 Michel Sabe1*†
Michel Sabe1*† Chaomei Chen2†
Chaomei Chen2† Othman Sentissi1
Othman Sentissi1 Jeroen Deenik3,4
Jeroen Deenik3,4 Davy Vancampfort5,6
Davy Vancampfort5,6 Joseph Firth7,8
Joseph Firth7,8 Lee Smith9
Lee Smith9 Brendon Stubbs10,11
Brendon Stubbs10,11 Simon Rosenbaum12,13
Simon Rosenbaum12,13 Felipe Barreto Schuch14
Felipe Barreto Schuch14 Marco Solmi15,16,17,18
Marco Solmi15,16,17,18- 1Division of Adult Psychiatry, Department of Psychiatry, University Hospitals of Geneva, Thonex, Switzerland
- 2College of Computing and Informatics, Drexel University, Philadelphia, PA, United States
- 3Scientific Research Department, GGz Centraal, Amersfoort, Netherlands
- 4School for Mental Health and Neuroscience, Maastricht University, Maastricht, Netherlands
- 5Katholieke Universiteit Leuven Department of Rehabilitation Sciences, Leuven, Belgium
- 6University Psychiatric Center Katholieke Universiteit Leuven, Leuven, Belgium
- 7Division of Psychology and Mental Health, Manchester Academic Health Science Centre, University of Manchester, Manchester, United Kingdom
- 8Greater Manchester Mental Health National Health Service Foundation Trust, Manchester Academic Health Science Centre, Manchester, United Kingdom
- 9Centre for Health, Performance and Wellbeing, Anglia Ruskin University, Cambridge, United Kingdom
- 10Physiotherapy Department, South London and Maudsley National Health Service Foundation Trust, London, United Kingdom
- 11Department of Psychological Medicine, Institute of Psychiatry, Psychology and Neuroscience, King's College London, London, United Kingdom
- 12Discipline of Psychiatry and Mental Health, Medicine and Health, University of New South Wales, Kensington, NSW, Australia
- 13School of Health Sciences, Medicine and Health, University of New South Wales, Kensington, NSW, Australia
- 14Department of Sports Methods and Techniques, Federal University of Santa Maria, Santa Maria, Brazil
- 15Department of Psychiatry, University of Ottawa, Ottawa, ON, Canada
- 16Department of Mental Health, The Ottawa Hospital, Ottawa, ON, Canada
- 17Ottawa Hospital Research Institute, Clinical Epidemiology Program, University of Ottawa, Ottawa, ON, Canada
- 18Department of Child and Adolescent Psychiatry, Charité Universitätsmedizin, Berlin, Germany
The sheer volume of research publications on physical activity, mental health, and wellbeing is overwhelming. The aim of this study was to perform a broad-ranging scientometric analysis to evaluate key themes and trends over the past decades, informing future lines of research. We searched the Web of Science Core Collection from inception until December 7, 2021, using the appropriate search terms such as “physical activity” or “mental health,” with no limitation of language or time. Eligible studies were articles, reviews, editorial material, and proceeding papers. We retrieved 55,353 documents published between 1905 and 2021. The annual scientific production is exponential with a mean annual growth rate of 6.8% since 1989. The 1988–2021 co-cited reference network identified 50 distinct clusters that presented significant modularity and silhouette scores indicating highly credible clusters (Q = 0.848, S = 0.939). This network identified 6 major research trends on physical activity, namely cardiovascular diseases, somatic disorders, cognitive decline/dementia, mental illness, athletes' performance, related health issues, and eating disorders, and the COVID-19 pandemic. A focus on the latest research trends found that greenness/urbanicity (2014), concussion/chronic traumatic encephalopathy (2015), and COVID-19 (2019) were the most active clusters of research. The USA research network was the most central, and the Chinese research network, although important in size, was relatively isolated. Our results strengthen and expand the central role of physical activity in public health, calling for the systematic involvement of physical activity professionals as stakeholders in public health decision-making process.
Introduction
Physical activity can be considered as medicine and has been used in both the treatment and prevention of a variety of chronic conditions (1). Longitudinal cohort studies demonstrate that a low cardiorespiratory fitness constitutes the largest attributable fraction for all-cause mortality (2). There is also overwhelming evidence that low physical activity (i.e., not meeting physical activity recommendations) is considered as an important risk factor for chronic conditions including some cancers, cardiovascular disease, diabetes, dementia, and in particular for a patient with mental illness (schizophrenia, bipolar disorder, or major depressive disorder) (3–5). Patients with mental illness have poor physical health compared with the general population, with reduced life expectancy and a higher risk of premature death beyond suicide, from natural causes (6). At least partially, among other factors, their poor physical health is due to higher sedentary behavior and lower physical activity compared with the general population (7, 8). Physical activity, and its structured form of exercise, seem to affect the brain and mind, beyond physical health, both as a factor associated with poor mental health and quality of life and as a treatment for mental disorders (9). Indeed, exercise has shown to be efficacious in a number of mental disorders, according to a previous umbrella review pooling 27 systematic reviews (10, 11). Exercise is also now seen as a potential preventive or disease-modifying treatment of dementia and brain aging (12) or as a possible treatment for negative symptoms in schizophrenia (13).
Importantly, systematic reviews, meta-analysis, and umbrella reviews have offered a deep synthesis of specific research questions addressed within the exponential volume of physical activity literature related to mental health and wellbeing. However, such systematic methods may not be appropriate to encompass hundreds or thousands of new publications per year. In fact, systematic reviews have to be narrow in their inclusion criteria and offer a comprehensive view on a specific and restricted research or clinical question. For instance, a meta-analysis can inform if an intervention is efficacious for a given population on an outcome of interest (14, 15) or an umbrella review can assess the credibility of an association between a risk factor and an incident condition (16–19). Nevertheless, none of the two offers an insight on the temporal trend of research, the complex network of topics, authors, publications, networks, institutions, and their bibliometric performance. Gaining such overarching views of how an entire field of research on a particular topic is important and useful, in order to gauge how the academic literature is developing and inform the next steps for the science to pursue.
The integration of developments in data visualization, text mining, and network analysis has permitted the emergence of a new framework and a new generation of research synthesis of both evidence and influence, named research weaving (20). This framework combines visual analytics and scientometrics to visualize and delineate the development of a field, its underlying intellectual structure and the dynamics of scholarly communication over time (21). A comprehensive delineation of how scientometrics and bibliometrics overlap and distinct can be found in Hood and Wilson 2001 paper (22).
To the best of our knowledge, no broad-ranging scientometric study of research trends and influence networks of physical activity, mental health and wellbeing has yet been conducted. Thus, in this article, we present one to bridge the gap.
Materials and methods
Search strategy and data collection
We searched the Web of Science Core Collection (WOSCC) on December 7, 2021, using a combination of keywords and Medical Subject Headings such as “physical activity,” “mental health,” and “mental illness*.” WOSCC provides full references and complete citations of articles published in major journals since 1900 and is one of the largest comprehensive sources for bibliometric studies (23). The full protocol with the search key is available on osf.io. This current study protocol is based on a first large-scale scientometric analysis (24). The database source was limited to the Web of Science Citation Index Expanded. The document types are limited to “article,” “review,” “editorial material,” and “proceeding papers,” without restrictions on language or time. The dataset was extracted from the WOSCC in tag-delimited plain text files.
In order to assess the quality of the reference filtering process and the homogeneity of the dataset, we independently inspected each of the most cited references (604 articles in total), and a randomly selected sample of 10% of included articles to allow a margin of error (i.e., inclusion of non-relevant papers) of 5% with a 95% confidence interval (Supplementary Table 1; Figure 1).
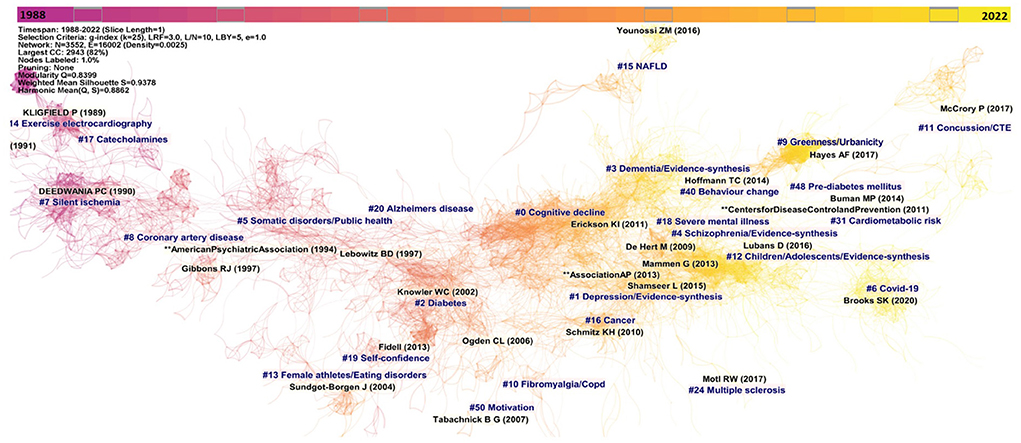
Figure 1. Co-citation reference network with cluster visualization (1988–2021). The unit of measure are articles and constitutes nodes. Nodes are organized according to year of publication. The size of a node (article) is proportional to the number of times the node has been co-cited. Colored shades indicate the passage of the time, from past (purplish) to the present time (yellowish).
Objectives
The primary outcome was to visualize research trends on physical activity related to mental health and wellbeing and to characterize the evolution of research trends using networks of co-cited references and networks of co-occurring keywords assigned to relevant publications.
The secondary outcome was to provide clinicians, researchers, and policymakers with a specific unit of measure of the research network (countries, institutions, authors, and journals) and to identify emerging trends and limitations.
Data analysis
Two different software tools for constructing bibliometric networks were used: Bibliometrix R package (3.1.4) (25) and CiteSpace (version 5.8.R4) (21). Bibliometric outcomes included citation counts, co-citations, and co-occurrences. A co-citation count is defined as the frequency with which two published articles are cited together by subsequently published articles (26). Co-occurrence networks are based on how frequently two entities, such as keywords, appear in the same articles.
The Bibliometrix R package was used for the analysis of publication outputs and the trend of growth. CiteSpace was used for the study of several types of networks, namely, networks of co-cited references, networks of co-cited authors, and co-occurrence networks of authors, keywords, institutions, and countries. For instance, the co-cited (authors') institutions network accounts for the cooperation between two or more institutions, which reflects the cooperation between authors and the influence networks.
CiteSpace produces a variety of metrics of significance, with temporal metrics such as citation burstness, structural metrics such as betweenness centrality, modularity, and silhouette score as well as a combination of both, namely, the sigma metric. The betweenness centrality of a node measures the fraction of shortest paths in an underlying network passing through the node (27). The burstness of the frequency of an entity over time indicates a specific duration of a surge of the frequency (28). The sigma indicator combines structural and temporal properties of a node, namely, its betweenness centrality and citation burst (29). Modularity (the Q score) measures the quality of dividing a network into clusters, and the silhouette score (the S score) of a cluster measures the quality of a clustering configuration (30). The Q score ranges from 0 to +1. The cluster structure is considered significant with a Q score >0.3, and higher values indicate a well-structured network. The S score ranges from −1 to +1. If the S score is >0.3, 0.5, or 0.7, the network is considered homogenous, reasonable, or highly credible, respectively. In addition, we conducted a structural variation analysis that focuses on novel boundary-spanning connections to detect transformative papers ranked on their divergence modularity (31). These transformative papers can potentially change to the existing structure of knowledge.
We extracted cluster labels from keywords associated with articles that are responsible for the formation of a cluster selected by the likelihood ratio test (p < 0.001). Each cluster was closely inspected, and eventually cluster labels were improved based on the authors' judgment.
The second level of the data filtering process was applied during the generation of networks within each dataset (e.g., most cited reference) in order to detect duplicates, references without authors, or any non-relevant unit of measure that was excluded (e.g., DSM reference; CIM-10) or merged (e.g., author Motl RW and Motl W Robert).
The g-index was used for all calculations. This index permits to give credit to lowly cited or non-cited papers while giving credit for highly cited papers, thus partially alleviating bias from highly cited papers as seen with the h-index (32). CiteSpace general parameters are reported in Supplementary Information 1.
Results
Analysis of publication outputs, major journals, and growth trend prediction
We report a flowchart with detail of the 56,442 retrieved documents from the WOS Science citation index expanded and the different steps of our scientometric study: identification and screening of studies, software analyses, and expert review's interpretation (Supplementary Figure 1).
Among the retrieved documents, 1,089 documents were excluded, and 55,353 documents encompassing 1,306,828 references were retained (47,105 articles; 6,671 reviews; 564 editorial material; 1,013 proceeding papers). The data filtering process consisted of the inspection of each 604 highly cited papers, editorial material, and proceeding papers and the inspection of 10% randomly selected titles of the retrieved documents. Only 4% (n = 224 articles) were not relevant (Supplementary Figure 1).
The retained 55,353 articles were published between 1905 and May 2022 in 24 different languages (95.1% of articles in English). The annual scientific production is still in 2022 exponential with a mean annual growth rate of 6.8% since 1989 (n = 17) and 2022 (n = 5,604) (Supplementary Figures 2, 3).
The first article identified was a Franz SI and Hamilton GV article on “the effects of exercise upon the retardation in conditions of depression” published in the American Journal of Insanity (33).
Analysis of co-citation reference: Clusters of research and most cited papers
Clusters of research
We constructed a synthesized network of co-cited references based on articles published during the 1988–2021 time period as suggested by CiteSpace after the removal of empty time intervals to optimize time slicing (Figure 1). In this network, each node represents a highly co-cited article. We further explored the latest research trends with the extraction of co-citation networks for the 2016-(May) 2022 time period, and the monthly time sliced networks for the year of 2021 (Supplementary Figure 4). All three networks presented significant modularity and silhouette scores indicating highly credible clusters (Q = 0.8481, S = 0.9394; Q = 0.7712, S = 0.9445; and Q = 0.4854, S = 0.8376, respectively).
The 1988–2021 network identified 50 different clusters, with a single constellation of 26 clusters that reveals six distinct major trends of research on physical activity, namely cardiovascular disease, somatic disorders, cognitive decline/dementia, mental illness, athletes' performance, related health issues and eating disorders and COVID-19 pandemic.
The earliest research trend identified concerns physical activity and cardiovascular diseases consisting of four distinct clusters during the years 1991 to 1997 as follows, with clusters number (clusters' size decreased from cluster number #0), label, silhouette score, size, pooled mean year of publication, the most representative reference; #14, “exercise electrocardiography” (S = 0.987; 65; 1987) (34), #7 “silent ischemia” (S = 0.964; 145; 1989) (35), #17 “catecholamine” (S = 0.987; 46; 1989) (36), and #8 “coronary artery disease” (S = 0.962; 141; 1994) (37). This research trend then vanished until it recently reappeared in the 2016–2021 network with cluster #14 “cardio-metabolic health markers” (S = 0.991; 6; 2014) (38), #31 “cardiometabolic risk” (S = 0.999; 5; 2014) (39), and continues to evolve, as shown in the 2021 network with cluster #9 “cardiovascular disease” (S = 0.998; 4; 2016) (40).
The second major trend of research emerged in 1995 on “somatic disorders/public health,” cluster #5 (S = 0.953; 238; 1995) (41) that directly evolved into cluster #2 “diabetes” (S = 0.918; 289; 2001) (42) and further develop into a relatively isolated cluster #10 “fibromyalgia/copd” (S = 0.981; 97; 2005) (43), compared to a succession of other clusters on somatic disorders #16 “cancer” (S = 0.993; 52; 2009) (44), #15 “NAFLD” (S = 0.998; 55; 2011) (45), #48 “pre-diabetes” (S = 0.994; 4; 2012) (46) and #24 “multiple sclerosis” (S = 0.999; 9; 2014) (47).
The third major trend concerned cognitive decline and dementia and started in 1997 with a small cluster #20 “Alzheimer's disease” (S = 0.993; 16; 1997) (48), then evolved in a much larger cluster #3 “dementia” (S = 0.916; 269; 2014) (49), and the largest cluster of the network, cluster #0 “cognitive decline” (S = 0.923; 324; 2006) (50). This cluster continues as the most prominent cluster of the 2016–2021 network #0 “evidence-synthesis/cognitive decline” (S = 0.938; 221; 2015) (51) and also extended to a cluster on frailty, #9 “frailty” (S = 0.991; 15; 2014) (52).
The fourth major trend on research concerned mental illness. This trend started in 2007 with a small cluster #18 “severe mental illness” (S = 0.985; 46; 2007) (53), and rapidly evolved in two major clusters, #1 “depression” (S = 0.823; 292; 2009) (42), and #4 “schizophrenia” (S = 0.912; 267; 2015) (54). The 2016-2021 network confirmed the importance of this major trend with #2 “evidence-synthesis/depression” (S = 0.819; 142; 2016) (55). This trend now mainly focus on evidence-synthesis and became #12 “children/adolescents/evidence-synthesis” (S = 0.963; 75; 2016) (56).
The fifth trend concerns physical activity, athlete's performance, related health issues, and eating disorders with a succession of small and isolated clusters: #19 “self-confidence” (S = 0.995; 38; 1998) (57), #13 “female athletes/eating disorders” (S = 0.967; 74; 2000) (58), #50 “motivation” (S = 0.997; 4; 2005) (59), and #11 “concussion/chronic traumatic encephalopathy” (S0 = 0.996; 11; 2014) (60). A focus on the 2021 network reveals the latest cluster of the trend, #7 “elite athletes” (S = 0.986; 75; 2017) (61).
The sixth and last trend concerned COVID-19 pandemic and starts with cluster #6 “COVID-19' (S = 0.968; 26; 2019) (62), that continues to evolve in the 2016–2021 network with #1 “COVID-19” (S = 0.987; 172; 2019) (63), #20 “post-COVID-19/long COVID” (S = 1; 4; 2019) (64) and became in 2021 the most important cluster with #0 “COVID” (S = 0.818; 147; 2019) (63), and #4 “COVID/children” (S = 0.837; 59; 2019) (65).
Finally, two recent isolated clusters that we cannot relate to a specific trend have also emerged: cluster #9 “greenness/urbanicity” (S = 0.998; 2015) (66), and #40 “behavior change” (S = 0.996; 7; 2013) (67).
The link walkthrough over time between clusters based on burstness dynamics for the 1988–2021 network is available as a video on osf.io.
Most cited papers
We report the top 10 most co-cited references for the 1988–2021 time period in Table 1. The top three most co-cited articles in our network were the Schuch et al.'s meta-analysis on exercise as a treatment of depression (55), followed by the Erickson et al.'s randomized-controlled trial (RCT) on exercise increasing the size of the anterior hippocampus in older adults (50), and the Ngandu et al.'s RCT on the multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring vs. control to prevent cognitive decline in at-risk elderly people (54).
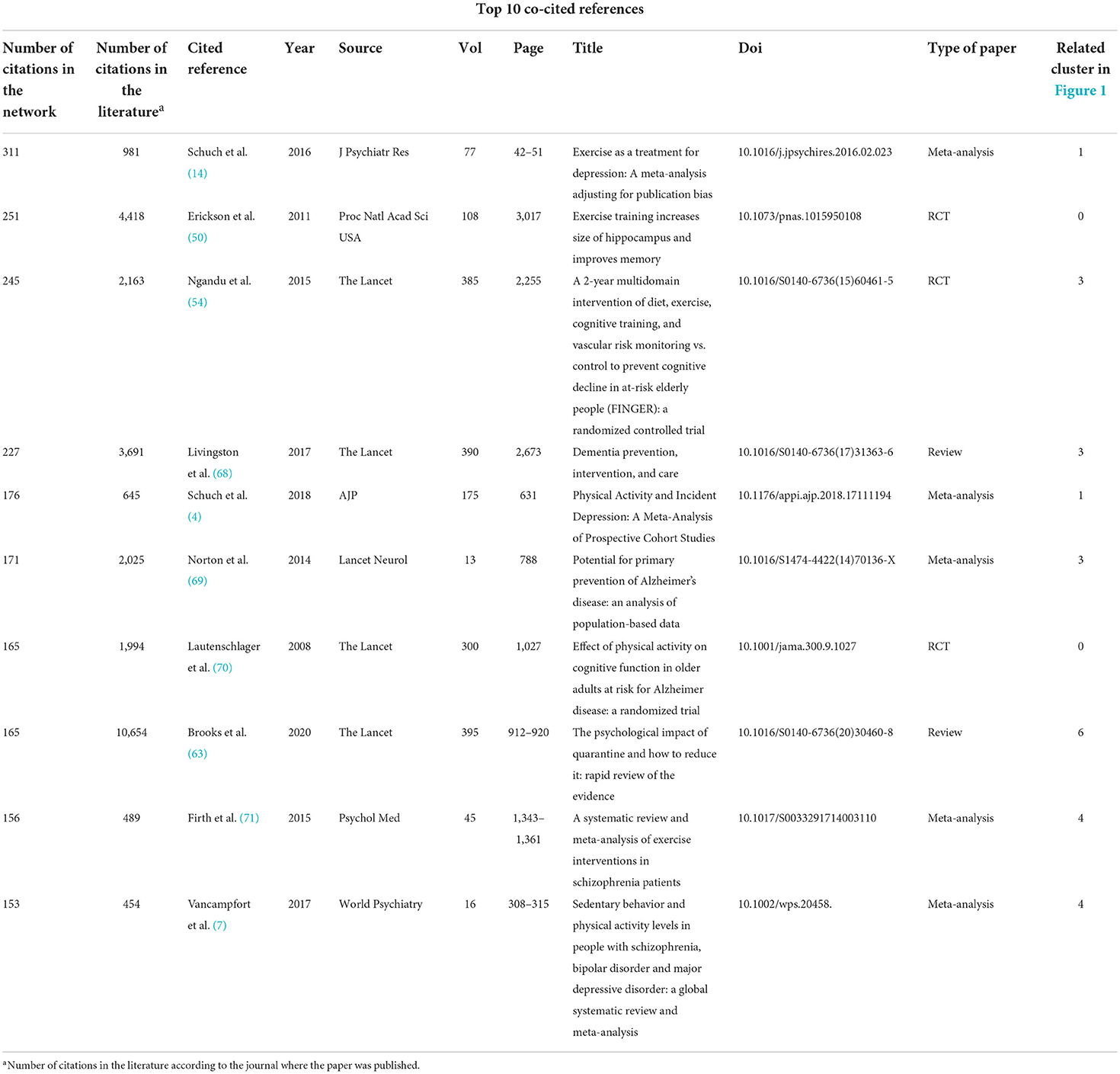
Table 1. The top 10 most cited journals and reference.
Moreover, we produced the analysis of burstness for the top references of the 1988–2021, 2016–2021, and 2021 time periods (Supplementary Tables 2P–R). The analysis of burstness revealed that the top three references with the latest and strongest beginning of citation burst were the Warburton and Bredin paper on health benefits of physical activity (72), the Brooks et al. paper on the psychological impact of quarantine (63), and the Stubbs et al. EPA guidance on physical activity as a treatment for severe mental illness (11).
Another important aspect of scientometric studies is the detection of potentially transformative papers, by conducting a structural variation analysis for the 2016–2021 and the 2021–2021 time period (Supplementary Table 3). For the 2016–2021 time period, the top three identified articles based on the strongest centrality divergence were the Stubbs et al. study on factors influencing physical activity among 204,186 people across 46 low-and middle-income countries (73), Vancampfort et al.'s meta-analysis on sedentary behavior and physical activity levels in people with severe mental illness (7), and Vancampfort et al.'s review on physical activity and metabolic disease among people with severe mental illness (74). For the time period January 2021 to May 2021, the top three studies were the Aguilar et al.'s study on the association between leisure-time exercise and depressive symptoms (75), the Schuch et al.'s study on the ELSA-Brasil cohort concerning the association between leisure-time, transport, depression and anxiety symptoms (76), and the van Sluijs et al.'s review on physical activity behaviors during adolescence (77).
Analysis of co-occurrence of keywords
The use of author keywords can help identify the latest trends of research and choose search keywords for future reviews. The co-occurrence author keywords network for 1988–2021 is shown in Supplementary Figure 5, and the 2016–2021 time period is shown in Figure 2. In this network, each node is a highly co-occurring keyword. Both networks presented significant modularity and silhouette scores indicating credible clusters (Q = 0.3327, S = 0.6823 and Q = 0.3971, S = 0.6614 respectively).
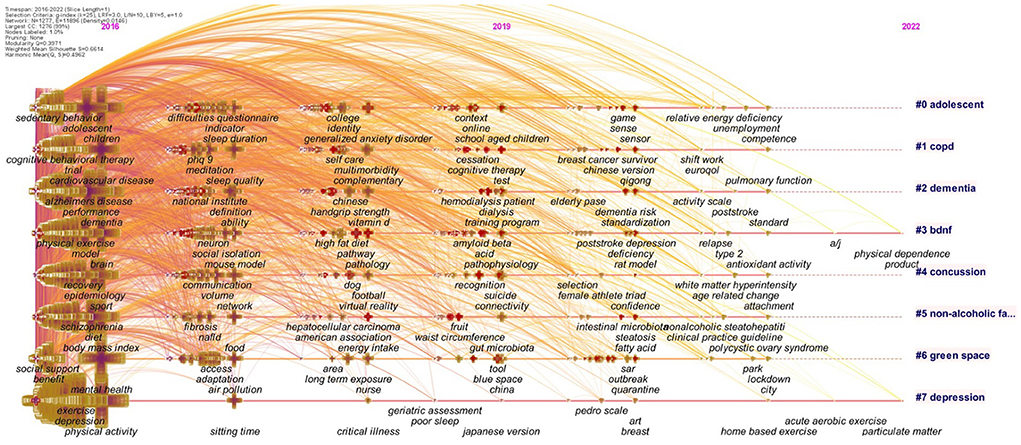
Figure 2. Co-occurrence authors' keyword network (2016–2021). In this co-occurrence author's keywords analysis, the size of the cross is proportional to the frequency of keyword occurrence.
The 1988–2021 network presented six different clusters: #0 “mental health”; #1 “hippocampus”; #2 “quality of life”; #3 “coronary artery disease”; #4 “obesity,” and #5 “dementia,” and the 2016–2021 network presented seven different clusters: #0 “adolescent”; #1 “copd”; #2 “dementia”; #3 “bdnf”; #4 “concussion”; #5 “non-alcoholic fatty liver disease”; #6 “green space” and #7 “depression”.
The burstness analysis extracted the top 30 co-cited keywords; the latest and strongest beginning of citation bursts for the 1988–2021 network were “quality of life,” “major depression,” “controlled trial,” “meta-analysis,” and “sedentary behavior,” and for the 2016–2021 network were “psychological impact,” “acute respiratory syndrome,” “rat model,” “epidemic,” and “deficiency” (Supplementary Tables 3S–V).
Analysis of influence and co-operation network
Co-cited countries and co-cited institutions network
We produced the co-cited countries and co-cited institutions network (Figures 3A,B). Units of measures were authors' countries and authors' institutions. A significant modularity and silhouette score were found (Q = 0.5321; S = 0.785).
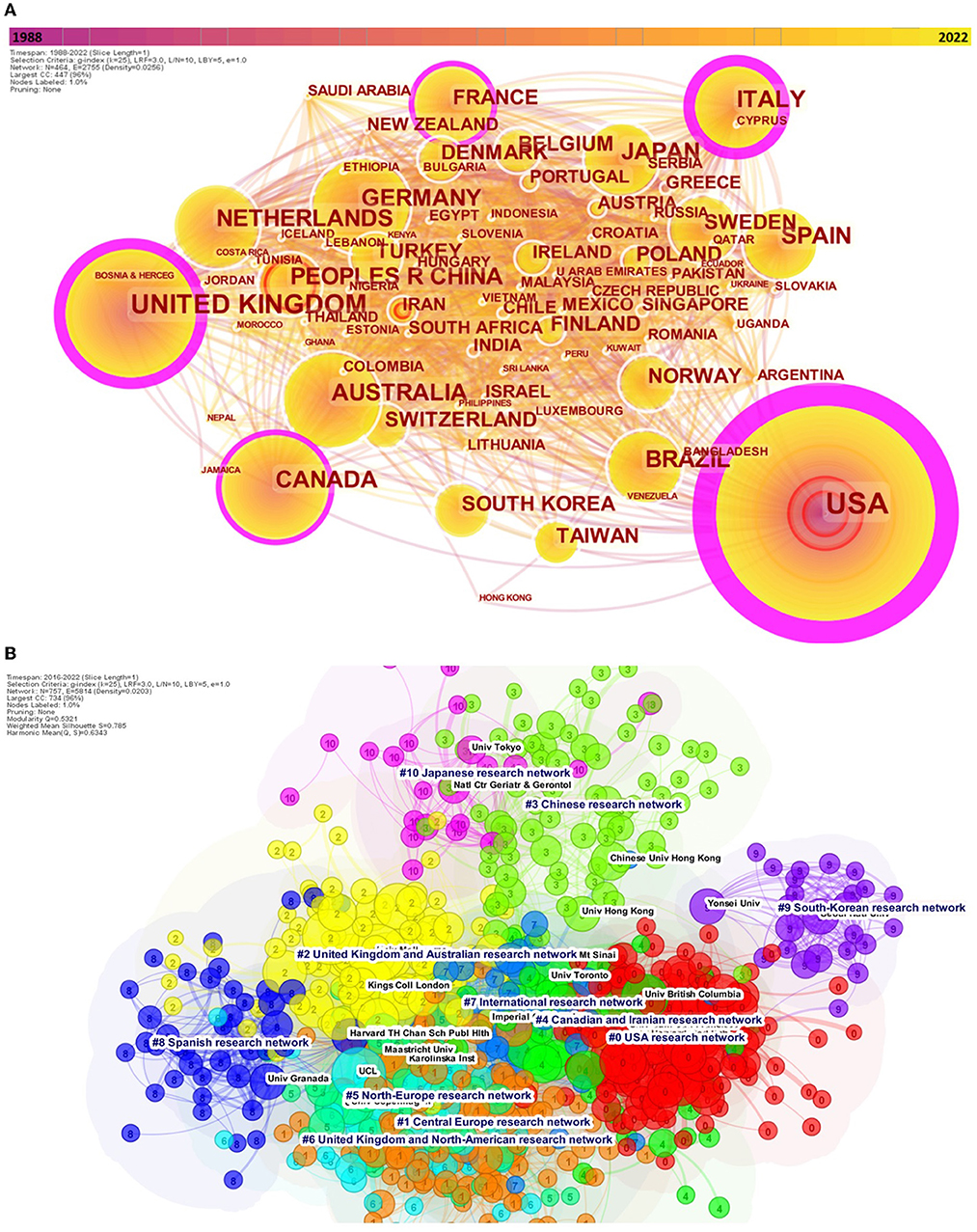
Figure 3. Co-cited author's countries (A) (1988–2021) and co-cited author's institutions network with corresponding clusters (B) (2016–2021). Both the co-cited author's countries and co-cited author's institutions permits to reveal the collaborative country network. Betweenness centrality organize the network, with the countries presenting the most important centrality being at the center of the network. Nodes are according to each network, countries or institutions. The outermost purple ring denotes the centrality level, and highly central nodes are considered pivotal points in the research field. We limited the nodes to the 80 first countries.
Overall, 176 different countries were identified. In the 1988–2021 network, the country with the most important number of author's citation were the United States of America (USA) (n = 17,988), followed by the United Kingdom (n = 5,720) Australia (n = 4,431), Canada (n = 3,773), and People's Republic of China (n = 3,160). Similarly, in the 2016–2021 network, the most cited top countries were identical; however, China was now in fourth place (Supplementary Figure 6; Supplementary Table 4). The analysis of burstness reveals confirmed that China was from far the country with the most important strength of burst these last 2 years (231.72), whereas the USA latest important burst date to the 1998–2003 period (83.54) (Supplementary Tables 2A,B). The co-cited author's institutions network reveals what institutions are the most cited. We produced the last five-year network (2016–2021) and identified 757 different organizations (Figure 3B, Supplementary Figure 7).
The most central network was the USA research network #0, with the greatest betweenness centrality to other clusters, such as the Central Europe research network #1, or the United Kingdom and Australian research network #2. The Chinese research network #3, although important in size, was relatively isolated, sharing few links with the Japanese research network #10, whereas the Spanish #8 and the South Korean #9 network were more isolated (Supplementary Table 4). The burstness analysis revealed that the five institutions with the latest and strongest strength of citation burst were as follows: Central South University (China), University of Extremadura (Spain), Federal University of Santa Maria (Brazil), University of Paris (France), and University of Lisbon (Portugal) (Supplementary Tables 2C,D). The sigma score revealed that the institutions with the greatest scores were Charité (#1; 2016), Medical University of Vienna (#1; 2017), and Peking University (#3; 2016).
Co-authorship, co-cited and co-cited journals network
Our dataset includes 1,306,827 citations with an average of 31.85 citations per document. About 175,508 different authors were found, with an average of 3.17 authors and 5.76 co-authors per document in 4,193 different sources (e.g., books and journals) (Supplementary Figure 1).
We produced the co-authorship networks, which are the social networks encompassing researchers that reflect collaboration among them, each node representing a different highly cited co-author (Supplementary Figure 8, Supplementary Table 4). The network revealed that French researchers are closely collaborating within France and on physical exercise and aging/depression (#9; 2018). The burstness analysis revealed that the co-authors that were the most participating in articles these last years were Stubbs B, Smith L, De Hert M, Vancampfort D and Probst M (Supplementary Tables 2G,H). We further produce the co-cited author network that permits to visualize “who cites who” for the last 5 years (2016–2021 network) was also conducted (Supplementary Figure 9). The burstness analysis revealed that the most co-cited first authors according to our datasets were Brooks SK, Wang CY, Ogden CL, Holmes EA, and Kandola SA. Furthermore, the latest top cited authors (as first authors) with the most important strength of burst were Brooks SK, Schuch FB, Wang CY, Firth J, and Stubbs B (Supplementary Tables 3I,J).
The top five journals with the most documents were as follows: the International Journal of Environmental Research and Public Health (n = 1,164) in first place with a massive raise of documents these last 3 years; PLOS ONE (n = 1,017); BMC Public Health (n = 625); BMJ OPEN (n = 513) and the Journal of Affective Disorders (n = 453) (Supplementary Figure 10). We conducted the co-cited journal network that retained 2,879 journals and showed the highly cited journals with high betweenness centrality (Supplementary Figure 11).
The top five highly cited journals were Archives of General Psychiatry (JAMA), The Lancet, PLOS ONE, Medicine and Science in Sports and Exercise, and the New England Journal of Medicine (Table 2). The burstness analysis further reveals that five journals with the latest beginning of burst were Frontiers in Psychology, The Lancet Psychiatry, International Journal of Environmental Research and Public Health, Nutrients, and Frontiers in Psychiatry (Supplementary Tables 2E,F).
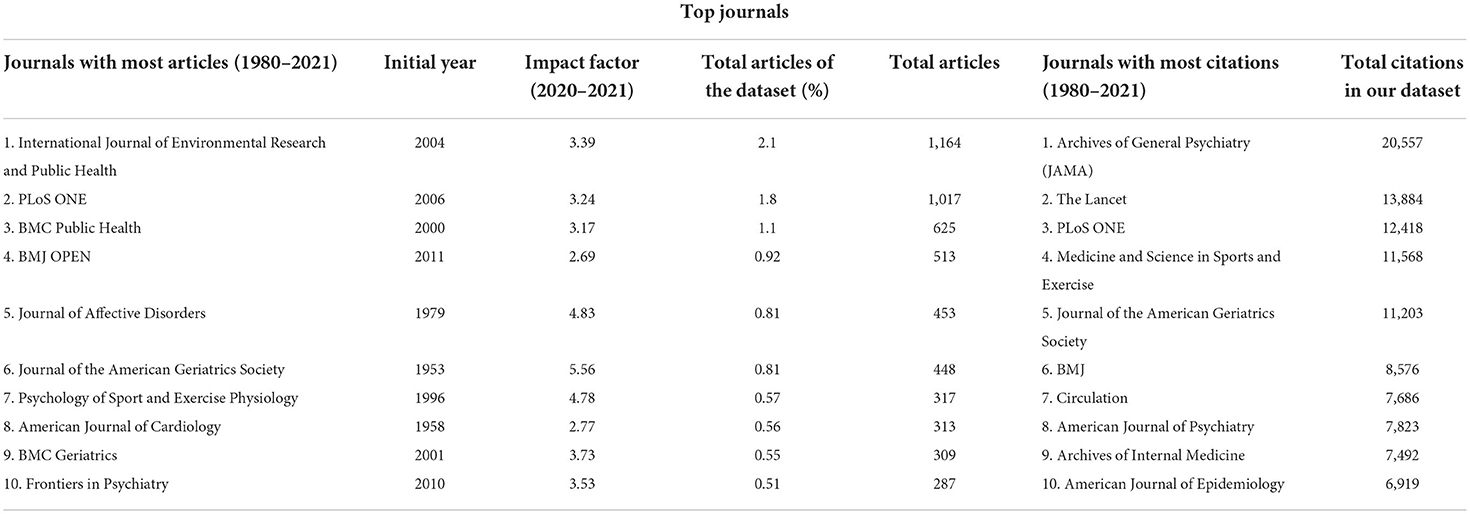
Table 2. Journals with most articles and citations.
Discussion
Summary of the main findings
To the best of our knowledge, this is the first broad scientometric that proposes a comprehensive overview of the development of research on physical activity, mental health, and wellbeing.
We retained 55,353 documents revealing an exponential growth of scientific production since the 90s. The USA holds for decades the leading position in research; however, China is very active since 2020 with an important burst of citations, mainly due to publication on COVID-19. The King's College London and Harvard University were the most influential institutions in terms of citation count. In supplement to actual reviews, this scientometric study reveals the influence and collaboration network, which could help researchers to identify major scholarly communities and establish potential research collaboration.
Identification of research trends
The six distinct major trends of research identified expose the history and the latest development of research on physical activity, mental health, and wellbeing. The first major trend of research concerns physical activity and cardiovascular disease, reminding the past and present intertwine. First research focused on cardiovascular disease (35). The large body of research on evidence synthesis of the last decades that mainly focused on the prevention to treatment role of physical activity for cardiovascular disease started with guidelines for exercise testing (37, 78), and that continues to date with consideration of cardiometabolic risk factors (39).
The extension of prevention and treatment of physical activity to other somatic disorders constituted the second major trend, making levels of physical activity a public health priority (41), that continues to date (79). Another trend, which emerged after 2000, is the potential of physical activity for the prevention and treatment of dementia with increased importance of evidence-synthesis studies (51, 80, 81).
Physical activity has also been explored as a potential intervention for the prevention and treatment of dementia. As regards to prevention, it has been demonstrated that physical activity is a protective factor against Alzheimer's disease and other types of dementia (82, 83). As a treatment, recently an umbrella review has pooled evidence from as many as 27 systematic reviews, including 18 with meta-analyses, overall reporting on 28,205 participants with mild cognitive impairment or dementia (84). The authors showed that mind-body intervention and mixed physical activity interventions had a small effect on global cognition, whereas resistance training had a large effect on global cognition in those with mild cognitive impairment. In people affected by dementia, a small effect of physical activity/exercise emerged in improving global cognition in Alzheimer's disease and all types of dementia. Importantly, physical activity/exercise also improved other outcomes not strictly related to cognition, including the risk of falls, and neuropsychiatric symptoms.
Adjacently, a massive body of evidence has organized an important trend of research on the benefits of physical activity for both prevention and treatment of severe mental disorders, in particular depression (4, 85, 86) and schizophrenia (71, 87). More recently, the evidence has focused on evidence-synthesis (10, 74) and mental health/wellbeing (9).
Other lesser, although highly relevant trends were also uncovered, such as the importance of physical activity for athlete's performance (88, 89). While most of the research efforts in that area have focused on how to optimize performance in the context of professional athletics (90), perfectionism, and excessive physical activity can also be a symptom of mental disorders, and eating disorders in particular (58). This research trends now focus on concussion and its consequence (chronic traumatic encephalopathy) (60).
Finally, a large body of research has focused on physical activity and COVID-19. Physical activity is a protective factor for COVID-19 complications (91). During COVID-19 research has also focused on restrictions and physical activity (63). Finally, physical activity's relevance has also been shown to extend beyond the clinical sciences and start to dialogue with greenness and urban planning (66, 92, 93).
Although various trends of research have developed these last decades, we can identify two important gaps, the one of the roles of physical activity in the prevention or treatment of substance-use disorders, and the one regarding the socioeconomic inequalities in access to physical exercise (94). Meta-review covering this subject (10) concluded that exercise can improve multiple mental health outcomes in those with alcohol-use disorders and substance-use disorders; however, further research is needed in these conditions, notably with the use of mind-body practices (95, 96).
Strengths and limitations
This work has strengths and weaknesses. Strengths are its novel evidence-synthesis approach, complete systematic reviews, and meta-analysis, by providing information on the evolution of research trends over time, the visualization of networks of authors, countries, and institutions, and that go beyond common measures of academic bibliometric performance (i.e., impact factor, H-Index, number of papers or citations). This novel research framework permits repeatable, reproducible, and comparable analysis with less bias than conventional time-consuming reviews that are vulnerable to biased coverage/selection.
Limitations are that, despite the quality check procedures outlined in the methods, this is not a systematic review. Furthermore, gathered data were only obtained from WOSCC, which can limit retrieved publication (94, 97). Also, the centrality and number of citations are not necessarily indicative of the quality of a work, as faulty publications can be highly cited because they are frequently criticized as well (98). Finally, no reporting guidance is available for scientometric studies yet, given their recent introduction in the literature.
Conclusion
In conclusion, researchers have consistently focused on the role of physical activity on cardiovascular disease, other somatic disorders, dementia, mental disorders, athlete's performance, and eating disorders and more recently on COVID-19 pandemic, which clearly shows the role of physical activity as medicine across physical and mental disorders. More recently, the literature has focused on green space, urban planning, and behavior change, further expanding the multidisciplinary reach of physical activity. Taken together our results strengthen and expand the specific and central role of physical activity in public health, calling for the systematic involvement of physical activity professionals as stakeholders in the public health decision-making process.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
MSa and MSo: conceptualization and writing—original draft preparation. MSa, CC, and MSo: methodology, formal analysis, and investigation. MSa, CC, OS, JD, DV, JF, LS, BS, SR, FS, and MSo: writing—review and editing. CC and MSo: supervision. All authors contributed to the article and approved the submitted version.
Funding
Open access funding was provided by the University of Geneva.
Conflict of interest
Author OS has received advisory board honoraria from Otsuka, Lilly, Lundbeck, Sandoz, and Janssen in an institutional account for research and teaching. Author JF has received consultancy fees from Parachute BH for a separate project. Author BS is on the Editorial Board of Ageing Research Reviews, Mental Health and Physical Activity, the Journal of Evidence Based Medicine and the Brazilian Journal of Psychiatry. Author BS has received honorarium from a co-edited a book on exercise and mental illness, advisory work from ASICS & ParachuteBH for unrelated work. Author MSo has received honoraria/has been a consultant for Angelini, Lundbeck and Otsuka.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.943435/full#supplementary-material
References
1. Thompson WR, Sallis R, Joy E, Jaworski CA, Stuhr RM, Trilk JL. Exercise is medicine. Am J Lifestyle Med. (2020) 14:511–23. doi: 10.1177/1559827620912192
2. Lee D-C, Artero EG, Sui X, Blair SN. Mortality trends in the general population: the importance of cardiorespiratory fitness. J Psychopharmacol. (2010) 24(4 Suppl.):27–35. doi: 10.1177/1359786810382057
3. Rezende LFM, Sá TH, Markozannes G, Rey-López JP, Lee IM, Tsilidis KK, et al. Physical activity and cancer: an umbrella review of the literature including 22 major anatomical sites and 770 000 cancer cases. Br J Sports Med. (2018) 52:826–33. doi: 10.1136/bjsports-2017-098391
4. Schuch FB, Vancampfort D, Firth J, Rosenbaum S, Ward PB, Silva ES, et al. Physical activity and incident depression: a meta-analysis of prospective cohort studies. Am J Psychiatry. (2018) 175:631–48. doi: 10.1176/appi.ajp.2018.17111194
5. Svensson M, Brundin L, Erhardt S, Hållmarker U, James S, Deierborg T. Physical activity is associated with lower long-term incidence of anxiety in a population-based, large-scale study. Front Psychiatry. (2021) 12:714014. doi: 10.3389/fpsyt.2021.714014
6. Correll CU, Solmi M, Veronese N, Bortolato B, Rosson S, Santonastaso P, et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: a large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry. (2017) 16:163–80. doi: 10.1002/wps.20420
7. Vancampfort D, Firth J, Schuch FB, Rosenbaum S, Mugisha J, Hallgren M, et al. Sedentary behavior and physical activity levels in people with schizophrenia, bipolar disorder and major depressive disorder: a global systematic review and meta-analysis. World Psychiatry. (2017) 16:308–15. doi: 10.1002/wps.20458
8. Hallgren M, Herring MP, Owen N, Dunstan D, Ekblom Ö, Helgadottir B, et al. Exercise, physical activity, and sedentary behavior in the treatment of depression: broadening the scientific perspectives and clinical opportunities. Front Psychiatry. (2016) 7:36. doi: 10.3389/fpsyt.2016.00036
9. Firth J, Solmi M, Wootton RE, Vancampfort D, Schuch FB, Hoare E, et al. A meta-review of “lifestyle psychiatry” the role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry. (2020) 19:360–80. doi: 10.1002/wps.20773
10. Ashdown-Franks G, Firth J, Carney R, Carvalho AF, Hallgren M, Koyanagi A, et al. Exercise as medicine for mental and substance use disorders: a meta-review of the benefits for neuropsychiatric and cognitive outcomes. Sports Med. (2020) 50:151–70. doi: 10.1007/s40279-019-01187-6
11. Stubbs B, Vancampfort D, Hallgren M, Firth J, Veronese N, Solmi M, et al. Epa guidance on physical activity as a treatment for severe mental illness: a meta-review of the evidence and position statement from the European Psychiatric Association (Epa), Supported by the International Organization of Physical Therapists in Mental Health (Ioptmh). Eur Psychiatry. (2018) 54:124–44. doi: 10.1016/j.eurpsy.2018.07.004
12. van der Kolk NM, de Vries NM, Kessels RPC, Joosten H, Zwinderman AH, Post B, et al. Effectiveness of home-based and remotely supervised aerobic exercise in Parkinson's disease: a double-blind, randomised controlled trial. Lancet Neurol. (2019) 18:998–1008. doi: 10.1016/S1474-4422(19)30285-6
13. Sabe M, Kaiser S, Sentissi O. Physical exercise for negative symptoms of schizophrenia: systematic review of randomized controlled trials and meta-analysis. Gen Hosp Psychiatry. (2020) 62:13–20. doi: 10.1016/j.genhosppsych.2019.11.002
14. Schuch FB, Vancampfort D, Richards J, Rosenbaum S, Ward PB, Stubbs B. Exercise as a treatment for depression: a meta-analysis adjusting for publication bias. J Psychiatr Res. (2016) 77:42–51. doi: 10.1016/j.jpsychires.2016.02.023
15. Stubbs B, Vancampfort D, Rosenbaum S, Ward PB, Richards J, Soundy A, et al. Dropout from exercise randomized controlled trials among people with depression: a meta-analysis and meta regression. J Affect Disord. (2016) 190:457–66. doi: 10.1016/j.jad.2015.10.019
16. Solmi M, Köhler CA, Stubbs B, Koyanagi A, Bortolato B, Monaco F, et al. Environmental risk factors and nonpharmacological and nonsurgical interventions for obesity: an umbrella review of meta-analyses of cohort studies and randomized controlled trials. Eur J Clin Invest. (2018) 48:e12982. doi: 10.1111/eci.12982
17. Arango C, Dragioti E, Solmi M, Cortese S, Domschke K, Murray RM, et al. Risk and protective factors for mental disorders beyond genetics: an evidence-based atlas. World Psychiatry. (2021) 20:417–36. doi: 10.1002/wps.20894
18. Gastaldon C, Solmi M, Correll CU, Barbui C, Schoretsanitis G. Risk factors of postpartum depression and depressive symptoms: umbrella review of current evidence from systematic reviews and meta-analyses of observational studies. Br J Psychiatry. (2022). doi: 10.1192/bjp.2021.222. [Epub ahead of print].
19. Solmi M, Radua J, Stubbs B, Ricca V, Moretti D, Busatta D, et al. Risk factors for eating disorders: an umbrella review of published meta-analyses. Rev Bras Psiquiatria. (2021) 43:314–23. doi: 10.1590/1516-4446-2020-1099
20. Nakagawa S, Samarasinghe G, Haddaway NR, Westgate MJ, O'Dea RE, Noble DWA, et al. Research weaving: visualizing the future of research synthesis. Trends Ecol Evol. (2019) 34:224–38. doi: 10.1016/j.tree.2018.11.007
21. Chen C. Citespace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol. (2006) 57:359–77. doi: 10.1002/asi.20317
22. Hood W, Wilson C. The literature of bibliometrics, scientometrics, and informetrics. Scientometrics. (2001) 52:291–314. doi: 10.1023/A:1017919924342
23. Mongeon P, Paul-Hus A. The journal coverage of Web of Science and Scopus: a comparative analysis. Scientometrics. (2016) 106:213–28. doi: 10.1007/s11192-015-1765-5
24. Sabe M, Pillinger T, Kaiser S, Chen C, Taipale H, Tanskanen A, et al. Half a century of research on antipsychotics and schizophrenia: a scientometric study of hotspots, nodes, bursts, and trends. Neurosci Biobehav Rev. (2022) 136:104608. doi: 10.1016/j.neubiorev.2022.104608
25. Aria M, Cuccurullo C. Bibliometrix: an R-tool for comprehensive science mapping analysis. J Informetr. (2017) 11:959–75. doi: 10.1016/j.joi.2017.08.007
26. Small H. Co-citation in the scientific literature: a new measure of the relationship between two documents. J Am Soc Inf Sci. (1973) 24:265–9. doi: 10.1002/asi.4630240406
27. Freeman LC. A set of measures of centrality based on betweenness. Sociometry. (1977) 40:35–41. doi: 10.2307/3033543
28. Kleinberg J. Bursty and hierarchical structure in streams. Data Min Knowl Discov. (2003) 7:373–97. doi: 10.1023/A:1024940629314
29. Chen C, Ibekwe-SanJuan F, Hou J. The structure and dynamics of cocitation clusters: a multiple-perspective cocitation analysis. J Am Soc Inf Sci Technol. (2010) 61:1386–409. doi: 10.1002/asi.21309
30. Shibata N, Kajikawa Y, Takeda Y, Matsushima K. Detecting emerging research fronts based on topological measures in citation networks of scientific publications. Technovation. (2008) 28:758–75. doi: 10.1016/j.technovation.2008.03.009
31. Chen C. Predictive effects of structural variation on citation counts. J Am Soc Inf Sci Technol. (2012) 63:431–49. doi: 10.1002/asi.21694
32. Egghe L. Theory and practise of the G-index. Scientometrics. (2006) 69:131–52. doi: 10.1007/s11192-006-0144-7
33. Franz SI, Hamilton GV. The effects of exercise upon the retardation in conditions of depression. Am J Psychiatry. (1905) 62:239–56. doi: 10.1176/ajp.62.2.239
34. Lachterman B, Lehmann KG, Abrahamson D, Froelicher VF. “Recovery only” St-segment depression and the predictive accuracy of the exercise test. Ann Intern Med. (1990) 112:11–6. doi: 10.7326/0003-4819-112-1-11
35. Deedwania PC, Carbajal EV. Silent ischemia during daily life is an independent predictor of mortality in stable angina. Circulation. (1990) 81:748–56. doi: 10.1161/01.CIR.81.3.748
36. Moses J, Steptoe A, Mathews A, Edwards S. The effects of exercise training on mental well-being in the normal population: a controlled trial. J Psychosom Res. (1989) 33:47–61. doi: 10.1016/0022-3999(89)90105-0
37. Gibbons RJ, Balady GJ, Beasley JW, Bricker JT, Duvernoy WF, Froelicher VF, et al. Acc/Aha guidelines for exercise testing. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Exercise Testing). J Am Coll Cardiol. (1997) 30:260–311. doi: 10.1161/01.CIR.96.1.345
38. Buman MP, Winkler EA, Kurka JM, Hekler EB, Baldwin CM, Owen N, et al. Reallocating time to sleep, sedentary behaviors, or active behaviors: associations with cardiovascular disease risk biomarkers, Nhanes 2005-2006. Am J Epidemiol. (2014) 179:323–34. doi: 10.1093/aje/kwt292
39. Chastin SF, Palarea-Albaladejo J, Dontje ML, Skelton DA. Combined effects of time spent in physical activity, sedentary behaviors and sleep on obesity and cardio-metabolic health markers: a novel compositional data analysis approach. PLoS ONE. (2015) 10:e0139984. doi: 10.1371/journal.pone.0139984
40. Carney RM, Freedland KE. Depression and coronary heart disease. Nat Rev Cardiol. (2017) 14:145–55. doi: 10.1038/nrcardio.2016.181
41. Pate RR, Pratt M, Blair SN, Haskell WL, Macera CA, Bouchard C, et al. Physical activity and public health. A Recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA. (1995) 273:402–7. doi: 10.1001/jama.1995.03520290054029
42. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. (2002) 346:393–403. doi: 10.1056/NEJMoa012512
43. Wolfe F, Häuser W, Hassett AL, Katz RS, Walitt BT. The development of fibromyalgia–i: examination of rates and predictors in patients with rheumatoid arthritis (Ra). Pain. (2011) 152:291–9. doi: 10.1016/j.pain.2010.09.027
44. Speck RM, Courneya KS, Mâsse LC, Duval S, Schmitz KH. An update of controlled physical activity trials in cancer survivors: a systematic review and meta-analysis. J Cancer Surviv. (2010) 4:87–100. doi: 10.1007/s11764-009-0110-5
45. Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology. (2012) 55:2005–23. doi: 10.1002/hep.25762
46. American Diabetes Association. Standards of medical care in diabetes−2013. Diabetes Care. (2013) 36(Suppl. 1):S11–66. doi: 10.2337/dc13-S011
47. Motl RW. Benefits, safety, and prescription of exercise in persons with multiple sclerosis. Expert Rev Neurother. (2014) 14:1429–36. doi: 10.1586/14737175.2014.983904
48. Henderson VW, Paganini-Hill A, Miller BL, Elble RJ, Reyes PF, Shoupe D, et al. Estrogen for Alzheimer's disease in women: randomized, double-blind, placebo-controlled trial. Neurology. (2000) 54:295–301. doi: 10.1212/WNL.54.2.295
49. Rosenbaum S, Tiedemann A, Sherrington C, Curtis J, Ward PB. Physical activity interventions for people with mental illness: a systematic review and meta-analysis. J Clin Psychiatry. (2014) 75:964–74. doi: 10.4088/JCP.13r08765
50. Erickson KI, Voss MW, Prakash RS, Basak C, Szabo A, Chaddock L, et al. Exercise training increases size of hippocampus and improves memory. Proc Nat Acad Sci USA. (2011) 108:3017. doi: 10.1073/pnas.1015950108
51. Groot C, Hooghiemstra AM, Raijmakers PG, van Berckel BN, Scheltens P, Scherder EJ, et al. The effect of physical activity on cognitive function in patients with dementia: a meta-analysis of randomized control trials. Ageing Res Rev. (2016) 25:13–23. doi: 10.1016/j.arr.2015.11.005
52. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. (2013) 381:752–62. doi: 10.1016/S0140-6736(12)62167-9
53. DeHert M, Schreurs V, Vancampfort D, Van Winkel R. Metabolic syndrome in people with schizophrenia: a review. World Psychiatry. (2009) 8:15–22. doi: 10.1002/j.2051-5545.2009.tb00199.x
54. Ngandu T, Lehtisalo J, Solomon A, Levälahti E, Ahtiluoto S, Antikainen R, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (finger): a randomised controlled trial. Lancet. (2015) 385:2255–63. doi: 10.1016/S0140-6736(15)60461-5
55. Schuch FB, Vancampfort D, Rosenbaum S, Richards J, Ward PB, Veronese N, et al. Exercise for depression in older adults: a meta-analysis of randomized controlled trials adjusting for publication bias. Rev Bras Psiquiatria. (2016) 38:247–54. doi: 10.1590/1516-4446-2016-1915
56. Lubans D, Richards J, Hillman C, Faulkner G, Beauchamp M, Nilsson M, et al. Physical activity for cognitive and mental health in youth: A systematic review of mechanisms. Pediatrics. (2016) 138:e20161642. doi: 10.1542/peds.2016-1642
57. Jones G, Hanton S, Swain A. Intensity and interpretation of anxiety symptoms in elite and non-elite sports performers. Pers Individ Dif. (1994) 17:657–63. doi: 10.1016/0191-8869(94)90138-4
58. Sundgot-Borgen J, Torstveit M. Prevalence of eating disorders in elite athletes is higher than in the general population. Clin J Sport Med. (2004) 14:25–32. doi: 10.1097/00042752-200401000-00005
59. Stoeber J, Rambow A. Perfectionism in adolescent school students: relations with motivation, achievement, and well-being. Pers Individ Dif. (2007) 42:1379–89. doi: 10.1016/j.paid.2006.10.015
60. McKee AC, Daneshvar DH, Alvarez VE, Stein TD. The neuropathology of sport. Acta Neuropathol. (2014) 127:29–51. doi: 10.1007/s00401-013-1230-6
61. Reardon CL, Hainline B, Aron CM, Baron D, Baum AL, Bindra A, et al. Mental health in elite athletes: International Olympic Committee Consensus Statement (2019). Br J Sports Med. (2019) 53:667. doi: 10.1136/bjsports-2019-100715
62. Wang B, Li R, Lu Z, Huang Y. Does comorbidity increase the risk of patients with Covid-19: evidence from meta-analysis. Aging. (2020) 12:6049–57. doi: 10.18632/aging.103000
63. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
64. Mazza MG, De Lorenzo R, Conte C, Poletti S, Vai B, Bollettini I, et al. Anxiety and Depression in Covid-19 Survivors: Role of Inflammatory and Clinical Predictors. Brain Behav Immun. (2020) 89:594–600. doi: 10.1016/j.bbi.2020.07.037
65. Biddle SJH, Ciaccioni S, Thomas G, Vergeer I. Physical activity and mental health in children and adolescents: an updated review of reviews and an analysis of causality. Psychol Sport Exerc. (2019) 42:146–55. doi: 10.1016/j.psychsport.2018.08.011
66. Hartig T, Mitchell R, de Vries S, Frumkin H. Nature and health. Annu Rev Public Health. (2014) 35:207–28. doi: 10.1146/annurev-publhealth-032013-182443
67. Hoffmann K, Sobol NA, Frederiksen KS, Beyer N, Vogel A, Vestergaard K, et al. Moderate-to-high intensity physical exercise in patients with Alzheimer's disease: a randomized controlled trial. J Alzheimers Dis. (2016) 50:443–53. doi: 10.3233/JAD-150817
68. Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. (2020) 396:413–46. doi: 10.1016/S0140-6736(20)30367-6
69. Norton S, Matthews FE, Barnes DE, Yaffe K, Brayne C. Potential for primary prevention of Alzheimer's disease: an analysis of population-based data. Lancet Neurol. (2014) 13:788–94. doi: 10.1016/S1474-4422(14)70136-X
70. Lautenschlager NT, Cox KL, Flicker L, Foster JK, van Bockxmeer FM, Xiao J, et al. Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease: a randomized trial. JAMA. (2008) 300:1027–37. doi: 10.1001/jama.300.9.1027
71. Firth J, Cotter J, Elliott R, French P, Yung AR. A systematic review and meta-analysis of exercise interventions in schizophrenia patients. Psychol Med. (2015) 45:1343–61. doi: 10.1017/S0033291714003110
72. Warburton DER, Bredin SSD. Health benefits of physical activity: a systematic review of current systematic reviews. Curr Opin Cardiol. (2017) 32:541–56. doi: 10.1097/HCO.0000000000000437
73. Stubbs B, Koyanagi A, Schuch FB, Firth J, Rosenbaum S, Gaughran F, et al. Physical activity levels and psychosis: a mediation analysis of factors influencing physical activity target achievement among 204 186 people across 46 low- and middle-income countries. Schizophr Bull. (2017) 43:536–45. doi: 10.1093/schbul/sbw111
74. Vancampfort D, Stubbs B. Physical activity and metabolic disease among people with affective disorders: prevention, management and implementation. J Affect Disord. (2017) 224:87–94. doi: 10.1016/j.jad.2016.07.042
75. Aguilar BAS, Tebar WR, Silva SCB, Gomes LQ, Damato TMM, Mota J, et al. Leisure-time exercise is associated with lower depressive symptoms in community dwelling adults. Eur J Sport Sci. (2022) 22:916–25. doi: 10.1080/17461391.2021.1895892
76. Schuch FB, Werneck AO, Vancampfort D, Stubbs B, Teychene M, Lotufo PA, et al. Cross-sectional associations of leisure and transport related physical activity with depression and anxiety. J Psychiatr Res. (2021) 140:228–34. doi: 10.1016/j.jpsychires.2021.05.053
77. van Sluijs EMF, Ekelund U, Crochemore-Silva I, Guthold R, Ha A, Lubans D, et al. Physical activity behaviours in adolescence: current evidence and opportunities for intervention. Lancet. (2021) 398:429–42. doi: 10.1016/S0140-6736(21)01259-9
78. Thompson PD, Buchner D, Pina IL, Balady GJ, Williams MA, Marcus BH, et al. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: A Statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity). Circulation. (2003) 107:3109–16. doi: 10.1161/01.CIR.0000075572.40158.77
79. WHO. Who Guidelines on Physical Activity and Sedentary Behaviour. Geneva: World Health Organization (2020).
80. Sofi F, Valecchi D, Bacci D, Abbate R, Gensini GF, Casini A, et al. Physical activity and risk of cognitive decline: a meta-analysis of prospective studies. J Intern Med. (2011) 269:107–17. doi: 10.1111/j.1365-2796.2010.02281.x
81. Colcombe S, Kramer AF. Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol Sci. (2003) 14:125–30. doi: 10.1111/1467-9280.t01-1-01430
82. Ahlskog JE. Aerobic exercise: evidence for a direct brain effect to slow Parkinson disease progression. Mayo Clinic Proc. (2018) 93:360–72. doi: 10.1016/j.mayocp.2017.12.015
83. Mentis A-FA, Dardiotis E, Efthymiou V, Chrousos GP. Non-genetic risk and protective factors and biomarkers for neurological disorders: a meta-umbrella systematic review of umbrella reviews. BMC Med. (2021) 19:6. doi: 10.1186/s12916-020-01873-7
84. Demurtas J, Schoene D, Torbahn G, Marengoni A, Grande G, Zou L, et al. Physical activity and exercise in mild cognitive impairment and dementia: an umbrella review of intervention and observational studies. J Am Med Direct Assoc. (2020) 21:1415–22.e6. doi: 10.1016/j.jamda.2020.08.031
85. Strawbridge WJ, Deleger S, Roberts RE, Kaplan GA. Physical activity reduces the risk of subsequent depression for older adults. Am J Epidemiol. (2002) 156:328–34. doi: 10.1093/aje/kwf047
86. Rebar AL, Stanton R, Geard D, Short C, Duncan MJ, Vandelanotte C, et al. Meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol Rev. (2015) 9:366–78. doi: 10.1080/17437199.2015.1022901
87. Vancampfort D, Knapen J, Probst M, Scheewe T, Remans S, De Hert M, et al. Systematic review of correlates of physical activity in patients with schizophrenia. Acta Psychiatr Scand. (2012) 125:352–62. doi: 10.1111/j.1600-0447.2011.01814.x
88. Chen Y, Buggy C, Kelly S. Winning at all costs: a review of risk-taking behaviour and sporting injury from an occupational safety and health perspective. Sports Med. (2019) 5:15. doi: 10.1186/s40798-019-0189-9
89. Wyss T, Boesch M, Roos L, Tschopp C, Frei KM, Annen H, et al. Aerobic fitness level affects cardiovascular and salivary alpha amylase responses to acute psychosocial stress. Sports Med. (2016) 2:33. doi: 10.1186/s40798-016-0057-9
90. Burton D. Advances in sport and exrecise psychology measurement. In: Duda IJL, editor. Measuring Competitive State Anxiety. Morgantown: Fitness Information Technology, Inc. (1998). p. 129–48.
91. Sallis R, Young DR, Tartof SY, Sallis JF, Sall J, Li Q, et al. Physical inactivity is associated with a higher risk for severe covid-19 outcomes: a study in 48 440 adult patients. Br J Sports Med. (2021) 55:1099. doi: 10.1136/bjsports-2021-104080
92. Akpinar A. How is quality of urban green spaces associated with physical activity and health? Urban Forest Urban Green. (2016) 16:76–83. doi: 10.1016/j.ufug.2016.01.011
93. Bedimo-Rung AL, Mowen AJ, Cohen DA. The significance of parks to physical activity and public health: a conceptual model. Am J Prev Med. (2005) 28(2 Suppl. 2):159–68. doi: 10.1016/j.amepre.2004.10.024
94. Stalsberg R, Pedersen AV. Are differences in physical activity across socioeconomic groups associated with choice of physical activity variables to report? Int J Environ Res Public Health. (2018) 15:922. doi: 10.3390/ijerph15050922
95. Wang D, Wang Y, Wang Y, Li R, Zhou C. Impact of physical exercise on substance use disorders: a meta-analysis. PLoS ONE. (2014) 9:e110728. doi: 10.1371/journal.pone.0110728
96. Vancampfort D, Stubbs B, Van Damme T, Smith L, Hallgren M, Schuch F, et al. The efficacy of meditation-based mind-body interventions for mental disorders: a meta-review of 17 meta-analyses of randomized controlled trials. J Psychiatr Res. (2021) 134:181–91. doi: 10.1016/j.jpsychires.2020.12.048
97. Visser M, van Eck NJ, Waltman L. Large-scale comparison of bibliographic data sources: scopus, web of science, dimensions, crossref, and microsoft academic. Quant Sci Stud. (2021) 2:20–41. doi: 10.1162/qss_a_00112
Keywords: physical exercise, mental illness, evidence synthesis, scientometrics, CiteSpace
Citation: Sabe M, Chen C, Sentissi O, Deenik J, Vancampfort D, Firth J, Smith L, Stubbs B, Rosenbaum S, Schuch FB and Solmi M (2022) Thirty years of research on physical activity, mental health, and wellbeing: A scientometric analysis of hotspots and trends. Front. Public Health 10:943435. doi: 10.3389/fpubh.2022.943435
Received: 17 May 2022; Accepted: 15 July 2022;
Published: 09 August 2022.
Edited by:
Peter Kokol, University of Maribor, SloveniaReviewed by:
Jernej Zavrsnik, University of Alabama, United StatesBoštjan Šimunič, Scientific Research Center Koper, Slovenia
Copyright © 2022 Sabe, Chen, Sentissi, Deenik, Vancampfort, Firth, Smith, Stubbs, Rosenbaum, Schuch and Solmi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michel Sabe, bWljaGVsLnNhYmVAaGN1Z2UuY2g=
†These authors have contributed equally to this work and share first authorship