
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Public Health , 16 September 2022
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.979076
 Marianno Franzini1Luigi Valdenassi1Sergio Pandolfi1*
Marianno Franzini1Luigi Valdenassi1Sergio Pandolfi1* Umberto Tirelli2
Umberto Tirelli2 Giovanni Ricevuti3
Giovanni Ricevuti3 Vincenzo Simonetti1Massimiliano Berretta4Francesco Vaiano1
Vincenzo Simonetti1Massimiliano Berretta4Francesco Vaiano1 Salvatore Chirumbolo5*
Salvatore Chirumbolo5*The recent paper by Cenci et al. (1) provided us with an overview of the biological action of medical ozone (O3) on infectious agents, with a particular focus on its anti-viral activity. Ozone is an allotrope of oxygen, a triatomic oxygen molecule that recently showed an ability to counteract the progress of COVID-19 and the development of severe-impact SARS-CoV-2 infection on humans (2, 3). Cenci et al. reported that the way by which ozone targets the SARS-CoV-2 infection involves a hormetic mechanism.
According to Calabrese, hormesis can be considered as a biphasic dose response mechanism characterized by stimulation from a low dose and an inhibition from the highest one (4–6). Hormesis is a paradoxical chemical phenomenon where a chemical toxicant, such as a xenobiotic, or a physical insult, which dose-dependently should inhibit biological functions, at a defined range of low doses behaves in a quite opposite way (6). In this circumstance, any dose-response curve characterized by a hormetic mechanism shows a U-shaped behavior (4–6). This would mean that a noxious chemical compound may have a beneficial or therapeutic activity within a defined range of low doses.
Therefore, hormesis can be used in pharmacological science if the chemical toxicant is dosed in a defined range of concentrations. In this perspective, medical ozone, usually administered in a calibrated oxygen-ozone mixture via autologous blood (30–85 μg/ml, i.e., 0.014–0.040 ppm), acts in a way completely different from the widely known gaseous ozone used for sanitization of indoor environments in different dose ranges (0.3–1.2 ppm) (1). While chemical ozone used for sanitization acts as a toxicant and directly kills microbes, ozone used in medicine (medical ozone) is employed in the hormetic range and triggers a complex network of signaling pathways leading to the activation of a cellular stress response. This response involves mitochondria, i.e., the “mitochondria associated endoplasmic reticulum membranes” or MAM, and regulates the activation of the inflammasome NLRP3, inducing a pro-inflammatory signal, and the ROS-mediated signaling toward the Nrf2-Keap1-ARE system, inducing an antioxidant and pro-survival signal (1, 7).
Cenci et al. (8) report that medical ozone acts via a hormetic mechanism, targeting the complex cellular machinery of the oxidative stress response, and using ozone-derived organic electrophiles, such as 4-hydroxynonenale (4-HNE) or PUFA-derived mediators such as LOPs or even cholesterol-derived oxysterols (1, 9, 10).
However, in Cenci et al., the topic appears to be particularly focused on the ability of ozone to activate a pro-inflammatory status, a consideration that is somehow contradictory with the evidence reporting medical ozone as able to suppress COVID-19 inflammation (1, 11). The role of mitochondria is particularly crucial, and Cenci et al. introduced the concept of “mito-hormesis” (1). Mito-hormesis is a mechanism where mitochondrial ROS (mtROS) and mitochondrial electrophiles (mtRES) behave as TLR-signaling molecules triggering mitochondria to modulate the macrophage's innate immune function in a hormetic way (12). Interestingly, SARS-CoV-2 hijacks and impairs host mitochondrial functions, leading to COVID-19 pathogenesis (13, 14).
The activity of ozone against SARS-CoV-2 is not directly addressed, therefore, but mediated by mtROS and mtRES (i.e., 4-HNE) in a hormetic mechanism. Despite ozone being transiently produced by activated neutrophils (15), and therefore participating in the inflammatory response, medical ozone acts via a hormetic mechanism, using its secondary mediators (LOPs) and accounting for a rigorous protocol of therapeutic dosages (8).
Despite many decades of protocol attempts and experimental science, which might even raise some critical opinion about initial empiricism in using medical ozone, physicians have reached a sound overview of how ozone acts on cell systems, resulting effectively in numerous contexts, such as in the SARS-CoV-2 infection and post-COVID (11, 16), in the migration and proliferation of neural stem cells (17), in multiple sclerosis (18, 19), in musculoskeletal disorders (20), in chronic fatigue syndrome (21), in retina maculopathy (22), and in knee osteoarthritis (23).
Ozone has pleiotropic properties, which are not solely confined to its simplistic anti-oxidant (24, 25) or anti-inflammatory (26) capability, despite ozone's ability to also target pro-inflammatory innate immune cells (27), but to its modulatory ability to use reactive oxygen species (ROS) as signaling molecules, rather than intracellular toxicants. This is a very important point to be emphasized.
A mitochondrial perspective of COVID-19 pathogenesis (28, 29), where the whole mitochondria homeostasis, biogenesis, and turnover, and their involvement in the complex cellular machinery of aging, survival, and metabolism (30) were recently addressed, may further elucidate ozone bioactivity in the SARS-CoV-2 infection (1).
Mito-hormesis accounts for the use of ROS as signaling molecules, which can be achieved by triggering ROS only in their hormetic range of concentrations and in the complex interplay of hypoxic/normoxic stimuli (31). The initial pro-oxidant activity of LOPs induces small amounts of H2O2, which turn into pro-survival (and anti-inflammatory) mechanisms in the cellular response to stressors (32). Therefore, all the successful strategies of medical ozone account for the ability of medical ozone employers in eliciting low doses of ROS by low calibrated doses of ozone itself. Ozone is a subtle regulatory substance, obviously, if used in a standardized and rigorous medical protocol (3, 33).
As ozone dosages, administration strategies, and methods are particularly critical, physicians using ozone therapy must be highly skilled.
The very urgent need for physicians using the oxygen-ozone (O2-O3) mediated therapy, is not only represented by implementing the number and frequency of the many educational and training courses, high scholarly and expert masters, and practical guidelines but enhancing the scientific debate within the few Scientific Committees and Societies dealing with the use of ozone in medicine and therapy (21, 33), even in COVID-19 (2, 11, 34, 35) and in post-COVID or PASC (16).
In Italy, the International Scientific Society of Oxygen Ozone Therapy (SIOOT), for example, leading the research for more than 40 years, is addressing the huge concern to sensitize physicians and caregivers on the correct use of medical ozone for therapy, with the awesome endowment of highly skilled experts, a renowned international experience and the very animated scientific debate within the activity of the same SIOOT members. Table 1 shows the recently published protocol on the use of ozone in COVID-19.
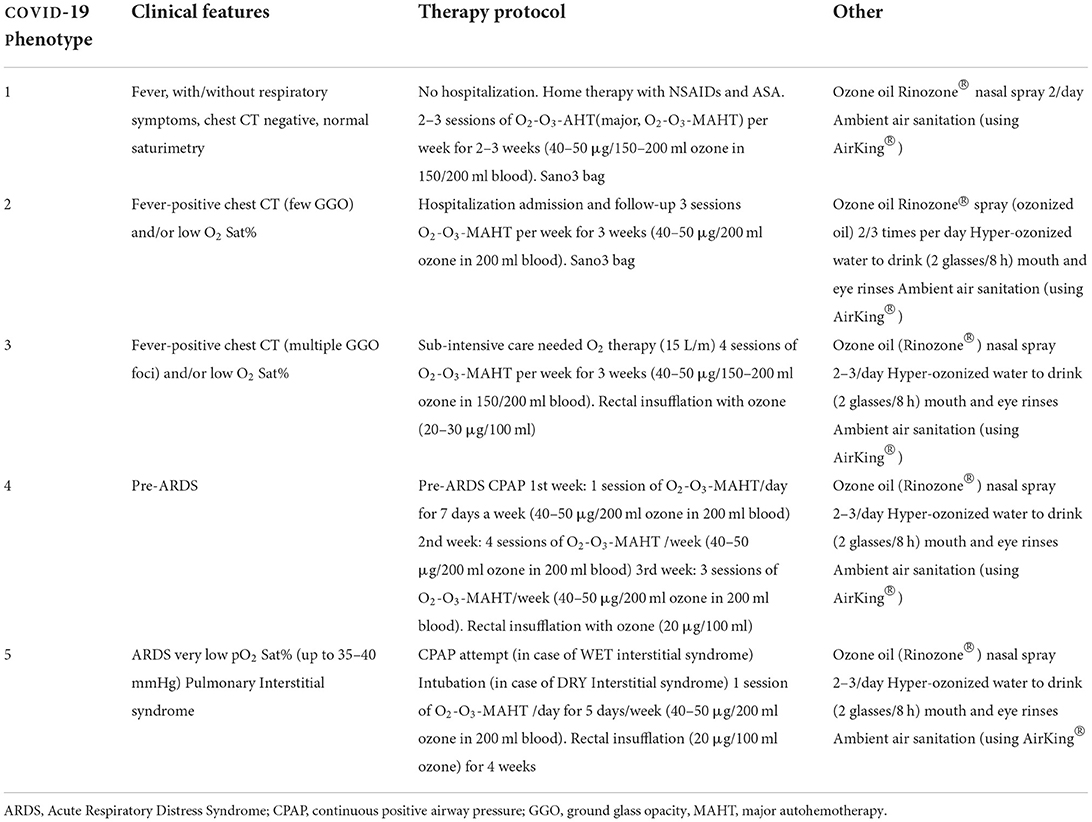
Table 1. SIOOT protocol for the treatment of SARS-CoV-2 infection.
The ability to use the correct medical practice and the best sound and reliable methodology of the therapy approach with ozone needs to be updated continuously with training courses, due to the increase in complex pathologies, such as COVID-19 and post-COVID, the ongoing difficulty in addressing complex multisystemic pathologies by current medicine, and the increase of colleagues using to oxygen-ozone therapy devices and methods, sometimes without full expertise.
As ozone is a toxicant, as reported by the same recent publication from Cenci et al., its handling is particularly burdensome, if not correctly addressed (33). The potentiality of the medical ozone in treating many complex pathologies, of immune, auto-immune, osteoarticular, and neuralgic origin, finds its ability in the fine modulation of the interplay oxidative response/inflammation, held by the mitochondria in the mito-hormetic mechanism (36). This evidence obliges physicians to use oxygen-ozone with the caution recommended by the Scientific Societies built up with this purpose (34).
Finally, from a therapeutic point of view, ozone can be successfully used independently of age and sex distribution, as the hormetic principle is a foundation of the cell survival mechanism, and therefore is perfectly working in any living situation, with particular emphasis during those processes leading to inflammation. Sensitivity to ozone is not dependent on the individual BMI, sex, race, or age. The range within which ozone is used is arranged depending on the pathology or ailment to be treated by the oxygen-ozone therapy.
Ozone therapy is a great opportunity for medical science and its use is spreading widely therefore needs further scientific insights to be made.
MF: supervision, validation, and paper administration. LV: supervision and validation. SP: supervision, revision in conceptualization, and validation. UT, MB, and FV: validation. GR and VS: validation and references. SC: conceptualization, writing draft, revision, supervision, and submission. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cenci A, Macchia I, La Sorsa V, Sbarigia C, Di Donna V, Pietraforte D, et al. Mechanisms of action of ozone therapy in emerging viral diseases: immunomodulatory effects and therapeutic advantages with reference to SARS-CoV-2. Front Microbiol. (2022) 13:1–20. doi: 10.3389/fmicb.2022.871645
2. Yousefi B, Banihashemian SZ, Feyzabadi ZK, Hasanpour S, Kokhaei P, Abdolshahi A, et al. Potential therapeutic effect of oxygen-ozone in controlling of COVID-19 disease. Med Gas Res. (2022) 12:33–40.
3. Chirumbolo S, Valdenassi L, Simonetti V, Bertossi D, Ricevuti G, Franzini M, et al. Insights on the mechanisms of action of ozone in the medical therapy against COVID-19. Int Immunopharmacol. (2021) 96:107777. doi: 10.1016/j.intimp.2021.107777
4. Agathokleous E, Calabrese EJ. Hormesis: a general biological principle. Chem Res Toxicol. (2022) 35:547–9. doi: 10.1021/acs.chemrestox.2c00032
5. Calabrese EJ. Hormesis: a fundamental concept in biology. Microb Cell. (2014) 1:145–9. doi: 10.15698/mic2014.05.145
6. Calabrese EJ. Hormesis: path and progression to significance. Int J Mol Sci. (2018) 19:2871. doi: 10.3390/ijms19102871
7. Degechisa ST, Dabi YT, Gizaw ST. The mitochondrial associated endoplasmic reticulum membranes: a platform for the pathogenesis of inflammation-mediated metabolic diseases. Immun Inflamm Dis. (2022) 10:e647. doi: 10.1002/iid3.647
8. Bocci VA, Zanardi I, Travagli V. Ozone acting on human blood yields a hormetic dose-response relationship. J Transl Med. (2011) 9:66. doi: 10.1186/1479-5876-9-66
9. Bocci V. Ozone as Janus: this controversial gas can be either toxic or medically useful. Mediators Inflamm. (2004) 13:3–11. doi: 10.1080/0962935062000197083
10. Bocci V. Is it true that ozone is always toxic? The end of a dogma. Toxicol Appl Pharmacol. (2006) 216:493–504. doi: 10.1016/j.taap.2006.06.009
11. Franzini M, Valdenassi L, Ricevuti G, Chirumbolo S, Depfenhart M, Bertossi D, et al. Oxygen-ozone (O2-O3) immunoceutical therapy for patients with COVID-19. Preliminary evidence reported. Int Immunopharmacol. (2020) 88:106879. doi: 10.1016/j.intimp.2020.106879
12. Timblin GA, Tharp KM, Ford B, Winchester JM, Wang J, Zhu S, et al. Mitohormesis reprogrammes macrophage metabolism to enforce tolerance. Nat Metab. (2021) 3:618–35. doi: 10.1038/s42255-021-00392-w
13. Ajaz S, McPhail MJ, Singh KK, Mujib S, Trovato FM, Napoli S, et al. Mitochondrial metabolic manipulation by SARS-CoV-2 in peripheral blood mononuclear cells of patients with COVID-19. Am J Physiol Cell Physiol. (2021) 320:C57–65. doi: 10.1152/ajpcell.00426.2020
14. Singh KK, Chaubey G, Chen JY, Suravajhala P. Decoding SARS-CoV-2 hijacking of host mitochondria in COVID-19 pathogenesis. Am J Physiol Cell Physiol;319. (2020) C258–67. doi: 10.1152/ajpcell.00224.2020
15. Wentworth P Jr, McDunn JE, Wentworth AD, Takeuchi C, Nieva J, Jones T, et al. Evidence for antibody-catalyzed ozone formation in bacterial killing and inflammation. Science. (2002) 298:2195–9. doi: 10.1126/science.1077642
16. Tirelli U, Franzini M, Valdenassi L, Pisconti S, Taibi R, Torrisi C, et al. Fatigue in post-acute sequelae of SARS-CoV-2 (PASC) treated with oxygen-ozone autohemotherapy - preliminary results on 100 patients. Eur Rev Med Pharmacol Sci. (2021) 25:5871–5.
17. Tricarico G, Isakovic J, Song MS, Rustichelli F, Travagli V, Mitrecic D, et al. Ozone influences migration and proliferation of neural stem cells in vitro. Neurosci Lett. (2020) 739:135390. doi: 10.1016/j.neulet.2020.135390
18. Molinari F, Simonetti V, Franzini M, Pandolfi S, Vaiano F, Valdenassi L, et al. Ozone autohemotherapy induces long-term cerebral metabolic changes in multiple sclerosis patients. Int J Immunopathol Pharmacol. (2014) 27:379–89. doi: 10.1177/039463201402700308
19. Molinari F, Rimini D, Liboni W, Acharya UR, Franzini M, Pandolfi S, et al. Cerebrovascular pattern improved by ozone autohemotherapy: an entropy-based study on multiple sclerosis patients. Med Biol Eng Comput. (2017) 55:1163–75. doi: 10.1007/s11517-016-1580-z
20. Akkawi ME, Mohd Taufek NH, Abdul Hadi AD, Nik Lah NNNF. The prevalence of prescribing medications associated with geriatric syndromes among discharged elderly patients. J Pharm Bioallied Sci. (2020) 12:S747–S751.
21. Tirelli U, Franzini M, Valdenassi L, Pandolfi S, Berretta M, Ricevuti G, et al. Patients with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) greatly improved fatigue symptoms when treated with oxygen-ozone autohemotherapy. J Clin Med. (2021) 11:29. doi: 10.3390/jcm11010029
22. Borrelli E, Diadori A, Zalaffi A, Bocci V. Effects of major ozonated autohemotherapy in the treatment of dry age related macular degeneration: a randomized controlled clinical study. Int J Ophthalmol. (2012) 5:708–13.
23. Lopes de Jesus, Dos Santos CC, de Jesus, FC, Monteiro LM, Sant'Ana I, Trevisani VFM. Comparison between intra-articular ozone and placebo in the treatment of knee osteoarthritis: a randomized, double-blinded, placebo-controlled study. PLoS ONE. (2017) 12:e0179185. doi: 10.1371/journal.pone.0179185
24. Nasezadeh P, Shahi F, Fridoni M, Seydi E, Izadi M, Salimi A, et al. Moderate O3/O2 therapy enhances enzymatic and non-enzymatic antioxidant in brain and cochlear that protects noise-induced hearing loss. Free Radic Res. (2017) 51:828–37. doi: 10.1080/10715762.2017.1381695
25. Galiè M, Covi V, Tabaracci G, Malatesta M. The role of Nrf2 in the antioxidant cellular response to medical ozone exposure. Int J Mol Sci. (2019) 20:4009. doi: 10.3390/ijms20164009
26. Simonetti V, Franzini M, Iaffaioli RV, Pandolfi S, Valdenassi L, Quagliariello V, et al. Anti-inflammatory effect of ozone in human melanoma cells and its modulation of tumor microenvironment. Int J Adv Res. (2018) 6:1196–203.
27. Karatieieva S, Muzyka N, Semenenko S, Bakun O, Kozlovskaya I. Ultrastructural changes of wound macrophages under the influence of intravenous ozone therapy in patients with diabetes and inflammatory processes of soft tissues. Georgian Med News. (2018) (276):98–101. doi: 10.21474/IJAR01/7476
28. Saleh J, Peyssonnaux C, Singh KK, Edeas M. Mitochondria and microbiota dysfunction in COVID-19 pathogenesis. Mitochondrion. (2020) 54:1–7. doi: 10.1016/j.mito.2020.06.008
29. Prasun P. COVID-19: A Mitochondrial Perspective. DNA Cell Biol. (2021) 40:713–9. doi: 10.1089/dna.2020.6453
30. Shenoy S. Coronavirus (Covid-19) sepsis: revisiting mitochondrial dysfunction in pathogenesis, aging, inflammation, and mortality. Inflamm Res. (2020) 69:1077–85. doi: 10.1007/s00011-020-01389-z
31. Eaton L, Pamenter ME. What to do with low O2: Redox adaptations in vertebrates native to hypoxic environments. Comp Biochem Physiol A Mol Integr Physiol Jun. (2022) 17:111259. doi: 10.1016/j.cbpa.2022.111259
32. Gebicki J, Wieczorkowska M. COVID-19 infection: mitohormetic concept of immune response. Cell Death Discov. (2020) 6:60. doi: 10.1038/s41420-020-00297-9
33. Chirumbolo S, Simonetti V, Valdenassi L, Pandolfi S, Vaiano F, Franzini M, et al. Editorial - A practical assessment to prevent serious complications in the use of a gaseous mixture of oxygen-ozone injected by needle-mediated infiltration. Eur Rev Med Pharmacol Sci. (2022) 26:2224–6.
34. Izadi M, Cegolon L, Javanbakht M, Sarafzadeh A, Abolghasemi H, Alishiri G, et al. Ozone therapy for the treatment of COVID-19 pneumonia: a scoping review. Int Immunopharmacol. (2021) 92:107307. doi: 10.1016/j.intimp.2020.107307
35. Varesi A, Chirumbolo S, Ricevuti G. Oxygen-ozone treatment and COVID-19: antioxidants targeting endothelia lead the scenery. Intern Emerg Med. (2022) 17:593–6. doi: 10.1007/s11739-021-02865-y
Keywords: ozone, SARS-CoV-2, hormesis at cell level, hormesis effect, anti-oxidant
Citation: Franzini M, Valdenassi L, Pandolfi S, Tirelli U, Ricevuti G, Simonetti V, Berretta M, Vaiano F and Chirumbolo S (2022) The biological activity of medical ozone in the hormetic range and the role of full expertise professionals. Front. Public Health 10:979076. doi: 10.3389/fpubh.2022.979076
Received: 28 June 2022; Accepted: 19 August 2022;
Published: 16 September 2022.
Edited by:
Zhimin Tao, Jiangsu University, ChinaCopyright © 2022 Franzini, Valdenassi, Pandolfi, Tirelli, Ricevuti, Simonetti, Berretta, Vaiano and Chirumbolo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sergio Pandolfi, c2VyZ2lvcGFuZG9sZmlzMkBnbWFpbC5jb20=; Salvatore Chirumbolo, c2FsdmF0b3JlLmNoaXJ1bWJvbG9AdW5pdnIuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.