 Eric T. C. Lai
Eric T. C. Lai Pui Hing Chau
Pui Hing Chau Ken Cheung4
Ken Cheung4 Jean Woo
Jean Woo
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 10 February 2023
Sec. Aging and Public Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1056800
This article is part of the Research Topic Social Determinants of Health for the Global Aging Population in Pandemic and Disaster Environments View all 13 articles
Background: Extreme hot weather events are happening with increasing frequency, intensity and duration in Hong Kong. Heat stress is related to higher risk of mortality and morbidity, with older adults being particularly vulnerable. It is not clear whether and how the older adults perceive the increasingly hot weather as a health threat, and whether community service providers are aware and prepared for such future climate scenario.
Methods: We conducted semi-structure interviews with 46 older adults, 18 staff members of community service providers and two district councilors of Tai Po, a north-eastern residential district of Hong Kong. Transcribed data were analyzed using thematic analysis until data saturation was reached.
Results: It was agreed upon among the older adult participants that the weather in recent years has become increasingly hot and this led to some health and social problems for them, although some participants perceived that hot weather did not have any impact in their daily lives and they were not vulnerable. The community service providers and district councilors reported that there is a lack of relevant services in the community to support the older adults in hot weather; and there is generally a lack of public education regarding the heat-health issue.
Conclusions: Heatwaves are affecting older adults' health in Hong Kong. Yet, discussions and education effort regarding the heat-health issue in the public domain remain scarce. Multilateral efforts are urgently needed to co-create a heat action plan to improve community awareness and resilience.
Against the backdrop of global climate change, extreme weather events will become more frequent, intense and last longer (1). Luo and Lau (2) showed that in the Southern China region, from 1980's to 2010's, there has been significant increase in the frequency of heat wave (+0.19 events per decade), heat wave days (+2.86 days per decade) and the duration of the longest heat wave (+0.38 days per decade). Locally, the Hong Kong Observatory (HKO) has reported that the numbers of hot night (highest night-time temperature >28°C) and very hot day (highest daytime temperature >33°C) have been respectively on the rising trend. In 2021 alone, Hong Kong has recorded 61 hot nights and 54 very hot days, both hit the record high since 1884 (3). In 2022, the first very hot weather warning (VHWW) in the year was issued on 29 April, 2022, which was a record earliest date for such warning. Moreover, Hong Kong's unique mountainous topography has limited the development of its land, resulting in only around 24% of its territory being developed (4). High-rise buildings are thus concentrated in urban areas; the ventilating airways from the sea to the inland areas are blocked to different extents, exacerbating the urban heat island effect (5).
Extreme hot weather brings negative impacts on people's health and wellbeing (6, 7). In Hong Kong, it has been reported that extreme hot weather events are related to higher risk of adverse health outcomes such as mortality (8, 9), asthma hospitalization (10) acute myocardial infarction among patients with diabetes mellitus (11), all-cause accident and emergency department visits (12) and suicide deaths (13). Moreover, the impact of extreme hot temperature could be more serious for the vulnerable groups in the population. Older adults aged over 65-year-old are more prone to heat-related illnesses than younger age groups (14–16). Their ability of thermoregulation has become less effective following the natural aging process. For example, their ability to control vasodilation to increase blood flow to the skin could be deteriorated. Their decreased sensitivity to thirst could lead to dehydration amid very hot weather. Previous studies have found that the heat-related mortality rate of the older adults has increased globally by more than 53% in the past two decades (17). Several studies projected that the heat-related mortality rate would continue to rise when considering the current rising trends of temperature and aging population (18, 19). In a local study, Wang and colleagues (20) observed 2.53% and 5.33% increases in mortality risk for older adults suffering from a single hot night and five hot nights respectively. When the older adults suffer from two hot days and three hot nights consecutively, their daily mortality risk rises by 5.87%. The older adult's ability to perspire could also be hindered by common medications for chronic diseases such as beta blockers and anticholinergics (21, 22).
Given the health impact brought by extreme hot weather, it is therefore important for individuals to take appropriate adaptive response to minimize the health risks. It was shown that proper actions in response to weather warning might help mitigate the adverse outcomes among the older adults (23). In the health decision-making literature, individuals are often expected to go through cognitive processes that involve weighing risks for consequences against the benefits of taking actions. Grothmann and Patt (24) posited that there are two important cognitive factors involved–risk perception and perceived adaptive capacity. Risk perception measures how an individual perceive the risk of whether a certain event could happen and hence ultimately drives relevant adaptive behaviors. This process involves judging how likely one is exposed to the extreme weather conditions, how harmful such conditions would be to things that one has reason to value (e.g., health), and how one weighs these risks over other priorities in life. This has also been previously theorized in health behavior models that predict behavioral changes, such as the health belief model (25) and the protection motivation theory (26). On the other hand, there are two dimensions for adaptive capacity. First, subjective adaptive capacity concerns how people perceive the resources at their disposal. Gardner and Stern (27) suggested with empirical data that people often perceive little control over global and regional environmental problems. The other dimension concerns, objectively, the social resources available (28). Adger (29) argued that the capacity of individuals to adapt to climate change “is a function of their access to resources,” corroborating that social determinants have a substantial influence on behaviors conducive to health (30, 31). For instance, in the case of the 1995 Chicago heat wave, socioeconomic resources had substantial impact for older adults to adapt to the impact of hot weather, partly through the ownership and utilization of cooling devices (32). A more recent study in Brazil showed that less developed cities showed stronger associations of heatwaves and all-cause hospitalizations (33).
Although older adults are considered as more vulnerable to heat-related illnesses, previous studies showed that older adults or the general population seldom perceived so. In a population-representative cross-sectional survey of older adults in Australia, Hansen and colleagues (34) reported that, when asked whether the older adults concern their health amid a heatwave, only 3 to 6% of the respondents reported that they did. Around 30% said they were not concerned at all in the case when a heatwave is coming. Abrahamson and colleagues (35) conducted semi-structured interviews with 73 older adults in the UK and found that few respondents considered themselves either old or at risk of suffering from the effect of heat; most also claimed that they have taken appropriate steps to mitigate the impact of heat. A recent systematic review by Vu and colleagues (36) echoed that many older people surveyed in Australia, UK, USA and Canada were not aware of their susceptibility to hot weather. In eastern China, a cross-sectional study also reported that the older adults and the lower educated were less likely to perceive hot weather as a health threat (37). A recent population-based telephone survey in Hong Kong showed that about half of around 1,000 respondents recognized that climate change posed as a health risk (38). However, risk perception and behavioral adaptations in the older adults, and the view from frontline service providers, were seldom assessed in the local context. Therefore, in this study, we would like to address the following questions:
• What are the perceptions of the older adults in Hong Kong toward hot weather and what measures are they taking in the face of it?
• What are the current services provided by elderly service providers, particularly the community centers, that targeted at helping the older adults to survive the hot weather?
• What are the possible enablers and barriers and facilitators for those services and measures?
This study consists of two parts. In the first part we examined the perceptions of the older adults toward hot weather and their adaption strategies through focus group discussion. And in the second part, we assessed the perceptions from the point of view of frontline service providers–the problems or barriers they face during heatwaves.
In the first part of the study, older adults, were recruited from two public housing estates of Tai Po district in Hong Kong: Kwong Fuk Estate and Tai Wo Estate. Tai Po is located northeastern of New Territories in Hong Kong. This district has the total population of 316,470, accounting for 4.3% of the total population of Hong Kong. The proportion of the population aged 65 or above is 18.5%, which is similar to the Hong Kong average of 19.6%. Tai Po was one of the districts of the second phase of the New Town development in Hong Kong which started in 1979. This district comprises residential and industrial areas to create a self-contained district. Tai Po is also well-known for its natural landscapes, surrounded by the mountain ranges on the north, west and south, and fronting Tolo Harbor on the east. Kwong Fuk Estate and Tai Wo Estate are two of the eight public housing estates in Tai Po, providing home to some 23,000 population. The former consists of eight residential buildings completed in 1983, while the later consists of twelve residential buildings completed in 1989. Therefore, the two estates were chosen on the basis that they represent typical settings of residential districts of Hong Kong with a wide variety of community facilities having been built in close proximity to the housing estates, ranging from shopping malls, community centers, recreational facilities, and open space.
In the second part, participants were the community service providers and district councilors, who were recruited from the community centers or through bulk email. In Hong Kong, the District Council serves as the interface between the Government and the community and coordinate activities in the provision of services and facilities at the district level. Community support services for the older adults are mainly coordinated under the Social Welfare Department. There are two types of community centers, namely Neighborhood Elderly Center (NEC) and District Elderly Community Center (DECC). Both NEC and DECC provide comprehensive services to facilitate older population to age-in-place, whereas NEC are at the neighborhood level and DECC are at the district level. There are 171 NEC and 41 DECC in Hong Kong as at mid-2022 (39, 40).
The study was approved by the Survey and Behavioral Research Ethics Committee of the Chinese University of Hong Kong (ref: SBRE-20-799) and the Institutional Review Board of the University of Hong Kong /Hospital Authority, Hong Kong West Cluster (ref: UW22-304). All participants provided informed consent to participate in the study. Demographic information was collected prior to the start of focus group. Participants were advised that they were free to refuse to answer any question and could withdraw from the study at any time. All identifiers were removed from the transcripts and questionnaires and replaced with pseudonyms.
We used purposive sampling of participants for the current study with the following selection criteria. Purposive sampling is widely used in qualitative study to recruit information-rich participants who are knowledgeable about the neighborhood and the phenomenon under study (41). The first part of the study included older adults who (1) were aged 60 or above, (2) were Chinese origin, (3) resided in one of the two housing estates (Kwong Fuk Estate and Tai Wo Estate) in Tai Po for at least 1 year, and (4) able to communicate verbally in Cantonese. Recruitment efforts included flyers, referrals from elderly centers, and word of mouth. The second part of the study included service provider or social workers, who had at least 1 year experience working at the NECC or DEC, as well as district councilors in the Tai Po district.
There were eleven focus groups, consisting of eight focus groups for older adults and three focus groups for community service providers/district councilors, all of which were conducted in the community centers near the given housing estates between May and July 2021 and online platform in July 2022. Each focus group had 4–8 participants and lasted for approximately 60–90 min. All focus groups were audio recorded and transcribed verbatim.
A semi-structured question guide was created for facilitators to use when conducting focus groups. The focus group interviews with the older adults began with broad questions regarding how participants described hot weather in Hong Kong, the impact of hot weather on their daily lives, the adaption strategies they used under the hot weather and also the factors in the social environment that facilitate or hindered adaption. For the focus group interviews with community service providers/district councilors, we asked whether there have been existing programmes or coordinated community efforts regarding extreme heat, what the way forward is and what potential barriers they foresee.
Data analysis followed a thematic analysis approach involving key stages of organization, reduction and refinement (42). Initially, four researchers independently read each transcript to familiarize with the entire dataset and generated an initial list of codes that were relevant to research aims. These codes were then categorized into the potential themes. Initial codes and the potential themes were discussed among the four researchers in order ensure similarities and to review the emergent themes and refine codes. This process of reviewing themes and recoding data continued until all three researchers reached the agreement regarding the emergent themes and coding schemes. Data saturation was reached when no new themes emerged from the data (43).
A total of 46 older adults, 18 staff members of NGOs and 2 Tai Po district councilors joined our focus group interviews. The characteristics of the older adult participants were shown in Table 1.
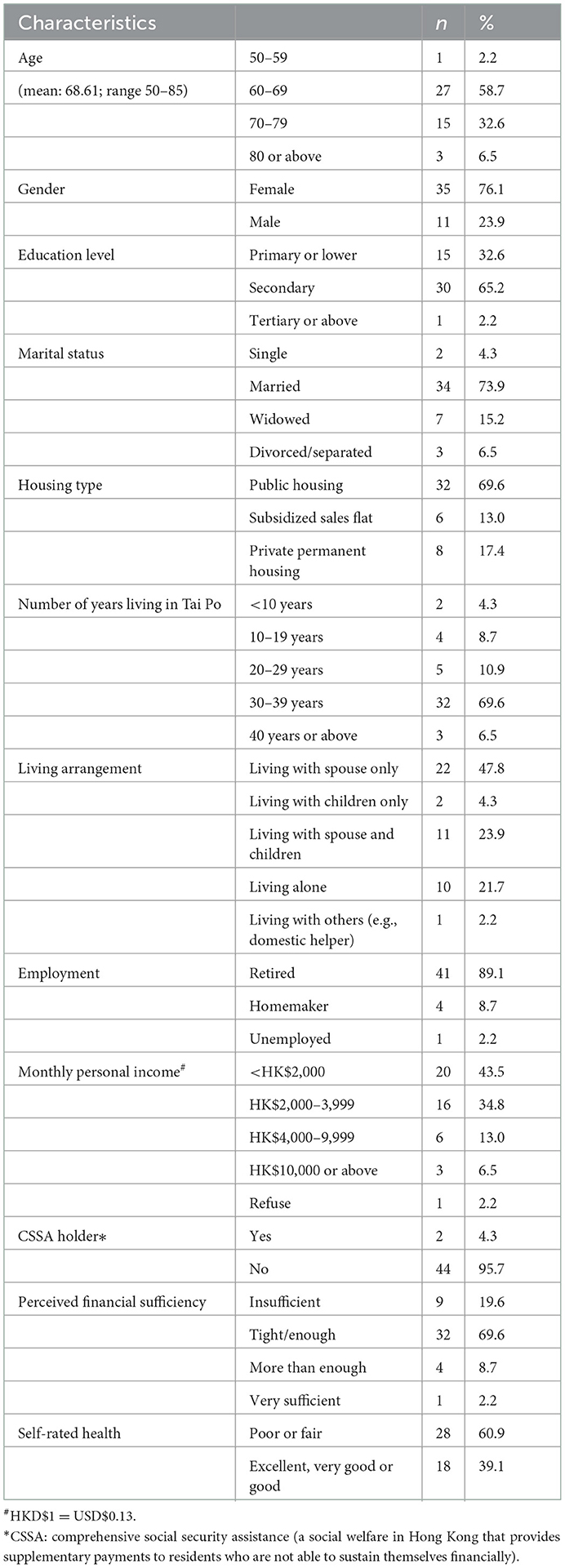
Table 1. Demographic characteristics of the older adult participants (n = 46).
We grouped findings from all participants into five main themes: (1) Perceived impact of hot weather, (2) Adaptation appraisal, (3) Enabling social environment, (4) Perceived barriers to adaptation to hot weather, and (5) new services that could be implemented. We presented the illustrative quotes for each theme in Table 2.
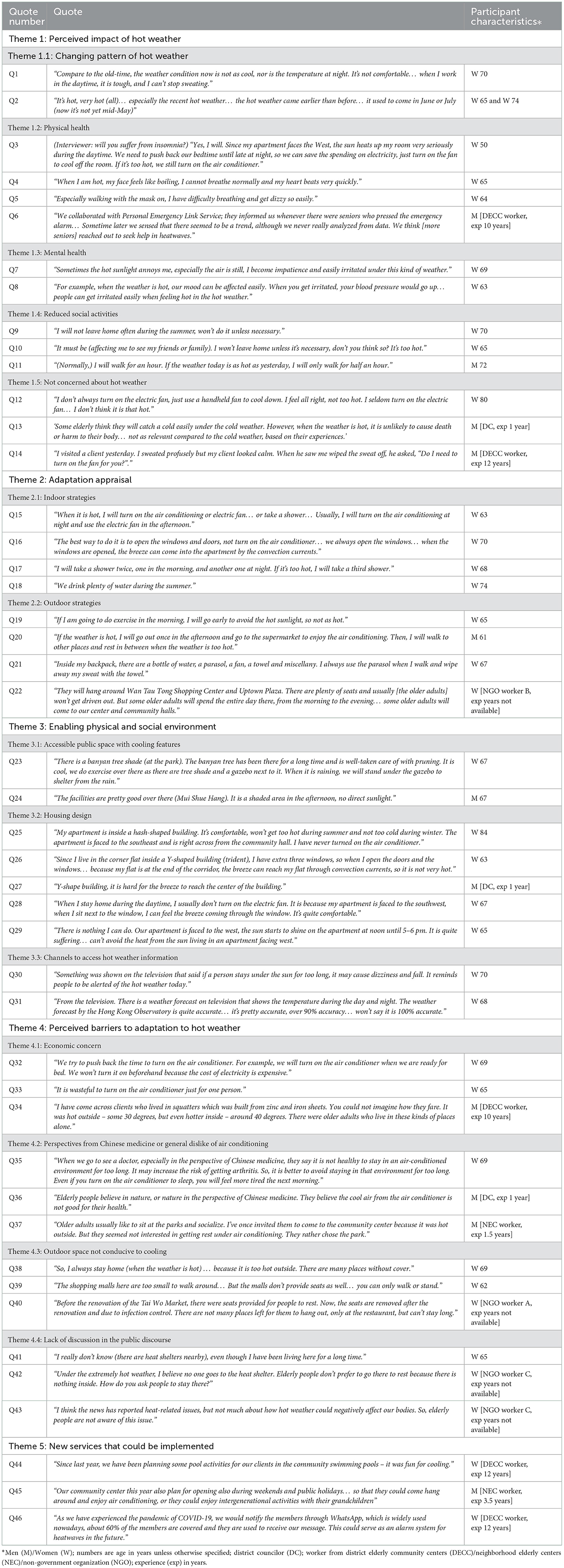
Table 2. Illustrative quotes for each theme.
It was generally agreed among the participants that summers in Hong Kong are becoming increasingly hotter and arrive significantly earlier than one or two decades ago (Quote (Q) 1 and Q2, Table 2).
Some of the older adults expressed that the increasingly hot weather is affecting their physical health. Symptoms such as poorer sleep quality, headache, dizziness and racing heart were sometimes experienced when they went outdoor during summertime (Q3 to Q6). Notably, universal masking intervention during the COVID-19 pandemic has exacerbated the discomfort brought by extreme heat (Q5).
Hot weather also affects mental health–some of the participants reported that they feel more irritable when the temperature is hot (Q7 and Q8).
Some participants reported that they inclined to go out less to avoid heat in hot summer. In such a way, they felt that this situation reduced socialization with friends and relatives (Q10) and physical activities in the outdoor areas (Q9 and Q11).
However, some participants felt that the increasingly hot weather does not have much impact on their health or daily activities (Q12). A district councilor quoted from the older adults whom he came across in his duties, saying that they felt the cold in winter could lead to respiratory diseases, while the heat in summer is less relevant to health (Q13). Another community worker reported an episode of home visit in a hot summer, and his client did not seem to be bothered at all (Q14).
For the older adults who found that the increasingly hot temperature bothers them during summertime, they came up with various solutions to deal with the situation. Here, we grouped the solutions into indoor and outdoor ones. Generally, the participants were aware that there are strategies that they can adopt to stay away from heat and staying indoor during extreme heat is usually more advisable.
When the participants stayed home, they would employ strategies that could improve ventilation, such as opening the windows and turning on fans (Q15 and Q16). They would also use methods to cool themselves directly, such as bathing (Q17). Some participants suggested that they increased hydration during the heat (Q18). Air conditioners have been mentioned as a way of cooling, despite the older adults used it more sparingly (discussed more in Theme 4).
When the participants needed to go outside, some of them reported that they make plans to avoid the heat. For instance, they chose to go out at a time of the day when the heat is less intense, i.e., early mornings or late evenings (Q19). They would reduce the number of times that they need to go out by, say, group several days' of grocery shopping in 1 day. Some of the participants were adept at planning routes between two points through which they could enjoy shaded walkways (Q20). They also plan what to pack in their bags during extreme heat, mainly portable fans, umbrella, towels and a bottle of water (Q21). Despite of the measures they prepare for outdoors, a staff member of NGO reported that some older adults whom they serve preferred to stay in air-conditioned malls during most of the daytime in summer, while some of them would prefer to go to local community centers (Q22).
Participants were generally satisfied with the outdoor environment of the Tai Po district, in particular the parks and greenery that are available to them to seek shelter from heat where there is good ventilation (Q23 and Q24).
Views varied on the design of the buildings in which the live. Some opined that the so-called “hash-shaped” (it is actually a double-tower design resembling two hollow squares joining at one corner of each square) design of their building facilitated ventilation such their homes are much cooling than outside (Q25). Participants who resided in Y-shaped towers, which have semi-enclosed public areas inside buildings, had mixed opinions–some said they feel good ventilation while some disagreed (Q26 and Q27). Participants also agreed that the orientation of the buildings matter for good ventilation because directly facing the sunlight during the day builds up heat in the flat (Q28 and Q29) (Photos of the façade of the buildings in Supplementary material).
Regarding information about hot weather in the public domain, the participants were aware of the hot weather warning issued by the HKO. Most of them received the information regarding hot weather from radio and television channels (Q30 and Q31) and they are generally satisfied with information about hot weather in the public domain.
The opinions on the use of air conditioners as a cooling strategy at home have been mixed. On one hand, the participants agreed that air conditioners are indispensable tools that bring optimum thermal comfort; on the other hand, the costs for electricity have been a concern for most of them given they were all retired with very limited income. Consequently, they adopted various other strategies to limit its use. For example, they only use air conditioners when most of the household members are present, a way what they claimed to be more “cost-efficient” (Q32 and Q33). To the more extreme end, some frontline workers opined that they came across cases in much worse housing conditions with older adults living alone faring poorly in hot weather since they could not afford to rent more proper housing (Q34).
Interestingly, some older adult participants perceived that the “cold” and “damp” from the air conditioners is not good for their health from the Chinese medicine perspective, which could make them feel more tired and musculoskeletal pain (Q35 and Q36). If they were to choose, sometimes they would prefer natural wind rather than air conditioners. A community frontline worker said that his clients rather enjoy the breeze in the park rather than air conditioning in the community center (Q37).
The participants opined that there are not adequate shading devices in their neighborhood, especially in places which they frequently go, such as the bus stops and podium (Q38). Even though there are air-conditioned malls in the neighborhood, the older adults could hardly find a place to sit and relax inside the malls (Q39 and Q40). It appeared that malls generally do not seem to welcome older adults merely sit in the malls and seek shelter from heat (Q22).
The increasingly hot weather is giving, to some extent, more hassles to the older adults in their daily lives. However, the impact of heat is seldom discussed in any public discourse regarding what proper actions to take in the face of more frequent and intense extreme heat. The participants generally did not perceive the government has done adequately to address the problem of extreme heat. Although the government opens the community heat shelters at night when VHWW is hoisted, most of the participants expressed that they were not aware of this at all. Some frontline NGO workers also felt that the community heat shelters were not attractive for the older adults, and that discussions of the heat-health issue were almost non-existent in the public domain (Q41 to Q43).
Service providers generally agreed that as compared to services targeting at the cold weather, there were sparse services targeting at the hot weather. Even though there are still regular services provided by the NEC/DECC such as home visits and community health talks, the activities were not designed to heed to the health needs of the older adults in hot weather. The frontline service workers have brainstormed some forms of activities for future considerations. One participant mentioned a water exercise group in their community center to encourage older adults to maintain physical activity during summer, but that was suspended due to the pandemic (Q44). One service provider shared their plan to open the community centers on Sunday and public holidays. In this way, the older adults could have intergeneration activities and at the same time having a cool shelter (Q45). Another frontline worker also suggested that one could send picture reminders to their clients via texting apps such as WhatsApp to remind them to take appropriate precautions during hot weather (Q46). Taken together, solutions that are creative and without additional manpower and financial resources are urgently warranted.
This study provides insights into the perception and awareness of extreme hot weather among the older adults in a north-eastern neighborhood in Hong Kong and how these older adults adapt to the hot weather and the possible barriers that they face. It was agreed upon among the participants that the weather in recent years has become increasingly hot and this led to some health and social problems for them, although some participants perceived that hot weather did not have any impact in their daily lives and they were not vulnerable. Despite the seriousness, the heat-health issues so far have not received proportionate attention in the public domain. Public education in this regard has been sparse. From the service providers' point of view, there is also a lack of relevant community services or support for older adults in hot weather. However, the older adults we interviewed were generally flexible and adapting to the increasingly hot weather with their own means, albeit their conception about air-conditioners from the Chinese medicine point of view might have limited their use. Indoor environment and community facilities are important resources for older adults to adapt to hot weather.
Our findings that some older adults perceived that hot weather did not constitute a health concern and that they are not vulnerable groups are consistent with previous findings in Western settings (35, 44). There could be two reasons for this finding. First, understandably, some participants noted that they endured intense manual labor jobs in the pre-air-conditioned era, further strengthening the belief that they were well in control of their health and adaptation was not necessarily. Second, older adults might be less likely to adopt adaptive behaviors given their physiological decline following the natural process of aging such that they become less sensitive to ambient temperature and thirst (14). We also highlighted that extreme hot weather affects older adults' mental health when some participants reported that they felt more anxious when the weather is hot and such weather conditions limited their social and physical activities, which was similar to what was reported in a previous study in Adelaide of Australia (45).
Overall, the older adults who we interviewed mostly agreed that the changing climate increasingly become a problem to them, and they were reasonably flexible to adapt. A previous local cross-sectional study reported that perception of risk of extreme hot weather is not related to the utilization and ownership of cooling devices in the Hong Kong population (38). Our study corroborated by showing that almost all the older participants we interviewed owned air-conditioners, but they are more reluctant to use them. Although the use of air-conditioners has been considered as one of the strong protective factors against heat-related illnesses (46), its use could be limited especially in older adults given the concern for the cost of electricity, a finding which is consistent with a previous qualitative study conducted in a sample of older adults in Australia (47). This is perhaps partly reflective of the relatively lower socioeconomic status of our participants, who mainly lived in public housing estates, compared to the rest of the Hong Kong population.
We found that our participants often reported that they reduce the frequency of going out when the outdoor temperature, as informed by the media, is hot. This is opposite to what was reported in a small study with 29 older adult households of Detroit of the United States (48). Using hourly logs to record the participants' behaviors, White-Newsome and colleagues (48) reported that the older adults were more like to go outside of their places of residence when outdoor temperature increased. This is perhaps because the building density of Detroit is less than that of Hong Kong, resulting in a less intense urban heat island and greater thermal comfort even amidst the heat. Reduced ventilation in typical residential neighborhoods in Hong Kong also discourages outdoor activities.
Heat action plans are now common in many developed countries (21, 49). However, the perspectives of public health were not integrated in the current climate action plan even given mounting local and international evidence of the heat-health relationship. Currently, the HKO issues VHWW signal to alert the public and, accordingly, the Home Affairs Department operates temporary night-time heat shelters when such warning is hoisted. The night-time heat shelters only seemed to have lukewarm reception in the public because they are usually situated not according to the geographical distribution of urban heat hazard spots (50) and there are no meaningful activities to engage their users, discounting the usefulness and attractiveness of these centers. It is welcome to see that, as of recently, the HKO added messages along with the VHWW signal to remind the public to take particular care of older adults and other vulnerable groups in the case of heat. However, other than that, as noted by our community service providers in this study, the discussion of the heat-health issue has only very recently started to gain traction in the public discourse. The Hong Kong government recently published the Climate Action Plan 2050, which proposed that as a part of the plan to mitigate urban heat, the government will work to improve building design and increase urban vegetation. However, little was discussed on how to prepare the local community to become more aware and prepared for the future climate scenario. Resources are often available in the community, but there is a lack of ingenuity and collective will to integrate and coordinate these resources into helping especially the vulnerable groups to adapt to extreme hot weather. For instance, several of our older adults participants and community service providers opined that publicly air-conditioned spaces in Hong Kong such as shopping malls can provide a cool environment for the older adults without the worry of costs of electricity. Unlike in other settings, these public spaces in Hong Kong are often within walkable distances within a community hence the older adults can reach easily (47). Nonetheless, it was mostly agreed upon by our participants that these spaces often lack places for older adults to sit and relax.
Contextualizing the heat-health issue in the older population entails an understanding of the underlying social, cultural, and institutional factors. It is therefore context-specific for the older adults in Hong Kong to believe that the use of air-conditioners has implications to their health from the angle of Chinese medicine, as discussed by some of our participants. Such aversion could have stemmed from the idea that “nefarious Wind” could cause “disharmony” in the body and causes symptoms generally called “external wind cold” such as headaches, generalized aches and runny nose (51). While part of it could be related to influenza-like illnesses, this conception could affect older adults' attitude to use air-conditioners. It is therefore suggested that when formulating heat-health messages to the older adults in Hong Kong or more broadly the Chinese community, a wide variety of alternative strategies could be suggested in addition to the use of air-conditioners such that older adults could be provided with ample choices of strategies to adapt.
In addition to public air-conditioned spaces, as our participants noted, another indoor space that was deemed to be an important shelter from heat is their homes. Compact living spaces in high-rise buildings is one of the unique characteristics of urban configuration of Hong Kong, which often linked to poor thermal comfort resulting from intense solar radiation, poor ventilation, and the slow release of heat from building materials, particularly during intense heat in summertime (52). As a matter of fact, air conditioning at home still remains a major solution for older adults to relieve from heat. It is welcome to see local charities started community initiatives to subsidize electricity bills for older adults who are financially incapable (53). The government could also consider the possibility of formal subsidy for electricity for needy older adults during hot seasons or minor home modifications to improve indoor thermal comfort. However, in the long run, our city has to adopt of adaptive design following the future climate scenario. Strategies such as using higher albedo materials covering urban built surfaces (e.g., building ceilings or pavements), facilitation of air turbulence within a community or incorporation of blue-green spaces were all proven to bring better thermal comfort for urban dwellers (54). The use of air-conditioning could therefore be minimized.
Our interviews revealed that the community service providers were in general not well equipped with heat-health knowledge. This is in line with the lack of public discourse and could potentially explain a lack of coordinated and targeted efforts to mitigate the heat situation faced by the older adults. Empowering the frontline workers of DECC and NEC in Hong Kong as well as the district councilors will constitute a salient strategy as they have expansive reach to older adults in the community. Reaching out to particularly vulnerable targets, such as those living in inadequate housing, living alone or those with dementia, will be essential. Creative strategies such as texting picture reminders to their clients will also be potentially helpful.
The current study has recruited both older adults and frontline workers in the community, who have enriched our insights from the angle of service providers in addition to the subjective experience of the older adults. Our interviews were conducted in summertime such that the participants did not have to rely on memory to recall the experience of hot weather. However, the current study has limitations. First, our older adult participants were mostly sampled from the two designated public housing estates in Tai Po district. Our sample and hence their opinions might not be representative for older adults in other housing types and from other districts. Future studies could consider recruiting samples from other districts in Hong Kong to confirm the findings in this study. However, in a broader sense, this sample of participants were knowledgeable about the climatic conditions on a neighborhood scale. The meanings and processes of everyday lives in the midst of extreme hot weather expressed by the participants would therefore be relevant to other highly dense urbanized settings. Second, the convenience sampling nature of our study implied that our sample was only constituted of subjects who were more aware of the issue of heat than the general population. Future quantitative studies, such as a territory-wide questionnaire, could confirm the extent to which the older population are aware of the heat-health issue. Third, our sample was only limited to those who were able to independently walk to the community center, which rendered us unable to assess the views of those most vulnerable to heat.
Our findings showed that older adults in Hong Kong are concerned that extreme hot weather constituted a surging problem for them physically, mentally and socially. While some of the older adults we interviewed were reasonably flexible and adaptive, some others believe that there is no need to adapt, which could be problematic in the long run as the future climate scenario continues to unfold. Discussions and education effort regarding the heat-health issue in the public domain remain scarce. Multilateral efforts are urgently needed to co-create a heat action plan to improve community awareness and resilience.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Survey and Behavioral Research Ethics Committee of the Chinese University of Hong Kong. The patients/participants provided their written informed consent to participate in this study.
EL, KL, and JW conceptualized the study. EL, PC, and KL coordinated the recruitment of subjects and supervised the data transcription process by research assistants. EL, PC, KC, and MK conducted the data analysis, synthesized the findings, reviewed the literature, and wrote the manuscript. All authors participated in critically reviewing and intellectually input to the drafts of the manuscript. All authors contributed to the article and approved the submitted version.
This study was funded by Research Grants Council Research Impact Fund (R4046-18F).
The authors would like to thank for the participants who have participated the focus group interviews.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1056800/full#supplementary-material
1. IPCC. Summary for policymakers. In:Pörtne H-O, Roberts DC, Poloczanska ES, Mintenbeck K, Tigno Mr, Alegría A, Craig M, Langsdorf S, Löschke S, Möller V, Okem A, Rama B, editors. Climate Change 2022: Impacts, Adaptation, and Vulnerability. Contribution of Working Group II to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge; New York, NY: Cambridge University Press (2022). p. 3–33. doi: 10.1017/9781009325844.001
2. Luo M, Lau N-C. Heat waves in southern China: synoptic behavior, long-term change, and urbanization effects. J Clim. (2017) 30:703–20. doi: 10.1175/JCLI-D-16-0269.1
3. HKO. The Year's Weather−2021. (2022). Available online at: https://www.weather.gov.hk/en/wxinfo/pastwx/2021/ywx2021.htm (accessed November 11, 2022).
4. Development Bureau and Planning Department, Towards A Planning Vision and Strategy Transcending 2030. (2017). Available online at: https://www.pland.gov.hk/pland_en/p_study/comp_s/hk2030plus/document/2030+Booklet_Eng.pdf
5. Shi Y, Ren C, Cai M, Lau KKL, Lee TC, Wong WK. Assessing spatial variability of extreme hot weather conditions in Hong Kong: a land use regression approach. Environ Res. (2019) 171:403–15. doi: 10.1016/j.envres.2019.01.041
6. Cissé G, McLeman R, Adams H, Aldunce P, Bowen K, Campbell-Lendrum D, et al. Health, wellbeing, and the changing structure of communities. In:Pörtne H-O, Roberts DC, Poloczanska ES, Mintenbeck K, Tigno Mr, Alegría A, Craig M, Langsdorf S, Löschke S, Möller V, Okem A, Rama B, editors. Climate Change 2022: Impacts, Adaptation, and Vulnerability. Contribution of Working Group II to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge; New York, NY: Cambridge University Press (2022). p. 1041–170. doi: 10.1017/9781009325844.009
7. Rohr JR, Cohen JM. Understanding how temperature shifts could impact infectious disease. PLoS Biol. (2020) 18:e3000938. doi: 10.1371/journal.pbio.3000938
8. Leung Y, Yip K, Yeung K. Relationship between thermal index and mortality in Hong Kong. Meteorol Appl. (2008) 15:399–409. doi: 10.1002/met.82
9. Yi W, Chan AP. Effects of temperature on mortality in Hong Kong: a time series analysis. Int J Biometeorol. (2015) 59:927–36. doi: 10.1007/s00484-014-0895-4
10. Lam HC-y, Li AM, Chan EY-y, Goggins WB. The short-term association between asthma hospitalisations, ambient temperature, other meteorological factors and air pollutants in Hong Kong: a time-series study. Thorax. (2016) 71:1097–109. doi: 10.1136/thoraxjnl-2015-208054
11. Lam HCY, Chan JCN, Luk AOY, Chan EYY, Goggins WB. Short-term association between ambient temperature and acute myocardial infarction hospitalizations for diabetes mellitus patients: a time series study. PLoS Med. (2018) 15:e1002612. doi: 10.1371/journal.pmed.1002612
12. Chau PH, Lau K, Qian X, Luo H, Woo J. Visits to the accident and emergency department in hot season of a city with subtropical climate: association with heat stress and related meteorological variables. Int J Biometeorol. (2022) 66:1955–71.
13. Chau PH, Yip PSF, Lau EHY, Ip YT, Law FYW, Ho RTH, et al. Hot weather and suicide deaths among older adults in Hong Kong, 1976–2014: a retrospective study. Int J Environ Res Public Health. (2020) 17:3449. doi: 10.3390/ijerph17103449
14. Ebi KL, Capon A, Berry P, Broderick C, de Dear R, Havenith G, et al. Hot weather and heat extremes: health risks. Lancet. (2021) 398:698–708. doi: 10.1016/S0140-6736(21)01208-3
15. Jay O, Capon A, Berry P, Broderick C, de Dear R, Havenith G, et al. Reducing the health effects of hot weather and heat extremes: from personal cooling strategies to green cities. Lancet. (2021) 398:709–24. doi: 10.1016/S0140-6736(21)01209-5
16. Meade RD, Akerman AP, Notley SR, McGinn R, Poirier P, Gosselin P, et al. Physiological factors characterizing heat-vulnerable older adults: a narrative review. Environ Int. (2020) 144:105909. doi: 10.1016/j.envint.2020.105909
17. Watts N, Amann M, Arnell N, Ayeb-Karlsson S, Beagley J, Belesova K, et al. The 2020 report of the Lancet Countdown on health and climate change: responding to converging crises. Lancet. (2021) 397:129–70. doi: 10.1016/S0140-6736(20)32290-X
18. Åström C, Åström DO, Andersson C, Ebi KL, Forsberg B. Vulnerability reduction needed to maintain current burdens of heat-related mortality in a changing climate—magnitude and determinants. Int J Environ Res Public Health. (2017) 14:741. doi: 10.3390/ijerph14070741
19. Lee JY, Kim H. Projection of future temperature-related mortality due to climate and demographic changes. Environ Int. (2016) 94:489–94. doi: 10.1016/j.envint.2016.06.007
20. Wang D, Lau KKL, Ren C, Goggins WBI, Shi Y, Ho HC, et al. The impact of extremely hot weather events on all-cause mortality in a highly urbanized and densely populated subtropical city: a 10-year time-series study (2006–2015). Sci Total Environ. (2019) 690:923–31. doi: 10.1016/j.scitotenv.2019.07.039
21. United Nations Office for Disaster Risk Reduction - Regional Office for Asia Pacific. Heatwaves: Addressing a Sweltering Risk in Asia-Pacific. (2022). Available online at: https://www.undrr.org/publication/heatwaves-addressing-sweltering-risk-asia-pacific
22. Wilson L, Black D, Veitch C. Heatwaves and the elderly: the role of the GP in reducing morbidity. Aust Fam Phys. (2011) 40:637–40.
23. Chau P, Chan K, Woo J. Hot weather warning might help to reduce elderly mortality in Hong Kong. Int J Biometeorol. (2009) 53:461–8. doi: 10.1007/s00484-009-0232-5
24. Grothmann T, Patt A. Adaptive capacity and human cognition: the process of individual adaptation to climate change. Glob Environ Change. (2005) 15:199–213. doi: 10.1016/j.gloenvcha.2005.01.002
25. Becker MH. The health belief model and sick role behavior. Health Educ Monogr. (1974) 2:409–19. doi: 10.1177/109019817400200407
26. Floyd DL, Prentice-Dunn S, Rogers RW. A meta-analysis of research on protection motivation theory. J Appl Soc Psychol. (2000) 30:407–29. doi: 10.1111/j.1559-1816.2000.tb02323.x
27. Gardner GT, Stern PC. Environmental Problems and Human Behavior. Boston, MA: Allyn & Bacon (1996).
28. Kafeety A, Henderson SB, Lubik A, Kancir J, Kosatsky T, Schwandt M. Social connection as a public health adaptation to extreme heat events. Can J Publ Health. (2020) 111:876–9. doi: 10.17269/s41997-020-00309-2
29. Adger WN. Social aspects of adaptive capacity. Climate change, adaptive capacity and development. World Sci. (2003) 29–49. doi: 10.1142/9781860945816_0003
30. Commission on Social Determinants of Health. Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health: Final Report of the Commission on Social Determinants of Health. World Health Organization (2008). Available online at: https://apps.who.int/iris/handle/10665/43943
31. Eady A, Dreyer B, Hey B, Riemer M, Wilson A. Original mixed methods research-Reducing the risks of extreme heat for seniors: communicating risks and building resilience. Health Promot Chronic Dis Prev Can. (2020) 40:215. doi: 10.24095/hpcdp.40.7/8.01
32. Browning CR, Wallace D, Feinberg SL, Cagney KA. Neighborhood social processes, physical conditions, and disaster-related mortality: the case of the 1995 Chicago heat wave. Am Sociol Rev. (2006) 71:661–78. doi: 10.1177/000312240607100407
33. Xu R, Zhao Q, Coelho MS, Saldiva PH, Abramson MJ, Li S, et al. Socioeconomic level and associations between heat exposure and all-cause and cause-specific hospitalization in 1,814 Brazilian cities: a nationwide case-crossover study. PLoS Med. (2020) 17:e1003369. doi: 10.1371/journal.pmed.1003369
34. Hansen A, Bi P, Pisaniello D, Nitschke M, Tucker G, Newbury J, et al. Heat-health behaviours of older people in two Australian states. Aust J Ageing. (2015) 34:E19–25. doi: 10.1111/ajag.12134
35. Abrahamson V, Wolf J, Lorenzoni I, Fenn B, Kovats S, Wilkinson P, et al. Perceptions of heatwave risks to health: interview-based study of older people in London and Norwich, UK. J Public Health. (2009) 31:119–26. doi: 10.1093/pubmed/fdn102
36. Vu A, Rutherford S, Phung D. Heat health prevention measures and adaptation in older populations—a systematic review. Int J Environ Res Public Health. (2019) 16:4370. doi: 10.3390/ijerph16224370
37. Li J, Xu X, Ding G, Zhao Y, Zhao R, Xue F, et al. A cross-sectional study of heat wave-related knowledge, attitude, and practice among the public in the Licheng District of Jinan City, China. Int J Environ Res Public Health. (2016) 13:648. doi: 10.3390/ijerph13070648
38. Gao Y, Chan EY, Lam HC, Wang A. Perception of potential health risk of climate change and utilization of fans and air conditioners in a representative population of Hong Kong. Int J Disaster Risk Sci. (2020) 11:105–18. doi: 10.1007/s13753-020-00256-z
39. Social Welfare Department. List of Neighbourhood Elderly Centre Hong Kong: HKSAR Government. (2022). Available online at: https://www.swd.gov.hk/en/index/site_pubsvc/page_elderly/sub_csselderly/id_neighbourhood/ (accessed November 11, 2022).
40. Social Welfare Department. List of District Elderly Community Centres Hong Kong: HKSAR Government. (2022). Available online at: https://www.swd.gov.hk/en/index/site_geoinfomap/page_eldermap/sub_ccss/id_decc/ (accessed November 11, 2022).
41. Palinkas LA, Horwitz SM, Green CA, Wisdom JP, Duan N, Hoagwood K. Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Adm Policy Ment Health. (2015) 42:533–44. doi: 10.1007/s10488-013-0528-y
42. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
44. Sheridan SC, A. survey of public perception and response to heat warnings across four North American cities: an evaluation of municipal effectiveness. Int J Biometeorol. (2007) 52:3–15. doi: 10.1007/s00484-006-0052-9
45. Hansen A, Bi P, Nitschke M, Ryan P, Pisaniello D, Tucker G. The effect of heat waves on mental health in a temperate Australian city. Environ Health Perspect. (2008) 116:1369–75. doi: 10.1289/ehp.11339
46. Bouchama A, Dehbi M, Mohamed G, Matthies F, Shoukri M, Menne B. Prognostic factors in heat wave–related deaths: a meta-analysis. Arch Intern Med. (2007) 167:2170–6. doi: 10.1001/archinte.167.20.ira70009
47. Hansen A, Bi P, Nitschke M, Pisaniello D, Newbury J, Kitson A. Perceptions of heat-susceptibility in older persons: Barriers to adaptation. Int J Environ Res Public Health. (2011) 8:4714–28. doi: 10.3390/ijerph8124714
48. White-Newsome JL, Sánchez BN, Parker EA, Dvonch JT, Zhang Z, O'Neill MS. Assessing heat-adaptive behaviors among older, urban-dwelling adults. Maturitas. (2011) 70:85–91. doi: 10.1016/j.maturitas.2011.06.015
49. Sheehan MC, Fox MA, Kaye C, Resnick B. Integrating health into local climate response: Lessons from the US CDC Climate-Ready States and Cities Initiative. Environ Health Perspect. (2017) 125:094501. doi: 10.1289/EHP1838
50. Hua J, Zhang X, Ren C, Shi Y, Lee TC. Spatiotemporal assessment of extreme heat risk for high-density cities: a case study of Hong Kong from 2006 to 2016. Sustain Cities Soc. (2021) 64:102507. doi: 10.1016/j.scs.2020.102507
51. Chinese Medicine Regulatory Office. Health Preservation in Four Seasons in Chinese Medicine - Prevention of Heat Stroke in Summer Hong Kong: Department of Health, HKSAR Government. (2021). Available online at: https://www.cmro.gov.hk/html/eng/useful_information/public_health/pamphlet/Health_Preservation_in_Four_Seasons.html (accessed November 11, 2022).
52. Kwok YT, Lau KKL, Ng EYY. The influence of building envelope design on the thermal comfort of high-rise residential buildings in Hong Kong. In: Proceedings of the 10th Windsor Conference: Rethinking Comfort. Windsor: NCEUB (2018).
53. Service HKCSS. Elderly Concession Scheme. (2022). Available online at: https://www.hkcss.org.hk/elderly-concession-scheme/?lang=en (accessed October 19, 2022).
Keywords: extreme heat, older adult, health inequalities, adaptation, climate change
Citation: Lai ETC, Chau PH, Cheung K, Kwan M, Lau K and Woo J (2023) Perception of extreme hot weather and the corresponding adaptations among older adults and service providers–A qualitative study in Hong Kong. Front. Public Health 11:1056800. doi: 10.3389/fpubh.2023.1056800
Received: 29 September 2022; Accepted: 09 January 2023;
Published: 10 February 2023.
Edited by:
Soohyoung Rain Lee, Yeshiva University, United StatesReviewed by:
Zhiwei Xu, The University of Queensland, AustraliaCopyright © 2023 Lai, Chau, Cheung, Kwan, Lau and Woo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eric T. C. Lai,  ZXRjbGFpQGN1aGsuZWR1Lmhr
ZXRjbGFpQGN1aGsuZWR1Lmhr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.