 Huixiang Zhong
Huixiang Zhong Jin Yang
Jin Yang Na Zhao1
Na Zhao1- 1National Institute of Hospital Administration, National Health Commission of the People's Republic of China, Beijing, China
- 2Department of Medical Record Management Statistics, Affliated Huadu Hospital, Southern Medical University, Guangzhou, Guangdong, China
- 3Department of Endocrinology and Metabolism, Peking University Third Hospital, Peking University, Beijing, China
- 4Outpatient Department, Yantai Affliated Hospital of Binzhou Medical University, Yantai, Shandong, China
Background: Post-retirement migrants are rapidly increasing in China, but the impact of internal migration on hospitalization among older adults remains under-researched. Understanding this impact is essential for health policies development and improvement. This study aims to identify the most vulnerable population, evaluate the association between migration and hospitalization, and discuss potential causes of the association.
Methods: 14,478 older adults were extracted from the 2018 to 2019 Chinese Longitudinal Healthy Longevity Survey (CLHLS) database and divided into four groups according to migration experience and age at migration: non-migrants, pre-adulthood migrants, pre-retirement migrants, and post-retirement migrants. Post-retirement migrants were key research subjects. We employed Pearson's chi-square test to compare group differences in outcome and covariates, and multivariate logistic regression analysis to examine the association between migration and hospitalization by regions and chronic conditions.
Results: Significant intergroup differences were observed in demographic characteristics, socioeconomic factors, health habits, and health-related factors. Post-retirement migrants displayed following characteristics: female predominance (61.6%; 1,472/2,391), tending toward urban areas (80.9%; 1,935/2,391), and the highest prevalence rate of chronic disease (46.7%; 1,116/2,391). Urban migrants in eastern China were more likely to be hospitalized (OR = 1.65; 95% CI: 1.27–2.15), especially those who were diagnosed with chronic disease (OR = 1.51; 95% CI: 1.04–2.19) or with unconfirmed chronic conditions (OR = 1.98; 95% CI: 1.36–2.89).
Conclusions: Internal migration is associated with the hospitalization of post-retirement migrants moving to eastern China. Improved chronic disease management and early interventions might lower the hospitalization. Effective policies should be formulated to reduce the disparity in primary care services across China, thereby facilitating the access of migrants to these services.
Introduction
Internal migration, the movement within countries, has become a common occurrence in China. Motivated by caring for the younger generation, elderly care or reunion with family and jobs (1), older adults out of the migrant population have been increasing. According to the report on China's migrant population development 2015 issued by the National Health Commission of the People's Republic of China (2), the older migrants had accounted for 5.3 percent (13,040,000/247,000,000) of the total migrants. Given the older migrants' annual growth rate (6.6 percent) and the extended life expectancy since 2016 (3, 4), older migrants are expected to rise steadily in China.
Older adults' redistribution in space necessitates the redistribution of health resource (5). Since primary care and health insurance in China are intimately tied to the household registration system (6, 7), migration unavoidably decreases the migrants' access to health services (8, 9). Thus far the declining access has been demonstrated in many aspects except inpatient services. However, hospitalization provides both vital evidence for the effectiveness of primary care services and reliable indication of the impact of migration on migrants' health (10, 11). As such, clarifying the association between migration and hospitalization is critical for identifying at-risk groups, and then enabling policy makers to develop or improve subsequent healthcare policy.
Elderly population over 65 years old in China has reached 191 million in 2020 (12), three-quarters of whom has at least one chronic disease (13). Aiming to provide the same basic public health services (BPHS) to all citizens, the Chinese government has been implementing BPHS equalization program from 2009 onwards (14). By BPHS, every Chinese older adult should have had access to free health management services, and chronic disease health management for those who suffer from hypertension and diabetes mellitus. Nonetheless, older migrants' utilization of BPHS has been found insufficient (15–17). Considerable migrants receive deficient chronic disease management (18). In addition, previous research has discovered a strong substitution element between outpatient services and inpatient services (19). Owing to the non-portability of health insurance (20), Chinese migrants are unable to meet the expenses at the location where they receive outpatient services, thereby reducing outpatient visits and preferring treatment delay (21, 22). Inadequate access to care has been linked to physical disability, cognitive impairment, and an increased risk of mortality (23).
In light of the above, it is reasonable to conjecture that older migrants would use more inpatient services in the context of the limited effectiveness of primary care and the reduction in outpatient care. As yet this assumption has not been confirmed in China, and to some extent this will be tested in this study.
China exhibits an uneven distribution of medical resources and a wide variation in medical standards between urban and rural areas, as well as across provinces (24, 25). In this regard, the association between migration and hospitalization is presumed to be significant in certain areas. To identify these areas will allow for more targeted interventions.
This study describes the characteristics of post-retirement migrants and evaluates the association between migration and hospitalization by comparing them with non-migrants. Considering the regional heterogeneity of migrants, the association would be evaluated stratified by urban-rural distribution and geographical region, and then further stratified by chronic disease so as to study the effectiveness of health management for migrants with chronic conditions.
Materials and methods
Data source and participants
Data were extracted from the Eighth Chinese Longitudinal Healthy Longevity Survey (CLHLS) conducted between 2018 and 2019, which extended its scope of the investigation into 23 mainland provinces to represent approximately 85% of the Chinese elderly population (≥65 years) (26). The CLHLS adopted several measures to provide comparative, accurate, and representative information, including the development of internationally accepted questionnaires, face-to-face interviews, and double data entry (27). All CLHLS data are available at Peking University Open Research Data Platform.
A total of 15,874 individuals aged 65 years or older, having lived in their current address for at least 2 years, were selected from the 2018 CLHLS database (Figure 1). Individuals with missing outcome were excluded. For some variables with missing data, we performed multiple imputation instead of deleting (28). A total of 14,478 participants were included in the analysis.
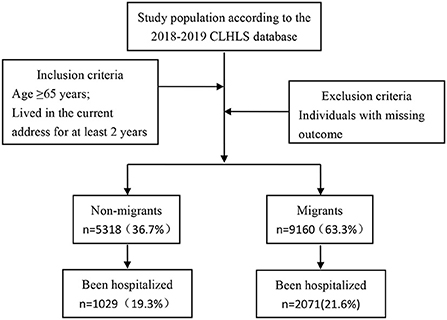
Figure 1. Flowchart of sample selection based on 2018–2019 CLHLS data.
Migration
Internal migration could be defined by the respondents' age and the following questions: (1) “How many years did you live in the current address?” and (2) “Do you currently live in the city you were born?”. Migrants were defined as the respondents who answered “more than 2 years” to the first question and “no” to the second question; and non-migrants were defined as the respondents who answered the years same as age to the first question and “yes” to the second question. For the convenience of expression, internal migration is denoted as migration in the following paragraphs.
Age at migration was the core explanatory variables.
As several research have highlighted the importance of seeing migration within a life course context with certain life course events such as employment or retirement (29), we divided age at migration into three categories: pre-adulthood (1–17 years), pre-retirement (18–59 years for male, 18–54 years for female), and post-retirement (60 years and above for male, 55 years and above for female). The post-retirement migrants would be focused on in this study. By directly comparing with non-migrants and indirectly comparing with pre-adulthood and pre-retirement migrants, more characteristics of post-retirement migrants which associate with hospitalization are expected to be discovered.
Migrants whose destination located in urban areas were referred to as urban migrants, while others were rural migrants.
Outcome variable
The outcome variable was hospitalization. A questionnaire was applied to determine the number of patients hospitalized in the past 2 years using a dichotomous response, in which “yes” corresponded to “hospitalized at least once” and “no” corresponded to “not hospitalized.”
Covariates
As shown in Table 1, Demographic variables included gender (male, female), age (65–79, 80–94, ≥95 years), education attainment (never educated, primary school, middle school, college and above), residential area (urban, rural), and geographical region (north, northeast, east, central-south, and west). The classification of geographical region was based on CLHLS guidelines. The study cohort lived in the following cities: Tianjin, Hebei, Shanxi, and Beijing (north), Liaoning, Jilin, and Heilongjiang (northeast), Jiangsu, Zhejiang, Anhui, Fujian, Jiangxi, and Shanghai (east), Hainan, Henan, Hunan, Hubei, Guangdong, and Guangxi (central-south), Sichuan, Shanxi, and Chongqing (west).
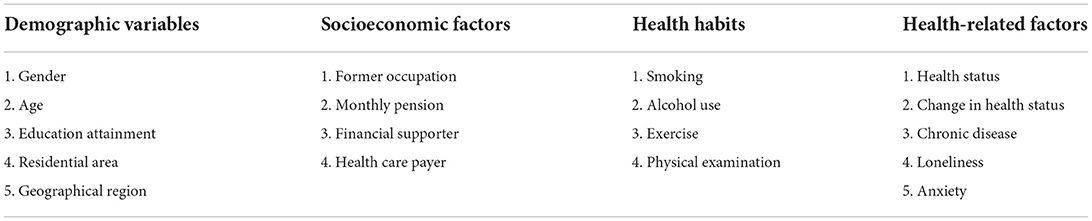
Table 1. Profile of the study cohort according to covariates.
Socioeconomic variables included former occupation (agriculture, professional and managerial, others), monthly pension (including retirement and insurance pension, measured in RMB; 0, 0–2,000, >2,000), financial supporter (owner, family, others), and health care payer (insurance company, household member, or others). Former occupation came from the question “what is your occupation before the age of 60 years?”. For ease of comparison, several options were combined, and agriculture, forestry, animal husbandry, and fishery workers were included in the “agriculture” category, professional and technical personnel and governmental, institutional, and managerial personnel were included in the “professional and managerial” category, whereas other occupations were assigned to the “others” category. Similar combination occurred in the topic “health care payer,” and “owner” remains “owner,” “urban employee/resident medical insurance,” “cooperative” and “private” were aggregated into “insurance,” “spouse” and “children” were aggregated into “household members,” and other payers were aggregated into “others.”
Health habits were smoking (yes, no), alcohol use (yes, no), exercise (yes, no), and physical examination (yes, no).
Health-related factors were health status (good, average, bad), change in health status (better, no change, worse), chronic disease (yes, unconfirmed, no), loneliness (yes, no) and anxiety (yes, no). Both health status and change in health status were self-reported, and derived from the questions “how do you rate your health at present?” and “how do you rate your health at present compared with one year ago?”, respectively.
Statistical analysis
Group differences in outcome and covariates were compared using the Pearson's chi-square test. The association between age at migration, covariates and hospitalization was assessed by univariate logistic regression analysis before constructing multivariate regression models. Multivariate binary logistic regression analysis with LR forward-stepwise method, of which put in criteria is p < 0.05 and removed in p > 0.10, were performed to determine the variables significantly associated with hospitalization. The LR forward-stepwise method guarantees the absence of multicollinearity between variables entering the models. The reliability of the multivariate regression model was analyzed using the Hosmer and Lemeshow goodness-of-fit test (30), and the goodness-of-fit was considered acceptable if the value of the chi-square statistic was low accompanied by p > 0.05 in this test. Statistical significance in this study was defined at a p-value which <0.05. Statistical analysis was conducted using SPSS version 25.0 (IBM, SPSS Inc, Chicago, IL, USA).
Results
Descriptive statistics
Sample characteristics
Table 2 summarizes sample characteristics by age at migration. 25.6% of the post-retirement migrants had been hospitalized within 2 years, and the proportion was significantly higher than other subgroups.
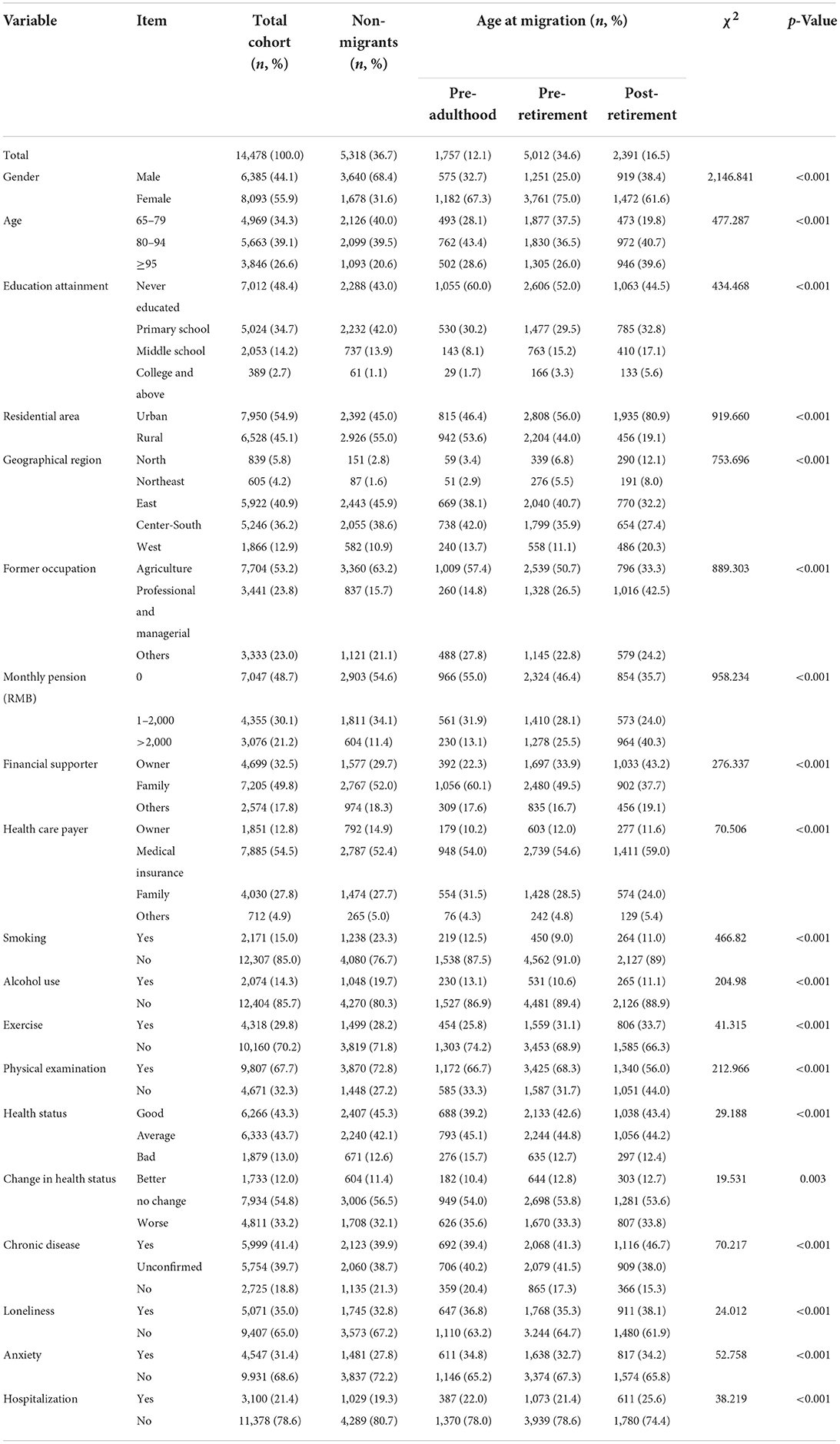
Table 2. Profile of the study cohort.
A total of 55.9% of the respondents were females, and the male-to-female ratios of migrants and that of non-migrants were completely contrary. 2,391 older adults migrated to their current residence after retirement, accounting for 16.5% of total participants, and 80.9% (1,351/2,391) of them migrated across urban areas; in contrast, migration before adulthood or retirement were more likely to happen in rural areas, 52.4% (920/1,750) and 42.9% (2,150/5,012), respectively. Migrants who migrated after retirement showed two characteristics compared with other subsets, the lowest illiteracy rate (44.5%; 1,063/2,391) and the most dispersed geographical distribution.
With regard to socioeconomic status, agricultural practitioners dominated a prime position, except for those who migrated after retirement. 48.7% of the respondents did not receive pensions; accordingly, 49.7% relied on family for living expenses. 54.5% had health insurance paid by the insurance company. An upward trend in socioeconomic status was clear as the age of migration increased.
Comparing health habits revealed that those who migrated later were more likely to develop positive health habits.
43.7% of the participants reported a good health status while 13.0% reported bad, 33.2% deemed their health status worsened, and 63.3% were diagnosed with chronic disease. Loneliness and anxiety were more commonly reported by post-retirement migrants. It's noteworthy that the highest health satisfaction degree (43.4%; 1,038/2,391), prevalence rate of chronic disease (46.7%; 1,116/2,391) occurred simultaneously in the post-retirement migration group.
There were significant intergroup differences in migration-related variables, demographic variables, socioeconomic factors, health habits, health-related factors and outcome variable.
Regression analyses
Effect of age at migration and covariates on hospitalization
From Table 3, it could be found that age at migration and all the covariates were positively associated with hospitalization. The effect of age at migration on hospitalization slightly decreased when adjusting for all the covariates [Model 1; Hosmer and Lemeshow goodness-of-fit χ2 (8df) =5.813, p = 0.668], still, older adults who migrated after retirement remained the most likely to be hospitalized. As the positive association occurred in urban area [Model 2; Hosmer and Lemeshow goodness-of-fit χ2 (8df) =4.655, p = 0.794] rather than in rural area [Model 3; Hosmer and Lemeshow goodness-of-fit χ2 (8df) =5.270, p = 0.728], participants settled in rural area would be excluded in the following hierarchical analyses.
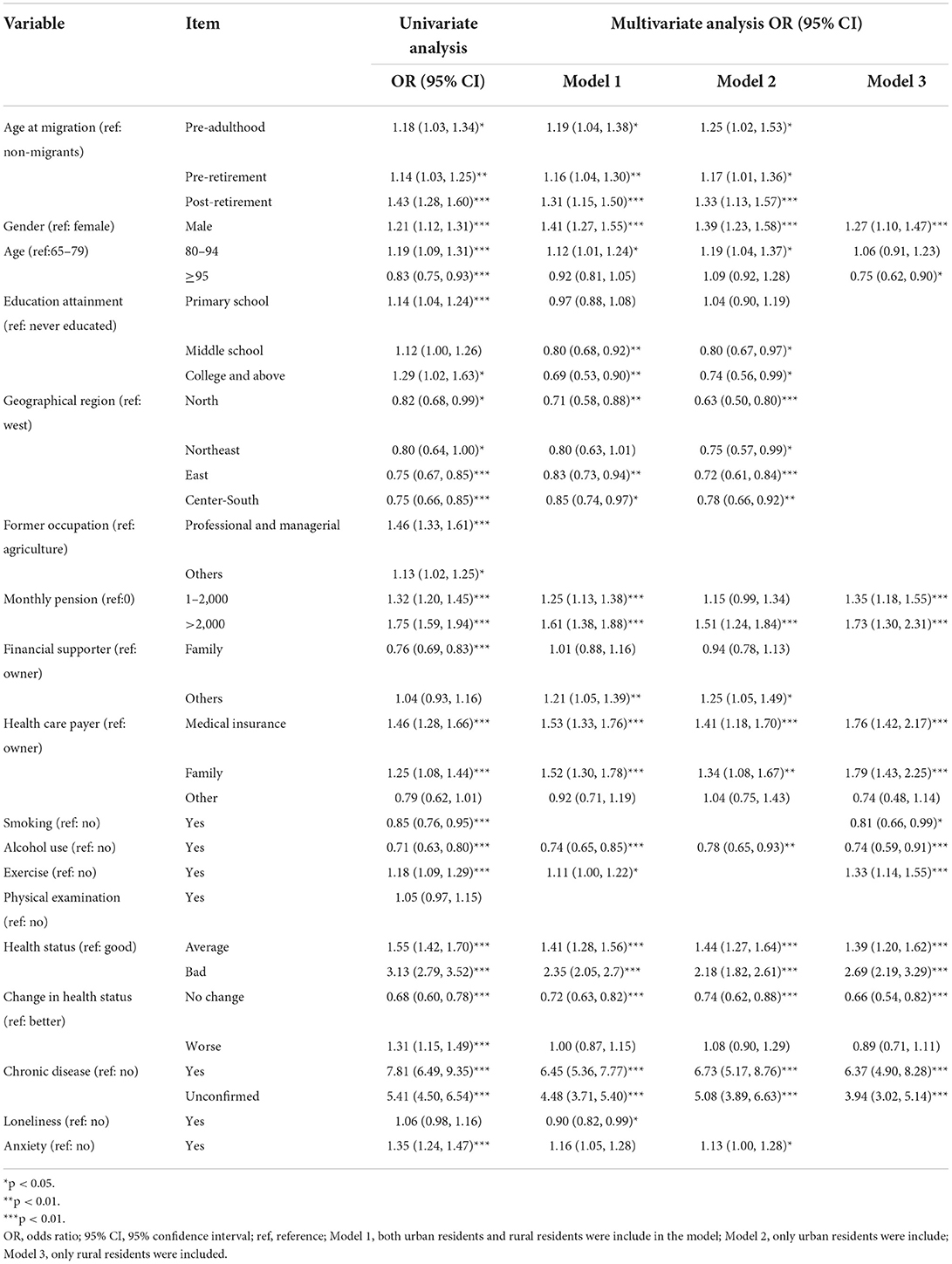
Table 3. Results of logistic regressions on hospitalization in the study cohort.
In terms of the risk factors of hospitalization, there were obvious urban-rural disparities, as only half of the covariates (gender, age, monthly pension, health care payer, smoking, alcohol use, health status, change in health status, and chronic disease) appeared both in Model 2 and Model 3. Among these common risk factors, chronic disease presented the most noticeable effect.
Risk factors of hospitalization by geographical region among urban migrants
With a view to regional economic and health disparities, multivariate logistic regression models with urban residents included were constructed for each geographical region in China. The results in Table 4 show that migration significantly increased the risk of post-retirement migrants' hospitalization in the eastern region only (OR = 1.65; 95% CI: 1.27–2.15).

Table 4. Risk factors of hospitalization by geographical region among urban migrants in China.
Impacts of age at migration on hospitalization by chronic disease among urban migrants in Eastern China
For determining whether the risk of hospitalization among eastern China's migrants was associated with chronic conditions, we grouped the urban residents based on their chronic conditions and constructed separate multivariate logistic regression models. As presented in Table 5, after controlling for gender, age, financial supporter, health status, and change in health status, we found that age at migration had no impact on hospitalization by comparing migrants without chronic disease with native counterparts. With respect to migrants diagnosed with chronic disease, pre-adulthood migration and pre-retirement migration were found irrelevant to hospitalization, whereas post-retirement migrants were at a higher risk of hospitalization (OR = 1.51; 95% CI: 1.04–2.19). Notably, the highest OR (1.98; 95% CI: 1.36–2.89) in the study reveals the population group most susceptible to hospitalization, the post-retirement urban migrants with unconfirmed chronic conditions living in eastern China. The above results have strongly suggested that the migrants with chronic conditions might receive inadequate health management.
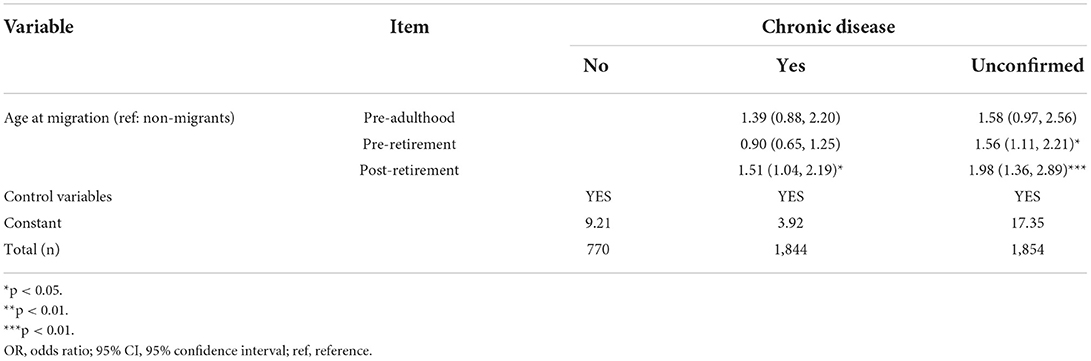
Table 5. OR and 95% CI by chronic disease among urban migrants in eastern China.
Discussion
This study investigated the distribution of older migrants across China and the association between migration and hospitalization whereby the population most at-risk could be identified. The large sample size increased the reliability of the results. Moreover, the definite chronological order that migration occurred before hospitalization in this study has provided an irreplaceable condition for determining causality further.
Characteristics of post-retirement migrants
Post-retirement migrants, whether from urban areas or rural areas, were more likely to settle in urban areas. On one hand, the convenient traffic conditions and advanced medical care services in urban areas hold irresistible attraction for older adults in pursuit of better living quality (1). On the other hand, the urbanization process in China has been expanding dramatically, and the urbanization rate was lifted to 63.89% according to the Seventh National Population Census of the People's Republic of China (12).
Females comprised a dominant proportion of migrants. In China, in case of children's migration and resettlement, older women tend to migrate in virtue of strong family ties and a strong sense of responsibility for caring for grandchildren (31).
It seems to be contradictory that post-retirement migrants who reported the highest prevalence rate of chronic disease also declared the best health status. Notwithstanding, the perception of health status varies with each individual and is outside of objective evaluation criteria. The defect of self-assessed health status would be the prime cause of the discrepancy.
Association between migration and hospitalization
Despite the confounding effect caused by covariates, the risk of hospitalization among all migrants was higher than that among the native population, suggesting the activity of migration did associate with hospitalization.
Prior research has found that early experiences related to migration may have consequences for late-life disease, and the relation is not mitigated by the higher socioeconomic status achieved by early migrants (32). Partially corresponding with this discovery, the risk of being hospitalized among total pre-adulthood migrants ranked higher than that among pre-retirement migrants. Nevertheless, pre-adulthood and pre-retirement migrants with chronic diseases showed insignificant trend toward hospitalization. These two groups of older migrants generally attain indigenous health insurance as natives, hence the better health management in contrast to post-retirement migrants.
Post-retirement migrants who migrated to eastern China was more likely to be hospitalized. Furthermore, the older migrants in unconfirmed chronic conditions displayed the maximum possibility of hospitalization. Given this, improving chronic disease management for post-retirement migrants in eastern China would help to yield a lower hospitalization rate.
These findings shed light on the high rate of hospitalization among older migrants in China. Post-retirement migrants were in need of effective chronic disease management, and a health surveillance system applied to them would be conducive to health promotion and medical resource saving (20).
Potential reasons for the association and policy implication
The adaptation process regarding daily life, social relationships, and obtaining social support is difficult for older urban migrants (33), who are liable to fall into a state of social isolation and loneliness (34, 35). Migrating in later life is therefore associated with mental health problems, such as depression, anxiety and stress symptoms (32, 36–40). The high association between migration and mental illness may explain why mental illness was excluded in multivariate analyses, as two highly associated variables do not simultaneously exist in regression models. However, previous studies has proved that mental illness indirectly links to physical health impairment and accelerating progression of pre-existing diseases (41), and then cause hospitalization. The mental illness among migrants should be a concern. In order to eliminate social inequalities in mental health outcomes among migrants, more public policies related to mental health services should be established, and community intervention should be prioritized (42).
Patient migration is becoming globally common (43). The eastern region is the most economically developed area in China, and possesses more high-quality medical resources than other regions (24, 44). As a result, patients who could not be diagnosed or cured migrated to eastern China to seek for appropriate treatment. Additionally, eastern China has paced the whole country in providing settlement services for non-local inpatients, hence greatly facilitating hospitalization procedures for migrants. This progress particularly occurs in the Yangtze River Delta region. The combination of regional advantages partly explains why post-retirement migrants in eastern China more inclined to be admitted to hospitals.
However, economic development and improvement of health resources rarely improve access to primary services for Chinese older migrants (15). Migration has significantly reduced migrants' probabilities of hypertension awareness and receiving physician advice (45). The lack of primary care would undoubtedly accelerate the process of health deterioration, consequently leading to hospitalization. The founding that the post-retirement migrants with chronic diseases used more inpatient services is a powerful indicator of potentially insufficient health management, which suggests an efficient system is needed to ensure equal primary care in China.
In view of the above, the authorities in eastern China should develop measures as quickly as possible to guarantee adequate primary health services for migrants. Professional medical examination should be promptly provided to older migrants with unconfirmed chronic conditions. The diagnosed patients should be included in the local system of health management. Moreover, the local-migrant gaps in primary care and outpatient services utilization are normally attributable to the place of insurance participation as well as the categories of health insurance (46). It is essential to perfect the instrument of settlement services for non-local medical treatment and to promote the transfer of migrants' social medical insurance across different regions.
Limitations
This study has some limitations. First, limited by the content of the questionnaire based on CLHLS, we were able to distinguish the migrants but unable to assess the reasons for migration and the past medical history of this population. The results of regression analysis indicate the content of association as it may not be scientific enough to draw a causal connection by merely clarifying the chronological order. Second, the impact of short-term migration on hospitalization cannot be determined, for merely the older adults who had lived in their current residence for not <2 years were involved in this study. Third, the obtainment of primary care and outpatient services could not be acquired, thus rendering it difficult to directly verify the extent to which the deficiency of these services contributed to the increase in hospitalization. Lastly, the specific causes of hospitalization have not been determined yet, preventing identification of the main diseases affecting the migrant population. A follow-up study is underway to address these limitations.
Conclusions
Migration is associated with hospitalization among older adults in China. Despite the best socioeconomic status and health habits, the post-retirement urban migrant population is segmented into unique susceptibilities to hospitalization, especially by those with chronic diseases and unconfirmed chronic conditions in eastern China. It is required to supply this vulnerable population with high-quality chronic disease management. Effective policies should be formulated to improve the access of migrants to primary care services, and to narrow the gap in health care services across China. Nevertheless, further studies are necessary to investigate the reasons for migration, and the causal relationships between migration and hospitalization.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Biomedical Ethics Committee, Peking University. The patients/participants provided their written informed consent to participate in this study.
Author contributions
HZ conceived and designed the study and wrote the manuscript. YZ supervised the project, critically revised the manuscript for important intellectual content, and procured funding. HZ and NZ analyzed data. JY supervised the project and analyzed the formal. XL reviewed the manuscript. All authors approved the final manuscript.
Funding
This research was partly supported by the National Key Research and Development Program of China, grant number 2018YFC0114500 and 2018YFC0114506.
Acknowledgments
The authors are grateful to the CLHLS project team for providing valuable data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Dou X, Liu Y. Elderly migration in China: types, patterns, and determinants. J Appl Gerontol. (2017) 36:751–71. doi: 10.1177/0733464815587966
2. National Health Commission of the People's Republic of China. Report on China's Migrant Population Development 2015. Beijing: China Population Publishing House (2016).
3. Chen H, Qian Y, Dong Y, Yang Z, Guo L, Liu J, et al. Patterns and changes in life expectancy in China, 1990-2016. PLoS ONE. (2020) 15:e0231007. doi: 10.1371/journal.pone.0231007
4. National Health Commission of the People's Republic of China. Report on China's Migrant Population Development 2018. Beijing: China Population Publishing House (2019).
5. Bryant ES, El-Attar M. Migration and redistribution of the elderly: a challenge to community services. Gerontologist. (1984) 24:634–40. doi: 10.1093/geront/24.6.634
6. Ma C, Huo S, Chen H. Does integrated medical insurance system alleviate the difficulty of using cross-region health Care for the Migrant Parents in China– evidence from the China migrants dynamic survey. BMC Health Serv Res. (2021) 21:1053. doi: 10.1186/s12913-021-07069-w
7. Ferreira FBL. [Social health insurance in China: principal reforms and inequalities]. Salud Colect. (2017) 13:5–17. doi: 10.18294/sc.2017.999
8. Zhang X, Yu B, He T, Wang P. Status and determinants of health services utilization among elderly migrants in China. Global Health Res Policy. (2018) 3:8. doi: 10.1186/s41256-018-0064-0
9. Li H, Zhu W, Xia H, Wang X, Mao C. Cross-sectional study on the management and control of hypertension among migrants in primary care: what is the impact of segmented health insurance schemes? J Am Heart Assoc. (2019) 8:e012674. doi: 10.1161/JAHA.119.012674
10. Saluja S, Hochman M, Bourgoin A, Maxwell J. Primary care: the new Frontier for reducing readmissions. J Gen Intern Med. (2019) 34:2894–7. doi: 10.1007/s11606-019-05428-2
11. Sung NJ, Choi YJ, Lee JH. Primary page in South Korea. Int J Environ Res Public Health. (2018) 15. doi: 10.3390/ijerph15020272
12. Office of the Leading Group of the State Council for the Seventh National Population Census. Major Figures on 2020 Population Census of China. Beijing: China Statistics Press (2021).
13. Wang LM, Chen ZH, Zhang M, Zhao ZP, Huang ZJ, Zhang X, et al. [Study of the prevalence and disease burden of chronic disease in the elderly in China]. Zhonghua Liu Xing Bing Xue Za Zhi. (2019) 40:277–83. doi: 10.3760/cma.j.issn.0254-6450.2019.03.005
14. Wang L, Wang Z, Ma Q, Fang G, Yang J. The development and reform of public health in China from 1949 to 2019. Global Health. (2019) 15:45. doi: 10.1186/s12992-019-0486-6
15. Tang D, Wang J. Basic public health service utilization by internal older adult migrants in China. Int J Environ Res Public Health. (2021) 18:270. doi: 10.3390/ijerph18010270
16. Lin Y, Wang T, Zhu T. Do Migration characteristics influence the utilization of basic public health services in internal elderly migrants in China? Front Public Health. (2021) 9:514687. doi: 10.3389/fpubh.2021.514687
17. Tang S, Long C, Wang R, Liu Q, Feng D, Feng Z. Improving the utilization of essential public health services by Chinese elderly migrants: strategies and policy implication. J Glob Health. (2020) 10:010807. doi: 10.7189/jogh.10.010807
18. Su L, Sun L, Xu L. Review on the prevalence, risk factors and disease management of hypertension among floating population in China during 1990-2016. Global Health Res Policy. (2018) 3:24. doi: 10.1186/s41256-018-0076-9
19. Elek P, Molnár T, Váradi B. The closer the better: does better access to outpatient care prevent hospitalization? Eur J Health Econ. (2019) 20:801–17. doi: 10.1007/s10198-019-01043-4
20. Li Y, Lu C, Liu Y. Medical insurance information systems in China: mixed methods study. JMIR Med Inform. (2020) 8:e18780. doi: 10.2196/18780
21. Zhu D, Guo N, Wang J, Nicholas S, Chen L. Socioeconomic inequalities of outpatient and inpatient service utilization in China: personal and regional perspectives. Int J Equity Health. (2017) 16:210. doi: 10.1186/s12939-017-0706-8
22. Niu L, Liu Y, Wang X, Li H, Chen J, Sriplung H. The effect of migration duration on treatment delay among rural-to-urban migrants after the integration of urban and rural health insurance in china: a cross-sectional study. Inquiry. (2020) 57:46958020919288. doi: 10.1177/0046958020919288
23. Zhang X, Dupre ME, Qiu L, Zhou W, Zhao Y, Gu D. Age and sex differences in the association between access to medical care and health outcomes among older Chinese. BMC Health Serv Res. (2018) 18:1004. doi: 10.1186/s12913-018-3821-3
24. Wan S, Chen Y, Xiao Y, Zhao Q, Li M, Wu S. Spatial analysis and evaluation of medical resource allocation in China based on geographic big data. BMC Health Serv Res. (2021) 21:1084. doi: 10.1186/s12913-021-07119-3
25. Chai KC, Zhang YB, Chang KC. Regional disparity of medical resources and its effect on mortality rates in China. Front Public Health. (2020) 8:8. doi: 10.3389/fpubh.2020.00008
26. Yang L, Martikainen P, Silventoinen K, Konttinen H. Association of socioeconomic status and cognitive functioning change among elderly Chinese people. Age Ageing. (2016) 45:674–80. doi: 10.1093/ageing/afw107
27. Yi Z. Introduction to the Chinese Longitudinal Healthy Longevity Survey (CLHLS) Chapter 2. In: Yi Z, Poston DL, editors. Healthy Longevity in China. Netherland: Springer Netherlands (2008), p. 23–38. doi: 10.1007/978-1-4020-6752-5_2
28. Gao M, Kuang W, Qiu P, Wang H, Lv X, Yang M. The time trends of cognitive impairment incidence among older Chinese people in the community: based on the CLHLS cohorts from 1998 to 2014. Age Ageing. (2017) 46:787–93. doi: 10.1093/ageing/afx038
29. Evandrou M, Falkingham J, Green M. Migration in later life: evidence from the British Household Panel Study. Popul Trends. (2010) 74–91. doi: 10.1057/pt.2010.22
30. Hosmer DL, Lemeshow S. Applied Logistic Regession. New York, NY: John Wiley and Sons (2000). doi: 10.1002/0471722146
31. Liang Z, Li Z, Ma Z. Changing patterns of the floating population in China during 2000-2010. Popul Dev Rev. (2014) 40:695–716. doi: 10.1111/j.1728-4457.2014.00007.x
32. Guo M, Stensland M, Li M, Dong X, Tiwari A. Is migration at older age associated with poorer psychological well-being? Evidence from Chinese Older Immigrants in the United States. Gerontologist. (2019) 59:865–76. doi: 10.1093/geront/gny066
33. Ruan Y, Zhu D, Lu J. Social adaptation and adaptation pressure among the “drifting elderly” in China: a qualitative study in Shanghai. Int J Health Plann Manage. (2019) 34:e1149–65. doi: 10.1002/hpm.2750
34. Park HJ, Morgan T, Wiles J, Gott M. Lonely ageing in a foreign land: social isolation and loneliness among older Asian migrants in New Zealand. Health Soc Care Community. (2019) 27:740–7. doi: 10.1111/hsc.12690
35. Li Q, Zhou X, Ma S, Jiang M, Li L. The effect of migration on social capital and depression among older adults in China. Soc Psychiatry Psychiatr Epidemiol. (2017) 52:1513–22. doi: 10.1007/s00127-017-1439-0
36. Thapa DK, Visentin DC, Kornhaber R, Cleary M. Prevalence and factors associated with depression, anxiety, and stress symptoms among older adults: a cross-sectional population-based study. Nurs Health Sci. (2020) 22:1139–52. doi: 10.1111/nhs.12783
37. Singh NS, Bass J, Sumbadze N, Rebok G, Perrin P, Paichadze N, Robinson WC. Identifying mental health problems and Idioms of distress among older adult internally displaced persons in Georgia. Soc Sci Med. (2018) 211:39–47. doi: 10.1016/j.socscimed.2018.05.007
38. Bradley DE, Van Willigen M. Migration and psychological well-being among older adults: a growth curve analysis based on panel data from the Health and Retirement Study, 1996-2006. J Aging Health. (2010) 22:882–913. doi: 10.1177/0898264310368430
39. Bhugra D. Migration and mental health. Acta Psychiatr Scand. (2004) 109:243–58. doi: 10.1046/j.0001-690X.2003.00246.x
40. Gubernskaya Z. Age at migration and self-rated health trajectories after age 50: understanding the older immigrant health paradox. J Gerontol B Psychol Sci Soc Sci. (2015) 70:279–90. doi: 10.1093/geronb/gbu049
41. Ohrnberger J, Fichera E, Sutton M. The relationship between physical and mental health: a mediation analysis. Soc Sci Med. (2017) 195:42–9. doi: 10.1016/j.socscimed.2017.11.008
42. Dopp AR, Lantz PM. Moving upstream to improve children's mental health through community and policy change. Adm Policy Ment Health. (2020) 47:779–87. doi: 10.1007/s10488-019-01001-5
43. Tarkowski K, Bojar I, Kister A, Raczkiewicz D. Changes in interregional migration of patients hospitalized in Poland - 2013-2017. Ann Agric Environ Med. (2019) 26:469–503. doi: 10.26444/aaem/105389
44. Ding J, Hu X, Zhang X, Shang L, Yu M, Chen H. Equity and efficiency of medical service systems at the provincial level of China's mainland: a comparative study from 2009 to 2014. BMC Public Health. (2018) 18:214. doi: 10.1186/s12889-018-5084-7
45. Fang H, Jin Y, Zhao M, Zhang H, J AR, Zhang D, Hou Z. Does migration limit the effect of health insurance on hypertension management in China? Int J Environ Res Public Health. (2017) 14:1256. doi: 10.3390/ijerph14101256
Keywords: older adults, migration, inpatient services, primary care, chronic disease
Citation: Zhong H, Yang J, Zhao N, Li X and Zhang Y (2022) The positive association between internal migration and hospitalization among the older adults in China: Regional heterogeneity and chronic disease management. Front. Public Health 10:977563. doi: 10.3389/fpubh.2022.977563
Received: 24 June 2022; Accepted: 05 August 2022;
Published: 01 September 2022.
Edited by:
Xiaodong Sun, Affiliated Hospital of Weifang Medical University, ChinaCopyright © 2022 Zhong, Yang, Zhao, Li and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yanli Zhang, emhhbmd5YW5saUBuaWhhLm9yZy5jbg==