
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health , 09 November 2022
Sec. Public Health Education and Promotion
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.976941
This article is part of the Research Topic Promoting Health Equity During a Pandemic: Approaches to Address Vaccination Burden and Health Inequities Amongst Under-Served Populations in U.S. and Mexico View all 19 articles
 María Gudelia Rangel Gómez1,2*
María Gudelia Rangel Gómez1,2* Saúl Salazar2
Saúl Salazar2 Ana María López Jaramillo2
Ana María López Jaramillo2 Isaura Angélica Lira Chávez2
Isaura Angélica Lira Chávez2 Alejandra Romero Rangel2
Alejandra Romero Rangel2 Martha Leticia Caballero Abraham3Luis Gutiérrez Reyes4
Martha Leticia Caballero Abraham3Luis Gutiérrez Reyes4 Cecilia B. Rosales5 on behalf of the network of agencies and promoters of the Ventanillas de Salud and Mobile Health Units
Cecilia B. Rosales5 on behalf of the network of agencies and promoters of the Ventanillas de Salud and Mobile Health UnitsOver the years, the Mexican population in the United States has faced high prevalence of health-related inequalities and disadvantages and represents one of the most vulnerable migrant groups in the country. To help reduce the gaps in health care for the Mexican population, the Mexican government, in collaboration with strategic allies from various sectors, launched the Ventanillas de Salud (VDS) strategy, which was subsequently reinforced through the Mobile Health Units (MHU) care model. Both the VDS strategy and the MHU care model are intended to contribute to the development of initiatives, projects, and actions in health that will benefit the Mexican community living in the United States, which lacks or has difficulty accessing health services. This article provides a descriptive, analytical analysis of the VDS strategy and the MHU care model, as unique collaborative models, which can be replicated, and have achieved a positive impact on the health of Mexican and other Hispanic communities in the United States, at both the individual and community level.
According to data from the Current Population Survey 2020, the Hispanic population in the United States (62.1 million people) represents 18.6% of the total population (331 million), while the community of Mexican origin (38.5 million) accounts for 11.5%. Within this Hispanic community, the majority have American citizenship (80.2% Hispanics and 81.2% Mexicans), either by birth or naturalization; one in 10 obtained Legal Permanent Resident status and one in 10 lacks documents for their legal stay in the United States. In absolute numbers, 10.8 million of all Hispanics lack medical coverage, of which 7.2 million are of Mexican origin (1). The lack of access to medical services, coupled with poor financial conditions and limited English proficiency, which are common barriers to accessing medical care for the immigrant population, have a negative impact on the quality of life and poor health status of Mexicans in the United States.
Given this outlook, and in response to needs, in 2001, a collaborative project was implemented between Mexico and the United States called Binational Health Week (BHW). This annual event takes place in October when health is promoted and access to various medical services and prevention activities is facilitated (2).
Based on the experience of the BHW, and as a result of pressure from community leaders and local organizations requesting the continuity of the services provided, in 2003, the Ventanillas de Salud (VDS) strategy was implemented as a pilot project in the Mexican Consulates in San Diego and Los Angeles, California, with the support of the United States-Mexico Border Health Commission (USMCB), the United States-Mexico Health Initiative (currently the Health Initiative of the Americas), the University of California and The California Endowment [(3), p. 19]. In 2004, the VDS strategy was formalized and extended to other consulates. Subsequently, in 2016, as part of a strategy to strengthen the VDS, the Mexican Section of the United States-Mexico Border Health Commission implemented the Mobile Health Units (MHU) care model (4).
The VDS strategy and the MHU care model are designed to facilitate access to health services and contribute to fostering a culture of self-care among the Mexican population living in the United States, and to promote disease prevention and control [(4), p. 7–14]. However, even though the programmatic goal of VDS is to serve the Mexican population living in the United States, VDS also served other Hispanic populations living in the same communities. Therefore, we use the term “Hispanic” throughout this article to refer to the population served.
Secondary data sources with lack of personally identifiable information were reviewed. First, the database of the Current Population Survey 2020 (1) of the United States Census Bureau, which contains a representative sample of the Hispanic community in the United States, was analyzed to determine the typical characteristics of the population (5).
The database of the System of Continuous Information and Health Reports of Mexicans in the United States (SICRESAL-MX) was consulted. This technological tool was developed by the Mexican Section of the USMBHC, which has a record of the people served, and preventive services provided by both the VDS and the MHU. This document includes the analysis of 6.4 million records of people who received twenty million services during the period from 2019–2021. The analysis was descriptive, based on simple frequencies, and cross-referenced basic sociodemographic variables.
No personally identifiable information was included in the analysis thereby avoiding the need for the participation of human subjects and the approval of ethics committees.
Ventanillas de Salud (VDS) is a Mexican Government Strategy, undertaken by the Ministry of Health (SS) and the Ministry of Foreign Affairs (SRE), through the Institute of Mexicans Abroad (IME). It is implemented in the Mexican Consular Network in the United States and operated by local agencies, with the support of strategic allies in that country, such as government organizations, civil society and private organizations and academic institutions (6).
The mission of VDS is to improve access to basic and preventive health services, increase public health insurance coverage, and establish a medical home, through counseling, education, timely detection, and referrals to quality health facilities, in a safe environment. Fifty-one VDS currently operate in the Mexican consular network in the US, as shown in Map 1.
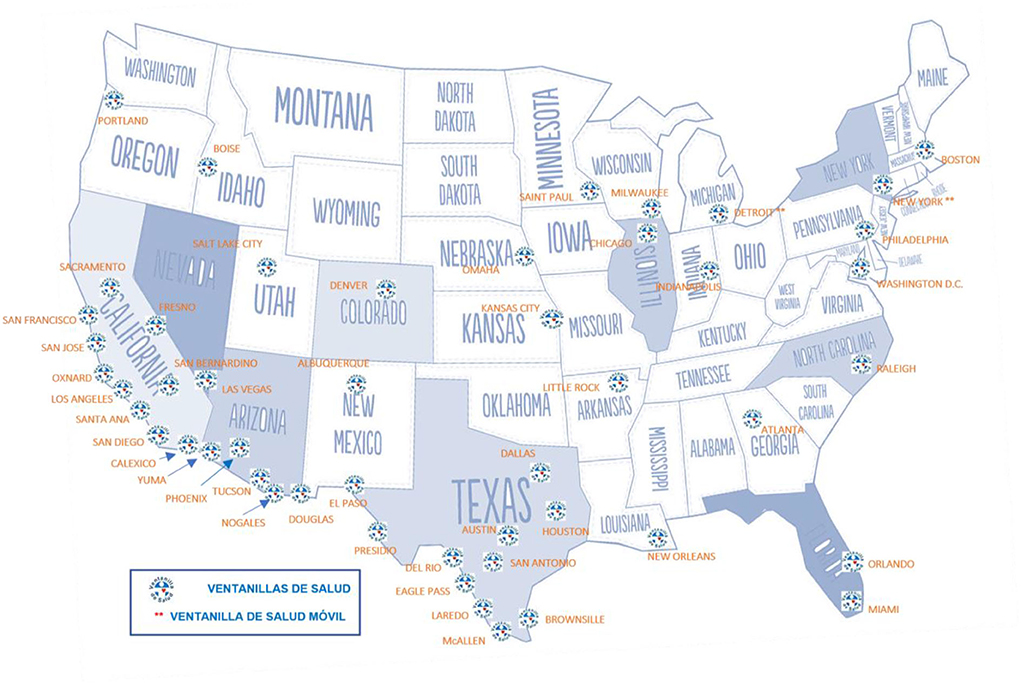
Map 1. Geographical location of Ventanillas de Salud in the United States. Source: Mexican section of the Mexico-United States Border Health Commission, 2020.
VDS serves Hispanics in a situation of vulnerability who live in the United States, by promoting a sense of responsibility to improve their own health and quality of life and the acquisition of accurate health-related information. VDS facilitates access to preventive health services and fosters a culture of self-care, including active participation in health matters.
VDS has the following characteristics:
1) Services are based on the conditions that most affect the Mexican population;
2) By focusing on the individual needs of each user, they create a relationship of trust and empathy with the population served;
3) They have specialized, culturally appropriate materials to provide information in the source language;
4) They are operated by personnel trained in disease prevention and control and provide resources and options for access to health services in collaboration with community health centers and institutions, and
5) They work to improve the physical and mental health conditions of the Mexican population in the United States, and to maintain a healthy environment based on local and binational collaboration [(4), p. 8].
To fulfill its mission, VDS has over six hundred allies which include health institutions such as hospitals and federal health centers, community clinics, government organizations and educational institutions, which contribute to providing screening services, delivery of printed educational material, and help with navigating the health system in the United States, among others. These collaborative partners comprise a broad and valuable network that provides comprehensive preventive health services including health education, screening, and referrals.
To strengthen the VDS, the Mobile Health Units's (MHU) care model was created to provide preventive health services to remote communities with difficult access to health services. Eleven MHU currently operate in cities with a large concentration of Hispanic populations: Chicago, Dallas, Denver, Las Vegas, Los Angeles, Miami, New York, Orlando, Phoenix, Raleigh, and Tucson (Map 2).
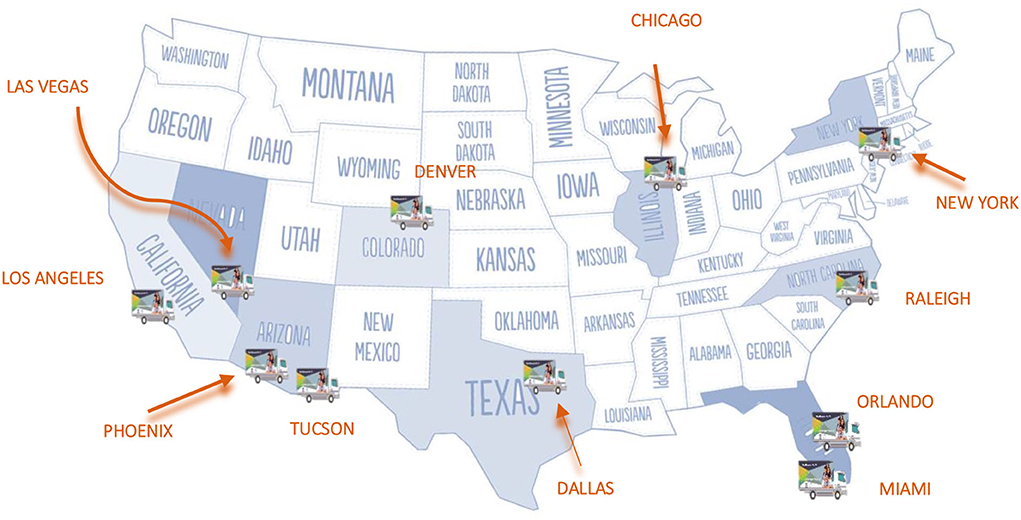
Map 2. Geographical location of Mobile Health Units in the United States. Source: Mexican section of the Mexico-United States Border Health Commission, 2020.
The VDS strategy was initiated in response to the success of the Binational Health Week and its acceptance by the community. During this event, preventive and health promotion services are offered annually to Hispanics who typically experience barriers to accessing such services in the United States. Such improved access and acceptance led community leaders and local organizations to request long term continuity of these services. In 2003, the VDS strategy was implemented as a pilot project at the Mexican Consulates in San Diego and Los Angeles, California, with the support of the United States-Mexico Border Health Commission and the United States-Mexico Health initiative (known as the Health Initiative of the Americas), from the University of California and The California Endowment. In 2004, the VDS strategy was formally launched and extended to other consulates. With the aim of strengthening and expanding the coverage of preventive health services for the Mexican community in the United States to remote communities unable to access health services, in 2016, the first phase of the MHU care model was implemented in Dallas, Los Angeles, New York, Phoenix and Chicago. Its services were subsequently extended to Denver, Las Vegas, Raleigh, Orlando, Miami, and Tucson (7).
The VDS strategy is an example of government and institutional collaboration with strategic allies in Mexico and the United States. The resources, both monetary and in kind, required to provide basic preventive services, are contributed by the following actors:
- Mexican goverment
• Seed money
• Institutional collaboration
- Consular network
• Space on their premises
• Technology and support office
• Alliances
• Training
- Lead agencies
• Manage and operate the VDS
• Select and hire staff
• Generate intervention projects
• Organize fairs and events
- Network of associated agencies
• Provide specialied personnel
• Perform screening tests and administration fof vaccines
• Carry out workshops and deliver educational materials and workshops
• Participate in health fairs and training
The VDS strategy has an advisory board comprised of nine members, including leaders in the health and migrant assistance sectors, who represent different sectors: government, academia, the non-government sector, and international organizations, from Mexico and the United States. The purpose of the Advisory Board is to provide advice on management, innovation, and binational managerial strengthening processes with the various sectors to improve strategy (8).
In general, VDS and MHU focus on conditions with the highest incidence rates among the Mexican population living in the United States, grouping services into five categories:
1) Counseling on prevention and health promotion issues through advice on priority health issues, such as nutrition, obesity, diabetes, women's health, child health, mental health, addictions, HIV/AIDS, and access to services, among others.
2) Timely detection of various ailments, using measurements such as body mass index, cholesterol and glucose tests, and HIV/AIDS and COVID-19 tests.
3) Referrals to health services available in their locality (community clinics), related to cultural and language particularities, to receive medical care if necessary and/or establish a medical home.
4) Administration of flu and COVID-19 vaccines and for other illnesses.
5) Advice on health insurance alternatives in the United States.
Activities undertaken by VDS and MHU are based on training health promoters in priority health issues to strengthen their skills and provide comprehensive preventive health services for users (9). During 2020 and the first semester of 2021, various training sessions and webinars were held whose main topics were COVID-19 and mental health.
In addition, these activities were supported using culturally adapted educational materials in Spanish focusing on health promotion and disease prevention. Between 2020 and the first semester of 2021, technical content was developed on various priority health topics (such as healthy lifestyle; chronic-degenerative diseases; health promotion; sexual and reproductive health; child health; mental health and COVID-19), which subsequently allowed the design of 301 educational materials. The material is disseminated in community events and through social media networks: Facebook, Twitter, Instagram, YouTube, and the VDS strategy website.
Likewise, in 2018, the Mexican Section of USMBHC launched the mental health initiative. In collaboration with the Pan American Health Organization (PAHO), it implemented training in the Mental Health Gap Action Programme (mhGAP) Intervention Guide designed to help health personnel and community health workers (promotores de salud) reduce gaps in mental health. The training covers issues such as risk factors and warning signs of mental illness and information on depression, anxiety, trauma, and psychosis either to help a person cope with the mental health problem and/or to refer them in a timely manner to professional help [(10), p. 14].
SICRESAL-MX, the data collection system previously described in the methods section, is the official mechanism for registering users of VDS and MHU services and for generating real-time quantitative data describing the sociodemographic and health conditions of users and the VDS and MHU services received by users. The database is a rich source of information with about 283 variables. Its importance lies in the fact that the capture of such data through the registration process enables its analysis through descriptive statistics for decision-making and the strengthening of preventive health services.
The VDS strategy has met the needs of their users by providing comprehensive health services through culturally adapted preventive health promotion actions, by contributing to disease control, and preventing the use of emergency service through timely detection.
The MHU care model has taken these services to remote communities that are unable to access health services, thus, reaching a sector of a vulnerable community and broadening the scope of services.
According to data from SICRESAL-MX, between 2019 and 2021, the VDS and MHU served approximately 6.4 million people and provided 20.7 million services, of which 88.2% corresponded to counseling or advice, 8.1% to screening, 3.1% to vaccination services, 0.2% to information on other issues, and 0.1% to referrals. Tables 1, 2 shows the disaggregation of services and people served by type of strategy, year, and service.
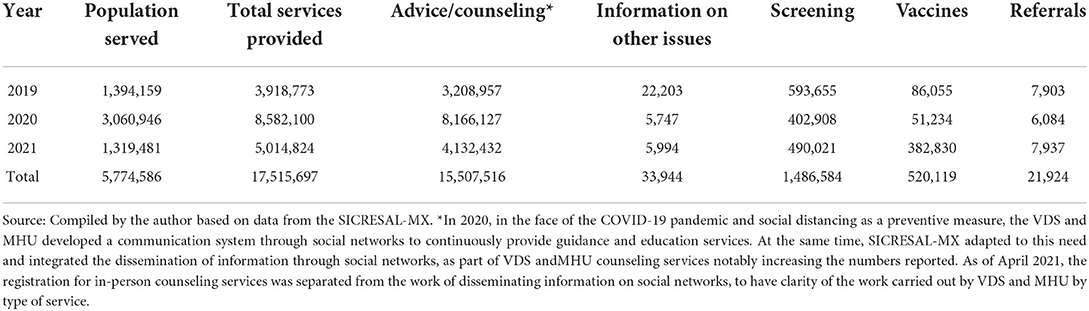
Table 1. Population served and services provided at VDS, January 2019—December 2021.

Table 2. Population served and services provided in MHU, January 2019—December 2021.
This level of care has achieved a favorable impact on the health of Hispanic VDS service community in the United States by offering preventive services that enable identifying ailments and raising health issue awareness. In addition, it contributes to disease control and prevents the use of emergency services through timely detection, service availability advice, and aiding in the establishment of a medical home. Likewise, because of the COVID-19 pandemic, services were expanded to adapt to the new context.
Of those receiving screening services for specific conditions at the VDS and MHU, the most important data are presented below (Table 3):
• Glucose screening showed that two out of every 10 people screened at VDS and three out of 10 at MHU displayed high levels.
• An alarming piece of data is that around three-quarters of people screened in VDS and MHU have overweight and obesity problems, especially men.
• In general, three out of 10 users attended VDS and MHU had high cholesterol levels. Once again, a higher percentage of men experienced this condition compared with women, especially among those who attended VDS.
• While six of every 10 persons had high blood pressure, women experienced a higher prevalence than men.
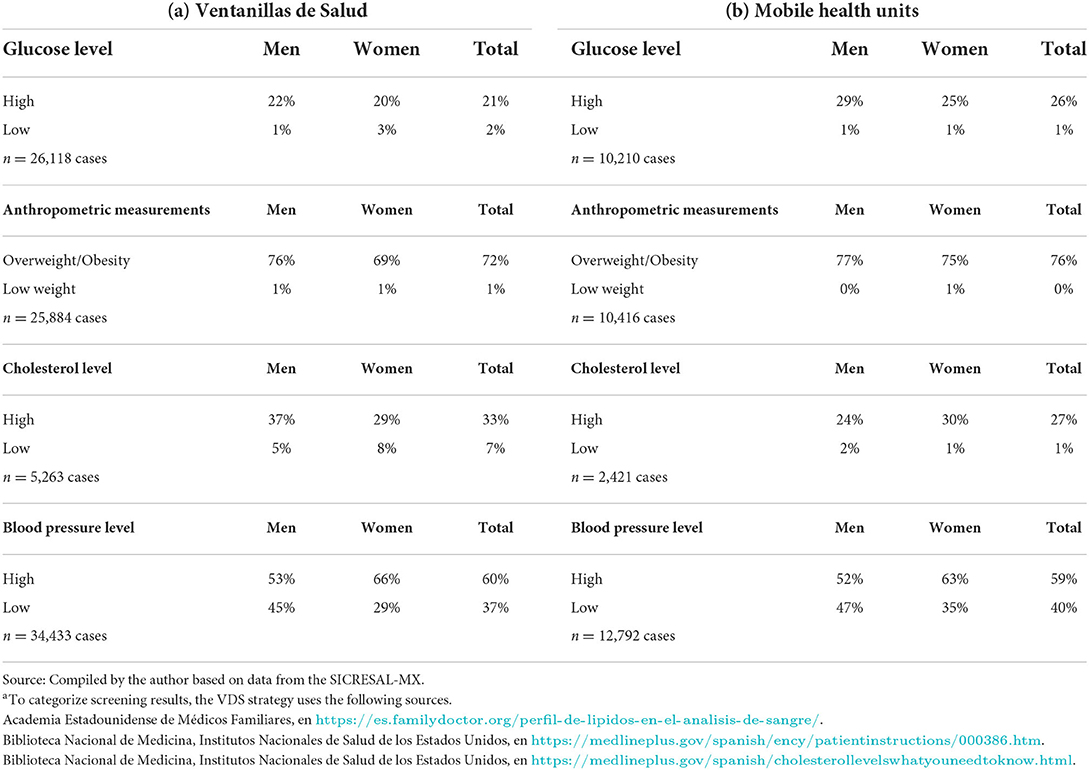
Table 3. Percentage distribution of results of anthropometric measurement and glucose, cholesterol, and blood pressure tests, of the population served at VDS and MHU, by sex and type of strategy, January 2019—December 2021a.
During the period of analysis (2019–2021), data from the SICRESAL-MX related to family history of illness of 41,000 people receiving either VDS and/or MHU services showed that 55% have a family history of diabetes and 20% have a family history of obesity. In addition, 452 mental health screenings were performed during this period indicating the prevalence of the following: depression (40%), anxiety (16%), psychosis (14%), violence (8%), sexual problems (8%), and other more rare conditions (14%).
During the period of analysis, just over 154,000 people were served at VDS and MHU and provided information on their medical coverage (Table 4). These data show that in general this is a highly vulnerable population since 94% lack any type of health coverage, and more so among VDS (96%) than MHU users (85%). Moreover, when separated by age group, people aged 65 or over have the highest percentage of medical coverage, especially among MHU users.
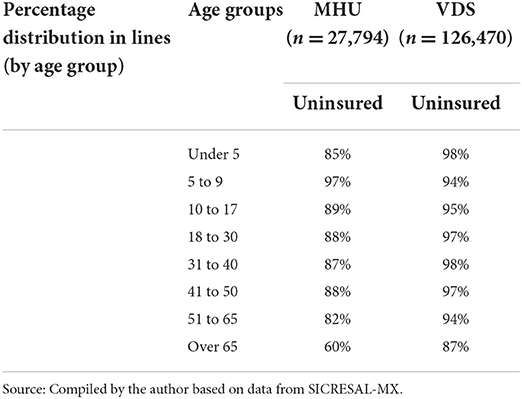
Table 4. Percentage distribution (in lines and columns) of population served at VDS and MHU by age group and medical insurance status, January 2019—December 2021.
The services provided by VDS and MHU in the United States are crucial for several reasons:
First, there is a large and growing size of Hispanic population living in the United States. According to data from the most recent Census conducted in 2020, the total Hispanic population living in the United States amounted to 62.1 million, of whom approximately 62% were of Mexican origin (38.5 million people).
Second, it addresses the predominant characteristics that act as barriers to medical care among this population such as their economic status, limited command of the English language, and limited access to health services that result in them suffering from poorer health.
Third, the VDS and MHU address conditions that stem from a history of chronic-degenerative illnesses and diseases among the Mexican population, such as obesity, diabetes, and hypertension, documented both in Mexico, through the National Survey of Health and Nutrition (11), and the United States through the National Health Interview Survey (12).
Fourth, in recent years mental health has become a major concern in offering preventive and holistic care and giving it the same level of care as physical health problems receive. VDS and MHU began an initiative to approach healthcare among Mexicans in the United States to detect mental health signs and symptoms, and to refer them to access local or online services.
Fifth in the face of the COVID-19 pandemic, VDS and MHU adapted its services and system and type of care offered to continue providing in person preventive services, such as administering vaccines, also, providing remote services, showing their ability to adapt and respond to emerging needs.
Given these characteristics and based on the results of the quantitative analysis, both VDS and MHU are considered successful models in managing to detect the specific needs of their users and adapting to the context where they are implemented. They have also been strengthened over the years, thanks to their network of strategic allies in each consular district, which in turn manifests their perseverance, coordination, and institutional commitment.
VDS and MHU have proven to be an important model of collaboration. Through alliances with institutions from different sectors, VDS and MHU have managed to direct outreach to a vulnerable sector of the Hispanic population to reduce the gap in access to health services. It is a unique care model, serving co-nationals in another country, contributing not only to the benefit of the health and wellness of Mexicans in the United States, but also to the health and wellness of other neighboring Hispanics.
The ability of the VDS/MHU to effectively organize and manage health outreach services and to connect clients to these services, particularly in the area of COVID-19 and mental health, is a testament to the strength of its diverse network of collaborators in Mexico and the United States.
In conclusion, we would like to suggest the following actions to strengthen the VDS and MHU services and ensure the continuity of the strategy. First, VDS and MHU should identify and formalize collaborations with strategic allies to promote the supply and distribution of the COVID-19 vaccine and others vaccines to the neediest and most vulnerable migrant communities. Second, it is also important to strengthen the mental health module. The relevancy of this module was highlighted by the COVID-19 pandemic and the detrimental impact on mental health related to social distancing and sheltering in place. Third, the VDS and MHU requires greater dissemination of the work carried out to strengthen their actions and give continuity to the strategy.
The VDS strategy has been instrumental in providing much needed health-related preventive services to hard-to-reach populations and communities which they would otherwise have been unable to obtain.
The datasets generated for this study are available on reasonable request to the corresponding author.
IL and SS first draft and data analysis. MR, AL, AR, MC, LG, and CR revision and final draft. All authors contributed to the article and approved the submitted version.
Initial funding for the project provided by the Mexican Government.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer KD declared a past co-authorship with the authors MG and CR to the handling editor.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. US Census Bureau,. Current Population Survey Annual Social Economic (ASEC) Supplement. (2020). Available online at: https://www.census.gov/programs-surveys/cps.html (accessed June 15, 2022).
2. Instituto de los Mexicanos en el Exterior. Semana Binacional de Salud (2016). Available online at: https://www.gob.mx/ime/acciones-y-programas/semana-binacional-de-salud-60728 (accessed June 15, 2022).
4. Secretaría de Salud. Estrategia Ventanillas de Salud. Secretaria de Salud, Secretaría de Relaciones Exteriores, Instituto de los Mexicanos en el Exterior, Comisión de Salud Fronteriza México-Estados Unidos. (2018). p. 28.
5. US Census Burea,. La Oficina del Censo publica estimaciones del conteo del 2020, comunicado de prensa. (2022). Available at https://www.census.gov/newsroom/press-releases/2022/2020-census-estimates-of-undercount-and-overcount/2020-census-estimates-of-undercount-and-overcount-spanish.html (accessed June 15, 2022).
6. VDS, strategy web page: https://ventanillasdesaludums.org/
7. Rangel Gomez MG, Tonda J, Zapata GR, Flynn M, Gany F, Lara J, et al. Ventanillas de Salud: a collaborative and binational health access and preventive care program. Front Public Health. (2017) 5:151. doi: 10.3389/fpubh.2017.00151
8. Rangel Gómez MG, López Jaramillo AM, Svarch A, Tonda J, Lara J, Anderson EJ, et al. Together for health: an initiative to access health services for the hispanic/mexican population living in the United States. Front Public Health. (2019) 7:273. doi: 10.3389/fpubh.2019.00273
9. Rangel G, Rogelio Z, Eduardo G, Josana T, Patricia C. Ventanillas de Salud: Un Programa que Busca Mejorar las Condiciones de Salud de los Migrantes Mexicanos que Viven en Estados Unidos. In: Migración y Salud Perspectivas sobre la Población Migrante, Secretaría de Gobernación/CONAPO. (2016). pp. 95–102.
10. Secretaría de Salud. Informe Ejecutivo. Estrategia Ventanillas de Salud. Resultados 2020 y proyectos estratégicos 2020-junio 2021. Secretaria de Salud, Secretaría de Relaciones Exteriores, Instituto de los Mexicanos en el Exterior, Comisión de Salud Fronteriza México-Estados Unidos. (2021). p. 58.
11. INEGI-INSP. Encuesta Nacional de Salud y Nutrición 2018 (ENSANUT), Presentación de Resultados. (2019). Available online at: https://ensanut.insp.mx/encuestas/ensanut2018/doctos/informes/ensanut_2018_presentacion_resultados.pdf (accessed June 15, 2022).
12. National Center for Health Statistics. National Health Interview Survey, published by Centers for Disease Control and Prevention (CDC), U.S Department of Health and Human, 2018, databased. (2019). Available online at: https://www.cdc.gov/nchs/nhis/ (accessed June 1, 2020).
Keywords: migration, health, Ventanillas de Salud, Mobile Health Units, binational collaboration
Citation: Rangel Gómez MG, Salazar S, López Jaramillo AM, Lira Chávez IA, Romero Rangel A, Caballero Abraham ML, Gutiérrez Reyes L and Rosales CB (2022) Ventanillas de Salud (VDS) and Mobile Health Units (MHU): A binational collaborative models. Front. Public Health 10:976941. doi: 10.3389/fpubh.2022.976941
Received: 23 June 2022; Accepted: 10 October 2022;
Published: 09 November 2022.
Edited by:
Christiane Stock, Charité Medical University of Berlin, GermanyReviewed by:
Pietra Check, Tufts University, United StatesCopyright © 2022 Rangel Gómez, Salazar, López Jaramillo, Lira Chávez, Romero Rangel, Caballero Abraham, Gutiérrez Reyes and Rosales. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Gudelia Rangel Gómez, Z3JhbmdlbDIwMDlAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.