 Yuan-yuan Guo
Yuan-yuan Guo Zhi-jie Li1†
Zhi-jie Li1† Jun Gong
Jun Gong
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 14 September 2022
Sec. Digital Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.960740
This article is part of the Research Topic Machine Learning in Disease Screening, Diagnosis, and Surveillance View all 20 articles
Thyroid tumors, one of the common tumors in the endocrine system, while the discrimination between benign and malignant thyroid tumors remains insufficient. The aim of this study is to construct a diagnostic model of benign and malignant thyroid tumors, in order to provide an emerging auxiliary diagnostic method for patients with thyroid tumors. The patients were selected from the Chongqing General Hospital (Chongqing, China) from July 2020 to September 2021. And peripheral blood, BRAFV600E gene, and demographic indicators were selected, including sex, age, BRAFV600E gene, lymphocyte count (Lymph#), neutrophil count (Neu#), neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), red blood cell distribution width (RDW), platelets count (PLT), red blood cell distribution width—coefficient of variation (RDW–CV), alkaline phosphatase (ALP), and parathyroid hormone (PTH). First, feature selection was executed by univariate analysis combined with least absolute shrinkage and selection operator (LASSO) analysis. Afterward, we used machine learning algorithms to establish three types of models. The first model contains all predictors, the second model contains indicators after feature selection, and the third model contains patient peripheral blood indicators. The four machine learning algorithms include extreme gradient boosting (XGBoost), random forest (RF), light gradient boosting machine (LightGBM), and adaptive boosting (AdaBoost) which were used to build predictive models. A grid search algorithm was used to find the optimal parameters of the machine learning algorithms. A series of indicators, such as the area under the curve (AUC), were intended to determine the model performance. A total of 2,042 patients met the criteria and were enrolled in this study, and 12 variables were included. Sex, age, Lymph#, PLR, RDW, and BRAFV600E were identified as statistically significant indicators by univariate and LASSO analysis. Among the model we constructed, RF, XGBoost, LightGBM and AdaBoost with the AUC of 0.874 (95% CI, 0.841–0.906), 0.868 (95% CI, 0.834–0.901), 0.861 (95% CI, 0.826–0.895), and 0.837 (95% CI, 0.802–0.873) in the first model. With the AUC of 0.853 (95% CI, 0.818–0.888), 0.853 (95% CI, 0.818–0.889), 0.837 (95% CI, 0.800–0.873), and 0.832 (95% CI, 0.797–0.867) in the second model. With the AUC of 0.698 (95% CI, 0.651–0.745), 0.688 (95% CI, 0.639–0.736), 0.693 (95% CI, 0.645–0.741), and 0.666 (95% CI, 0.618–0.714) in the third model. Compared with the existing models, our study proposes a model incorporating novel biomarkers which could be a powerful and promising tool for predicting benign and malignant thyroid tumors.
The incidence of thyroid tumors has been increasing over the past 20 years, and it was the eighth most commonly diagnosed tumors in the world among endocrine tumors (1–3). According to the National Cancer Registry, thyroid tumors in China will continue to grow at an annual rate of 20% (4, 5). Therefore, identifying benign and malignant tumors owns great significance for early clinical intervention and treatment. Although ultrasonography and fine needle aspiration biopsy (FNAB) cytology methods can diagnose most thyroid tumors, there were still some patients who were misdiagnosed or overtreated. In addition, the limitations of those examinations included the need for a highly experienced cytopathologist for accurate interpretation, and not suitable for early screening of disease.
At present, many biomarkers of thyroid tumors have been discovered by researchers. Ozmen found that higher NLR and PLR were associated with worse survival in differential thyroid tumors (6). Another study from Turkey suggested that mean platelet volume (MPV) levels can be used as an easily available biomarker for monitoring the risk of papillary thyroid carcinoma (PTC) in patients with thyroid nodules, enabling early diagnosis of PTC (7). And Liu found that lower pretreatment platelet count (PLT) levels may indicate a poor prognosis for PTC (8). In particular, the BRAFV600E gene is also an important biomarker for the occurrence and progression of papillary thyroid tumors (9). In addition, the review by Qian and Iryani mentions that many genetic biomarkers can differentiate benign from malignant thyroid tumors (10, 11). However, most studies just investigated the diagnostic performance of individual biomarkers, and few studies have integrated these biomarkers to construct models that can be used to diagnose benign and malignant thyroid tumors in clinical practice. Previous studies have the shortcomings of small sample size and large differences in diagnostic performance between different biomarkers.
Machine learning (ML) is an emerging artificial intelligence discipline that analyzes multiple data types and uses them to explore disease risk factors, accurate diagnosis, and prognosis (12). Moreover, it can integrate multiple clinical indicators, explore the nonlinear relationship between predictors and clinical outcomes, and solve problems such as poor performance of logistic methods in traditional clinical modeling. Sui developed a deep-learning AI model (ThyNet) using ultrasound images to differentiate between malignant tumors and benign thyroid nodules with an AUC of 0.875 (95% CI, 0.871–0.880) (13). Although there have been some studies using ML algorithms to diagnose benign and malignant thyroid tumors, the data selected are mostly image data, which makes data collection more complicated.
Therefore, this study aims to apply ML algorithms to build a predictive model of thyroid tumors with demographic, peripheral blood laboratory, and genetic biomarkers to provide an accurate and reliable prediction method for the early discrimination of benign and malignant thyroid tumors.
Patients with thyroid tumor included in the current study, were selected from the Chongqing General Hospital (Chongqing, China) from July 2020 to September 2021. According to WHO 2017 classification and the eighth edition of the AJCC/TNM classification (TNM-8) (14), operating records and final pathologic reports were reviewed to ascertain tumor categories, they were divided into benign groups and malignant groups. Benign groups are defined as thyroid follicular nodular disease, follicular adenoma, follicular adenoma with papillary architecture, oncocytic adenoma of the thyroid, and benign thyroid nodules. While, malignant groups are defined as follicular thyroid carcinoma, invasive encapsulated follicular variant papillary carcinoma, papillary thyroid carcinoma, oncocytic carcinoma of the thyroid, follicular-derived carcinomas, high-grade, and anaplastic follicular cell-derived thyroid carcinoma (15).
This study was exempt from ethical review by the Institutional Review of the Chongqing General Hospital. The study methods were carried out in accordance with the relevant guidelines and regulations.
The data was collected from the electronic medical record (EMR) system of the Chongqing General Hospital, which contains laboratory examination records, diagnosis and treatment process records, doctor orders, etc. Patient's peripheral blood indicators, BRAFV600E gene, and demographic indicators were selected, including age, sex, lymphocyte count (Lymph#), neutrophil count (Neu#), red blood cell distribution width (RDW), red blood cell distribution width - coefficient of variation (RDW–CV), platelets count (PLT), neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), alkaline phosphatase (ALP), parathyroid hormone (PTH), and BRAFV600E gene mutation as predictors to build a ML model to identify benign and malignant thyroid tumors. All the peripheral blood tests and BRAFV600E gene results were obtained at the first examination after the patient was admitted to the hospital.
The BRAFV600E gene mutation was detected by real-time PCR using the ABI QuantStudio®5 Real-Time PCR System, according to the manufacturer's instructions (Human BRAFV600E Mutation assay Kit, YZY MED, Wuhan, China) The DNA from FNAB specimen was extracted using a companion kit, which was provided by the same manufacturer. The DNA concentration was quantified in a Nano-300 Micro Spectrophotometer (ALLSHENG Instrument Co., Ltd. Hangzhou, China) as per the manufacturer's instructions. The DNA was immediately used to carry out the test of BRAFV600E gene mutation.
All the statistical analyses and model building were conducted in R for windows (version 4.0.1, https://www.r-project.org/). For information on hardware devices in the development environment, please see Supplementary Table 1.
The data were presented as count with percentage for categorical variables, median with interquartile range (IQR), or mean with SD for continuous variables. For the variables with miss rate <30%, missforest algorithm was used to fill. First, the Mann–Whitney U-test or t-test was performed for the continuous variables, and the chi-square test for categorical variables was carried out used for univariate analysis. The variables after univariate analysis were analyzed by the least absolute shrinkage and selection operator (LASSO). Afterward, random forest (RF), extreme gradient boosting (XGBoost), light gradient boosting machine (LightGBM) and adaptive boosting (AdaBoost) were used to establish prediction models. We used the grid search algorithm to find the optimal parameters of each algorithm to optimize the performance of the model. Sensitivity (SEN), specificity (SPE), precision, recall, F1, and the area under the curve (AUC) were intended to determine the model performance.
A total of 2,423 patients met the inclusion criteria and were enrolled in the study. In total, 381 patients were excluded due to missing clinical data. At last, a total of 2,042 patients with 12 predictors were included in the final study. Table 1 shows the information of the whole cohort. In the whole cohort, 1,481 malignant patients and 561 benign patients were included. The average age of patients was 42.03 ± 11.30 years, ranging from 14 to 76 years, women accounted for 77.34% (1,580 cases) and men 22.66% (463 cases). The specific screening process and study protocol are shown in Figure 1.
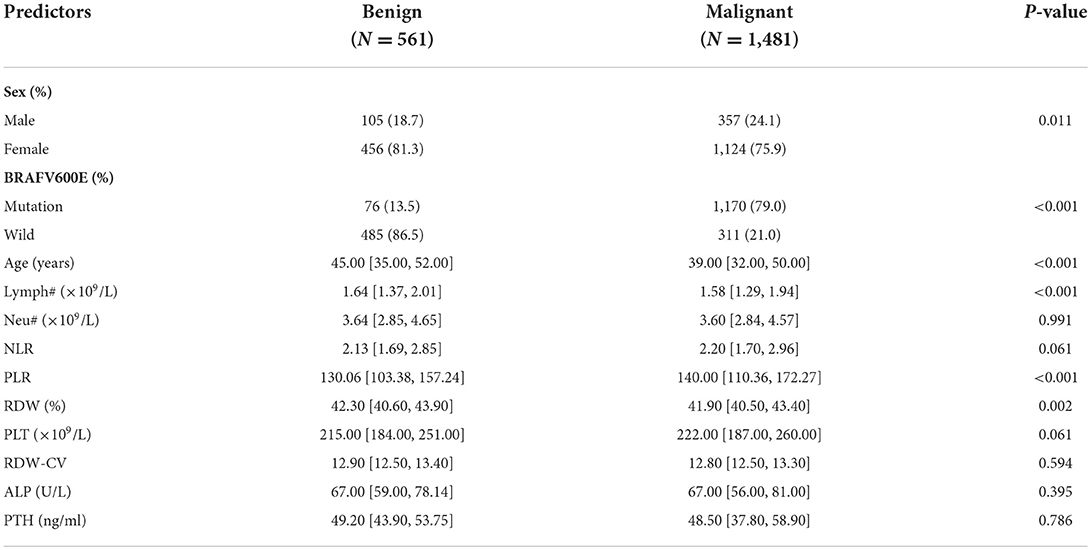
Table 1. Clinical characteristics and variables of patients in all cohorts.
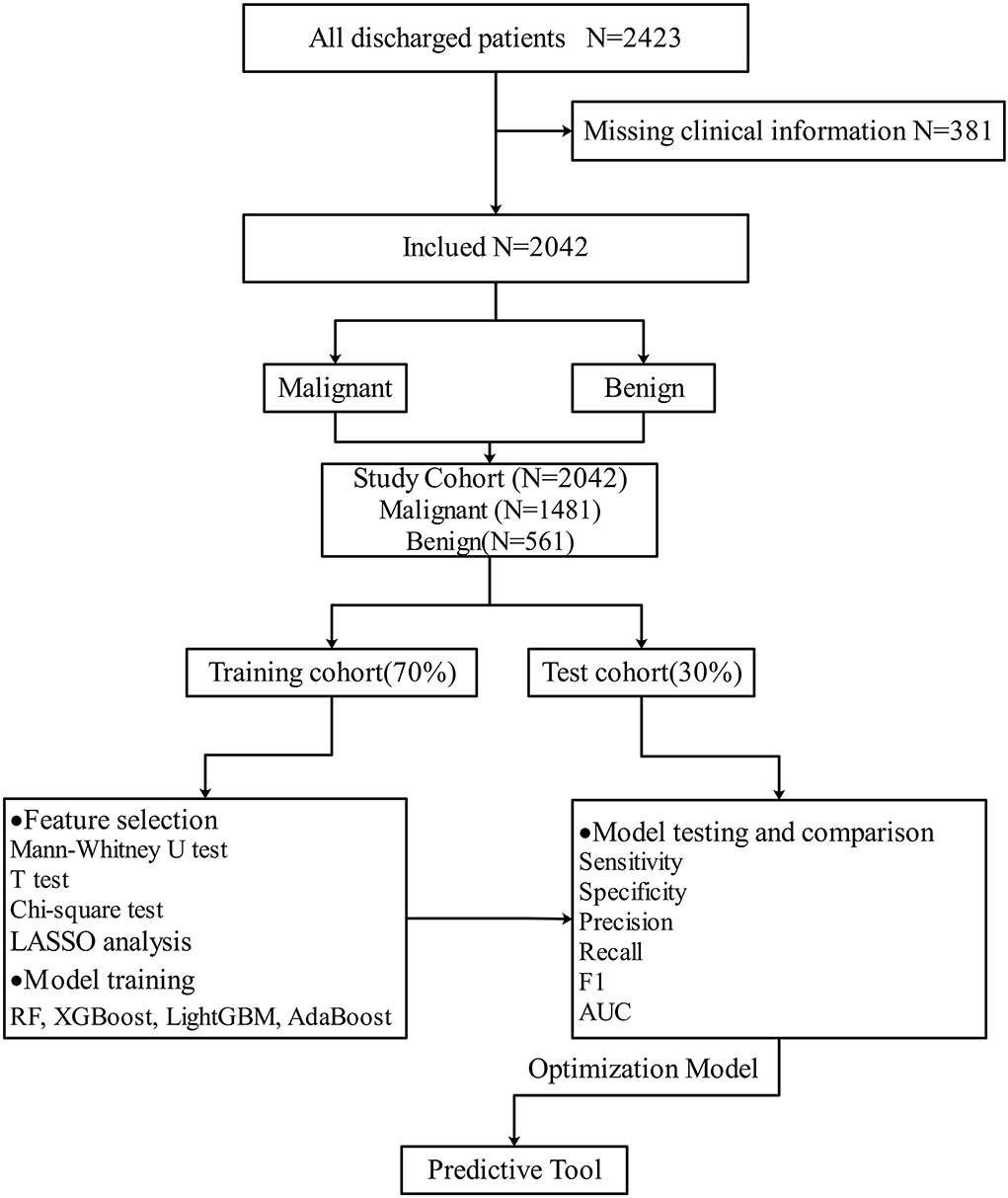
Figure 1. Flowchart of research object.
The data were split into a training cohort (70%, N = 1,429) and a test cohort (30%, N = 613) by random number table. In the training cohort, there were 395 cases of the benign group and 1,034 cases of the malignant group. In the test cohort, there were 166 cases of the benign group and 447 cases of the malignant group. The predictors we collected were used as input variables of ML algorithms. Whether malignancy or benign was regarded as the outcome event (yes = 1, no = 0) to establish prediction model by using training cohort, and the test cohort was used to verify the ability of the established prediction model previously. According to Table 2, univariate analysis results indicated that 6 predictors were statistically significant between the malignant group and benign group in training cohort. We performed the LASSO analysis on the 6 indicators with statistically significant, and the results showed that these 6 indicators were all selected by LASSO (Figure 2). Therefore, our final diagnostic model included the 6 indicators of sex, age, Lymph#, PLR, RDW, and BRAFV600E.
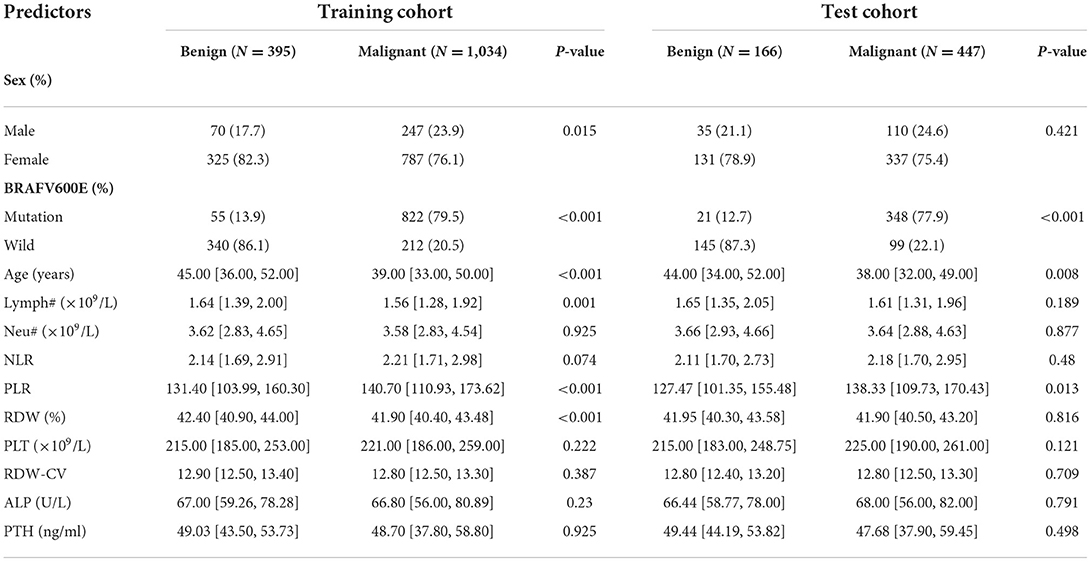
Table 2. Clinical characteristics and variables of patients in training cohort and test cohort.
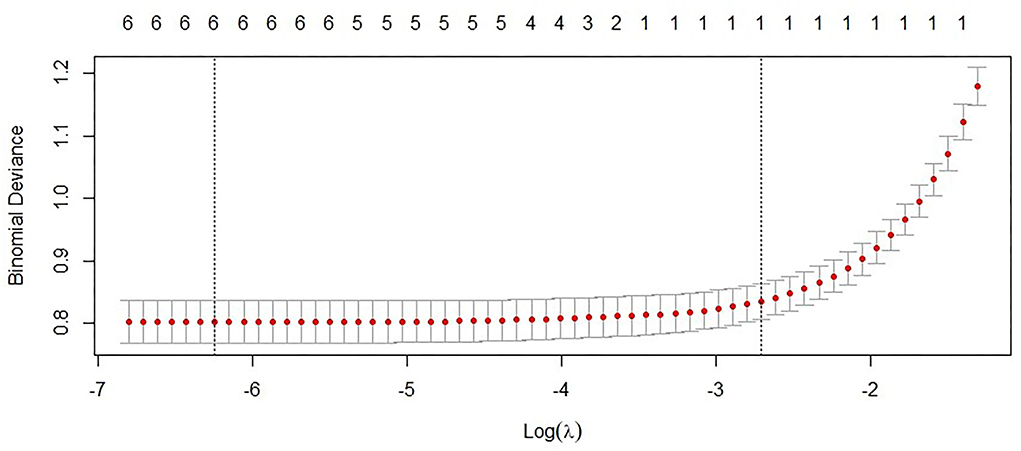
Figure 2. LASSO analysis of indicators after univariate analysis.
We built 3 ML models with different predictors, the first model included all the predictors we included, the second model included predictors after feature selection, and the third model included patient peripheral blood predictors. For the specific construction steps of the model, please see Supplementary Figure 1, and the detailed description of the three models can be found in Supplementary Table 2. In addition, we also used the grid search algorithm to find the optimal parameters of the ML algorithm. The grid search algorithm permutes and combines each possible parameter value, and then substitutes the results of all possible combinations into the algorithm for model training. The optimal parameter combination was selected from all possible parameter combinations. In our research, we selected the optimal parameters of four ML algorithms: RF, XGBoost, LightGBM, and Adaboost through the grid search algorithm. Please see Table 3 for the optimal parameters of each algorithm.
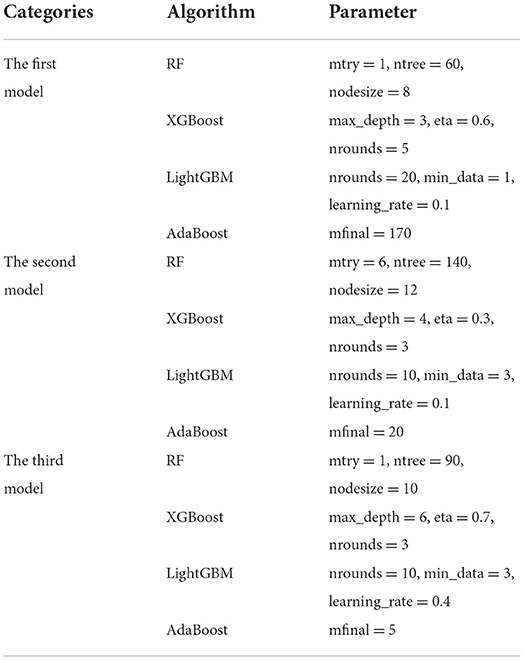
Table 3. The optimal parameters of the three models.
In Table 4, the metrics of three models were compared in terms of SEN, SPE, AUC, etc., in the test cohort. The SEN and precision are indicators to measure the positive predictive performance of the model. In the first and second models, the SEN indicator exceeds 0.7, and the precision indicator reaches 0.9, suggesting that the model we established can well identify malignant patients from thyroid tumor patients. The SPE is an indicator of the model's negative predictive performance, and in our study, the highest SPE was 0.892, indicating that our model could also predict patients with benign thyroid tumor well. The AUC is a comprehensive indicator for comparing prediction performance. Among the three models constructed with different predictors, the first model including all predictors performed best with the highest AUC of 0.874 (95% CI, 0.841, 0.906). The second model had the highest AUC of 0.853 (95% CI, 0.818, 0.889; Figure 3). However, we performed the Delong test on the optimal AUC of the first and second models (z = 1.65, P = 0.099), and the results showed that the difference was not statistically significant. The third model selects peripheral blood predictors, and the best AUC is 0.698 (95% confidence interval, 0.651, 0.745). In the third model, we selected biomarkers in patients' peripheral blood to establish a prediction model, and the performance of the model is inferior to the first and second models. Biomarkers in peripheral blood are easy to obtain, and the AUC of the model is close to 0.7, suggesting that it also has a certain predictive value.
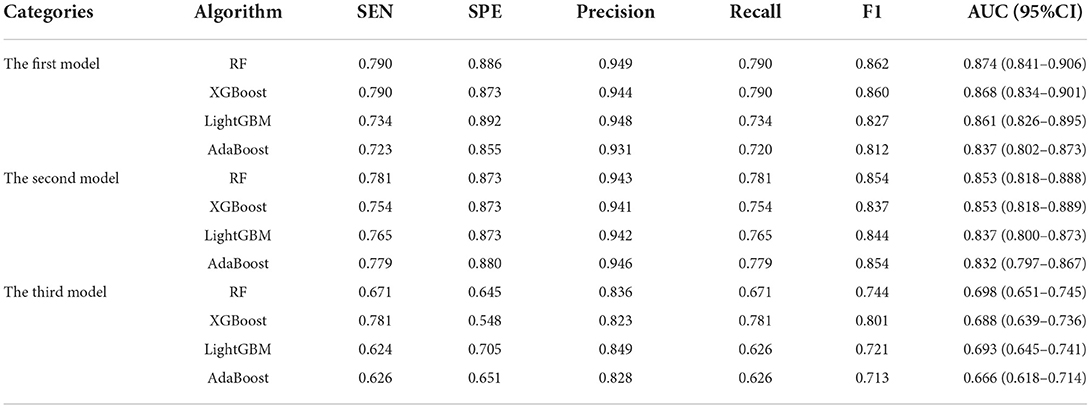
Table 4. Performance evaluation table of three models.
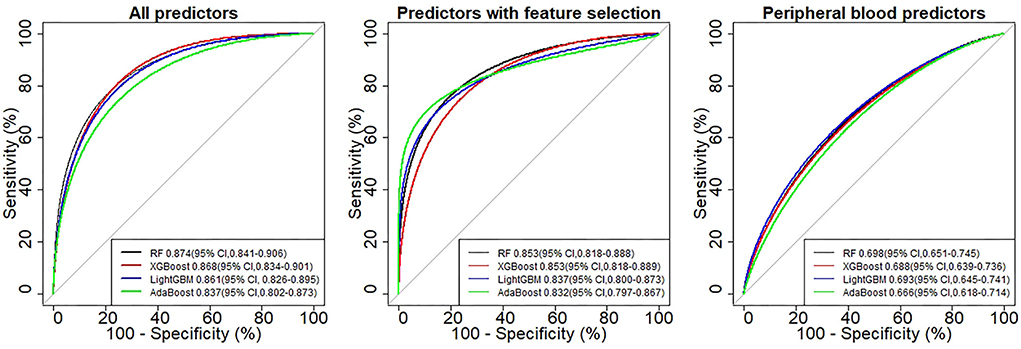
Figure 3. ROC curve of four models in different categories.
To balance the diagnostic performance and simplicity of the model, according to the comprehensive evaluation of the performance indicators of the model and the Delong test analysis, the second model, using the RF algorithm, was the best at predicting benign and malignant thyroid tumors. The importance ranking of predictors in the RF algorithm is as follows: BRAFV600E, age, PLR, RDW, Lymph#, and sex (Figure 4).
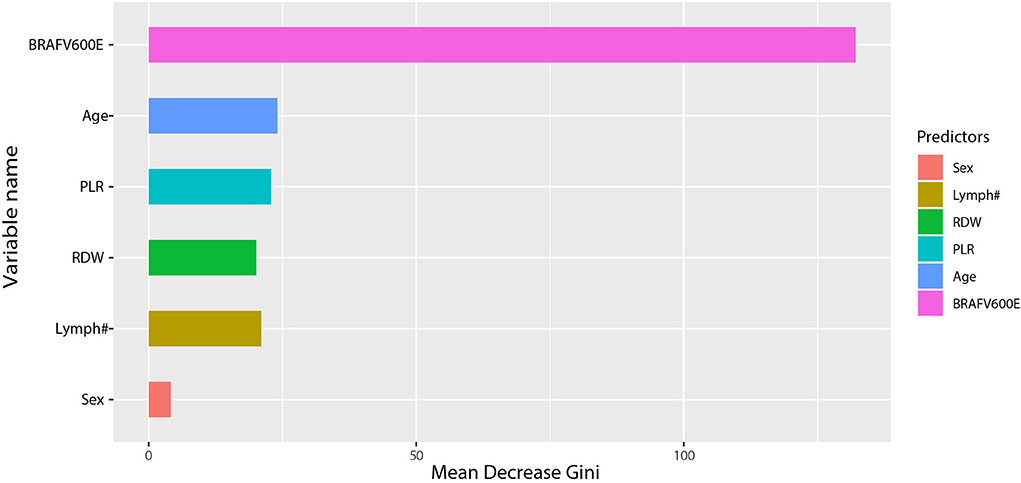
Figure 4. Importance ranking of prediction indicators after feature selection.
In this study, we developed the ML-based predictive models to identify benign and malignant thyroid nodules. The current gold diagnostic standard for thyroid tumors meeting appropriate criteria is a cyto-pathologic assessment of FNAB. However, high operator requirements were needed in FNAB, and the accuracy of diagnosis largely depends on the operator's personal level of experience. Therefore, it is crucial to provide more objective and direct parameters that can help with the identification of benign and malignant thyroid lesions. Thus, predictors including BRAFV600E gene mutation, Lymph#, Neu#, RDW, PLT, NLR, PLR, ALP, PTH, and clinical characters of patients were enrolled and the ML algorithm was used to predict benign and malignant thyroid tumors in our study.
Recent advances in understanding the molecular pathogenesis of thyroid tumors have enabled the application of molecular tests to provide more objective information and play a role in making more personalized clinical treatments (16). A large number of biomarkers such as BRAFV600E, RAS, EIF1AX, PIK3CA, PTEN and AKT1, SWI/SNF, ALK, and CDKN2A, have been excavated, demonstrating the potential of molecular diagnostic detection(17). Nevertheless, the BRAFV600E is the most prevalent mutation detected in PTC, with an average frequency of 60%−70%, and the tests for BRAFV600E mutation are commonly available in the current clinical practice (18). The BRAFV600E protein kinase has received extensive attention because of its function in promoting cell proliferation, growth, and division, and numerous studies have investigated the relationship between the BRAFV600E mutations and various clinicopathological features. In vitro tests have shown a high concordance between the BRAFV600E mutations and the aggressive characteristics of PTC, while clinical trials have shown contrasting results, making it controversial whether the BRAFV600E mutations can be used as an aggressive marker for PTC. Most studies suggest that the BRAFV600E mutations are associated with worse clinical pathology, such as lymph node metastasis, distant metastasis, worse tumor stage, aggressive subtype, tumor size, male, and old age, and therefore, recommend the central lymph node dissection based on total thyroidectomy with more stringent radioiodine therapy and a close follow-up after surgery (19). However, some studies did not find such an association (20). The differences in these studies may be due to the different sample sizes included in the studies, epidemiological characteristics of the patients, papillary carcinoma subtypes, types of specimens used for molecular testing, and testing methods. In this study, the BRAFV600E gene mutation status was important for all algorithms, which is consistent with a recent study. The BRAFV600E mutation has both high specificity and sensitivity to predict thyroid malignancy in the Chinese population. It can accurately complete cytopathology in the guidance of thyroid surgery (21). In our study, the diagnostic performance accuracy of the BRAFV600E gene was 0.810, and the AUC was 0.827, which had a high-diagnostic value.
The peripheral blood routine test and the blood biochemical test have major advantages over the traditional pathological test of tumor lesions in terms of quick and simple sample acquisition, low collection cost, minimal trauma, and preoperative detection, which should be paid more attention to in research (22). Lymph#, Neu#, RDW-CV, PLT, NLR, PLR, ALP, PTH, and other related indicators can quickly and accurately detect the values of blood, in order to effectively indicate abnormalities of infection, anemia, and cruor. In recent years, a wide variety of blood indicators with different changes were concerned and discussed in the study of malignant tumor diseases. The preoperative NLR and RDW–CV are convenient, practical, and easily measured biomarkers for clinical diagnosis and prognostic assessment of patients with esophageal cancer. Moreover, the NLR was more effective than RDW–CV, acting as an independent prognostic biomarker for esophageal cancer (23). On the contrary, the RDW–CV has attracted more attention in cervical, ovarian, and endometrial cancer as studies have shown the hierarchical independent relationship between the RDW and these kinds of cancers (24). The preoperative blood count from peripheral blood may provide prognostic value in patients with pathologic stage I NSCLC undergoing surgical resection. Of significance in patients with pT1 N0 NSCLC, the high lymphocyte count and high platelet count were associated with higher recurrence (25). Even the NLR, PLR, and LMR, which are the derived indexes of peripheral whole blood cell counts, were developed into new indexes, and have fairly good values of prognostic(26–28). However, the values of NLR and PLR to distinguish between benign and malignant of thyroid nodules is still controversial. Our study found that the Lymph#, RDW–CV, and PLR were statistically different between benign and malignant thyroid nodules (P < 0.05).
Recently, the ML algorithms have been extensively used in the medical field, emerging as a powerful tool in dealing with many health care problems. In our study, the ML-based model for diagnosing benign and malignant thyroid tumors showed the highest AUC of 0.874 (95% CI, 0.841, 0.906), which suggests that our model has a high value in diagnosing benign and malignant thyroid tumors. To evaluate the accuracy and simplicity of the model, feature selection is often used to screen indicators with predictive value. We screened out six predictors from 12 predictors by the univariate analysis method. Compared with the inclusion of 12 predictors, the model established by these six predictors also has good predictive performance and was identified as the optimal model. From the perspective of algorithm selection, when the indicators contained in the model are consistent, the performance of the four algorithms is not significantly different. One of the reasons is that if there is a clear correlation between the independent and dependent variables, then most ML algorithms can handle this nonlinear relationship and have good predictive performance. At present, many scholars have studied the use of artificial intelligence algorithms to accurately identify benign and malignant thyroid tumors (Table 5). The performance of our model is inferior to that of Hong-Bo Zhao, Sui, Peng et al., and similar to that of Masuda, Kim, Su Yeon Ko et al. Current researches mainly use ultrasound or CT images combined with intelligent algorithms to accurately diagnose benign and malignant thyroid tumors, and has excellent performance. In general, CT and ultrasound images have better predictive performance because they contain more information about benign and malignant tumors. However, from the perspective of patient's genetic markers and peripheral blood markers, our predictors are easy to obtain and has good value in identifying benign and malignant thyroid tumors.
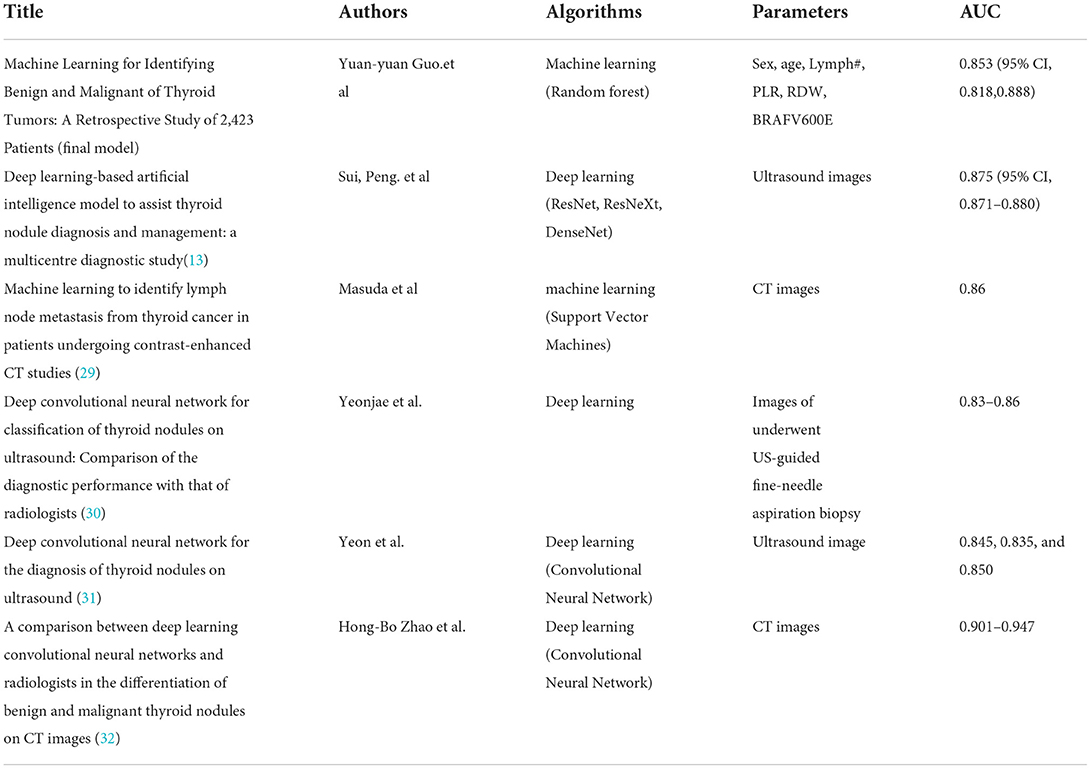
Table 5. Comparison of the newly created model with the existing model.
In conclusion, the prediction model established in this study can distinguish benign with the risk of identifying malignant thyroid nodules, which could be further developed into a clinical decision support system. Our study also had some limitations. First, all of the data come from southwest China, so there may be a selection bias. Second, only four algorithms were selected to establish the prediction model, therefore it is still necessary to try whether there are other better predictive algorithms. Third, the missing rate ≥30% of the variables were not included in the study. Therefore, further analysis is required to identify these factors related to identifying benign and malignant of thyroid nodules.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Y-yG, Z-jL, and PL took part in the research design and helped to draft the manuscript. J-xZ and CS contributed the acquisition of data. CD and JG performed the statistical analysis. All authors contributed to the article and approved the final manuscript.
This work was supported by a grant for the Science and Technology and Health Commission program of Chongqing (2020FYYX157).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.960740/full#supplementary-material
1. Alessandro A, La MC. Novel therapeutic clues in thyroid carcinomas: the role of targeting cancer stem cells. Med Res Rev. (2017) 37:1299–317. doi: 10.1002/med.21448
2. Ferrari SM, Fallahi P, Elia G, Ragusa F, Ruffilli I, Paparo SR, et al. Thyroid autoimmune disorders and cancer. Semin Cancer Biol. (2020) 64:135–46. doi: 10.1016/j.semcancer.2019.05.019
3. Lin JS, Bowles EJA, Williams SB, Morrison CC. Screening for thyroid cancer: updated evidence report and systematic review for the US preventive services task force. JAMA. (2017) 317:1888–903. doi: 10.1001/jama.2017.0562
4. Fang C, Juan X, Chunchun S, Fengyan H, Lihua W, Yanli J, et al. Burden of thyroid cancer from 1990 to 2019 and projections of incidence and mortality until 2039 in China: findings from global burden of disease study. Front Endocrinol. (2021) 12:738213. doi: 10.3389/fendo.2021.738213
5. Junyi W, Fangfang Y, Yanna S, Zhiguang P, Li L. Thyroid cancer: incidence and mortality trends in China, 2005-2015. Endocrine. (2020) 68:163–73. doi: 10.1007/s12020-020-02207-6
6. Ozmen S, Timur O, Calik I, Altinkaynak K, Simsek E, Gozcu H, et al. Neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) may be superior to C-reactive protein (CRP) for predicting the occurrence of differentiated thyroid cancer. Endocr Regul. (2017) 51:131–6. doi: 10.1530/endoabs.41.EP1151
7. Baldane S, Ipekci SH, Sozen M, Kebapcilar L. Mean platelet volume could be a possible biomarker for papillary thyroid carcinomas. Asian Pac J Cancer Prev. (2015) 16:2671–4. doi: 10.7314/APJCP.2015.16.7.2671
8. Xiangxiang L, Huang Z, He X, Zheng X, Jia Q, Tan J, et al. Blood prognostic predictors of treatment response for patients with papillary thyroid cancer. Biosci Rep. (2020) 40:BSR20202544. doi: 10.1042/BSR20202544
9. Shiyang L, Bo J, Shuyu L, Lu Z, Weihong Z, Kun W, et al. Oestrogen receptor alpha in papillary thyroid carcinoma: association with clinical features and BRAFV600E mutation. Jpn J Clin Oncol. (2021) 51:1051–8. doi: 10.1093/jjco/hyab058
10. Iryani AM, Mat JS, Leong NK, Jacqueline JJ, Barani K, Haji HO, et al. Papillary thyroid cancer: genetic alterations and molecular biomarker investigations. Int J Med Sci. (2019) 16:450–60. doi: 10.7150/ijms.29935
11. Qian X, Qiang J, Jian T, Zhaowei M. Serum biomarkers for thyroid cancer. Biomark Med. (2020) 14:807–15. doi: 10.2217/bmm-2019-0578
12. Ngiam KY, Khor IW. Big data and machine learning algorithms for health-care delivery. Lancet Oncol. (2019) 20:e262–73. doi: 10.1016/S1470-2045(19)30149-4
13. Sui P, Yihao L, Weiming L, Longzhong L, Qian Z, Hong Y, et al. (2021). Deep learning-based artificial intelligence model to assist thyroid nodule diagnosis and management: a multicentre diagnostic study. Lancet Digital Health. 3:e250–9. doi: 10.1016/S2589-7500(21)00114-X
14. Angela B, Ancu?a-Elena Z, Doina P, Elena B, Nicole B, Adela N, et al. A 15 year institutional experience of well-differentiated follicular cell-derived thyroid carcinomas; impact of the new 2017 TNM and WHO Classifications of Tumors of Endocrine Organs on the epidemiological trends and pathological characteristics. Endocrine. (2020) 67:630–42. doi: 10.1007/s12020-019-02158-7
15. Baloch ZW, Asa SL, Barletta JA, Ghossein RA, Juhlin CC, Jung CK, et al. Overview of the 2022 WHO classification of thyroid neoplasms. Endocr Pathol. (2022) 33:27–63. doi: 10.1007/s12022-022-09707-3
16. Sik PK, Hoon KS, Hun OJ, Young KS. Highly accurate diagnosis of papillary thyroid carcinomas based on personalized pathways coupled with machine learning. Brief Bioinform. (2020) 22:bbaa336. doi: 10.1093/bib/bbaa336
17. Ichiro A, Yin LAK. Anaplastic thyroid carcinoma: current issues in genomics and therapeutics. Curr Oncol Rep. (2021) 23:31–31. doi: 10.1007/s11912-021-01019-9
18. Youn KS, Taeeun K, Kwangsoon K, Seong BJ, Soo KJ, Kwon JC, et al. Highly prevalent BRAF V600E and low-frequency TERT promoter mutations underlie papillary thyroid carcinoma in Koreans. J Pathol Transl Med. (2020) 54. doi: 10.4132/jptm.2020.05.12
19. Chunping L, Tianwen C, Zeming L. Associations between BRAF(V600E) and prognostic factors and poor outcomes in papillary thyroid carcinoma: a meta-analysis. World J Surg Oncol. (2016) 14:241. doi: 10.1186/s12957-016-0979-1
20. Zhang Q, Liu SZ, Zhang Q, Guan YX, Chen QJ, Zhu QY, et al. Meta-analyses of association between BRAFV600E mutation and clinicopathological features of papillary thyroid carcinoma. Cell Physiol Biochem. (2016) 38:763–76. doi: 10.1159/000443032
21. Qunzi Z, Yong W, Qin Y, Ping W, Jianyu R. BRAF V600E as an accurate marker to complement fine needle aspiration (FNA) cytology in the guidance of thyroid surgery in the Chinese population: evidence from over 1000 consecutive FNAs with follow-up. JPN J Clin Oncol. (2020) 51:590–4. doi: 10.1093/jjco/hyaa209
22. Yalun L, Huizhe W, Chengzhong X, Xiaoyun H, Fangxiao Z, Yangjie P, et al. Prognostic evaluation of colorectal cancer using three new comprehensive indexes related to infection, anemia and coagulation derived from peripheral blood. J Cancer. (2020) 11:3834–45. doi: 10.7150/jca.42409
23. Han F, Liu Y, Cheng S, Sun Z, Sheng C, Sun X, et al. Diagnosis and survival values of neutrophil-lymphocyte ratio (NLR) and red blood cell distribution width (RDW) in esophageal cancer. Clin Chim Acta. (2019) 488:150–8. doi: 10.1016/j.cca.2018.10.042
24. Lingling Z, Youjun X, Lingling Z. The potential value of red blood cell distribution width in patients with invasive hydatidiform mole. J Clin Lab Anal. (2019) 33:e22846. doi: 10.1002/jcla.22846
25. Sulibhavi A, Asokan S, Miller MI, Moreira P, Daly BD, Fernando HC, et al. Peripheral blood lymphocytes and platelets are prognostic in surgical pT1 non-small cell lung cancer. Ann Thorac Surg. (2019) 109:337–42. doi: 10.1016/j.athoracsur.2019.09.006
26. Yonatan B, Caitlin O, Wendy H, Julian K, Peter C, Tristan T, et al. Platelet-lymphocyte ratio as a predictor of prognosis in head and neck cancer: a systematic review and meta-analysis. Oncol Res Treat. (2019) 42:665–77. doi: 10.1159/000502750
27. Yixi W, Hao Z, Yuhan Y, Tao Z, Xuelei M. Prognostic value of peripheral inflammatory markers in preoperative mucosal melanoma: a multicenter retrospective study. Front Oncol. (2019) 9:995. doi: 10.3389/fonc.2019.00995
28. Xinwen Z, Jialin D, Zhenyu W, Hao X, Xiaomin C, Yang L, et al. Are the derived indexes of peripheral whole blood cell counts (NLR, PLR, LMR/MLR) clinically significant prognostic biomarkers in multiple myeloma? a systematic review and meta-analysis. Front Oncol. (2021) 11:766672. doi: 10.3389/fonc.2021.766672
29. Masuda T, Nakaura T, Funama Y, Sugino K, Sato T, Yoshiura T, et al. (2021). Machine learning to identify lymph node metastasis from thyroid cancer in patients undergoing contrast-enhanced CT studies. Radiography. 27:920–6. doi: 10.1016/j.radi.2021.03.001
30. Yeonjae K, Yangsean C, Sujin H, Kisun P, Hyunjin K, Minkook S, et al. Deep convolutional neural network for classification of thyroid nodules on ultrasound: comparison of the diagnostic performance with that of radiologists. Eur J Radiol. (2022) 152:110335–110335. doi: 10.1016/j.ejrad.2022.110335
31. Yeon KS, Hye LJ, Hyun YJ, Hyesun N, Eunhye H, Kyunghwa H, et al. Deep convolutional neural network for the diagnosis of thyroid nodules on ultrasound. Head Neck. (2019) 41:885–91. doi: 10.1002/hed.25415
Keywords: thyroid tumor, machine learning, predictive model, BRAFV600E gene mutation, risk-factors
Citation: Guo Y-y, Li Z-j, Du C, Gong J, Liao P, Zhang J-x and Shao C (2022) Machine learning for identifying benign and malignant of thyroid tumors: A retrospective study of 2,423 patients. Front. Public Health 10:960740. doi: 10.3389/fpubh.2022.960740
Received: 03 June 2022; Accepted: 23 August 2022;
Published: 14 September 2022.
Edited by:
Yi-Ju Tseng, National Yang Ming Chiao Tung University, TaiwanReviewed by:
Jaydip Sen, Praxis Business School, IndiaCopyright © 2022 Guo, Li, Du, Gong, Liao, Zhang and Shao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pu Liao, bGlhb3B1QHVjYXMuYWMuY24=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.