 Aduragbemi Banke-Thomas1,2*†Peter M. Macharia3,4†Prestige Tatenda Makanga5Lenka Beňová6Kerry L. M. Wong7Uchenna Gwacham-Anisiobi8Jia Wang9Tope Olubodun10Olakunmi Ogunyemi11Bosede B. Afolabi2,12Bassey Ebenso13Ibukun-Oluwa Omolade Abejirinde14,15
Aduragbemi Banke-Thomas1,2*†Peter M. Macharia3,4†Prestige Tatenda Makanga5Lenka Beňová6Kerry L. M. Wong7Uchenna Gwacham-Anisiobi8Jia Wang9Tope Olubodun10Olakunmi Ogunyemi11Bosede B. Afolabi2,12Bassey Ebenso13Ibukun-Oluwa Omolade Abejirinde14,15- 1School of Human Sciences, University of Greenwich, London, United Kingdom
- 2Maternal and Reproductive Health Research Collective, Lagos, Nigeria
- 3Population Health Unit, Kenya Medical Research Institute-Wellcome Trust Research Programme, Nairobi, Kenya
- 4Centre for Health Informatics, Computing, and Statistics, Lancaster Medical School, Lancaster University, Lancaster, United Kingdom
- 5Surveying and Geomatics Department, Faculty of Science and Technology, Midlands State University, Gweru, Zimbabwe
- 6Department of Public Health, Institute of Tropical Medicine, Antwerp, Belgium
- 7Department of Infectious Disease Epidemiology, London School of Hygiene and Tropical Medicine, London, United Kingdom
- 8Nuffield Department of Population Health, University of Oxford, Oxford, United Kingdom
- 9School of Computing and Mathematical Sciences, University of Greenwich, London, United Kingdom
- 10Department of Community Medicine and Primary Care, Federal Medical Centre Abeokuta, Abeokuta, Nigeria
- 11Lagos State Ministry of Health, Lagos, Nigeria
- 12Department of Obstetrics and Gynaecology, College of Medicine, University of Lagos, Lagos, Nigeria
- 13Leeds Institute of Health Sciences, University of Leeds, Leeds, United Kingdom
- 14Women's College Hospital Institute for Health System Solutions and Virtual Care, Toronto, ON, Canada
- 15Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada
Maternal and perinatal mortality remain huge challenges globally, particularly in low- and middle-income countries (LMICs) where >98% of these deaths occur. Emergency obstetric care (EmOC) provided by skilled health personnel is an evidence-based package of interventions effective in reducing these deaths associated with pregnancy and childbirth. Until recently, pregnant women residing in urban areas have been considered to have good access to care, including EmOC. However, emerging evidence shows that due to rapid urbanization, this so called “urban advantage” is shrinking and in some LMIC settings, it is almost non-existent. This poses a complex challenge for structuring an effective health service delivery system, which tend to have poor spatial planning especially in LMIC settings. To optimize access to EmOC and ultimately reduce preventable maternal deaths within the context of urbanization, it is imperative to accurately locate areas and population groups that are geographically marginalized. Underpinning such assessments is accurately estimating travel time to health facilities that provide EmOC. In this perspective, we discuss strengths and weaknesses of approaches commonly used to estimate travel times to EmOC in LMICs, broadly grouped as reported and modeled approaches, while contextualizing our discussion in urban areas. We then introduce the novel OnTIME project, which seeks to address some of the key limitations in these commonly used approaches by leveraging big data. The perspective concludes with a discussion on anticipated outcomes and potential policy applications of the OnTIME project.
Introduction
Maternal mortality remains a huge challenge in many countries globally, with its burden substantially higher in low- and middle-income countries (LMICs) where 99% of maternal deaths occur (1). Despite a 38% reduction in global maternal mortality between 2000 and 2017, ~295,000 maternal deaths occur annually from preventable causes related to pregnancy and childbirth (1). Similarly, 98% of the three million perinatal deaths reported globally occurs in LMICs (2). These deaths are mostly associated with complications of pregnancy and childbirth, including pre-eclampsia/eclampsia, hemorrhage, sepsis, and abortion (3). Presently, the consensus strategy for minimizing pregnancy and childbirth related deaths is mainly focused on increasing access to prompt emergency obstetric care (EmOC) provided by skilled health personnel (4, 5). EmOC is a package of nine clinical and surgical evidence-based interventions including parenteral antibiotics, uterotonic drugs, parenteral anticonvulsants, manual removal of placenta, removal of retained products of conception, assisted vaginal delivery, neonatal resuscitation, blood transfusion and cesarean section (5). EmOC has been shown to reduce maternal deaths amongst women who reach health facilities by 15–50% and intrapartum stillbirths by 45–75% (6).
In emergency situations, pregnant women with obstetric complications need to travel to health facilities with capacity to provide EmOC. Delays in reaching such health facilities significantly affects pregnancy outcomes for mothers and newborns (7–10). Many of the health facilities that pregnant women with obstetric emergencies require for care are hospitals, classed as secondary and tertiary level health facilities, which are often located in urban settings. Women living in urban areas have been assumed to have better physical access EmOC compared to their rural counterparts due to relatively shorter travel distances to health facilities (11). However, emerging evidence shows that this so called “urban advantage” is shrinking and, in some LMIC settings, almost non-existent partly because while travel distances might be shorter, travel time can get longer (9, 12, 13). In urban LMIC settings, typically characterized by poor spatial planning, haphazardly built environments, growing informal settlements, poor road infrastructure, and extreme traffic congestion prolong travel time, delay care-seeking, and aggravate the risk of long-term morbidity and mortality for women and their babies. When these issues are considered against the backdrop of rapid urbanization in which 70% of the world's population is expected to live in urban areas by 2050, with nearly 90% of the projected additional 2.5 billion urban residents concentrated in Africa and Asia alone (14), urgent action is needed for service planning.
To optimize access to EmOC and ultimately reduce preventable maternal deaths within the context of urbanization, it is imperative to accurately identify areas and population groups that are physically marginalized in urban areas. Identification of these areas of geographical inequities will provide a useful starting point to engage in dialogues with policymakers on urban health and planning, as well as to inform multisectoral policies and action. Underpinning such assessments of geographical inequities are accurate estimates of travel time to EmOC facilities. In this perspective paper, we discuss strengths and weaknesses of the commonly used approaches in estimating travel time to EmOC services in LMICs, contextualizing our discussion in urban areas. We then introduce a novel initiative called the OnTIME project, which is attempting to address some of the key limitations in the commonly used approaches in LMICs by leveraging big data. The perspective concludes with a discussion on anticipated outcomes and potential policy applications of the project.
Common methods for estimating travel time to EmOC in LMICs
Broadly, methods that have been used for estimating travel time to EmOC in LMICs can be grouped into reported and modeled approaches. Reported approaches entail asking health workers or women to estimate their travel times to health facilities. Some concerns with this approach have been raised. First, since health workers themselves did not make the journeys, their estimates are at best “guestimates” of the journeys that women might have undertaken to reach the health facility. In cases where women are asked to report their travel time, issues of recall bias have been highlighted by researchers, especially as they traveled in an emergency (15, 16).
On the other hand, modeled approaches are commonly used to estimate travel time to health facilities in LMICs (17). They range from simple approaches such as Euclidean model, to sophisticated methods that include network analysis, cost distance analysis and gravity models as summarized in Figure 1. These methods have been detailed by Ouma et al. (17). Briefly, Euclidean distances are the simplest to compute and assume straight line of travel from residence to EmOC locations, however, they ignore the influence of transport variables such as travel barriers, road network and slope. Gravity models combines availability and accessibility across defined spatial units to overcome this limitation of Euclidean approaches. However, the method may suffer from the modifiable areal unit problem, is dependent on the availability of population at very fine geographic units and service provider capacity data which are not always available in resource limited settings. Network analysis entails computing travel time along existing travel routes to a specified health facility. The method relies on a well-mapped transportation network and settlements, assumes travel can only occur along the roads and it is computationally intensive. On the other hand, cost distance analysis relies on travel speeds across land covers, road network and elevation, to define the least time needed to get to a health facility from residences. A common problem underlying all these approaches is reliance of empirical data (which is rarely available) to parametrise a model that represents the journey between where a need is triggered and the location of the service provider (18).
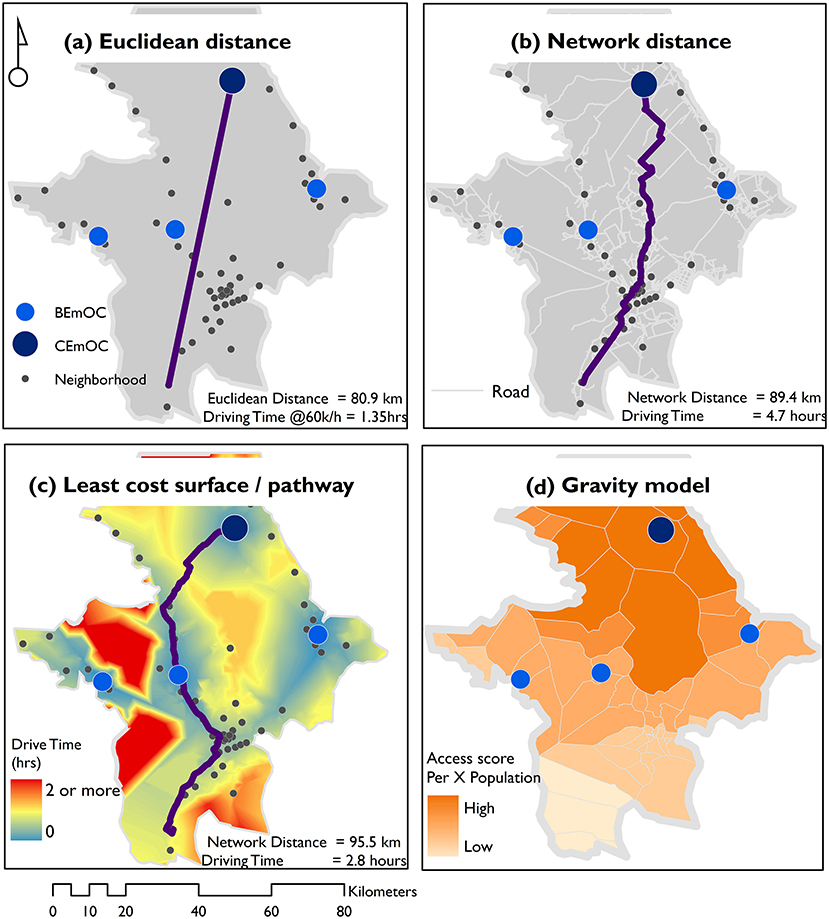
Figure 1. Common methods for estimating travel time to health facilities in LMICs. An illustration of common approaches used to compute geographic access to health service providers in LMICs including (a), Euclidean distance, (b) network distance, (c) least cost path distance, and (d) gravity models.
Despite the widespread application of modeled approaches, they have a range of known limitations, some of which are accentuated by the intrinsic dynamics and variability of conditions that typify urban contexts (19). One fundamental limitation is that it is hard to create accurate models that replicate actual journeys. This is often due to inadequate data on where the journey was initiated, the health facility visited, the route used, its condition at the time of travel (traffic, weather, accidents), the mode(s) of transport and the speed of travel. As a result, empirical models tend to make assumptions about travel speeds and mode of transport, rarely accounting for the dynamism of traffic conditions, weather conditions, and unforeseen travel circumstances such as waiting time, police checkpoints, or impassability of roads. As regards traffic in particular, urbanization and the expansion of the middle class in urban LMIC areas have resulted in a rapid increase in vehicular traffic, leading to significant traffic congestion (20). For example, commuters in Lagos, the largest megacity in sub-Saharan Africa spend an average of 30 h a week (equivalent to 75% of a 40-h working week) in traffic, with some taking up to 3 h to travel 10 km (21). In Asia, three megacities of India—Bengaluru, Mumbai, and New Delhi—are part of the top 10 highly ranked cities with populations over eight million and with the highest levels of traffic congestion across the globe (22). Previous research which compared modeled travel time estimates with those collected from replication of travel journeys made by pregnant women in Lagos showed that while the median replicated drive time was 50–52 min, mean errors of >45 min were reported for the cost-friction surface approach and Open Street Route Mapping (23). Ignoring variability in traffic conditions results in as much as three-fold overestimation of geographic coverage and masks intra-urban inequities in accessibility to emergency care (19). Another limitation of modeled approaches, as they have been commonly used, relates to establishing the travel destination. Majority of the modeled approaches estimate travel time to the nearest health facility. Yet, it is well established that even in emergencies, pregnant women may bypass the nearest health facility for a myriad of reasons including trust, cost, and the real or perceived quality of care. Women might also be referred from one facility to others. When this occurs, their journeys are typically a lot more complex, harder to model and does not always follow the path of the least resistance a common approach to modeled approaches (24–27). These limitations can result in underestimated time to access care, with significant implications for underserved populations that require targeted policies and action (28).
The constraints reported by researchers regarding pushing the frontier to reflect closer-to-reality travel time estimates relate to capacity to accurately parametrise a model that mimics the dynamics of the journey between the residence and service provider (29, 30). Data required for improved model parameterization include residential location of service users, location of the utilized facility providing EmOC, route used, mode of transport, traffic and weather variables, travel speed and transport barriers, among other travel dynamics (31). However, collecting such data is time-consuming, expensive, and probably impractical especially in low resource settings where there are many competing needs for resources. Also, the dynamics change dramatically, so data from last year or even last month may become less useful for understanding travel of mothers in an emergency. To move forward, such data needs to be real-time or at least close to real time.
Leveraging big data for EmOC access
We have previously shown that Google Maps provides closer to reality estimates relative to modeled estimates based on travel time derived from replicated journeys of women seeking EmOC services (23). Consequently, we conducted a study using Google Maps to assess travel time of pregnant women to EmOC in Lagos, Nigeria—the most populated metropolis in sub-Saharan Africa (32). Our state-wide application of this method clearly showed areas of geographical inequity, one of which aligned with a gap in EmOC access that the Lagos state government addressed during the year of the study and others matched areas requiring attention to improve EmOC access (32, 33). Post-study dissemination efforts confirmed the high value that policymakers place on the insights generated using closer-to-reality estimates (34). Building on this success, the “On Tackling In-transit delays for Mothers in Emergency” (OnTIME) project is a novel initiative bringing together researchers, policy makers and the digital technology sector to leverage big data to generate closer-to-reality assessments of travel time to EmOC services in urban LMIC settings (www.ontimeconsortium.org/).
To achieve the project's goal, data on travel time and functionality of public and private hospitals in selected LMIC urban settings will be utilized. The travel time data will be computed using Google Maps Platform Directions API, the same one that helps calculate directions in Google Maps. Google Navigation uses real-time traffic conditions along with historical traffic patterns and road network data to predict accurate travel times. Therefore, the role of traffic congestion, time of the day, day of week, weather variation, and other unpredictable events will be indirectly embedded. Data on facility functionality will be collected from existing health facility registries in LMIC countries and verified by the OnTIME research team. Putting both datasets together will help characterize travel time to facilities providing EmOC. Furthermore, data on mode of transport commonly used by pregnant women in the country and in urban areas under consideration will be sourced to further refine travel time estimates. Finally, recognizing that obstetric referral patterns vary (35), the project will provide estimates accounting for different pathways in urban LMIC settings, including through referral. The plan is to then feed all the data into a digital dashboard with different visualization and scenario building options that can guide decisions around service delivery modalities, infrastructural and transportation priorities, and locations of future health facilities. It will also aid a more accurate estimation of the gaps between demand and supply of EmOC at a population level. Such evidence will be invaluable for service planning and policymaking, as closer-to-reality travel times reduce the number of generalizations and assumptions typically applied in empirical models in urban settings.
The pilot phase of the OnTIME project will focus on urban settings with an estimated population greater than one million in Nigeria. Outputs of this phase will be used to further refine the approach which could then be applied during subsequent project phases when the focus expands to other urban LMIC conurbations.
Discussion
Urbanization poses a complex challenge for structuring an effective health service delivery system that is inclusive and responsive, especially in LMICs. It is an even greater challenge when consideration is given to the sprawling slum areas in many LMICs (36). Many of those living in slums are poor, who tend to live in unsafe conditions and have limited access to personal means of transport. This is driving widespread intra-urban inequities placing the urban poor at higher risks of poor outcomes even though health services are available and seemingly within reach (12, 37).
Clearly the roadmap toward equitable and responsive urban health service planning needs to rely on closer-to-reality travel time data that is available and valid—a task that the OnTIME Consortium is taking on, one urban LMIC setting at a time. The activities of the consortium are geared toward the development of a co-produced, context-specific, and action-oriented dashboard to support evidence-based decision-making and to guide targeted investments needed to support the advancement of robust urban health systems. Our expectation is that this dashboard and the underlying dataset will contribute to improving access to care and ultimately in reducing urban maternal and perinatal mortality in LMICs. The more accurate methods for estimating time to travel are, the better-informed urban planners and policy makers will become.
The OnTIME project has potential to inform decision-making for service planning on a granular, grassroot and closer-to-the-community basis is clear, as it will provide the evidence base needed for strategic response to EmOC service provision (38). To deal with issue of bypassing, the project also brings in the important element of choice that women have in deciding which hospital they go to in an emergency by assessing the first, second and third nearest public and private options available to the pregnant woman, since it is widely recognized that several non-travel-related factors influence the choice of where women seek EmOC (24, 39). Of course, a woman may still choose to go farther away from home for care in an emergency, but our approach of including options is a step change in the field of accessibility assessments. Our approach allows for prospective assessments which will be useful for service planning. As has already been established, our approach also allows for retrospective assessments when actual residence location and attribute data on the hospital that was utilized are available (32).
The promise of the OnTIME project in tackling in-transit delays for mothers in emergencies goes beyond its application for the supply-side focus. There is also a huge potential for the OnTIME approach to serve demand-side innovation which can inform health-seeking and choice of facility for EmOC amongst pregnant women. This will be very important as there is evidence that travel time strongly influence hospital choice, even in urban areas where alternatives are widely available (40). Despite the promise, some key gaps will still need to be addressed in future. Health care access is multi-dimensional and entails availability (physical availability), acceptability (perception of quality), accommodation (structures to support care access), affordability (cost), and accessibility (geographical accessibility) (41). While the precise nature of influences of acceptability, accommodation, affordability, and availability on EmOC access will need to be incorporated in future efforts, the OnTIME consortium is currently focused on accessibility. Capturing closer-to-reality data on EmOC accessibility constitutes the very next frontier for policy and research in EmOC access in urban LMIC settings, as the other access dimensions can only be properly understood if accessibility is reflective of reality. The OnTIME project will generate this evidence and in so doing, this initiative aims to advance the urban health agenda for equitable and responsive health systems and contribute to global efforts to reduce maternal and perinatal mortality (42).
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
AB-T, PMM, PTM, LB, and IOA conceptualized the study and prepared the first draft of the manuscript. AB-T, PMM, PTM, LB, KW, UG-A, and IOA conducted the literature review that informed the study. AB-T, PMM, PTM, KW, UG-A, JW, and IOA synthesized the retrieved data. All authors were involved in the preparation of subsequent drafts and approved the final version.
Funding
The OnTIME project led by AB-T was funded by Google. AB-T and BA were funded by Bill and Melinda Gates Foundation (Investment ID: INV-032911). PMM was supported by Newton International Fellowship (Number NIF/R1/201418) of the Royal Society and acknowledges the support of the Wellcome Trust to the Kenya Major Overseas Programme (Number 203077). LB was funded in part by the Research Foundation–Flanders (FWO) as part of her Senior Postdoctoral Fellowship.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. WHO UNICEF UNFPA World Bank Group UNDP. Trends in Maternal Mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva: World Health Organization (2019). p. 1–119. Available online at: https://www.unfpa.org/sites/default/files/pub-pdf/Maternal_mortality_report.pdf 2 (accessed July 15, 2022).
2. UNICEF WHO World Bank UNPD. A Neglected Tragedy: The Global Burden of Stillbirths. New York, NY: United Nations Children's Fund (2020). p. 1–90.
3. GBD 2015 Maternal Mortality Collaborators. Global, regional, and national levels of maternal mortality, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. (2016) 388:1775–812. doi: 10.1016/S0140-6736(16)31470-2
4. United Nations. Sustainable Development Goals: 17 Goals to Transform Our World. Sustainable Development Goals (2016). Available online at: http://www.un.org/sustainabledevelopment/sustainable-development-goals/ (accessed October 12, 2020).
5. WHO UNFPA UNICEF Averting Maternal Deaths and Disabilities. Monitoring Emergency Obstetric Care: A Handbook. Geneva: WHO Press (2009).
6. Paxton A, Maine D, Freedman L. The evidence for emergency obstetric care. Int J Gynaecol Obstetr. (2005) 88:181–93. doi: 10.1016/j.ijgo.2004.11.026
7. Chavane LA, Bailey P, Loquiha O, Dgedge M, Aerts M, Temmerman M. Maternal death and delays in accessing emergency obstetric care in Mozambique. BMC Pregnancy Childbirth. (2018) 18:71. doi: 10.1186/s12884-018-1699-z
8. Banke-Thomas A, Avoka CK, Gwacham-Anisiobi U, Benova L. Influence of travel time and distance to the hospital of care on stillbirths: a retrospective facility-based cross-sectional study in Lagos, Nigeria. BMJ Global Health. (2021) 6:e007052. doi: 10.1136/bmjgh-2021-007052
9. Banke-Thomas A, Avoka CK, Gwacham-Anisiobi UC, Omololu O, Balogun MR, Wright KO, et al. Travel of pregnant women in emergency situations to hospital and maternal mortality in Lagos, Nigeria: a retrospective cohort study. BMJ Global Health. (2022) 7:e008604. doi: 10.1136/bmjgh-2022-008604
10. Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc Sci Med. (1994) 38:1091–110. doi: 10.1016/0277-9536(94)90226-7
11. Vearey J, Luginaah I, Magitta NF, Shilla DJ, Oni T. Urban health in Africa: a critical global public health priority. BMC Public Health. (2019) 19:340. doi: 10.1186/s12889-019-6674-8
12. Matthews Z, Channon A, Neal S, Osrin D, Madise N, Stones W. Examining the “urban advantage” in maternal health care in developing countries. PLoS Med. (2010) 7:e1000327. doi: 10.1371/journal.pmed.1000327
13. Norris M, Klabbers G, Pembe AB, Hanson C, Baker U, Aung K, et al. A growing disadvantage of being born in an urban area? Analysing urbansingag disparities in neonatal mortality in 21 African countries with a focus on Tanzania. BMJ Global Health. (2022) 7:e007544. doi: 10.1136/bmjgh-2021-007544
14. United Nations. World Urbanization Prospects: The 2018 Revision. New York, NY: United Nations (2019). Available online at: https://population.un.org/wup/Publications/Files/WUP2018-Report.pdf (accessed July 15, 2022).
15. Rudolfson N, Gruendl M, Nkurunziza T, Kateera F, Sonderman K, Nihiwacu E, et al. Validating the global surgery geographical accessibility indicator: differences in modeled versus patient-reported travel times. World J Surg. (2020) 44:2123–30. doi: 10.1007/s00268-020-05480-8
16. Banke-Thomas A, Wright K, Collins L. Assessing geographical distribution and accessibility of emergency obstetric care in sub-Saharan Africa: a systematic review. J Glob Health. (2019) 9:010414. doi: 10.7189/jogh.09.010414
17. Ouma P, Macharia PM, Okiro E, Alegana V, Ouma P, Macharia PM, et al. Methods of measuring spatial accessibility to health care in Uganda. In: Makanga PT, editor. Practicing Health Geography Global Perspectives on Health Geography. Cham: Springer (2021). p. 77–90.
18. Ouma PO, Maina J, Thuranira PN, Macharia PM, Alegana VA, English M, et al. Access to emergency hospital care provided by the public sector in sub-Saharan Africa in 2015: a geocoded inventory and spatial analysis. Lancet Glob Health. (2018) 6:e342–50. doi: 10.1016/S2214-109X(17)30488-6
19. Ahmed S, Adams AM, Islam R, Hasan SM, Panciera R. Impact of traffic variability on geographic accessibility to 24/7 emergency healthcare for the urban poor: a GIS study in Dhaka, Bangladesh. Wilson FA, editor. PLoS ONE. (2019) 14:e0222488. doi: 10.1371/journal.pone.0222488
20. Oxford Analytica. African Population Growth Will Add to Traffic Woes. Expert Briefings (2016). Available online at: https://doi.org/10.1108/OXAN-DB212671 (accessed April 14, 2022).
21. Obi D. Lagos Commuters Lose 75% of Weekly Working Hours to Traffic. News (2018). Available online at: https://businessday.ng/news/article/lagos-commuters-lose-75-of-weekly-working-hours-to-traffic/ (accessed February 19, 2020).
22. TomTom. TomTom Traffic Index Ranking. (2021). Available online at: https://www.tomtom.com/en_gb/traffic-index/ranking/ (accessed April 15, 2022).
23. Banke-Thomas A, Wong KLM, Ayomoh FI, Giwa-Ayedun RO, Benova L. “In cities, it's not far, but it takes long”: comparing estimated and replicated travel times to reach life-saving obstetric care in Lagos, Nigeria. BMJ Global Health. (2021) 6:e004318. doi: 10.1136/bmjgh-2020-004318
24. Banke-Thomas A, Balogun M, Wright O, Ajayi B, Abejirinde IOO, Olaniran A, et al. Reaching health facilities in situations of emergency: qualitative study capturing experiences of pregnant women in Africa's largest megacity. Reprod Health. (2020) 17:145. doi: 10.1186/s12978-020-00996-7
25. Yao J, Agadjanian V. Bypassing health facilities in rural Mozambique: spatial, institutional, and individual determinants. BMC Health Serv Res. (2018) 18:1006. doi: 10.1186/s12913-018-3834-y
26. Kruk ME, Mbaruku G, McCord CW, Moran M, Rockers PC, Galea S. Bypassing primary care facilities for childbirth: a population-based study in rural Tanzania. Health Policy Plan. (2009) 24:279–88. doi: 10.1093/heapol/czp011
27. Akin JS, Hutchinson P. Health-care facility choice and the phenomenon of bypassing. Health Policy Plan. (1999) 14:135–51. doi: 10.1093/heapol/14.2.135
28. Delamater PL, Messina JP, Shortridge AM, Grady SC. Measuring geographic access to health care: raster and network-based methods. Int J Health Geogr. (2012) 11:15. doi: 10.1186/1476-072X-11-15
29. Ebener S, Guerra-Arias M, Campbell J, Tatem AJ, Moran AC, Amoako Johnson F, et al. The geography of maternal and newborn health: the state of the art. Int J Health Geogr. (2015) 14:19. doi: 10.1186/s12942-015-0012-x
30. Matthews Z, Rawlins B, Duong J, Molla YB, Moran AC, Singh K, et al. Geospatial analysis for reproductive, maternal, newborn, child and adolescent health: gaps and opportunities. BMJ Global Health. (2019) 4:e001702. doi: 10.1136/bmjgh-2019-001702
31. Macharia PM, Ray N, Giorgi E, Okiro EA, Snow RW. Defining service catchment areas in low-resource settings. BMJ Global Health. (2021) 6:e006381. doi: 10.1136/bmjgh-2021-006381
32. Banke-Thomas A, Wong KLM, Collins L, Olaniran A, Balogun M, Wright O, et al. An assessment of geographical access and factors influencing travel time to emergency obstetric care in the urban state of Lagos, Nigeria. Health Policy Plan. (2021) 36:1384–96. doi: 10.1093/heapol/czab099
33. Bassey J. Lagos Targets 1m Mothers, Children as 110-bed MCC Opens in Eti-Osa. Business Day (2019). Available online at: https://businessday.ng/health/article/lagos-targets-1m-mothers-children-as-110-bed-mcc-opens-in-eti-osa/ (accessed July 15, 2022).
34. Banke-Thomas A. From Research paper? Policy. #Stakeholder briefing on geographical access to critical #maternalhealth services in #Lagos. Sharing findings with @ProfAkinAbayomi, Honourable Commissioner for Health, @followlasg. We discussed “hotspots” that need to be add. [@abankethomas] (2021). Available online at: https://twitter.com/abankethomas/status/1435831583466983424 (accessed July 15, 2022).
35. Banke-Thomas A, Avoka C, Olaniran A, Balogun M, Wright O, Ekerin O, et al. Patterns, travel to care and factors influencing obstetric referral: evidence from Nigeria's most urbanised state. Soc Sci Med. (2021) 291:114492. doi: 10.1016/j.socscimed.2021.114492
36. UNSTATS. Make Cities and Human Settlements Inclusive, Safe, Resilient and Sustainable. Sustainable Cities and Communities (2021). Available online at: https://unstats.un.org/sdgs/report/2021/goal-11/ (accessed April 13, 2022).
37. Magadi MA, Zulu EM, Brockerhoff M. The inequality of maternal health care in urban sub-Saharan Africa in the (1990s). Popul Stud. (2011) 57:347–66. doi: 10.1080/0032472032000137853
38. Banke-Thomas A, Wright K, Sonoiki O, Ilozumba O, Ajayi B, Okikiolu O, et al. Multi-stakeholder perspectives on access, availability and utilization of emergency obstetric care services in Lagos, Nigeria: a mixed-methods study. J Public Health Africa. (2017) 8:717. doi: 10.4081/jphia.2017.717
39. Geleto A, Chojenta C, Musa A, Loxton D. Barriers to access and utilization of emergency obstetric care at health facilities in sub-Saharan Africa: a systematic review of literature. Syst Rev. (2018) 7:183. doi: 10.1186/s13643-018-0842-2
40. McGuirk MA, Porell FW. Spatial patterns of hospital utilization: the impact of distance and time - PubMed. Inquiry. (1984) 21:84–95.
41. Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. (1981) 19:127–40. doi: 10.1097/00005650-198102000-00001
Keywords: urbanization and developing countries, emergency obstetric care, access, equity, travel time, big data, digital technology
Citation: Banke-Thomas A, Macharia PM, Makanga PT, Beňová L, Wong KLM, Gwacham-Anisiobi U, Wang J, Olubodun T, Ogunyemi O, Afolabi BB, Ebenso B and Abejirinde IO (2022) Leveraging big data for improving the estimation of close to reality travel time to obstetric emergency services in urban low- and middle-income settings. Front. Public Health 10:931401. doi: 10.3389/fpubh.2022.931401
Received: 29 April 2022; Accepted: 11 July 2022;
Published: 29 July 2022.
Edited by:
Peter Ouma Okuma, Government of Kenya, KenyaReviewed by:
Yogesh D. Sabde, RD Gardi Medical College, IndiaCopyright © 2022 Banke-Thomas, Macharia, Makanga, Beňová, Wong, Gwacham-Anisiobi, Wang, Olubodun, Ogunyemi, Afolabi, Ebenso and Omolade Abejirinde. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aduragbemi Banke-Thomas, a.bankethomas@gre.ac.uk
†These authors share first authorship