformin idealistic and realistic expectations, also the odds of glyburide idealistic expectations, and those of unrealistic expectations. There are three ways to create expectations: direct personal experience, observation, and suggestion of others (27). Dissimilarity in such circumstances could explain differences between urban and non-urban residents, but more investigation is needed to identify the specific reasons. Diabetes education in the last year lessened the odds of misperceptions. Alsunni et al. (22) found individuals who had undergone proper education about diabetes had less misconceptions, underlining the importance of educational programs. Diabetes self-management education is essential in the care of all people with diabetes to provide knowledge and skills. And the 2022 National Standards for Diabetes Self-Management Education and Support recommend the collaboration between the person and the health care team considering the individual's concerns, needs and priorities (37).
Obtaining socially acceptable responses could have led to overestimation or underestimation of expectations. This study focused on the most frequently employed diabetes medication, so dipeptidyl peptidase 4 inhibitors (DPP-4), thiazolidinediones, and sodium glucose co-transporter 2 inhibitors users were not considered. Only persons with diabetes from primary care without current pregnancy or advanced complications were included, so it is not possible to generalize results to those with gestational diabetes or under diabetes management in secondary or tertiary care. More research is needed, and future investigations should include these types of cases. More than half of the study population were women, which was not surprising. In Mexico, there are more women than men according to the 2020 population census and diabetes is more prevalent in women (38, 39). The association analysis had the advantage of being multivariate, but the study design was cross-sectional. Future longitudinal studies are required for definitive conclusions on factors determining idealistic, realistic, and unrealistic expectations.
This study contributes to narrowing the knowledge gap about idealistic, realistic, and unrealistic expectations in the Mexican or Latino population regarding pharmacological medication in persons with type 2 diabetes. The frequency varied by expectation and type of medication. Insulin users had more idealistic and realistic expectations; and combined therapy users expected more to discontinue the medication upon reaching the glucose goal. Time since diagnosis, place of residence, and sex were factors associated to expectations. Especially, diabetes education reduced the odds of misperceptions. Health policy makers, health managers, and the diabetes care team together must ensure that people with diabetes be trained. Understanding personal preferences and expectations is relevant because it makes it easier to select the medication that will most benefit the individual. A person-centered communication, shared decision making, and management of expectations must be reinforced in persons with type 2 diabetes undergoing pharmacological medication in primary care.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Institutional Review Board and Ethics Committee of the Mexican Social Security Institute (No. 2020-1909-062 and 2021-1909-101) and the School of Public Health and Nutrition (20-FASPYN-SA-22.TP). The patients/participants provided their written informed consent to participate in this study.
Conceptualization and methodology: AS and AJ. Data curation and investigation: AJ, YR, and LH. Formal analysis and validation: AS and HC. Project administration: AS, FG, and GN. Supervision and writing—original draft: AS. Writing—review and editing: AS, AJ, YR, HC, FG, LH, and GN. All authors contributed to the article and approved the submitted version.
Tania Montserrat Pérez Payró and Metzli Margarita Carreón Juárez, for their participation in the collection and data entry.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes−2022. Diabetes Care. (2022) 45:S17–S38. doi: 10.2337/dc22-S002
2. International Diabetes Federation,. IDF Diabetes Atlas. 10th edition. (2021). Available online at: https://diabetesatlas.org/ (accessed August 31, 2022).
3. American Diabetes Association. American Diabetes Association 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes−2022. Diabetes Care. (2022) 45:S125–S143. doi: 10.2337/dc22-S009
4. International Diabetes Federation. IDF Diabetes Atlas. 10th edition. Brussels: International Diabetes Federation (2021).
5. Khunti K, Seidu S, Kunutsor S, Davies M. Association between adherence to pharmacotherapy and outcomes in type 2 diabetes: a meta-analysis. Diabetes Care. (2017) 40:1588–96. doi: 10.2337/dc16-1925
6. Pound P, Britten N, Morgan M, Yardley L, Pope C, Daker-White G, et al. Resisting medicines: a synthesis of qualitative studies of medicine taking. Soc Sci Med. (2005) 61:133–55. doi: 10.1016/j.socscimed.2004.11.063
7. Dohnhammar U, Reeve J, Walley T. Patients' expectations of medicines - a review and qualitative synthesis. Heal Expect. (2016) 19:179–93. doi: 10.1111/hex.12345
8. Asadi-Lari M, Tamburini M, Gray D. Patients' needs, satisfaction, and health related quality of life: towards a comprehensive model. Health Qual Life Outcomes. (2004) 2:32. doi: 10.1186/1477-7525-2-32
9. Doggrell SA, Warot S. The association between the measurement of adherence to anti-diabetes medicine and the HbA1c. Int J Clin Pharm. (2014) 36:488–97. doi: 10.1007/s11096-014-9929-6
10. Capoccia K, Odegard PS, Letassy N. Medication adherence with diabetes medication. Diabetes Educ. (2016) 42:34–71. doi: 10.1177/0145721715619038
11. Asche C, LaFleur J, Conner C, A. Review of diabetes treatment adherence and the association with clinical and economic outcomes. Clin Ther. (2011) 33:74–109. doi: 10.1016/j.clinthera.2011.01.019
12. Currie CJ, Peyrot M, Morgan CL, Poole CD, Jenkins-Jones S, Rubin RR, et al. The impact of treatment noncompliance on mortality in people with type 2 diabetes. Diabetes Care. (2012) 35:1279–84. doi: 10.2337/dc11-1277
13. Kennedy-Martin T, Boye K, Peng X. Cost of medication adherence and persistence in type 2 diabetes mellitus: a literature review. Patient Prefer Adherence. (2017) 11:1103–17. doi: 10.2147/PPA.S136639
14. Bowling A, Rowe G, Lambert N, Waddington M, Mahtani K, Kenten C, et al. The measurement of patients' expectations for health care: a review and psychometric testing of a measure of patients' expectations. Health Technol Assess (Rockv). (2012) 16:1–509. doi: 10.3310/hta16300
15. Laferton JAC, Kube T, Salzmann S, Auer CJ, Shedden-Mora MC. Patients' expectations regarding medical treatment: a critical review of concepts and their assessment. Front Psychol. (2017) 8: doi: 10.3389/fpsyg.2017.00233
16. Dolovich L, Nair K, Sellors C, Lohfeld L, Lee A, Levine M. Do patients' expectations influence their use of medications? Qualitative study Can Fam Physician. (2008) 54:384–93.
17. Thompson AGH, Sunol R. Expectations as determinants of patient satisfaction: Concepts, theory and evidence. Int J Qual Heal Care. (1995) 7:127–41. doi: 10.1093/intqhc/7.2.127
18. Gibson DS, Nathan AG, Quinn MT, Laiteerapong N. Patient expectations of hypertension and diabetes medication: excessive focus on short-term benefits. SAGE Open Med. (2018) 6:205031211882111. doi: 10.1177/2050312118821119
19. Fairchild PC, Nathan AG, Quinn M, Huang ES, Laiteerapong N. Patients' future expectations for diabetes and hypertension treatments: “Through the diet… I think this is going to go away”. J Gen Intern Med. (2017) 32:49–55. doi: 10.1007/s11606-016-3871-3
20. Moennig E, Perez-Nieves M, Hadjiyianni I, Cao D, Ivanova J, Klask R. Initiation of basal insulin analog treatment for type 2 diabetes and reasons behind patients' treatment persistence behavior: real-world data from Germany. Exp Clin Endocrinol Diabetes. (2018) 126:287–97. doi: 10.1055/s-0043-116386
21. Naegeli AN, Hayes RP. Expectations about and experiences with insulin therapy contribute to diabetes treatment satisfaction in insulin-naïve patients with type 2 diabetes. Int J Clin Pract. (2010) 64:908–16. doi: 10.1111/j.1742-1241.2010.02363.x
22. Alsunni A, Albaker W, Badar A. Determinants of misconceptions about diabetes among Saudi diabetic patients attending diabetes clinic at a tertiary care hospital in Eastern Saudi Arabia. J Fam Community Med. (2014) 21:93. doi: 10.4103/2230-8229.134764
23. Patil R. Popular misconceptions regarding the diabetes management: where should we focus our attention? J Clin Diagnostic Res. (2013) 7:287–91. doi: 10.7860/JCDR/2013/4416.2749
24. Salazar Fonseca E, Ponce Rosas E, Jiménez Galván I, Cervantes Naranjo A, Jiménez Hernández J, Madrigal de León H. Mitos y creencias sobre la diabetes en pacientes de una unidad médica de atención primaria en la Ciudad de México. Arch Med Fam. (2018) 20:15–21.
25. Mann DM, Ponieman D, Leventhal H, Halm EA. Misconceptions about diabetes and its management among low-income minorities with diabetes. Diabetes Care. (2009) 32:591–3. doi: 10.2337/dc08-1837
26. Al-Saeedi M, Elzubier AG, Bahnassy AA, Al-Dawood KM. Treatment-related misconceptions among diabetic patients in Western Saudi Arabia. Saudi Med J. (2002) 23:1243–6.
27. Janzen JA, Silvius J, Jacobs S, Slaughter S, Dalziel W, Drummond N. What is a health expectation? Developing a pragmatic conceptual model from psychological theory. Heal Expect. (2006) 9:37–48. doi: 10.1111/j.1369-7625.2006.00363.x
28. Kravitz RL. Measuring Patients' Expectations and Requests. Ann Intern Med. (2001) 134:881. doi: 10.7326/0003-4819-134-9_Part_2-200105011-00012
29. Boye K, Ross M, Mody R, Konig M, Gelhorn H. Patients' preferences for once-daily oral versus once-weekly injectable diabetes medications: The REVISE study. Diabetes, Obes Metab. (2021) 23:508–19. doi: 10.1111/dom.14244
30. Valentine KD, Scherer LD. Interpersonal (mis)perceptions and (mis)predictions in patient–clinician interactions. Curr Opin Psychol. (2022) 43:244–8. doi: 10.1016/j.copsyc.2021.07.021
31. Farhat R, Assaf J, Jabbour H, Licha H, Hajj A, Hallit S, et al. Adherence to oral glucose lowering drugs, quality of life, treatment satisfaction and illness perception: a cross-sectional study in patients with type 2 diabetes. Saudi Pharm J. (2019) 27:126–32. doi: 10.1016/j.jsps.2018.09.005
32. Wei L, Champman S, Li X, Li X, Li S, Chen R, et al. Beliefs about medicines and non-adherence in patients with stroke, diabetes mellitus and rheumatoid arthritis: a cross-sectional study in China. BMJ Open. (2017) 7:e017293. doi: 10.1136/bmjopen-2017-017293
33. von Arx L-BW, Gydesen H, Skovlund S. Treatment beliefs, health behaviors and their association with treatment outcome in type 2 diabetes. BMJ Open Diabetes Res Care. (2016) 4:e000166. doi: 10.1136/bmjdrc-2015-000166
34. American Diabetes Association. 5. Facilitating behavior change and well-being to improve health outcomes: standards of medical care in diabetes−2022. Diabetes Care. (2022) 45:S60–S82. doi: 10.2337/dc22-S005
35. Wu S-FV, Courtney M, Edwards H, McDowell J, Shortridge-Baggett LM, Chang P-J. Self-efficacy, outcome expectations and self-care behaviour in people with type 2 diabetes in Taiwan. J Clin Nurs. (2007) 16:250–7. doi: 10.1111/j.1365-2702.2006.01930.x
36. Reisi M, Mostafavi F, Javadzade H, Mahaki B, Tavassoli E, Sharifirad G. Impact of health literacy, self-efficacy, and outcome expectations on adherence to self-care behaviors in Iranians with type 2 diabetes. Oman Med J. (2016) 31:52–9. doi: 10.5001/omj.2016.10
37. Davis J, Fischl AH, Beck J, Browning L, Carter A, Condon JE, et al. 2022 National standards for diabetes self-management education and support. Diabetes Care. (2022) 45:484–94. doi: 10.2337/dc21-2396
38. National National Institute of Statistics Geography Informatics (INEGI). Population and Housing Census. (2020). Available online at: https://www.inegi.org.mx/programas/ccpv/2020/default.html#Tabulados (accessed August 30, 2022).
39. Shamah-Levy T, Romero-Martinez M, Barrientos-Gutierrez T, Cuevas-Nasu L, Bautista-Arredondo S, Colchero M, et al. Encuesta Nacional de Salud y Nutricion 2021 sobre Covid-19. Resultados nacionales. Cuernavaca, Mexico: Instituto Nacional de Salud Publica. (2022). Available online at: https://www.insp.mx/novedades-editoriales/encuesta-nacional-de-salud-y-nutricion-2021-sobre-covid-19-resultados-nacionales (accessed August 30, 2022).
Keywords: expectations, diabetes, primary care, therapeutic misconception, individual preference
Citation: Salinas Martínez AM, Juárez Montes AG, Ramírez Morado Y, Cordero Franco HF, Guzmán de la Garza FJ, Hernández Oyervides LC and Núñez Rocha GM (2023) Idealistic, realistic, and unrealistic expectations of pharmacological treatment in persons with type 2 diabetes in primary care. Front. Public Health 11:1058828. doi: 10.3389/fpubh.2023.1058828
Received: 30 September 2022; Accepted: 11 January 2023;
Published: 02 February 2023.
Edited by:
I-Shiang Tzeng, National Taipei University, TaiwanReviewed by:
Nazma Akter, Marks Medical College and Hospital, BangladeshCopyright © 2023 Salinas Martínez, Juárez Montes, Ramírez Morado, Cordero Franco, Guzmán de la Garza, Hernández Oyervides and Núñez Rocha. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana María Salinas Martínez,  YW5hLnNhbGluYXNtQHVhbmwubXg=; YW1zYWxpbmFzbWFydGluZXpAZ21haWwuY29t
YW5hLnNhbGluYXNtQHVhbmwubXg=; YW1zYWxpbmFzbWFydGluZXpAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.