 Zheng Zang1,2*†
Zheng Zang1,2*†- 1School of Marxism, Soochow University, Suzhou, China
- 2Soochow University Base, Jiangsu Research Centre for Socialist Theory System With Chinese Characteristics, Suzhou, China
For the past few decades, studies of care types choice have been restricted to the scope of individual characteristics and health status. Meanwhile, the historiography of the research largely ignores the role of filial culture within China. This study sets out to examine the influence of the factors in the cultural context of filial piety on the choice of care types for older people with disability in China. According to the characteristics of filial culture, the factors influencing the choice of care type for the older people in China are summarized as family endowment and support. The study concludes that gender, residence, living alone or not, family income, real estate, pension and community service have momentous effects on the choice of care type of older people with disability; informal care has a substitutive effect on formal care. The research was based on cross-sectional data of CLHLS 2018 and utilized binary logistic regression analysis to compare the factors influencing the choice of old disabled people between formal and informal care. The study implies that in the context of filial culture, the older people's choice of care types is affected by family endowment and community service supply for the older people in China. In the background of filial culture, the government should give informal care official support such as cash and services, so as to change its attribute of private domain of it and enhance the quality of long-term care.
Introduction
In the study of quality of care, the choice of care types, as an important factor in long-term care, has attracted an increasing attention. There is increasing evidence which suggests that formal care has a higher quality of care than informal one (1–6). This is not only reflected in the assessment of physical and functional health of the care recipient, but also means that the psychological stress of them is reduced due to the reduced mental and life burden of their family members (7–10). Regrettably, in the past, the research on choice of care types in long-term care in Chinese academia focused more on individual characteristics and health status (11–13). And the historiography of the research largely ignores the role of filial culture within China (14, 15).
Background and problem statement
Under the dual background of aging and filial culture, balancing formal and informal care is one of the effective ways to optimize the long-term care system and meet the caring needs of older people with disabilities (16–18). With the extension of life expectancy and the decline of human fecundity, the proportion of the aging population in China is growing rapidly, which makes China face the challenge of aging population (19). The extension of life expectancy is often accompanied by the decline of self-care ability. In other words, aging and disability occur at the same time (20). Another challenge of the aging population is the huge economic burden of long-term care on families and society (21). Care is one of the core concepts of social policy (22). The World Health Organization (WHO) proposes that long-term care is a system of activities carried out by informal caregivers (family, friends and/or neighbors) and/or professionals (health, social and others), so as to ensure that people who lack full self-care ability can maintain the highest possible quality of life according to their personal priorities and enjoy the greatest possible independence, autonomy, participation, personal enrichment and human dignity (23). In this article, formal care includes social services and nanny care (24, 25). Informal caregivers include spouse, children, grandchildren, daughter-in-law, son-in-law, other relatives, friends and neighbors (26, 27). There is also a care type which is a combination of formal and informal care (28). However, many researchers believe that this is not the mainstream type of care, so it will not be discussed in this article (29, 30).
Current research on formal and informal care is mainly focused on the research in Europe, America, Japan and Korea (6, 17, 25, 26). Fewer researchers in developing countries conducted research on this topic due to young demographic structure and the low pressure of aging. In the last decade or so, due to the rapid development of the aging population in China, Chinese researchers have been conducting research on formal and informal caregiving, drawing on research findings from developed countries (12, 18, 20). There has been much academic debate about the relationship between formal and informal care. Some studies from developed countries have suggested there might be three different relationships between them, which are complementary, alternative and parallel (31–34). According to the view of complementary one, there is a supplementary relationship between formal and informal care, that is, the more family care the older people with disability receive, the more social support they will receive (31). From the perspective of alternative relationship, the increase of informal care will produce a crowding out effect on formal care, which not only reduces the probability of older people with disability entering the nursing home or delays entry (32), but also reduces the use timing and probability of formal care services (33). In the view of parallel relationship, informal and formal care have an impact on the choice of care mode for older people with disability at the same time, rather than mutual influence. After the disabled use formal care, the demand for informal care will decline, but still maintain at a fixed level (34).
Theoretical framework
Traditionally, China has been dominated by informal care in the form of family care. Formal long-term care in China started late, but there has been a long practice of 'quasi' long-term care services based on institutionalized care of older people (20). In contrast to institutional long-term care, formal home-based and community-based long-term care in China has started to develop in the last decade or so (18). With regard to the long-term care insurance system that accompanies long-term care services, there has been a marked acceleration in the pace of government-led long-term care insurance in China's mainland over the last 5 years (21). At present, the formal care service system for older people with disability in China has not been established, and the existing care service supply cannot effectively meet the caring needs of older people with disability, resulting in the limited substitution of formal care for informal one (13, 15). At the same time, the service contents of formal and informal care are quite different, so it is difficult to realize the perfect replacement of informal care (18). With the influence of traditional culture, especially filial piety culture, informal care is still the main way of care in China (14, 20). However, with the empty nest and fewer children, the supply of informal care represented by family care cannot meet the caring needs of the existing older people with disabilities (21). Some researchers believe that informal care for the older people, as an important part of long-term care, is not free, and may exceed the economic expenditure of formal one (35, 36). Therefore, more and more researchers realize that the evaluation of informal care can help to formulate long-term care policies for its sustainable development (37). At present, the related research mainly includes: the cost of disease care of older people (38), caregiver's economic burden and opportunity cost (39), caregiver's emotional and health cost (40, 41), the trend of informal care cost (42, 43), assessment tools of older people (44), care management (45), the impact of informal care on the health of the older people (46), the comprehensive assessment of the older people (47), the impact of informal care on the health of the older people (43), etc. Informal care faces heavy burden and opportunity cost. More importantly, with the change of traditional concepts and the full opening of the pension service market, formal care services have developed rapidly and become another choice for older people with disability. This article uses CLHLS 2018 (The Chinese Longitudinal Healthy Longevity Survey in 2018) data to analyze the choice of care mode and its influencing factors for the older people with disability in China. Previous studies using CLHLS on older people's care type choices have focused on factors such as gender, education, income, widowhood, ethnic minority status, health status, number of children, and the availability of health insurance and pensions (48–51). However, the information and data collected in the CLHLS on the number of sons, housing status, community services, neighborhood relations and other information of older people in relation to the cultural context of filial piety is often overlooked. Traditional filial culture believes that filial piety is a naturally occurring affection (52). The essence of filial piety, in Mencius' view, is to provide for one's old age (53). As a son or daughter, he or she is obligated to take care of his or her parents, which includes not only taking care of their daily lives, but also comforting their hearts. Whether the children were paying respect and whether they were providing care in times of illness or elderly were most important in determining a sense of filial discrepancy in the parent (54). This feature is reflected in the proverb “Raise children to prevent aging, accumulate grain to prevent hunger.” The culture of filial piety has had a great influence not only in traditional Chinese society, but also in East Asian countries such as Japan and Korea. In traditional East Asian societies, the problem of aging is basically solved within the family (55). In a previous interview with the head of the Japan Welfare Council, when it came to what the biggest challenge of developing a formal long-term care model in Japan was, it was believed that Japan had been traditionally influenced by the Confucian filial culture for a long time making the concept of family-based informal care prevalent. In the midst of rapid aging in Japan, to shift the focus of long-term care from family to society, the need to transform and break through the concept of filial culture was the most difficult and long-term task at that time. In light of this, the article argues that it may be more useful and beneficial in Chinese society to consider cultural factors of filial piety as an influencing factor in the choice of type of care for the older people. The number of activities of daily living (ADL) that cannot be completed is used to measure the disability degree of the older people, and emphasize the functional orientation between informal and formal care among groups with different disability degrees, so as to provide reference for promoting healthy aging.
In this article, we investigate the significant influence of each independent variable on the dependent variable, and test the research hypothesis. The selection of independent variables, in addition to the usual choice of individual characteristics and health status, embodies the characteristics of Chinese filial piety culture mainly in two aspects, namely “raising children for aging” and “living and working in peace and contentment”. “Raising male children for aging” can be reflected in the family endowment represented by the number of sons, family income level, whether to own housing. “Living and working in peace and contentment” can be reflected in whether the community can provide services for the older people. Based on the ideas described above, the following hypotheses were proposed:
Hypothesis 1 (H1). Different care types have different care effects.
Hypothesis 2 (H2). Disabled individuals with different individual characteristics have different preferences for different care types.
Hypothesis 3 (H3). Older people with disability with different physical and mental health status have different preferences for care types.
Hypothesis 4 (H4). Older people with disability with different family endowments have different preferences for care types.
Hypothesis 5 (H5). Whether the community provides services for the older people has an impact on the choice of care types for older people with disability.
Materials and methods
The research was based on cross-sectional data of CLHLS 2018 to compare the influencing factors of older people with disability between formal care and informal care.
Data sources
The data used in this article is from Chinese Longitudinal Healthy Longevity Survey (CLHLS) of Peking University Center for aging health and family research in 2018. The data survey is a follow-up survey of the older people organized by the Research Center for Healthy Aging and Development of Peking University and the National Development Research Institute of China, covering 23 provinces and autonomous regions in China. The respondents are the older people aged 65 and above and the adult family members aged 35–64. The questionnaire is divided into two types: the surviving respondents' questionnaire and the family members of the deceased older people questionnaire. The survey contents of the surviving respondents' questionnaire include the basic situation of the older people and their families, socio-economic background and family structure, economic source and status, self-evaluation of health quality of life, cognitive function, personality and psychological characteristics, daily activities, life-style, life care, disease treatment and medical expenses. The survey contents of the family members of the deceased older people include the time and the cause of death in addition to all the survey content of the surviving one. After the baseline survey in 1998, the survey was conducted in 2000, 2002, 2005, 2008–2009, 2011–2012, 2014 and 2017–2018. The latest follow–up survey data (2017–2018) used in this article interviewed 15,874 older people aged 65 and above, and collected the information of 2,226 older people who died during 2014–2018. CLHLS included a large number of disabled and elderly population samples, and the disability degree of the older people was measured by the Activities of Daily Living Scale (ADLs) and the Instrumental Activities of Daily Living Scale (IADLs), which is helpful to compare the disability degree of the older people in addition. At the same time, CLHLS data is highly representative and reliable.
In this study, the older people who need long-term care were selected according to the six indicators of ADL (bathing, dressing, eating, going to the toilet, controlling defecation and walking indoors) and the time needed to be cared for by others. According to international practice, an older person, who is partially or totally unable to care for himself/herself on at least one of the six indicators or who requires the care of another person for more than 90 days, is considered to be in need of long-term care (7, 9, 12). Through screening from CLHLS 2018, 3510 eligible people were selected as the research sample.
Variable selection
Dependent variable
There are two dependent variables: one is the choice of daily care for the older people with caring needs, including formal and informal care. Formal care includes social services and nanny care (24, 25). Informal caregivers include spouse, children, grandchildren, daughter-in-law, son-in-law, other relatives, friends and neighbors (26, 27). In the initial processing of data, formal care was assigned to 1, while informal care was assigned to 0. The second is the effect of care, including fully meeting the needs of care and not fully meeting the needs of care. The question is measured as the questionnaire “whether the help you get in the six daily activities of e1–e6 can meet your needs” (where e1–e6 stands for the six indicators of ADL) to measure, as the evaluation of control nursing effect. Through the “data conversion” processing, the answer is “fully satisfied” is assigned to 1; the answers are “basically satisfied” and “not satisfied” as “not fully satisfied,” are assigned to 0.
Independent variable
According to previous studies (48, 50, 51), and considering the availability of specific data, this article selects a total of 20 independent variables, including individual characteristics, physical and mental health status, family endowment, community services for the older people. The main variables and their assignments are shown in Table 1. The reliability and validity of the collected data were tested using the Cronbach Alpha coefficient and the KMO and Bartlett tests. The reliability of the variables was analyzed using SPSS. The reliability of the variables was 0.829, which was reliable and passed the reliability test, while the KMO coefficient was 0.708, which had good validity and allowed for factor analysis.

Table 1. Description of variables.
Characteristics of the sample
At present, according to the results of China's seventh census in 2020, the average age of the Chinese population is 38.8 years old (56). Of the Chinese population, 51.24% are male; 48.76% are female (57). In China, 18.70% of the population is aged 60 and over, of which 13.50% is aged 65 and over (58).
Through the analysis of the data, the sample number of older people with disability in CLHLS data in 2018 is 3,510, and the estimated overall disability rate is 22.11%. From the internal structure of the older people with disability, the average age is 95.24 years old. The proportion of the older people is relatively large. What's more, the older they are, the more disabled they are. The proportion of older people with disability in Chinese women is 35.1% higher than that in men, which is 67.55%. The proportion of older people with disability in rural areas is 69.72%, which is 39.44% higher than that in cities and towns. Informal care provided by family members and neighbors is the main care mode for the older people with disability in China, accounting for 85.48%. The proportion of formal social long-term care is relatively small, only 14.52%. In China, 86.20% of older women with disability choose informal care. In rural areas, 93.38% of the older people with disability choose informal care. There are significant gender and urban-rural differences in the long-term care choices of older people with disability in China.
From the perspective of individual characteristics through the analysis of the sample, the average length of education of the older people with disability in China is about 3 years, which is basically equal to the level of primary school. The older people with disability living with their spouses accounts for 30.28%, and the older people with disability living alone accounts for 16.53%. 52.35% of disabled old people enjoy medical insurance, but 94.50% of disabled old people have to pay for care by themselves or their families. From the evaluation of their health status, the vast majority of disabled old people's health status is poor. Because formal care is largely based on trust in others, this article takes trust in others as an independent variable and finds that most older people with disability have higher trust in others.
From the perspective of the background characteristics of filial piety culture through the analysis of the sample, “raising male children for old age” and “living and working in peace and contentment” are two important contents of filial piety culture. In terms of family endowment, the older people with disability in China have an average of 2.8 sons. In addition, 83.62% of the disabled old people own their houses. However, only 26.91% of the older people enjoy retirement insurance benefits. Most old people think their family income is average level. In terms of community services for the older people, only 13.79% of the communities provide daily care services, 17.57% provide spiritual comfort services, and 11.59% provide daily shopping services. 22.59% of the communities will organize community and recreational activities; 21.47% of the communities provide legal aid services. Generally, the three services for the older people provided by the community were health knowledge publicity (42.83%), visiting doctors and drug delivery (36.76%), and mediation of neighborhood disputes (31.15%).
Model construction
In this article, when describing the effect of care style for older people with disability, we use the interactive analysis method for the Chi-square test. Because the choice of daily care for older people with disability is a dependent variable, which belongs to a binary variable, the factors influencing the choice of care mode: individual characteristics, health status, family endowment, community service supply for the older people, as control variables, are included in the model for analysis. Therefore, the Binary Logistic Model was used for regression analysis. The Binary Logistic Regression Model was constructed as follows:
In this model: P is the probability that the daily care of the older people is formal care. 1–P is the probability of informal care. Xi denotes the ith influencing factor. βi is the partial regression coefficient of the ith influencing factor. α is a constant term.
Results
Influencing factors of care satisfaction of older people with disability
According to Table 2, and the Chi-square test, there is no significant difference in formal and informal care satisfaction. Informal care has an alternative effect on formal care. Meanwhile, there are likely significant differences in the satisfaction degree of the older people with different individual characteristics. Among them, age, years of education, living in urban or rural areas, medical insurance, physical health and trust in others all significantly affect the degree of care satisfaction. In terms of family endowments, the number of sons and whether or not to own housing has no significant effect on care satisfaction. However, family income level and whether or not to enjoy retirement benefits significantly likely affect care satisfaction.
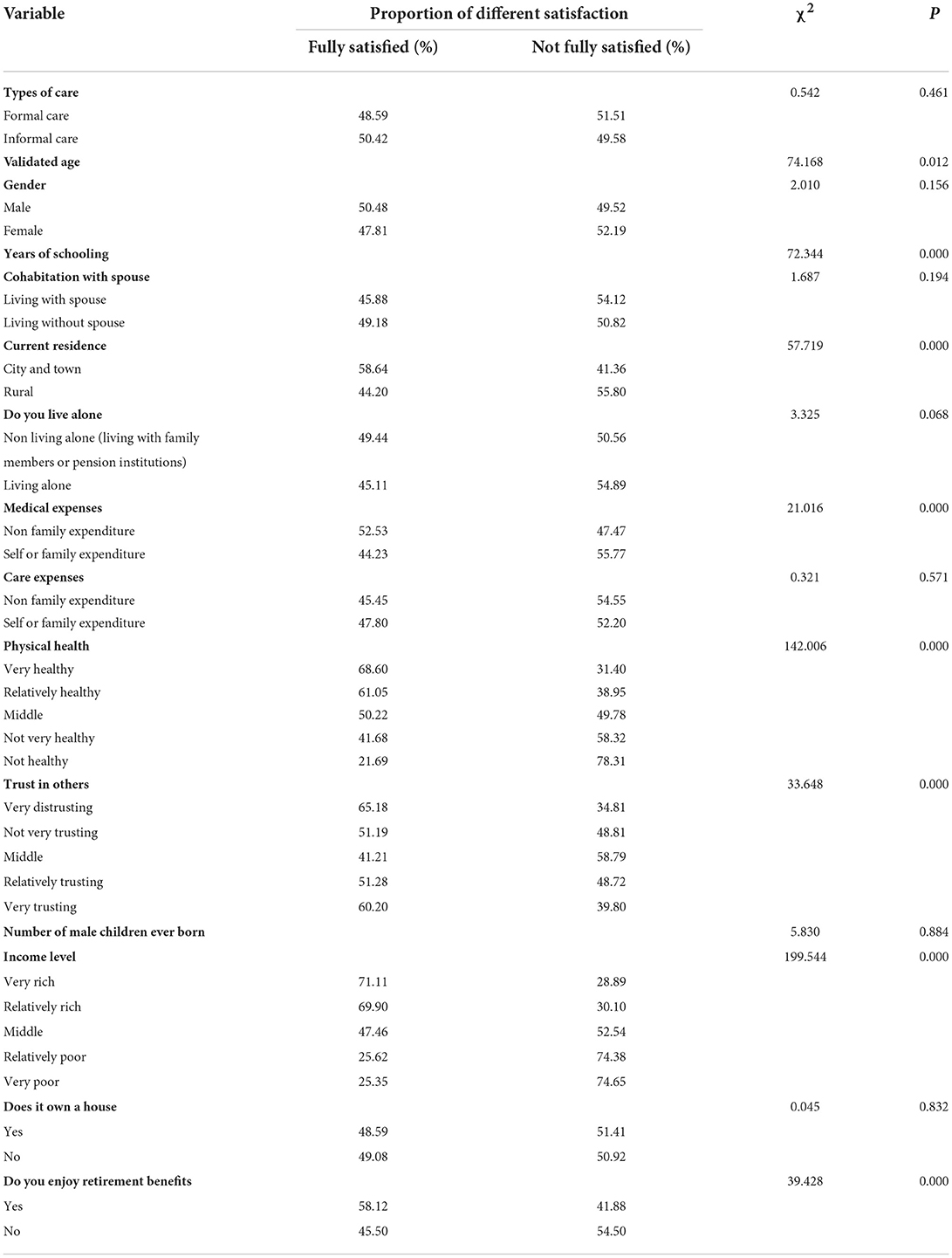
Table 2. Care effects on older people with disability of different characteristics.
Multiple factors influencing the arrangement of care for the older people
According to the above model, a binary logistic regression analysis using SPSS was conducted to identify the factors influencing the care arrangements for the older people. According to the model fitting information generated by Binary Logistic Regression, χ2 = 488.932, significance level (Sig = 0.000) < 0.01, R2 = 0.508, which indicates that the model has good fitting degree and good explanatory ability, as shown in Table 3.
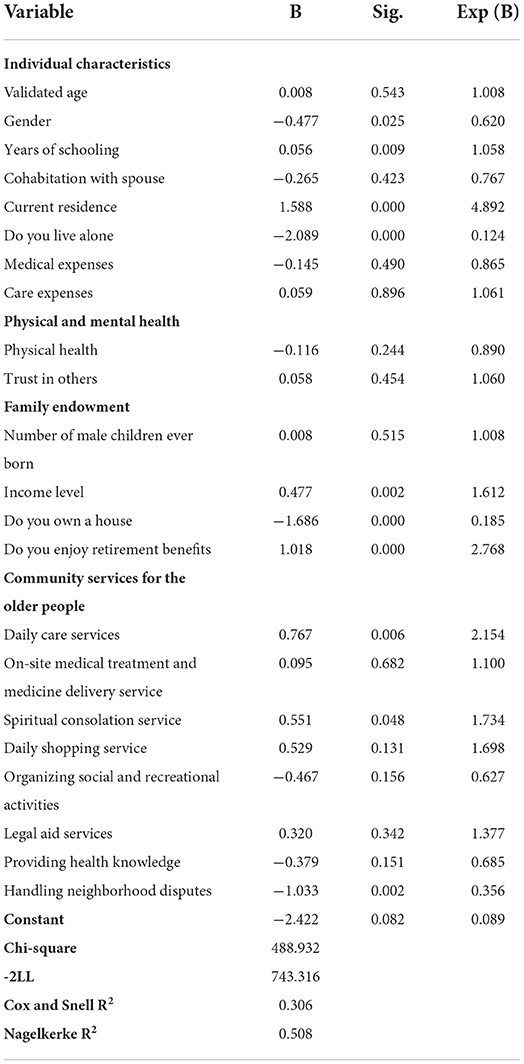
Table 3. Logistic regression analysis of factors influencing the choice of care types for older people with disability.
The influence of individual characteristics on the choice of care types for older people with disability
From Table 3, we can see that gender, education years, residence and whether living alone have a likely significant impact on the choice of care type of older people with disability. The model showed that there is likely no difference in the choice of care type among age, living with spouse or not, payment method of medical expenses and payment method of care expenses. Female older people with disability tend to choose formal care, which is 1.6 times that of male older people with disability. In addition, the educated older people are more likely to choose formal care, which may be less influenced by traditional filial piety culture such as “raising children to guard against old age.” For the choice of care type, older people with disability living in rural and urban areas are different. The older people with disability living in urban areas are 4.89 times more likely to choose formal care than those living in rural areas. Coupled with the influence of traditional filial piety, most rural older people will mainly focus on informal care. Urban older people are better off and can afford to pay for nannies or aged care facilities, while traditional filial influence is less influential, so they are more likely to choose formal care. Compared with the older people who are not living alone, the older people who live alone are more likely to choose formal care, and the probability is eight times of that of the older people who are not living alone.
The influence of family endowment on the choice of care types for older people with disability
It can be seen from Table 3 that family income, whether they own their housing and whether they enjoy retirement benefits have a likely significant impact on their choice of care types. The older people with disability with higher incomes are more likely to choose formal care. The older people with disability without their own housing are more likely to choose formal care, which is 5.4 times of those with real estate. This may be due to the influence of the traditional filial piety culture of “hate to leave a place where one has lived for a long time ” and “living and working in peace and contentment.” The older people with real estate prefer to receive informal care at home. The older people with pension benefits are more likely to receive formal care, which is 2.77 times of those without pension benefits. The number of sons has no significant effect on the choice of care type of older people with disability, indicating that the traditional concept of “raising male children for old age” is likely weakening in China.
The impact of community-based services on the choice of care types for older people with disability
It can be seen from Table 3 that “visiting doctors and delivering medicine,” “daily shopping service,” “organizing social and recreational activities,” “providing legal aid activities” and “providing health knowledge” provided by the community have no likely significant impact on the choice of care types for the older people with disability. The “living care service” “spiritual comfort” and “solving neighborhood disputes” provided by the community have a likely significant impact on the choice of care types for older people with disability. If the community provides “living care service” and “spiritual comfort service,” the older people with disability are more likely to choose formal care. In communities providing “neighborhood disputes” services, older people with disability are more likely to choose informal care.
Discussion and conclusions
Based on the latest 2018 CLHLS data, this article explores the factors that affect the choice of older people with disabilities between formal and informal care. At present, the main ways of caring for the older people in China are informal care based on family and formal care services provided by relying on social resources such as community and pension institutions (20). The study found that: (1) There are differences in the satisfaction degree of the older people with different characteristics. The accessibility of care resources is an important factor affecting the satisfaction of the older people. Family member care is usually the primary choice for the older people. (2) There is no significant correlation between the type of care and the degree of care satisfaction. Informal care has an alternative effect on formal care. (3) Male, rural, non-living alone, low-income, owing real estate, no pension older people tend to choose informal care; female, urban, living alone, high-income, pension, comprehensive community services for the older people tend to choose formal care.
Based on the above conclusion, this article argues that informal care can replace formal one, and that informal care itself is less costly and can reduce the burden on social pensions (59). Therefore, informal care should be encouraged by, giving cash subsidies, proper vacations and social endowment insurance to some caregivers to encourage them to continue to provide informal care (5). These measures could give formal support to informal care, thereby changing the private domain attributes of in-formal care at present. This is a disguised respect for the right to informal care services (60).
Informal care is still the main care model for older people with disability in China nowadays. The results of this study show that 85.48% of older people with disability choose informal care through the analysis of the sample, although the number of male children does not significantly affect the choice of care type for the older people. However, through the analysis of the sample, older people with disability in China now have an average of 2.8 sons, so they still have a broad and realistic basis for playing a role in family care service for older peoples. The choice of informal care for older people with disability may be due to the lack of necessary formal care services (61). However, from the perspective of economy, emotional needs and cultural inheritance, families are still important places for China's older people to provide for aging (18). Although the changes in social and economic development and family structure have weakened the function of family support for thousands of years, social pension services can not completely replace family support, family is the link to maintaining the emotional needs of the older people, and is also the first choice for the older people after their disability (62).
Traditional filial piety culture still has a strong influence in China. Thus, by encouraging the older people to return to the familiar community, with the help of various services and facilities provided by the community, the operation cost of public finance can be reduced and the emotional needs and spiritual dependence of the older people can be satisfied. Influenced by the Chinese culture of filial piety, increasing long-term care services for the older people at the community level and establishing a large number of community-based, fully functional embedded micro-aged care institutions should better meet the needs of the older people at different times and in different self-care situations, allowing them to enjoy continuous professional and personalized services in a familiar environment (63).
Finally, although family care can replace professional care, the long-term care of the older people must depend on the social pension service for older people with disability without children and widowed. In addition, some families will choose formal care because of various reasons (64). Therefore, it is necessary to further improve the long-term care system and to increase the input to formal care institutions. In addition, speeding up the full implementation of the long-term care insurance system can effectively reduce the cost of formal care and enable more older people to have the ability to choose professional care (65).
In the case of China, the traditional culture of filial piety regards long-term care for the older people as one of the main obligations of the family (52). However, as China faces the peak of its aging population, the increase in the number of only-child families since the implementation of family planning policies, the widespread employment of women and the diversification of family living patterns, it may be difficult to sustain a family approach to old age based on the traditional concept of filial piety (20). In this sense, the traditional concept of filial piety is also facing a possible transformation. Long-term care for older people has gradually evolved from a responsibility of traditional family to a practical social issue. What is the current state of demand for long-term care among older people in the context of China's aging population, and how to make the long-term care system work and develop in a healthy way, are questions that the article does not address but that may merit further research. At the same time, although this article analyzes the influencing factors of care types choice in the context of filial culture in China's mainland, it is lacked an analysis about the persistence and challenges to filial piety and care types choice of older people in Hong Kong, which is strongly influenced by the intersection of Chinese and Western cultures (66). In addition, this article is not able to analyze how the cultural meaning and social practice of filial care for aging parents have been transformed in Chinese immigrant families in the Western context (67).
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
The author confirms being the sole contributor of this work and has approved it for publication.
Funding
This work was supported by the Chinese Ministry of Education of Humanities and Social Science Project (Grant Number 19YJCZH235; PI: ZZ), the Borui Special Project of Soochow University on the Creation of a Strong Sense of the Chinese National Community (Grant Number 21BRRT002; PI: ZZ), and the Major Projects of China's Ministry of Education's Key Research Center for Humanities and Social Sciences (Grant Number 17JJD720007).
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Chappell N, Blandford A. Informal and formal care: exploring the complementarity. Ageing Soc. (1991) 11:299–317. doi: 10.1017/S0144686X00004189
2. Hickenbottom SL, Fendrick AM, Kutcher JS, Kabeto MU, Katz SJ, Langa KMA, et al. National study of the quantity and cost of informal caregiving for the elderly with stroke. Neurology. (2002) 58:1754–9. doi: 10.1212/WNL.58.12.1754
3. Bolin K, Lindgren B, Lundborg P. Informal and formal care among single-living elderly in Europe. Health Econ. (2008) 17:393–409. doi: 10.1002/hec.1275
4. Wimo A, Wimo A, Sjolund BM, Jönsson L, Skoldunger A, Winblad B, et al. Trends in informal care in Sweden: is it decreasing? Cross-sectional studies with the RUD instrument. Alzheimer and Dementia. (2009) 5:410. doi: 10.1016/j.jalz.2009.04.1001
5. Nordberg G, von Strauss E, Kåreholt I, Johansson L, Wimo A. The amount of informal and formal care among non-demented and demented elderly persons-results from a Swedish population-based study. Int J Geriatr Psychiatry. (2010) 20:862–71. doi: 10.1002/gps.1371
6. Rodríguez M. Use of informal and formal care among community dwelling dependent elderly in Spain. Eur J Public Health. (2014) 24:668–73. doi: 10.1093/eurpub/ckt088
7. Kiyak HA, Teri L, Borson S. Physical and functional health assessment in normal aging and in Alzheimer's disease: self-reports vs family reports. Gerontologist. (1994) 34:324–30. doi: 10.1093/geront/34.3.324
8. Bond MJ, Clark MS, Davies S. The quality of life of spouse dementia caregivers: changes associated with yielding to formal care and widowhood. Soc Sci Med. (2003) 57:2385–95. doi: 10.1016/S0277-9536(03)00133-3
9. Bravell ME, Berg S, Bo M. Health, functional capacity, formal care, and survival in the oldest old: a longitudinal study. Arch Gerontol Geriatr. (2008) 46:1–14. doi: 10.1016/j.archger.2007.02.003
10. Vossius C, Rongve A, Testad I, Wimo A, Aarsland D. The use and costs of formal care in newly diagnosed dementia: a three-year prospective follow-up study. Am J Geriatric Psychiatry. (2014) 22:381–8. doi: 10.1016/j.jagp.2012.08.014
11. Tsai CH, Lai TM. Predicting the need of formal care in Taiwan: analysis of a national random sample. Arch Gerontol Geriatr. (2011) 53:298–302. doi: 10.1016/j.archger.2010.12.003
12. Ku L, Liu LF, Wen MJ. Trends and determinants of informal and formal caregiving in the community for disabled elderly people in Taiwan. Arch Gerontol Geriatr. (2013) 56:370–6. doi: 10.1016/j.archger.2012.11.005
13. Research Team of Harmonious Community (2006). Analysis of the living condition of the aged and their demands for home-based care in the Chenghua District of Chengdu. J Chengdu Univ Technol (Social Sciences). (2006) 21–5. doi: 10.3969/j.issn.1672-0539.2006.04.006
14. De-Hui LI, Xiao-Lu LU, Wang L. SWOT analysis on internet + community family medical model-taking “care for life” project as an example. J Jiangxi Univ Trad Chin Med. (2017) 29:84–88.
15. Guo JP, Cui YJ, Yin Y. SWOT analysis of rural home care for the aged-taking Liuhe district of Nanjing as an example. Hubei Agric Sci. (2018) 57:168–72,76. doi: 10.14088/j.cnki.issn0439-8114.2018.23.038
17. Ham S, HongBaeg E. The relationship between formal care and informal care: focusing on home care service for elderly. Korean J Soc Welf. (2017) 69:203–25. doi: 10.20970/kasw.2017.69.4.008
18. Liu H. Formal and informal care: complementary or substitutes in care for elderly people? Empirical evidence from China. SAGE Open. (2021) 11:215824402110164. doi: 10.1177/21582440211016413
19. Li S, Jiang T, Song Z, Han Z. Economic impacts of policy adopted by china for its aging population. Singapore Econ Rev. (2020) 67:1517–43. doi: 10.1142/S0217590820500186
20. Liu M, Ma QP. Population Aging and Prospect of China's Elderly Care and Its Related Industries. (2021). Hershey, PA: IGI Global. doi: 10.4018/978-1-7998-4126-5.ch005
21. Jiang Y, Zhao T, Zheng H. Population aging and its effects on the gap of urban public health insurance in China. China Econ Rev. (2021) 68:101646. doi: 10.1016/j.chieco.2021.101646
22. Williams F. In and beyond new labour: towards a new political ethics of care. Critic Social Policy. (2001) 21:467–93. doi: 10.1177/026101830102100405
23. Norton EC. Long-term care. In Culyer AJ, Newhouse JP, editor. Handbook of Health Economics. New York, NY: North-Holland (2000).
24. Ward-Griffin C, Marshall VW. Reconceptualizing the relationship between “public” and “private” eldercare. J Aging Stud. (2003). doi: 10.1016/S0890-4065(03)00004-5
25. Viitanen TK. Informal and Formal Care in Europe. IZA Discussion Papers (2007). doi: 10.2139/ssrn.970484
26. Swinkels JC, Suanet B, Deeg DJ, van Groenou MIB. Trends in the informal and formal home-care use of older adults in the Netherlands between 1992 and 2012. Ageing Soc. (2016) 36:1870–90. doi: 10.1017/S0144686X1500077X
27. Kalwij A, Pasini G, Wu M. Home care for the elderly: the role of relatives, friends and neighbors. Rev Econ Househ. (2012) 12:379–404. doi: 10.1007/s11150-012-9159-4
28. McNamee P, Gregson BA, Buck D, Bamford CH, Bond J, Wright K, et al. Costs of formal care for frail older people in England: the resource implications of study. Soc Sci Med. (1999) 48:331–41. doi: 10.1016/S0277-9536(98)00351-7
29. Almberg B, Jansson W, Grafström M, Winblad B. Differences between and within genders in caregiving strain: a comparison between caregivers of demented and non-caregivers of non-demented elderly people. J Adv Nurs. (2010) 28:849–58. doi: 10.1046/j.1365-2648.1998.00711.x
30. Houser A, Gibson MJ, Redfoot DL. Trends in Family Caregiving and Paid Home Care for Older People with Disabilities in the Community: Data from the National Long-Term Care Survey. Washington, DC: Aarp Public Policy Institute (2010).
31. Langa KM, Chernew ME, Kabeto MU, Katz SJ. The explosion in paid home care in the 1990s: who received the additional services? Med Care. (2001) 2:147–57. doi: 10.1097/00005650-200102000-00005
32. Van Houtven CH, Norton C. Informal care and health care use of older adults. J Health Econ. (2004) 6:1159–80. doi: 10.1016/j.jhealeco.2004.04.008
33. Bonsang E. Does informal care from children to their elderly parents substitute for formal care in Europe. J Health Econ. (2009) 1:143–54. doi: 10.1016/j.jhealeco.2008.09.002
34. Li LW. Longitudinal changes in the amount of informal care among publicly paid home care recipients. Gerontologist. (2005) 4:465–73. doi: 10.1093/geront/45.4.465
35. Oliva-Moreno J, Peña-Longobardo LM, García-Mochón L, del Río Lozano M, Mosquera Metcalfe I, García-Calvente MDM, et al. The economic value of time of informal care and its determinants (the CUIDARSE study). PLoS ONE. (2019) 14:e0217016. doi: 10.1371/journal.pone.0217016
36. Mosca I, Van Der Wees PJ, Mot ES, Wammes JJ, Jeurissen PP. Sustainability of long-term care: puzzling tasks ahead for policy-makers. Int J Health Policy Manag. (2016) 6:195–205. doi: 10.15171/ijhpm.2016.109
37. Krol M, Papenburg J, Van Exel J. Does including informal care in economic evaluations matter? A systematic review of inclusion and impact of informal care in cost-effectiveness studies. Pharm Econ. (2015) 33:123–35. doi: 10.1007/s40273-014-0218-y
38. Zrubka Z. Measurement and health economic evaluation of informal care. Orv Hetil. (2017) 158:1363–72. doi: 10.1556/650.2017.30841
39. Rowen D, Dixon S, Hernández-Alava M, Mukuria C. Estimating informal care inputs associated with EQ-5D for use in economic evaluation. Eur J Health Econ. (2016) 17:733–44. doi: 10.1007/s10198-015-0718-5
40. Jansson WM, Grafström, Winblad B. Daughters and sons as caregivers for their demented and non-demented elderly parents. A part of a population-based study carried out in Sweden. Scand J Soc Med. (1997) 25:289. doi: 10.1177/140349489702500412
41. Swinkels JC, Tilburg TGV, Groenou MBV. Why do spouses provide personal care? A study among care-receiving Dutch community welling older adults. Health Soc Care Commun. (2021) 30:e953–61. doi: 10.1111/hsc.13497
42. Van den Berg B, Brouwer W, van Exel J, Koopmanschap M, van den Bos GA, Rutten F, et al. Economic valuation of informal care: lessons from the application of the opportunity costs and proxy good methods. Soc Sci Med. (2006) 62:835–45. doi: 10.1016/j.socscimed.2005.06.046
43. Abtan R, Rotondi NK, Macpherson A, Rotondi MA. The effect of informal caregiver support on utilization of acute health services among home care clients: a prospective observational study. BMC Health Serv Res. (2018) 18:1–7. doi: 10.1186/s12913-018-2880-9
44. Ross L, Neergaard MA, Petersen MA, Groenvold M. Measuring the quality of end-of-life care: development, testing, and cultural validation of the Danish version of views of informal carers' evaluation of services-short form. Palliat Med. (2018) 32:804–14. doi: 10.1177/0269216317740274
45. Hirschman KB, Hodgson NA. Evidence-based interventions for transitions in care for individuals living with dementia. Gerontologist. (2018) 58:129–40. doi: 10.1093/geront/gnx152
46. Sinn CLJ, Betini RSD, Wright J, Eckler L, Chang BW, Hogeveen S, et al. Adverse events in home care: identifying and responding with inter RAI scales and clinical assessment protocols. Can J Aging-Revue. (2018) 37:60–9. doi: 10.1017/S0714980817000538
47. Denewet N, Breucker D, Luce S, Kennes S, Higuet BS, Pepersack T. Comprehensive geriatric assessment and comorbidities predict survival in geriatric oncology. Acta Clin Belgica. (2016). 71:206–13. doi: 10.1080/17843286.2016.1153816
48. Lin WJ, Wang H, Zhou ZP. Care selection of older adults in china: informal or formal care-empirical study based on the data of CLHLS and CHARLS. J Shanghai Univ Fin Econ. (2014) 16:1–62.
49. Li Z. Determinants of living arrangements among the Chinese Elderly: new evidence from the CLHLS 2011 wave. Chin Stud. (2015) 4:32–43. doi: 10.4236/chnstd.2015.41006
50. Cheng X. Life Quality of elderly and living arrangements: empirical study based on CLHLS data. Social Secur Stud. (2016) 2016:31–7. doi: 10.3969/j.issn.1674-4802.2016.01.004
51. Lin W. The relationship between formal and informal care among Chinese older adults: based on the 2014 CLHLS dataset. BMC Health Serv Res. (2019) 19:1–8. doi: 10.1186/s12913-019-4160-8
52. Yu TD, Dimond MF. Filial piety. J Gerontol Nurs. (1998) 24:13–8. doi: 10.3928/0098-9134-19980301-05
54. Cheng ST, Chan AC. Filial piety and psychological well-being in well older Chinese. J Gerontol B Psychol Sci Soc Sci. (2006) 61:P262–9. doi: 10.1093/geronb/61.5.P262
55. Sung K-t. Measures and dimensions of filial piety in Korea. Gerontologist. (1995) 35:240–7. doi: 10.1093/geront/35.2.240
56. Press Conference on Key Data Results of the Seventh National Population Census. Available online at: http://www.stats.gov.cn/ztjc/zdtjgz/zgrkpc/dqcrkpc/ggl/202105/t20210519_1817702.html (accessed August 2, 2022).
57. Seventh National Population Census Bulletin (No. 4). Available online at: http://www.stats.gov.cn/ztjc/zdtjgz/zgrkpc/dqcrkpc/ggl/202105/t20210519_1817697.html (accessed August 2, 2022).
58. Seventh National Population Census Bulletin (No. 5). Available online at: http://www.stats.gov.cn/ztjc/zdtjgz/zgrkpc/dqcrkpc/ggl/202105/t20210519_1817698.html (accessed August 2, 2022).
59. Verbakel E, Metzelthin SF, Kempen G. Caregiving to older adults: determinants of informal caregivers' subjective well-being and formal and informal support as alleviating conditions. J Gerontol B Psychol Soc. (2016) 2016:gbw047. doi: 10.1093/geronb/gbw047
60. Pfau-feeinger B, Geissler B. Care and Social Integration in European Societies. 4th ed. Polity Press: Cambridge (2005). doi: 10.46692/9781847421340
61. Holly A, Lufkin TA, Norton EC, Van Houtven C. Informal Care And Medical Care Utilization in Europe and the United States. Rochester: Social Science Electronic Publishing (2007).
62. Hazif-Thomas C, Tritschler-LeMa MH, Thomas P. Family caregivers of demented elderly people and access to medical care: who gets worn out, why and what for? Open J Psychiatry. (2013) 3:251–5. doi: 10.4236/ojpsych.2013.32023
63. Mundt J, Lusch RF. Informal and formal care for the elderly: decision determinants and their implications. Health Marketing Q. (1997) 14:53. doi: 10.1300/J026v14n03_05
64. Hopp FP. Patterns and predictors of formal and informal care among elderly persons living in board and care homes. Gerontologist. (1999) 39:167–76. doi: 10.1093/geront/39.2.167
65. Litwin H, Attias-Donfut C. The inter-relationship between formal and informal care: a study in France and Israel. Ageing Soc. (2009) 29:71–91. doi: 10.1017/S0144686X08007666
66. Ng ACY, Phillips DR, Lee WKM. Persistence and challenges to filial piety and informal support of older persons in a modern Chinese society: a case study in Tuen Mu, Hong Kong. J Aging Stud. (2002) 16:132–53. doi: 10.1016/S0890-4065(02)00040-3
Keywords: quality of care, older people with disability, informal care, formal care, aging, long-term care, influencing factor
Citation: Zang Z (2022) The care types choice in filial culture: A cross-sectional study of disabled elderly in China. Front. Public Health 10:954035. doi: 10.3389/fpubh.2022.954035
Received: 26 May 2022; Accepted: 02 August 2022;
Published: 06 September 2022.
Edited by:
Miodraga Stefanovska-Petkovska, Universidade de Lisboa, PortugalReviewed by:
Sarvarubini Nainee, Tunku Abdul Rahman University, MalaysiaMack Shelley, Iowa State University, United States
Copyright © 2022 Zang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zheng Zang, emFuZ3poZW5nQHN1ZGEuZWR1LmNu
†ORCID: Zheng Zang orcid.org/0000-0001-5662-0741