 Prince A. Adu1,2
Prince A. Adu1,2 Sarafa A. Iyaniwura1,3Bushra Mahmood4
Sarafa A. Iyaniwura1,3Bushra Mahmood4 Dahn Jeong1,2Jean Damascene Makuza1,2
Dahn Jeong1,2Jean Damascene Makuza1,2 Georgine Cua1,2Mawuena Binka1,2Héctor A. Velásquez García1,2
Georgine Cua1,2Mawuena Binka1,2Héctor A. Velásquez García1,2 Notice Ringa1,2Stanley Wong1Amanda Yu1Mike A. Irvine1
Notice Ringa1,2Stanley Wong1Amanda Yu1Mike A. Irvine1 Michael Otterstatter1,2Naveed Z. Janjua1,2,5*
Michael Otterstatter1,2Naveed Z. Janjua1,2,5*- 1British Columbia Centre for Disease Control, Vancouver, BC, Canada
- 2School of Population and Public Health, University of British Columbia, Vancouver, BC, Canada
- 3Department of Mathematics, University of British Columbia, Vancouver, BC, Canada
- 4Department of Medicine, University of British Columbia, Vancouver, BC, Canada
- 5Centre for Health Evaluation & Outcome Sciences, St. Paul's Hospital, Vancouver, BC, Canada
Background: Vaccine hesitancy threatens efforts to bring the coronavirus disease 2019 (COVID-19) pandemic to an end. Given that social or interpersonal contact is an important driver for COVID-19 transmission, understanding the relationship between contact rates and vaccine hesitancy may help identify appropriate targets for strategic intervention. The purpose of this study was to assess the association between interpersonal contact and COVID-19 vaccine hesitancy among a sample of unvaccinated adults in the Canadian province of British Columbia (BC).
Methods: Unvaccinated individuals participating in the BC COVID-19 Population Mixing Patterns Survey (BC-Mix) were asked to indicate their level of agreement to the statement, “I plan to get the COVID-19 vaccine.” Multivariable multinomial logistic regression was used to assess the association between self-reported interpersonal contact and vaccine hesitancy, adjusting for age, sex, ethnicity, educational attainment, occupation, household size and region of residence. All analyses incorporated survey sampling weights based on age, sex, geography, and ethnicity.
Results: Results were based on survey responses collected between March 8, 2021 and December 6, 2021, by a total of 4,515 adults aged 18 years and older. Overall, 56.7% of respondents reported that they were willing to get the COVID-19 vaccine, 27.0% were unwilling and 16.3% were undecided. We found a dose-response association between interpersonal contact and vaccine hesitancy. Compared to individuals in the lowest quartile (least contact), those in the fourth quartile (highest contact), third quartile and second quartile groups were more likely to be vaccine hesitant, with adjusted odd ratios (aORs) of 2.85 (95% CI: 2.02, 4.00), 1.91(95% CI: 1.38, 2.64), 1.78 (95% CI: 1.13, 2.82), respectively.
Conclusion: Study findings show that among unvaccinated people in BC, vaccine hesitancy is greater among those who have high contact rates, and hence potentially at higher risk of acquiring and transmitting infection. This may also impact future uptake of booster doses.
Introduction
The Coronavirus Disease 2019 (COVID-19) pandemic continues to have adverse social, economic and health impact on societies across the globe. As of August 7, 2022, over 580 million confirmed cases of (COVID-19), have been reported globally, with over 6.4 million deaths (1). The availability of approved safe and effective COVID-19 vaccines offered hope and optimism to end the COVID-19 pandemic, and a potential way to return to pre-pandemic normalcy, even though the emergence of new severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants presents new challenges. Current data indicates high effectiveness of the COVID-19 vaccines against infection, transmission, severe disease, and death (2–6).
However, the potential population-level reduction in transmission, morbidity, and mortality due to COVID-19 ultimately depends on high vaccine uptake which is in turn threatened by vaccine hesitancy, a complex and context specific behavior defined as “the delay in acceptance or refusal of vaccines despite availability of vaccination services” (7). In fact, due to the recent global resurgence of highly infectious vaccine-preventable diseases such as measles, the World Health Organization (WHO) named vaccine hesitancy as one of the ten greatest threats to global health in 2019 (8). Varying degrees of COVID-19 vaccine hesitancy have been reported across the world. In Bangladesh, two cross sectional studies showed vaccine hesitancy of 32.5% (9) and 27.4% (10). A recent scoping review of COVID-19 vaccine hesitancy in Africa showed vaccine acceptance ranged from 6.9 to 97.9% (11). A systematic review of COVID-19 vaccine hesitancy in the U.S revealed vaccine acceptance rate ranging from 12 to 91.4% (12).
As of July, 2022, the following COVID-19 vaccines had received authorization for use in Canada from Health Canada: Pfizer-BioNTech Cominarty, Moderna Spikevax, AstraZeneca Vaxzevria, Janssen (Johnson & Johnson), Novavax Nuvaxovid and Medicago Covifenz (13, 14). In British Columbia (BC), Pfizer-BioNTech Cominarty and Moderna Spikevax COVID-19 vaccine were the first to receive authorization for use on September 16, 2021, according to the British Columbia Centre for Disease Control (14). A study by Statistics Canada conducted in March/April 2021 indicated that 88% of Canadians aged 12 and older were willing to get vaccinated for COVID-19 when a vaccine is available to them or have already received one dose of the vaccine (15). Ogilvie et al. (16) also reported a 79.8% COVID-19 vaccine acceptance rate among the general population of British Columbia, Canada.
Some factors associated with COVID-19 vaccine hesitancy include age, gender, chronic medical condition, fears about COVID-19, income, employment status, ethnicity, location of residence, religion, marital status, educational level etc., (17). As individuals with high interpersonal or social contacts may have a higher risk of COVID-19 transmission, vaccine uptake among this population is critical to curbing the spread of COVID-19. Although COVID-19 vaccine uptake and interpersonal contact have been investigated independently in light of their association with COVID-19 transmission, we are not aware of any study that has examined the relationship between these two important factors that affect COVID-19 transmission dynamics. Hence, the purpose of this study was to evaluate the association between interpersonal contact rate and COVID-19 vaccine hesitancy.
Methods
This study used data from the BC COVID-19 Population Mixing Patterns Survey (BC-Mix), a repeated online survey developed to assess population mixing patterns in BC during the COVID-19 pandemic. The ongoing survey was launched in September 2020 and is open to all BC residents aged 18 years or older. Anonymous links to the survey are circulated via advertisements placed on social media platforms (including Facebook, Instagram, YouTube and Twitter), on flyers distributed at grocery stores, community centers and places of worship, including those frequented by ethnic minority groups. Suspected duplicate responses are removed prior to analyses. Also, survey responses that do not have completion rate of at least 33%, and valid non-missing responses for the sex and age questions are excluded for weighting and further analyses. Using the 2016 Census data (18) as reference, the survey data is weighted with the following auxiliary variables: age, sex, geography, and ethnicity, using the weighting adjustment technique (19). As of June 2022, more than 88,000 individuals had participated in the survey. Further details about the survey development, design and domains are described in detail elsewhere (20–22). We followed the checklist for Reporting Results of Internet E-Surveys (CHERRIES) (23). The domain on vaccine hesitancy was added to the survey on March 8, 2021.
Measures
To assess vaccine hesitancy, participants were asked whether they had received any of the approved COVID-19 vaccines. Individuals who answered that they had not yet received the COVID-19 vaccine at the time of the survey were asked to indicate their level of agreement with the statement, “I plan to get the COVID-19 vaccine.” Responses were rated on a five-point scale ranging from 1 to 5, with 1 being “Strongly disagree” and 5 being “Strongly agree.” For the purposes of analyses, the responses were recoded, with those who responded, “Strongly Disagree” or “Disagree” coded as “unwilling to receive COVID-19 vaccine or vaccine hesitant” and those who responded “Agree” and “Strongly Agree” coded as “willing to receive a COVID-19 vaccine.” Individuals who chose “Neutral” were considered “undecided.”
Interpersonal contact was assessed by the number of in-person, face-to-face contacts that a participant had within the past 24 h. The number of contacts was categorized by quartiles.
We assessed age, sex, ethnicity, educational attainment, occupation, household size, employment status and health region of participants (24), based on self-reported data from survey questions. The literature guided our choice of these characteristics as confounders in our assessment of the association between interpersonal contact and vaccine hesitancy.
Additional variables such as material and social deprivation index were derived using census and location data (25). Further details (including definitions and response categories) on all the survey questions relevant to this study are provided in Supplementary Table 1 of the Supplementary material.
Analyses
Participant characteristics were summarized using weighted frequencies and percentages and are presented in Table 1. Survey methodology and weighting technique have been described elsewhere (20). Characteristics of study participants were stratified by contact rate (Table 2) and also by COVID-19 vaccine hesitancy (Table 3).
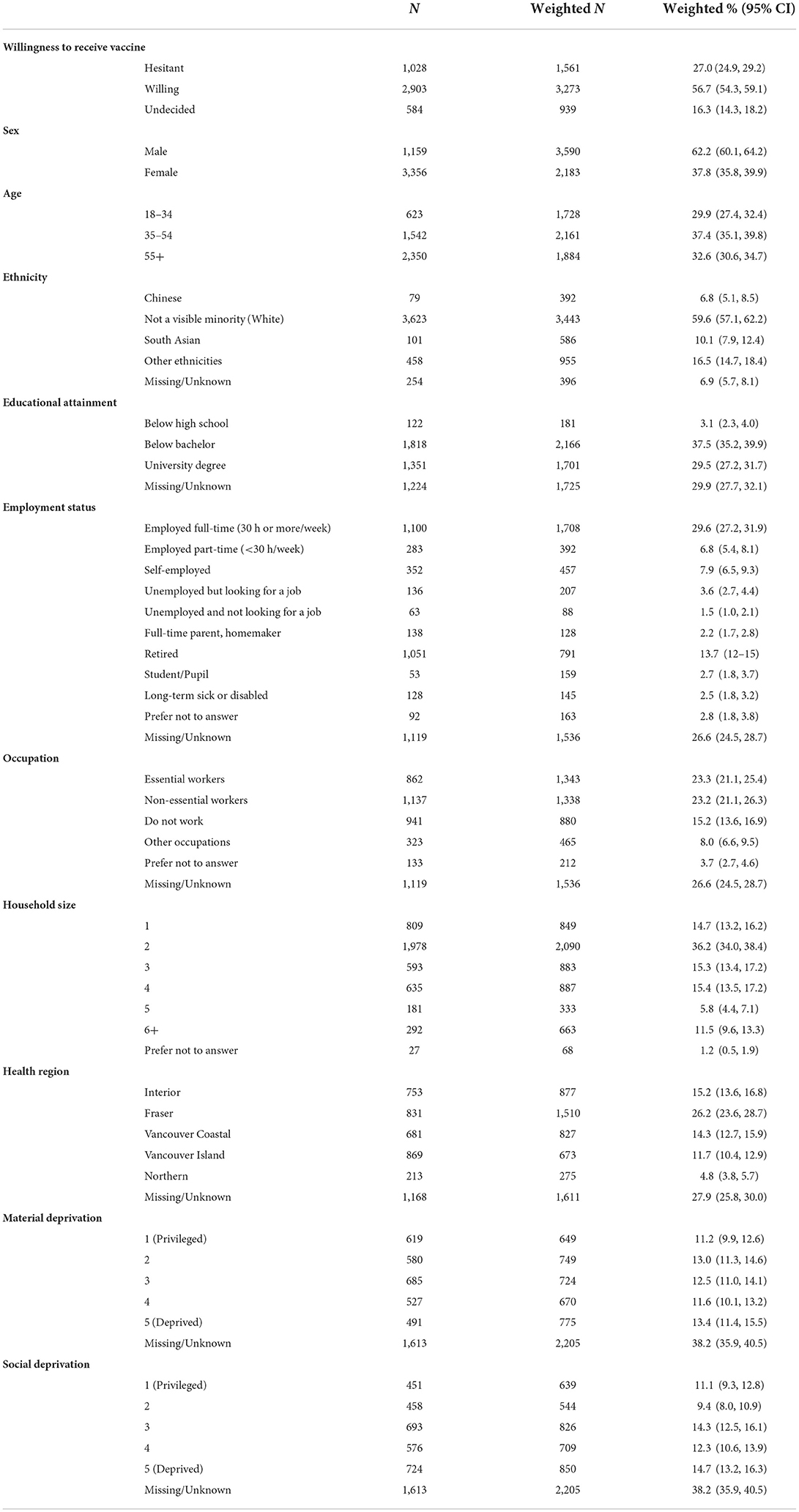
Table 1. Characteristics of study participants (unweighted N = 4,515), March 8, 2021-December 6, 2021.
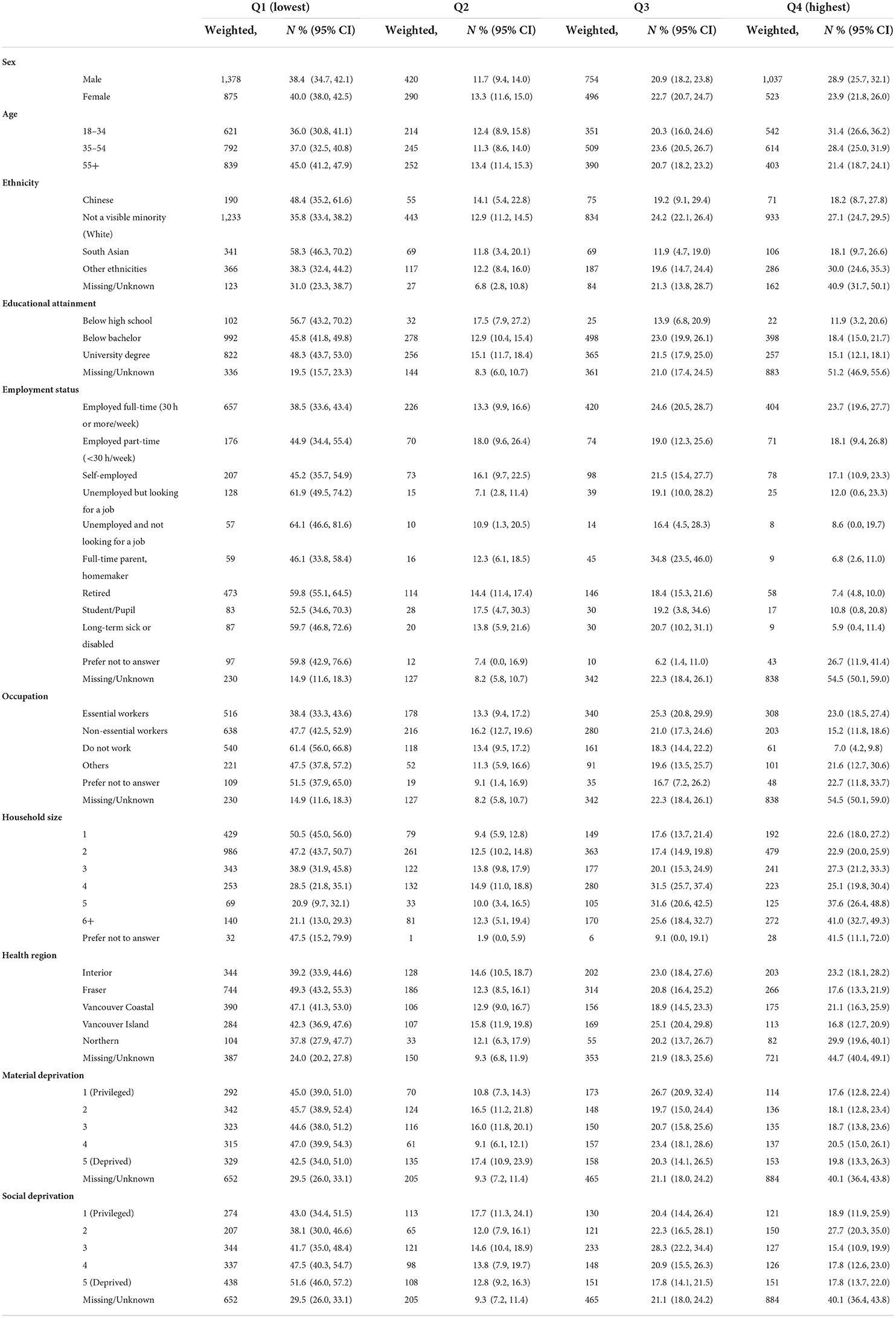
Table 2. Characteristics of study participants by interpersonal contact (unweighted, N = 4,515), March 8, 2021- December 6, 2021.
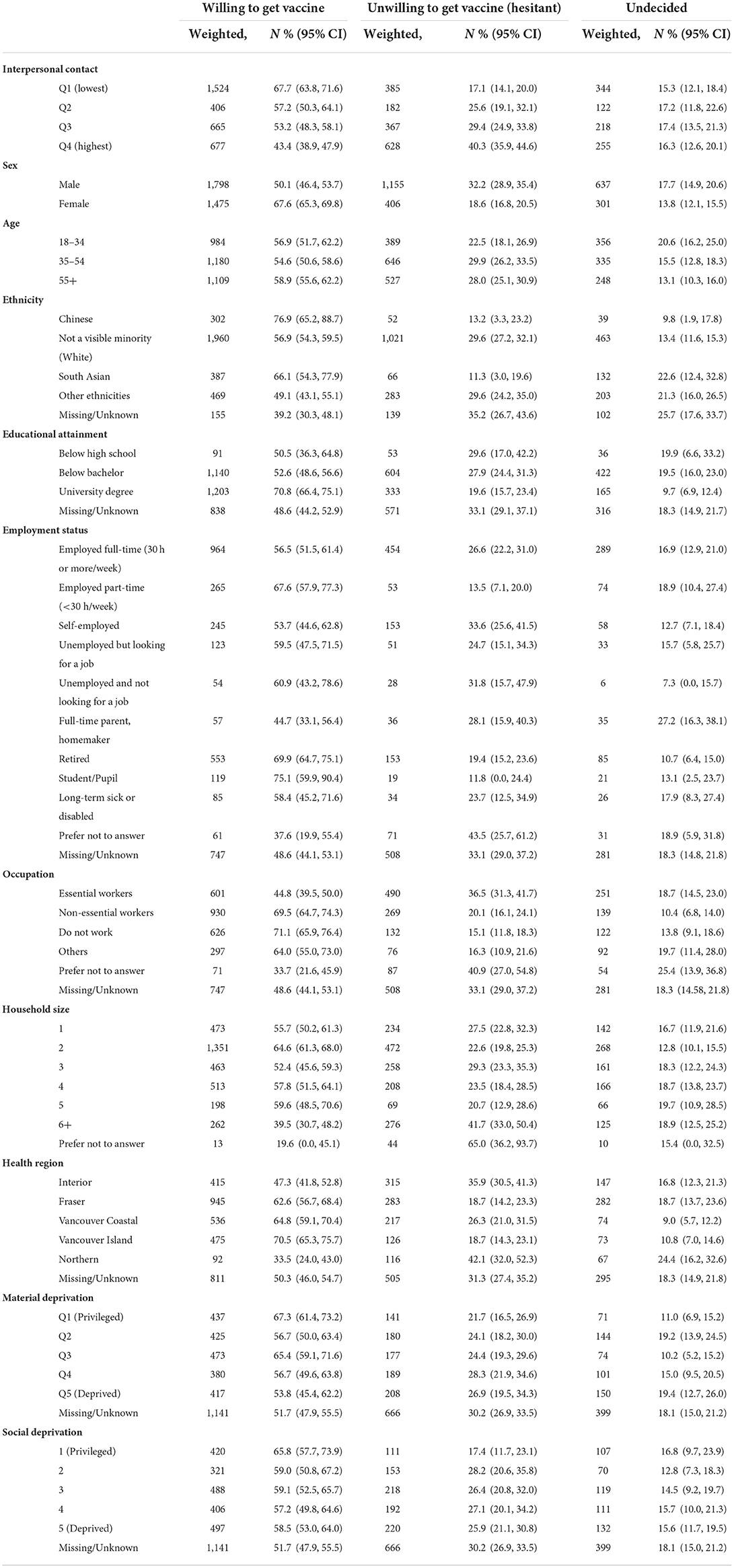
Table 3. Characteristics of study participants by vaccine hesitancy (unweighted, N = 4,515), March 8, 2021-December 6, 2021.
We investigated the association between interpersonal contact (primary exposure) and COVID-19 vaccine hesitancy (outcome measure) while accounting for demographic and other variables using multivariable multinomial logistic regression (Table 4). In a sensitivity analysis, we repeated this analysis but for the outcome variable, we considered those who had already received the vaccine as willing to receive it (Supplementary Tables 2, 3 of the Supplementary material).
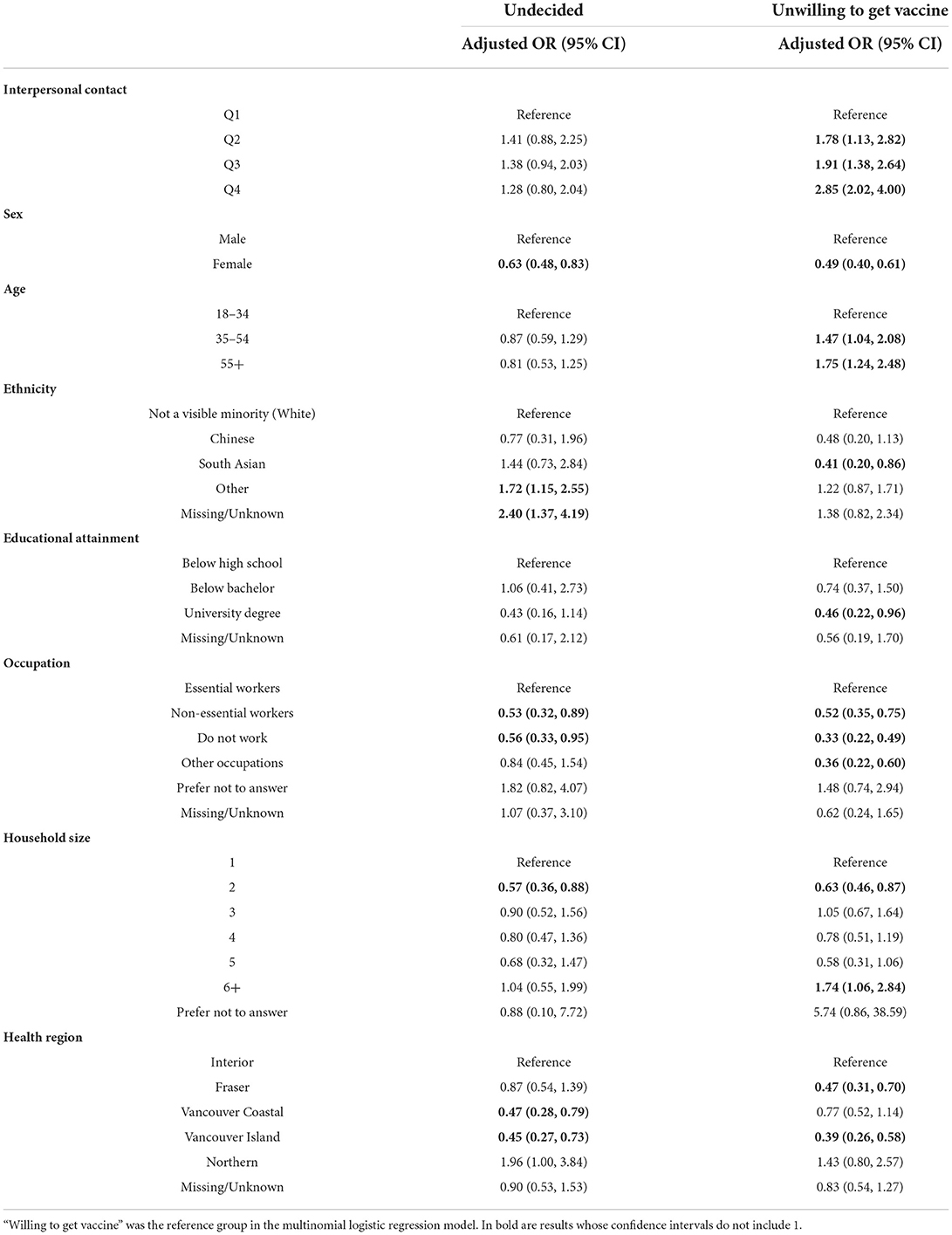
Table 4. Multivariable multinomial logistic regression model for association between interpersonal contact and vaccine hesitancy, March 8, 2021-December 6, 2021.
All analyses incorporated survey sampling weights that were estimated based on age, sex, geography (region), and ethnicity distribution as described elsewhere (20). All tests were two-sided significant at the 0.05 level. Analyses were performed in SAS software version 9.4 (26).
Ethics approval
Informed consent was obtained from all participants. Ethical approval for this study was provided by the University of British Columbia Behavioral Research Ethics Board (No: H20-01785).
Results
Participant characteristics (overall)
Out of 15,796 respondents completing the survey between March 8 and December 6, 2021, 11,127 (70.4%) had received COVID-19 vaccine and 154 (1.0%) had missing/non-valid responses, so were ineligible for analysis, leaving 4,515 (28.6%) eligible records for analysis (i.e., people who had not yet been vaccinated and who provided valid responses to the willingness to get vaccinated question). The results presented here are based on weighted survey responses from these 4,515 responses.
The majority of participants were male (62.2%), between 35 and 54 years old (37.4%), identified as White (59.6%), had a full-time employment (29.6%), and lived with one other person in their household (36.2%). The Fraser Health region contributed the largest number of participants (26.2%). Also, 37.5% of respondents had below bachelor's education, while 29.5% had a University degree (Table 1).
Overall, 56.7% of respondents reported that they were willing to get the COVID-19 vaccine, 27.0% were unwilling (vaccine hesitant) and 16.3% were undecided about getting the COVID-19 vaccine (Table 1). However, when people who had already received the vaccine were included with those who said were willing to receive the vaccine, the proportion willing to get the vaccine was 86.5% (Supplementary Table 2 in the Supplementary material).
Participant characteristics by interpersonal contact
Characteristics of study participants by interpersonal contact are summarized in Table 2. Whereas, 28.9% of contacts made by males were in the highest quartile, only 23.9% of contacts made by females were in the highest quartile of interpersonal contacts. Among the 18–34 years age group, 31.4% of contacts were in the highest quartile, compared to 28.4 and 21.4% in the highest quartile among the 35–54 and ≥55 years age groups, respectively. Whereas, 23.0% of contacts made by essential workers were in the highest quartile, only 15.2% of contacts made by non-essential workers were in the highest quartile of interpersonal contacts distribution.
Participant characteristics by vaccine hesitancy
The characteristics of study participants by vaccine hesitancy are presented in Table 3. Among individuals with the least interpersonal contacts, only 17.1% were vaccine hesitant compared to 40.3% among those with the highest interpersonal contact. Whereas, 32.2% of males were vaccine hesitant, only 18.6% of females were deemed vaccine hesitant. Also, 36.5% of essential workers were vaccine hesitant compared to 20.1% of non-essential workers. Vaccine hesitancy was identified in 29.6% of Whites, 13.2% of Chinese, and 11.3% of South Asians. Individuals in large households (≥ 6 household members) were more likely to report vaccine hesitancy, compared to those in smaller households. Also, people in the most privileged quintiles (Q1) of both material and social deprivation indices were more willing to receive the COVID-19 vaccine (67.3 and 65.8 %, respectively) compared to those in the least privileged (correspondingly 53.8 and 58.5%).
Association between interpersonal contact and vaccine hesitancy
Results from the multivariable multinomial logistic regression model assessing the association between interpersonal contact and vaccine hesitancy are shown in Table 4. In the model, we found a dose-response association between interpersonal contact and vaccine hesitancy; compared to individuals in the lowest quartile (least contact), those in the fourth quartile (reporting the highest number of contacts), third quartile and second quartile were more likely to be vaccine hesitant, adjusted odd ratios (aORs) 2.85 (95% CI: 2.02, 4.00), 1.91 (95% CI: 1.38, 2.64) and 1.78 (95% CI: 1.13, 2.82). In the sensitivity analysis where the outcome variable (willingness to vaccinate) included individuals who had already received the vaccine, we also found that compared to individuals in the lowest quartile (least contact), those in the fourth quartile (highest contact) were more likely to be vaccine hesitant, aOR =1.65 (95% CI: 1.26, 2.16) (Supplementary Table 3 of the Supplementary File).
Discussion
To our knowledge, this is the first study to investigate the association between vaccine hesitancy and interpersonal contacts, a major risk factor for COVID-19 transmission. Overall, we found that 56.7% of our study population was willing to receive COVID-19 vaccines. This compares to the 79.8% vaccine acceptance reported in a study (16) conducted in the same province (BC), almost a year prior to our study. Although differences in the time periods in which the two studies were conducted could account for the variability in these rates, some of differences may be related to the differences in sample characteristics. Specifically, whereas our study drew a sample of BC residents from social media, the previous study sampled from research cohorts who had consented to be contacted for future research and therefore participants in that study would be more likely to be health conscious and thus less likely to be vaccine hesitant. Also, because we surveyed at a time when a larger proportion of the population had already received vaccines, the sample population remaining to receive the vaccine was more likely to be composed of people with anti-vaccination sentiments. In our sensitivity analyses, where individuals who had received the vaccine were included with those who indicated they were willing to be vaccinated, vaccine acceptance was 86.5%, slightly higher than the previous study (16).
We found that individuals with high interpersonal contact were more likely to be vaccine hesitant compared to those with low contacts. Specifically, we found a dose-response association between interpersonal contact and vaccine hesitancy; compared to individuals in the lowest quartile (least contact), those in the fourth quartile (i.e., those with the highest contact), third quartile and second quartile groups had 185, 91, and 78% increased odds of vaccine hesitancy, respectively. Consistently, in the sensitivity analyses where individuals who had already received were assumed to be willing to receive the vaccine, we also found that, compared to individuals in the lowest quartile, those in the fourth quartile of interpersonal contact had a 65% increased odds of vaccine hesitancy. These findings are concerning, given that COVID-19 transmission is driven by interpersonal contact. Therefore, vaccine hesitancy among people who are more likely to transmit the virus due to their high levels of interpersonal contacts, presents a major threat to the expected gains from current and future vaccination efforts.
The gendered patterns of vaccine hesitancy from the COVID-19 literature were also reflected in our study. Contrary to other findings (16, 27, 28) our investigation showed that the likelihood of getting a COVID-19 vaccine was higher among females than males. This discrepancy may be due to differences in the type of sample [as discussed previously in regard to (16)], and time frame [responses in the study by (27) were collected before vaccines were widely available in the U.S.]. Nonetheless, more research with population-based samples is required to elucidate this matter.
Another concerning finding was that individuals who lived in larger households (six or more people in household) were more likely to be vaccine hesitant. This is alarming given individuals in larger households are more likely to be in cramped spaces with limited ability to properly distance from one another.
Racial and ethnic disparities in vaccination have been highlighted in many studies (17). Paul et al. (29) report that individuals with ethnic minority backgrounds have higher distrustful attitudes toward vaccination. These attitudes, which may be fueled by anti-intellectualism and misinformation and lack of appropriate information in accessible language and formats (30), could lead to lower perceived risk of COVID-19 infection and severity of illness. Ongoing racism, historical contexts related to racism, such as unethical research trials on Black and Indigenous Peoples (31–33) may lead to skepticism, distrust and lower perceived benefits of COVID-19 vaccination among these populations. Vaccine hesitancy among ethnic and racial minorities is concerning given the disproportionate burden of COVID-19 outcomes among these groups (34, 35). Studies, particularly in the U.S and UK, have reported lower vaccine acceptance in racial minority populations (35–39). However, we found that whereas 29.6% of Whites reported vaccine hesitancy, 13.2% of Chinese and 11.3% of South Asians were vaccine hesitant in our analysis. These findings are consistent with a Canadian national survey where vaccine hesitancy was lower among South Asian and Chinese population compared to the White population, although higher among Black population (40). These findings reflect the heterogeneity and diverse experiences of minority groups across the world. The disproportionately higher burden of COVID-19 among racialized or minority groups in Canada particularly prior to vaccine availability (41) potentially highlighted the importance of vaccines in preventing further infections to members of this group; potentially making people more willing to accept vaccines. However, the higher burden of COVID-19 among South Asians population in UK did not affect vaccine hesitancy, highlighting differences in underlying beliefs, perceptions, and trust in the healthcare system. In addition, it has been largely recognized that vaccine hesitancy among minority groups, especially the Black community in the U.S, is fuelled by the deep-rooted and long-standing mistrust in the healthcare system and the government, driven by historical events in medical care and research (42, 43). However, the role of trust in the healthcare system and government in shaping vaccine acceptance among various groups is not very clear. Further investigations are needed to understand the differences in vaccine hesitancy and drivers of vaccine hesitancy among various ethnic groups in Canada.
It was expected that individuals considered as essential workers would be less vaccine hesitant. These are individuals in occupations deemed essential to not only the pandemic response but also maintaining essential services. Essential work includes occupations in the health sector (e.g., medical, social work, psychology), natural resources, agriculture and related production occupations, manufacturing and utilities, sales and service occupations, trades, transport and equipment operators and related occupations. In BC, these groups were prioritized in the roll-out of COVID-19 vaccination. We found that individuals in these occupations had higher odds of vaccine hesitancy and reported greater interpersonal contacts compared to those in non-essential work. Similar findings were uncovered by Ogilvie et al. where essential non-healthcare workers were found to have lower adjusted odds of intending to receive COVID-19 vaccine (16). A disconcerting facet to this is the heightened risk among this population, due to their unavoidably high contact rates with the public.
Implication
Whereas, these are important findings which can inform strategic vaccine-acceptance messaging, it is expected that more routine systems are built to monitor vaccine hesitancy, to inform education and communication needs related to the pandemic control. The findings of this study can be used to inform public health interventions aimed at improving vaccine uptake.
Tackling misinformation about vaccination will be critical to reducing the morbidity and mortality of the disease. COVID-19 vaccine hesitancy has been associated with mistrust of vaccine benefit (29), safety concerns over vaccine development, and side effects (15). Unwillingness to receive the vaccine is also driven by misinformation or distrust of government and healthcare systems (44–47). Therefore, health communication strategies aimed at building trust between at-risk communities may be needed to address this issue (34). To make COVID-19 vaccination communication more effective, we can create targeted approaches to change behaviors and promote vaccination among vaccine hesitant individuals.
Motivational interviewing, which aims to support decision making by eliciting and strengthening a person's motivation to change their behavior based on their own arguments for change has been shown to be effective in increasing vaccine uptake (48). Additionally, medical reminders (49) and provider recommendations (48) are also effective strategies in promoting vaccinations. Among communities of color, where issues of misinformation and mistrust of the medical system appear to be a significant factor for vaccine hesitancy, a multipronged approach based on partnerships with trusted community resources such as faith-based leaders, community organizers, and community mentors can be a helpful tool in tackling low rates of vaccine uptake in these communities (50). Furthermore, it has been noted that the misinformation that drive vaccine hesitancy attitudes are propagated via social media (11). These same platforms could be used for such targeted campaigns, given their effective knowledge dissemination potential.
Findings from this investigation can also be useful to optimize predictive transmission models by including the impact of vaccine hesitancy on transmission risk.
Limitations and strengths
Like all surveys, our findings are subject to social desirability bias. Although our online-based study minimizes the role of social desirability bias, it cannot be ruled out entirely as exerting some influence. In addition, although vaccine willingness or hesitancy has been highly volatile and changing depending on evolving information, our survey only captured respondent's attitudes at one period in time (March 2021 to December 2021). Further studies should examine changing trends of vaccine hesitancy. Despite these limitations, a major novelty to this study is our ability to account for each individual's contact behaviors. Furthermore, our study investigated the characteristics and factors associated with vaccine hesitancy among people who remain unvaccinated in the province, as this population may differ from the population who were ready to receive the vaccine as soon as it became available to them. Future vaccination strategies may need to be staggered, to target different aspects related to vaccination acceptance among hesitant subgroups.
Conclusion
Despite public campaigns urging people to get vaccinated, vaccine hesitancy remains a challenge in pandemic response. We found vaccine hesitancy to be greater among individuals with higher interpersonal contacts, suggesting the need for targeted interventions to increase vaccine acceptance among this population.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by University of British Columbia Behavioral Research Ethics Board (No: H20-01785). The patients/participants provided their written informed consent to participate in this study.
Author contributions
NJ and PA conceptualized the study. All authors reviewed and agreed on the final submission.
Funding
This work was supported by Michael Smith Foundation for Health Research COVID-19 Research Response Fund (Award #: COV-2020-1183).
Acknowledgments
The authors would like to express their gratitude to all participants of the British Columbia COVID-19 Population Mixing Patterns (BC-Mix) survey.
Conflict of interest
Author NJ has advised and spoken for AbbVie, not related to this project or COVID-19.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.971333/full#supplementary-material
References
1. Johns Hopkins Coronavirus Resource Center. COVID-19 Map. (2022). Available online at: https://coronavirus.jhu.edu/map.html (accessed August 7, 2022).
2. Bernal JL, Andrews N, Gower C, Robertson C, Stowe J, Tessier E, et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on covid-19 related symptoms, hospital admissions, and mortality in older adults in England: test negative case-control study. BMJ. (2021) 373:n1088. doi: 10.1136/bmj.n1088
3. Haas EJ, Angulo FJ, McLaughlin JM, Anis E, Singer SR, Khan F, et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data. Lancet. (2021) 397:1819–29. doi: 10.1016/S0140-6736(21)00947-8
4. Nasreen S, Chung H, He S, Brown KA, Gubbay JB, Buchan SA, et al. Effectiveness of COVID-19 vaccines against symptomatic SARS-CoV-2 infection and severe outcomes with variants of concern in Ontario. Nat Microbiol. (2022) 7:379–85. doi: 10.1038/s41564-021-01053-0
5. Skowronski DM, Setayeshgar S, Febriani Y, Ouakki M, Zou M, Talbot D, et al. Two-dose SARS-CoV-2 vaccine effectiveness with mixed schedules and extended dosing intervals: test-negative design studies from British Columbia and Quebec, Canada. medRxiv. (2021). doi: 10.1101/2021.10.26.21265397
6. Velásquez García HA, Wilton J, Smolina K, Chong M, Rasali D, Otterstatter M, et al. Mental health and substance use associated with hospitalization among people with COVID-19: a population-based cohort study. Viruses. (2021) 13:2196. doi: 10.3390/v13112196
7. MacDonald NE, SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: definition, scope and determinants. Vaccine. (2015) 33:4161–4. doi: 10.1016/j.vaccine.2015.04.036
8. World Health Organization. Ten Health Issues WHO Will Tackle This Year. (2019). Available online at: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed July 13, 2021).
9. Ali M, Hossain A. What is the extent of COVID-19 vaccine hesitancy in Bangladesh? a cross-sectional rapid national survey. BMJ Open. (2021) 11:e050303. doi: 10.1136/bmjopen-2021-050303
10. Ali M. What is driving unwillingness to receive the COVID-19 vaccine in adult Bangladeshi after one year of vaccine rollout? analysis of observational data. IJID Reg. (2022) 3:177–82. doi: 10.1016/j.ijregi.2022.03.022
11. Ackah BBB, Woo M, Stallwood L, Fazal ZA, Okpani A, Ukah UV, et al. COVID-19 vaccine hesitancy in Africa: a scoping review. Glob Health Res Policy. (2022) 7:21. doi: 10.1186/s41256-022-00255-1
12. Yasmin F, Najeeb H, Moeed A, Naeem U, Asghar MS, Chughtai NU, et al. COVID-19 vaccine hesitancy in the United States: a systematic review. Front Public Health. (2021) 9:770985. doi: 10.3389/fpubh.2021.770985
13. Government of Canada. Drug and Vaccine Authorizations for COVID-19: Authorized Drugs, Vaccines and Expanded Indications. (2022). Available online at: https://www.canada.ca/en/health-canada/services/drugs-health-products/covid19-industry/drugs-vaccines-treatments/authorization/list-drugs.html (accessed July 20, 2022).
14. British Columbia Centre for Disease Control. Vaccines Available in B.C. (2022). Available online at: http://www.bccdc.ca/health-info/diseases-conditions/covid-19/covid-19-vaccine/vaccines-for-covid-19 (accessed July 20, 2022).
15. Statistics Canada. Canadians' Willingness to Get a COVID-19 Vaccine: Group Differences Reasons For Vaccine Hesitancy. (2020). Available online at: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00073-eng.htm (accessed July 26, 2021).
16. Ogilvie GS, Gordon S, Smith LW, Albert A, Racey CS, Booth A, et al. Intention to receive a COVID-19 vaccine: results from a population-based survey in Canada. BMC Public Health. (2021) 21:1017. doi: 10.1186/s12889-021-11098-9
17. Hassan W, Kazmi SK, Tahir MJ, Ullah I, Royan HA, Fahriani M, et al. Global acceptance and hesitancy of COVID-19 vaccination: a narrative review. Narra J. (2021) 1. doi: 10.52225/narra.v1i3.57
18. Government of Canada SC. Census Profile, 2016 Census - British Columbia [Province] and Canada [Country]. (2017). Available online at: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/details/page.cfm?Lang=E&Geo1=PR&Code1=59&Geo2=PR&Code2=01&SearchText=Canada&SearchType=Begins&SearchPR=01&B1=All&type=0 (accessed July 25, 2021).
19. Bethlehem JG. Applied Survey Methods: A Statistical Perspective. Hoboken, NJ: Wiley (2009). p. 375. doi: 10.1002/9780470494998
20. Adu PA, Binka M, Mahmood B, Jeong D, Buller-Taylor T, Damascene MJ, et al. Cohort profile: the british columbia COVID-19 population mixing patterns survey (BC-Mix). BMJ Open. (2022) 12:e056615. doi: 10.1136/bmjopen-2021-056615
21. Iyaniwura SA, Falcão RC, Ringa N, Adu PA, Spencer M, Taylor M, et al. Mathematical modeling of COVID-19 in British Columbia: an age-structured model with time-dependent contact rates. Epidemics. (2022) 39:100559. doi: 10.1016/j.epidem.2022.100559
22. Ringa N, Otterstatter MC, Iyaniwura SA, Irvine MA, Adu P, Janjua NZ, et al. Social contacts and transmission of COVID-19 in British Columbia, Canada. Front Public Health. (2022) 10:867425. doi: 10.3389/fpubh.2022.867425
23. Eysenbach G. Improving the quality of web surveys: the checklist for reporting results of internet E-Surveys (CHERRIES). J Med Internet Res. (2004) 6:e34. doi: 10.2196/jmir.6.3.e34
24. British Columbia Government. Health Boundaries - Province of British Columbia. Health Boundaries. Available online at: https://www2.gov.bc.ca/gov/content/data/geographic-data-services/land-use/administrative-boundaries/health-boundaries (accessed July 19, 2022).
25. Pampalon R, Hamel D, Gamache P, Raymond G. A deprivation index for health planning in Canada. Chronic Dis Can. (2009) 29:178–91. doi: 10.24095/hpcdp.29.4.05
27. Szilagyi PG, Thomas K, Shah MD, Vizueta N, Cui Y, Vangala S, et al. National trends in the US public's likelihood of getting a COVID-19 vaccine—April 1 to December 8, 2020. JAMA. (2021) 325:396–8. doi: 10.1001/jama.2020.26419
28. Rayhan MA, Mudatsir M, Nurjannah N, Ichsan I, Amir-Behghadami M, Khader YS, et al. Acceptance and willingness to purchase a hypothetical COVID-19 vaccine in a region under Shariah law: a cross-sectional study in Aceh, Indonesia. Narra J. (2022) 2:85. doi: 10.52225/narra.v2i2.85
29. Paul E, Steptoe A, Fancourt D. Attitudes towards vaccines and intention to vaccinate against COVID-19: implications for public health communications. Lancet Reg Health Eur. (2021) 1:100012. doi: 10.1016/j.lanepe.2020.100012
30. Puri N, Coomes EA, Haghbayan H, Gunaratne K. Social media and vaccine hesitancy: new updates for the era of COVID-19 and globalized infectious diseases. Hum Vaccines Immunother. (2020) 16:2586–93. doi: 10.1080/21645515.2020.1780846
31. Lux M. Perfect subjects: race, tuberculosis, and the Qu'Appelle BCG vaccine trial. Can Bull Med Hist. (1998) 15:277–95. doi: 10.3138/cbmh.15.2.277
32. Mosby I. Administering colonial science: nutrition research and human biomedical experimentation in aboriginal communities and residential schools, 1942–1952. Hist Soc Soc Hist. (2013) 46:145–72. doi: 10.1353/his.2013.0015
33. Park J. Historical origins of the tuskegee experiment: the dilemma of public health in the United States. Uisahak. (2017) 26:545–78. doi: 10.13081/kjmh.2017.26.545
34. Razai MS, Osama T, McKechnie DGJ, Majeed A. Covid-19 vaccine hesitancy among ethnic minority groups. BMJ. (2021) 372:n513. doi: 10.1136/bmj.n513
35. Kadambari S, Vanderslott S. Lessons about COVID-19 vaccine hesitancy among minority ethnic people in the UK. Lancet Infect Dis. (2021) 21:1204–6. doi: 10.1016/S1473-3099(21)00404-7
36. Hussain B, Latif A, Timmons S, Nkhoma K, Nellums LB. Overcoming COVID-19 vaccine hesitancy among ethnic minorities: a systematic review of UK studies. Vaccine. (2022) 40:3413–32. doi: 10.1016/j.vaccine.2022.04.030
37. Nguyen LH, Joshi AD, Drew DA, Merino J, Ma W, Lo C-H, et al. Self-reported COVID-19 vaccine hesitancy and uptake among participants from different racial and ethnic groups in the United States and United Kingdom. Nat Commun. (2022) 13:636. doi: 10.1038/s41467-022-28200-3
38. Robertson E, Reeve KS, Niedzwiedz CL, Moore J, Blake M, Green M, et al. Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain Behav Immun. (2021) 94:41–50. doi: 10.1016/j.bbi.2021.03.008
39. Gaughan CH, Razieh C, Khunti K, Banerjee A, Chudasama YV, Davies MJ, et al. COVID-19 vaccination uptake amongst ethnic minority communities in England: a linked study exploring the drivers of differential vaccination rates. J Public Health. (2022). doi: 10.1093/pubmed/fdab400
40. Statistics Canada. COVID-19 Vaccine Willingness Among Canadian Population Groups. (2021). Available online at: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2021001/article/00011-eng.htm (accessed August 1, 2022).
41. Xia Y, Ma H, Moloney G, García HAV, Sirski M, Janjua NZ, et al. Geographic concentration of SARS-CoV-2 cases by social determinants of health in metropolitan areas in Canada: a cross-sectional study. CMAJ. (2022) 194:E195–204. doi: 10.1503/cmaj.211249
42. Momplaisir FM, Kuter BJ, Ghadimi F, Browne S, Nkwihoreze H, Feemster KA, et al. Racial/Ethnic differences in COVID-19 vaccine hesitancy among health care workers in 2 large academic hospitals. JAMA Netw Open. (2021) 4:e2121931. doi: 10.1001/jamanetworkopen.2021.21931
43. Egede LE, Walker RJ. Structural racism, social risk factors, and covid-19 — a dangerous convergence for black Americans. N Engl J Med. (2020) 383:e77. doi: 10.1056/NEJMp2023616
44. Jennings W, Stoker G, Bunting H, Valgarðsson VO, Gaskell J, Devine D, et al. Lack of trust, conspiracy beliefs, and social media use predict COVID-19 vaccine hesitancy. Vaccines. (2021) 9:593. doi: 10.3390/vaccines9060593
45. Loomba S, de Figueiredo A, Piatek SJ, de Graaf K, Larson HJ. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat Hum Behav. (2021) 5:337–48. doi: 10.1038/s41562-021-01056-1
46. Qunaibi E, Basheti I, Soudy M, Sultan I. Hesitancy of Arab healthcare workers towards COVID-19 vaccination: a large-scale multinational study. Vaccines. (2021) 9:446. doi: 10.3390/vaccines9050446
47. Trent M, Seale H, Chughtai AA, Salmon D, MacIntyre CR. Trust in government, intention to vaccinate and COVID-19 vaccine hesitancy: a comparative survey of five large cities in the United States, United Kingdom, and Australia. Vaccine. (2021) 40:2498–505. doi: 10.1016/j.vaccine.2021.06.048
48. Benedict KM, Santibanez TA, Black CL, Ding H, Graitcer SB, Bridges CB, et al. Recommendations and offers for adult influenza vaccination, 2011-2012 season, United States. Vaccine. (2017) 35:1353–61. doi: 10.1016/j.vaccine.2016.04.061
49. Milkman KL, Patel MS, Gandhi L, Graci HN, Gromet DM, Ho H, et al. A megastudy of text-based nudges encouraging patients to get vaccinated at an upcoming doctor's appointment. Proc Natl Acad Sci U S A. (2021) 118:e2101165118. doi: 10.1073/pnas.2101165118
Keywords: interpersonal contact, COVID-19, vaccine hesitancy, transmission, Canada
Citation: Adu PA, Iyaniwura SA, Mahmood B, Jeong D, Makuza JD, Cua G, Binka M, García HAV, Ringa N, Wong S, Yu A, Irvine MA, Otterstatter M and Janjua NZ (2022) Association between close interpersonal contact and vaccine hesitancy: Findings from a population-based survey in Canada. Front. Public Health 10:971333. doi: 10.3389/fpubh.2022.971333
Received: 16 June 2022; Accepted: 26 August 2022;
Published: 04 October 2022.
Edited by:
Fuqiang Cui, Peking University, ChinaReviewed by:
Mohammad Ali, La Trobe University, AustraliaBrian J. Piper, Geisinger Commonwealth School of Medicine, United States
Harapan Harapan, Syiah Kuala University, Indonesia
Copyright © 2022 Adu, Iyaniwura, Mahmood, Jeong, Makuza, Cua, Binka, García, Ringa, Wong, Yu, Irvine, Otterstatter and Janjua. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Naveed Z. Janjua, bmF2ZWVkLmphbmp1YUBiY2NkYy5jYQ==