 Enzo Miranda Santos1
Enzo Miranda Santos1 Jean de Melo Silva
Jean de Melo Silva Anderson Nogueira Barbosa
Anderson Nogueira Barbosa Gemilson Soares Pontes
Gemilson Soares Pontes- 1Programa de Pós-Graduação em Hematologia, Universidade Do Estado Do Amazonas (UEA), Manaus, Amazonas, Brazil
- 2Programa de Pós-Graduação em Imunologia Básica e Aplicada—PPGIBA, Instituto de Ciências Biológicas, Universidade Federal Do Amazonas—UFAM, Manaus, Amazonas, Brazil
- 3Laboratório de Virologia e e Imunologia, Institituto Nacional de Pesquisa da Amazônia (INPA), Manaus, Amazonas, Brazil
Hemophilia is a recessive genetic disease caused by a mutation on the X chromosome that has been linked to a high risk of transfusion-transmitted infections, especially sexually transmitted infections. The purpose of this retrospective study was to characterize the clinical and epidemiological profile and describe the prevalence of sexually transmitted viral infections in patients with hemophilia in the Northern Brazilian state of Amazonas. We assessed clinical, laboratory and sociodemographic data of hemophiliac patients (n = 311) for the period 2011–2019. The majority of the study population was composed of people with a low level of education aged 21–30 years old. The prevalence of HCV, HBV, and HTLV-1/2 infections among the study population were 10.52, 0.52, and 1.05%, respectively. No HIV infection was found among the patients. Between 2011 and 2015 the prevalence of HCV increased by over 100% and the incidence peaked in 2013. The severe hemophilia was associated with the presence of inhibitor factor (Odds Ratio [OD] 9.83; 95% IC: 3.41–27.62, p < 0.0001) or target joint (OD 6.59; 95% IC: 3.27–13.34, p < 0.0001). The presence of inhibitor was positive and significantly correlated with HCV infection (r = 1.00, p < 0.0001). Our results showed that HCV infection is highly prevalent in patients with hemophilia and might be involved in the development of inhibitors. Thus, these data provide new insights into the clinical and epidemiological profile of patients suffering from hemophilia in the Northern Brazilian state of Amazonas.
Introduction
Coagulopathies affect a considerable number of individuals worldwide and hemophilia represents the most common inherited hemorrhagic disorder (1). Hemophilia is a sex-linked disorder, characterized by the impairment of the blood clotting process (2, 3). In some cases, this disorder arises due to a de novo mutation (not inherited) and also due to the development of autoantibodies (known as inhibitors) against coagulation factors (1, 4, 5). Hemophilia A is the most frequent subtype, characterized by the deficiency of coagulation factor VIII, while hemophilia B refers to a deficiency of coagulation factor IX (6).
Hemophilia affects ~189,514 people around the world. Hemophilia A occurs in one of every 5,000–10,000 male births, while the prevalence of hemophilia B is one of every 30,000–40,000 male births (7). In absolute numbers, Brazil has the fourth-largest population of patients with hemophilia in the world, which is comprised of 10,821 individuals with hemophilia A and 2,139 with hemophilia B (8, 9). In the Northern Brazilian state of Amazonas, it is estimated that 274 people live with hemophilia A and 37 with hemophilia B (9).
During the 1980s, most hemophiliac patients in Brazil were treated with cryoprecipitate, fresh frozen plasma and plasma-derived clotting factor concentrates. These treatments put patients at high risk of acquiring many blood-borne infectious diseases, such as HIV and hepatitis C (10). Only in 1994, the government of Brazil starts to import the viral inactivated factors VIII (FVIII) and IX (FIX), which resulted in the decrease of blood-transmitted viruses in hemophiliac patients (6, 11). However, the recombinant factor FVIII (rFVIII) became available in Brazil just in 2013 (6). According to the Brazilian Ministry of Health, the prevalence of sexually transmitted infections among people with hemophilia is 1.14% (HIV), 0.97% (HBV), 3.97% (HCV), and 0.1% (HTLV-1/2). However, these numbers are not accurate when prevalence rates are assessed based on Brazilian regions, especially in the north region (12, 13).
The Amazonas is the largest state in Brazil, composed of 62 municipalities, with an estimated population of 4 million people (14). Around 311 patients live with hemophilia in the Amazonas according to the Hematology and Hemotherapy Foundation of Amazonas (HEMOAM). Nevertheless, the clinical epidemiological profile of these patients is unknown. Thus, the purpose of this study was to describe the clinical and epidemiological characteristics and the prevalence of sexually transmitted viral infections in patients living with hemophilia in the Brazilian state of Amazonas.
Materials and methods
Ethical aspects
This study was approved by the Human Research Ethics Committee of the Hematology and Hemotherapy Hospital Foundation of Amazonas (approval number: 3.328.121). Confidentiality was assured to all participants. All analyses were performed following relevant guidelines and regulations.
Study population
This was an observational retrospective study conducted with hemophiliac patients treated at the Hospital Foundation of Hematology and Hemotherapy of Amazonas (HEMOAM). A total of 311 patients with a previous diagnosis of hemophilia A (n = 274) and B (n = 37) were included. Clinical and socio-demographic information was collected from the hospital's electronic databases. The study population was comprised of patients of either sex and different ethnicities who were aged from 1 to 92 years old.
Obtention of clinical records
To obtain the clinical data related to viral infections, the patient's clinical records related to the 2011–2019 period were acquired from the Hemovida Web Coagulopathies system. The following information was collected from June 2019 to March 2020: date of birth, date of sample collection, sex, age, results of laboratory tests, comorbidities, treatment, and patient's residence. Patients with incomplete clinical data were excluded from the study.
Statistical analysis
Descriptive analysis was used to evaluate the total number of patients according to sociodemographic information and the prevalence of viral infections. Prevalence ratio (PR) was used for associations between hemophilia and viral prevalence rates, while the Odds ratio (OR) analysis was used for the associations between the severity of hemophilia and the presence of inhibitor or target joint. OR and PR analyses were done through the chi-square test and Yate's correction with a 95% confidence interval (CI) calculated by the method Koopman asymptotic score and Baptista-Pike, respectively. Spearman's test was applied to assess the correlation between disease severity and the presence of inhibitor, target joint, or positivity for HCV. The correlation was considered strongly positive when r > 0.7 All analyzes were performed using the GraphPad Prism v8.0.1 software and values p < 0.05 were considered significant.
Results
Sociodemographic characteristics of the study population
We analyzed clinical and sociodemographic data of 311 (292 men and 19 women) patients from the northern Brazilian state of Amazonas who have hemophilia. Of those, 88.10% (n = 274) had hemophilia A and 11.90% (n = 37) hemophilia B. Among individuals with hemophilia A, 95.26% (n = 261) were men and 4.73% (n = 13) were women, while for hemophilia B, 83.78% (n = 31) were man and 16.22% (n = 6) were women (Table 1). The mean age observed in patients with hemophilia A was 26.29 ± 15.22 years and 31.49 ± 16.01 years in patients with hemophilia B. The majority of the study population self-identified as brown-skinned (57.56%) and single (57.88%). Regarding the level of education, over 50% of patients did not complete their elementary education. Only 16.08% (n = 50) of the study population graduated from high school as the highest education degree (Table 1).
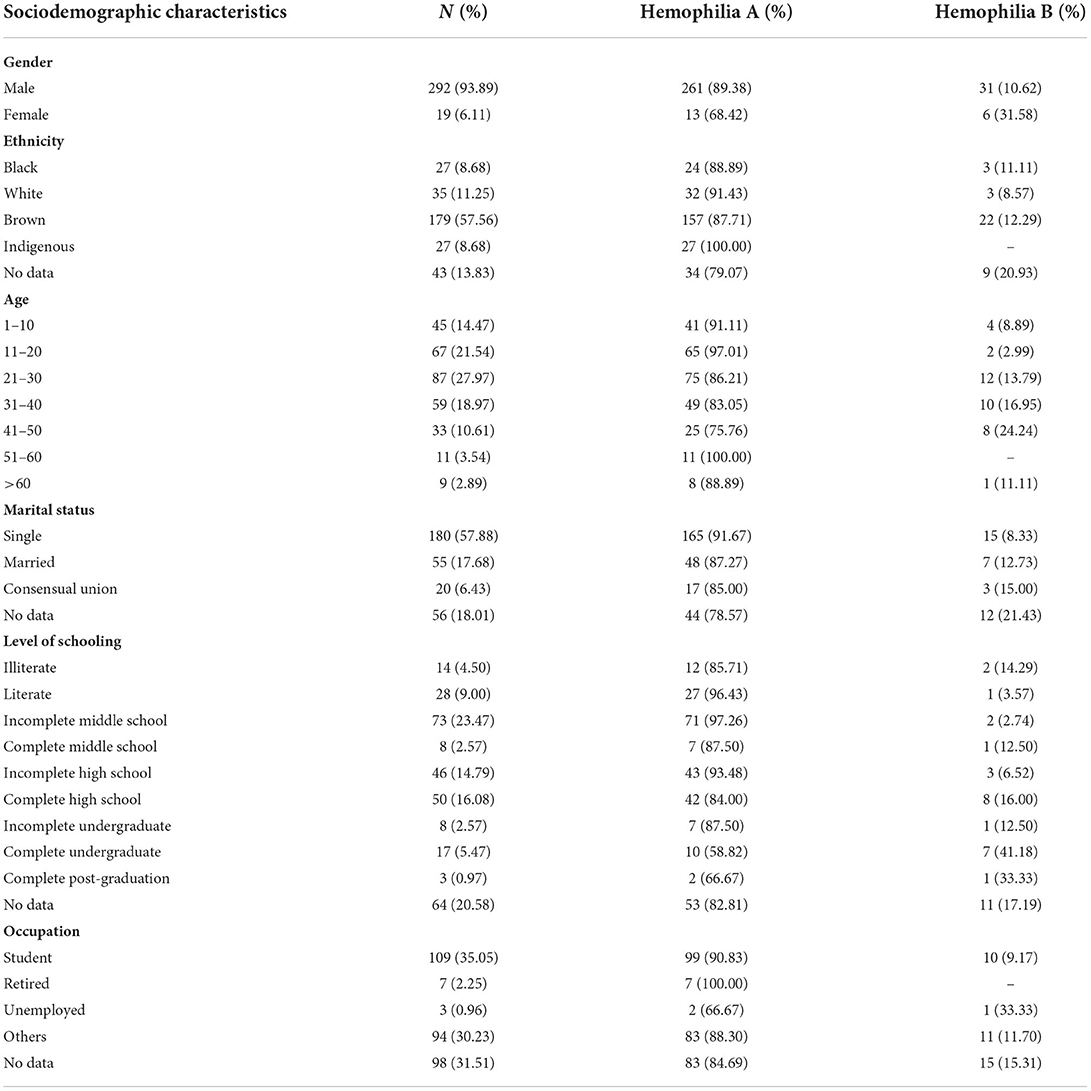
Table 1. Sociodemographic profile of hemophiliac patients.
The state of Amazonas consists of 62 municipalities. The study population comprises patients of 21 municipalities, the majority (65%) living in the city of Manaus, the capital of the state of Amazonas. The remaining 35% of the study population resides in small towns situated in the countryside of the state. Jutaí (n = 13) and Tefé (n = 11) were the municipalities in the countryside with the highest number of hemophiliac patients (Figure 1). No residency information was found for 24 patients.
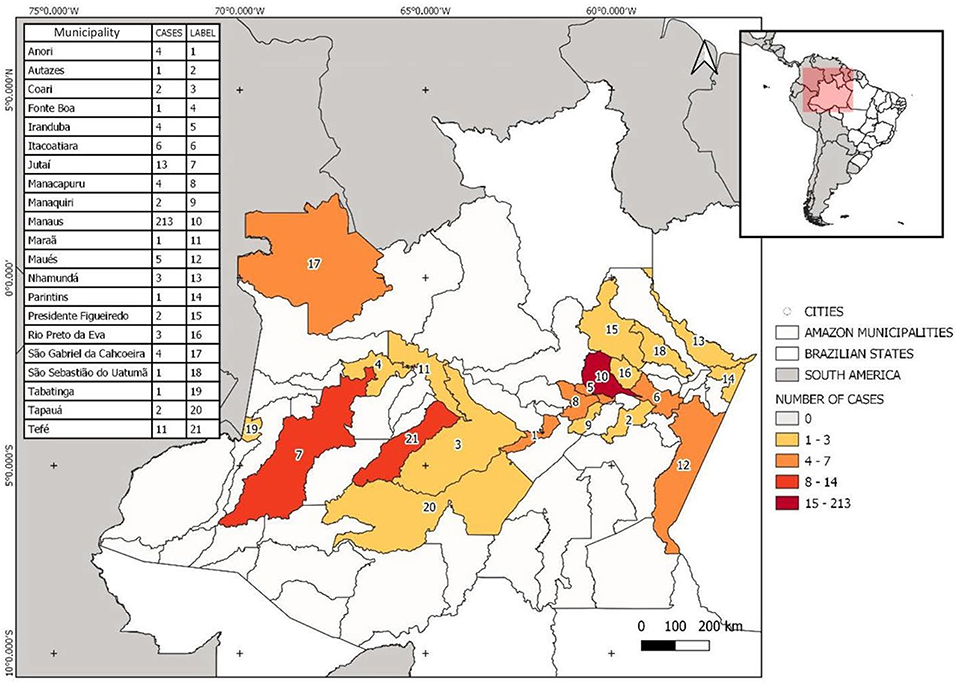
Figure 1. Site map showing the distribution of hemophiliac patients per location within the state of Amazonas. The map was built using the WGS1984 datum (worldclim software v.2.0).
Epidemiological profile of blood-borne viruses
Only 190 patients had the laboratory records available. Overall, the prevalence of blood-borne viruses was 12.10% (n = 23). The majority of those infected were men aged 31–40 years old (n = 22) (Figure 2A). Only one woman showed seropositivity for HCV infection, which was the most widespread viral infection (10.45%) in the study population (Supplementary Table 1). Two patients showed seropositivity for HTLV-1/2 (1.05%) and only one patient (0.52%) was positive for HBV infection (laboratory results were positive for anti-HBsAg, anti-HBc and molecular diagnostic). No HIV infection was found in the study population.
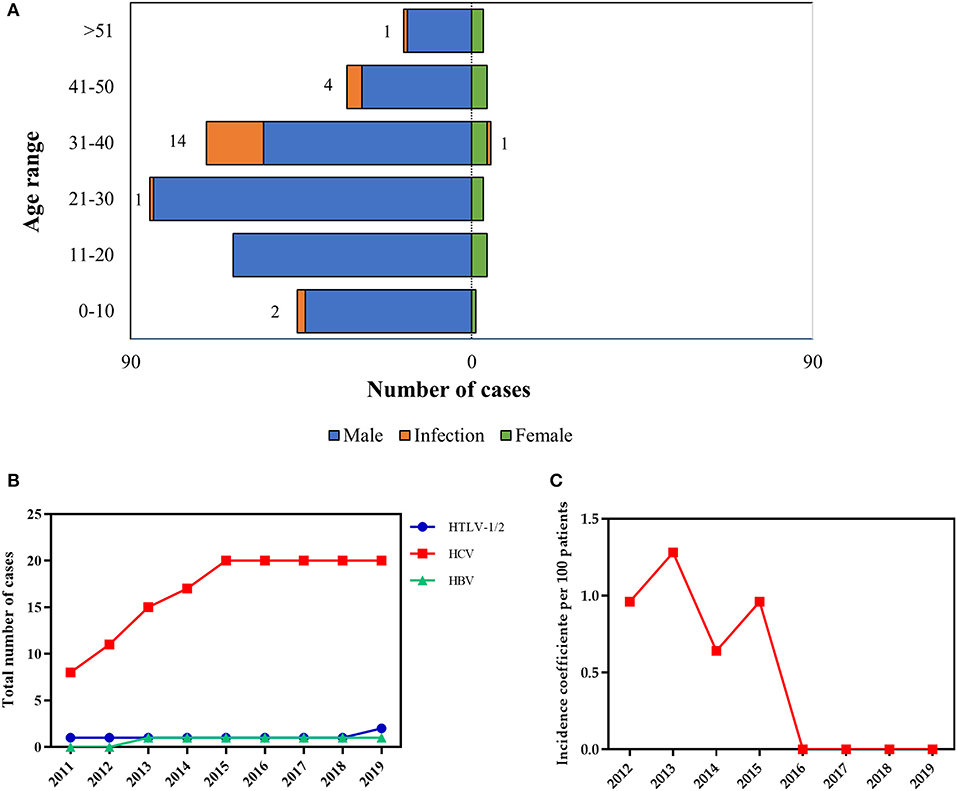
Figure 2. Prevalence and incidence rates of viral infections in patients with hemophilia. (A) Numbers of viral infections according to age and sex. (B) prevalence HTLV 1/2, HCV, and HBV and (C) incidence coefficient of HCV infection according to age.
Next, we evaluated viral infection prevalence rates from 2011 to 2019 (2020 and 2021 data were not yet available, likely as a result of the coronavirus pandemic). Prevalence rates of HCV infection rose by over 100% between 2011 and 2015, after stabilizing through 2019 (Figure 2B). When we looked at the HCV incidence during the same period, the incidence coefficient (per 100 patients) ranged from 0.68 to 1.28% (Figure 2C). The incidence of HCV infection peaked in 2013.
Clinical aspects related to hemophilia severity
The bivariate analysis carried out to check the correlation between severity, HCV infection, inhibitor and target joint showed that all factors are highly and positively correlated (Figure 3). However, only the correlation between HCV infection and the presence of autoantibodies was statistically significant (r = 1.00, p < 0.0001). Thus, the presence of HCV infection may be a predisposing factor for the development of inhibitors in the context of hemophilia.
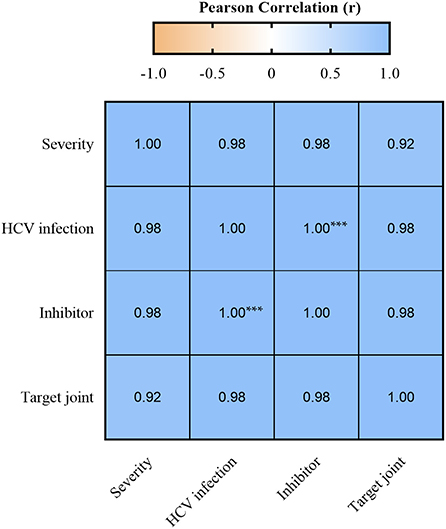
Figure 3. Pearson's correlation between HCV infection, inhibitor, target joint, and severity. Values of r > 0.7 were considered strong positive. ***p < 0.0001.
When we looked at the activity of the circulating coagulation factor, we found that 20 patients (7.43%) had autoantibodies (inhibitors), with 16 (80%) of them having severe hemophilia (Table 2). In addition, a total of 46 patients (16.73%) had the clinical condition target joint and 33 (69.57%) of them were suffering from severe hemophilia. The presence of inhibitors was directly associated with severe hemophilia (OD 9.83; 95% IC: 3.41–27.62, p < 0.0001), as was the target joint (OD 6.59; 95% IC: 3.27–13.34, p < 0.0001) (Table 2).
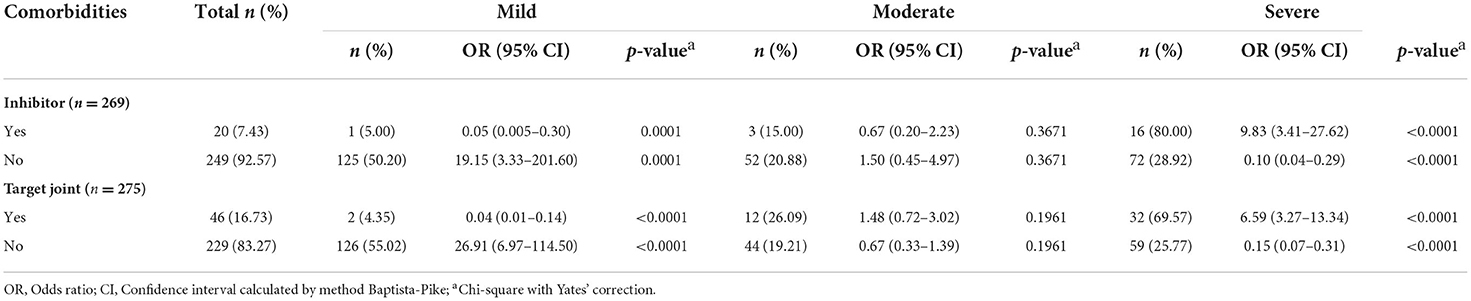
Table 2. Association between presence of comorbidities and severity of hemophilia.
Discussion
Epidemiological characteristics of hemophilia in Brazil are still overlooked and poorly described, especially in the Amazonian region. This study outlined epidemiological and clinical aspects of patients suffering from hemophilia in the Northern Brazilian state of Amazonas. Our findings showed that most of the hemophiliac patients in the state of Amazonas consist of unmarried brown-skinned men aged 20–29 years old, with low levels of education and economic status. The frequency of hemophilia observed among women was similar to elsewhere in Brazil and the world (7, 9). The degree of education can influence the clinical prognostic and treatment adherence when associated with other socioeconomic variables (15, 16).
Treatment adherence is a big challenge in the Amazonas state since hemophilia treatment centers exist only in the capital of Amazonas and the majority of small towns in the countryside are at a great distance from Manaus (17). In many cases, long river travel is the only means of transportation available to access health services. As described earlier, 35% of the study population is from hard-to-reach cities, which can undermine the treatment and medical support. This situation may put these patients at high risk of acquiring infectious diseases and developing hemophilia-related comorbidities. However, we found no significant association between these factors and the increase of susceptibility to infectious diseases or the development of comorbidities.
The study population showed an overall prevalence of 12.10% for blood-borne viruses and the most prevalent virus was HCV (10.45%). In Brazil, the prevalence of HCV has been estimated between 0.69 and 1.89%, with a total of 265.815 cases notified in the 1999–2020 period (18–21). Before 1993, HCV and HBV infections were highly prevalent among patients with hemophilia, which dramatically changed after the implementation of mandatory serological and molecular screening during blood donations (6, 13, 22). Nowadays, the estimated seroprevalence for HCV infection in patients with hemophilia is around 3.6% (9). In this study, only one patient was positive for HBV (0.52%), even though the Western Brazilian Amazon is considered highly prevalent for HBV infection (23). The incidence of HCV infection hit its peak in 2013 and the highest prevalence rate was observed in 2015 when the reporting process for hepatitis C cases in Brazil was changed (21). The medical records of the patients did not show any clinical manifestations related to HCV infection, but we emphasize that the laboratory follow-up is not carried out regularly. Considering HCV infection, there is a risk of developing hepatocellular carcinoma in this population, mainly due to the silent evolution (24–28). Our findings also suggest an association between HCV infection and the development of inhibitors.
Some patients with hemophilia A during the administration of FVIII-containing products can develop autoantibodies (inhibitors) against the FVIII factor. The presence of these inhibitors reduces the patient's response to FVIII replacement, resulting in episodes of bleeding that are difficult to control (29). Although the mechanism of inhibitor development in patients with hemophilia is still not completely understood, several factors might be involved such as family history, ethnicity, FVIII gene mutation type, treatment intensity and other unknown environmental factors (30, 31). Our results showed a direct association between positivity for HCV and the presence of inhibitors. Although there are reports of an association between HCV infection and autoantibody development, the present study provides new information on the influence of HCV infection on the development of inhibitors that should be further investigated in more detail (32, 33).
Although our study did not include the patient's genetic aspects or environmental factors, we believe that these factors can influence the severity of the disease, contributing to the development of inhibitors that inactivate the clotting factors. Some studies reported that aspects such as age at the first treatment and intensity of treatment at the first doses are capable of contributing to the worsening of hemophilia (30, 34). Physical aspects can lead to the involvement of some joints. For example, young hemophiliac patients from Taiwan who had a higher degree of obesity were more prone to develop spontaneous joint injuries (35). In this study, we found that the presence of inhibitor and joint target were directly associated with the severity of hemophilia. The factors associated with the presence or development of these comorbidities need further investigation to improve the clinical management of the hemophiliac patient.
HTLV-1/2 infection was found in two patients. Brazil has the largest absolute number of HTLV-1/2 infections in the world and the prevalence varies depending on the region and the population group, ranging from 0.04 to 1% among blood donors (36). North and Northeast regions concentrate the highest rates (37). According to the Ministry of Health, the prevalence of HTLV-1/2 in hemophiliacs is estimated as 0.12% for hemophilia A and 0.10% for hemophilia B (22). Our study showed that the prevalence of HTLV-1/2 (1.14%) in the study population is higher than in the Brazilian population in general. These data indicate that the susceptibility to acquiring HTLV-1/2 infection may be increased in the study population. However, additional studies are required to better clarify the epidemiological aspects of HTLV-1/2 infection among hemophiliac patients in the State of Amazonas.
Although our results propose new data regarding viral infections in hemophiliacs in Amazonas, with results never described before, we understand the limitations of our study, such as the lack of updated epidemiological data, which makes it difficult to obtain complete data. New computer systems have been proposed to organize the sociodemographic data of all patients, especially hemophiliacs (38). The prevalence of HCV and HTLV 1/2 is still above the national average, and further epidemiological studies are needed with a focus on this population to better understand the clinical aspects. Our results demonstrate that some infectious diseases have high prevalence rates. In addition, the absence of routine serological tests is still frequent in the hemophiliac population. Hemophiliac patients in Amazonas have higher prevalence rates for HCV and HTLV 1/2, compared to other population groups, which reveals the need for further studies to provide a better assessment of the hemophiliac population. This study improves the current knowledge on hemophilia epidemiology in the Amazon region, which is important to evaluate factors that can influence the disease prognosis. Also, our findings may help the patient clinical management at the individual and collective levels.
Limitations in this study included the use of secondary data, the possibility of underreporting infections and incorrect records. The quality of monitoring systems varies between regions in Brazil and can have a direct impact on data quality. Generally, underreporting is most pronounced in more vulnerable areas where the access to health services is lower. Furthermore, another limitation is that the diagnosis of HCV is not categorized in the system by the method (serologic or molecular), which makes no distinction between active infections and previous infections.
Conclusions
In conclusion, this study demonstrated that HCV infection is widespread and could be involved in the induction of inhibitor development in hemophiliac patients of the Amazonas state. The presence of inhibitor or target joints is associated with hemophilia severity. Our findings also draw attention to the specific characteristics of the Amazonian region such as the socio-economic status of the population and the difficulty to reach places, which could impact the treatment adherence and prognosis of hemophilia. Our results enhance the current knowledge on the epidemiology of hemophilia, which is important for assessing factors that may influence the disease's prognosis and may help the clinical management of patients both individually and collectively.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were reviewed and approved by Human Research Ethics Committee of the Hematology and Hemotherapy Hospital Foundation of Amazonas. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author contributions
Conceptualization: GP and ES. Methodology and Investigation: ES, JS, and AB. Validation, data curation, writing-review and editing: GP and AB. Formal analysis and resources: GP, ES, and AB. Writing—original draft preparation: ES and JS. Supervision, project administration and funding acquisition: GP. All authors contributed to the article and approved the submitted version.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior- Brasil (CAPES)- Finance code PROCAD AMAZÔNIA 88881.200581/201801, Pró-Estado Program (#007/2018 and #005/2019) and FAPEAM – POSGRAD 2021.
Acknowledgments
The authors acknowledge the Fundação de Hematologia e Hemoterapia do Amazonas and Fundação de Amparo à Pesquisa do Estado do Amazonas (FAPEAM–Pró-Estado Program) for all support provided during this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.963790/full#supplementary-material
References
1. Peyvandi F, Jayandharan G, Chandy M, Srivastava A, Nakaya SM, Johnson MJ, et al. Genetic diagnosis of haemophilia and other inherited bleeding disorders. Haemophilia. (2006) 12:82–9. doi: 10.1111/j.1365-2516.2006.01263.x
2. Garcés MF, Linares A, Sarmiento IC, Caminos JE. Molecular study in children with hemophilia A in Colombia: analysis of intron 1 and 22 inversion using long-distance PCR technique. Rev Fac Med. (2017) 65:245–51. doi: 10.15446/revfacmed.v65n2.57012
3. Roussel NA. Gaining insight into the complexity of pain in patients with haemophilia: state-of-the-art review on pain processing. Haemophilia. (2018) 24:3–8. doi: 10.1111/hae.13509
5. Franchini M, Gandini G, Di Paolantonio T, Mariani G. Acquired hemophilia A: a concise review. Am J Hematol. (2005) 80:55–63. doi: 10.1002/ajh.20390
6. Ferreira A, LEITE I, Bustamante-Teixeira MT, Guerra M. Hemophilia A in Brazil—epidemiology and treatment developments. J Blood Med. (2014) 5:175. doi: 10.2147/JBM.S68234
8. Guedes VG, Thomas S, Wachholz PA, Souza SAL. Challenges and perspectives in the treatment of patients with haemophilia in brasil. Rev Assoc Med Bras. (2018) 64:872–5. doi: 10.1590/1806-9282.64.10.872
9. Brasil. Prevalência das Coagulopatias Hereditárias e demais transtornos hemorrágicos por diagnóstico, Brasil, 2019. (2020). 27 p.
10. Tabor E. The epidemiology of virus transmission by plasma derivatives: clinical studies verifying the lack of transmission of hepatitis B and C viruses and HIV type 1. Transfusion. (1999) 39:1160–8. doi: 10.1046/j.1537-2995.1999.39111160.x
11. Fontes EMA, Amorim L, Carvalho SM, Farah MB. Hemophilia care in the state of Rio de Janeiro, Brazil. Pan Am J Public Heal. (2003) 13:124–8. doi: 10.1590/S1020-49892003000200013
12. Brasil. Perfil das Coagulopatias Hereditárias no Brasil: 2015. 1st ed. In: Ministério da Saúde, editor. Brasília (2017). 68 p.
13. Silva TPS. Avaliação da Qualidade de vida relacionada à saúde em pacientes com hemofilias A e B atendidos na Fundação Hemominas—Minas Gerais. Fundação Oswaldo Cruz (2015). 74 p.
14. Instituto Brasileiro de Geografia e Estatistica (IBGE). População estimada. Dir Pesqui Coord Popul e Indicadores Sociais, Estim da Popul Resid com data Ref 1o julho 2019 (2020).
15. Carneiro JDA, Blanchette V, Ozelo MC, Antunes S V, Villaca PR, Young NL, et al. Comparing the burden of illness of haemophilia between resource-constrained and unconstrained countries: the São Paulo–Toronto Hemophilia Study. Haemophilia. (2017) 23:682–8. doi: 10.1111/hae.13230
16. Salomon T, Chaves DG, Brener S, Martins PRJ, Mambrini JVM, Peixoto S V. Determining the health-related quality of life in individuals with haemophilia in developing economies: results from the Brazilian population. Haemophilia. (2017) 23:42–9. doi: 10.1111/hae.13130
18. Pereira LMMB, Martelli CMT, Moreira RC, Merchan-Hamman E, Stein AT, Cardoso RMA, et al. Prevalence and risk factors of Hepatitis C virus infection in Brazil, 2005 through 2009: a cross-sectional study. BMC Infect Dis. (2013) 13:1–12. doi: 10.1186/1471-2334-13-60
19. Wedemeyer H, Duberg AS, Buti M, Rosenberg WM, Frankova S, Esmat G, et al. Strategies to manage hepatitis C virus (HCV) disease burden. J Viral Hepat. (2014) 21:60–89. doi: 10.1111/jvh.12249
20. Bruggmann P, Berg T, Øvrehus ALH, Moreno C, Brandão Mello CE, Roudot-Thoraval F, et al. Historical epidemiology of hepatitis C virus (HCV) in selected countries. J Viral Hepat. (2014) 21:5–33. doi: 10.1111/jvh.12350
21. Brasil Ministério da Saúde. Boletim epidemiológico: hepatites virais 2021. (2021). Available online at: https://www.gov.br/saude/pt-br/media/pdf/2021/julho/26/boletim-epidemiologico-de-hepatite-2021.pdf (accessed March 5, 2022). p. 1–80.
22. Brasil. Perfil das Coagulopatias Hereditárias: 2016. 1st ed. In: Ministério da Saúde, editor. Brasília (2018). p. 57.
23. Lampe E, Mello FCA, do Espírito-Santo MP, Oliveira CMC, Bertolini DA, Gonçales NSL, et al. Nationwide overview of the distribution of hepatitis B virus genotypes in Brazil: a 1000-sample multicentre study. J Gen Virol. (2017) 98:1389–1398. doi: 10.1099/jgv.0.000789
24. Villar LM, Milagres FAP, Lampe E, Cruz HM, de Scalioni P, de Magalhães AFM, et al. Determination of hepatitis B, C and D prevalence among urban and Amerindian populations from the Eastern Brazilian Amazon: a cross sectional study. BMC Infect Dis. (2018) 18:1–19. doi: 10.1186/s12879-018-3279-2
25. Jardim LL, van der Bom JG, Caram-Deelder C, Gouw SC, Leal Cherchiglia M, Meireles Rezende S. Mortality of patients with haemophilia in Brazil: first report. Haemophilia. (2019) 25:e146–52. doi: 10.1111/hae.13730
26. Thalappillil A, Ragni MV, Comer DM, Yabes JG. Incidence and risk factors for hepatocellular cancer in individuals with haemophilia: a national inpatient sample study. Haemophilia. (2019) 25:221–8. doi: 10.1111/hae.13668
27. Giouleme O, Paschos P, Katsoula A, Panteliadou K, Vakalopoulou S, Garipidou V. Hepatitis C infection in a Greek population with inherited bleeding disorders. Haemophilia. (2018) 24:e74–6. doi: 10.1111/hae.13427
28. Pimentel JPD. Hepatite C em pacientes hemofílicos: perfil imunológico e caracterização dos diferentes genótipos virais. Universidade Federal do Amazonas (2009). 86 p.
29. Jardim LL, Chaves DG, Rezende SM. Development of inhibitors in hemophilia A: an illustrated review. Res Pract Thromb Haemost. (2020) 4:752–60. doi: 10.1002/rth2.12335
30. Garagiola I, Palla R, Peyvandi F. Risk factors for inhibitor development in severe hemophilia A. Thromb Res. (2018) 168:20–7. doi: 10.1016/j.thromres.2018.05.027
31. Gouw SC, van den Berg HM, Le Cessie S, van der Bom JG. Treatment characteristics and the risk of inhibitor development: a multicenter cohort study among previously untreated patients with severe hemophilia A. J Thromb Haemost. (2007) 5:1383–90. doi: 10.1111/j.1538-7836.2007.02595.x
32. Marconcini ML, Fayad L, Shiozawa MBC, Dantas-Correa EB, De Lucca Schiavon L, Narciso-Schiavon JL. Autoantibody profile in individuals with chronic hepatitis C. Rev Soc Bras Med Trop. (2013) 46:147–53. doi: 10.1590/0037-8682-0039-2013
33. Clifford BD, Donahue D, Smith L, Cable E, Luttig B, Manns M, et al. High prevalence of serological markers of autoimmunity in patients with chronic hepatitis C. Hepatology. (1995) 21:613–9. doi: 10.1002/hep.1840210302
34. Peyvandi F, Garagiola I. Product type and other environmental risk factors for inhibitor development in severe hemophilia A. Res Pract Thromb Haemost. (2018) 2:220–7. doi: 10.1002/rth2.12094
35. Chang C-Y, Li T-Y, Cheng S-N, Pan R-Y, Cheng C-N, Wang H-J, et al. Obesity and overweight in patients with hemophilia. J Chinese Med Assoc. (2019) 82:289–94. doi: 10.1097/JCMA.0000000000000047
36. Murphy EL, Cassar O, Gessain A. Estimating the number of HTLV-2 infected persons in the world. Retrovirology. (2015) 12:05. doi: 10.1186/1742-4690-12-S1-O5
37. Rosadas C, Miranda AEB, Gonçalves DU, Caterino-de-Araújo A, Assone T, Ishak R. Prevalência da infecção por HTLV-1/2 no Brasil. (2020). 25–33 p.
Keywords: hemophilia, prevalence, HTLV, HCV, autoantibodies, Amazonas
Citation: Santos EM, Silva JdM, Barbosa AN and Pontes GS (2022) Clinico-epidemiological and sociodemographic profile of patients with hemophilia in the Brazilian Amazon: High prevalence of hepatitis C infection and its possible corrrelation with inhibitor development. Front. Public Health 10:963790. doi: 10.3389/fpubh.2022.963790
Received: 07 June 2022; Accepted: 19 August 2022;
Published: 08 September 2022.
Edited by:
Maria Da Conceição Almeida, Gonçalo Moniz Institute (IGM), BrazilReviewed by:
Guenka Ivanova Petrova, Medical University Sofia, BulgariaLuiz Fernando Almeida Machado, Federal University of Pará, Brazil
Copyright © 2022 Santos, Silva, Barbosa and Pontes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gemilson Soares Pontes, Z2VtaWxzb24ucG9udGVzQGlucGEuZ292LmJy