 Yuanyuan Lu
Yuanyuan Lu Yuhang Zhao2†
Yuhang Zhao2† Xiaofang Shangguan
Xiaofang Shangguan Benyan Lv
Benyan Lv Rui Huang
Rui Huang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 13 October 2022
Sec. Aging and Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.970032
Objectives: The patients' attitude is critical in disease control. This study aims to explore the determinants of patients' attitude and satisfaction.
Methods: A total of 844 patients in the rural areas of Shandong, Henan, and Sichuan provinces with hypertension or diabetes were randomly selected for investigation. The outcome variables were the patients' attitude and satisfaction toward chronic disease control, which were measured through patient self-reported. Binary logistic regression models were used to explore the determinants of patients' attitude and satisfaction.
Results: Teachers were more likely to regard that chronic disease management was helpful in their chronic disease control than that in farmers (OR = 3.994, 95% confidence interval (CI) = 1.309–12.188). Moreover, the probability of health institutions recording chronic diseases changes and guiding rehabilitation for patients regularly is considered helpful 2.688 times more than those that are not. In addition, receiving chronic disease management services can make patients repute that chronic disease management services are helpful in controlling chronic diseases more capably (OR = 1.582, 95% CI = 2.198–10.771). In terms of satisfaction, patients who do not know regular follow-up tend to be dissatisfied with chronic diseases control result (OR = 0.376, 95% CI = 0.192–0.737; OR = 0.592, 95%CI = 0.417–0.841).
Conclusion: The government increases the promotion of chronic disease management in rural areas to improve patients' awareness. Health institutions also can provide diversified services to meet the needs of more people. At last, paying more attention to the timeliness of health services need to be considered to develop a health plan.
Chronic diseases have been becoming the main cause of death and disability in the world (1). Diabetes and cardiovascular disease are major chronic diseases (2). According to the report, the number of diabetes globally has reached 425 million, which will increase to 629 million in 2045 (3). The estimated number of adults suffering from hypertension globally was expected to reach 1.56 billion by 2025 (4). Treatment for characteristics of chronic diseases is long-term and expensive and will consume vast healthcare resources (5). Simultaneously, demand for high-quality healthcare has been greatly and continuously rising with the development of the economy in recent decades. The need for long-term and expensive healthcare, on the one hand, lays a heavy burden on the healthcare system, and on the other hand, greatly threats the equity of the system (6, 7), especially in rural China where the healthcare resources are insufficient (8).
Adhering to chronic disease management is critical to improving health and quality of life for patients (9). It has been suggested for chronic disease control and prevention (1, 10, 11). Focusing on the joint intervention of patients, medical staffs, and medical policies, the chronic care model was proposed in 1998 (12), and was advanced with the expansion and extension of innovative care for chronic conditions. In the United Kingdom, supported by teamwork under chronic disease managers' supervision, ~90% of patients receive healthcare from community health institutions (13). Under the political commitment to universal health coverage in China, central and local governments have funded interventions for hypertension and diabetes. A series of strategies and programs have been developed to control the incremental trend of chronic disease morbidity. These included defining the responsibilities of different health agencies, developing a supportive community environment, training chronic disease staff, providing population-based public health interventions such as establishing health files and providing health promotion services, and individual-based health interventions which include regular follow-up services and guidance in healthy life (14–16). They were included in the national essential public health services (EPHSs) and have been accessible to every patient for free since 2009. The health management services for chronic disease patients mainly include establishing health records, regular follow-up visits, and health promotion (17, 18).
Nevertheless, the effect of chronic diseases on control is dissatisfied by the public (19). The dissatisfaction of patients was that their expectations have not been met and do not achieve their requirements (20). Limited research shows that patients prefer to manage their health by participating in medical decisions. Patient involvement in healthcare has become a national priority. However, the majority of chronic disease interventions are designed without patients in practice (19). Based on knowledge, attitude, belief, practice (KABP), patients' acceptance and satisfaction with medical services are the main factors that affect individual decision-making behavior, and that will affect patients' health (21–23). In addition, the capacity of health systems in rural and urban did not improve at the same rate. In rural areas, EPHS is the main provider of resident health (24). Compared to the contributions of the demand side, most interventions mainly focused on the implementation of the supply side (25). Therefore, this study is conducted to explore the determinants of patient attitudes and satisfaction, including patients' knowledge, attitudes, beliefs, and practices about chronic disease control, to provide information for further improvement in the rural chronic disease management (CDM) system.
A cross-sectional survey was conducted in rural areas of Henan, Shandong, and Sichuan Province in China, from June to August 2016. Stratified random sampling was used to select rural areas in 53 cities from three provinces. To ensure the quality of the investigation, investigators had been trained before the investigation started. During the implementation of the survey, the quality of the survey was controlled by reviewing the questionnaires on the day. The validity of the questionnaire was evaluated and verified through expert consultation and group discussion. Because the survey questions are simple, and most of them are established facts, the quality of the survey can be guaranteed, and the reliability test has not been carried out.
In total, 997 patients were investigated, and 844 of them provided valid information in the end (the criteria for valid questionnaires were filling time > 5 min and question completion rate ≥ 90.0%). Interviewers were face-to-face conducted with each participant. All participants read consent before they participate in the interview.
Neither patients nor the public was involved in the design, planning, conduct, or reporting of this study.
The outcome variables were the patients' attitude and satisfaction toward chronic disease control, which were measured through patient self-reported. For the attitude, participants were asked “How about the chronic diseases services provided by health agencies for your disease control?” Possible responses ranged from very helpful, helpful, moderate, and unhelpful to very unhelpful. “Very helpful and helpful” were categorized as helpful, and the rest as unhelpful. Similarly, satisfaction was measured by the answer to the following question: How satisfied you are with the result of chronic disease control? The answers ranged from very satisfied, satisfied, moderate, and dissatisfied to very dissatisfied. Participants were classified as satisfied (containing very satisfied and satisfied) and dissatisfied (containing moderate, dissatisfied, and very dissatisfied). Various demographic, socioeconomic, and chronic disease service variables were included in the analysis based on the literature review. Detailed indicators and codes are shown in Table 1 (26–29).
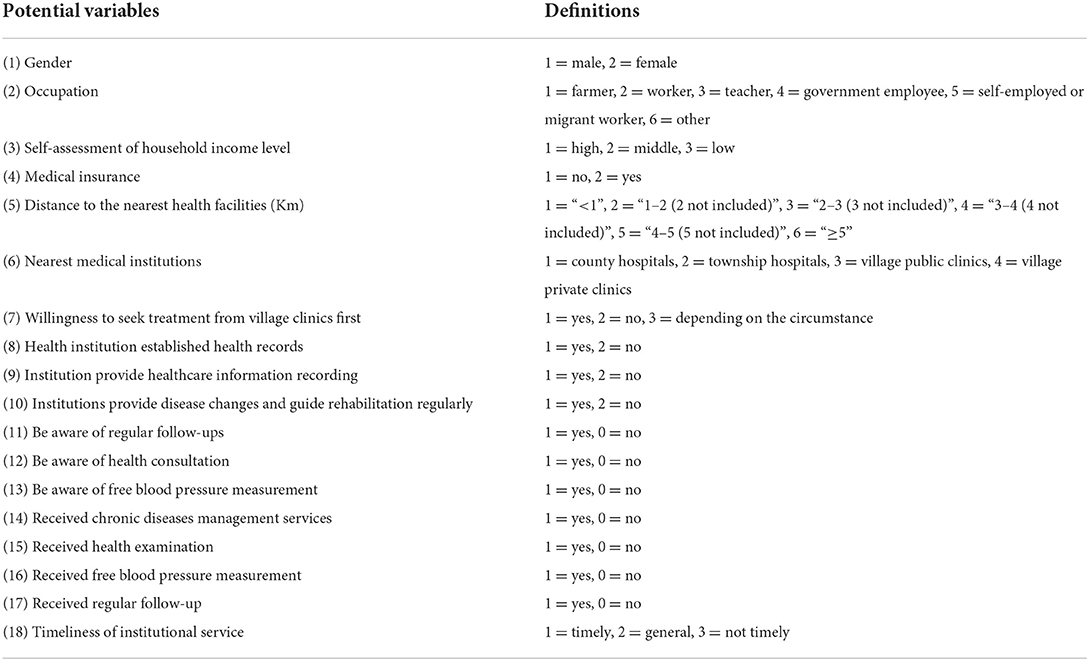
Table 1. Definitions of potential variables.
The database was established using EpiData version 3.1 (Atlanta, GA, USA) and double-entered independently to avoid entry errors. All statistical analyses were carried out by SPSS version 24.0 (SPSS Inc., Chicago, IL USA). Chi-square tests were used to explore differences in covariate values between helpful and unhelpful (satisfied and dissatisfied) groups. Associated factors were filtered by the Wald statistic of the backward stepwise method, and finally, statistically significant variables were included in the binary logistic regression model. P-values < 0.05 (two-sides) were set as a statistically level in this study.
The characteristics of patients are shown in Table 2. The average age of participants was 60 years. More than half of them were farmers (60.94%). Approximately 60% of participants were willing to choose the village clinic first, and only 16.67% were reluctant to visit the doctor at the village clinic primary. Most participants (65.65%) knew that primary health institutions provided the measurement of blood pressure and blood glucose freely, while 11.45% of them have ever received chronic disease management. Moreover, 41.9% of participants considered that the services were provided timely.
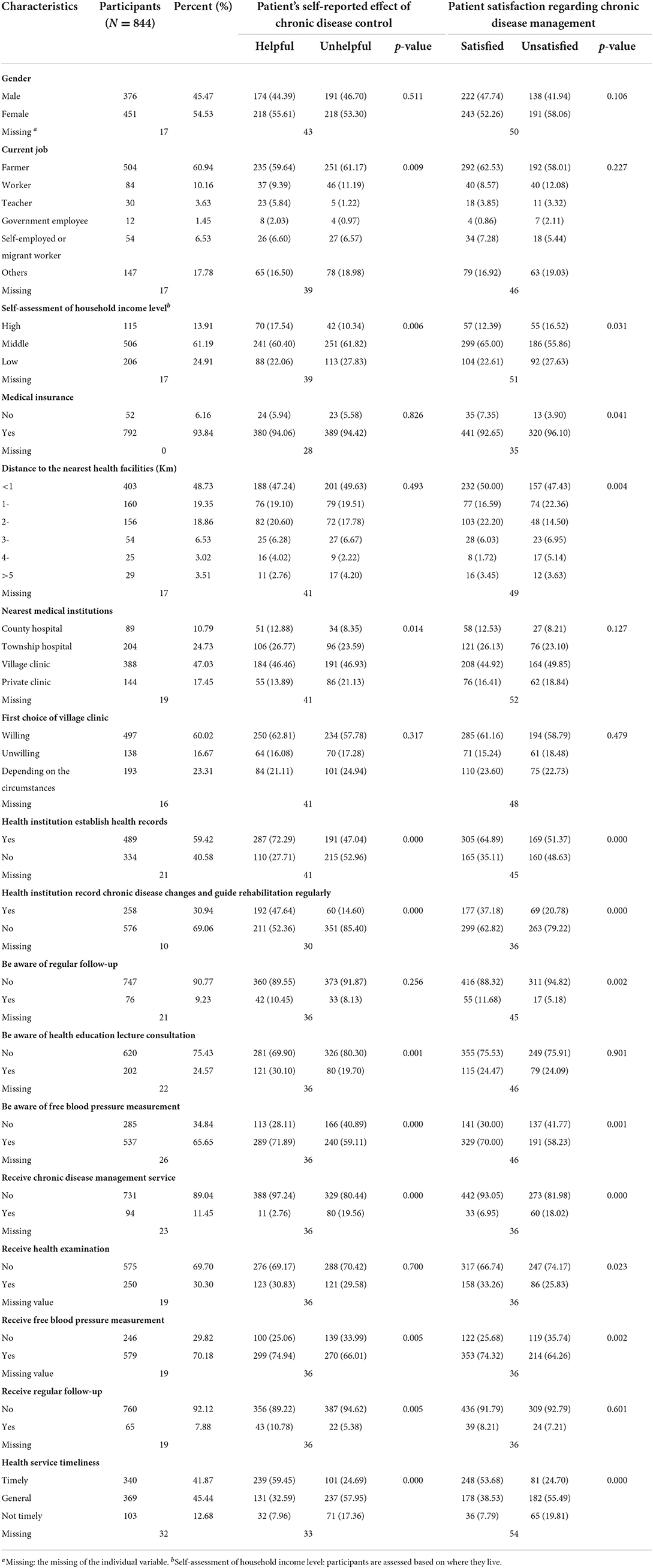
Table 2. The characteristics of participants, the comparison of patient satisfaction regarding chronic disease management, and the self-reported effect of chronic disease control in rural China.
The comparison of patient satisfaction and self-reported is shown in Table 2. Roughly 58.84% of participants were satisfied with chronic disease management. The significant differences in satisfaction were found in the subgroups of self-reported household income level, whether have medical insurance or not, distance to the nearest health facilities, whether health institutions established health records or not, whether health institutions updated the health record or not, whether health institution record chronic disease changes and guide rehabilitation regularly or not, whether the respondents were aware of the free follow-up and free blood pressure measurement services or not, the timeliness of health service, whether respondents received services of chronic disease management, free blood measurement, and follow-up services or not.
Approximately half of the patients reported chronic disease management was helpful for their health status. The significant differences in the attitude were found among the subgroup of occupation, self-reported household income level, the nearest medical institution, whether health institutions establish health records, whether record chronic disease changes and guide rehabilitation regularly or not, and whether aware of the services of blood measurement and health promotion or not, the timeliness of health services, whether received the services of chronic disease management, free blood measurement, and follow-up services or not.
Results of binary logistic regression analysis are shown in Table 3. It illustrates that satisfaction was significantly associated with patients' awareness of CDM services. Teachers and government employees were more likely to dissatisfy with CDM than farmers (OR = 0.884, 95% CI = 0.352–2.218; OR = 0.195, 95%CI = 0.044–0.867). Patients who did not purchase health insurance and willing to choose a village clinic firstly were unlikely to dissatisfy. Besides that who do not know regular follow-up tends to be dissatisfied (OR = 0.376, 95% CI = 0.192–0.737). Furthermore, patients who do not know free blood pressure measurement services are prone to be dissatisfied (OR = 0.592, 95% CI = 0.417–0.841). The odds of the effect of those who received service timely toward disease control were 4.466 times than who do not (OR = 4.466, 95% CI = 2.603–7.665).
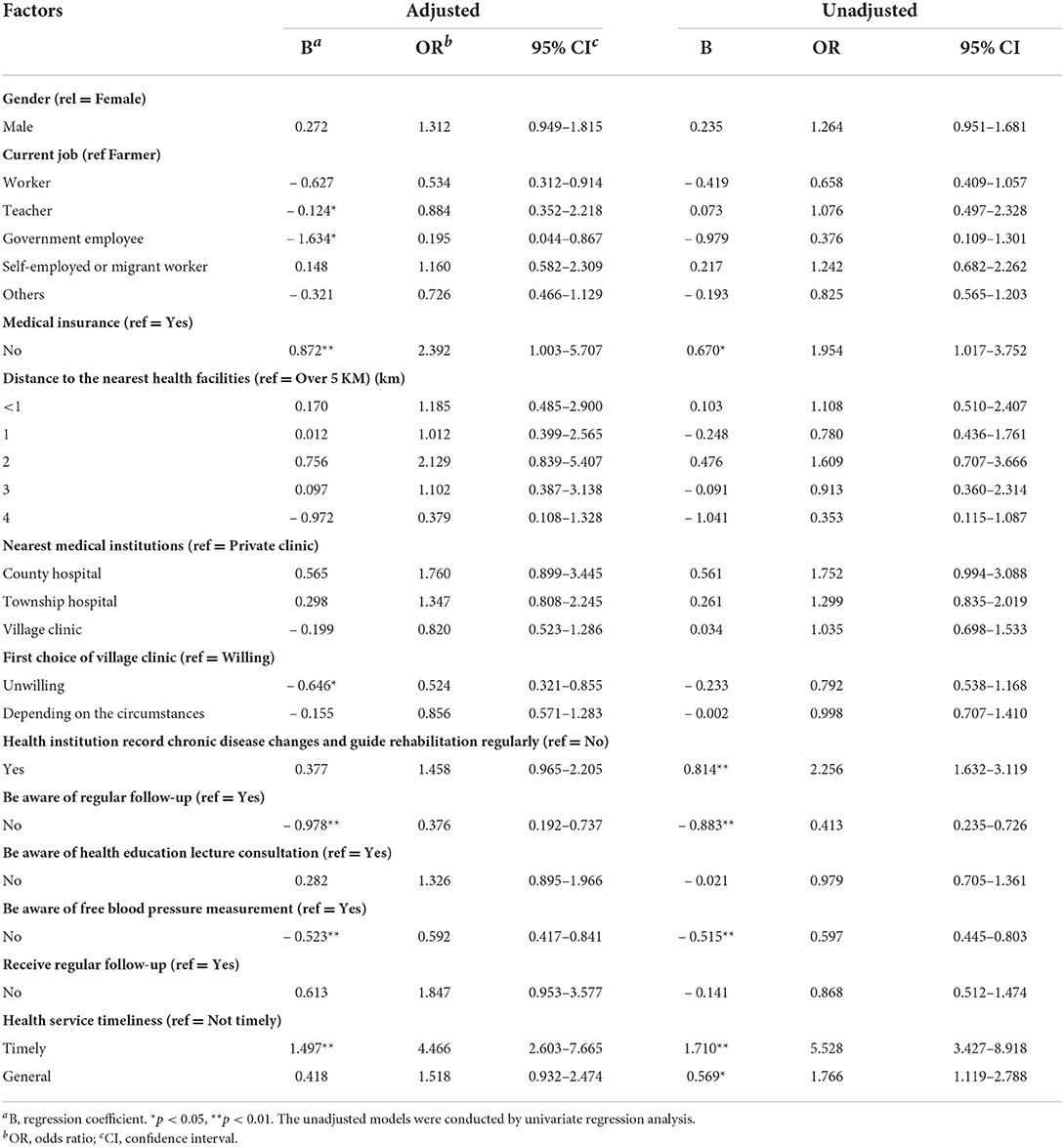
Table 3. Factors associated with patient satisfaction regarding chronic disease management.
Compared to the farmer, the CDM seemed more helpful to the teacher (OR = 3.994, 95% CI = 1.309–12.188). The higher income the patients were, the more helpful to the health status they reported. Besides, the odds of the effect of health records on disease control were 1.539 times greater than those who did not have health records (OR = 1.539, 95% CI = 1.074–2.204). Moreover, updating the health record and guiding patients or rehabilitation regularly was reported more helpful (OR = 2.688, 95% CI = 1.804–4.004). It is noteworthy that those who received chronic disease management services reported more help than that who did not receive them before (OR = 4.866, 95% CI = 2.198–10.771). The effect of those who received service timely to disease control was 2.927 times greater than that of those who did not (OR = 2.927, 95% CI = 1.708–5.015). More details are shown in Table 4.
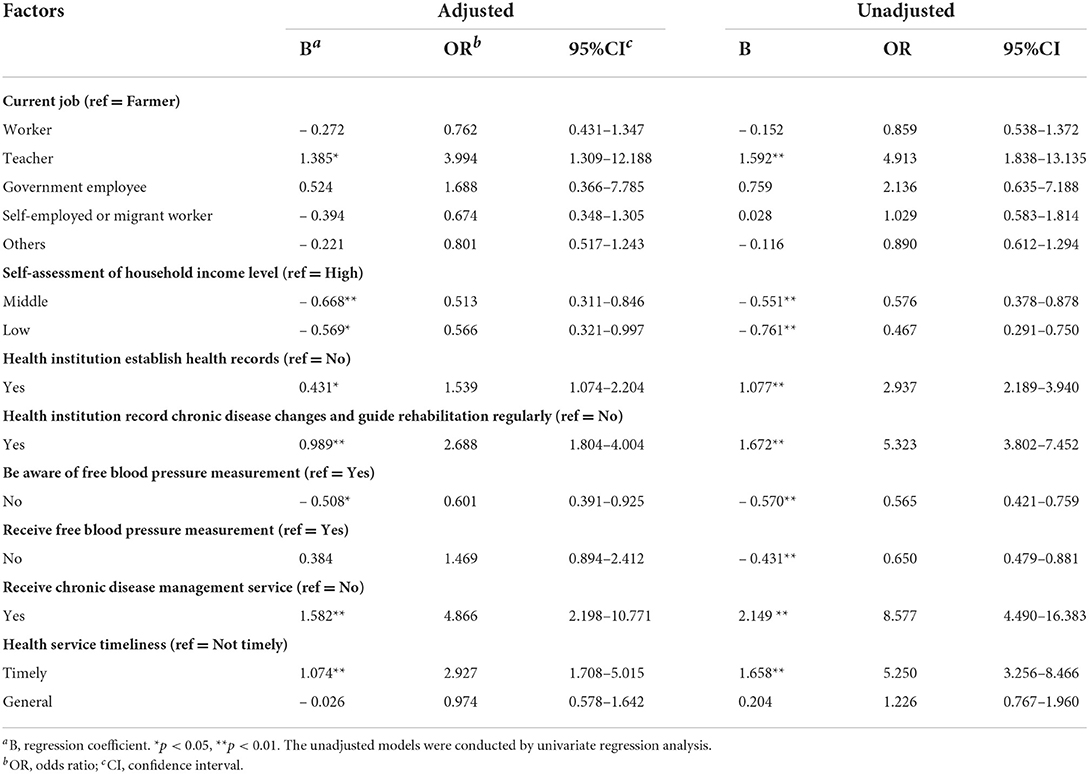
Table 4. Outcome of logistic regression analysis for examining associated factors of self-reported effect of chronic disease control.
Although the Chinese government has established a relatively wide rural tertiary service network since 2009 (30, 31), findings of this study indicated that < 60% of patients regarded CDM services as helpful and were satisfied with them. Similar findings can be retrieved from a previous study (32). This calls for more attention to the influencing factors of chronic disease management. Among the influencing factors, patient adherence to intervention measures directly affected the prevention and control effect. The average adherence rate of patients with chronic diseases was reported to be ~50% and was lower than that in developing countries (29). Thus, increasing adherence had a greater effect on health than specific medical therapy improvements (26, 29). Another study revealed the underlying reason that patients with chronic diseases tend to have weak awareness of self-management, and at the same time, lack sufficient family support (33). In comparison, this study was more concerned with the impact of variables, such as demographic and socioeconomic, chronic disease management, and timeliness of services on patient attitudes and satisfaction.
The results indicated that the occupation of patients had a significant impact on their attitude and satisfaction. Compared with farmers, teachers tended to consider CDM services helpful to their health. Nevertheless, they were less likely to satisfy with the current services. According to surveys by the National Bureau of Statistics (China), teachers generally receive a higher level of education than farmers do. Previous studies have shown that education is negatively correlated with satisfaction (34). We, therefore, speculated that different attitudes and satisfaction between teachers and farmers may be caused by different levels of education: teachers may have higher expectations and therefore higher standards for good CDM services. However, CDM services in China are currently in the process of transferring from hospital care to primary healthcare (35). In this context, primary healthcare institutions can only provide basic care, such as blood pressure measurement. This is especially the case in rural areas where the shortage of professional health workers is substantial. The significant gap between provision and patient expectation may result in lower satisfaction. Therefore, the professional competence of healthcare professionals, as well as a sufficient number of healthcare professionals and equipment, are critical during the construction of primary healthcare institutions. For integrating chronic disease management services, the “Hospital-Community” model has been adopted to deepen cooperation between the hospital and primary healthcare institutions in many urban areas in south-eastern China (4, 36). However, it is relatively lacking in rural areas. To improve the quality of service for chronic disease management, more attention should be paid to search for more effective and permanent ways for improving the professional ability of healthcare professionals in rural areas in the subsequent research and work plan.
Findings also revealed that patients who were aware of free services were more likely to be satisfied with CDM services than those who did not know. With the rapid development of China, the investment in essential public health services (EPHSs) has also been increasing. The per capita funding standard has increased from 15 RMB in 2009 to 55 RMB in 2018, and the type of services has increased rapidly (37, 38). Patients go to primary healthcare institutions to receive free chronic disease services, which varied substantially to reduce the in-hospital healthcare financial burden (38). These gaps may cause changes in patient behaviors and satisfaction. It is possible for patients to accept these services and be satisfied after they are aware of the content of EPHS. Therefore, while improving the quality of EPHS services, it is also necessary to strengthen publicity so that more people can know the content of service projects and increase the effectiveness of primary healthcare institutions. Although previous traditional media have a positive effect on health promotion, with the coverage of the network, the influence of new media should not be underestimated. It can also be promoted through short videos, in addition to interpersonal networks, such as doctors, family and friends, and village bulletin boards (3).
Finally, the study found that the timely service of primary healthcare institutions had a close relationship with patient attitude and satisfaction. Timely service provision was significantly correlated with a more positive attitude and higher satisfaction than that was not delivered timely. Chronic diseases are usually with longer causes and were cured slowly, and patients have more opportunities to seek health services from healthcare providers (24). It means that timely service could not only solve the patient's problems but also give them psychological comfort. Previous studies reported that the health level of local residents is determined by healthcare institutions (38). However, the medical resources of rural and urban areas vary greatly. According to reports, the health professionals in urban areas were 10.87 per 1,000 population, but only 4.28 in 2017 (39). Therefore, in order to achieve better results, the government needs to place more investment in the construction of primary healthcare institutions.
Patient adherence is critical in chronic disease management. The attitudes toward chronic disease management and satisfaction with the result of chronic disease control are inextricably linked to their adherence. In this study, we intend to identify factors that influence patient attitudes toward chronic disease management and satisfaction with the result of chronic disease control. The study showed that factors such as awareness, service utilization, timeliness, and initiative of health institutions all have a significant effect on patient attitudes and satisfaction. Based on the survey results, we recommend that the government increase the promotion of chronic disease management services in rural areas (traditional media and new media), provide diversified services to meet the needs of more people, and pay more attention to the timeliness of health services.
This study has several limitations. First, participants only include patients affected by chronic hypertension and/or diabetes, which may neglect patients affected by other chronic diseases. Next, factors such as the self-assessment of household income levels and timeliness of health services are very subjective and difficult to estimate. We have to assume that the evaluation criteria for each participant are the same in the analysis. Finally, patients' attitudes toward chronic disease management and satisfaction with the result of chronic disease control may be affected by the attitudes of the servant, but we have not taken them into account.
The datasets presented in this article are not readily available because the data involves personal privacy, please consult the corresponding author for more details. Requests to access the datasets should be directed to RH, aHlzMTk4MTA2MTJAMTYzLmNvbQ==.
The studies involving human participants were reviewed and approved by Xinxiang Medical College Ethics Committee (ID: XMU71804159). The patients/participants provided their written informed consent to participate in this study.
BL and RH designed and planned the study. YL and YZ analyzed the data and drafted the article. All authors participated in the survey, completed the data acquisition, participated in data analysis and result interpretation, carefully revised all contents of the manuscript, critically reviewed, and approved the submitted manuscript.
Thanks to all research participants for their contributions to the research, including investigators and staff.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer XG declared a shared affiliation with author(s) YL, YZ, XS, and RH to the handling editor at the time of the review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Beaglehole R, Epping-Jordan J, Patel V, Chopra M, Ebrahim S, Kidd M, et al. Alma-ata: rebirth and revision 3 - improving the prevention and management of chronic disease in low-income and middle-income countries: a priority for primary health care. Lancet. (2008) 372:940–9. doi: 10.1016/S0140-6736(08)61404-X
2. Logan H, Guo Y, Dodd VJ, Muller K, Riley J. The burden of chronic diseases in a rural north florida sample. BMC Public Health. (2013) 13:906. doi: 10.1186/1471-2458-13-906
3. International Diabetes Federation,. IDF Diabetes Atlas, 8th Edn. Brussels: International Diabetes Federation. (2017). Available online at: https://diabetesatlas.org/atlas/eighth-edition/ (accessed May 13, 2019).
4. Background Information on High Blood Pressure (Hypertension),. (2019). Available online at: http://ish-world.com/public/background-info.htm (accessed May 16, 2019).
5. Tang SF, Dong D, Ji L, Fu H, Feng ZC, Bishwajit G, et al. What contributes to the activeness of ethnic minority patients with chronic illnesses seeking allied health services? A cross-sectional study in rural Western China. Int J Env Res Pub He. (2015) 12:11579–93. doi: 10.3390/ijerph120911579
6. Xie X, Wu QH, Hao YH, Yin H, Fu WQ, Ning N, et al. Identifying determinants of socioeconomic inequality in health service utilization among patients with chronic non-communicable diseases in China. PLoS ONE. (2014) 9:e100231. doi: 10.1371/journal.pone.0100231
7. Gao J, Tang SL, Tolhurst R, Rao KQ. Changing access to health services in urban China: implications for equity. Health Policy Plann. (2001) 16:302–12. doi: 10.1093/heapol/16.3.302
8. Du Q, Nass O, Bergsjo P, Kumar BN. Determinants for high maternal mortality in multiethnic populations in Western China. Health Care Women Int. (2009) 30:957–70. doi: 10.1080/07399330903052137
9. Viswanathan M, Golin CE, Jones CD, Ashok M, Blalock SJ, Wines RCM, et al. Interventions to improve adherence to self-administered medications for chronic diseases in the United States a systematic review. Ann Int Med. (2012) 157:785. doi: 10.7326/0003-4819-157-11-201212040-00538
10. Miranda ML, Casper M, Tootoo J, Schieb L. Putting chronic disease on the map: building gis capacity in state and local health departments. Prev Chronic Dis. (2013) 10:E100. doi: 10.5888/pcd10.120321
11. Epping-Jordan JE, Galea G, Tukuitonga C, Beaglehole R. Chronic diseases 2—preventing chronic diseases: taking stepwise action. Lancet. (2005) 366:1667–71. doi: 10.1016/S0140-6736(05)67342-4
12. Wagner EH. Chronic disease management: what will it take to improve care for chronic illness? Eff Clin Pract. (1998) 1:2–4.
13. Erler A, Bodenheimer T, Baker R, Goodwin N, Spreeuwenberg C, Vrijhoef HJ, et al. Preparing primary care for the future—perspectives from the Netherlands, England, and USA. Z Evid Fortbild Qual Gesundhwes. (2011) 105:571–80. doi: 10.1016/j.zefq.2011.09.029
14. Xiao NZ, Long Q, Tang XJ, Tang SL. A community-based approach to non-communicable chronic disease management within a context of advancing universal health coverage in China: progress and challenges. BMC Public Health. (2014) 14:1–6. doi: 10.1186/1471-2458-14-S2-S2
15. Yip WC, Hsiao WC, Chen W, Hu S, Ma J, Maynard A. Early appraisal of china's huge and complex health-care reforms. Lancet. (2012) 379:833–42. doi: 10.1016/S0140-6736(11)61880-1
16. Tang S, Brixi H, Bekedam H. Advancing universal coverage of healthcare in China: translating political will into policy and practice. Int J Health Plann Manage. (2014) 29:160–74. doi: 10.1002/hpm.2207
17. Sun X, Chen YC, Tong XT, Feng ZC, Wei L, Zhou DH, et al. The use of annual physical examinations among the elderly in rural China: a cross-sectional study. BMC Health Serv Res. (2014) 14:1–8. doi: 10.1186/1472-6963-14-16
18. National Sessional Public Health Service Project. Third Edition. (2017). Available online at: http://www.nhc.gov.cn/cms-search/xxgk/getManuscriptXxgk.htm?id=d20c37e23e1f4c7db7b8e25f34473e1b (accessed May 17, 2019).
19. Maimela E, Van Geertruyden JP, Alberts M, Modjadji SE, Meulemans H, Fraeyman J, et al. The perceptions and perspectives of patients and health care providers on chronic diseases management in rural south africa: a qualitative study. BMC Health Serv Res. (2015) 15:143. doi: 10.1186/s12913-015-0812-5
20. Bidaut-Russell M, Gabriel SE, Scott CG, Zinsmeister AR, Luthra HS, Yawn B. Determinants of patient satisfaction in chronic illness. Arthritis Rheum. (2002) 47:494–500. doi: 10.1002/art.10667
21. Fenton JJ, Jerant AF, Bertakis KD, Franks P. The cost of satisfaction: a national study of patient satisfaction, health care utilization, expenditures, and mortality. Arch Int Med. (2012) 172:405–11. doi: 10.1001/archinternmed.2011.1662
22. Einaudi MA, Gire C, Loundou A, Le Coz P, Auquier P. Quality of life assessment in preterm children: physicians' knowledge, attitude, belief, practice—a kabp study. BMC Pediatr. (2013) 13:58. doi: 10.1186/1471-2431-13-58
23. Tang S, Bishwajit G, Ji L, Feng D, Fang H, Fu H, et al. Improving the blood pressure control with the proactive attitude of hypertensive patients seeking follow-up services: evidence from China. Medicine. (2016) 95:e3233. doi: 10.1097/MD.0000000000003233
24. Tian MM, Wang H, Tong XT, Zhu K, Zhang XJ, Chen X. Essential public health services' accessibility and its determinants among adults with chronic diseases in China. PLos ONE. (2015) 10:e0125262. doi: 10.1371/journal.pone.0125262
25. Bastiaens H, Van Royen P, Pavlic DR, Raposo V, Baker R. Older people's preferences for involvement in their own care: a qualitative study in primary health care in 11 European countries. Patient Educ Couns. (2007) 68:33–42. doi: 10.1016/j.pec.2007.03.025
26. Burkhart PV, Sabate E. Adherence to long-term therapies: evidence for action. J Nurs Scholarship. (2003) 35:207. doi: 10.1111/j.1547-5069.2003.tb00001.x
27. Haidet P, Kroll TL, Sharf BF. The complexity of patient participation: lessons learned from patients' illness narratives. Patient Educ Couns. (2006) 62:323–9. doi: 10.1016/j.pec.2006.06.005
28. Dong XX, Liu L, Cao SY, Yang HJ, Song FJ, Yang C, et al. Focus on vulnerable populations and promoting equity in health service utilization—an analysis of visitor characteristics and service utilization of the Chinese community health service. BMC Public Health. (2014) 14:1–8. doi: 10.1186/1471-2458-14-503
29. Hamine S, Gerth-Guyette E, Faulx D, Green BB, Ginsburg AS. Impact of mhealth chronic disease management on treatment adherence and patient outcomes: a systematic review. J Med Int Res. (2015) 17:e52. doi: 10.2196/jmir.3951
30. Wong WCW, Jiang SF, Ong JJ, Peng MH, Wan E, Zhu SZ, et al. Bridging the gaps between patients and primary care in china: a nationwide representative survey. Ann Fam Med. (2017) 15:237–45. doi: 10.1370/afm.2034
31. Lancet T. China's major health challenge: control of chronic diseases. Lancet. (2011) 378:457. doi: 10.1016/S0140-6736(11)61232-4
32. Dong Ting LS-Z, Li J-P. Elderly diabetic and hypertension patients' satisfaction with nursing care in community health service centers of Sichuan Province: a 2,931-case study. J Nursing. (2017) 24:7–10. doi: 10.16460/j.issn1008-9969.2017.09.007
33. Ya-jing H. Self-management consciousness in old patients with diabetes mellitus accompanying hypertension. J Chinese PLA Postgraduate Med School. (2011) 32:170–71.
34. Batbaatar E, Dorjdagva J, Luvsannyam A, Savino MM, Amenta P. Determinants of patient satisfaction: a systematic review. Perspect Public Health. (2017) 137:89–101. doi: 10.1177/1757913916634136
35. Chen S, Burstrom B, Sparring V, Qian D. Vertical integrated service model: an educational intervention for chronic disease management and its effects in rural China—a study protocol. Bmc Health Serv Res. (2018) 18:567. doi: 10.1186/s12913-018-3355-8
36. Ma X SQ, Bao Y, Lu H, Zuo Y, Jia W. The preliminary exploration on the hospital-community management model for diabetes patients. Shanghai Med J. (2010) 33:685–7.
37. Chen S. Vertical Integrated service model: an educational intervention for chronic disease management and its effects in rural China—a study protocol. BMC Health Serv Res. (2018) 18:567.
38. Tang S MQ, Chen L, Bekedam H, Evans T. Tacking the challenges to health equality in China. Lancet. (2008) 372:1493–501. doi: 10.1016/S0140-6736(08)61364-1
39. National Bureau of Statistics(China) (2017). Available online at: http://www.stats.gov.cn (accessed May 20, 2019).
Keywords: chronic disease, cross-sectional survey, attitude, patient satisfaction, rural population
Citation: Lu Y, Zhao Y, Shangguan X, Lv B and Huang R (2022) Patient attitude and determinants toward chronic diseases control: A cross-sectional survey in rural China. Front. Public Health 10:970032. doi: 10.3389/fpubh.2022.970032
Received: 15 June 2022; Accepted: 21 September 2022;
Published: 13 October 2022.
Edited by:
Fei Sun, Michigan State University, United StatesReviewed by:
Xiang Gao, Huazhong University of Science and Technology, ChinaCopyright © 2022 Lu, Zhao, Shangguan, Lv and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Benyan Lv, bHZiZW55YW5Ac2luYS5jb20=; Rui Huang, aHlzMTk4MTA2MTJAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.