
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 25 July 2022
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.938067
This article is part of the Research TopicImproving Immunization Programmes Uptake and Addressing Vaccine HesitancyView all 17 articles
 Arkadiusz Dziedzic1
Arkadiusz Dziedzic1 Julien Issa2,3
Julien Issa2,3 Salman Hussain4
Salman Hussain4 Marta Tanasiewicz1
Marta Tanasiewicz1 Robert Wojtyczka5
Robert Wojtyczka5 Robert Kubina6
Robert Kubina6 Marta Dyszkiewicz Konwinska2,7
Marta Dyszkiewicz Konwinska2,7 Abanoub Riad8*
Abanoub Riad8*Since healthcare professionals (HCPs) play a critical role in shaping their local communities' attitudes toward vaccines, HCPs' beliefs and attitudes toward vaccination are of vital importance for primary prevention strategies. The present study was designed as a cross-sectional survey-based study utilizing a self-administered questionnaire to collect data about COVID-19 vaccine booster hesitancy (VBH) among Polish HCPs and students of medical universities (MUSs). Out of the 443 included participants, 76.3% were females, 52.6% were HCPs, 31.8% were previously infected by SARS-CoV-2, and 69.3% had already received COVID-19 vaccine booster doses (VBD). Overall, 74.5% of the participants were willing to receive COVID-19 VBD, while 7.9 and 17.6% exhibited their hesitance and rejection, respectively. The most commonly found promoter for acceptance was protection of one's health (95.2%), followed by protection of family's health (81.8%) and protection of community's health (63.3%). Inferential statistics did not show a significant association between COVID-19 VBH and demographic variables, e.g., age and gender; however, the participants who had been previously infected by SARS-CoV-2 were significantly more inclined to reject the VBD. Protection from severe infection, community transmission, good safety profile, and favorable risk-benefit ratio were the significant determinants of the COVID-19 VBD acceptance and uptake. Fear of post-vaccination side effects was one of the key barriers for accepting COVID-19 VBD, which is consistent with the pre-existing literature. Public health campaigns need to highlight the postulated benefits of vaccines and the expected harms of skipping VBD.
Over the last 2 years, it became evident that coronavirus disease 2019 (COVID-19) transmission chains can be interrupted by herd immunity achieved either by massive vaccination of the community or natural infection (1, 2). Besides the ethical questions about building herd immunity by infection, cost/benefit analysis of this strategy had never been favorable because the burden of casualties was unpredictable (2). For this reason, achieving herd immunity by vaccination was more convincing and reliable.
Since the start of COVID-19 mass vaccination campaigns in December 2020, about 59.3% of the world population has been fully vaccinated (3). As defined by the U.S. Centers for Disease Control and Prevention (CDC), a fully vaccinated person is an individual who is “2 weeks after receiving all recommended doses in the primary series of their COVID-19 vaccination” (4).
Alongside the increase of fully vaccinated individuals toward achieving herd immunity, a decline in the humoral immunity after 6 months of vaccination with the second dose has been reported leading to a new rise of COVID-19 infections (5, 6). Additionally, several COVID-19 variants have been reported since the beginning of the pandemic where only five are classified as variants of concern (VOC) according to their effect on the pandemic situation; Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), Delta (B.1.617.2), and Omicron (B.1.1.529) (7). Consequently, the VOCs affected the incidence of COVID-19 infections through rapid dissemination of the infection leading to hospitalization and mortality. Based on the aforementioned obstacles that restrict the process of attaining herd immunity, the mass vaccination campaign needs to continue side by side with the booster or third dose vaccination as a mediator in increasing the immoral immunity and enhancing the vaccine effectiveness (8).
As of September 2021, booster dose vaccination campaigns have been initiated in Poland (9). Despite the type of primary vaccination, the first to receive the booster does were health care professionals (HCPs) that are at risk of COVID-19 infection, together with the individuals aged 50 years old and above that are fully vaccinated for at least 6 months (9). Subsequently, in December 2021 all people aged from 18 to 49 were able to get vaccinated with the booster dose (10). Reportedly, on April 20, 2022, The Polish Ministry of Health announced the launch of the second booster dose vaccination campaign for people aged 80 years old and above who have received the first booster dose for at least 150 days also the immunocompromised individuals from the age of 12 years old were allowed to take the second booster dose if needed (11). Regardless of the efforts promoting third dose vaccination, only 51.8% of the fully vaccinated Poles have taken the first booster dose (12). A study by Rzymski et al. (13) reported a significant level of hesitancy for receiving the COVID-19 vaccine booster dose among the Polish community; furthermore, another study by Babicki and Mastalerz-Migas (14) reported a low level of booster dose acceptance among Poles. The previously experienced vaccine side effects and the booster dose safety and effectiveness were the primary reasons for the hesitancy toward COVID-19 third dose vaccination (13). Therefore, the present study was carried out to specifically target Polish HCPs and evaluate their views and attitudes toward COVID-19 vaccine booster doses (VBD).
The World Health Organization (WHO) defines vaccine hesitancy as “delay in acceptance or refusal of vaccines despite availability of vaccine services” (15). The risk factors of vaccine hesitancy can be classified according to the 3-C model of the WHO-Strategic Advisory Group of Experts on Immunization (SAGE), including complacency, convenience, and confidence (16). The three core elements of vaccine hesitancy are usually mediated by individuals' vaccine-related knowledge and health literacy levels (17–19). The health-related beliefs and attitudes of HCPs play a significant role in primary prevention and health promotion as they are broadly perceived as role models and credible sources of health information (19, 20). Therefore, COVID-19 booster dose hesitancy among HCPs may negatively impact public confidence in booster doses (21).
The overarching goal of this study was to evaluate COVID-19 vaccine booster hesitancy (VBH) among HCPs and medical universities students (MUSs) in Poland. The primary objective was to estimate the prevalence of COVID-19 VBH among Polish HCPs and MUSc, while the secondary objectives were: (i) to evaluate the demographic, anamnestic, and psychosocial drivers of COVID-19 VBD-related acceptance and (ii) to assess the correlation between COVID-19 VBD-related acceptance and actual VBD uptake among the target population.
The present work had been designed as an analytical cross-sectional survey-based study that was carried out between December 2021 and January 2022. A self-administered questionnaire (SAQ) was used for the purpose of data collection after being digitally designed using KoBoToolbox (Harvard Humanitarian Initiative, Cambridge, MA, USA, 2021) (22). The study had been designed and reported in full compliance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies (23).
The target population of this study were HCPs and MUSc in Poland. The exclusion criteria were: (i) not working as a HCP or studying at a medical university, (ii) providing insufficient demographic information, and (iii) not providing their informed consent a priori. The participation in this study was completely voluntary, the participants received no financial rewards or any other means of incentives to take part in this study. The participants' interest, especially the students, in participating in this study was not coerced by any means of threats. The participants' identity was kept anonymous in order to control the Hawthorne's effect and information bias.
A non-random sampling strategy was used for data collection through convenience recruitment. The participants were invited to this study through multiple channels in two major academic centers, Katowice and Poznan. A uniform resource locator (URL) and quick response (QR) code for the questionnaire were sent to the potential participants as they were able to download it from the project promoting sources, such as Medical Universities websites, scientific societies and professional regulatory bodies.
The pragmatic sample size required for this study was computed using Epi-Info™ version 7.2.5 (CDC. Atlanta, GA, USA, 2021), specifically through the module of “Population Survey” (24, 25). Following the assumptions of 5% as an error margin, 97% as a confidence level, 71% as an expected outcome frequency which was based on a recent study for Polish adults, and 10% as a postulated proportion of faulty responses due to careless/insufficient efforts, the required sample was 427 responses (13).
A total of 456 responses were received from the potential participants, 13 of which were excluded due to insufficiency of demographic information that were crucial to their classification and subsequent analysis.
The SAQ that was used in this study had been used in previous studies concerned with evaluating COVID-19 VBH in Czechia and Germany (21, 26). The psychometric validation process comprised of content validity evaluation and test re-test reliability which showed that this SAQ had substantial reliability denoted by a mean Cohen's kappa coefficient of 0.80 ± 0.19 (IQR: 0.60–1.00) (21).
The SAQ was consisted of 17 items that were divided into four basic sections; (i) demographic information: gender, age, profession, and geographic region, (ii) COVID-19-related anamnesis: prior infection, its onset and severity, vaccination history, number of doses, and post-vaccination hospitalization and medical care, (iii) willingness to receive COVID-19 VBD evaluated by a 5-point Likert scale ranging from “Totally Disagree = 1” to “Totally Agree = 5,” and (iv) psychosocial drivers of COVID-19 VBH; e.g., protection against severe infection and community transmission.
The attitudes toward COVID-19 VBD were stratified into three levels based on the responses to the 5-point Likert scale: “VBD Rejection” group included those who responded “Totally Disagree” and “Disagree,” “VBD Hesitancy” group included those who responded “Not Sure,” and “VBD Acceptance” group included those who responded “Agree” and “Totally Agree.” To facilitate the subsequent analyses, the participants who received the third dose of the vaccine were denoted as “Triple Vaccinated.”
The proposed study protocol had been reviewed and approved by the Ethics Committee of the Medical University of Silesia on 20 July 2021 (PCN/CBN/0022/KB/161/21). The Declaration of Helsinki for research involving human subjects and the European Union (EU) General Data Protection Regulation (GDPR) governed the process of data collection, storing, and handling (27, 28). All the participants provided their informed consent digitally prior to their participation, and no information or responses were collected before that point. The study participants were allowed to leave the study at any moment without the need to justify their decision. No identifying personal data, e.g., email or telephone number was collected from the participants; therefore, retrospective identification of the participants was not possible.
All descriptive and inferential statistical tests were performed using the Statistical Package for the Social Sciences (SPSS) version 28.0 (SPSS Inc. Chicago, IL, USA, 2021) except for regression analyses that were performed using the R-based open software “Jamovi” (29, 30). Shapiro Wilk test was used to evaluate the distribution of numerical variables with a significance level (Sig.) of 5%. Frequencies (n) and percentages (%) were used to evaluate present the categorical and ordinal variables such as gender, pregnancy, vaccination status, attitudes toward COVID-19 VBD, and psychosocial drivers, while means, standard deviations and interquartile ranges (μ ± SD “IQR”) were used for numerical variables, e.g., age. Subsequently, inferential tests such as Chi-squared test (χ2), Fisher's exact test, and Mann-Whitney (U) test were used to evaluate the association between dependent and independent variables. Bivariate correlation using the non-parametric test of Spearman's rank was performed between COVID-19 VBD attitudes and actual uptake. Finally, the multivariable logistic regression was used to estimate the adjusted odds ratio (AOR) of various psychosocial drivers for COVID-19 VBD acceptance and actual uptake. The regression analysis was adjusted for the demographic and anamnestic variables that were found to be significant in the univariate analysis. All inferential tests were performed with a confidence level (CI) of 95% and a significance level (Sig.) of 5%.
A total of 443 participants were included in this study, out of which 233 (52.6%) were HCPs and 210 (47.4%) were MUSc. In general, females were the vast majority (76.3%), followed by males (22.8%) and diverse-gender (0.9%) participants without significant differences between professionals' and students' groups. Out of the 338 participating females, only 7 (2.1%) were pregnant and they all belonged to the professionals' group. The mean age of the sample was 31.1 ± 11.4 with a statistically significant difference (Sig. <0.001) between professionals (38.8 ± 10.9) and students (22.6 ± 2.3) (Table 1).
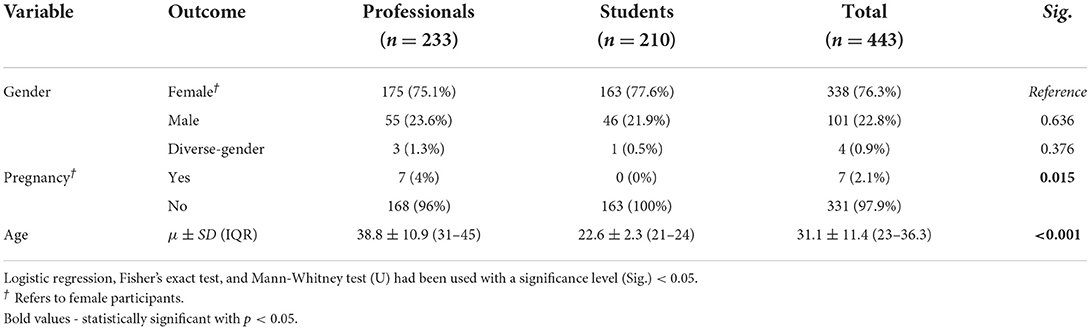
Table 1. Demographic characteristics of polish healthcare professionals and students responding to COVID-19 VBH survey, December 2021–January 2022 (n = 443).
The most participating region was Silesian Voivodeship (54.4%), followed by the Greater Poland Voivodeship (28.9%), and the Lesser Poland Voivodeship (8.1%).
Nearly one-third (31.8%) of the participants reported being infected previously with COVID-19, and the vast majority of them were infected before receiving the first dose (73%), followed by those who were infected after the second dose (22.7%), and those who were infected between the doses (4.3%). According to the Australian guidelines for clinical classification of COVID-19 patients, most of our participants experienced mild infection (66%), followed by moderate (29.1%), asymptomatic (2.8%), and severe infection (2.1%). There was no significant difference between professionals' and students' groups in terms of COVID-19 infection-related anamnesis.
The vast majority of the participants (93.7%) reported receiving at least one dose of COVID-19 vaccines without a significant difference between professionals and students. As expected, the most common vaccine type was Pfizer-BioNTech (78.3%) which was significantly (Sig. <0.001) more common among professionals (89.3%) than students (66.7%). AstraZeneca-Oxford was the second most common vaccine type (13%) and it was significantly (Sig. <0.001) more common among students (22.9%) than professionals (3.7%). To a limited extent, Moderna and Janssen vaccines were received by 4.8 and 3.9% of the participants. Most of the participants were triple vaccinated (74%), with a significant difference (Sig. <0.001) between professionals (79%) and students (68.7%). Only 4.3% of the whole sample received a single vaccine dose, and 3.4 and 4.3% reported post-vaccination hospitalization and seeking medical care (Table 2).
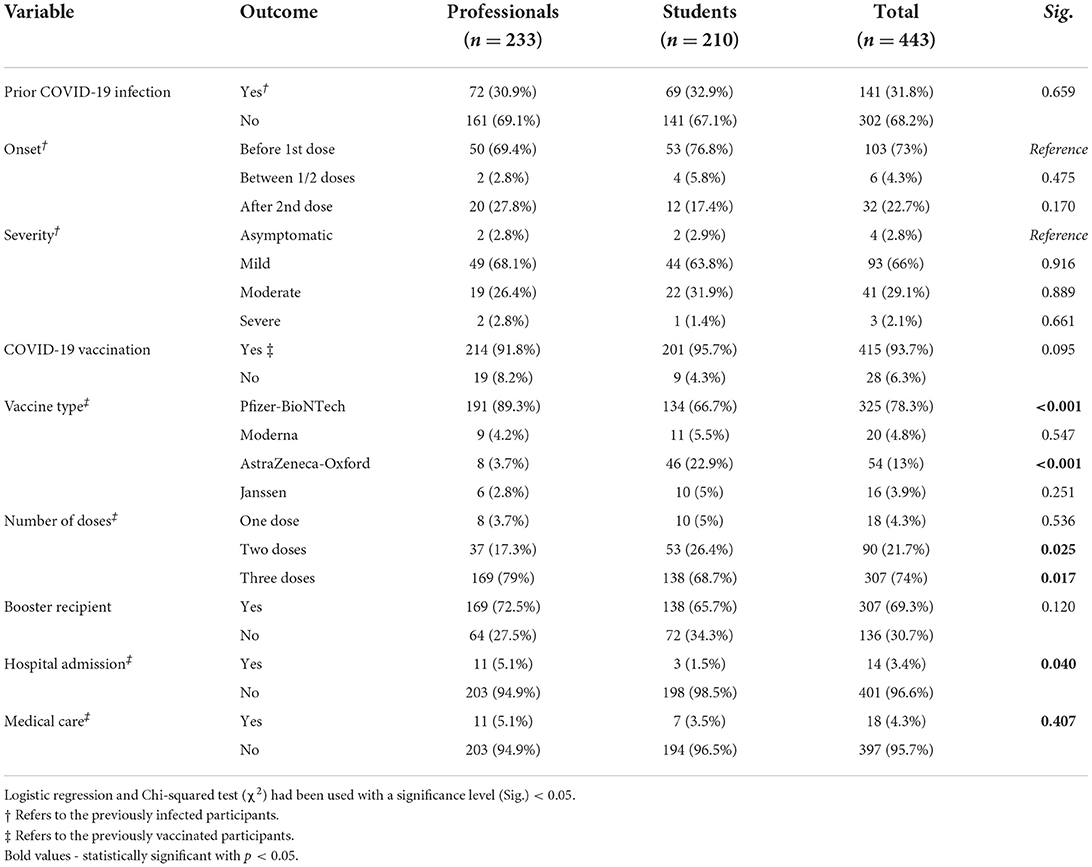
Table 2. Anamnestic characteristics of polish healthcare professionals and students responding to COVID-19 VBH survey, December 2021–January 2022 (n = 443).
Overall, almost three-quarters (74.5%) of the participants indicated their acceptance to receive COVID-19 VBD, while 17.6% indicated their rejection, and 7.9% were hesitant. No significant difference between professionals and students in terms of VBD-related attitudes. The triple vaccinated individuals had a significantly (Sig. <0.001) higher level of VBD acceptance (87.9 vs. 44.1%) and a significantly (Sig. <0.001) lower level of VBD rejection (8.1 vs. 39%) compared with their counterparts who did not receive the third dose, respectively.
When asked about their reasons to accept COVID-19 VBD, the most commonly reported promoted was protection of one's own health (96.3%), followed by protection of family's health (82.5%), and protection of community's health (65%). On the other hand, work or study place endorsement (5%) and avoidance of frequent testing (20%) were the least reported promoters. The students were significantly more inclined to indicate testing avoidance (20 vs. 11.2%) and having easier social life with less restrictions (58.8 vs. 43.5%) than the professionals, respectively (Table 3).
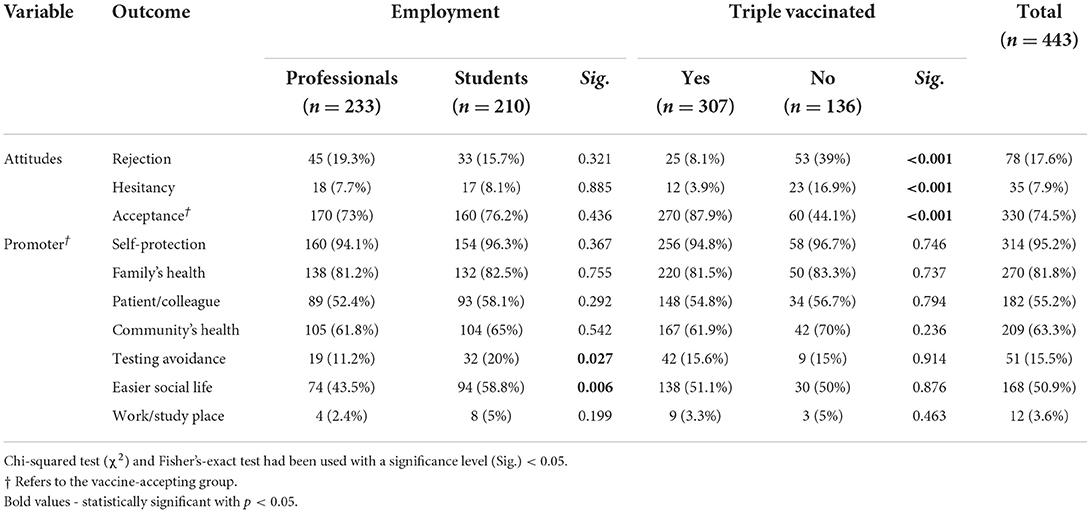
Table 3. Attitudes toward COVID-19 VBD of polish healthcare professionals and students responding to COVID-19 VBH survey, December 2021–January 2022 (n = 443).
More than three-quarters (76.1%) of the participants agreed with the notion that VBD were capable of preventing severe infection, with a significant difference (Sig. <0.001) between triple vaccinated participants (87.9%) and their counterparts (49.3%) and with no significant difference (Sig. = 0.495) between professionals (76.4%) and students (75.7%). Similarly, the notion that VBD were able to prevent symptomatic infection was significantly (Sig. <0.001) more accepted by the triple vaccinated participants (73.6%) than their counterparts (38.2%). Moreover, the notion that VBD were able to prevent community transmission was significantly (Sig. <0.001) more accepted by the triple vaccinated participants (65.1%) than their counterparts (27.9%).
Interestingly, 68.4% of the participants did not agree to postpone receiving of their VBD until they found convincing evidence that the VBD would control the emerging variants. While there was no statistically significant (Sig. = 0.407) difference between professionals (72.1%) and students (64.3%) in the notion of variants control, the triple vaccinated participants (80.8%) were significantly (Sig. <0.001) more inclined to disagree with this notion compared with their counterparts (40.4%).
About three-quarters (75.4%) of the participants agreed with the notion that VBD would be as safe as the primer doses, with a significant difference (Sig. <0.001) between triple vaccinated participants (86.3%) and their counterparts (50.7%) and with no significant difference (Sig. = 0.280) between professionals (73.8%) and students (77.1%). Almost two-thirds (66.6%) of the participants disagreed with the notion the VBD would cause severe side effects interfering with their daily routine, with a significant difference (Sig. <0.001) between triple vaccinated participants (76.9%) and their counterparts (43.4%) and with no significant difference (Sig. = 0.777) between professionals (65.7%) and students (67.6%) (Figure 1).
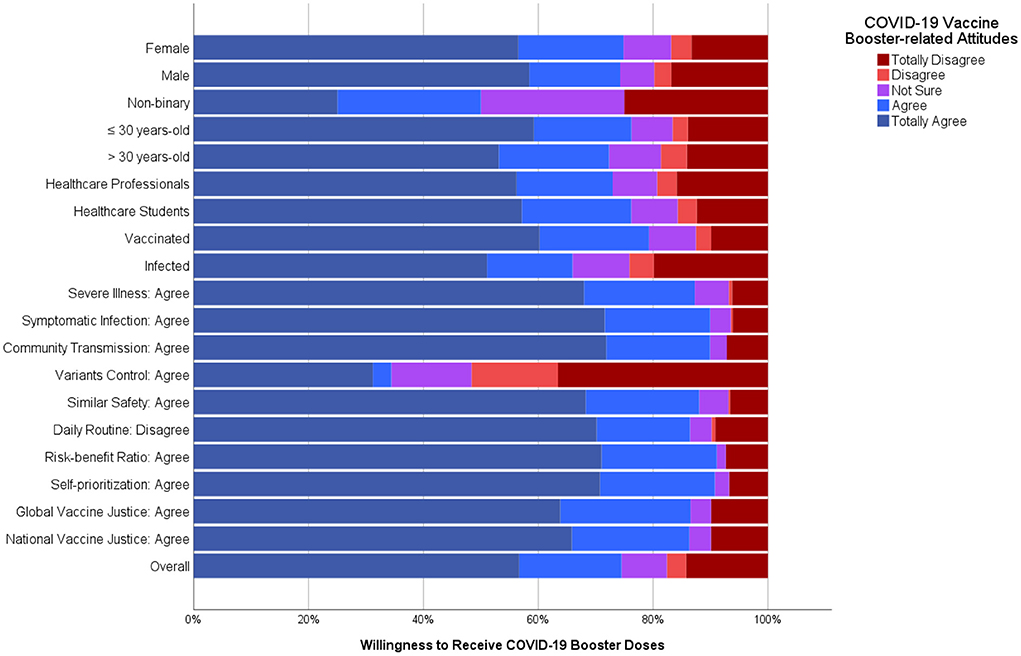
Figure 1. Determinants of COVID-19 vaccine booster-related attitudes of polish healthcare professionals and students responding to COVID-19 VBH survey, December 2021–January 2022 (n = 443).
A large proportion of the participants agreed that the benefits of VBD would outweigh their risks (70.9%) and that they should be prioritized to receive the VBD based on their occupational risk (73.5%). However, the differences between professionals and students were not statistically significant for both notions, the triple vaccinated participants had significantly higher agreement levels with both of them (84.4 and 88.2%, respectively) compared with their counterparts (40.4 and 40.4%, respectively).
The positions of our participants from the ethical dilemmas of vaccine justice either globally or nationally was almost equally distributed between agreement and disagreement, without significant differences between professionals and students (Table 4).
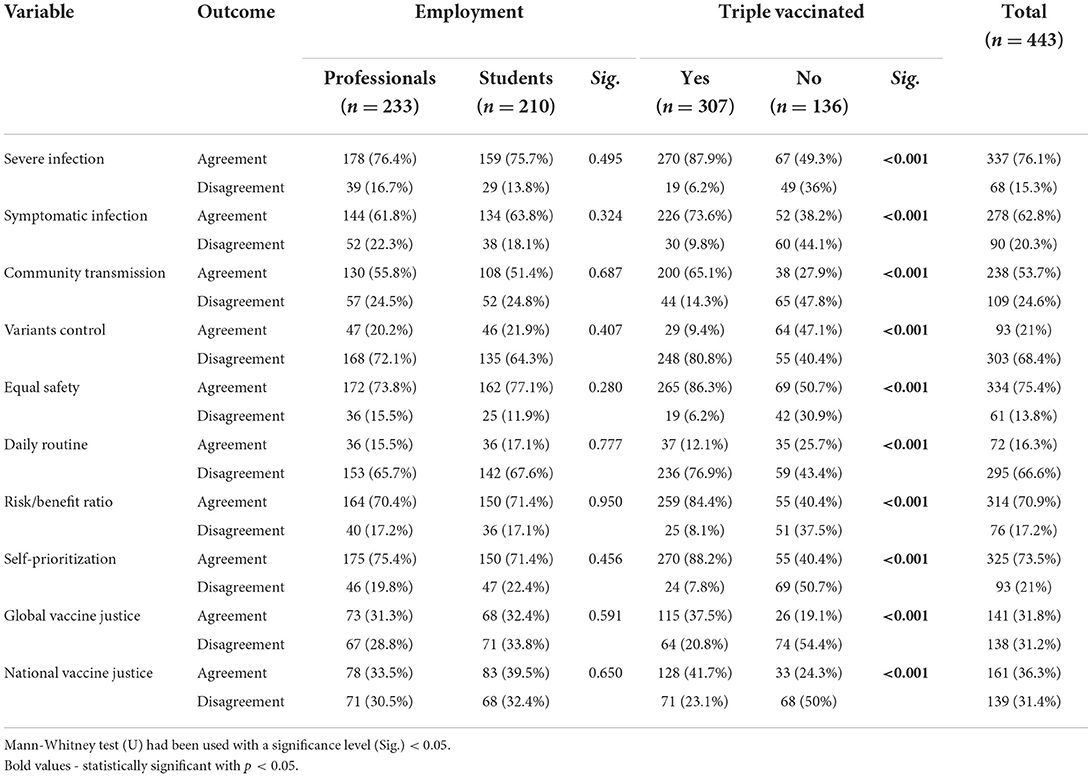
Table 4. Determinants of COVID-19 VBH among polish healthcare professionals and students responding to COVID-19 VBH survey, December 2021–January 2022 (n = 443).
On evaluating the demographic and anamnestic determinants of COVID-19 VBD-related attitudes, no significant difference was found among genders, age groups, pregnancy statuses, COVID-19 infection onset, COVID-19 infection severity, or vaccine type. The participants who had been previously infected by SARS-CoV-2 were significantly more inclined to reject the VBD (24.1 vs. 14.6%) and less inclined to accept the VBD (66 vs. 78.5%) than their counterparts. Contrarily, the participants who had been previously vaccinated against SARS-CoV-2 were significantly less inclined to reject the VBD (12.5 vs. 92.9%) and more inclined to accept the VBD (79.3 vs. 3.6%) than their counterparts. Hospital admission (35.7 vs. 11.7%) and seeking medical care (33.3 vs. 11.6%) were significantly associated with higher levels of COVID-19 VBD rejection (Table 5).
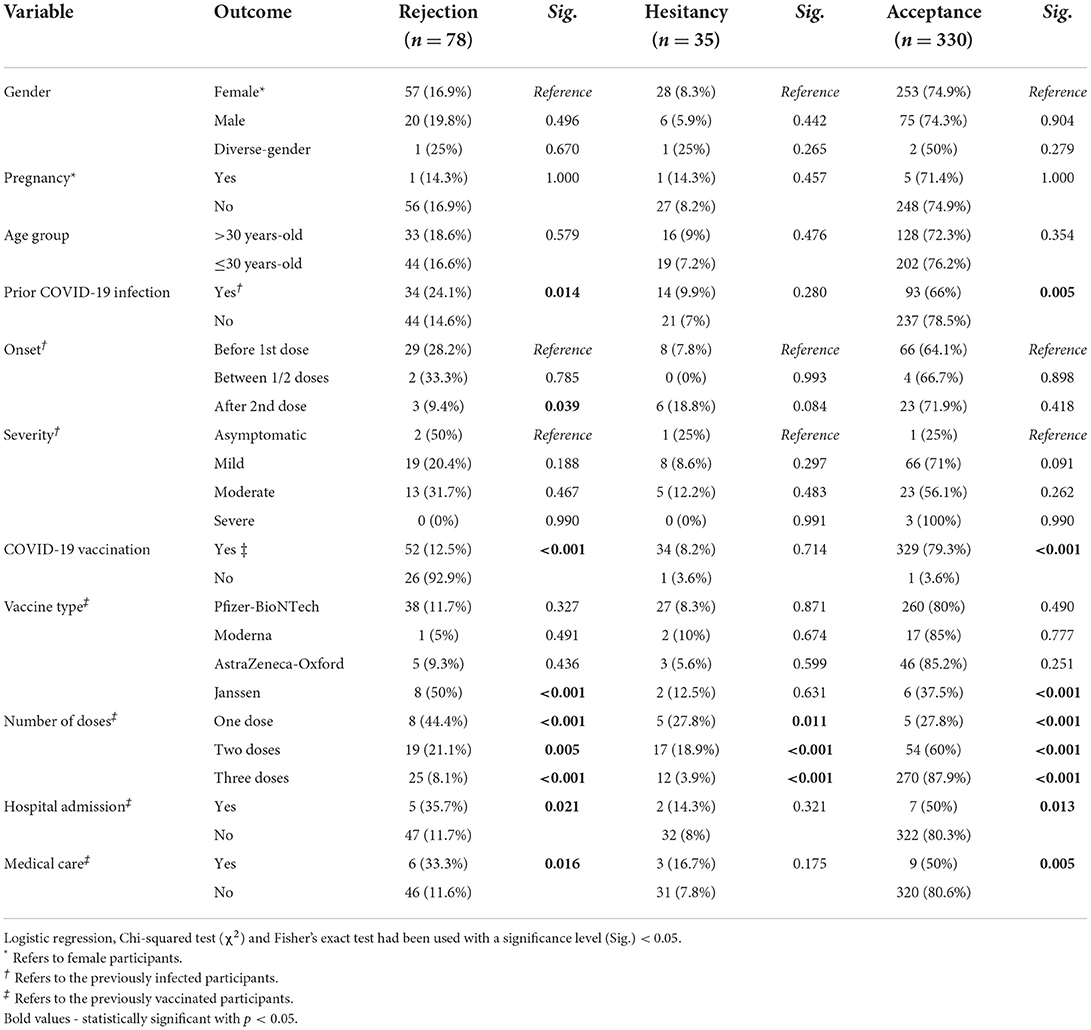
Table 5. Demographic and anamnestic determinants of COVID-19 vaccine booster acceptance among polish healthcare professionals and students responding to COVID-19 VBH survey, December 2021–January 2022 (n = 443).
On evaluating the demographic and anamnestic determinants of COVID-19 VBD actual uptake, no significant difference was found among genders, age groups, pregnancy statuses, COVID-19 infection onset, COVID-19 infection severity, post-vaccination hospitalization, or seeking medical care. The participants who had been previously infected by SARS-CoV-2 had a significantly (Sig. <0.001) lower uptake level (58.2%) than their counterparts (74.5%). The participants who had been previously vaccinated against SARS-CoV-2 using Pfizer-BioNTech (80%) and Moderna (80%) had higher levels of VBD uptake than those who received AstraZeneca-Oxford (57.4%) and Janssen (0%) (Table 6).
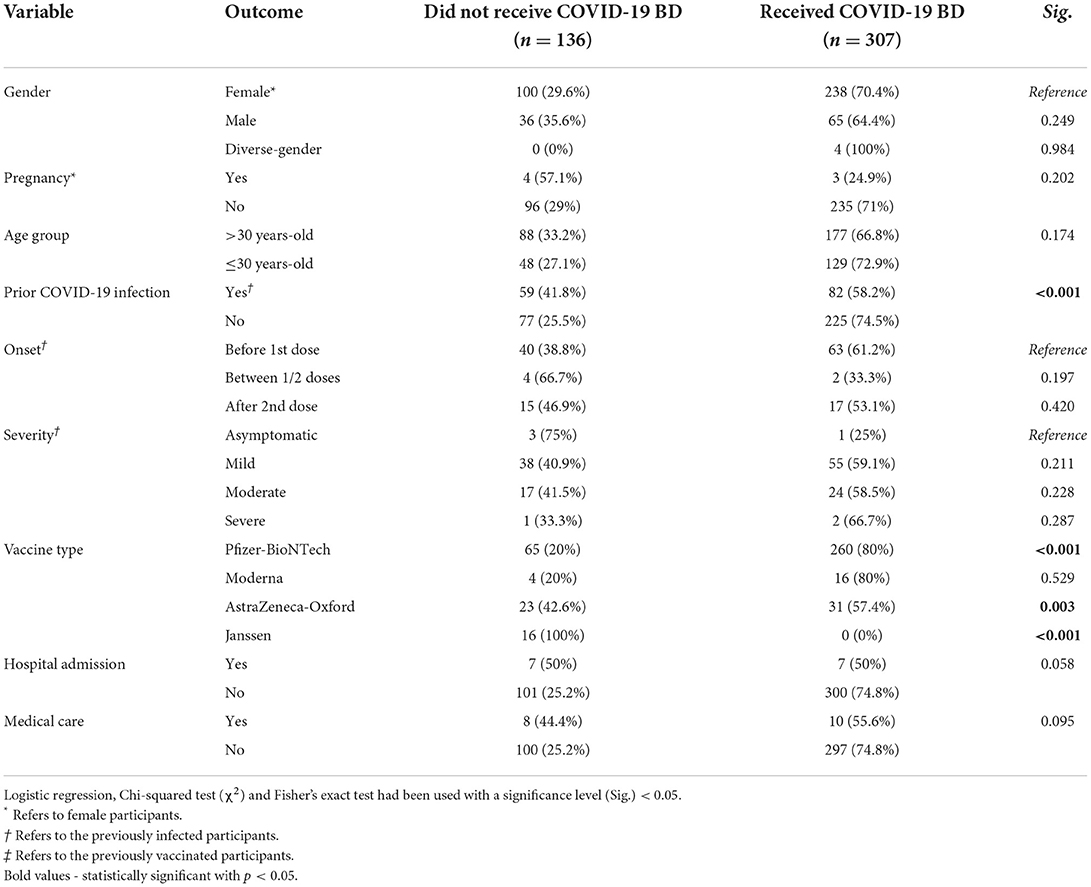
Table 6. Demographic and anamnestic determinants of COVID-19 vaccine booster uptake among polish healthcare professionals and students responding to COVID-19 VBH survey, December 2021–January 2022 (n = 443).
The bivariate correlation between COVID-19 VBD-related attitudes and actual uptake revealed that there had been moderate and positive correlation between VBD-related acceptance and number of doses (ρ = 0.508; Sig. <0.001) and being triple vaccinated (ρ = 0.464; Sig. <0.001). Contrarily, there correlation was moderate and negative between VBD-related rejection and number of doses (ρ = −0.437; Sig. <0.001) and being triple vaccinated (ρ = −0.373; Sig. <0.001) (Table 7).
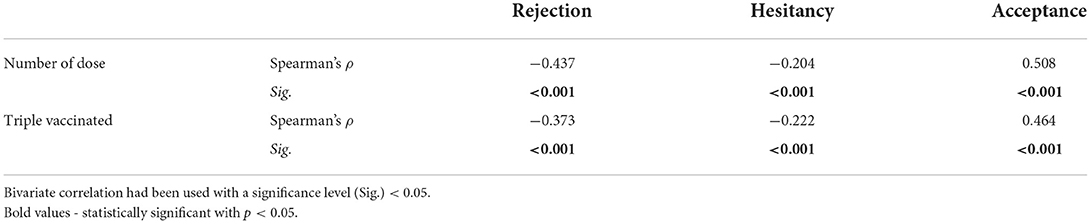
Table 7. Correlation between vaccine doses & willingness to receive COVID-19 vaccine booster doses.
The multivariable logistic regression of psychosocial drivers of COVID-19 VBD-related acceptance was adjusted for prior infection, vaccine type, number of doses, hospitalization, and medical care. The participants who agreed with the severe infection notion had an increased adjusted odds ratio (AOR) of 5.142 (CI 95%: 2.346–11.269) times to accept COVID-19 VBD. Similarly, agreement with the symptomatic infection (AOR: 5.502; CI 95%: 2.717–11.139), community transmission (AOR: 5.898; CI 95%: 3.041–11.438), equal safety (AOR: 3.733; CI 95%: 1.622–8.592), favorable risk-benefit ratio (AOR: 9.573; CI 95%: 4.461–20.544), and self-prioritization (AOR: 17.407; CI 95%: 8.382–36.150) had an increased odd to accept COVID-19 VBD. On the other hand, agreement with the notion of variant control decreased the odds of accepting COVID-19 VBD (AOR: 0.143; CI 95%: 0.072–0.286). Ignoring the ethical dilemmas globally (AOR: 2.584; CI 95%: 1.274–5.242) and nationally (AOR: 2.426; CI 95%: 1.233–4.772) was associated with increased odds of VBD acceptance (Table 8).
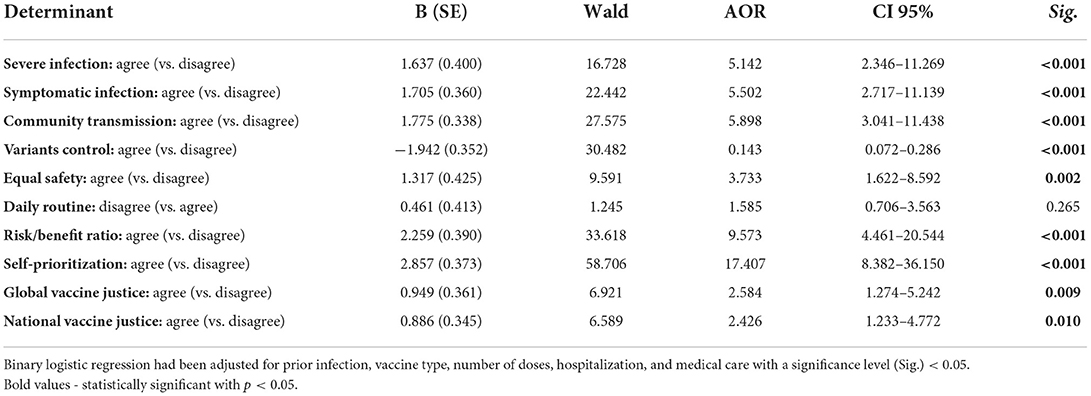
Table 8. Psychosocial determinants of COVID-19 vaccine booster acceptance among polish healthcare professionals and students responding to COVID-19 VBH survey, December 2021–January 2022 (n = 443).
The multivariable logistic regression of psychosocial drivers of COVID-19 VBD actual uptake was adjusted for prior infection and vaccine type. The participants who agreed with the severe infection notion had an increased adjusted odds ratio (AOR) of 4.283 (CI 95%: 2.051–8.941) times to receive COVID-19 VBD. Similarly, agreement with the symptomatic infection (AOR: 4.347; CI 95%: 2.284–8.275), community transmission (AOR: 4.179; CI 95%: 2.268–7.700), equal safety (AOR: 2.323; CI 95%: 1.024–5.273), favorable risk-benefit ratio (AOR: 3.589; CI 95%: 1.779–7.241), and self-prioritization (AOR: 6.984; CI 95%: 3.690–13.216) had an increased odd to receive COVID-19 VBD. On the other hand, agreement with the notion of variants control decreased the odds of receiving COVID-19 VBD (AOR: 0.169; CI 95%: 0.091–0.314). Ignoring the ethical dilemmas globally (AOR: 2.501; CI 95%: 1.360–4.600) and nationally (AOR: 1.819; CI 95%: 1.012–3.269) was associated with increased odds of VBD acceptance (Table 9).
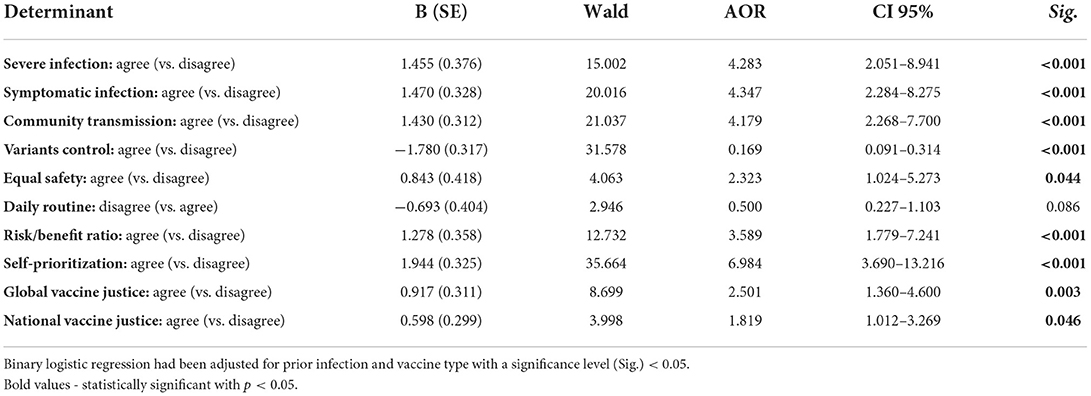
Table 9. Psychosocial determinants of COVID-19 vaccine booster uptake among polish healthcare professionals and students responding to COVID-19 VBH survey, December 2021–January 2022 (n = 443).
Vaccine acceptance is perceived essential to curb the COVID-19 pandemic. The present cross-sectional study involved Polish HCPs and MUSs to understand the drivers of VBH among this particular population subset. Our findings revealed that almost three-quarters (74.5%) of the participants favored receiving the COVID-19 VBD, while 17.6 and 7.9% indicated their rejection and uncertainty, respectively. These results are consistent with the previously published studies by Rzymski et al. (13) and Babicki and Mastalerz-Migas (14), who found that about 71 and 70% of Polish adults were interested in receiving COVID-19 VBD as soon as possible. Likewise, the studies in other high-income countries, such as the Czech Republic (71.3%), Germany (87.8%), Italy (85.7%), Japan (97.9%), Singapore (73.8%), and the United States (92.2%), exhibited high levels of COVID-19 VBD acceptance, especially among HCPs (21, 26, 31–34). On the other hand, the studies in low- and middle-income countries such as Algeria (51.6%), China (60.1%), and Jordan (44.6%) exhibited lower acceptance levels, especially among non-HCPs groups (35–37). A suggested explanation for intra- and inter-country variance in VBH levels is the respondents' health literacy level which is supposed to be higher among HCPs compared with other population subsets; therefore, the study among adult Americans by Yadete et al. (38) found lower acceptance for COVID-19 VBD (62%) than what Pal et al. (33) reported for American HCPs (92.2%). Similarly, Babicki and Mastalerz-Migas (14) found significant differences in COVID-19 VBD acceptance between Polish HCPs and non-HCPs. It is irrefutable that elements of the health belief model such as perceived susceptibility, perceived benefits, and perceived barriers contribute to this significant difference between HCPs and other groups; therefore, the goal of this study was to explore VBH drivers among HCPs, including the psychosocial benefits and barriers (39–41).
Regarding the representativeness of our sample, the latest figures published by the EU Labor Force Survey in 2021 revealed that 82.5% of Polish HCPs were females, thus justifying the female predominance of our sample (75.1%) (42). Similarly, the Organization for Economic Co-operation and Development (OECD) revealed that about 75% of Polish students enrolled in health and welfare-related programs were females, which is similar to our female students' proportion (77.6%) (43). The median age of the Polish population was 41.7 years in the year 2020, while the mean age of the sample was 31.1 ± 11.4 years, with a statistically significant difference (Sig. <0.001) between professionals (38.8 ± 10.9 years) and students (22.6 ± 2.3 years) (44). According to the Public Opinion Research Center (CBOS; Warsaw, Poland) report of 2021, about 61% of the fully vaccinated Polish citizens, i.e. those who received two primer doses, received Pfizer-BioNTech, while 22% received AstraZeneca-Oxford, 12% received Moderna, and only 3% received Janssen (45). Interestingly, Pfizer-BioNTech was the most administered vaccine among our participants who received primer doses only (60.2%), followed by AstraZeneca-Oxford (21.3%), Janssen (14.8%), and Moderna (3.7%). It is worthy to note that Pfizer-BioNTech was significantly (Sig. <0.001) more common among HCPs (89.3%) than MUSc (66.7%), while AstraZeneca-Oxford were significantly (Sig. <0.001) more common among MUSc (22.9%) than HCPs (3.7%). The decision to prioritize HCPs for receiving COVID-19 vaccines in early 2021 in Poland can explain this significant difference between HCPs and MUSs in terms of vaccines types, as the authorization of Pfizer-BioNTech was earlier and the number of its purchased doses was higher than other COVID-19 vaccine brands (46).
Around one-third (32%) of our participants had a prior COVID-19 infection, with a different severity. As per the WHO data, by April 14, 2022, 5.9 million total COVID-19 cases were reported in Poland, representing 15.5% of the total population, with a total of 54,165,921 vaccine doses have been administered by April 10, 2022 (47). This difference could be attributed to the inclusion of only HCPs and MUSc in our study. In most participants (73%), COVID-19 infections occurred before the vaccination, while around 23% of cases occurred after the second dose of the vaccine. Similarly, Klugar et al. (21) found that around 90.9% of COVID-19 infections occurred before the first dose, while only 7.3% after the second dose among Czech HCPs.
The most common reason influencing VBD acceptance among our participants was the protection of one's health (96.3%), followed by protection of family's health (82.5%), community's health (65%) and patients' or colleagues' health (56.7%). Similarly, Attia et al. (26) found that among German university staff and students, the most commonly reported promoter was the protection of one's health (95.6%), followed by the protection of the community's health (91.6%) and family's health (91.2%). In the Czech Republic, protection of family's health (83%) was the most commonly reported promoter, followed by protection of one's health (82.7%), patients' or colleagues' health (70.4%) and community's health (66.4%) (21). Even for primer doses, the HCPs' most frequently reported reason for accepting them in the United States was the protection of family's health (86.7%), followed by protection of one's health (82.9%), and community's health (68.8%) (48). In Palestine, COVID-19 vaccine acceptance was substantially higher among the nurses who were more concerned about protecting their families and patients (49). Likewise, Szmyd et al. (50) revealed that the most commonly reported COVID-19-related concern among Polish HCPs was health deterioration in family members (70.3%) which was significantly (Sig. <0.001) more common than Polish non-HCPs (55.9%). Moreover, Szmyd et al. (50) found that the physicians' family members (67.5%) were reportedly (Sig. <0.001) more infected by SARS-CoV-2 than non-HCPs' family members (54.7%).
About 13.8% of our participants disagreed with the statement that COVID-19 VBD will be as safe as the primer doses, with a considerable difference between those who were triple-vaccinated (6.2%) and non-tripled vaccinated (30.9%); thus, indicating the role of post-vaccination safety and side effects in determining the attitudes toward COVID-19 VBD. Al-Qerem et al. (37) found that fear of severe side effects following COVID-19 VBD (34.1%) and the incapacity to tolerate primer doses side effects (24.6%) were the most commonly reported reasons for COVID-19 VBD rejection among Jordanian adults. Likewise, post-vaccination side effects were main reasons for COVID-19 VBH in Algeria (35). Heretofore all authorized COVID-19 vaccines have been proven safe since phase II/III trials conducted by manufacturers (51). Therefore, the continuation of phase IV studies conducted by independent institutions and regulators is vital to protect the public confidence in vaccines (51–55).
The participants who had been previously infected by SARS-CoV-2 were significantly more inclined to reject the VBD, whereas the participants who had been previously vaccinated against SARS-CoV-2 were more willing to accept the VBD. A Lebanese web-based cross-sectional study using the health belief model also supported the notion that HCPs who had been previously diagnosed with COVID-19 were significantly associated with a lower level of vaccine acceptance (56). The misconception of natural immunity triggered by prior infection can explain this finding, and it had been one of the key drivers for vaccine hesitancy proposed by the WHO-SAGE (56, 57).
The applied comprehensive multivariable logistic regression model for the psychosocial drivers of COVID-19 VBD-related acceptance and uptake revealed that the participants who agreed with severe infection, symptomatic infection, and community transmission notions had higher odds of accepting. The effectiveness of vaccines, especially VBD, was a primary promoter for COVID-19 VBD-related acceptance among Algerian adults, American adults, German university students and staff, and Italian university students (26, 34, 35, 38). Using the ministry of health database, a nationwide population-based study from Israel found that COVID-19 VBD reduced the risk of developing COVID-19 infection and severe illness among VBD recipients (58). In our study, effectiveness against the emerging variants was a prominent determinant for VBD-related acceptance and uptake, consistent with what was found earlier among Czech HCPs and German university students and staff (21, 26).
The risk-benefit profile of VBD impacted COVID-19 booster dose acceptance because a positive association between the COVID-19 VBD acceptance and perceived susceptibility, as well as benefit. Public health campaigns are expected to highlight the postulated benefits of vaccines, especially in terms of effectiveness against symptomatic and severe infection, along with the expected harms of unvaccinated population (26, 59).
The present study is the first to particularly target HCPs and MUSs in Poland. Participants' identity was kept confidential and anonymous to control Hawthorne's effect. The crucial findings may help promote the booster dose uptake worldwide.
The non-random sampling technique used to recruite participants of this study may partially limited the representativeness of obtained results. HCPs and MUSc are much more aware than the general population in terms of the risk-benefit profile of vaccines, and they are more prone to show high vaccine uptake and acceptance; Hence, this study's findings should not be directly applied to the general population. The non-random sampling approach used might be linked with selection bias; whereas, the sample was relatively representative considering metropolitan areas of vast majority of participants. Some professional groups were disproportionally represented in our sample, as a few of their members participated in this study; therefore, future studies on HCPs should aim for representing professional groups proportionately. In addition, online surveys could contribute to measurement bias as fraction of participants tend not to fully respond to the all questionnaire items. Our findings will support a rationale for efficient dissemination of booster doses of COVID-19 vaccines.
A high vaccine acceptance among HCPs and MUSc in Poland indicate the positive attitude of these groups toward mass inoculation. The previous infection by SARS-CoV-2 significantly increased a risk of VBD hesitancy. Protection from severe infection, community transmission, good safety profile, and favorable risk-benefit ratio were the significant determinants of the COVID-19 VBD acceptance and uptake. The enhanced public health campaigns are designed to highlight the postulated benefits of vaccines and the expected harms of skipping VBD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the Medical University of Silesia. The patients/participants provided their written informed consent to participate in this study.
AR: conceptualization, methodology, and formal analysis. AD: software and funding acquisition. JI and AD: validation. AD, JI, and MK: investigation. AR, JI, and SH: writing—original draft preparation. AD, MT, RW, and RK: writing—review and editing. AR and AD: supervision and project administration. All authors have read and agreed to the published version of the manuscript.
The work of AR was supported by Masaryk University grants numbers MUNI/IGA/1104/2021 and MUNI/A/1402/2021. JI was a participant of the STER Internationalization of Doctoral Schools Program from NAWA Polish National Agency for Academic Exchange No. PPI/STE/2020/1/00014/DEC/02. The work of SH was supported by Operational Programme Research, Development and Education—Project, Postdoc2MUNI (No. CZ.02.2.69/0.0/0.0/18_053/0016952). The work of AD was supported by grant of Medical University of Silesia: PCN-1-203/K/1/I and PCN-176/K/0/I.
This work is dedicated to the more than 116,000 fatalities and their families who have fallen victim to COVID-19 in Poland.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.938067/full#supplementary-material
1. Kadkhoda K. Herd immunity to COVID-19: alluring and elusive. Am J Clin Pathol. (2021) 155:471–2. doi: 10.1093/ajcp/aqaa272
2. Randolph HE, Barreiro LB. Herd immunity: understanding COVID-19. Immunity. (2020) 52:737–41. doi: 10.1016/j.immuni.2020.04.012
3. Ritchie H, Edouard M, Lucas R-G, Cameron A, Charlie G, Esteban O-O, et al. Coronavirus pandemic (COVID-19). Our World Data. (2022). Available online at: https://ourworldindata.org/coronavirus (accessed April 27, 2022).
4. Stay Up to Date With Your COVID-19 Vaccines. Centers Disease Control and Prevention (2022). Available online at: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/stay-up-to-date.html (accessed April 27, 2022).
5. Levin EG, Lustig Y, Cohen C, Fluss R, Indenbaum V, Amit S, et al. Waning immune humoral response to BNT162b2 COVID-19 vaccine over 6 months. N Engl J Med. (2021) 385:e84. doi: 10.1056/NEJMoa2114583
6. Chemaitelly H, Tang P, Hasan MR, AlMukdad S, Yassine HM, Benslimane FM, et al. Waning of BNT162b2 vaccine protection against SARS-CoV-2 infection in Qatar. N Engl J Med. (2021) 385:e83. doi: 10.1056/NEJMoa2114114
7. Aleem A, Akbar Samad AB, Slenker AK. Emerging Variants of SARS-CoV-2 and Novel Therapeutics Against Coronavirus (COVID-19). Treasure Island, FL: StatPearls Publishing.
8. Chenchula S, Karunakaran P, Sharma S, Chavan M. Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: a systematic review. J Med Virol. (2022) 94:2969–76. doi: 10.1002/jmv.27697
9. Zdrowia M,. Komunikat nr 12 Ministra Zdrowia w sprawie szczepień przeciw COVID-19 dawka przypominajaca oraz dawka dodatkowa uzupełniajaca schemat podstawowy. Serwis Rzeczyposp Pol (2021). Available online at: https://www.gov.pl/web/zdrowie/komunikat-nr-12-ministra-zdrowia-w-sprawie-szczepien-przeciw-covid-19-dawka-przypominajaca-oraz-dawka-dodatkowa-uzupelniajaca-schemat-podstawowy (accessed April 27, 2022).
10. The Chancellery of the Prime Minister. Prime Minister After Receiving a Booster Dose of the Vaccination: ”Getting vaccinated is the Best Gift We Can Give to Ourselves and Our Loved ones." Website Repub Pol (2021). Available online at: https://www.gov.pl/web/primeminister/prime-minister-after-receiving-a-booster-dose-of-the-vaccination-getting-vaccinated-is-the-best-gift-we-can-give-to-ourselves-and-our-loved-ones (accessed April 27, 2022).
11. Ministerstwo, Zdrowia,. Druga dawka przypominajaca dla osób 80+. Serwis Rzeczyposp Pol. Available online at: https://www.gov.pl/web/zdrowie/druga-dawka-przypominajaca-dla-osob-80 (accessed April 27, 2022).
12. Szczepienie przeciwko COVID-19. Raport szczepień przeciwko COVID-19. Serwis Rzeczyposp Pol. Available online at: https://www.gov.pl/web/szczepimysie/raport-szczepien-przeciwko-covid-19 (accessed April 27, 2022).
13. Rzymski P, Poniedziałek B, Fal A. Willingness to receive the booster COVID-19 vaccine dose in Poland. Vaccines. (2021) 9:1286. doi: 10.3390/vaccines9111286
14. Babicki M, Mastalerz-Migas A. Attitudes of poles towards the COVID-19 vaccine booster dose: an online survey in Poland. Vaccines. (2022) 10:68. doi: 10.3390/vaccines10010068
15. MacDonald NE, Eskola J, Liang X, Chaudhuri M, Dube E, Gellin B, et al. Vaccine hesitancy: definition, scope and determinants. Vaccine. (2015) 33:4161–4. doi: 10.1016/j.vaccine.2015.04.036
16. Strategic Advisory Group of Experts on Immunization (SAGE). Report of the Sage Working Group on Vaccine Hesitancy. (2014). Available online at: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed October 1, 2021).
17. Rosselli R, Martini M, Bragazzi NL. The old and the new: vaccine hesitancy in the era of the Web 2.0. Challenges and opportunities. J Prev Med Hyg. (2016) 57:E47.
18. Riad A, Huang Y, Abdulqader H, Morgado M, Domnori S, Koščík M, et al. Universal predictors of dental students' attitudes towards COVID-19 vaccination: machine learning-based approach. Vaccines. (2021) 9:1158. doi: 10.3390/vaccines9101158
19. Riad A, Abdulqader H, Morgado M, Domnori S, Koščík M, Mendes JJ, et al. Global prevalence and drivers of dental students' COVID-19 vaccine hesitancy. Vaccines. (2021) 9:566. doi: 10.3390/vaccines9060566
20. Oberg EB, Frank E. Physicians' health practices strongly influence patient health practices. J R Coll Physicians Edinb. (2009) 39:290–1. doi: 10.4997/JRCPE.2009.422
21. Klugar M, Riad A, Mohanan L, Pokorná A. COVID-19 vaccine booster hesitancy (VBH) of healthcare workers in Czechia: national cross-sectional study. Vaccines. (2021) 9:1437. doi: 10.3390/vaccines9121437
22. Harvard Humanitarian Initiative,. Welcome to KoBoToolbox. KoBoToolbox Doc (2022). Available online at: https://support.kobotoolbox.org/welcome.html (accessed January 4, 2022).
23. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. UroToday Int J. (2007) 335:806–8. doi: 10.1136/bmj.39335.541782.AD
24. English Proficiency Index 2021. Education First (2021). Available online at: https://www.ef.com/wwen/epi/ (accessed January 12, 2022).
25. Centers for Disease Control Prevention (CDC). Population Survey or Descriptive Study. StatCalc | User Guide. Available online at: https://www.cdc.gov/epiinfo/user-guide/statcalc/samplesize.html (accessed December 1, 2021).
26. Attia S, Mausbach K, Klugar M, Howaldt H-P, Riad A. Prevalence and drivers of COVID-19 vaccine booster hesitancy (VBH) among German University Students and Employees. Front Public Heal. (2012) 10:846861. doi: 10.3389/fpubh.2022.846861
27. WMA. World Medical Association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310:2191–4. doi: 10.1001/jama.2013.281053
28. Proton Technologies AG,. General Data Protection Regulation (GDPR) Compliance Guidelines. Horiz 2020 - Proj REP-791727-1 (2020). Available online at: https://gdpr.eu/ (accessed May 1, 2020).
29. SPSS Inc,. IBM SPSS Statistics 28. (2021). Available online at: https://www.ibm.com/support/pages/ibm-spss-statistics-28-documentation (accessed March 14, 2021).
30. The jamovi project. jamovi (Version 1.6) [Computer Software]. (2021). Available online at: https://www.jamovi.org (accessed February 11, 2022).
31. Massimi A, Voglino G, Gualano MR, Chee Koh SW, Tan HM, Lee WH, et al. COVID-19 vaccine booster hesitancy among healthcare workers: a retrospective observational study in Singapore. Vaccines. (2022) 10:464. doi: 10.3390/vaccines10030464
32. Batra K, Yoshida M, Kobashi Y, Kawamura T, Shimazu Y, Nishikawa Y, et al. Factors associated with COVID-19 vaccine booster hesitancy: a retrospective cohort study, Fukushima vaccination community survey. Vaccines. (2022) 10:515. doi: 10.3390/vaccines10040515
33. Pal S, Shekhar R, Kottewar S, Upadhyay S, Singh M, Pathak D, et al. COVID-19 vaccine hesitancy and attitude toward booster doses among US healthcare workers. Vaccines. (2021) 9:1358. doi: 10.3390/vaccines9111358
34. Folcarelli L, Del Giudice GM, Corea F, Angelillo IF. Intention to receive the COVID-19 vaccine booster dose in a university community in Italy. Vaccines. (2022) 10:146. doi: 10.3390/vaccines10020146
35. Lounis M, Bencherit D, Rais MA, Riad A. COVID-19 vaccine booster hesitancy (VBH) and its drivers in algeria: national cross-sectional survey-based study. Vaccines. (2022) 10:621. doi: 10.3390/vaccines10040621
36. Hu T, Li L, Lin C, Yang Z, Chow C, Lu Z, et al. An analysis of the willingness to the COVID-19 vaccine booster shots among urban employees: evidence from a megacity H in Eastern China. Int J Environ Res Public Health. (2022) 19:2300. doi: 10.3390/ijerph19042300
37. Al-Qerem W, Al Bawab AQ, Hammad A, Ling J, Alasmari F. Willingness of the Jordanian population to receive a COVID-19 booster dose: a cross-sectional study. Vaccines. (2022) 10:410. doi: 10.3390/vaccines10030410
38. Yadete T, Batra K, Netski DM, Antonio S, Patros MJ, Bester JC. Assessing acceptability of COVID-19 vaccine booster dose among adult Americans: a cross-sectional study. Vaccines. (2021) 9:1424. doi: 10.3390/vaccines9121424
39. Wong MCS, Wong ELY, Huang J, Cheung AWL, Law K, Chong MKC, et al. Acceptance of the COVID-19 vaccine based on the health belief model: a population-based survey in Hong Kong. Vaccine. (2021) 39:1148–56. doi: 10.1016/j.vaccine.2020.12.083
40. Wong LP, Alias H, Wong PF, Lee HY, AbuBakar S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum Vaccines Immunother. (2020) 16:2204–14. doi: 10.1080/21645515.2020.1790279
41. Shmueli L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health. (2021) 21:804. doi: 10.1186/s12889-021-10816-7
42. Eurostat. Majority of health jobs held by women. Products Eurostat News. (2021). Available online at: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/edn-20210308-1 (accessed May 2, 2022).
43. Organisation for Economic Co-operation and Development (OECD). Young women are better educated than young men, but gender gaps in labour market outcomes persist. Closing Gender Gap. Available online at: https://www.oecd.org/gender/Closing the Gender Gap - Poland FINAL.pdf (accessed May 2, 2022).
44. Statista. Poland - average age of the population 1950-2050. Economic and Politics. Available online at: https://www.statista.com/statistics/375688/average-age-of-the-population-in-poland/ (accessed May 2, 2022).
45. Małgorzata Omyła-Rudzka,. Efekty uboczne szczepień przeciw COVID-19 - doświadczenia respondentów. Public Opinion Research Centre (2021). Available online at: https://www.cbos.pl/SPISKOM.POL/2021/K_081_21.PDF (accessed May 2, 2022).
46. Dziedzic A, Riad A, Attia S, Klugar M, Tanasiewicz M. Self-reported adverse events of COVID-19 vaccines in polish healthcare workers and medical students. Cross-sectional study and pooled analysis of CoVaST project results in Central Europe. J Clin Med. (2021) 10:5338. doi: 10.3390/jcm10225338
47. World Health Organization (WHO). WHO Coronavirus Dashboard With Vaccine Data. Available online at: https://covid19.who.int/region/euro/country/pl (accessed May 2, 2022).
48. Kuter BJ, Browne S, Momplaisir FM, Feemster KA, Shen AK, Green-McKenzie J, et al. Perspectives on the receipt of a COVID-19 vaccine: a survey of employees in two large hospitals in Philadelphia. Vaccine. (2021) 39:1693–700. doi: 10.1016/j.vaccine.2021.02.029
49. Rabi R, Maraqa B, Nazzal Z, Zink T. Factors affecting nurses' intention to accept the COVID-19 vaccine: a cross-sectional study. Public Health Nurs. (2021) 38:781–8. doi: 10.1111/phn.12907
50. Szmyd B, Karuga FF, Bartoszek A, Staniecka K, Siwecka N, Bartoszek A, et al. Attitude and behaviors towards SARS-CoV-2 vaccination among healthcare workers: a cross-sectional study from Poland. Vaccines. (2021) 9:218. doi: 10.3390/vaccines9030218
51. Riad A, Schünemann H, Attia S, Peričić TP, Žuljević MF, Jürisson M, et al. COVID-19 vaccines safety tracking (CoVaST): protocol of a multi-center prospective cohort study for active surveillance of COVID-19 vaccines' side effects. Int J Environ Res Public Heal. (2021) 18:7859. doi: 10.3390/ijerph18157859
52. Lounis M, Rais MA, Bencherit D, Aouissi HA, Oudjedi A, Klugarová J, et al. Side effects of COVID-19 inactivated virus versus adenoviral vector vaccines: experience of Algerian healthcare workers. Front Public Heal. (2022) 10:896343. doi: 10.3389/fpubh.2022.896343
53. Riad A, Hocková B, Kantorová L, Slávik R, Spurná L, Stebel A, et al. Side effects of mRNA-based COVID-19 vaccine: nationwide phase IV study among healthcare workers in Slovakia. Pharmaceuticals. (2021) 14:873. doi: 10.3390/ph14090873
54. Klugar M, Riad A, Mekhemar M, Conrad J, Buchbender M, Howaldt H-P, et al. Side effects of mRNA-based and viral vector-based COVID-19 vaccines among German Healthcare Workers. Biology. (2021) 10:752. doi: 10.3390/biology10080752
55. Riad A, Sagiroglu D, Üstün B, Pokorná A, Klugarová J, Attia S, Klugar M. Prevalence and risk factors of CoronaVac side effects: an independent cross-sectional study among healthcare workers in Turkey. J Clin Med. (2021) 10:2629. doi: 10.3390/jcm10122629
56. Youssef D, Abou-Abbas L, Berry A, Youssef J, Hassan H. Determinants of acceptance of Coronavirus disease-2019 (COVID-19) vaccine among Lebanese health care workers using health belief model. PLoS ONE. (2022) 17:e0264128. doi: 10.1371/journal.pone.0264128
57. Larson HJ, Jarrett C, Schulz WS, Chaudhuri M, Zhou Y, Dube E, et al. Measuring vaccine hesitancy: the development of a survey tool. Vaccine. (2015) 33:4165–75. doi: 10.1016/j.vaccine.2015.04.037
58. Bar-On Bar-On YM, Goldberg Y, Mandel M, Bodenheimer O, Freedman L, Kalkstein N, et al. Protection of BNT162b2 vaccine booster against COVID-19 in Israel. N Engl J Med. (2021) 385:1393–400. doi: 10.1056/NEJMoa2114255
Keywords: cross-sectional studies, COVID-19 vaccines, decision making, healthcare professionals, vaccination hesitancy, Poland
Citation: Dziedzic A, Issa J, Hussain S, Tanasiewicz M, Wojtyczka R, Kubina R, Konwinska MD and Riad A (2022) COVID-19 vaccine booster hesitancy (VBH) of healthcare professionals and students in Poland: Cross-sectional survey-based study. Front. Public Health 10:938067. doi: 10.3389/fpubh.2022.938067
Received: 06 May 2022; Accepted: 04 July 2022;
Published: 25 July 2022.
Edited by:
Francesca Licata, University Magna Graecia of Catanzaro, ItalyReviewed by:
Atalay Mulu Fentie, Addis Ababa University, EthiopiaCopyright © 2022 Dziedzic, Issa, Hussain, Tanasiewicz, Wojtyczka, Kubina, Konwinska and Riad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abanoub Riad, YWJhbm91Yi5yaWFkQG1lZC5tdW5pLmN6
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.