
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 24 August 2022
Sec. Children and Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.961613
 Xingdi Yang1,2,3Jianjuan Zeng4Yiping Gu1,2,3Yiming Fang1,2,3Caiyun Wei1Shengkui Tan1,2,3*
Xingdi Yang1,2,3Jianjuan Zeng4Yiping Gu1,2,3Yiming Fang1,2,3Caiyun Wei1Shengkui Tan1,2,3* Xiaoying Zhang1,2,3*
Xiaoying Zhang1,2,3*Objectives: Birth defects (BDs) are a major contributor to perinatal and infant mortality, morbidity and lifelong disability worldwide. A hospital-based study on birth defects was designed in Guilin city in the Guangxi province of Southwestern China aiming to determine the prevalence of BDs in the studied region, and the classify the BDs based on clinical presentation and causation.
Methods: The study involved BDs among all pregnancy outcomes (live births, stillbirths, death within 7 days, and pregnancy terminations) born in the 42 registered hospitals of Guilin between 2018 and 2020. The epidemiological characteristics of BDs and the etiologic profile of BDs were evaluated in this study.
Results: Of the total 147,817 births recorded during the study period, 2,003 infants with BDs were detected, giving a total prevalence rate of 13.55 per 1,000 births. The top five BD types were congenital heart defects, polydactyly, syndactyly, malformations of the external ear, and talipes equinovarus, whereas, neural tube defects, congential esophageal atresia, gastroschisis, extrophy of urinary bladder, were the least common BD types in these 3 years. Only 8.84% of cases were assigned a known etiology, while most cases (91.16%) could not be conclusively assigned a specific cause.
Conclusion: This study provides an epidemiological description of BDs in Guilin, which may be helpful for understanding the overall situation in Southwest China of BDs and aid in more comprehensive studies of BDs in future healthcare systems, including funding investment, policy-making, monitor, prevention. Strong prevention strategies should be the priority to reduce BDs and improve the birth quality.
Birth defects (BDs) are defined as structural, functional, and/or biochemical-molecular anomalies that occur during the development of the embryo or fetus (1–3). BDs remain a major contributor to perinatal and infant mortality, morbidity and lifelong disability worldwide, and represent a major public health problem because they cause substantial personal, social, and financial burden, in addition to having a considerable impact on the population quality and social development (4, 5).
Hospital-based and population-based surveillance are the two main types of national BD surveillance systems (4, 6). In China, most BD research data are obtained from hospital-based systems (6, 7). According to the requirements of the Ministry of Health of China, the “Maternal and Child Health Monitoring Manual in China” monitors BDs among all early fetuses <28 weeks of gestation and perinatal infants between 28 weeks of gestation and 7 days after birth who are born in hospitals, and also collects maternal information, such as age, gravidity, parity, and physical condition (1, 3).
The overall prevalence of BDs might have increased, and approximately 3–5% of births worldwide are affected by BDs (2, 4). In China, the prevalence of BD ranges from 0.715 to 19.184% (8). Recently, increase attention has been paid to BDs in low-income provinces of southwestern China. Guilin is an underdeveloped city in the low-income province of Guangxi in southwestern China. In 2019, its cumulative gross domestic product was approximately CN ¥ 210.556 billion, which was much lower than the national per capita value in the same period, ranking 132 in mainland China, and becoming one of the key BD surveillance spots.
Furthermore, commonly used BD classification schemes were International Statistical Classification of Diseases and Related Health Problems (ICD), such as 9th or 10th revision (ICD-9, or ICD-10) (2, 9, 10). ICD is the standard used globally to classify diseases including birth defects. They based on clinical presentation, typically organized by anatomy or function, they are valuable for general purposes such as studies on morbidity and mortality, but not ideal in the evaluation of etiologies (2). Thus, we conducted a study to describe the epidemiological characteristics of BDs in Guilin between 2018 and 2020, along with classification of BDs based on clinical presentation and etiologic profile of BDs.
The data source for this study was the “Maternal and Child Health Monitoring Manual in China” from Guilin between 2018 and 2020; 42 hospitals were registered in the system. In this retrospective study, we only used the monitoring data without contacting or identifying the patients.
BDs were diagnosed by physical examination, ultrasonography, X-ray examination, and/or genetic diagnostic methods, based on the Chinese National Criteria of Birth Defects and Tiny Deformities and the clinical modification codes as congenital malformations, deformations, and chromosomal abnormalities (codes Q00–Q99) of ICD-10 (1, 6, 10). Experts from each registered hospital were responsible for the diagnostic confirmation and provision of technical support. Trained gynecological and pediatric or neonatal doctors were responsible for filling the case card of each infant with BD in the “Birth Defects Registration Form,” and uploading it into the surveillance system both on paper and online. In addition, each case card recorded maternal information (including her age, gravidity, parity, education, economic status, physical condition, and medication use during pregnancy), and we used this information to analyze the potential etiological profile of BDs in this study.
The study involved BDs among all pregnancy outcomes (live births, stillbirths, death within 7 days, and pregnancy terminations) during perinatal period (between 28 weeks of gestation and seven days after birth) born in the 42 registered hospitals of Guilin. Live births included singleton, twin and multiple live births. Stillbirth was defined as fetal death at 28 weeks estimated gestational age or more. Death within 7 days included neonatal death within the first 7 days after birth. If pregnant women with a prenatal diagnosis of a defective fetus wanted to terminate their pregnancies, they had to go to medical institutions that were qualified for prenatal diagnosis, and their medical records of BDs had to be ascertained and filled in the registration forms for BDs.
The studies were reviewed and approved by the Medical Ethics Committee of Guilin Medical University (number: GYLL2021012).
In this study, we first classified BDs based on the ICD-10 system to better understand the epidemiological characteristics of BDs (1, 10). Thus, nine categories were involved in the classification as the research outcome. The nine categories were the nervous system, the eyes, ears, face, and neck, the digestive system, the genital and urinary organs system, the musculoskeletal system, the circulatory system, the respiratory system, genetic abnormality, and other BD types. Infants with BDs from more than one defect category were included in each applicable major defect category (4).
In this study, we further implemented an etiological (known, unknown) classification to systematically capture the etiology of BDs. Briefly, the known etiology included four main criteria: genetic, environmental, gene-environment interactions and twinning (2, 11–15). The genetic etiology included chromosomal abnormalities (number and structure), single gene abnormalities and family history of malformations (2, 13, 16, 17). Environmental etiology included various types of environmental exposure recognized as human teratogens, such as, maternal infections (such as viruses, bacteria, and protozoa) (2, 12, 18), maternal medications (such as antibiotics and valproic acid) (2), occupational exposure (such as X-ray, agricultural pesticides, chemicals) (12), maternal illness (such as diabetes) (2, 19), and maternal smoking or alcohol (12, 13), or multiple known environmental factors exposures. Gene-environment interactions etiology included complex genetic and environmental interactions such as mother had family history of malformations as well as environmental exposure (14, 15). The twinning etiology included acardiac and conjoined twins (2).
Statistical analyses were performed using SPSS version 22.0. The prevalence rates of BDs were calculated as the total number of infants with BD cases (live births, stillbirths, death within 7 days, pregnancy terminations) divided by the total number of births (live births and stillbirths). The prevalence rates of BDs were calculated both across all years and for each year separately. The prevalence rates of different types of BDs were calculated and ranked in a descending order, separately. Infants with BDs from more than one defect category were included in each applicable major defect category for classification and ranking (4). The chi-square test was used to test the between-group differences. The etiological classification of birth defects was shown as case counts in each category. P < 0.05 was considered statistically significant.
This hospital-based study included 2,003 infants with BDs from among a total of 147,817 infants, giving a total prevalence rate of 13.55 per 1,000 births. The prevalence rate of BDs increased from 12.61 per 1,000 births (706/56,006) in 2018 to 15.53 per 1,000 births (648/41,740) in 2020 (overall: χ2 = 17.21, P = 0.000; 2018 vs. 2019: χ2 = 0.27, P = 0.61; 2019 vs. 2020: χ2 = 10.74, P = 0.001; 2018 vs. 2020: χ2 = 14.92, P = 0.000; Table 1). In this study, two time periods for diagnosis, i.e., “prenatal diagnosis” and “postpartum diagnosis within 7 days” were defined for BD screenings, and most BDs were diagnosed in live births in the time period of “postpartum diagnosis within 7 days.” Thus, “postpartum diagnosis within 7 days” was the main diagnosis time period for screening BDs in Guilin (Table 1).
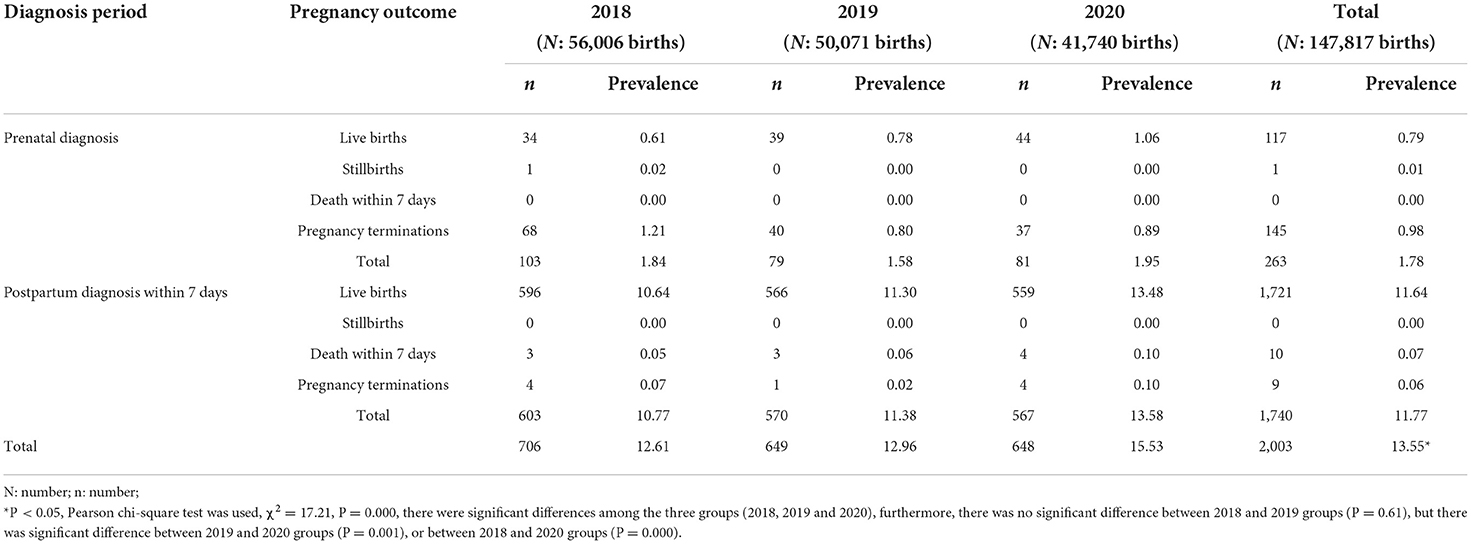
Table 1. Birth defects counts and prevalence (per 1,000 births) stratified by pregnancy outcome at different two diagnosis periods in Guilin, 2018–2020.
We found that the most common BDs involved the circulatory, musculoskeletal, facial, urogenital, genetic and digestive systems (Table 2). In the 3 years from 2018 to 2020, the five most common BDs were congenital heart defects (CHD), polydactyly, syndactyly, malformations of the external ear, and talipes equinovarus, with total prevalence rates of 3.43, 3.22, 1.14, 1.08, and 0.91 per 1,000 births, respectively. The total prevalence rate of CHD was the highest among all BDs, and its annual prevalence rate increased from 2.61 per 1000 births in 2018 to 4.56 per 1000 births in 2020 significantly, which is a significant increase (overall: χ2 = 26.48, P = 0.000; 2018 vs. 2019: χ2 = 5.80, P = 0.016; 2019 vs. 2020: χ2 =7.51, P = 0.006; 2018 vs. 2020: χ2 = 26.41, P = 0.000; Table 2). Among the CHD cases, the top five common subtypes of CHD in Guilin (2018–2020) were atrial septal defect, patent ductus arteriosus, ventricular septal defect, atrioventricular septal defect and Tetralogy of Fallot (Supplementary Table 1). However, neural tube defects (NTD), congential esophageal atresia, gastroschisis, extrophy of urinary bladder, were the least common BDs in these 3 years (total prevalence: 0.04, 0.03, 0.02, and 0.01 per 1,000 births, respectively). The overall prevalence rates and ranks of all observed BDs are presented in Table 2.

Table 2. Prevalence rates of different types of birth defects in Guilin, 2018–2020 (per 1,000 birth).
Overall, 8.84% of cases were assigned a known etiology; among the known etiology group, 177 cases were further classified into genetic etiology (97/177), environmental etiology (74/177), and gene-environmental etiology (6/177) (Table 3). As shown in Table 3, cases with a known etiology were mostly associated with chromosomal abnormalities (n = 54, 30.51%), family history (n = 34, 19.21%), maternal diabetes (n = 30, 16.95%), and maternal infection (n = 22, 12.43%). However, most cases (91.16%) could not be conclusively assigned a specific cause, which underscored the current knowledge gaps and challenges in BD prevention.
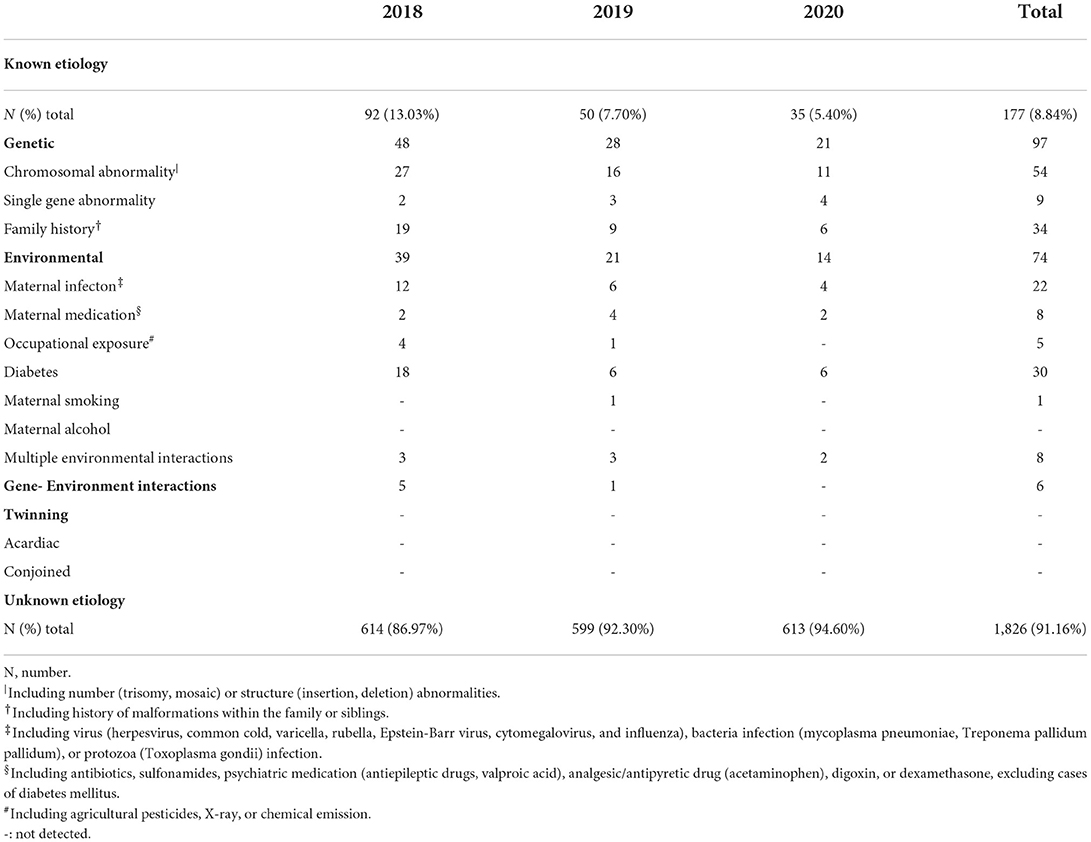
Table 3. Etiologic classification of birth defects in Guilin, 2018–2020.
In this hospital-based study, we used Guilin City's perinatal BD monitoring data to describe the epidemiological characteristics of common BDs and review the etiological identification of these BDs in Guilin, Guangxi province, China. The total prevalence of BDs was 13.55 per 1,000 births from 2018 to 2020, which was lower than the prevalence rate of 19.53 per 1,000 births in Liuzhou, another city in Guangxi (20).
Among the BDs, we found that CHD was the most common type of BD and its prevalence rate increased from 2.61 per 1000 births in 2018 to 4.56 per 1,000 births in 2020, the increase trend was consistent with the results of most previous studies in China and other countries (1, 9, 21). This phenomenon can be explained to some extent by the increasing proportion of older pregnant women, increasing social or natural environmental pressure, improvement in diagnostic techniques, for example, B-ultrasound, and advances in the ascertainment of CHD (1, 9). Although CHD was the most common type of BD in Guilin, the prevalence of CHD (total: 3.43 per 1,000 births) was still much lower than the global rate of 8–10 per 1,000 births (9). The low prevalence of CHD in Guilin may be due to several reasons. First, specialized BD monitoring and diagnosis centers in Guilin hospitals are underserved, with a scarcity of professional B-ultrasound physicians and specialist clinics, which can also be observed in other underdeveloped cities or countries. Second, in our study, data were collected from 28 weeks of gestation to 7 days after birth; however, some CHD cases may not be discovered during this period. Herein, CHD cases were mostly detected in the “Postpartum diagnosis within 7 days” (89.15%) (Supplementary Table 2). In the USA, the follow-up time for CHD cases is up to at least 1 year or without age limitation (4, 9). Third, some low-income pregnant women delivered in the hospital without any prenatal or postpartum diagnosis of CHD, resulting in missing or incomplete information. Our finding indicate that government should take action to reduce the prevalence of CHD: prioritize the prevention investment of BDs in healthcare system, promote CHD diagnosis and monitoring techniques innovations, strengthen training of related physicians in underdeveloped cities, narrow gaps of techniques between developed and underdeveloped cities/regions, increasing women's awareness of CHD.
Anencephaly, spina bifida and encephalocele, which are the three main types of neural tube defects (NTDs) (5, 22, 23). Mandatory folic acid supplementation is highly likely to be responsible for the NTDs being one of the least common BDs, which had also been observed in our study and other reports (3, 22). Forci K et al. (22) reported that a prevalence rate of NTD in Moroccan (2011–2016) was 1.00 per 1,000 births, which was a lower rate than those reported by previous Moroccan studies (e.g. 2008–2011: 1.21–2.18 per 1,000 births), and the decrease in NTDs in Morocco was due to the folic acid supplementation since 2008. Xie D et al. (3) reported that the prevalence rate of NTD in Hunan province of China declined from 1.44 per 1,000 births in 2005 to 0.33 per 1,000 births in 2014 since the Chinese government prompted folic acid supplement (3). In this study, we also found that the total prevalence rate of NTD in Guilin city of China was 0.04 per 1,000 births (2019–2020), this low prevalence rate was also due to the mandatory folic acid supplementation in Guilin since 2009. For example, in our study, about 99.00% of pregnant women in the 42 registered hospitals were supplemented with folic acid in 2019 (data not shown). NTD cases were always detected by prenatal diagnostic tests and followed by therapeutic termination of pregnancy (3, 22). Five of the six NTD cases (83.55%) in our study were diagnosed antenatally; all five cases (100%) underwent a pregnancy termination procedure (Supplementary Table 3). Furthermore, NTD cases have been reported to be associated with other malformations, and the rate of NTD-associated malformations varies from 12% to over 80% (5, 22, 24). In our study, half of the NTD cases (three cases) had multiple malformations, one anencephaly associated with cleft lip and palate, one spina bifida associated with congenital atresia of the rectum and anus, and one encephalocele with craniotabes (Supplementary Table 3), which demonstrate the importance of improving the prenatal diagnosis to reduce fetal BDs. Together, this study suggest that the prevention and control strategies implemented by the Ministry of Health should be further strengthen by enforcing folic acid supplementation, increasing women's awareness of BDs, providing more adequate medical care for pregnancy women, such as prenatal diagnosis (22).
Another highlight of this study was that we classified the common BDs according to their etiology. Determination of etiology is crucial for focusing research efforts on understanding the current gaps in knowledge, controlling the risk factors, and strengthening preventive measures. Few studies have attempted to estimate the proportion of BDs with or without a known etiology. In this study, we considered the etiology as known only if there was conclusive evidence that the etiology was associated with BD. However, some well-known risk factors, such as epidemiologic indicators (older age, multiple pregnancies, etc.), may be applicable to populations, but not to individual cases; therefore, these risk factors were not considered as known etiological factors (2). Twinning is another important criterion of known etiology (2), but we had no twinning sample; therefore, in this study, identifiable etiology consisted of genetic etiology, environmental etiology, and gene-environment interactions etiology. More and more attention has been paid to the role of gene-environment interactions as one of the causes for BDs (14, 15). In our study, six cases (6/2003) were found to be exposed to gene-environment interactions. Unfortunately, only 177 cases (8.84%) were assigned a known etiology in Guilin in 2018–2020, and the low proportion of BDs with known etiology may be attributed to several reasons. The first reason may be the low level of economic and technological development in Guilin; for example, although an increasing in the prevalence of genetic abnormalities in CHD patients was reported recently (2, 9), only 1 in 507 CHD patients underwent genetic testing in Guilin (data not shown). Second, there was incomplete data collection and specialists in registered hospitals did not record some exposures (such as maternal infection, medication, pregestational diabetes) or query relevant information. Third, most BDs are caused by complex gene-environment interactions, and the causes of these BDs are still unknown (11). There are large gaps in the current knowledge on the causes of BDs, which underscores the importance of accelerating basic and translational research.
In conclusion, this study provides an epidemiological description of BDs in Guilin: a total prevalence rate of BDs was 13.55 per 1,000 births, CHD was the top common type of BD (3.43 per 1,000 births), while NTD was well controlled, and the prevalence rate was only 0.04 per 1,000 births; 177 cases were assigned a known etiology, including genetic etiology, environmental etiology, and gene-environmental etiology. These data may be helpful for understanding the overall situation of BDs in Southwest China and aid in more comprehensive studies of BDs in future healthcare systems, including funding investment, policy-making, monitor, prevention. In order to reduce BDs, improve the birth quality, and promote developmental health, government should prioritize the prevention investment of BDs in healthcare system, promote diagnosis and monitoring techniques innovations, narrow gaps of techniques between developed cities/regions and underdeveloped cities/regions. And the prevention strategy implemented by the Ministry of Health should be further strengthen by enforcing essential nutrients (such as folic acid) supplementation, increasing women's awareness of BDs, providing more adequate medical care for pregnancy women, such as prenatal diagnosis.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Medical Ethics Committee of Guilin Medical University. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
ST and XZ contributed to data collection, analysis, interpretation, and manuscript preparation, full access to all of the data in the study and serves as the guarantor of the manuscript. XY, JZ, YG, YF, and CW collected the data, analyzed the data, and manuscript preparation. XZ and CW obtained fundings. All authors contributed to the study conception, design, and read and approved the final manuscript.
This study was funded by the National Natural Science Foundation of China (82160620), the Science and Technology Base and Talent Project of Guangxi Province (AD19245006), and the National College Students Innovation and Entrepreneurship Training Program (202110601027).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.961613/full#supplementary-material
BD, Birth defect; CHD, congenital heart defect; NTD, neural tube defect.
1. Zhou Y, Mao X, Zhou H, Wang L, Qin Z, Cai Z, et al. Birth defects data from population-based birth defects surveillance system in a district of Southern Jiangsu, China, 2014–2018. Front Public Health. (2020) 8:378. doi: 10.3389/fpubh.2020.00378
2. Feldkamp ML, Carey JC, Byrne JLB, Krikov S, Botto LD. Etiology and clinical presentation of birth defects: population based study. BMJ. (2017) 357:j2249. doi: 10.1136/bmj.j2249
3. Xie D, Yang T, Liu Z, Wang H. Epidemiology of birth defects based on a birth defect surveillance system from 2005 to 2014 in Hunan Province, China. PLoS ONE. (2016) 11:e0147280. doi: 10.1371/journal.pone.0147280
4. Mai CT, Isenburg JL, Canfield MA, Meyer RE, Correa A, Alverson CJ, et al. National population-based estimates for major birth defects, 2010–2014. Birth Defects Res. (2019) 111:1420–35. doi: 10.1002/bdr2.1589
5. Oumer M, Tazebew A, Silamsaw M. Birth prevalence of neural tube defects and associated risk factors in Africa: a systematic review and meta-analysis. BMC Pediatr. (2021) 21:190. doi: 10.1186/s12887-021-02653-9
6. Xiong L, Chen Q, Wang A, Kong F, Xie D, Xie Z. The differences of population birth defects in epidemiology analysis between the rural and urban areas of Hunan Province in China, 2014–2018. Biomed Res Int. (2021) 2021:2732983. doi: 10.1155/2021/2732983
7. Dai L, Zhu J, Liang J, Wang YP, Wang H, Mao M. Birth defects surveillance in China. World J Pediatr. (2011) 7:302–10. doi: 10.1007/s12519-011-0326-0
8. Wang QQ, He CY, Mei J, Xu YL. Epidemiology of birth defects in Eastern China and the associated risk factors. Med Sci Monit. (2022) 28:e933782. doi: 10.12659/MSM.933782
9. Zhang Y, Zhang W, Xu H, Liu K. Epidemiological aspects, prenatal screening and diagnosis of congenital heart defects in Beijing. Front Cardiovasc Med. (2021) 8:777899. doi: 10.3389/fcvm.2021.777899
10. Lin YJ, Chiou JY, Huang JY, Su PH, Chen JY, Yang HJ. A comparative prevalence of birth defects between newborns of immigrant and native-born mothers in Taiwan: ten years of population-based data. Int J Environ Res Public Health. (2021) 18:12530. doi: 10.3390/ijerph182312530
11. Baldacci S, Gorini F, Santoro M, Pierini A, Minichilli F, Bianchi F. Environmental and individual exposure and the risk of congenital anomalies: a review of recent epidemiological evidence. Epidemiol Prev. (2018) 42:1–34. doi: 10.19191/EP18.3-4.S1.P001.057
12. Garland MA, Reynolds K, Zhou CJ. Environmental mechanisms of orofacial clefts. Birth Defects Res. (2020) 112:1660–98. doi: 10.1002/bdr2.1830
13. World Health Organization. Birth Defects. Available online at: https://www.who.int/news-room/fact-sheets/detail/birth-defects (accessed February 28, 2022).
14. Addissie YA, Troia A, Wong ZC, Everson JL, Kozel BA, Muenke M, et al. Identifying environmental risk factors and gene-environment interactions in holoprosencephaly. Birth Defects Res. (2021) 113:63–76. doi: 10.1002/bdr2.1834
15. Moreau JLM, Kesteven S, Martin E, Lau KS, Yam MX, O'Reilly VC, et al. Gene-environment interaction impacts on heart development and embryo survival. Development. (2019) 146:dev172957. doi: 10.1242/dev.172957
16. Talati AN, Webster CM, Vora NL. Prenatal genetic considerations of congenital anomalies of the kidney and urinary tract (CAKUT). Prenat Diagn. (2019) 39:679–92. doi: 10.1002/pd.5536
17. Feghali J, Marinaro E, Xie Y, Chen Y, Li S, Huang J. Family history in chiari malformation type I: presentation and outcome. World Neurosurg. (2020) 142:e350–6. doi: 10.1016/j.wneu.2020.06.238
18. Mawson AR, Croft AM. Rubella virus infection, the congenital rubella syndrome, and the link to autism. Int J Environ Res Public Health. (2019) 16:3543. doi: 10.3390/ijerph16193543
19. Tinker SC, Gilboa SM, Moore CA, Waller DK, Simeone RM, Kim SY, et al. Specific birth defects in pregnancies of women with diabetes: national birth defects prevention study, 1997–2011. Am J Obstet Gynecol. (2020) 222:176 e1–e11. doi: 10.1016/j.ajog.2019.08.028
20. Huang X, Chen J, Zeng D, Lin Z, Herbert C, Cottrell L, et al. The association between ambient air pollution and birth defects in five major ethnic groups in Liuzhou, China. BMC Pediatr. (2021) 21:232. doi: 10.1186/s12887-021-02687-z
21. Zhang X, Sun Y, Zhu J, Zhu Y, Qiu L. Epidemiology, prenatal diagnosis, and neonatal outcomes of congenital heart defects in eastern China: a hospital-based multicenter study. BMC Pediatr. (2020) 20:416. doi: 10.1186/s12887-020-02313-4
22. Forci K, Bouaiti EA, Alami MH, Mdaghri Alaoui A, Thimou Izgua A. Incidence of neural tube defects and their risk factors within a cohort of Moroccan newborn infants. BMC Pediatr. (2021) 21:124. doi: 10.1186/s12887-021-02584-5
23. Wang B, Pang Y, Zhang Y, Zhang L, Ye R, Yan L, et al. Thorium and fetal neural tube defects: an epidemiological evidence from large case-control study. Genes Environ. (2021) 43:51. doi: 10.1186/s41021-021-00227-w
Keywords: birth defects, hospital-based surveillance, epidemiology, etiology, congenital heart defects, neural tube defects
Citation: Yang X, Zeng J, Gu Y, Fang Y, Wei C, Tan S and Zhang X (2022) Birth defects data from hospital-based birth defect surveillance in Guilin, China, 2018–2020. Front. Public Health 10:961613. doi: 10.3389/fpubh.2022.961613
Received: 05 June 2022; Accepted: 08 August 2022;
Published: 24 August 2022.
Edited by:
Guodong Ding, Shanghai Children's Hospital, ChinaReviewed by:
Rui Zhang, The Affiliated Hospital of Qingdao University, ChinaCopyright © 2022 Yang, Zeng, Gu, Fang, Wei, Tan and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shengkui Tan, eHNrdGFuMjAwOEBzaW5hLmNu; Xiaoying Zhang, eGlhb3lpbmd6aGFuZzc5QDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.