 Yongkang Wang
Yongkang Wang Weizhong She2
Weizhong She2 Guijun Chi
Guijun Chi Junsheng Wang
Junsheng Wang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 21 October 2022
Sec. Public Mental Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.961361
This article is part of the Research Topic Global Excellence in Public Mental Health: Asia and Australasia Volume II View all 13 articles
Background: Despite the positive relationship between self-rated health and general physical activity, very little research has touched upon the relationship between self-rated health and vigorous physical activity. Such research will help to promote self-rated health among adolescents by addressing the close relationship between self-rated health and the components of physical activity.
Purpose: In this study, the relationship between self-rated health and vigorous physical activity among Chinese adolescents were analyzed.
Methods: The current study was based on a collaborative survey conducted by the WHO in several nations, and the data generated by Health Behavior in School-aged Children every 4 years on health behavior were adopted. The school class was taken as a basic unit for sampling. Cluster sampling was performed systematically, and the possibility was proportional to the population. The sampling was conducted to collect typical cases. The class teachers were informed of the sampling activities, and they were to collect data on the students by distributing the questionnaires.
Results: The research included 116,828 respondents from 36 countries. Among them, 51.82% were girls and 48.18% were boys. A total of 98.54% of the respondents considered their health status as fair or above when completing the questionnaire, while 1.46% believed that their health status was poor. Moreover, more than 86% of the respondents participated in vigorous exercise more than weekly, and better self-health ratings were found among respondents who exercised more than weekly (once a week: OR = 1.95, CI: 1.86–2.04; two or three times a week: OR = 1.69, CIL: 1.63–1.76; four or six times a week: OR = 1.30, CI: 1.25–1.35). Certain respondents reported better results for self-rated health (4–6 h every week: OR = 1.36, CI: 1.30–1.43; 2 or 3 h every week: OR = 1.48, CI: 1.42–1.55; 1 h every week: OR = 1.64, CI: 1.57–1.72).
Conclusion: In this study, empirical evidence is provided for the relationship between self-rated health and vigorous physical activity among adolescents. From the results, it can be observed that there is a positive relationship between self-rated health and vigorous physical activity among adolescents.
Self-rated health (SRH) has been identified as a standard measure for evaluating perceived health status in public health surveys (1). SRH refers to one's perception of one's overall health status, physical health and mental health (2, 3). SRH is usually measured by using a five- or four-point Likert Scale, which can indicate one's perceived health status (2). According to the World Health Organization (WHO), SRH is more important than traditional morbidity and mortality in evaluating health outcomes in adolescents (4–7). SRH consists of several components, such as general physical functioning, psychological health and health behaviors (8). In numerous previous studies, SRH has been proved to be an important indicator of several health outcomes, including body fatness (9), mental health (10, 11), morbidity (12) and mortality (13, 14). Accordingly, a high prevalence of poor SRH has been well-documented in previous studies (15–17). For example, a population-based survey indicated that 11% of participants rated their health as poor and a decline in SRH with age was found among adolescents residing in urban areas (15). In another large sample survey, 20.9% of Iranian adolescents rated their SRH as poor (17). However, data from a longitudinal cohort study demonstrated that a generally high (%) SRH was reported in Swedish adolescents, especially in boys (18). Furthermore, gender differences in SRH were also found in the previous studies, where boys reported higher SRH than girls (15, 18). By contrast, one Chinese cross-sectional study revealed that the gender differences in SRH were not significant among Chinese adolescents (19). In addition, data from the Health Behavior in School-aged Children (HBSC) survey indicated that more adolescents reported higher SRH and boys rated their health as better than girls.
The positive association between health-related behaviors such as physical activity (PA) and health outcomes has been well-documented in previous studies (20–23). PA is an important predictor of self-perceived health in adolescents (24). Thus, results from a review study showed that most of the included cross-sectional studies reveal that high PA is associated with better SRH in adolescents (8, 25). Furthermore, only four studies did not report a significant association between physical activity and SRH in children and adolescents, which can be explained by the limitations of the studies' designs (8). In addition, a dose-response association between PA and SRH was reported in this review, which indicated that higher PA is linked with higher SRH (8). For example, data from one cross-sectional study indicated that, compared with adolescents recognized to be physically inactive, those adolescents who participated in PA every day were over 11-times more likely to rate their perceived health as “good or excellent” (OR: 11.5; 95% CI: 2.0–65.8) (26). Similarly, one Canadian study also revealed that more physically active adolescents were more likely to report “very good or excellent” SRH than their inactive peers (11). A longitudinal study also reported similar findings (3, 27). For instance, a prospective study (with 4 years of follow-up) revealed that adolescents with insufficient PA tended to rate their perceived health as “poor” (3, 28).
There are an increasing number of researchers showing that an increase in PA from moderate to vigorous plays a critical role in preventing non-communicable diseases (NCDs), such as type II diabetes, cardiovascular disease, obesity and some cancers (29–31). Despite the positive associations between overall PA and SRH, few studies have focused on the relationship between vigorous PA (VPA) and SRH. Identifying strong associations between different types of PA and SRH could be beneficial for the promotion of intense PA in adolescents. Therefore, the present study aimed to explore the association between VPA and SRH in adolescents using public data.
For the implementation of “Health Behavior in School-aged Children” (HBSC), a cross-sectional study was conducted and relevant research was performed according to the international HBSC protocol (32). This was a collaborative survey by the WHO that was conducted across different nations, and data on health behavior were collected using the HBSC regularly, that is, every 4 years. The samples are representative of adolescents aged between 11 and 15 years in the nation. The class at the school was considered a basic sampling unit. The cluster sampling was systematic, and the probability was proportional to the population. The sampling was performed to obtain samples that were representative of the nation. The teachers of the classes to be sampled were informed, and they collected information on the students by sending them information sheets. There was a brief introduction to the survey on the information sheets, and the students gave the sheets to their guardians or parents. If students refused to take the survey, then they were required to sign opt-forms and give them back. The data were collected anonymously, and standard measures were also taken to protect the students' private information. The teachers responsible for the survey were well-trained, and they sent a self-compiled, anonymous and standard questionnaire to the respondents. The specific information on the protocol, the theoretical framework and the purpose of the international research are described elsewhere (33, 34). Based on the survey performed in 2013 and 2014, the feedback rate was 85% and above in most of the schools and classes and among most of the students (35). The data were collected randomly, and the respondents were representative of the nation; there were 108,666 girls and 105,414 boys.
To measure VPA, the two questions below were asked. The first one was “how often did you do a workout by which you sweat or get out of breath after class?” The answers included never, less than once a month, once a month, once a week, 2 to 3 times a week, 4 to 6 times a week and every day. The second one was “how long did you spend on a workout after class by which you sweat or get out of breath?” The answers included about 7 h or more, about 4 to 6 h, about 2 to 3 h, about 1 h, about half an hour and none. The reliability and validity of the questions were tested several times and determined to be good, as described elsewhere (36, 37).
Self-rated health was assessed using a Likert response scale, with a single question — “Would you say your health is…?”—and a four-point response scale was used including the categories excellent, good, fair and poor. SRH is a standardized indicator that has frequently been used in various areas of health research (38, 39).
Information on the study participants' sex, age and country were included as covariates, in line with previously published studies (40, 41). These variables were adjusted for further statistical analysis.
Statistical Package Social Science (SPSS) version 23.0 was used for all the statistical analyses in this study. Descriptive analysis was used to report the sample characteristics; percentages and means with standard deviations are used to describe categorical and continuous variables. An ordinal regression model within a generalized linear model was used to establish the association between independence and outcome. After excluding missing cases of variables included in this study, 116,828 samples were included for final analysis. Parameters on model fit and diagnosis were also reported. The significance of the statistical test was set up as p < 0.05.
Table 1 presents the sample characteristics of this study. According to Table 1, 116,828 participants from 36 countries were involved in this research, of which 48.18% were boys and 51.82% were girls. In terms of age composition, adolescents aged 15 made up the largest proportion of the whole sample, at 37.10%. This was closely followed by the group of adolescents aged 13, which accounted for 35.08%, while adolescents aged 11 comprised the smallest proportion of the sample, at 27.83%. Table 2 depicts the participants' results regarding their SRH and the frequency and duration of VPA per week.

Table 1. Sample characteristics of this study.
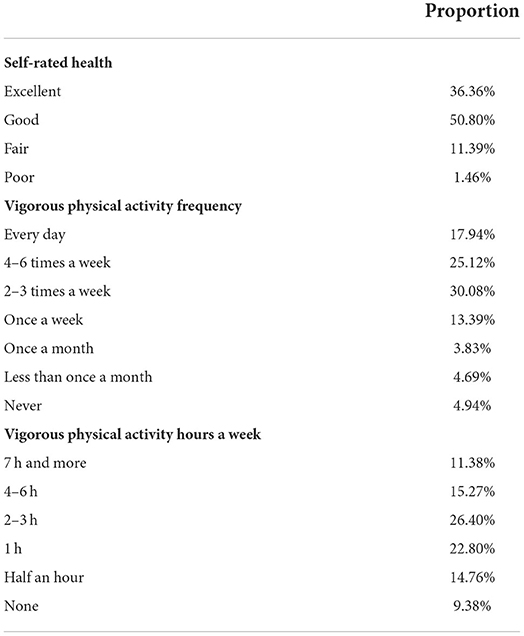
Table 2. Descriptive results for outcome and independents.
As shown in Table 2, 98.54% of the adolescents in the study gave a fair or above rating for their health, while only 1.46% of the adolescents rated their health as poor. In addition, more than 86% of the adolescents engaged in vigorous exercise at least once a week. Meanwhile, 13.46% of the adolescents had conducted vigorous exercise no more than once a month, while 4.94% had never carried out VPA. Furthermore, over 90% of the adolescents did at least half an hour of VPA per week, with the majority choosing to exercise for 2–3 h a week.
Table 3 reveals the relationship between the frequency and duration of VPA and SRH among adolescents. Generally, worse SRH was observed among participants who participated in less VPA in terms of both frequency and hours (once a week: OR = 1.95, CI: 1.86–2.04; 2–3 times a week: OR = 1.69, CI: 1.63–1.76; 4–6 times a week: OR = 1.30, CI: 1.25–1.35). In addition, less vigorously active adolescents were more likely to report worse SRH (4–6 h per week: OR = 1.36, CI: 1.30–1.43; 2–3 h per week: OR = 1.48, CI: 1.42–1.55; 1 h per week: OR = 1.64, CI: 1.57–1.72) compared with those reporting 7 h or more. The results for the covariates included in the model were also shown in Table 3.

Table 3. Results for the associations between vigorous physical activity and self-rated health.
The main aim of the present study was to analyse the association between VPA and SRH in adolescents, using public data based on a large sample size from the HBSC survey in 42 European countries. This study mainly that after controlling for some significant covariates, there was a significant association between VPA and SRH in adolescents. More specifically, more participations in VPA and more durations of VPA were both two potential contributors to adolescents' SRH. More analysis is displayed below.
The current study indicated that adolescents who reported higher levels of VPA were more likely to rate better perceptions of health. This research finding was consistent with the previous studies. Another study (42) investigated the relationship between VPA and SRH. Similarly, another study found a positive correlation between more participation in PA at higher intensity, further demonstrating the roles of VPA on SRH outcomes in adolescents. Collectively, the current study, alongside previous studies, provides new insights into the current limited knowledge of VPA and health promotion research.
Some underlying mechanisms can be used in this study for a better understanding of the roles of VPA on SRH in adolescents. A recent meta-analytical study found that VPA would contribute to physical health outcomes (43), including lower risks of adiposity and cardiovascular diseases. This review suggests that adolescents participating in more VPA are likely to be healthier than those participating in less VPA, making those with higher VPA report better SRH. In addition to physical health outcomes, emerging evidence has suggested that participating in more VPA can to some extent promote mental health and well-being (44, 45). Similar to explaining the roles of VPA on physical health indicators, owing to contributions of VPA to mental health, it is also available that adolescents who reported VPA to display better mental health, then rating better perceived overall health. Although speculative, it is reasonable to assume the positive roles of VPA in the promotion of healthy adolescents, the actual underlying mechanism explaining the association between VPA and SRH should be further clarified.
This study also suggested that adolescents reported participating less in VPA. In comparison to those in a national study, 43.06% of the adolescents reported that they participated in VPA four or more times a week, and this prevalence is similar to that of their European counterparts (ranging from 37% to 57%) (46). Compared with that in another cross-sectional study, however, the prevalence of frequent (four or more times a week) VPA in the present study was lower than that in Icelandic adolescents (64.3%) (47). In addition, 86.54% of the adolescents in the present study participated in VPA more than once a week, which is in line with a previous study (48). In the aforementioned study, 84% of American adolescents engaged in VPA more than once a week (48). Owing to the health benefits of VPA, it should be considered to increase VPA in adolescents.
Compared with previous studies, the current study focused on VPA rather than moderate to vigorous physical activity, which can add new evidence to the literature. To our knowledge, previous studies primarily laid sufficient research interest and attention on MVPA and SRH, while very few studies collected information on VPA in insolation. Our study, based on a large sample size, provides new insights into, advancing the knowledge on the associations between PA at different intensities and health outcomes in adolescents. Considering our preliminary evidence in our study, regarding VPA and SRH, it helps strengthen the current PA guidelines to include more recommendations on PA at a higher intensity. However, the research findings in the present study were based on self-reported measures, which are subject to measurement errors. Thus, research findings concerning the association between VPA and SRH may be potentially influenced. Future studies are promising to use more advanced measures to estimate the associations between VPA and SRH in adolescents.
Although the results of the present study cannot provide causal evidence, the positive relationship implies that VPA might be an important contributor to SRH in adolescents. Given the findings from the present study, there is a potential to promote SRH by increasing VPA in adolescents. Future interventional studies should explore how to increase VPA levels in adolescents.
Several limitations of the present study should be noted. First, the data included in the analysis were from a cross-sectional study, which might not provide a causal explanation for the association between VPA and self-rated health in adolescents. The second limitation is the use of self-administrated measurements, which may have contributed to the overestimation of VPA and self-rated health in adolescents.
This study provides empirical evidence for the association between VPA and self-rated health in adolescents and indicates that VPA is positively associated with self-rated health in adolescents. For efficient health promotion in adolescents, it would be better to encourage adolescents to participate in more VPA.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
All data were anonymized and publicly available; therefore no ethical approval was required. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
YW and JW: writing—original draft. JW and GC: formal analysis. YW, JW, GC, and WS: writing—review and editing. All authors contributed to the article and approved the submitted version.
This study was supported by Beijing Social Science Foundation for Youths (project number: 19YTC033): Study on Correlation between Motor Ability and Physical Health Status of Primary School Students.
The authors would like to thank the availability of data provided by the HBSC survey.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Vaez M, Kristenson M, Laflamme L. Perceived quality of life and self-rated health among first-year university students. Soc Indic Res. (2004) 68:221–34. doi: 10.1023/B:SOCI.0000025594.76886.56
2. Herman KM, Hopman WM, Sabiston CM. Physical activity, screen time and self-rated health and mental health in Canadian adolescents. Preventive Med. (2015) 73:112–6. doi: 10.1016/j.ypmed.2015.01.030
3. Breidablik HJ, Meland E, Lydersen S. Self-rated health during adolescence: stability and predictors of change (Young-HUNT study, Norway). Eu J Public Health. (2009) 19:73–8. doi: 10.1093/eurpub/ckn111
4. Currie C, Nic Gabhainn S, Godeau E. The health behaviour in school-aged children: who collaborative cross-national (HBSC) study: origins, concept, history and development 1982–2008. Int J Public Health. (2009) 54:131–9. doi: 10.1007/s00038-009-5404-x
5. Shen H, Yan J, Hong JT, Clark C, Yang XN, Liu Y, et al. Prevalence of physical activity and sedentary behavior among Chinese children and adolescents: variations, gaps, and recommendations. Int J Public Health. (2020) 17:3066. doi: 10.3390/ijerph17093066
6. Shen H, Yan J, Hong JT, Clark C, Yang XN, Liu Y et al. Prevalence and selected sociodemographic of movement behaviors in schoolchildren from low-and middle-income families in Nanjing, China: a cross-sectional questionnaire survey. Children. (2020) 7:13. doi: 10.3390/children7020013
7. Rollo S, Antsygina O, Tremblay MS. The whole day matters: understanding 24-h movement guideline adherence and relationships with health indicators across the lifespan. J Sport Health Sci. (2020) 9:493–510. doi: 10.1016/j.jshs.2020.07.004
8. Zhang T, Lu G, Wu XY. Associations between physical activity, sedentary behaviour and self-rated health among the general population of children and adolescents: a systematic review and meta-analysis. BMC Public Health. (2020) 20:9447. doi: 10.1186/s12889-020-09447-1
9. Herman KM, Sabiston CM, Tremblay A, Paradis G. Self-rated health in children at risk for obesity: Associations of physical activity, sedentary behavior, and BMI. J Phy Act Health. (2014) 11:543–52. doi: 10.1123/jpah.2012-0124
10. Sampasa-Kanyinga H, Lien A, Hamilton HA, Chaput JP. Chaput, The Canadian 24-h movement guidelines and self-rated physical and mental health among adolescents. Can J Public Health. (2021) 3:568. doi: 10.17269/s41997-021-00568-7
11. Lachytova M, Katreniakova Z, Mikula P, Jendrichovsky M, Nagyova I. Associations between self-rated health, mental health problems and physical inactivity among urban adolescents. Eu J Public Health. (2017) 27:984–9. doi: 10.1093/eurpub/ckx051
12. Kaplan GA, Goldberg DE, Everson SA, Cohen RD, Salonen R, Tuomilehto J, et al. Perceived health status and morbidity and mortality: evidence from the kuopio ischaemic heart disease risk factor study. Int J Epidemiol. (1996) 25:259–65. doi: 10.1093/ije/25.2.259
13. Halford C, Wallman T, Welin L, Rosengren A, Bardel A, Johansson S, et al. Effects of self-rated health on sick leave, disability pension, hospital admissions and mortality A population-based longitudinal study of nearly 15,000 observations among Swedish women and men. BMC Public Health. (2012) 12:1103. doi: 10.1186/1471-2458-12-1103
14. DeSalvo KB, Bloser N, Reynolds K, He J, Muntner P. Mortality prediction with a single general self-rated health question. J General Int Med. (2006) 21:267–75. doi: 10.1111/j.1525-1497.2005.00291.x
15. Meireles AL, Xavier CC, de Souza Andrade AC, Proietti FA, Caiaffa WT. Self-rated health among urban adolescents: the roles of age, gender, and their associated factors. PLoS ONE. (2015) 10:e0132254. doi: 10.1371/journal.pone.0132254
16. Breidablik HJ, Meland E, Lydersen S. Self-rated health in adolescence: a multifactorial composite. Scand J Public Health. (2008) 36:12–20. doi: 10.1177/1403494807085306
17. Jafari-Adli S, Qorbani M, Heshmat R, Ranjbar SH, Taheri E, Motlagh ME, et al. Association of short stature with life satisfaction and self-rated health in children and adolescents: the CASPIAN-IV study. J Pediat Endocrinol Metabol. (2016) 29:1299–306. doi: 10.1515/jpem-2016-0215
18. Jerdén L, Burell G, Stenlund H, Weinehall L, Bergström E. Gender differences and predictors of self-rated health development among swedish adolescents. J Adolesc Health. (2011) 48:143–50. doi: 10.1016/j.jadohealth.2010.06.005
19. Xu Z, Su H, Zou Y, Chen J, Wu J, Chang W. Self-rated health of Chinese adolescents: distribution and its associated factors. Scandinavian J Car Sci. (2011) 25:780–6. doi: 10.1111/j.1471-6712.2011.00893.x
20. Biddle SJ, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med. (2011) 45:886–95. doi: 10.1136/bjsports-2011-090185
21. Poitras VJ, Gray CE, Borghese MM, Carson V, Chaput JP, Janssen I, et al. Tremblay, Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. App Physiol Nutri Metabol. (2016) 41(Suppl. 3) S197–239. doi: 10.1139/apnm-2015-0663
22. Chen Z, Chi G, Wang L, Chen S, Yan J, Li S. The combinations of physical activity, screen time, and sleep, and their associations with self-reported physical fitness in children and adolescents. Int J Environ Res Public Health. (2022) 19:5783. doi: 10.3390/ijerph19105783
23. Liu S, Yu Q, Hossain M, Doig S, Bao R, Zhao Y, et al. Meeting 24-h movement guidelines is related to better academic achievement: findings from the YRBS 2019 cycle. Int J Mental Health Promot. (2022) 24:13–24. doi: 10.32604/IJMHP.2021.017660
24. Martínez-López EJ, Hita-Contreras F, Moral-García JE, Grao-Cruces A, Ruiz JR, Redecillas-Peiró MT, et al. (2015). Association of low weekly physical activity and sedentary lifestyle with self-perceived health, pain, and well-being in a Spanish teenage population. Sci Sports. 30:342–51. doi: 10.1016/j.scispo.2015.04.007
25. Shi C, Yan J, Wang L, Shen H. Exploring the self-reported physical fitness and self-rated health, mental health disorders, and body satisfaction among Chinese adolescents: a cross-sectional study. Front Psychol. (2022) 13:3231. doi: 10.3389/fpsyg.2022.1003231
26. Ellis JC. The Impact of Postsecondary Fitness and Wellness Courses on Physical Activity Behaviors (Doctoral dissertation). Walden University (2013).
27. Sacker A, Cable N. Do adolescent leisure-time physical activities foster health and well-being in adulthood? Evidence from two British birth cohorts. Eu J Public Health. (2006) 16:331–5. doi: 10.1093/eurpub/cki189
28. Yoo SY, Choi YJ, Um YJ. Challenges and growth as a mental health professional from volunteering experiences in the community gambling awareness campaign. Int J Mental Health Promot. (2020) 22:83–91. doi: 10.32604/IJMHP.2020.011299
29. Yaya S, Bishwajit G. Patterns of physical activity and self-rated health among adult populations in South Asia. Central Asian Journal of Global Health, (2020). 9(1). doi: 10.5195/cajgh.2020.347
30. Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: the evidence. Cmaj. (2006) 174:801–9. doi: 10.1503/cmaj.051351
31. Humphreys BR, McLeod L, Ruseski JE. Physical activity and health outcomes: evidence from Canada. Health Econ. (2014) 23:33–54. doi: 10.1002/hec.2900
32. Haug E, Torsheim T, Samdal O. Physical environmental characteristics and individual interests as correlates of physical activity in Norwegian secondary schools: the health behaviour in school-aged children study. Int J Behav Nutri Phys Act. (2008) 5:1–10. Available online at: http://www.ijbnpa.org/content/5/1/47
33. Roberts C Freeman J Samdal O Schnohr CW De Looze ME Nic Gabhainn S The The Health Behaviour in School-aged Children (HBSC) study: methodological developments and current tensions. Int J Public Health. (2009) 54:140–50. doi: 10.1007/s00038-009-5405-9
34. Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M. Researching health inequalities in adolescents: the development of the health behaviour in school-aged children (HBSC) family affluence scale. Soc Sci Med. (2008) 66:1429–36. doi: 10.1016/j.socscimed.2007.11.024
35. Morgan K, Hallingberg B, Littlecott H, Murphy S, Fletcher A, Roberts C, et al. Predictors of physical activity and sedentary behaviours among 11-16 year olds: multilevel analysis of the 2013 health behaviour in school-aged children (HBSC) study in Wales. BMC Public Health. (2016) 16:1–10. doi: 10.1186/s12889-016-3213-8
36. Haugland S, Wold B. Subjective health complaints in adolescence—reliability and validity of survey methods. J Adolesc. (2001) 24:611–24. doi: 10.1006/jado.2000.0393
37. Vereecken CA, Maes L. A Belgian study on the reliability and relative validity of the Health Behaviour in School-Aged Children food-frequency questionnaire. Public Health Nutr. (2003) 6:581–8. doi: 10.1079/PHN2003466
38. Chai L, Xue J, Han Z. School bullying victimization and self-rated health and life satisfaction: The gendered buffering effect of educational expectations. Child Youth Serv Rev. (2020) 116:105252. doi: 10.1016/j.childyouth.2020.105252
39. Zhang A De Luca S Oh S Liu C Song X The The moderating effect of gender on the relationship between bullying victimization and adolescents' self-rated health: an exploratory study using the fragile families and wellbeing study. Child Youth Serv Rev. (2019) 96:155–62. doi: 10.1016/j.childyouth.2018.11.046
40. Galán I, Boix R, Medrano MJ, Ramos P, Rivera F, Pastor-Barriuso R. Physical activity and self-reported health status among adolescents: a cross-sectional population-based study. BMJ Open. (2013) 3:e002644. doi: 10.1136/bmjopen-2013-002644
41. Hodacova L, Hlaváčková E, Sigmundová D, Kalman M, Kopcakova J. Trends in life satisfaction and self-rated health in czech school-aged children: HBSC study. Cent Eur J Public Health. (2017) 25 Suppl 1:S51–s56. doi: 10.21101/cejph.a4820
42. Södergren M, Sundquist J, Johansson SE, Sundquist K. Physical activity, exercise and self-rated health: a population-based study from Sweden. BMC Public Health. (2008) 8:1–9. doi: 10.1186/1471-2458-8-352
43. García-Hermoso A, Ezzatvar Y, Ramírez-Vélez R, Olloquequi J, Izquierdo M. Is device-measured vigorous physical activity associated with health-related outcomes in children and adolescents? A systematic review and meta-analysis. J Sport Health Sci. (2021) 10:296–307. doi: 10.1016/j.jshs.2020.12.001
44. Costigan SA, Eather N, Plotnikoff RC, Hillman CH, Lubans DR. High-intensity interval training on cognitive and mental health in adolescents. Med Sci Sports Exe. (2016) 48:1985–93. doi: 10.1249/MSS.0000000000000993
45. Leahy AA, Mavilidi MF, Smith JJ, Hillman CH, Eather N, Barker D. Review of high-intensity interval training for cognitive and mental health in youth. Med Sci Sports Exe. (2020) 52:2224–34. doi: 10.1249/MSS.0000000000002359
46. Samdal O, Tynjälä J, Roberts C, Sallis JF, Villberg J, Wold B. Trends in vigorous physical activity and TV watching of adolescents from 1986 to 2002 in seven European countries. Eu J Public Health. (2007) 17:242–8. doi: 10.1093/eurpub/ckl245
47. Hrafnkelsdottir SM, Brychta RJ, Rognvaldsdottir V, Gestsdottir S, Chen KY, Johannsson E, et al. Less screen time and more frequent vigorous physical activity is associated with lower risk of reporting negative mental health symptoms among Icelandic adolescents. PLOS ONE. (2018) 13:e0196286. doi: 10.1371/journal.pone.0196286
Keywords: vigorous physical activity, self-rated health, adolescence, HBSC, survey
Citation: Wang Y, She W, Chi G and Wang J (2022) Vigorous physical activity and self-rated health during adolescence: A cross-sectional survey. Front. Public Health 10:961361. doi: 10.3389/fpubh.2022.961361
Received: 04 June 2022; Accepted: 30 September 2022;
Published: 21 October 2022.
Edited by:
Liye Zou, Shenzhen University, ChinaReviewed by:
Yanjie Zhang, The Chinese University of Hong Kong, ChinaCopyright © 2022 Wang, She, Chi and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Junsheng Wang, d2FuZ2p1bnNoZW5nQGN1cGVzLmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.