 Siyuan Lei
Siyuan Lei Xuanlin Li
Xuanlin Li Hulei Zhao
Hulei Zhao Yang Xie
Yang Xie Jiansheng Li
Jiansheng Li- 1Co-Construction Collaborative Innovation Center for Chinese Medicine and Respiratory Diseases by Henan & Education Ministry of P.R. China, Henan University of Chinese Medicine, Zhengzhou, China
- 2College of Basic Medical Science, Institute of Basic Research in Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou, China
- 3Department of Respiratory Diseases, The First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, China
Background: Sepsis is a major public health problem that cannot be ignored in China and even in the world. However, the prevalence of sepsis in Chinese adults varies among different studies.
Objective: To evaluate the prevalence of hospital-wide sepsis and intensive care unit (ICU) sepsis in Chinese adults.
Methods: PubMed, EMBASE, Cochrane Library, Web of science, China National Knowledge Infrastructure, Chinese biomedical literature service system, Wanfang Database, and VIP databases were systematically searched for studies on sepsis in China published before March 2, 2022. Random effects model was used to calculate pooled prevalence estimates with 95% confidence interval. Subgroup and sensitivity analyses were performed to address heterogeneity. Funnel plots and Egger's test were used to assess the publication bias.
Results: Overall, nine observational studies involving 324,020 Chinese patients (9,587 patients with sepsis) were analyzed. Four hospital-wide studies involving 301,272 patients showed pooled prevalence and mortality of 3.8% (95% CI: 2.9–4.7%, I2 = 99.9%) and 26% (95% CI: 16–36%, I2 = 98.0%), respectively. Five studies of ICU sepsis involving 22,748 patients presented pooled prevalence and mortality of 25.5% (95% CI: 13.9–37.0%, I2 = 99.8%) and 40% (95%CI: 34–47%, I2 = 95.9%), respectively. Subgroup analysis of sepsis in ICUs revealed that the pooled prevalence was higher among males [17% (95% CI 9–24%, I2 = 99.6%)], in lung infections [66% (95%CI: 54–77%, I2 = 98.7%)], and Gram-negative bacteria infections [37% (95%CI: 26–47%, I2 = 98.3%)]. The pooled prevalence of sepsis, severe sepsis and septic shock was 25.5% (95%CI: 13.9–37.0%, I2 = 99.8%), 19% (95%CI: 9–28%, I2 = 99.6%), and 13% (95%CI: 7–19%, I2 = 99.2%), respectively.
Conclusions: Sepsis is prevalent in 25.5% of ICU patients in China, and sex, sepsis severity, infection site, causative microorganism, and infection type are significant influencing factors. Larger trials are needed to evaluate the prevalence of sepsis in China, which may help the development of global strategies for sepsis management.
Systematic review registration: PROSPERO, identifier: CRD42022314274.
Introduction
Sepsis is a life-threatening organ dysfunction caused by a dysregulated host response to infection (1), which has become a leading cause of mortality and critical illness worldwide (2). Approximately 48.9 million cases of sepsis and 11 million sepsis-related deaths were recently reported, accounting for 19.7% of all global deaths (3). Sepsis is a major global public health concern characterized by high morbidity, high mortality, and heavy economic burden (4). Sepsis survivors often have long-term physical (5), psychological (6), and cognitive impairments (7) with significant health care and social implications. Thus, improving the prevention, recognition, and treatment of sepsis was declared as a global health priority by the World Health Organization (WHO) in 2017 (8). Sepsis is considered as the most expensive disease of hospitals in the United States, costing approximately $23.7 billion annually and accounting for 6.2% of the aggregate costs for all hospitalizations, which may be higher in low and middle-income countries (9, 10).
Several systematic reviews and meta-analyses have reported the global prevalence of sepsis (11–13). Fleischmann et al pooled data on sepsis from 1979 to 2015 across seven high-income countries and reported a population incidence rate of 288 hospital-treated sepsis cases and 148 severe sepsis cases per 100000 person-years (11). However, due to limited data, the incidence of sepsis in low and middle-income countries was not estimated. Markwart et al. assessed the epidemiology of sepsis acquired in hospitals and intensive care units (ICUs) separately and revealed that the pooled incidence of hospital-acquired sepsis was 15.4 cases per 1000 patients and that of ICU acquired sepsis was 44.8 cases per 1000 ICU patients (12). In a recent meta-analysis, the pooled incidence of hospital-treated sepsis was 189 per 100000 person-years, of which 26.7% of sepsis patients died, while the incidence of ICU-treated sepsis was 58 per 10,0000 person-years, of which 41.9% of patients died prior to hospital discharge (13).
In China, sepsis is a great challenge due to the progressive aggravation of the aging population. Recent research has focused on risk factors, mechanisms, and treatments for sepsis (14–16), but the management of epidemiology is also important. Although several studies (17–25) have reported the prevalence of sepsis in China, the prevalence of sepsis between studies was inconsistent, possibly owing to differences in the survey periods, sampling, study sites, diagnostic criteria, and sample demographic characteristics. As the most populous and largest developing country globally, the epidemiological status of sepsis in China cannot be ignored. However, so far there has been no independent systematic review and meta-analysis on the prevalence of sepsis in China. With the rapid development of critical care medicine in the past years, having a deeper insight into the epidemiologic patterns of sepsis in Chinese adults contributes to better managing this disease and providing an evidence-based basis for governments to make relevant public health strategic decisions. In addition, it also has important implications for estimating the burden of sepsis worldwide. Therefore, this review aimed to evaluate the prevalence and characteristics of hospital-wide and ICU sepsis in China.
Materials and methods
This systematic review and meta-analysis was performed according to the guidelines in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA 2020), and the protocol was submitted to the Prospective Register for Systematic Reviews (PROSPERO) (CRD42022314274).
Search strategy
Two researchers independently and systematically searched eight different databases, including PubMed, EMBASE, Cochrane Library, Web of science, China National Knowledge Infrastructure, Chinese biomedical literature service system, Wanfang Database, and VIP database from their inception to March 2, 2022. The Medical Subject Headings (MESH) terms and keywords used in the search were as follows: (“sepsis” OR “septicemia*” OR “septic shock*” OR “severe sepsis*” OR “systemic inflammatory response syndrome” OR “SIRS” OR “septic” OR “septicaemic shock”) AND (“epidemic*” OR “incidence” OR “Prevalence” OR “Morbidity” OR “occur” OR “screen” OR epidemiolog* OR “demograph*” OR “etiolog*” OR “rate”) AND (“China” OR “Chinese”). In addition, we screened the references of the identified articles and existing systematic reviews to further identify relevant studies. The complete search strategy is detailed in Supplementary Table 1.
Inclusion and exclusion criteria
Studies were included if they met all of the following criteria: (1)observational design, including cohort, case-control, or cross-sectional studies; (2) study population aged ≥18 years; (3)sepsis diagnosis in accordance with appropriate criteria (such as the sepsis-1 or sepsis-2 or sepsis-3) or the current relevant guidelines; (4) report on the incidence or prevalence of sepsis and available data related to the defined primary outcomes of the current systematic review; and (5) population-based design and conducted in hospital-wide or ICUs in China. The exclusion criteria were as follows: (1) conference abstracts, study protocols, case studies, reviews; (2) duplicate publications; and (3) incomplete data or no relevant outcome.
Study selection
Two reviewers independently screened the titles and abstracts to identify relevant articles. The full text of each potentially eligible article was then read to identify studies for analysis. Any disagreement was resolved through a discussion with a third investigator.
Data extraction
Two reviewers independently extracted data on participant and study characteristics according to the guideline for data extraction for systematic reviews and meta-analysis (26), such as first author, publication years, journal, study setting (hospital-acquired or ICU-acquired), sample size, study period, sepsis type, sepsis diagnostic criteria, mean or median age, patients source, sepsis cases, comorbid conditions, number of deaths, risk factors of mortality, duration of ICU or hospital stay, type of infection, infection site and microorganisms.
Risk of bias assessment
The quality of included studies was evaluated using the 10-item disease prevalence quality tool modified by Hoy et al. (27). Each study is assigned a total score ranging from 0 to 10, with higher scores indicating better study quality. The study quality was then classified based on these scores as low (0–5), moderate (6–8) or high (8–10), respectively.
Statistical analysis
We extracted sepsis events and the total sample size to calculate the prevalence of sepsis, number of deaths and sepsis events for each included study to calculate mortality. The random-effects model was used to separately estimate the ICU and hospital-wide prevalence of sepsis. The Chi-square test and I2 value were implemented to assess heterogeneity, and P < 0.1 or I2≥ 75% was defined as significant heterogeneity. Subgroup analysis was performed to determine whether the prevalence was influenced by sex and severity of sepsis. Sensitivity analyses was conducted by plotting the pooled prevalence and excluding one study each time to judge the robustness of our results. Funnel plots and Egger's test were used to assess publication bias. All statistical analyses were performed using Stata software (version 15.1), and P < 0.05 was considered statistically significant.
Results
Search results
A total of 12,006 articles were found, after removing 1,772 duplicates, the titles and abstracts of 10,201 articles were screened, and 33 articles were subjected to a full-text review. Of these, 24 articles were excluded: 7 articles were Master PhD thesis, 5 articles were conference abstracts, and 12 articles were neonatal studies (Supplementary Table 2). Finally, nine observational studies involving 9,587 patients with sepsis were included in the analysis. The search selection process is shown in Figure 1.
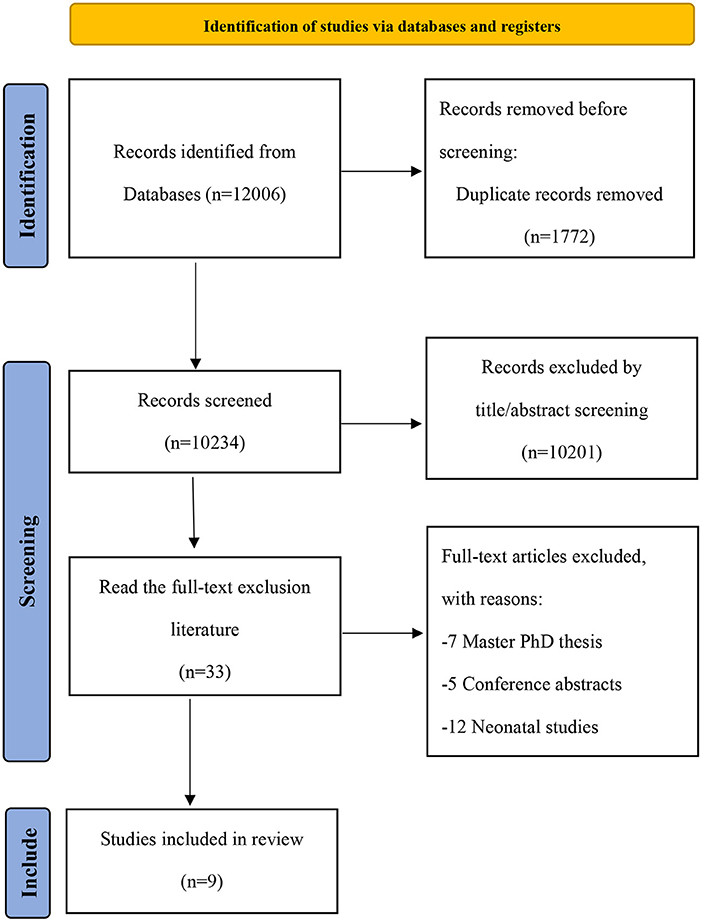
Figure 1. Literature screening flow chart.
Studies characteristics
The characteristics of the included studies are presented in Table 1. The studies were published between 2000 and 2021, and the sample size ranged from 1,297 to 171,707. Eight studies were published in English-language journals, while one study was in a Chinese-language journal. Of the nine studies, four (17, 20, 21, 25) were conducted in hospital-wide, and five (18, 19, 22–24) were conducted in ICUs. In addition, four (17, 20, 21, 25) studies were retrospective in design, four (18, 19, 22, 24) were prospective, and one (23) was a cross-section survey. The mean age of patients ranged from 36.8 years to 81 years. Sepsis was diagnosed following the Sepsis-1.0/3.0 criteria in three trials (23–25), American College of Chest Physicians/Society of Critical Care Medicine consensus in three studies (18–20), and current relevant guidelines in another three studies (17, 21, 22).
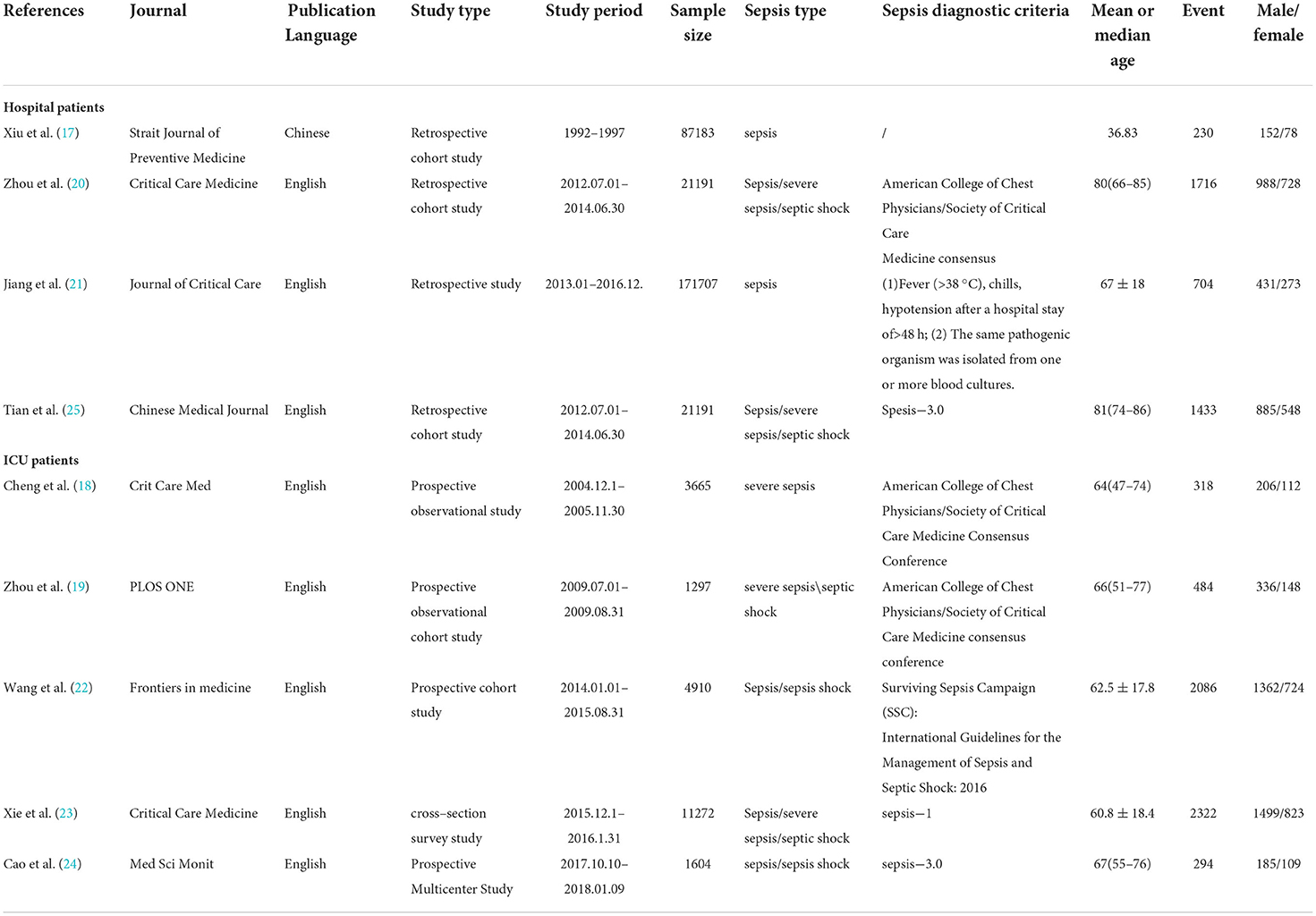
Table 1. Characteristics of studies included in the review.
Characteristics of patients in ICUs
The five (18, 19, 22–24) studies included 22,748 participants, most of whom were from the surgical, medical ward and emergency department before ICU admission. The mean Acute Physiology and Chronic Health Evaluation II (APACHE II) and Sepsis-related Organ Failure Assessment (SOFA) scores of these patients ranged from 18 to 26 and 7 to 10, respectively. These patients were mainly admitted to the ICU with respiratory, cardiovascular, neurological, gastrointestinal, and acute trauma, which were mostly comorbid with other underlying disease. Most patients diagnosed with sepsis developed acute organ dysfunction, with acute respiratory distress syndrome and acute kidney injury being the most common. The mean duration of ICU stay and hospital stay were 4–8 and 8–22 days, respectively. The characteristics of patients in ICUs are shown in Table 2.
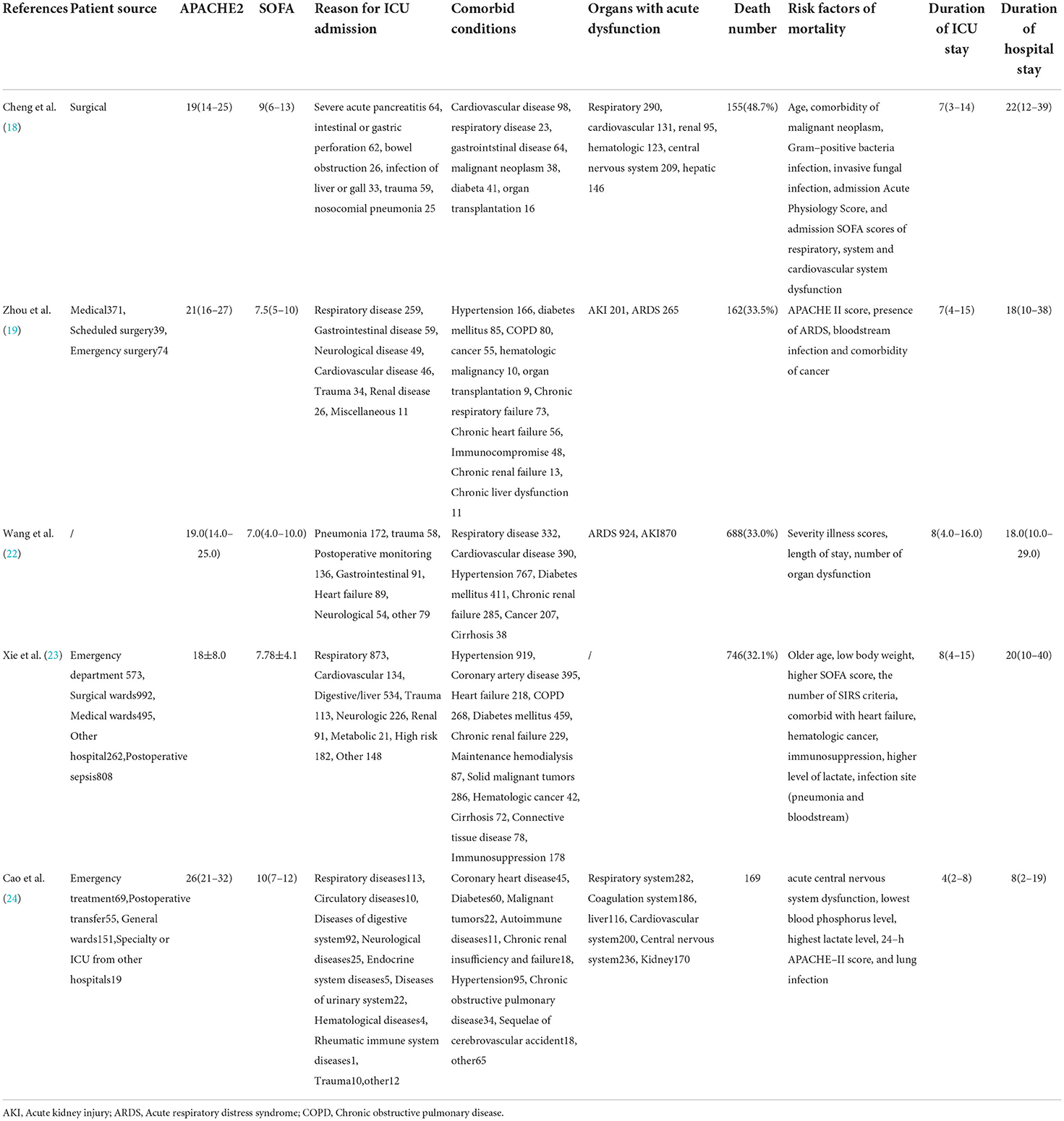
Table 2. Characteristics of ICU patients included in the review.
Characteristics of infection and causative organisms in ICU patients
All five (18, 19, 22–24) studies reported the source of infection, site of infection and the microorganism, and sources of infection including ICU acquired, hospital acquired and community-acquired infections. The sites of infection were mainly in the lung, abdomen, intestine, urinary tract, and bloodstream. The common causative microorganisms were Gram-negative bacteria, Gram-positive bacteria, and fungi. Four (18, 19, 22, 24) studies reported pathogenic bacteria, mainly Staphylococcus aureus, Klebsiella pneumoniae, Pseudomonas aeruginosa, Escherichia coli, and Acinetobacter baumannii. The characteristics of infection and organisms in ICUs are shown in Table 3.
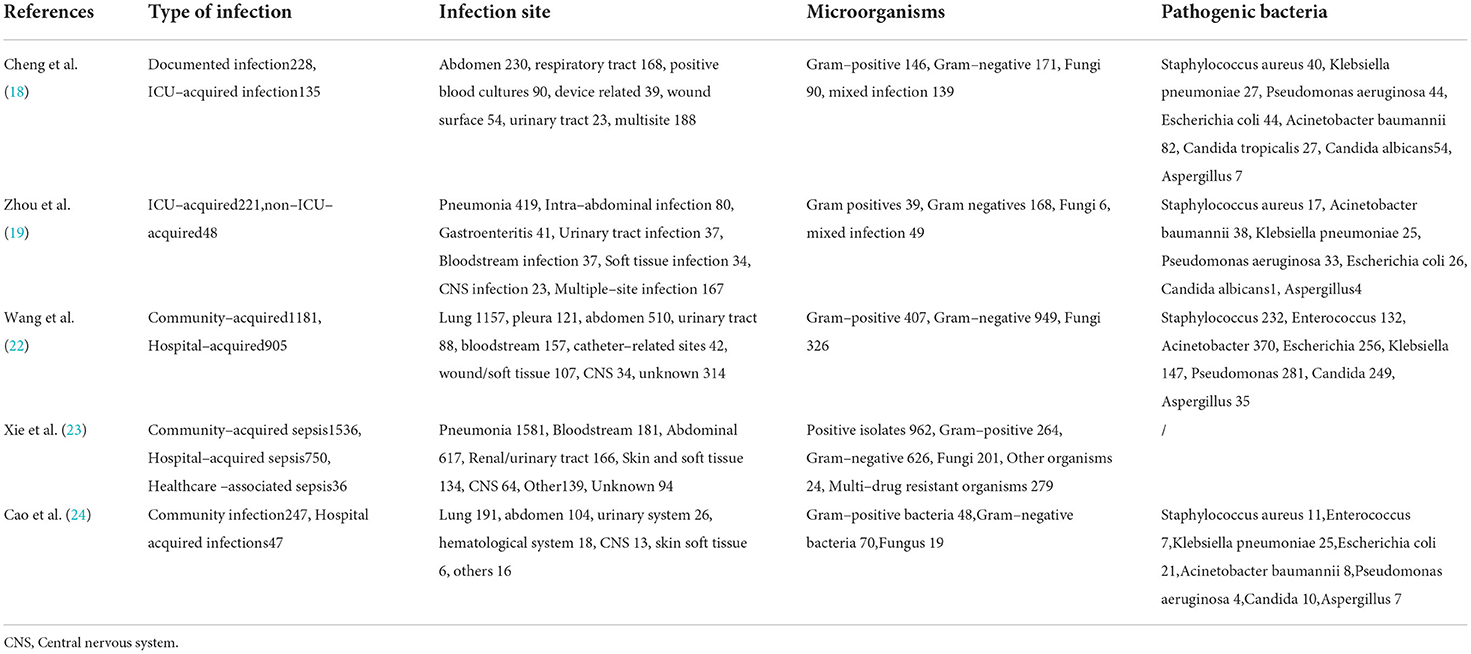
Table 3. Characteristics of infection in ICU patients included in the review.
Risk of bias assessment
The quality of the included studies is presented in Table 4. One (17) study with 5 points was judged as low quality, seven (18–22, 24, 25) study with 6–8 points were judged as moderate quality, and one (23) study with 9 was judged as high quality.
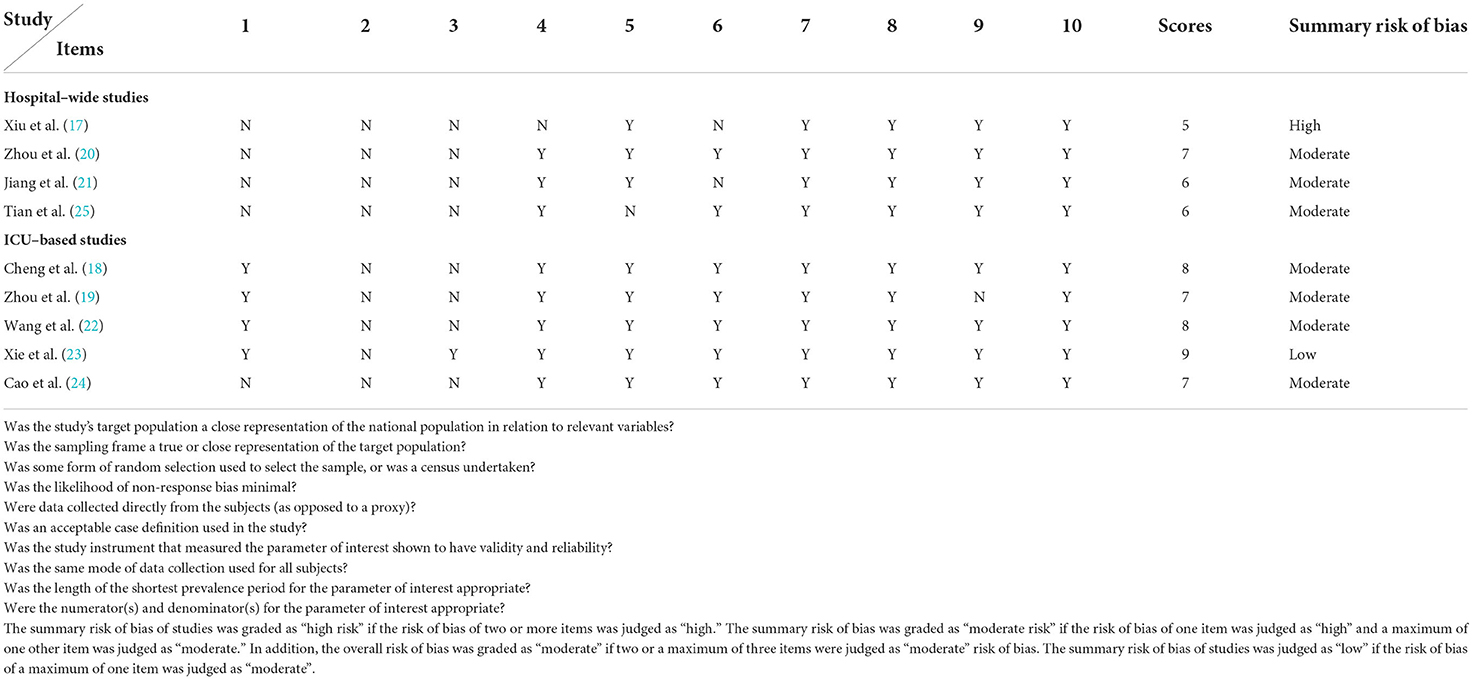
Table 4. Risk of bias for included studies.
Prevalence of sepsis in China
Four (17, 20, 21, 25) studies provided data on the prevalence of hospital-wide sepsis and five (18, 19, 22–24) studies provided data on ICU sepsis. The overall pooled prevalence was 3.8% (95%CI: 2.9–4.7%, I2 = 99.9%, P = 0.000) for hospital-wide sepsis and 25.5% (95%CI: 13.9–37.0%, I2 = 99.8%, P = 0.000) for ICU sepsis (Tables 5, 6).
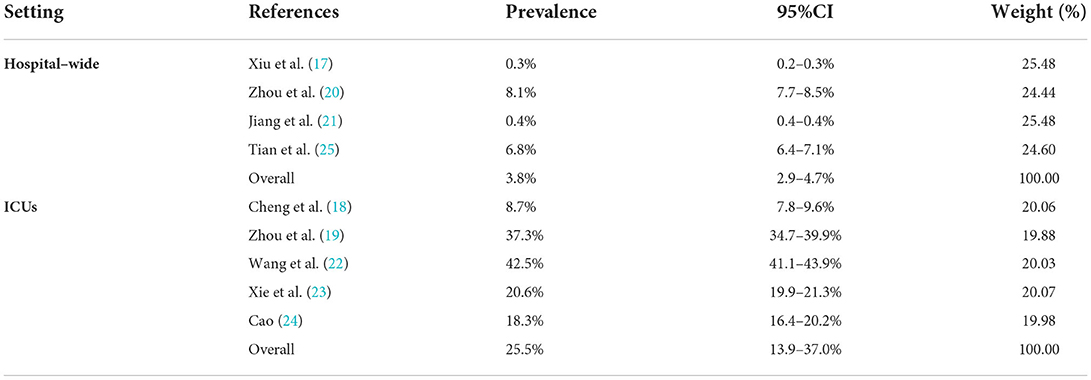
Table 5. The prevalence of sepsis in hospital–wide and ICUs in China.
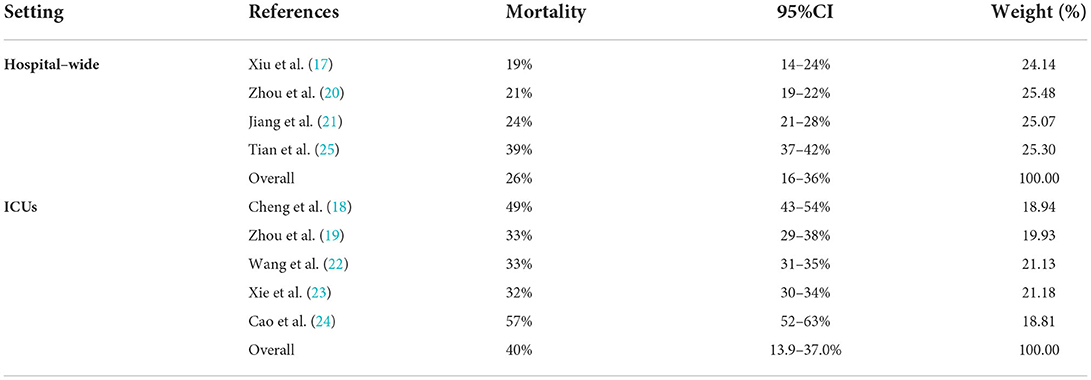
Table 6. The mortality of sepsis in hospital–wide and ICUs in China.
Hospital mortality of sepsis
All nine (17–25) studies provided the number of sepsis deaths. The estimated pooled of hospital mortality of sepsis was 26% (95%CI: 16–36%, I2 = 98.0%, P = 0.000) for hospital-wide and 40% (95%CI: 34–47%, I2 = 95.9%, P = 0.000) for ICU sepsis (Tables 5, 6).
Subgroup analysis of ICU sepsis
A separate meta-analysis was performed using random effects models for subgroup effects of sex, sepsis severity, site of infection, microorganisms, and type of infection on ICU sepsis. The pooled prevalence of ICU sepsis was 17% (95% CI 9–24%, I2 = 99.6%, P = 0.000) among males, and 9% (95% CI 5–12%, I2 = 99.1%, P = 0.000) for females (Table 7).
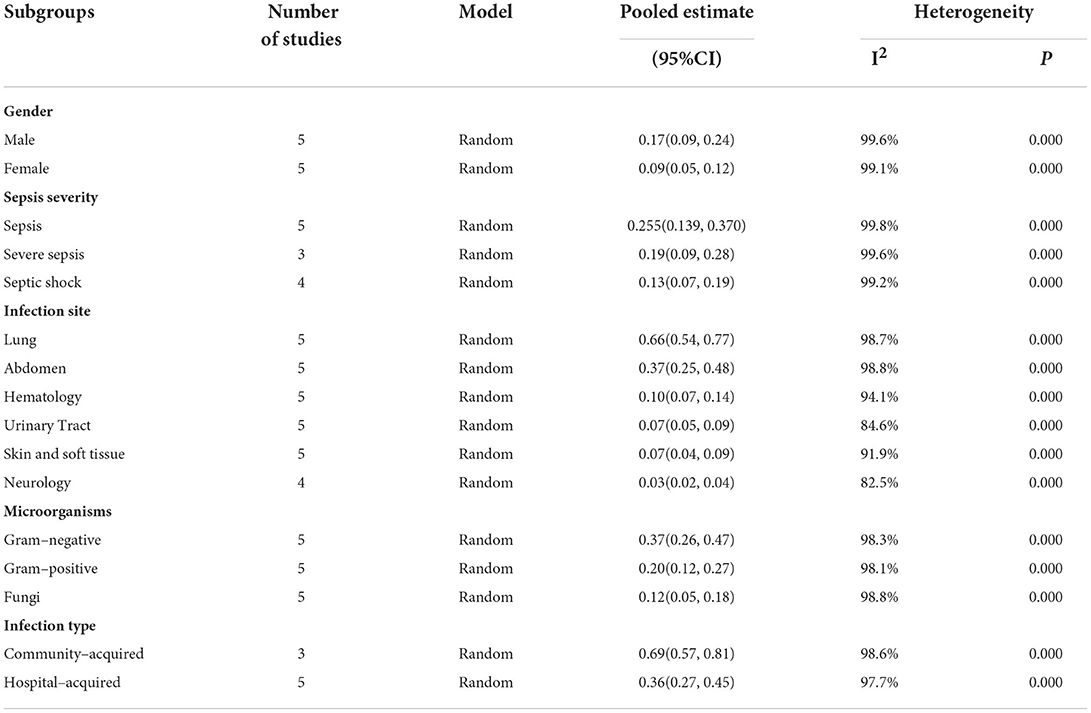
Table 7. Subgroup analysis of the prevalence of ICUs sepsis.
With respect to the severity of sepsis, the pooled prevalence of sepsis, severe sepsis, and septic shock in ICUs were 25.5% (95%CI: 13.9–37.0%, I2 = 99.8%, P = 0.000), 19% (95%CI: 9–28%, I2 = 99.6%, P = 0.000), and 13% (95%CI: 7–19%, I2 = 99.2%, P = 0.000), respectively (Table 7).
According to the site of infection, the pooled prevalence of ICU sepsis was the highest in pulmonary infections at 66% (95%CI: 54–77%, I2 = 98.7%, P = 0.000), followed by that in abdominal infections at 37% (95%CI: 25–48%, I2 = 98.8%, P = 0.000), hematologic infections at 10% (95%CI: 7–14%, I2 = 94.1%, P = 0.000), urinary tract infections at 7% (95%CI: 5–9%, I2 = 84.6%, P = 0.000), skin and soft tissue infections at 7% (95%CI: 4–9%, I2 = 91.9%, P = 0.000), and the lowest in neurology infections at 3% (95%CI: 2–4%, I2 = 82.5%, P = 0.001) (Table 7).
For the infected microorganisms, ICU sepsis was prevalent in 37% (95%CI: 26–47%, I2 = 98.3%, P = 0.000) of Gram–negative infections, 20% (95%CI: 12–27%, I2 = 98.1%, P = 0.000) of Gram–positive infections, and 12% (95%CI: 5–18%, I2 = 98.8%, P = 0.000) of fungi infections (Table 7).
In terms of the infection type, ICU sepsis was prevalent in 69% (95%CI: 57–81%, I2 = 98.6%, P = 0.000) of community–acquired infections and in 36% (95%CI: 27–45%, I2 = 97.7%, P = 0.000) of hospital–acquired infections (Table 7).
Sensitivity analyses
The sensitivity analyses showed that no individual study altered the pooled results, indicating that the pooled prevalence for ICU sepsis, hospital mortality for hospital–wide sepsis and ICU sepsis has good stability. However, there was large heterogeneity in the prevalence of hospital–wide sepsis (Supplementary Table 3).
Publication bias
The funnel plots and the Egger's test demonstrated that there was no publication bias on the prevalence for ICU sepsis (P = 0.452). The result of Egger's test was P = 0.017. Meanwhile, the asymmetric funnel plot showed that publication bias existed among the studies on the prevalence for hospital–wide sepsis (Figures 2, 3).
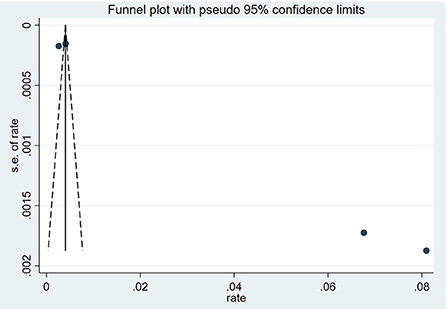
Figure 2. Funnel figure showing the prevalence of hospital–wide sepsis.
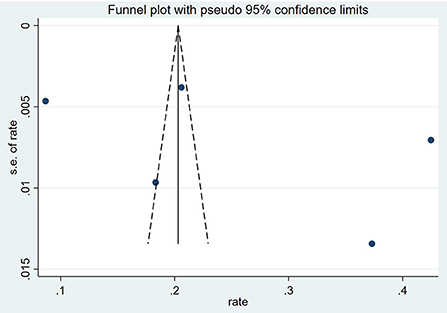
Figure 3. Funnel figure showing the prevalence of ICUs sepsis.
Discussion
In this systematic review of studies from China, the pooled prevalence was 3.8% (95%CI: 2.9–4.7%) for hospital–wide sepsis and 25.5% (95%CI: 13.9–37.0%) for ICU sepsis. The estimated pooled of hospital mortality for hospital–wide sepsis and ICU sepsis was 26% (95%CI: 16–36%) and 40% (95%CI: 34–47%), respectively. In addition, sex, sepsis severity, infection site, causative microorganisms and infection type were identified as significant factors of prevalence of ICU sepsis. To the best of our knowledge, this is the first meta–analysis to examine the prevalence of sepsis in China. Our findings could provide strong evidence about high prevalence of sepsis in China.
Sepsis could develop from healthcare–associated infections, and the WHO has provided strong evidence and recommendations on the effectiveness of infection prevention and control measures to reduce the incidence of hospital–wide sepsis (28). A 2011 global report by the WHO showed that the prevalence of hospital–wide sepsis ranges 5.7 to 19.1% (29), which indicates that sepsis still deserves our attention in hospital–wide. Our results were higher than those in the recent meta–analysis by Markwart et al. (12), which may be because most of the studies they included were from high–income countries and because sepsis has attracted great attention and active prevention and treatment in various countries in recent years. However, further improvements are needed considering that only 28% of countries worldwide have implemented functional measures, most of which are developed countries (30). Moreover, there may be objective reasons for the high prevalence in China, and these primarily could be due to the aging population, the large number of elderlies with comorbidities, and higher rates of antimicrobial resistance, which may lead to higher rates of hospital–wide sepsis.
Sepsis also has a more crucial impact in ICUs, and there have been several studies on the prevalence of ICU sepsis. A study analyzed more than 17,000 sepsis cases in the USA and found that 55% of these cases required ICU admission (31). In a Brazilian study, which included 317 ICUs, the incidence and mortality of ICU sepsis in adult was high at 30.2 and 55.7%, respectively (32). However, a prospective, multicenter, observational study in Italy conducted by Sakr et al. (33) indicated that the incidence of ICU sepsis was only 11.4%, and the ICU mortality was 41.3%, with the mortality rate increased with the severity of sepsis. In the current study the prevalence and mortality of ICU sepsis in China was 25.5 and 40%, lower than those reported in Brazil (32) but higher than those reported in Italy (33). These data suggest that the prevalence of ICU sepsis varies widely among countries, and the difference may be related to the higher burden of infectious diseases, varying patterns of underlying comorbidities, limited infection prevention strategies, and fewer resources for sepsis treatment and intensive care in low and middle–income countries. In addition, it may also be related to the large variation in development among regions in China and the insufficient attention paid by physicians to sepsis, leading to delayed treatment.
Subgroup analysis showed that the prevalence of ICU sepsis was higher in males than in females, consistent with the results of a German study (34). This may be related to the fact that comorbidities are more common in male (35). However, due to limited information, further studies are warranted to explore this phenomenon. We also found that the prevalence of ICU sepsis was negatively correlated with sepsis severity, which is similar to a previous finding (36) that sepsis is more prevalent than severe sepsis, and septic shock is the least prevalent.
As in other epidemiologic studies of sepsis (37–39), the most common site of infection in our study was the lung, followed by the abdomen. This finding indicated when the source of infection remains unknown in a sepsis patient in the ICU, clinicians should preferentially consider pulmonary and abdominal sources. Furthermore, it also suggested the importance of implementing effective strategies to prevent both community–acquired and hospital–acquired pneumonia. The analysis of microbiological characteristics of ICU sepsis in our study showed that Gram–negative bacteria were the most common pathogens, consistent with other studies (40, 41). However, several studies in developed countries reported a predominance of Gram–positive bacteria (42, 43). These differences may be explained by differences in underlying conditions, geographical variations, case mix, antibiotic prescription habits, invasive interventions, and the quality of care provided. Moreover, there might be bias in the results of microorganisms as not all studies reported microbiological findings. In addition, our study found that the majority of infections in ICU sepsis patients were acquired in the community, accounting for 69% of all ICU sepsis, in line with the results by Rudd et al. (3).
The strengths of this study are that it provided a comprehensive review of the prevalence of sepsis both hospital–wide and in ICUs in China and included a large number of studies, either in English or in Chinese. Second, we performed a pooled analysis of the characteristics of ICU sepsis according to sex, severity, microorganism, and site of infection. However, we also acknowledge several limitations in our study. Firstly, the definitions of sepsis were heterogeneous, and thus, the estimation of the prevalence might be biased. Second, our study did not cover all provinces and regions in China, restricting the generalizability of the findings. Differences in the prevalence of sepsis across regions could not be explored because of limited information in the included studies. Third, significant heterogeneity exists in our review. Despite our effort, the source of heterogeneity could not be identified because of the limited information in the primary studies. Lastly, important factors related to sepsis mortality, such as age, comorbidities, microbial distribution and use of medicine, were not analyzed due to insufficient data. More high–quality studies are required to report on the epidemiology of sepsis and resolve the many unknown factors related to sepsis.
Conclusions
This systematic review shows that the pooled prevalence of hospital–wide and ICU sepsis remains high in China. These findings provide evidence–based data that can help promote further sepsis research and prevention efforts throughout the nation, and contribute to develop global strategies for sepsis.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
JL and XL would answer for design and conception of the article. SL, XL, and HZ would answer for the collection, assembly of materials and would answer for data interpretation, analysis. SL and XL drafted the manuscript and contributed equally to the manuscript. XL, HZ, YX, and JL revised it. All authors reviewed and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Chinese Medicine Inheritance and Innovation Hundred and Ten Million Talent Project—Chief Scientist of Qi–Huang Project ([2020] No. 219); Zhong–yuan Scholars and Scientists Project (No.2018204); and Characteristic backbone discipline construction project of Henan Province (STG–ZYX03–202123).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.977094/full#supplementary-material
References
1. Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. (2021) 49:e1063–143. doi: 10.1097/CCM.0000000000005337
2. Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. (2021) 47:1181–247. doi: 10.1007/s00134-021-06506-y
3. Rudd KE, Johnson SC, Agesa KM, Shackelford KA, Tsoi D, Kievlan DR, et al. Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the Global Burden of Disease Study. Lancet. (2020) 395:200–11. doi: 10.1016/S0140-6736(19)32989-7
4. Reinhart K, Daniels R, Kissoon N, Machado FR, Schachter RD, Finfer S. Recognizing sepsis as a global health priority—a WHO resolution. N Engl J Med. (2017) 377:414–7. doi: 10.1056/NEJMp1707170
5. Mankowski RT, Anton SD, Ghita GL, Brumback B, Cox MC, Mohr AM, et al. Older sepsis survivors suffer persistent disability burden and poor long-term survival. J Am Geriatr Soc. (2020) 68:1962–9. doi: 10.1111/jgs.16435
6. Boede M, Gensichen JS, Jackson JC, Eißler F, Lehmann T, Schulz S, et al. Trajectories of depression in sepsis survivors: an observational cohort study. Crit Care. (2021) 25:161. doi: 10.1186/s13054-021-03577-7
7. Lei S, Li X, Zhao H, Feng Z, Chun L, Xie Y, et al. Risk of dementia or cognitive impairment in sepsis survivals: a systematic review and meta-analysis. Front Aging Neurosci. (2022) 14:839472. doi: 10.3389/fnagi.2022.839472
8. World Health Organization. World Health Assembly 70, Resolution 70.7: Improving the Prevention, Diagnosis and Clinical Management of Sepsis. (2017). Available online at: http://apps.who.int/gb/ebwha/pdf_files/WHA70/A70_R7-en.pdf (accessed May 29, 2017).
9. Torio CM, Andrews RM. National inpatient hospital costs: the most expensive conditions by payer, 2011. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD): Agency for Healthcare Research and Quality (US). (2013).
10. Seymour CW, Rea TD, Kahn JM, Walkey AJ, Yealy DM, Angus DC. Severe sepsis in pre-hospital emergency care: analysis of incidence, care, and outcome. Am J Respir Crit Care Med. (2012) 186:1264–71. doi: 10.1164/rccm.201204-0713OC
11. Fleischmann C, Scherag A, Adhikari NK, Hartog CS, Tsaganos T, Schlattmann P, et al. Assessment of global incidence and mortality of hospital-treated sepsis. current estimates and limitations. Am J Respir Crit Care Med. (2016) 193:259–72. doi: 10.1164/rccm.201504-0781OC
12. Markwart R, Saito H, Harder T, Tomczyk S, Cassini A, Fleischmann-Struzek C, et al. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. (2020) 46:1536–51. doi: 10.1007/s00134-020-06106-2
13. Fleischmann-Struzek C, Mellhammar L, Rose N, Cassini A, Rudd KE, Schlattmann P, et al. Incidence and mortality of hospital-and ICU-treated sepsis: results from an updated and expanded systematic review and meta-analysis. Intensive Care Med. (2020) 46:1552–62. doi: 10.1007/s00134-020-06151-x
14. Qu Z, Zhu Y, Wang M, Li W, Zhu B, Jiang L, et al. Prognosis and risk factors of sepsis patients in Chinese ICUs: a retrospective analysis of a cohort database. Shock. (2021) 56:921–6. doi: 10.1097/SHK.0000000000001784
15. Li C, Wang P, Zhang L, Li M, Lei X, Liu S, et al. Efficacy and safety of Xuebijing injection (a Chinese patent) for sepsis: a meta-analysis of randomized controlled trials. J Ethnopharmacol. (2018) 224:512–21. doi: 10.1016/j.jep.2018.05.043
16. Han GX, Song Y, Chen L, Zhai YZ, Dong J, Li TS, et al. The role of mitochondrial DNA mutations in a Han Chinese population on sepsis pathogenesis. Eur Rev Med Pharmacol Sci. (2017) 21:3247–52.
17. Xiu CY Li Y, Xu NF, Wang LL. Epidemiology of nosocomial sepsis. J Clin prevent Med. (2000) 4:22–3.
18. Cheng B, Xie G, Yao S, Wu X, Guo Q, Gu M, et al. Epidemiology of severe sepsis in critically ill surgical patients in ten university hospitals in China. Crit Care Med. (2007) 35:2538–46. doi: 10.1097/01.CCM.0000284492.30800.00
19. Zhou J, Qian C, Zhao M, Yu X, Kang Y, Ma X, et al. Epidemiology and outcome of severe sepsis and septic shock in intensive care units in mainland China. PLoS ONE. (2014) 9:e107181. doi: 10.1371/journal.pone.0107181
20. Zhou J, Tian H, Du X, Xi X, An Y, Duan M, et al. Population-based epidemiology of sepsis in a subdistrict of Beijing. Crit Care Med. (2017) 45:1168–76. doi: 10.1097/CCM.0000000000002414
21. Jiang ZQ, Wang SD, Feng DD, Zhang BX, Mao SH, Wu JN. Epidemiological risk factors for nosocomial bloodstream infections: a four-year retrospective study in China. J Crit Care. (2019) 52:92–6. doi: 10.1016/j.jcrc.2019.04.019
22. Wang M, Jiang L, Zhu B, Li W, Du B, Kang Y, et al. The prevalence, risk factors, and outcomes of sepsis in critically Ill patients in China: a multicenter prospective cohort study. Front Med (Lausanne). (2020) 7:593808. doi: 10.3389/fmed.2020.593808
23. Xie J, Wang H, Kang Y, Zhou L, Liu Z, Qin B, et al. The epidemiology of sepsis in Chinese ICUs: a national cross-sectional survey. Crit Care Med. (2020) 48:e209–18. doi: 10.1097/CCM.0000000000004155
24. Cao L, Xiao M, Wan Y, Zhang C, Gao X, Chen X, et al. Epidemiology and mortality of sepsis in intensive care units in prefecture-level cities in Sichuan, China: a prospective multicenter study. Med Sci Monit. (2021) 27:e932227. doi: 10.12659/MSM.932227
25. Tian HC, Zhou JF, Weng L, Hu XY, Peng JM, Wang CY, et al. Epidemiology of Sepsis-3 in a sub-district of Beijing: secondary analysis of a population-based database. Chin Med J (Engl). (2019) 132:2039–45. doi: 10.1097/CM9.0000000000000392
26. Taylor KS, Mahtani KR, Aronson JK. Summarising good practice guidelines for data extraction for systematic reviews and meta-analysis. BMJ Evid Based Med. (2021) 26:88–90. doi: 10.1136/bmjebm-2020-111651
27. Hoy D, Brooks P, Woolf A, Blyth F, March L, Bain C, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. (2012) 65:934–9. doi: 10.1016/j.jclinepi.2011.11.014
28. Hagel S, Ludewig K, Pletz MW, Frosinski J, Moeser A, Wolkewitz M, et al. Effectiveness of a hospital-wide infection control programme on the incidence of healthcare-associated infections and associated severe sepsis and septic shock: a prospective interventional study. Clin Microbiol Infect. (2019) 25:462–8. doi: 10.1016/j.cmi.2018.07.010
29. World Health Organization. Report on the burden of endemic health care-associated infection worldwide. World Health Organization, Geneva. (2011)
30. WHO. Available online at: https://www.who.int/antimicrobial-resistance/global-action-plan/database/en/ (accessed 16 Jan 2020).
31. Rhee C, Dantes R, Epstein L, Murphy DJ, Seymour CW, Iwashyna TJ, et al. Incidence and trends of sepsis in US hospitals using clinical vs claims data, 2009–2014. JAMA. (2017) 318:1241–9. doi: 10.1001/jama.2017.13836
32. Machado FR, Cavalcanti AB, Bozza FA, Ferreira EM, Angotti Carrara FS, Sousa JL, et al. The epidemiology of sepsis in Brazilian intensive care units (the Sepsis PREvalence Assessment Database, SPREAD): an observational study. Lancet Infect Dis. (2017) 17:1180–9. doi: 10.1016/S1473-3099(17)30322-5
33. Sakr Y, Jaschinski U, Wittebole X, Szakmany T, Lipman J, Ñamendys-Silva SA, et al. Sepsis in intensive care unit patients: worldwide data from the intensive care over nations audit. Open Forum Infect Dis. (2018) 5:ofy313. doi: 10.1093/ofid/ofy313
34. SepNet Critical Care Trials Group. Incidence of severe sepsis and septic shock in German intensive care units: the prospective, Multicentre INSEP study. Intensive Care Med. (2016) 42:1980–89. doi: 10.1007/s00134-016-4504-3
35. Mauvais-Jarvis F, Bairey Merz N, Barnes PJ, Brinton RD, Carrero JJ, DeMeo DL, et al. Sex and gender: modifiers of health, disease, and medicine. Lancet. (2020) 396:565–82. doi: 10.1016/S0140-6736(20)31561-0
36. Shankar-Hari M, Harrison DA, Rubenfeld GD, Rowan K. Epidemiology of sepsis and septic shock in critical care units: comparison between sepsis-2 and sepsis-3 populations using a national critical care database. Br J Anaesth. (2017) 119:626–36. doi: 10.1093/bja/aex234
37. Vincent JL, Sakr Y, Sprung CL, Ranieri VM, Reinhart K, Gerlach H, et al. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. (2006) 34:344–53. doi: 10.1097/01.CCM.0000194725.48928.3A
38. Finfer S, Bellomo R, Lipman J, French C, Dobb G, Myburgh J. Adult-population incidence of severe sepsis in Australian and New Zealand intensive care units. Intensive Care Med. (2004) 30:589–96. doi: 10.1007/s00134-004-2157-0
39. Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. (2009) 302:2323–9. doi: 10.1001/jama.2009.1754
40. Tanriover MD, Guven GS, Sen D, Unal S, Uzun O. Epidemiology and outcome of sepsis in a tertiary-care hospital in a developing country. Epidemiol Infect. (2006) 134:315–322. doi: 10.1017/S0950268805004978
41. Khwannimit B, Bhurayanontachai R. The epidemiology of, and risk factors for, mortality from severe sepsis and septic shock in a tertiary-care university hospital setting. Epidemiol Infect. (2009) 137: 1333–1341. 027 doi: 10.1017/S0950268809002027
42. Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. (2001) 29:1303–10. doi: 10.1097/00003246-200107000-00002
Keywords: sepsis, China, prevalence, systematic review, meta-analysis
Citation: Lei S, Li X, Zhao H, Xie Y and Li J (2022) Prevalence of sepsis among adults in China: A systematic review and meta-analysis. Front. Public Health 10:977094. doi: 10.3389/fpubh.2022.977094
Received: 01 July 2022; Accepted: 16 September 2022;
Published: 11 October 2022.
Edited by:
Eduardo Rodriguez-Noriega, Civil Hospital of Guadalajara, MexicoReviewed by:
Silvia-Giono Cerezo, Instituto Politécnico Nacional (IPN), MexicoAdriano Friganovic, University Hospital Centre Zagreb, Croatia
Copyright © 2022 Lei, Li, Zhao, Xie and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jiansheng Li, bGlfanM4QDE2My5jb20=
†These authors share first authorship