
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 27 September 2022
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.955458
 Fadi S. Qashqari1
Fadi S. Qashqari1 Radi T. Alsafi2
Radi T. Alsafi2 Saeed M. Kabrah2*
Saeed M. Kabrah2* Rayda'a A. AlGary2
Rayda'a A. AlGary2 Sara A. Naeem2
Sara A. Naeem2 Malak S. Alsulami2
Malak S. Alsulami2 Hatim Makhdoom3
Hatim Makhdoom3Introduction: The human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (HIV/AIDS) are worldwide public health issues. Since Saudi Arabia is growing more accessible to the outside world, it is critical to analyze the general population's knowledge of HIV/AIDS transmission modes and attitudes toward HIV/AIDS infected people, and the level of HIV/AIDS awareness. Therefore, this study aimed to assess the knowledge of HIV/AIDS transmission modes and attitudes toward HIV/AIDS infected people, as well as the level of HIV/AIDS awareness among the general population in the Kingdom of Saudi Arabia.
Methods: The current online community-based cross-sectional descriptive study was conducted among the general population of the Kingdom of Saudi Arabia using a self-administrated electronic questionnaire between October 2017 and February 2018. A score <3 was considered a negative response. In contrast, scores of 3 and 4 were considered positive responses. The sum score of each outcome was evaluated according to Bloom's cutoff point. The scores for knowledge and attitude were transformed into mean percentage scores by dividing the sum scores obtained by the respondents by the number of items multiplied by 100. Consequently, the overall mean percentage of scores for each category of knowledge and attitude at 60% and above was considered a good level, whereas <60% was deemed a poor level.
Results: A total of 2,081 subjects residing in the Kingdom of Saudi Arabia participated in this survey. The mean score of the participant's responses to knowledge items on HIV/AIDS transmission modes was 84.2 ± 15.8%. The mean score of the participant's responses to attitude items toward HIV/AIDS infected people was 50.1 ± 49.9%. The mean score of the participant's responses to attitude items toward the level of HIV/AIDS awareness in Saudi Arabia was 55.7 ± 3.6%. Many socio-demographic variables were significantly associated with mean scores of knowledge of HIV/AIDS transmission modes, mean scores of attitude toward HIV/AIDS infected people, and mean scores of attitude toward the level of HIV/AIDS awareness (P-value ≤ 0.05). The Spearman rank correlation explained significant negative linear correlations between knowledge of HIV/AIDS transmission modes-attitudes toward HIV/AIDS infected people and knowledge of HIV/AIDS transmission modes-attitudes toward the level of HIV/AIDS awareness of r = −0.040 and r = −0.070, respectively (P-value ≤ 0.05). Otherwise, there was a positive linear correlation between attitudes toward HIV/AIDS infected people-attitudes toward the level of HIV/AIDS awareness (r = 0.080, P-value = 0.072).
Conclusions: The study showed that a high percentage of the respondents had good knowledge of HIV/AIDS transmission modes. However, a low rate of the study respondents had positive attitudes toward HIV/AIDS infected people and the level of HIV/AIDS awareness among the general population in Saudi Arabia. Therefore, there is a dire need for advocacy campaigns and policies to help reduce HIV stigmatization levels.
Infection with the Human Immunodeficiency Virus (HIV) and the Acquired Immune Deficiency Syndrome (AIDS) continues to be a significant public health issue (1, 2). Even though the number of HIV cases in the Middle East and North Africa (MENA) region is low compared to other areas, recent research has revealed that HIV incidence is rising, particularly among high-risk populations (3). According to the most recent figures on the condition of the AIDS epidemic (2).
Because of social, cultural, and religious taboos, accurate data on HIV/ the prevalence and incidence of HIV/AIDS has been slow in many Middle Eastern nations compared to other regions (4). Nevertheless, data in some countries is inadequate, and there is significant variation within the region. Because HIV remains a contentious issue in the MENA region, data on its prevalence and trends are poor, under-reporting is likely, and it is impossible to collect precise figures or determine the specific causes of HIV levels and trends (5).
Understanding people's knowledge and attitudes about HIV/AIDS are one of the cornerstones of fighting the disease. The most common problem people living with HIV/AIDS (PLWHA) face is the general public's lack of knowledge or miseducation about the disease (6); this, in turn, leads to or precipitates discrimination against them, which leads to or precipitates problems with disclosure, social isolation, access to antiretroviral therapy, and psychological support (7, 8).
Furthermore, several factors are linked to HIV knowledge and play a significant influence in influencing the amount of HIV stigma. These determinants are primarily education and HIV attitudes. Increased HIV education and awareness are two excellent techniques for reducing stigma, among many others. As a result, as one's level of education rises, so does one's understanding of HIV, unfavorable views about PLWHA fall, and HIV stigma falls (9, 10).
The theory of planned behavior can be utilized as a framework for creating and executing educational interventions to prevent HIV/AIDS among addicts due to the intervention's strong impact on its structural components (11). Moreover, in high school female students, educational interventions based on the Health Belief Model were successful in promoting AIDS preventive beliefs by increasing knowledge and perceived susceptibility (12).
Several quasi-experimental studies that looked at the impact of educational and awareness interventions on HIV stigma back this up (13, 14). For example, a study in Canada found that raising participants' HIV awareness helped them become community influence champions, which reduced HIV stigma (13). Furthermore, a more sensitive cultural study found that the authors' educational and awareness interventions in a healthcare context reduced HIV stigma and prejudice in Egypt (14). Finally, the majority of the US Centers for Disease Control and Prevention (CDC) activities are centered on programs that combine public education and social marketing campaigns (15).
In Saudi Arabia, the rate of HIV infection increased by 0.5–2.5 percent between 1984 and 2009 (16). HIV infections are more common in Jeddah than in any other city in the Kingdom, which could be attributed, at least in part, to the fact that Jeddah is the country's principal seaport and airport, with higher population movement (17). While immigrants account for most HIV cases in Saudi Arabia, there has been a considerable increase in the proportion of cases among the Saudi population (18).
Even though the introduction of highly active antiretroviral medication has reduced mortality and improved quality of life, HIV remains a contentious topic and taboo in the MENA region (19). The region's data continues to reveal a low level of understanding, which is linked to a higher level of stigma (20, 21). A study of university students in the United Arab Emirates, for example, found serious knowledge gaps as well as high levels of fear and intolerance toward PLWHA (22). The study surveyed medical students at Qassim University in Saudi Arabia showed a modest level of knowledge and negative attitudes toward PLHIV (23).
Based on the preceding, it is critical to have a comprehensive understanding of the degree of knowledge and attitudes about HIV/AIDS so that suitable and relevant awareness and prevention programs may be planned. As a result, the goal of this study was to assess the knowledge of HIV/AIDS transmission modes and attitudes toward HIV/AIDS infected people, as well as the level of HIV/AIDS awareness among the general population in the Kingdom of Saudi Arabia.
The current online community-based cross-sectional descriptive study was conducted using a self-administrated electronic questionnaire to assess the Saudi population's knowledge regarding transmission modes of HIV/AIDS and their attitude toward HIV/AIDS-infected people. This questionnaire was distributed among the general population of the Kingdom of Saudi Arabia between October 2017 and February 2018.
A pre-tested structured, standard questionnaire consisting of 36 close-ended questions was randomly administered to the general population of the Kingdom of Saudi Arabia via social media platforms such as WhatsApp, Twitter, Facebook, Instagram, etc. Additionally, it was distributed in the public campaign regarding World AIDS Day in Heraa General Hospital.
The questionnaires were designed based on the AIDS Indicator Survey model developed by the MEASURE DHS program and the AIDS survey model with some indicators from the National HIV/AIDS prevention programs for young people (24). Five specialists checked the questionnaire's content validity in the fields of public health, epidemiology, and biostatistics. An online pilot study of 45 participants was conducted to ensure the survey's acceptability and consistency. Then, minor modifications were made according to the pilot study results.
The questionnaire was divided into four main sections: (1) socio-demographic characteristics (6 items), (2) knowledge of HIV/AIDS transmission modes (12 items), (3) attitude questions toward HIV/AIDS infected people (7 items), and (4) attitude questions toward the level of HIV/AIDS awareness in Saudi Arabia (11 items).
Adults aged 16 years or older (both genders) residing in Saudi Arabia and signed consent forms were included in the present study. To ensure that participants were still living in Saudi Arabia, they were asked to provide their housing address and the name of the neighborhood.
People less than 16 years or from a nation other than Saudi Arabia were excluded from the present study.
The sample size for this study was calculated to be a total of 384 individuals living in Saudi Arabia aged 18 and over, including Saudi and non-Saudi. This sample size was estimated as described by Kadam and Bhalerao (25), based on a confidence interval of 95% and 5% marginal error with a 0.05 alpha level (25).
The participants were asked to approve their participation before proceeding with the online survey. Ethical approval was obtained from the Faculty of Applied Medical Sciences ethics committee. Informed consent for an internet survey was also obtained from each participant. No monetary rewards were given for completing the questionnaire.
The Statistical Package for Social Science (IBM SPSS) version 20 was used for data analysis. Findings were presented as frequency and percentage tables; a Chi-square test was performed to identify relationships for categorical variables with P-value ≤ 0.05. The One-Way ANOVA test determined the mean differences in quantitative variables between the two groups. Meanwhile, Spearman's rank correlation coefficient (P-value ≤ 0.05) was applied to assess the association between knowledge and attitudes.
The measurement scale of knowledge and attitude questions was used on a five-point Likert scale (5 = Always true, 4 = Sometimes true, 3 = neutral, 2 = sometimes but infrequently true, and 1 = Never true) and (5 = Strongly Agree, 4 = agree, 3 = neutral, 2 = disagree, and 1 = strongly disagree), respectively, then changed and presented in this paper as a dichotomous classification. A score less than three was considered a negative response. In contrast, scores of 3 and 4 were considered positive responses. For the responses of participants to attitude items toward the level of HIV/AIDS awareness in Saudi Arabia, we kept the scale in its original form (5 = strongly agree, 4 = agree, 3 = neutral, 2 = disagree, and 1 = strongly disagree).
The sum score of each outcome was evaluated according to Bloom's cutoff point. The scores for knowledge and attitude were transformed into mean percentage scores by dividing the sum scores obtained by the respondents by the number of items multiplied by 100. Consequently, the overall mean percentage of scores for each category of knowledge and attitude at 60% and above was considered a good level, whereas <60% was deemed a poor level (26).
A total of 2,081 subjects residing in the Kingdom of Saudi Arabia participated in this survey. More than half of the participants (59.0%) had ages ranging between 20 and 29 years. Almost three-quarters (73.2%) of the study participants were females. The vast majority of the participants were Saudi people (94.3%). The marital status of more than half of the study participants (57.0%) was single. 67.6% of the study participants had a bachelor's degree. The monthly income of 68% of the study participants was ≤ 8,699 Saudi Arabian Riyals (Table 1).
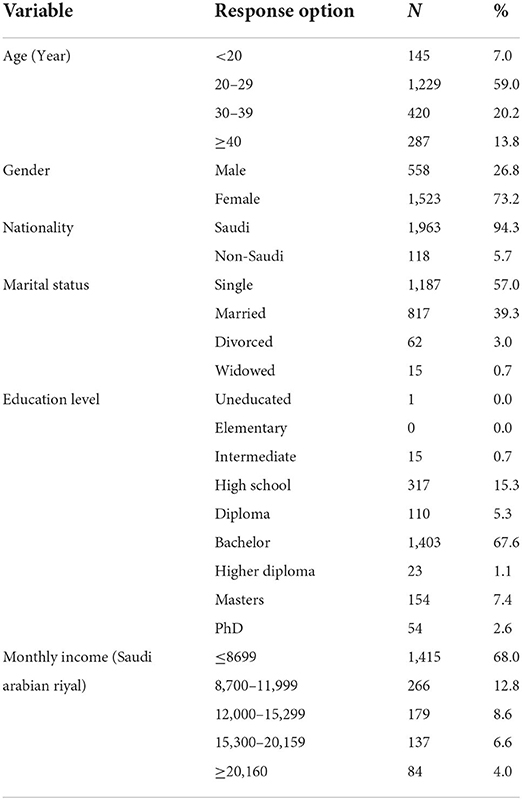
Table 1. Socio-demographic characteristics (N = 2,081).
Twelve items assessed the knowledge of HIV/AIDS transmission modes among the study participants. The highest level of good knowledge was for the item on HIV/AIDS general knowledge. In contrast, the lowest level of good knowledge was evident in responses to items related to HIV infection cases in Saudi Arabia. The mean score of the participant's responses to knowledge items regarding HIV/AIDS transmission modes was 84.2 ± 15.8% (Table 2).
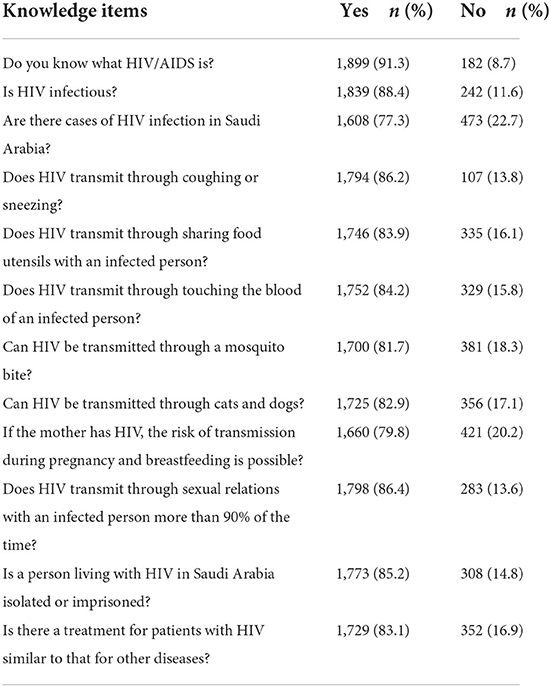
Table 2. Responses of participants to knowledge items on HIV/AIDS transmission modes (N = 2,081).
The attitude toward HIV/AIDS-infected people among the study participants was evaluated using seven items. The highest level of positive attitude was for the item supporting the dissemination of awareness about how HIV is transmitted. In contrast, the lowest level of positive attitude was evident in responses to items related to accepting the idea of marrying an HIV-infected person. The mean score of the participant's responses to attitude items toward HIV/AIDS infected people was 50.1 ± 49.9% (Table 3).
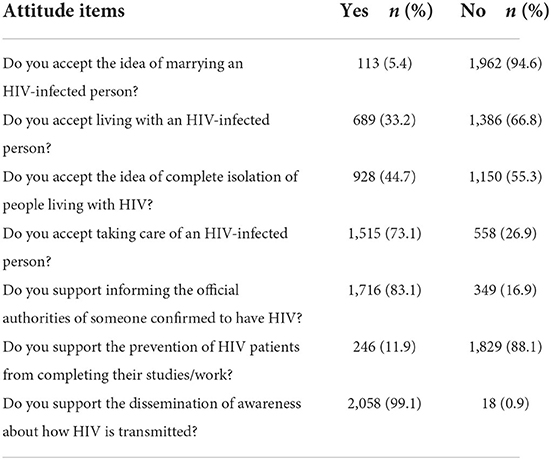
Table 3. Responses of participants to attitude items toward HIV/AIDS infected people (N = 2,081).
Almost 80.6% rated with strong agreement that “it is better to educate high school students and universities,” while 18.8% strongly disagreed with the question being asked as “the level of HIV awareness in Saudi Arabia is sufficient”. The mean score of the participant's responses to attitude items toward the level of HIV/AIDS awareness in Saudi Arabia was 55.7 ± 3.6% (Table 4).
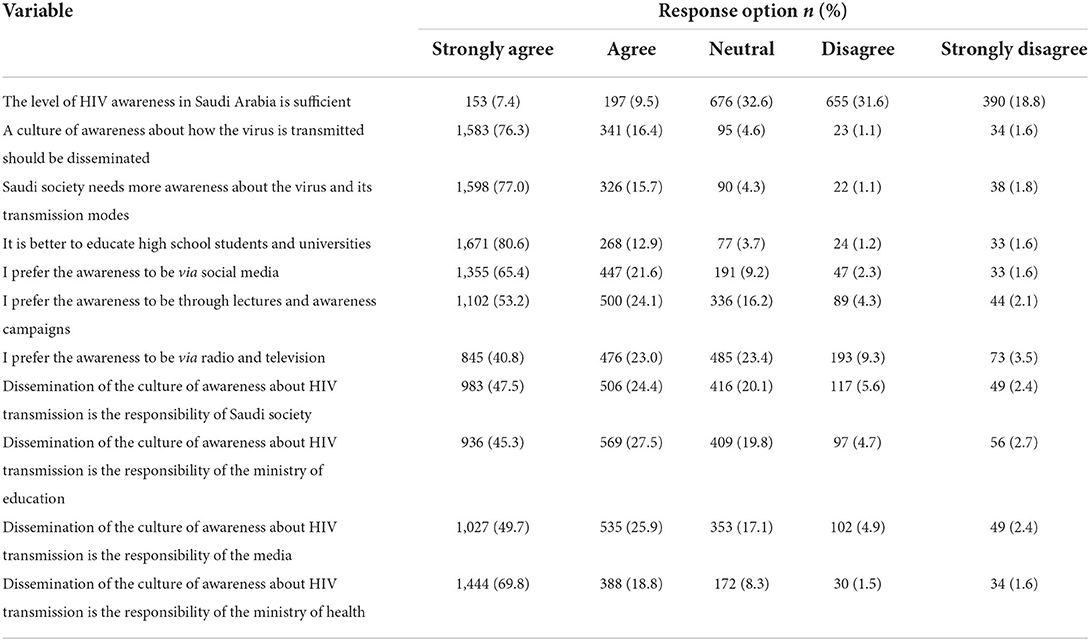
Table 4. Responses of participants to attitude items toward the level of HIV/AIDS awareness in Saudi Arabia (N = 2081).
Among study participants' characteristics variables, age, nationality, marital status, education level, and monthly income were significantly associated with mean scores of knowledge of HIV/AIDS transmission modes (P-value ≤ 0.05). Furthermore, a significant difference was found in age, education level, and monthly income with mean scores of attitude toward HIV/AIDS infected people (P-value ≤ 0.05). Furthermore, age, nationality, marital status, and education level have a significant relationship with mean scores of attitude toward the level of HIV/AIDS awareness (P-value ≤ 0.05) (Table 5).
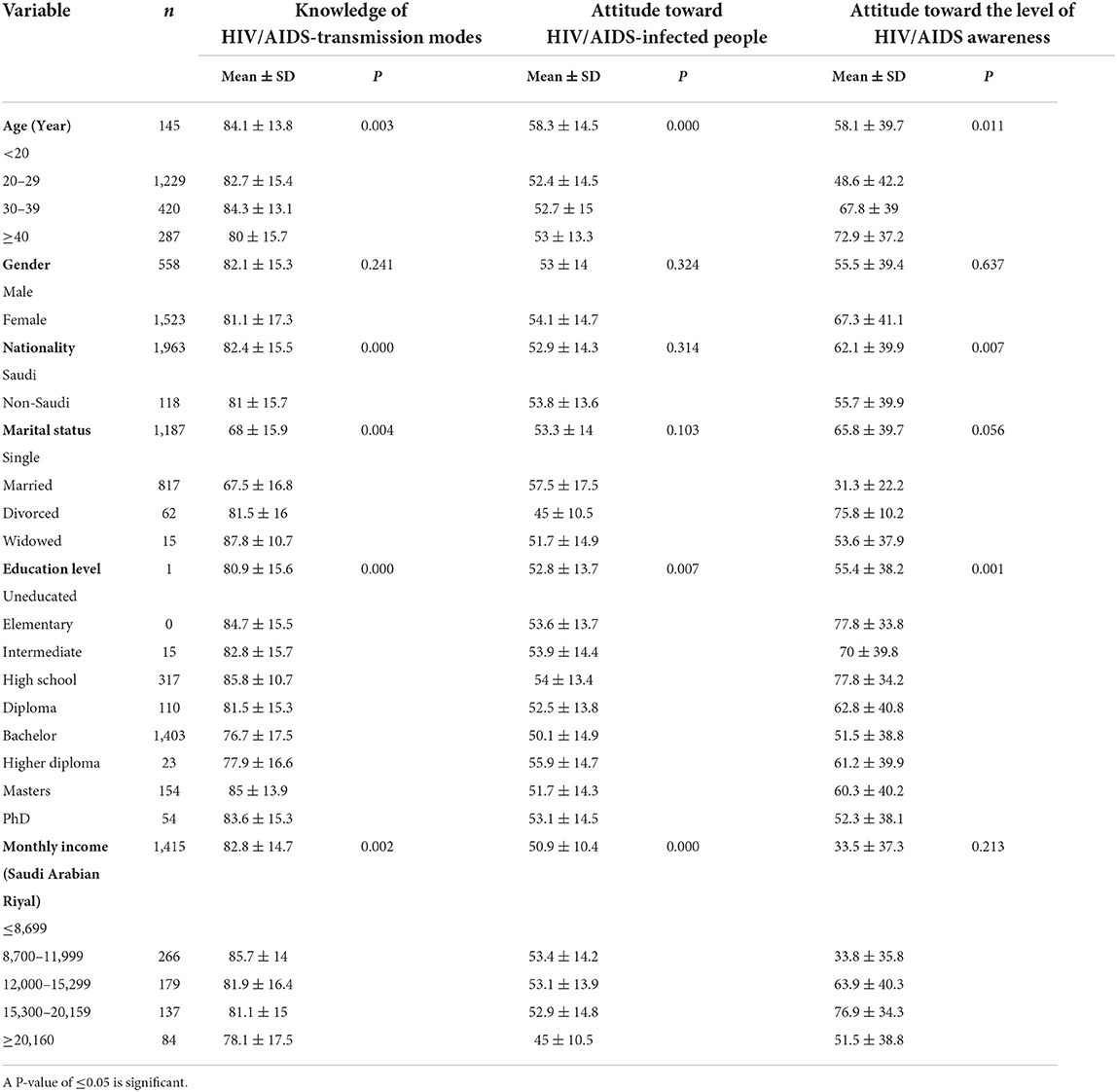
Table 5. Mean scores of knowledge of HIV/AIDS transmission modes, attitudes toward HIV/AIDS infected people, and attitudes toward the level of HIV/AIDS awareness.
Spearman rank correlation explained significant negative linear correlations between knowledge of HIV/AIDS transmission modes-attitudes toward HIV/AIDS infected people and knowledge of HIV/AIDS transmission modes-attitudes toward the level of HIV/AIDS awareness of r = −0.040 and r = −0.070, respectively (P-value ≤ 0.05). Otherwise, there was a positive linear correlation between attitudes toward HIV/AIDS infected people-attitudes toward the level of HIV/AIDS awareness (r = 0.080, p = 0.072) (Table 6).
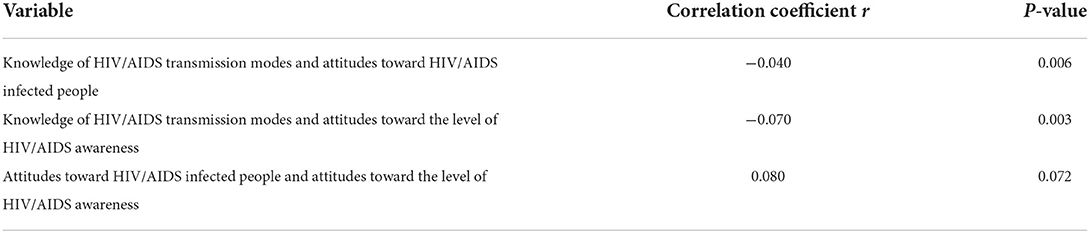
Table 6. Correlation between knowledge of HIV/AIDS transmission modes, attitudes toward HIV/AIDS infected people, and attitudes toward the level of HIV/AIDS awareness score.
The present study provided insights on knowledge of HIV/AIDS transmission modes and attitudes toward HIV/AIDS infected people, as well as the level of HIV/AIDS awareness among the general population in the Kingdom of Saudi Arabia. The mean score of the participant's responses to knowledge items on HIV/AIDS transmission modes was 84.2 ± 15.8%.
Earlier surveys of the general population of Saudi Arabia (5, 27), Saudi medical school students (23, 28), Saudi non-medical school students (29), other countries in the region (30, 31), other African countries (32, 33) have reported a low level of understanding of HIV/AIDS. However, higher knowledge levels have been linked to younger age groups, better education, and knowing someone living with HIV/AIDS, implying that educational initiatives could positively influence the level of knowledge regarding HIV/AIDS. This has been demonstrated in European longitudinal surveys, where 15 years of ongoing teaching efforts greatly enhanced HIV and AIDS knowledge among high school students in Greece (34).
Inadequate understanding might lead to needless anxieties about interacting with HIV/AIDS patients, contributing to stigmatization (33). When the knowledge scores of males and females were compared, males had a higher knowledge score. Males have a greater HIV prevalence than females, which can be linked. During the decade 2000–2009, men accounted for two-thirds of all new cases (18). The gap in knowledge scores between male and female participants could also be linked to gender imbalance at the education level. This gap could also be related to differences in age profile in males and females. Accordingly, we recommend future studies to statistically illuminate these issues.
The mean score of the participant's responses to attitude items toward HIV/AIDS infected people was 50.1 ± 49.9%. The mean score of the participant's responses to attitude items toward the level of HIV/AIDS awareness in Saudi Arabia was 55.7 ± 3.6%. These findings came from the fact that a low percentage of the study respondents had positive attitudes toward HIV/AIDS infected people and the level of HIV/AIDS awareness among the general population in Saudi Arabia. Several other surveys in Saudi Arabia and other parts of the world have found similar negative attitudes, but at a lower level (5, 30–32, 35).
People living with HIV/AIDS were also stigmatized in this group. Treatment initiation has been demonstrated to be hampered by social stigma. Mahajan et al. examined the occurrence of societal stigma linked with HIV/AIDS and its detrimental influence on AIDS preventive actions, as well as measures for reducing the stigma (36).
In terms of HIV/AIDS preventive efforts, South Africa has established an interesting example in terms of community-based HIV awareness and education campaigns, HIV prevention research, and the introduction of antiretroviral medication (ART). This holistic strategy has resulted in enhanced community awareness, which has reduced social stigma and resulted in increased uptake of volunteer counseling and HIV testing (37).
HIV awareness has recently increased due to initiatives, marketing, and social media. Promoting an awareness campaign, such as the CDC's “Get Tested” initiative, which suggests that all people aged 13 to 64 be tested for HIV, would be a further step in enhancing routine health care (38). The need to reduce societal stigma around HIV/AIDS, provide social protection, and improve the general public's awareness and attitudes toward people living with HIV/AIDS have all been cited as essential aspects of the epidemic's control (35, 39, 40).
A comprehensive approach is needed to change those unfavorable views, including more support for people living with HIV/AIDS and the improvement of the healthcare system's many sectors. Patients' confidentiality must be ensured, as many Saudi Arabian patients still feel embarrassed seeking appropriate care, resulting in insufficient therapy and delayed treatment. Patients are often ignorant of the technological technologies employed in hospitals to provide anonymity, and there is a need to raise awareness of this. In response to the outbreak, the Saudi Ministry of Health launched a national AIDS program to monitor and coordinate efforts to prevent, diagnose, and treat HIV across the country. Every Saudi citizen infected with HIV or AIDS is entitled to free medical care and has their privacy about how they became infected protected by law. Another strategy for combating discrimination and stigmatization would be support groups.
The findings of the current study should be evaluated in light of several limitations. Though the sample is of reasonable size, the convenience sampling method was used, which has likely led to selection bias in our study population and the generalizability of our findings. The study was cross-sectional in design, limiting the making of causal inferences. There were no qualitative questions provided. A qualitative component could have aided in a better understanding of negative views about HIV/AIDS patients and provided a complete picture of the causes behind those sentiments.
The study showed that a high percentage of the study respondents had good knowledge of HIV/AIDS transmission modes. However, a low percentage of the study respondents had positive attitudes toward HIV/AIDS infected people, and the level of HIV/AIDS awareness was also low. There were some statistically significant associations between several socio-demographic variables and mean scores of knowledge of HIV/AIDS transmission modes, mean scores of attitude toward HIV/AIDS-infected people, and mean scores of attitude toward the level of HIV/AIDS awareness. Significant negative linear correlations between knowledge of HIV/AIDS transmission modes-attitudes toward HIV/AIDS infected people, and knowledge of HIV/AIDS transmission modes-attitudes toward HIV/AIDS aware people were shown. Otherwise, there was a positive linear correlation between attitudes toward HIV/AIDS infected people-attitudes toward the level of HIV/AIDS awareness. Therefore, there is a dire need for advocacy campaigns and policies to help reduce HIV stigmatization.
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
This study was reviewed and approved by the Faculty of Applied Medical Sciences ethics committee. Written informed consent was obtained from all participants for their participation in this study.
SK and FQ had the idea for the paper, developed the conceptual approach, wrote the first draft, and revised the manuscript. RTA and SN conceptualized the study. RAA collected the data. MA and HM carried out statistical analyses. All authors have read and approved the final version of the manuscript.
The authors are grateful to all the participants for their valuable voluntary participation in this study. The Faculty of Applied Medical Sciences ethics committee is also appreciated for giving us ethical approval to conduct the study in Saudi Arabia.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Gallant JE. Human immunodeficiency virus medicine. J Infect Dis. (2017) 216:624–5. doi: 10.1093/infdis/jix238
2. UNAIDS. Global HIV & AIDS statistics-−2018 fact sheet. The Joint United Nations Programme on HIV/AIDS. Available online at: https://www.unaids.org/en/resources/fact-sheet (2018) (accessed March 2, 2022).
3. Gökengin D, Doroudi F, Tohme J, Collins B, Madani N. HIV/AIDS: trends in the Middle East and North Africa region. Int J Infect Dis. (2016) 44:66–73. doi: 10.1016/j.ijid.2015.11.008
4. Akala FA, Semini I. Characterizing the HIV/AIDS epidemic in the Middle East and North Africa: Time for Strategic Action. Washington, DC: The World Bank. (2010).
5. Alwafi HA, Meer AM, Shabkah A, Mehdawi FS, El-Haddad H, Bahabri N, et al. Knowledge and attitudes toward HIV/AIDS among the general population of Jeddah, Saudi Arabia. J Infect Public Health. (2018) 11:80–4. doi: 10.1016/j.jiph.2017.04.005
6. Herek GM, Capitanio JP, Widaman KF. HIV-related stigma and knowledge in the United States: prevalence and trends, 1991–1999. Am J Public Health. (2002) 92:371–7. doi: 10.2105/AJPH.92.3.371
7. Turan JM, Bukusi EA, Onono M, Holzemer WL, Miller S, Cohen CR. HIV/AIDS stigma and refusal of HIV testing among pregnant women in rural Kenya: results from the MAMAS Study. AIDS Behav. (2011) 15:1111–20. doi: 10.1007/s10461-010-9798-5
8. Zhang C, Li X, Liu Y, Qiao S, Zhang L, Zhou Y, et al. Stigma against people living with HIV/AIDS in China: does the route of infection matter? PLoS ONE. (2016) 11:e0151078. doi: 10.1371/journal.pone.0151078
9. Farotimi AA, Nwozichi CU, Ojediran TD. Knowledge, attitude, and practice of HIV/AIDS-related stigma and discrimination reduction among nursing students in southwest Nigeria. Iran J Nurs Midwifery Res. (2015) 20:705. doi: 10.4103/1735-9066.170011
10. Sohn A, Park S. HIV/AIDS knowledge, stigmatizing attitudes, and related behaviors and factors that affect stigmatizing attitudes against HIV/AIDS among Korean adolescents. Osong Public Health Res Perspect. (2012) 3:24–30. doi: 10.1016/j.phrp.2012.01.004
11. Abbaspour A, Jalili Z, Shojaeizadeh D. Study the effect of education based on the theory of planned behavior in the prevention of AIDS among addicts. Iran J Health Educ Health Promot. (2021) 9:201–11. doi: 10.52547/ijhehp.9.2.201
12. Rafiei N, Aghapoor S, Behnampour N, Heshmati H, Ghasemyani S. Promoting AIDS preventive beliefs in Turkmen students by using the health belief model in Aq-Qala. Iran J Health Educ Health Promot. (2019) 7:323–2. doi: 10.29252/ijhehp.7.4.323
13. Li AT-W, Fung KP-L, Maticka-Tyndale E, Wong JP-H. Effects of HIV stigma reduction interventions in diasporic communities: insights from the CHAMP study. AIDS Care. (2018) 30:739–45. doi: 10.1080/09540121.2017.1391982
14. Lohiniva A-L, Benkirane M, Numair T, Mahdy A, Saleh H, Zahran A, et al. HIV stigma intervention in a low-HIV prevalence setting: a pilot study in an Egyptian healthcare facility. AIDS Care. (2016) 28:644–52. doi: 10.1080/09540121.2015.1124974
15. Beer L, McCree DH, Jeffries IV WL, Lemons A, Sionean C. Recent US centers for disease control and prevention activities to reduce HIV stigma. J Int Assoc Provid AIDS Care (JIAPAC). (2019) 18:2325958218823541. doi: 10.1177/2325958218823541
16. Al-Mozaini MA, Mansour MK, Al-Hokail AA, Mohmed MA, Daham MAB, Al-Abdely HM, et al. HIV-care outcome in Saudi Arabia; a longitudinal cohort. J AIDS Clin Res. (2014) 5:370. doi: 10.4172/2155-6113.1000370
17. Madani TA, Al-Mazrou YY, Al-Jeffri MH, Al Huzaim NS. Epidemiology of the human immunodeficiency virus in Saudi Arabia; 18-year surveillance results and prevention from an Islamic perspective. BMC Infect Dis. (2004) 4:1–8. doi: 10.1186/1471-2334-4-25
18. Mazroa MAl, Kabbash IA, Felemban SM, Stephens GM, Al-Hakeem RF, Zumla AI, et al. HIV case notification rates in the Kingdom of Saudi Arabia over the past decade (2000–2009). PLoS ONE. (2012) 7:e45919. doi: 10.1371/journal.pone.0045919
19. Abu-Raddad LJ, Hilmi N, Mumtaz G, Benkirane M, Akala FA, Riedner G, et al. Epidemiology of HIV infection in the Middle East and North Africa. AidS. (2010) 24:S5–23. doi: 10.1097/01.aids.0000386729.56683.33
20. Badahdah AM. Stigmatization of persons with HIV/AIDS in Saudi Arabia. J Transcul Nurs. (2010) 21:386–92. doi: 10.1177/1043659609360873
21. Gańczak M, Barss P, Alfaresi F, Almazrouei S, Muraddad A, Al-Maskari F. Break the silence: HIV/AIDS knowledge, attitudes, and educational needs among Arab university students in United Arab Emirates. J Adolesc Health. (2007) 40:572. doi: 10.1016/j.jadohealth.2007.01.011
22. Kahhaleh J, El Nakib M, Jurjus A. Knowledge, attitudes, beliefs and practices in Lebanon concerning HIV/AIDS, 1996-2004. East Mediterr Health J. (2009) 15:920–33. doi: 10.26719/2009.15.4.920
23. Alawad M, Alturki A, Aldoghayyim A, Alrobaee A, Alsoghair M. Knowledge, attitudes, and beliefs about HIV/AIDS and people living with HIV among medical students at Qassim University in Saudi Arabia. Int J Health Sci (Qassim). (2019) 13:22.
24. WHO. National AIDS programmes: a guide to indicators for monitoring and evaluating national HIV/AIDS prevention programmes for young people. World Health Organization. Available online at: n.a;http://www.who.int/maternal_child_adolescent/documents/9241592575/en/ (accessed August 4, 2017).
25. Kadam P, Bhalerao S. Sample size calculation. Int J Ayurveda Res. (2010) 1:55. doi: 10.4103/0974-7788.59946
26. Bloom BS, Engelhart MD, Furst E, Hill WH, Krathwohl DR. Handbook I: Cognitive Domain. New York: David McKay. (1956).
27. Al-Ghanim SA. Exploring public knowledge and attitudes towards HIV/AIDS in Saudi Arabia. A survey of primary health care users. Saudi Med J. (2005) 26:812–8.
28. Al-Mazrou YY, Abouzeid MS, Al-Jeffri MH. Knowledge and attitudes of paramedical students in Saudi Arabia toward HIV/AIDS. Saudi Med J. (2005) 26:1183–9.
29. Al-Jabri AA, Al-Abri JH. Knowledge and attitudes of undergraduate medical and non-medical students in Sultan Qaboos University toward acquired immune deficiency syndrome. Saudi Med J. (2003) 24:273–7.
30. Tavoosi A, Zaferani A, Enzevaei A, Tajik P, Ahmadinezhad Z. Knowledge and attitude towards HIV/AIDS among Iranian students. BMC Public Health. (2004) 4:1–6. doi: 10.1186/1471-2458-4-17
31. Savaser S. Knowledge and attitudes of high school students about AIDS: A Turkish perspective. Public Health Nurs. (2003) 20:71–9. doi: 10.1046/j.1525-1446.2003.20110.x
32. Nubed CK, Akoachere J-FTK. Knowledge, attitudes and practices regarding HIV/AIDS among senior secondary school students in Fako Division, South West Region, Cameroon. BMC Public Health. (2016) 16:1–10. doi: 10.1186/s12889-016-3516-9
33. Tarkang EE, Lutala PM, Dzah SM. Knowledge, attitudes and practices regarding HIV/AIDS among senior high school students in Sekondi-Takoradi metropolis, Ghana. Afr J Primary Health Care Family Med. (2019) 11:1–11. doi: 10.4102/phcfm.v11i1.1875
34. Merakou K, Costopoulos C, Marcopoulou J, Kourea-Kremastinou J. Knowledge, attitudes and behaviour after 15 years of HIV/AIDS prevention in schools. Eur J Public Health. (2002) 12:90–3. doi: 10.1093/eurpub/12.2.90
35. Mahajan AP, Sayles JN, Patel VA, Remien RH, Ortiz D, Szekeres G, Coates TJ. Stigma in the HIV/AIDS epidemic: a review of the literature and recommendations for the way forward. AIDS. (2008) 22(Suppl. 2):S67. doi: 10.1097/01.aids.0000327438.13291.62
36. Parker R, Aggleton P, HIV. and AIDS-related stigma and discrimination: a conceptual framework and implications for action. Soc Sci Med. (2003) 57:13–24. doi: 10.1016/S0277-9536(02)00304-0
37. Mall S, Middelkoop K, Mark D, Wood R, Bekker L-G. Changing patterns in HIV/AIDS stigma and uptake of voluntary counselling and testing services: the results of two consecutive community surveys conducted in the Western Cape, South Africa. AIDS Care. (2013) 25:194–201. doi: 10.1080/09540121.2012.689810
38. CDC. Division of HIV/AIDS prevention, National center for HIV/AIDS, viral hepatitis, sexual transmitted diseases and tuberculosis prevention. HIV Among African Americans. Centers for Disease Control and Prevention. (2013).
39. Cluver LD, Orkin MF, Yakubovich AR, Sherr L. Combination social protection for reducing HIV-risk behavior amongst adolescents in South Africa. Journal of acquired immune deficiency syndromes (1999). (2016) 72:96. doi: 10.1097/QAI.0000000000000938
Keywords: attitude, HIV/AIDS, knowledge, Saudi Arabia, transmission modes
Citation: Qashqari FS, Alsafi RT, Kabrah SM, AlGary RA, Naeem SA, Alsulami MS and Makhdoom H (2022) Knowledge of HIV/AIDS transmission modes and attitudes toward HIV/AIDS infected people and the level of HIV/AIDS awareness among the general population in the kingdom of Saudi Arabia: A cross-sectional study. Front. Public Health 10:955458. doi: 10.3389/fpubh.2022.955458
Received: 28 May 2022; Accepted: 29 August 2022;
Published: 27 September 2022.
Edited by:
Ana Afonso, Universidade NOVA de Lisboa, PortugalReviewed by:
Hadi Tehrani, Mashhad University of Medical Sciences, IranCopyright © 2022 Qashqari, Alsafi, Kabrah, AlGary, Naeem, Alsulami and Makhdoom. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Saeed M. Kabrah, c21rYWJyYWhAdXF1LmVkdS5zYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.