
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 25 October 2022
Sec. Digital Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.979448
This article is part of the Research Topic Machine Learning Used in Biomedical Computing and Intelligence Healthcare, Volume III View all 9 articles
 Roland Roller1,2*†
Roland Roller1,2*† Manuel Mayrdorfer2,3†
Manuel Mayrdorfer2,3† Wiebke Duettmann2
Wiebke Duettmann2 Marcel G. Naik2,4Danilo Schmidt5
Marcel G. Naik2,4Danilo Schmidt5 Fabian Halleck2Patrik Hummel6Aljoscha Burchardt1Sebastian Möller1
Fabian Halleck2Patrik Hummel6Aljoscha Burchardt1Sebastian Möller1 Peter Dabrock7
Peter Dabrock7 Bilgin Osmanodja2‡
Bilgin Osmanodja2‡ Klemens Budde2‡
Klemens Budde2‡Patient care after kidney transplantation requires integration of complex information to make informed decisions on risk constellations. Many machine learning models have been developed for detecting patient outcomes in the past years. However, performance metrics alone do not determine practical utility. We present a newly developed clinical decision support system (CDSS) for detection of patients at risk for rejection and death-censored graft failure. The CDSS is based on clinical routine data including 1,516 kidney transplant recipients and more than 100,000 data points. In a reader study we compare the performance of physicians at a nephrology department with and without the CDSS. Internal validation shows AUC-ROC scores of 0.83 for rejection, and 0.95 for graft failure. The reader study shows that predictions by physicians converge toward the CDSS. However, performance does not improve (AUC–ROC; 0.6413 vs. 0.6314 for rejection; 0.8072 vs. 0.7778 for graft failure). Finally, the study shows that the CDSS detects partially different patients at risk compared to physicians. This indicates that the combination of both, medical professionals and a CDSS might help detect more patients at risk for graft failure. However, the question of how to integrate such a system efficiently into clinical practice remains open.
Kidney transplantation is the treatment of choice for patients with end-stage kidney disease (ESKD) although it requires lifelong post-transplant care (1, 2). Graft failure is often multifactorial (3, 4), therefore it is important to continuously account for a diverse set of potentially detrimental events in clinical care, depending on individual patient risk profiles. The heterogeneity of causes leading to graft failure makes it very challenging to predict the course of a transplant life and finally graft failure. Given the high number of graft failures affected by over-immunosuppression (infections, drug toxicity, cancer) and under-immunosuppression (rejection), adjustment of immunosuppressive treatment is one of the most powerful tools in clinical practice (3–5). However, it is often not clear how to interpret the current risk profile due to an overwhelming amount of data to be integrated for decision-making. This dilemma is further enhanced by the lack of time in clinical routine. Therefore, clinical decision support systems able to integrate and interpret the often highly complex status of a kidney transplant recipient are an interesting option to mitigate this problem. In recent years, an increasing number of machine learning (ML) solutions have been developed to support medical professionals. However, many publications revolve around novel ML models with the goal of outperforming baselines and pushing the boundaries in terms of better performance (6, 7). Only a few approaches go beyond the pure improvement of ML models and provide detailed technical analyses or insights about how and what the model has learnt (8, 9). Unfortunately, in most cases the system is not evaluated together with the end user. This renders interpretation of the actual impact in clinical routine difficult. In order to improve medical care in the real world, ML models not only have to be accurate and precise, they also need to be embedded in the patient journey and accepted by medical professionals. In this work, we present a Clinical Decision Support System aiming to detect in advance patients at risk of (a) rejection, and (b) death-censored graft failure, to occur within the next 90 days. Additionally, we evaluate the system together with medical professionals.
For simplicity, we refer to death-censored graft failure as graft failure, physician as MD (medical doctor), ML-based clinical decision support system as AI, and physicians with AI support as MD + AI. The study was approved by the ethics committee of Charité Universitätsmedizin Berlin (ID: EA4/156/20).
Baseline for this work is TBase (10), a database designed for kidney transplant recipients (KTR), implemented over 20 years ago at Charité. As patients are supposed to receive a follow-up at the transplant center 3–4 times a year, TBase includes fine-grained information about the patients over many years including demographics, laboratory data, medication, medical notes, diagnoses, radiology, and pathology reports. Death-Censored Graft Failure is defined as the initiation of renal replacement therapy (dialysis or re-transplantation). Graft loss due to death with a functioning graft is not included in the current work. Rejection is defined according to the Banff 2017 classification (11), as previously described (3).
The complete risk prediction scenario is built up around data points (DP), which describe the particular moment when new data about a patient is inserted in the database. If one of the endpoints occurs within the target prediction window of 90 days, the DP will be labeled as true, otherwise as false. According to those DPs, patient information (features) which are available at this moment, are extracted (e.g., the new and the previous lab values, or the current diagnoses) and used as input information of our model. Moreover, we enrich the data by additional information, such as mean scores or gradients of successive values. Each model uses about 300 different features, consisting of structured information (e.g., vital parameters, lab values, medication) and bag-of-word features (single word features taken from findings or diagnoses). Table 1 provides an overview of the most relevant features for each model. A more detailed overview of the features used, is provided in Supplementary Table 6.
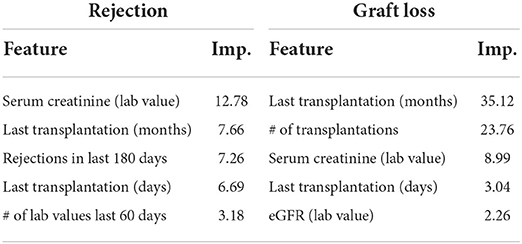
Table 1. Overview of the most relevant features (top 5) of each model (global features), including its importance (Imp.).
Next, data is filtered to generate a meaningful, reliable, valid, and realistic dataset: Only data points with a follow-up data point within the next 15–180 days are used. This filter has been implemented to exclude gaps in patient follow-up ensuring reliability of endpoint evaluation. The resulting dataset is referred to as “cohort.” The cohort includes 1,516 different patients, with a mean of 67.89 data points (moments during transplant life with new data input) per patient. The cohort is then cleaned and divided into a training, development, and test dataset for ML. An overview about additional data characteristics as well as the exclusion criteria is provided in the Supplementary material.
The ML component relies on Gradient Boosted Regression Trees (GBRTs). In comparison to neural methods, GBRTs can be quickly trained, and therefore quickly modified and further optimized, without the need of a strong computer cluster. Also, tree-based methods are well-established in the context of CDSS, and can be also easier understood by non-experts, thus exhibiting some sort of transparency.
The resulting dataset is strongly unbalanced, as it contains a larger number of negative instances compared to positive ones. That means, in most cases an endpoint does not occur in the target period for the given data point (Supplementary Table 3). As a large portion of negative data can influence the quality of the classifier, and slows down the training, negative samples are randomly down-sampled within the training split. Controlled upsampling (SMOTE) (12), and controlled downsampling (NCA) (13) did not lead to any significant improvements. For the final setup, a training ratio of 1:3 was chosen, as it showed the most promising results during the initial experiments.
For the internal validation, we randomly assigned 70% of the patients into the training, 15% into the development and 15% into the test split. This step is repeated 50 times for the cross-validation. That way, patients within training, development and test data always change. Therefore, reported mean scores and 95% CI (confidence interval) provide a good approximation of our model.
For the reader study instead, data is prepared differently: First, the test set is defined and all patients of the test set removed from the cohort. The test set contains 120 patients, which was the sample size calculated in the power analysis shown in Instructions for participants in Supplementary material. As endpoints have a low frequency, and to ensure that a sufficient number of events occur, data points are selected randomly, but in a controlled way. Each endpoint occurs at least 20 times in the reader study test set. Then, the remaining patients with their data points are split into a training and development set, using a split of 80 and 20%. Note, as opposed to the AI system, the physician can access the complete patient history, including text notes, medical reports, and a longer time range than the last two entries (e.g., laboratory tests) of the last year. The physicians in the reader study are informed that the endpoint frequency might not reflect real-world conditions but (14) are not informed about the exact distribution.
The final ML model relies on GBRTs implemented in python using scikit-learn, with 300 estimators, a learning rate of 0.1, max-depth of 3, and a random-state of 0. The model is trained on a Ubuntu 18.04.3 LTS server with a Intel Core i9-7900X 3.30GHz. The training of the model with ca. 10k training examples take about 2.5 min. This would describe one cross-validation step in our first experiment. The model with technical descriptions can be made available on request.
To provide an informative decision support system, a dashboard was developed including the following information: (a) current risk score, (b) development of the risk score over time within a graph, (c) categorization of the risk scores into a traffic light system (green, yellow, red), as well as (d) presentation of relevant features which influence the decision of the risk score. For each given data point, two dashboard-graphs (including the additional information) are generated, one for each endpoint.
Figure 1 presents an example of the dashboard, presenting the time on the x-axis and the risk score on the y-axis. All data points of the last year, including corresponding risk scores, are visualized in the graph. The graph itself is divided into different zones, a green zone indicating a low risk, a yellow zone which indicates a higher risk, and a red zone which indicates the highest risk. Each zone is defined by a threshold, which was generated on the development set by identifying the optimal F-Scores–F2 score for the border to the yellow zone, and F0.5 to indicate the red zone.
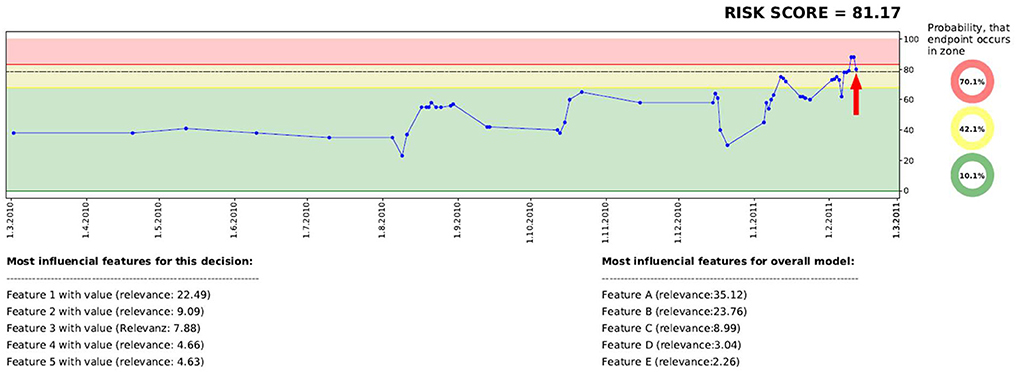
Figure 1. Visualization of the dashboard, including historic risk scores, a traffic light system, as well as a model and a decision-based explanation.
Overall, eight physicians, four junior MDs who have not completed their specialization and four senior MDs with specialization in internal medicine or nephrology, participate in the reader study (for participant demographics see Supplementary Table 5). MDs were to examine all information available about the kidney transplant recipient in the database mentioned above (see Data; additionally all string-based discharge summaries were available to the physicians) and to forecast the two endpoints, once without and once with the help of AI. Each MD examines 15 different DPs with the corresponding patient case history without CDSS, and then 15 other DPs of different patients with CDSS. The DPs are randomly assigned to the physicians in both parts of the study, so that no physician assesses the same patient twice. Before starting the second part of the experiment, each physician receives a small tutorial (see Procedure Supplementary material) to understand the dashboard of the CDSS. In the first step, the MD receives a data point of the cohort and estimates how likely, in terms of probability (0–100%), each endpoint might occur in our target period (90 days). In the second part, the dashboard with the AI prediction is presented simultaneously with patient data (MD + AI). In both rounds, each MD has up to 30 min time to study the de-identified medical history of the patients. Physicians were provided with the exact endpoint definitions.
In order to examine the significance of the different ROC (Receiver Operating Characteristic) scores in our study, the implementation of DeLong et al. (14) is applied (paired, one-tailed, in case of Table 2; and unpaired, one-tailed in case of Table 3). To explore the significance of the influence of the AI system, we use a two-tailed t-test implemented in SciPy.
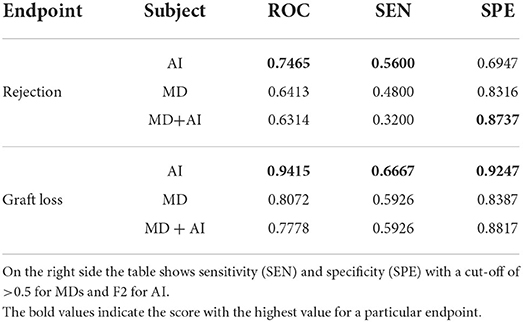
Table 2. AUC-ROC results on the reader study test set of AI, MD, and MD + AI for the endpoints death-censored graft failure and rejection.
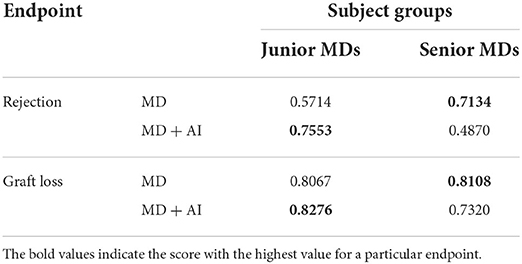
Table 3. AUC-ROC performance of junior and senior physician groups in both parts of the study.
The results of the internal validation are presented in Table 4. Considering the prediction period of 90 days, our model shows an AUC-ROC (Area Under the Curve of the Receiver Operating Characteristic) score of 0.83 and 0.95 for rejection and graft failure, respectively. The results also show that model performance shows only slight changes when extending the prediction period to 180 or 360 days.
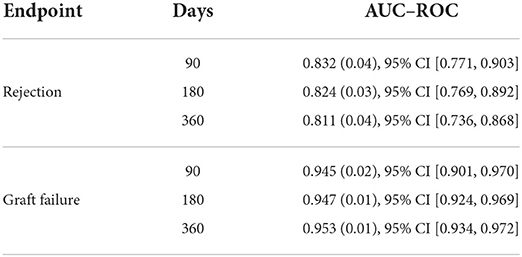
Table 4. Risk prediction results in terms of AUC-ROC including 95% CI during internal validation, using a resampling approach with 50-fold cross validation on retrospective data.
For the reader study, a new ML model is trained from scratch, using the configuration of the internal validation, but using a new split of training, development, and test data, as described above. The predictions of the ML model on the test set are used as CDSS for the physicians (MD + AI).
The results of the reader study are presented in Table 2 and Figure 2. The results show that AI outperforms MDs (graft failure 0.9415 vs. 0.8072, p = 0.005; rejection 0.7465 vs. 0.6413, p = 0.063). Moreover, MDs achieve slightly better results without CDSS. Finally, the table shows that using our cut-off (F2 for AI and > 0.5 for MDs) AI has got a higher sensitivity in comparison to MDs alone.
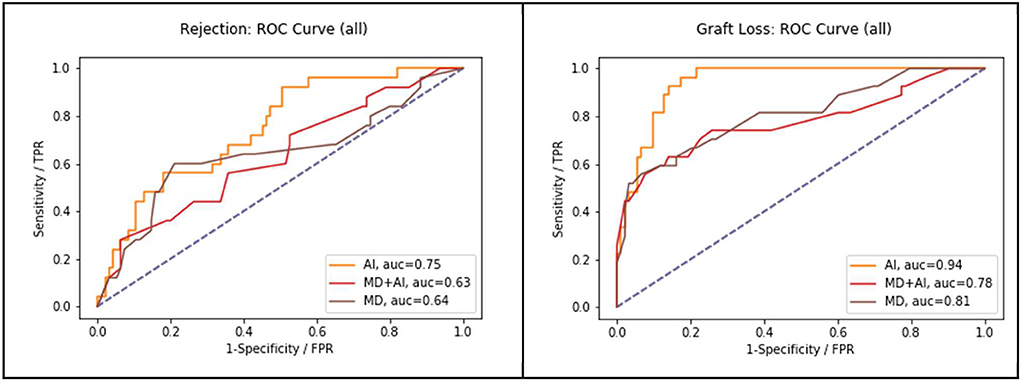
Figure 2. Performance of MD in comparison to AI and MD + AI, in terms of AUC-ROC on all three endpoints.
Comparison of the results of junior MDs and senior MDs are presented in Table 3. Without AI, senior MDs tend to score higher than junior MDs (graft failure 0.8108 vs. 0.8067; rejection 0.7134 vs. 0.5714). Moreover, junior MDs achieve higher results with CDSS for rejection (0.5714 vs. 0.7553, p = 0.075). Also, junior MDs with AI score higher than senior MDs with AI. And finally, senior MDs achieve a better score without AI.
To explore the influence of the CDSS on physicians, we calculate the difference of each prediction to the prediction made by the AI. MDs make a prediction in terms of probability (0–100%) and AI in terms of regression (0–100). Table 5 shows the mean difference scores, for all MDs as well as for junior and senior MDs separately. An additional box plot of the mean distance is presented in Figure 3. The table shows that in all cases the mean distance decreases if the physicians have access to the CDSS, and so does the standard deviation. Without the CDSS, physicians have on average a mean distance of 6 (overestimation of risk in comparison to AI). With the CDSS, the mean distance decreases in all cases, notably strong for junior MDs. Moreover, in the case of junior MD + AI, the mean distance to AI is below zero, which means that predictions are on average slightly below the score of the AI. In case of all MDs and junior MDs, the differences between MD and MD + AI are significant (p < 0.001). In the case of senior MDs we do not observe a significant difference. In addition to this, Figure 3 indicates that the variation of the predictions decreases with CDSS. In all three cases (MD + AI, junior MD + AI and senior MD + AI), more predictions are located closer to the prediction of the AI (located closer to the mean).
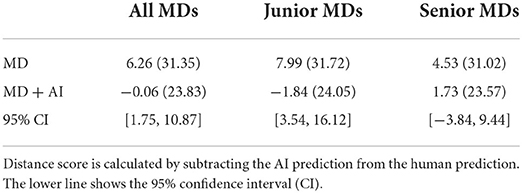
Table 5. Mean distance with standard deviation of estimation made by MD and MD + AI, to the prediction of the AI system.
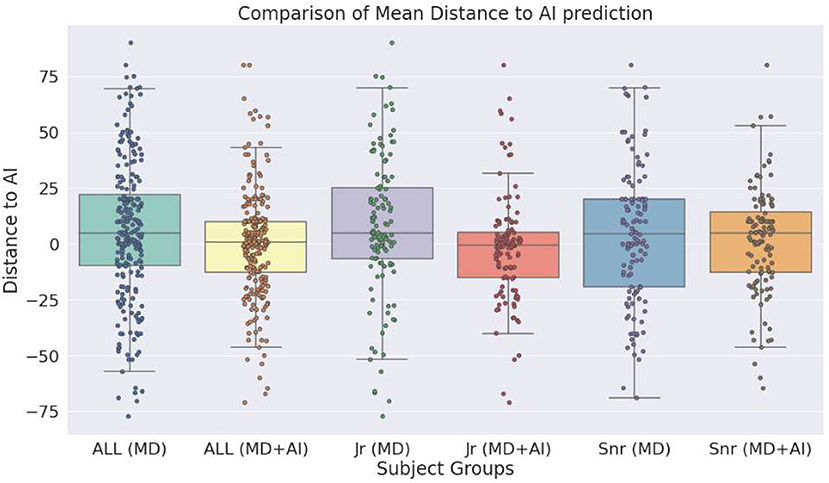
Figure 3. Box plot shows the distance of the estimations of medical doctors as well as medical doctors with clinical decision support system (CDSS), to the estimations of the CDSS alone.
The probability score of the physicians (cutoff = 50%) and the regression risk score (cutoff = F2-score; yellow and red zone in dashboard) were transformed into binary predictions: endpoint occurs, and endpoint does not occur (1/0).
Figure 4 presents the true/false positive predictions of the AI, as well as the physicians with and without CDSS. The figures show that in all cases some true positives (TPs) are not identified either by MD, AI, or MD + AI. Moreover, the figures present a large overlap, particularly for graft failure. Considering only MD and AI, the figure also shows that both make important contributions toward detecting many TPs. Even though AI scores higher in terms of ROC, it is not capable of detecting all critical cases, similar to MDs. Conversely, both together can detect more patients at risk beforehand, in comparison to MD or AI alone. For example, seven Rejections were accurately predicted by both MD and AI, and additionally MD detected five rejections not detected by AI, and AI seven rejections not detected by MD alone.
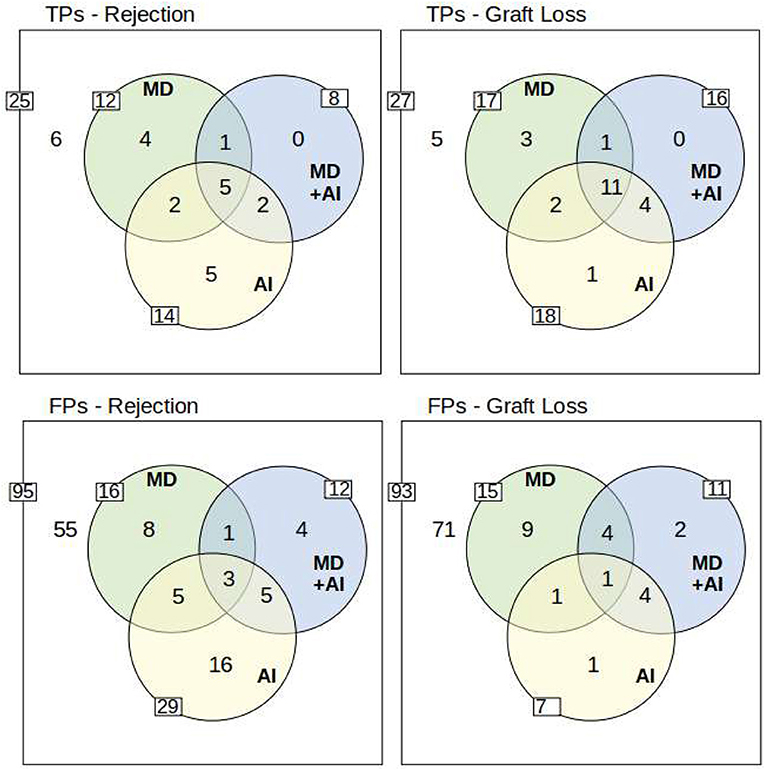
Figure 4. Overview of True Positives (TP) and False Positives (FP). The outer white rim describes the number of positives/negatives for each endpoint. The inner side of each circle indicates the number of true/false positives of AI, MD, and MD + AI. Moreover, the overlapping circles show the overlaps of true/false positive predictions between the different participants. The yellow circle of the AI system represents data points which were flagged with a yellow or red traffic light in the dashboard. To understand the example, take for instance TPs-Rejection: Overall 25 rejections (25 positives of 120 data points) occurred, from which 6 have not been detected by anyone in the study. AI predicted 14 (5 + 2 + 5 + 2) correctly, while MD predicted 12 (4 + 1 + 5 + 2), and MD+AI predicted 8 (1 + 5 + 2) correctly. Five TPs are predicted by all (see intersection of all three circles). Moreover, two TPs are predicted only by MD and AI, and two other TPs only by MD + AI and AI. Only one TP is identified by MD and MD + AI. Finally, 4 TPs are predicted correctly only by MD, and 5 other TPs only by AI. MD + AI does not predict any additional TP which is already found by MD or AI. The lower row presents the same scenario for falsely predicted data points. A more detailed overview including also the results for the red and yellow warning of the traffic light system is included in the Supplementary material.
The results indicate that MD + AI is oriented toward the AI system. Therefore, we can see a larger overlap between those two, and a smaller overlap to MD. AI was able to detect TPs that have not been identified by MD, and a reasonable amount of these is included in MD + AI. Yet, there are some TPs that have only been detected by AI alone. MD + AI did not lead to new TPs that had not been identified beforehand by either AI or MD.
As for false positives (FPs), AI has, except for graft failure, always the highest number of FPs. In case of rejection, AI makes 29 FP predictions, while the MDs makes only 16 and MD + AI only 12 FPs, respectively.
Table 6 shows positive predictive values (PPV) and sensitivity. The table shows that physicians alone can detect 48% of rejections and 63% of graft failures, while the PPV (precision) is 41 and 53%. The combination of both, MD and AI (MD U AI, not MD + AI), leads to an increased sensitivity, with a similar PPV level, in comparison to MD and MD + AI. For graft failure, 80% of the patients at risk can be detected, while only every second prediction is a FP–which is similar to the PPV of MD alone.
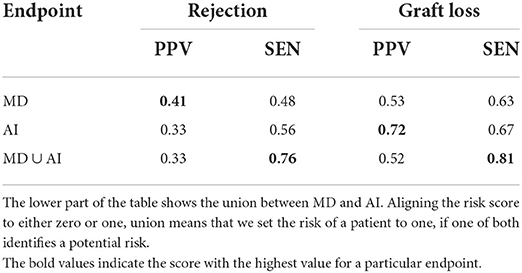
Table 6. Positive predictive value (PPV) and sensitivity (SEN) of MD and AI.
From a medical perspective, we observe that in case of FPs certain risk factors were present, and additionally that some endpoints occurred shortly after the target period of 90 days. Regarding FNs the retrospective second analysis revealed that no obvious known risk factors were present making it difficult to detect the endpoints for medical professionals.
Six endpoints are accurately predicted by AI but neither by MDs alone, nor by MD+AI. These data points are particularly interesting, as preventive measures, such as a closer monitoring could have avoided their occurrence if MDs would trust the CDSS enough to adjust the measures. Although difficult to objectively evaluate, from a medical perspective most of these cases are not obvious at first sight suggesting the potential for AI to detect additional kidney transplant recipients at risk.
Given the complexity of care after kidney transplantation and the diverse amount of potentially harming events, we evaluated a newly developed clinical decision support system (CDSS) for detection of patients at risk for rejection and graft failure in a reader study, in order to analyze assumptions made by physicians with and without the CDSS. First, our results shows that AI achieves better scores compared to physicians on our prediction tasks. Senior MDs perform better than junior MDs, but do not improve with the CDSS. Junior MDs with CDSS instead improve their capability to detect patients at risk. The fact that senior MDs alone perform better than junior MDs alone, might not be surprising. However, the reason why senior physicians have problems with the CDSS contrary to junior physicians remains unclear. One possible explanation is that junior MDs might be more open to new technologies. Also, as senior MDs have much more experience, they might have a stronger confidence in their opinion. This assumption might be supported by the fact that junior MDs converge stronger toward the suggestion of the CDSS. More studies are needed, to fully explore the reasons for these observations.
Another important result is that physicians and AI are able to detect different patients at risk. This highlights the potential benefit of a CDSS and provides strong arguments for its integration into clinical practice. At the same time, more research is needed on the appropriate mode of integration, given that AI resulted in many FPs and its recommendation did not improve senior MDs capabilities. Ultimately, multiple forms of explanations in a CDSS need to be explored and possibly adapted to the experience, the self-confidence and the affinity for technology of the different users.
Even though AI tends to outperform MDs, we need to keep in mind that ROC is just a score, which does not easily translate into a clinical benefit. When regarding sensitivity, specificity, and positive predictive value on the given task, we observe that physicians achieve higher sensitivity at the price of low specificity. One could conclude that MDs are more “cautious” than the AI used in this experiment. However, how can we benefit from such a system? The union of AI and MD could detect more critical patients—possibly by notifying the physician at the end of the treatment in case of a risk. Conversely, too many false alarms might also decrease the trust in such a system and might require too many resources (15). To integrate such a risk prediction model into clinical care, more extensive studies are required. More reliable results might increase the trust in the new technology and lead to a better efficiency.
The main goal of this study was to create a baseline model at a specific transplant center and to compare it to physicians' predictions and study its influence on their decision making. Hence, we are only able to compare our model to others available in terms of metrics and not directly on the same dataset. Recently, the most influential model is the iBox prognostication score, which uses 8 functional, histological, and immunological variables to predict 3, 5, and 7 year allograft survival with a Cox proportional hazards (PH) model, starting at the time of first allograft biopsy (16). It achieves a C-statistic of 0.81 during external validation, while our model shows AUC-ROC of 0.95 for a shorter prediction period of 90 days. While Cox PH is the statistical method of choice when making predictions for right-censored time-to-event data, it needs a clearly defined starting point. Making predictions only at the time of first allograft biopsy is impractical in the context of routine care, where our model is planned to be implemented. Additionally, a very long prediction time of up to 7 years is useful for the purpose of iBox—to serve as a surrogate endpoint in clinical trials, but not to guide everyday clinical decisions. Therefore, we chose to include every assessment of laboratory values as a distinct datapoint and make predictions for a shorter time-period of 90 days. By using this approach, observations are not statistically independent, but it enables the model to learn from more observations per patient and include data from the whole transplant lifespan. Most of the other models to predict allograft survival use comparable methodology and prediction time period as iBox but achieve worse results in terms of AUC-ROC or C-statistic. Only few models report results for a prediction period of 90 or 180 days, mostly achieving AUC-ROC values below 0.8 (17).
Our results are also relevant to a number of ethical issues surrounding AI-driven clinical decision support systems (18). Besides debates on what it takes to trust medical AI and institutions deploying them (19), and who bears moral and/or legal responsibilities for outcomes (20), there are also opportunities: AI could play a part in empowering health systems, health institutions, and clinicians by making capacities widely accessible (21). Our result that less experienced MDs improve their accuracy with the CDSS at hand provides a concrete example for such visions.
Similar to well-established diagnostic tests, or medical guidelines that are part of clinical routine, it might be possible that AI becomes an important part of evidence-based medicine in future. Thus, systems with high predictive power can even be perceived as having epistemic authority in their own right (22): instead of AI being a mere decision aid, burdens of proof in case of deviation from system recommendations might shift to MDs, and individuals and institutions might systematically defer to them. Our results indicate that reality will likely be more fragmented for at least two reasons. First, since our system and MDs have different strengths, system-, user-, and context-specific understanding of these strengths will be essential toward potentially reaping the benefits of a “convergence of human and artificial intelligence” (23) when seeking to optimize health outcomes. Second, the normative significance of various performance metrics is not definite and self-explanatory but requires continuous context-sensitive reflection and weighing involving different stakeholders. Besides, investigating the retrospective question, which factors caused false predictions, the prospective issue of what consequences a false prediction has for the patient will play a role in these discourses. For example, when predicting graft failure or rejection, the harms from FPs differ from those of FNs. Each way of privileging and weighing the metrics discussed reflects slightly different risk-benefit-tradeoffs, and high predictive power along one dimension, while promising and desirable, does not necessarily render the tool a gold standard for the task at hand.
While we use a large fine-grained German database collecting all routine clinical data for more than 20 years this approach has also some limitations. Ideally the model should be externally validated and may be adopted to a different data structure. It is important to highlight that the model should not be seen as an universal “out of the box” model. Instead, it provides a good “baseline” model, which can be improved or may provide the basis for a lean model that is easy to implement in different contexts. However, these issues are beyond the scope of this article, where we focused on the human-machine interaction that can influence future design and implementation of ML-models in kidney transplant care.
The data underlying this article cannot be shared publicly due to privacy/legal reasons. The data will be shared on reasonable request to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics Committee of Charité—University Medicine Berlin (EA4/156/20). Written informed consent for participation was obtained for all participants in the reader study.
RR: planning, technical development, and paper writing. MM: conceptual design, conduction of the study, paper writing, and technical implementation. BO: conduction of the study and paper writing. DS: technical implementation and technical support. KB: conceptual design and paper writing. All authors contributed to discussion and reviewed the paper. All authors contributed to the article and approved the submitted version.
This project was partially funded by the Federal Ministry of Education and Research (BMBF, Germany) in the project vALID: Al-Driven Decision-Making in the Clinic. Ethical, Legal, and Societal Challenges (Grant No. 01GP1903A/C/D), and by the European Union's Horizon 2020 research and innovation program under grant Agreement No. 780495 (BigMedilytics). Any dissemination of results here presented reflects only the author's view. The European Commission is not responsible for any use that may be made of the information it contains. MN was a participant in the BIH Charite Digital Clinician Scientist Program funded by the Charité—Universitätsmedizin Berlin, the Berlin Institute of Health and the German Research Foundation (DFG).
All authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.979448/full#supplementary-material
AI, artificial intelligence; AUC-ROC, area under the curve of the receiver operating characteristic; CI, confidence interval; CDSS, clinical decision support system; DP, data point; ESKD, end-stage kidney disease; FP, false positives; GBRTs, gradient boosted regression trees; KTR, kidney transplant recipients; ML, machine learning; MD, medical doctor; ROC, receiver operating characteristic; TP, true positives.
1. Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. (1999) 341:1725–30. doi: 10.1056/NEJM199912023412303
2. Oniscu GC, Brown H, Forsythe JL. Impact of cadaveric renal transplantation on survival in patients listed for transplantation. J Am Soc Nephrol. (2005) 16:1859–65. doi: 10.1681/ASN.2004121092
3. Mayrdorfer M, Liefeldt L, Wu K, Rudolph B, Zhang Q, Friedersdorff F, et al. Exploring the complexity of death-censored kidney allograft failure. J Am Soc Nephrol. (2021) 32:1513–26. doi: 10.1681/ASN.2020081215
4. Van Loon E, Senev A, Lerut E, Coemans M, Callemeyn J, Van Keer JM, et al. Assessing the complex causes of kidney allograft loss. Transplantation. (2020) 104:2557–66. doi: 10.1097/TP.0000000000003192
5. Sellarés J, De Freitas DG, Mengel M, Reeve J, Einecke G, Sis B, et al. Understanding the causes of kidney transplant failure: the dominant role of antibody-mediated rejection and nonadherence. Am J Transpl. (2012) 12:388–99. doi: 10.1111/j.1600-6143.2011.03840.x
6. Rank N, Pfahringer B, Kempfert J, Stamm C, Kühne T, Schoenrath F, et al. Deep-learning-based real-time prediction of acute kidney injury outperforms human predictive performance. NPJ Digit Med. (2020) 3:139. doi: 10.1038/s41746-020-00346-8
7. Harutyunyan H, Khachatrian H, Kale DC, Galstyan A. Multitask learning and benchmarking with clinical time series data. Sci Data. (2019) 6:96. doi: 10.1038/s41597-019-0103-9
8. Rethmeier N, Serbetci NO, Möller S, Roller R. EffiCare: better prognostic models via resource-efficient health embeddings. AMIA Ann Sympos Proc. (2020) 2020:1060–9. doi: 10.1101/2020.07.21.20157610
9. Kwon BC, Choi MJ, Kim JT, Choi E, Kim YB, Kwon S, et al. Retainvis: Visual analytics with interpretable and interactive recurrent neural networks on electronic medical records. IEEE Trans Vis Comp Graph. (2019) 25:299–309. doi: 10.1109/TVCG.2018.2865027
10. Schmidt D, Osmanodja B, Pfefferkorn M, Graf V, Raschke D, Duettmann W, et al. TBase-an integrated electronic health record and research database for kidney transplant recipients. JoVE. (2021) 170:e61971. doi: 10.3791/61971
11. Haas M, Loupy A, Lefaucheur C, Roufosse C, Glotz D, Seron DA, et al. The banff 2017 kidney meeting report: revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am J Transpl. (2018) 18:293–307. doi: 10.1111/ajt.14625
12. Chawla NV, Bowyer KW, Hall LO, Kegelmeyer WP. SMOTE: synthetic minority over-sampling technique. J Art Intell Res. (2002) 16:321–57. doi: 10.1613/jair.953
13. Goldberger J, Hinton GE, Roweis S, Salakhutdinov RR. Neighbourhood components analysis. Adv Neural Inform Process Syst. (2004). 17:513–20.
14. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. (1988) 44:837–45. doi: 10.2307/2531595
15. Ash JS, Sittig DF, Campbell EM, Guappone KP, Dykstra RH. Some unintended consequences of clinical decision support systems. In: Amia Annual Symposium Proceedings. Chicago, IL: American Medical Informatics Association (2007).
16. Loupy A, Aubert O, Orandi BJ, Naesens M, Bouatou Y, et al. Prediction system for risk of allograft loss in patients receiving kidney transplants: international derivation and validation study. BMJ. (2019) 366:l4923. doi: 10.1136/bmj.l4923
17. Kaboré R, Haller MC, Harambat J, Heinze G, Leffondré K. Risk prediction models for graft failure in kidney transplantation: a systematic review. Nephrol Dial Transpl. (2017) 32:ii68–76. doi: 10.1093/ndt/gfw405
18. Braun M, Hummel P, Beck S, Dabrock P. Primer on an ethics of AI-based decision support systems in the clinic. J Med Ethics. (2020) 47:e3. doi: 10.1136/medethics-2019-105860
19. Braun M, Bleher H, Hummel PJHCR. A leap of faith: is there a formula for “trustworthy” AI? Hast Center Rep. (2021) 51:17–22. doi: 10.1002/hast.1207
20. Price WN, Gerke S, Cohen IG. Potential liability for physicians using artificial intelligence. JAMA. (2019) 322:1765–6. doi: 10.1001/jama.2019.15064
21. Wahl B, Cossy-Gantner A, Germann S, Schwalbe NR. Artificial intelligence (AI) and global health: how can AI contribute to health in resource-poor settings? BMJ Glob Health. (2018) 3:e000798. doi: 10.1136/bmjgh-2018-000798
22. Grote T, Berens P. On the ethics of algorithmic decision-making in healthcare. J Med Ethics. (2019) 46:205–11. doi: 10.1136/medethics-2019-105586
Keywords: kidney transplantation, decision support (DS), graft failure, machine learning, rejection
Citation: Roller R, Mayrdorfer M, Duettmann W, Naik MG, Schmidt D, Halleck F, Hummel P, Burchardt A, Möller S, Dabrock P, Osmanodja B and Budde K (2022) Evaluation of a clinical decision support system for detection of patients at risk after kidney transplantation. Front. Public Health 10:979448. doi: 10.3389/fpubh.2022.979448
Received: 06 July 2022; Accepted: 03 October 2022;
Published: 25 October 2022.
Edited by:
Wenbing Zhao, Cleveland State University, United StatesReviewed by:
Talal Alqaoud, Kuwait Institute for Medical Specialization, KuwaitCopyright © 2022 Roller, Mayrdorfer, Duettmann, Naik, Schmidt, Halleck, Hummel, Burchardt, Möller, Dabrock, Osmanodja and Budde. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roland Roller, cm9sYW5kLnJvbGxlckBkZmtpLmRl
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.