
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 06 September 2022
Sec. Public Health Education and Promotion
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.931306
This article is part of the Research TopicPromoting Health Equity During a Pandemic: Approaches to Address Vaccination Burden and Health Inequities Amongst Under-Served Populations in U.S. and MexicoView all 19 articles
 Alicia Harvey-Vera1,2,3
Alicia Harvey-Vera1,2,3 Sheryl Munoz2,3Irina Artamonova1Daniela Abramovitz1Maria Luisa Mittal1Cecilia Rosales4
Sheryl Munoz2,3Irina Artamonova1Daniela Abramovitz1Maria Luisa Mittal1Cecilia Rosales4 Steffanie A. Strathdee1*
Steffanie A. Strathdee1* Maria Gudelia Rangel2,5
Maria Gudelia Rangel2,5Background: SARS-CoV-2 prevalence is elevated among people who inject drugs (PWID). In Tijuana, Mexico, COVID-19 vaccines became available to the general population in June 2021, but uptake among PWID was <10%. We studied COVID-19 vaccine uptake among PWID in Tijuana following implementation of a pop-up vaccination clinic.
Methods: Beginning in October, 2020, PWID in Tijuana aged ≥18 years were enrolled into a longitudinal cohort study. At baseline and semi-annually, participants underwent interviewer-administered interviews on health behaviors and COVID-19 exposures through April 5, 2022. From June 21—September 20, 2021, staff referred PWID to a temporary COVID-19 vaccine pop-up clinic that was coincidentally established near the study office. Participants attending the clinic completed a short interview on barriers to vaccination and were offered facilitated access to free Janssen® COVID-19 vaccine. All participants were reimbursed $5 for this interview, regardless of whether or not they chose to be vaccinated. Poisson regression was used to evaluate the effect of the pop-up clinic on COVID-19 vaccination uptake, controlling forpotential confounders.
Results: Of 344 participants, 136 (39.5%) reported having received at least one COVID-19 vaccine dose during the 10 months follow-up period, of whom 113 (83.1%) received vaccine at the pop-up clinic and 23 (16.9%) elsewhere. One third of those receiving COVID-19 vaccine during the pop-up clinic were previously vaccine hesitant. Attending the pop-up clinic was independently associated with higher rates of COVID-19 vaccination Adjusted Rate Ratio (AdjRR: 9.15; 95% CI: 5.68–14.74).
Conclusions: We observed a significant increase in COVID-19 vaccine uptake associated with attending a temporary pop-up vaccine clinic in Tijuana suggesting that efforts to improve vaccination in this vulnerable population should include convenient locations and staff who have experience working with substance using populations. Since COVID-19 vaccination rates remain sub-optimal, sustained interventions to increase uptake are needed.
Individuals with a diagnosis of substance use disorder, including opioid use disorder, have significantly higher risk of acquiring SARS-CoV-2 and worse clinical outcomes than other COVID-19 patients (1). In a previous study of people who inject drugs (PWID) in Tijuana and San Diego, SARS-CoV-2 prevalence was 37.5%, which was higher than the general population in both cities (2). PWID may experience severe COVID-19 illness due to comorbid conditions, including chronic kidney, liver and lung diseases (1, 3–5). Additionally, PWID have limited access to health care services and often experience stigma and discrimination that perpetuates medical mistrust, contributing to poor health care utilization (6, 7). Due to the high COVID-19 burden among PWID, there is a need to expand COVID-19 vaccination efforts for this population (2, 8, 9).
In Mexico, SARS-CoV-2 has caused over 5.5 million cases of COVID-19 (10). Mexico developed five stages for vaccination rollout (11). In Stage 1, Mexico vaccinated 100% of their healthcare personnel (1.25 million people) between December 2020 and February 2021 (12). In Stage 2 (February to May 2021), vaccination efforts were prioritized to municipalities with concentrated COVID-19 mortality, starting with those 60 years old and older (11, 13). Efforts expanded with Stage 3 (May to June 2021) prioritizing pregnant women in the second or third trimester and persons 50 years or older. Stage 4 (June to July 2021) expanded to persons 40 years or older, and finally, Stage 5 vaccinating the general population beginning in July 2021 (12). In Tijuana, Baja California, Mexico's most northwestern state abutting California, United States, COVID-19 vaccines became available according to the above schedule at mass vaccination sites throughout the city, where SinoVac-CoronaVac®, Oxford-AstraZeneca®, and J&J/Janssen® vaccines were offered (14).
By June 25, 2021, Baja California reported being close to becoming the first state in Mexico to achieve full vaccination for most of its adult residents (15, 16) following a donation of J&J/Janssen vaccine from the United States; however, vaccine uptake was lower in some marginalized populations (17). As in other Mexican cities, individuals in Tijuana seeking COVID-19 vaccination were required to register online and enter their CURP (Clave Única de Registro de Población; Mexican official unique identifier) to obtain an appointment and were asked to print the appointment card or present their CURP to verify their identity (18), which has been shown to be a barrier to health services in other settings (19). For low income residents such as most PWID, this may have represented a financial burden since those lacking computer or smartphone access were required to pay for computer time and printouts. Additionally, some COVID-19 vaccine queues were very long. People without reliable transportation may have faced additional barriers to access.
An earlier study conducted by our binational team found that only 7.6% of PWID living on either side of the San Diego-Tijuana border reported having had at least one COVID-19 vaccine dose by September 2021, and nearly one-third reported being vaccine hesitant (17). There was no difference in COVID-19 vaccine hesitancy between PWID residing in San Diego vs. Tijuana or by race/ethnicity but younger PWID and those who endorsed COVID-19 disinformation were more vaccine hesitant (17). Disinformation has been described as the deliberate spread of false information, as opposed to misinformation, which is spread without malicious intent (2, 20).
In an effort to increase COVID-19 vaccination among marginalized populations, a temporary pop-up vaccination clinic was set up in Tijuana's Zona Norte that offered assistance to access free COVID-19 vaccination. We studied predictors of COVID-19 vaccine uptake clinic among PWID, hypothesizing that PWID who attended the pop-up clinic would be more likely to be vaccinated. We also postulated that those endorsing more COVID disinformation beliefs would be less likely to become vaccinated.
Between October 28, 2020 and September 10, 2021, adults aged ≥18 or older who injected drugs within the last month and lived in San Diego County or Tijuana were recruited into a longitudinal cohort study, as previously described (2). Recruitment took place using street outreach whereby potential participants were approached in various locations, such as on the street, parks, bars, shelters, motels, river canyons and vacant lots. The current analysis was restricted to the 344 participants who were recruited in Tijuana, had not received a COVID-19 vaccination prior to the opening of the pop-up clinic and who underwent the necessary interviews to collect data on COVID-19 vaccination history. The study was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki). Informed consent was obtained from all participants and the protocol was approved by institutional review board at Xochicalco University in Tijuana.
After providing written informed consent, participants were provided with a photo ID with the study's logo and contact information. All underwent face-to-face interviewer-administered surveys using computer assisted personal interviews in the study office, which was located in the Zona Norte neighborhood in Tijuana. Surveys assessed socio-demographics, chronic health conditions (e.g., diabetes, asthma, hypertension), and potential experiences in their lifetime and during the last 6 months such as homelessness, number of hours spent on the street, injection and non-injection use of specific drugs, food insecurity (21), if they had been enrolled in a substance use treatment program, had been incarcerated or used a syringe services program (SSP).
To reduce participant burden, some survey items, including COVID-19 related beliefs, exposures and vaccination uptake were administered at a supplemental interview approximately 1 week following the baseline visit. We also asked participants about various COVID-19 related experiences (negative income impact, food insecurity, knows someone who died from COVID-19), potential exposures to COVID-19 and protective behaviors (e.g., social distancing, masking, COVID-19 testing). Perceived threat of COVID-19 was assessed by asking participants how worried they were about getting COVID-19 (or getting it again) on a 10 point scale (22).
We asked participants if they had ever received one or more doses of COVID-19 vaccine, and if so, to specify the date and location. To assess COVID-19 misinformation, we presented participants with seven statements about SARS-CoV-2 transmission, severity, immunity, symptoms, treatments and vaccines and asked them to classify each statement as “True”, “False,” or “Unsure” (17). These included the following: (1) COVID-19 cannot be easily spread from one person to another; (2) many thousands of people have not died from COVID-19; (3) most people are immune to COVID-19; (4) you can tell someone has COVID-19 from looking at them; (5) there are treatments that can cure COVID-19; (6) COVID-19 is about as dangerous as having the flu; and (7) COVID-19 vaccines are not safe for pregnant women. We then created a binary variable for each statement indicating whether the participant was misinformed or not, grouping “unsure” responses with responses that clearly indicated having endorsed misinformation.
COVID-19 disinformation was assessed through a six-item scale including conspiracy theory items as previously described (23). These included “COVID-19 was created by the pharmaceutical industry” or “the Chinese government”, “childhood vaccines cause autism” (24), as well as three additional items: “COVID-19 vaccines include a tracking device”, “alter DNA”, and “COVID-19 vaccines offered to ‘people like me' are not as safe”. We dichotomized responses to indicate endorsement of disinformation (“True” and “Unsure”) or not (“False”) and summed them into a total score ranging from 0–6. The mean inter-item correlation value was 0.31, which indicates optimal internal consistency (25). We also assessed COVID-19 vaccine hesitancy as Yes versus No or Unsure.
Follow-up visits were conducted every 6 months where the above measures, including COVID-19 vaccine uptake was re-assessed. Participants were compensated $20 USD for the baseline and follow-up surveys and $10 for the supplemental survey.
Blood samples were collected by venipuncture. Sera were batched and tested weekly by Genalyte® (San Diego, CA), using their Maverick™ Multi-Antigen Serology Panel (26) that detects IgG and IgM antibodies to five SARS-CoV-2 antigens.
Participants were shown how to self-collect anterior nasal swabs in the presence of study staff. Swabs which were placed in 3 mL of viral transport media for temporary storage, before being shipped for testing at the San Diego Center for AIDS Research laboratory. RT-PCR was conducted using a pooling approach based on the Fluxergy system® (Irvine, CA) to detect SARS-CoV-2 RNA.
Rapid HIV and HCV tests were conducted using MedMira's Miriad Rapid HIV/HCV Antibody Test (Halifax, Nova Scottia, CA). Reactive and indeterminate tests underwent a second rapid test with Oraquick® HIV or Oraquick® HCV, respectively (Orasure, Bethlehem, PA) and were confirmed by Western Blot at the UC San Diego Centers for AIDS Research.
Following the interview and specimen collection, participants were referred to available resources depending on their responses and stated needs (e.g., treatment for HIV, substance use). From June 21—September 20, 2021, participants who indicated that they had not had a prior COVID-19 vaccine were referred to a pop-up COVID-19 vaccine clinic, which was located nearby the study office in a neighborhood known for its high level of drug use and where sex work is quasi-legal.
Participants who attended the pop-up clinic were permitted to show their photo ID from our study as proof of identification and were provided with assistance obtaining their CURP if needed by clinic staff, all of whom had extensive experience with substance users. Participants were also invited to undergo a short interviewer-administered survey which included reasons why they had not yet received a COVID-19 vaccine. At the end of the survey they were reimbursed $5 USD and were offered facilitated access to free single-dose Janssen® COVID-19 vaccine by a licensed medical provider with pre- and post-test counseling. Monetary reimbursement was not contingent upon participants' decision to receive the vaccine.
All eligible participants who were not vaccinated prior to establishment of the pop-up clinic (i.e., June 21st, 2021) were included in this analysis. Participants were followed up until April 5th, 2022 and the outcome (i.e., whether they received a vaccine or not by the end of follow-up period) was assessed.
Characteristics of participants who were and were not COVID-19 vaccinated were summarized by generating frequencies and percentages for binary variables and means and standard deviations for continuous variables. The two groups were compared using Mann-Whitney U tests for continuous variables and Chi-square or Fisher's Exact tests for categorical variables. Since our primary objective was to assess whether the exposure to an intervention (visiting the pop-up clinic) was successful at increasing vaccination uptake, we undertook the following analytical approach. First, as suggested by VanderWeele (2019) (27), we selected a series of variables to further examine and determine potential confounders to control for in a multivariable model to estimate the intervention effect on the outcome. Initially, all the variables listed in Table 2 were selected based on subject-matter knowledge and the assumption that any could played a causal role on the outcome (vaccine uptake), primary exposure (visiting the pop-up clinic), or both.
Next, we regressed each individual variable listed in Table 2 on the vaccine uptake outcome by conducting univariate Poisson regressions with robust standard error estimations via generalized estimating equations (GEE) (28, 29). Whether a participant got vaccinated between June 21st, 2021 and April 5th, 2022 in conjunction with the natural logarithm of time spent “at risk” facilitated the estimation of the vaccine incidence rate. For those who got vaccinated, time spent “at risk” was calculated as the number of days between the dates when COVID-19 vaccination was first offered to the date of self-reported vaccination, whereas for those unvaccinated it was calculated as the number of days between when COVID-19 vaccination was first offered to the date when the participant was last seen. The estimates from the aforementioned regressions are listed in Table 2.
To identify variables that might play a causal role on the exposure, we regressed all of the variables listed in Table 2 on the exposure variable (i.e., attended the pop-up clinic) by conducting univariate logistic regressions with robust standard error estimation via GEE (results not shown).Next, considering each variable's effect size on the outcome or exposure, in conjunction with a level of statistical significance of 0.10 which is in an acceptable range supported in the literature (28), we narrowed down the candidates for inclusion in a multivariable model. Last, we created the final multivariable model by using the “purposeful selection of variables” strategy of Hosmer and Lemeshaw (1999, 2000) (30, 31), where subject matter significance, relationships among the independent variables (e.g., correlations, confounding, and interactions) and statistical significance were taken into consideration. In the final multivariable model, only covariates that maintained a significance level <0.10 were retained. All possible confounding interactions were assessed and ruled out. Multi-collinearity was ruled out based on appropriate values of the largest condition index and VIFs.
All statistical analyses were conducted using SAS, version 9.4.
A total of 344 cohort participants reported not having received any COVID-19 vaccine before June 21, 2021 and completed questions on COVID-19 vaccination during the study period ending April 5, 2021, and hence were eligible for this analysis. The majority were male (74.4%), Mexican (91.0%) and mean age was 43 years (SD = 9.6).
Of the 344 participants, 324 (94.2%) completed the supplemental survey which included questions on COVID-19 vaccine hesitancy. Of these, 62 (19.1%) reported that they were not interested in receiving the vaccine, 55 (17.0%) were unsure and 207 (63.9%) reported that they were willing to be vaccinated. Over nearly 10 months of follow-up, 136 (39.5%) reported having received at least one COVID-19 vaccine dose, of whom 113 (83.1%) received vaccine at the pop-up clinic and 23 (16.9%) received it elsewhere. Of 105 participants who received COVID-19 vaccine at the pop-up clinic and had previously answered questions on vaccine hesitancy, 36 (34.3%) had previously expressed being unwilling or unsure about being vaccinated against COVID-19.
Factors associated with receiving at least one dose of COVID-19 vaccine during the 10 month follow-up period are shown in Tables 1, 2. We observed no sociodemographic factors that predicted COVID-19 vaccine uptake. Considering behavioral characteristics, participants who reported engaging in sex work in the last 6 months were marginally more likely to receive COVID-19 vaccination (Table 1). Participants who reported using crack cocaine were less likely to have been vaccinated compared to those who did not report use of crack (2.2% vs. 7.7%, p = 0.03). Also, participants who reported increasing their handwashing or use of hand sanitizers were more likely to have been vaccinated compared to those who did not (11.0% vs. 3.8%, p = 0.01), but no other protective or health-related factors were predictive of vaccine uptake.
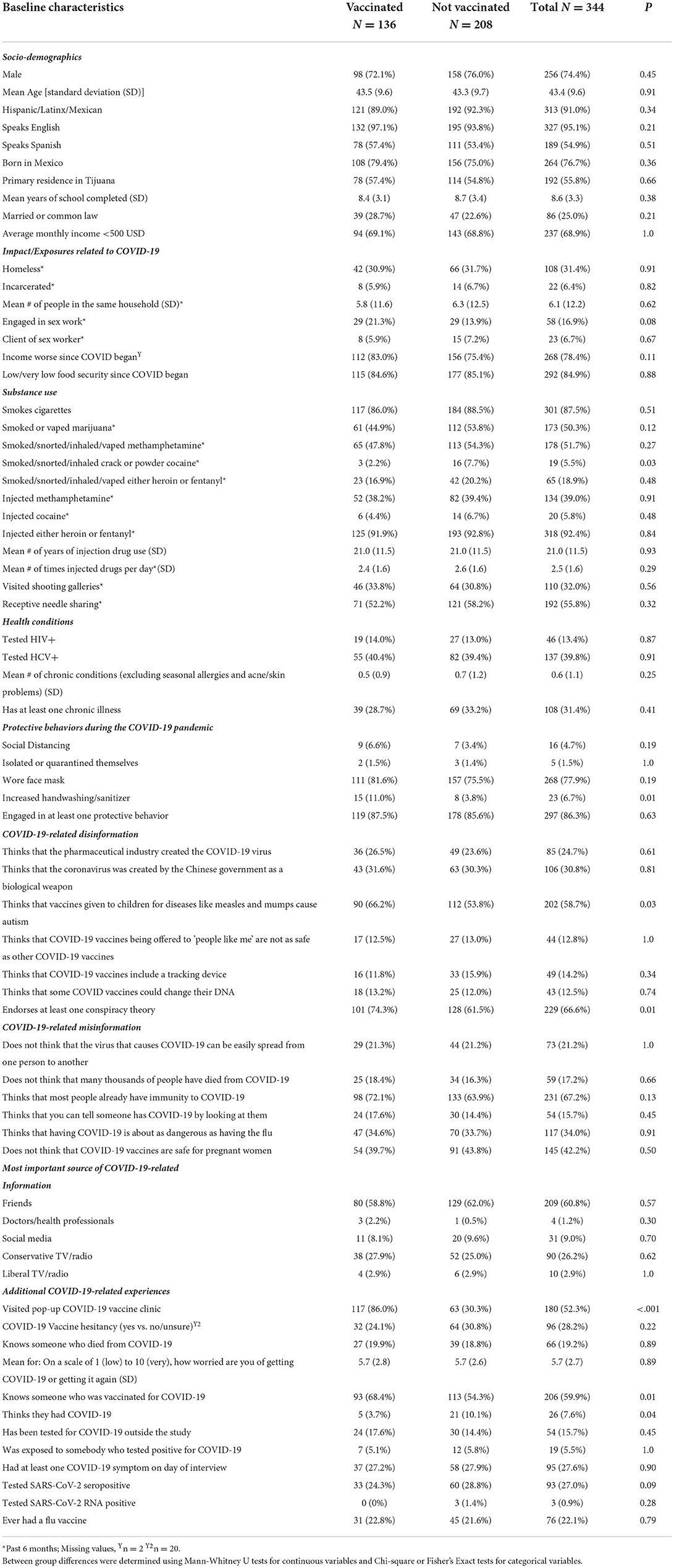
Table 1. Characteristics Associated with COVID-19 Vaccination among PWID in Tijuana, Mexico (n = 344).
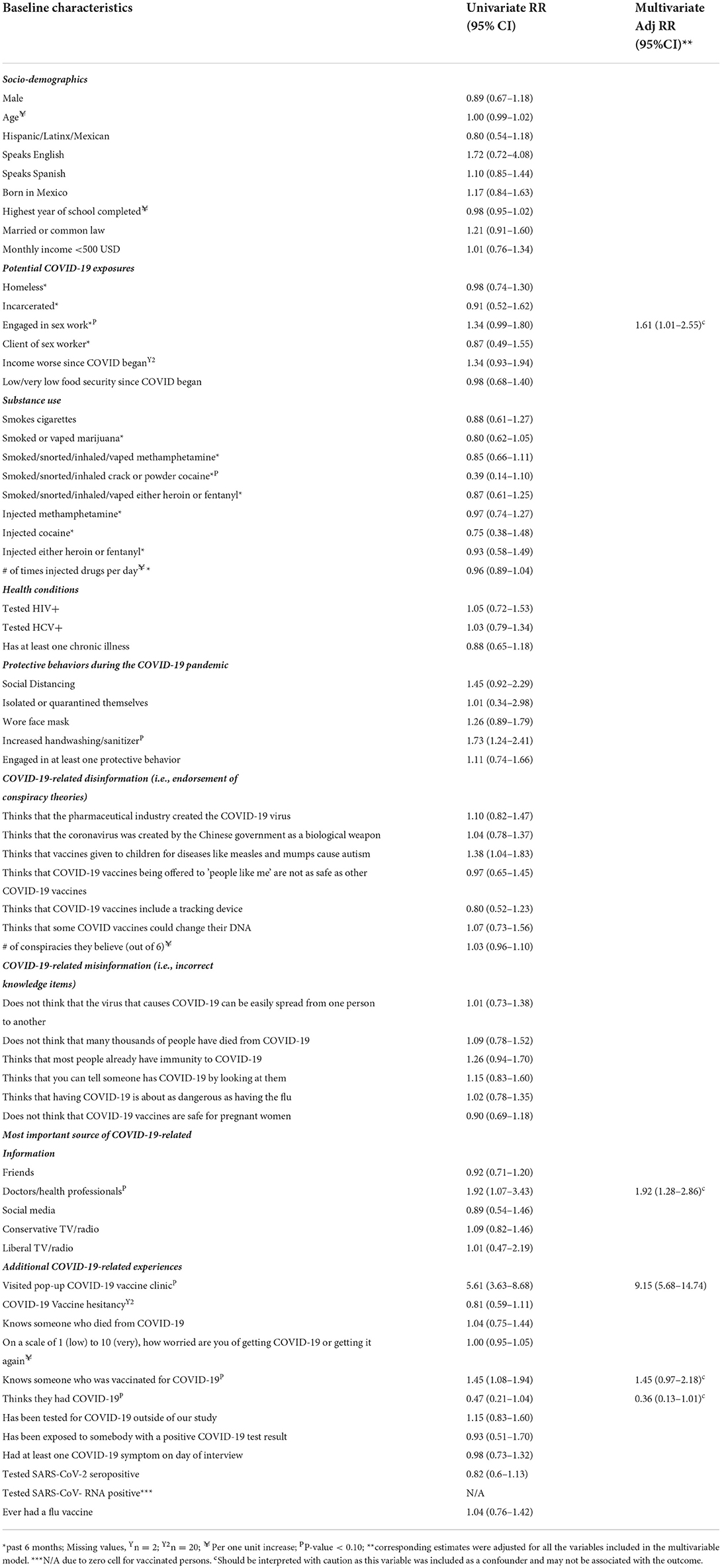
Table 2. Factors Associated with COVID-19 Vaccination among PWID in Tijuana, Mexico.
Surprisingly, participants who received COVID-19 vaccination were more likely to believe that childhood vaccines caused autism (66.2% vs. 53.8%, p = 0.03); however, no other COVID-19 disinformation measures were associated with COVID-19 vaccination. Similarly, we found no associations between COVID-19 vaccination and endorsing statements that reflect COVID-19 misinformation. COVID-19 vaccine hesitancy was not significantly associated with vaccine uptake.
The strongest predictor of COVID-19 vaccination was visiting the pop-up COVID-19 vaccine clinic after receiving a referral. Of those who received the COVID-19 vaccine, 86% visited the pop-up clinic, whereas only 30.3% of those unvaccinated visited the clinic (p <0.001), which corresponded to a Rate Ratio [RR] of 5.61 95% Confidence Interval (CI): 3.63–8.68; Table 2.
Knowing someone who had received COVID-19 was significantly associated with getting vaccinated, (RR: 1.45; 95% CI: 1.08–1.94) but participants who believed they had already had COVID-19 were less likely to get vaccinated (RR: 0.47; 95%CI: 0.21–1.04). Testing positive for SARS-CoV-2 antibodies or RNA was not associated with vaccination. Association between Pop-Up Clinic Attendance on COVID-19 Vaccine Uptake 3.5.Adjusting for Confounders
Of variables included in Table 2, obtaining most of their COVID−19 information from health providers, having had COVID-19, knowing more people who had received COVID-19 vaccines and engaging in sex work were identified as potential confounders. After adjusting for these variables, attending the pop-up clinic became even more strongly associated with COVID-19 vaccination in the multivariate model [Adjusted Rate Ratio (AdjRR: 9.15; 95% CI: 5.68–14.74), Adjustment for sociodemographic factors such as age and sex did not alter parameter estimates. No significant interactions were observed.
In this prospective study of PWID living in Tijuana during the COVID-19 epidemic, we found that attending a temporary pop-up vaccine clinic was independently associated with greater uptake of COVID-19 vaccination. Before this clinic was established, <10% of PWID in our study had received at least one COVID-19 vaccine dose (17), which is similar to a study of PWID in Oregon, USA (32). By the end of the 10 months follow-up period, the proportion of participants who had received at least one COVID-19 vaccine dose had increased to 39.5%. Although this level of vaccine coverage remains grossly sub-optimal, it is encouraging that at least one third of the study participants who were vaccinated during the pop-up clinic had previously reported being vaccine hesitant, suggesting that attendance at the clinic was influential in their decision to receive COIVID-19 vaccine.
Our findings should be interpreted cautiously due to the observational nature of our cohort study. Due to time constraints and the public health imperative to increase COVID-19 vaccination in this highly vulnerable population, we did not randomize participants to receive pop-up clinic referrals in a clinical trial design, which would have been more rigorous. Our study may have under-estimated the impact of the pop-up COVID-19 vaccination clinic since the clinic only operated during the first two months of the follow-up period and low statistical power may have attenuated the magnitude of some associations. Also, while we created a single multivariable model to assess the effect of the intervention on the outcome and adjusted for potential confounders which is common practice, some authors (33) suggest caution when trying to interpret the effects of the confounders on the outcome as they may not have the same interpretation as that of a “primary effect” on the outcome. We therefore limit our discussion to the potential effect of the pop-up clinic on COVID-19 vaccine uptake.
It is possible that some participants accepted the referral to the pop-up clinic because they were more interested in the $5 monetary reimbursement for completing the supplemental survey, rather than receiving COVID-19 vaccine. Indeed, a review of 11 clinical studies showed that financial incentives were associated with a seven-fold increase in adherence to the vaccine schedule for Hepatitis B virus, leading some researchers to advocate for contingency management to increase COVID-19 vaccine uptake (8, 34). In a study of PWID in Oregon, contingency management was associated with a significant increase in SARS-CoV-2 testing (35). However, financial incentives are not able to compensate for broad vaccination barriers (36), and some studies have shown that small compensations may not increase COVID-19 vaccination rates (37, 38). Therefore, it may not be realistic to expect that lower and middle-income countries could provide large enough financial incentives to significantly increase COVID-19 vaccination given limited resources and competing health priorities.
Despite the limitations of our study design and relatively short follow-up period, our findings have implications for improved COVID-19 vaccine uptake in this marginalized population. Greater uptake of COVID-19 vaccination associated with the pop-up clinic could have been due to its convenient location in the Zona Norte, the clinic staff's experience and familiarity with the issues facing people living with addiction, the ability of participants to use their photo ID from the study as proof of identification, or the assistance some participants received from clinic staff in obtaining their CURP. Since our observational study design was unable to determine which of these or other factors may have been most influential in the participants' decisions to receive vaccination, additional studies are required to examine client preferences to appropriately tailor services to their needs.
Although we did not find COVID-19 disinformation, misinformation or vaccine hesitancy to be significantly associated with lower vaccine uptake as we had hypothesized, it is noteworthy that two-thirds of our cohort endorsed at least one COVID-19 conspiracy theory, one third felt that COVID-19 was “no worse than the flu”, and close to 50% believed that COVID-19 vaccines are not safe for pregnant women. Apart from system-level barriers, widespread COVID-19 disinformation and government criticism was prevalent on both sides of the US-Mexico border (39) making it harder for people to discern false information from evidence-based sources. Based on these findings, additional interventions to address medical mistrust are needed.
In summary, our prospective evaluation found a significant increase in COVID-19 vaccine uptake associated with attending a pop-up vaccine clinic in Tijuana. Despite our encouraging findings, <50% of PWID in our study had received at least one COVID-19 vaccine dose. Sustained efforts to improve COVID-19 vaccination in this population should focus on removing logistical and structural barriers to ensure that their health and that of the general population are protected.
The datasets presented in this article are not readily available because the study is ongoing. Requests to access the datasets should be directed to DA, dabramovitz@health.ucsd.edu.
The studies involving human participants were reviewed and approved by Institutional Review Board at Xochicalco University and the Office of IRB Administration at the University of California San Diego. The patients/participants provided their written informed consent to participate in this study.
AH-V, SM, MR, and CR were responsible for participant referrals and data collection. DA and IA were responsible for data management and analysis. SS conceived the study design and oversaw the analysis. SS, AH-V, and DA interpreted the findings. MM, SS, AH-V, IA, and SM wrote the manuscript. AH-V, SM, IA, DA, MM, CR, SA, and MR reviewed and edited the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the National Institute on Drug Abuse (NIDA) at the National Institutes of Health (NIH) (R01DA049644-S1). Additional support was provided by the National Institute of Allergy and Infectious Diseases (P30 AI036214). UC San Diego Altman Clinical and Translational Research Institute SUSTAIN program (NIH/NCATS 1KL2TR001444).
The authors gratefully acknowledge the La Frontera study team and participants in San Diego and Tijuana and staff at Genalyte and Fluxergy for assistance interpreting laboratory results, laboratory staff at the Center for AIDS Research and Sharon Park for assistance with manuscript preparation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wang QQ, Kaelber DC, Xu R, Volkow ND. COVID-19 risk and outcomes in patients with substance use disorders: analyses from electronic health records in the United States. Mol Psychiatry. (2021) 26:30–9. doi: 10.1038/s41380-020-00880-7
2. Strathdee SA, Abramovitz D, Harvey-Vera A, Vera CF, Rangel G, Artamonova I, et al. Prevalence and correlates of SARS-CoV-2 seropositivity among people who inject drugs in the San Diego-Tijuana border region. PLoS ONE. (2021) 16:e0260286. doi: 10.1371/journal.pone.0260286
3. Koslik HJ, Joshua J, Cuevas-Mota J, Goba D, Oren E, Alcaraz JE, et al. Prevalence and correlates of obstructive lung disease among people who inject drugs, San Diego, California. Drug Alcohol Depend. (2020) 214:108158. doi: 10.1016/j.drugalcdep.2020.108158
4. Vasylyeva TI, Smyrnov P, Strathdee S, Friedman SR. Challenges posed by COVID-19 to people who inject drugs and lessons from other outbreaks. J Int AIDS Soc. (2020) 23:e25583. doi: 10.1002/jia2.25583
5. McGowan CR, Wright T, Nitsch D, Lewer D, Brathwaite R, Scott J, et al. High prevalence of albuminuria amongst people who inject drugs: a cross-sectional study. Sci Rep. (2020) 10:7059. doi: 10.1038/s41598-020-63748-4
6. Biancarelli DL, Biello KB, Childs E, Drainoni M, Salhaney P, Edeza A, et al. Strategies used by people who inject drugs to avoid stigma in healthcare settings. Drug Alcohol Depend. (2019) 198:80–6. doi: 10.1016/j.drugalcdep.2019.01.037
7. van Boekel LC, Brouwers EP, van Weeghel J, Garretsen HF. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: systematic review. Drug Alcohol Depend. (2013) 131:23–35. doi: 10.1016/j.drugalcdep.2013.02.018
8. Iversen J, Peacock A, Price O, Byrne J, Dunlop A, Maher L. COVID-19 vaccination among people who inject drugs: Leaving no one behind. Drug Alcohol Rev. (2021) 40:517–20. doi: 10.1111/dar.13273
9. Dunlop A, Lokuge B, Masters D, Sequeira M, Saul P, Dunlop G, et al. Challenges in maintaining treatment services for people who use drugs during the COVID-19 pandemic. Harm Reduct J. (2020) 17:26. doi: 10.1186/s12954-020-00370-7
10. Dirección General de Epidemiología. Covid-19 México: Información General 2022. Available online at: https://datos.covid-19.conacyt.mx/ (accessed March 15, 2022).
11. Secretaría, de Salud,. Etapas de Vacunación. Available online at: http://Vacunacovid.gob.mx/wordpress (accessed March 23, 2022).
12. Secretaría, de Salud,. Calendario de Vacunación. Available online at: http://vacunacovid.gob.mx/wordpress/calendario-vacunacion/ (accessed April 21, 2022).
13. Bautista-Arredondo S, Grupo Técnico Asesor de. Vacunación Covid. Actualización del análisis de priorización de las vacunas para COVID-19 en México y recomendaciones generadas. Santa María Ahuacatitlán: Salud pública de México. (2021).
14. Mendoza A, Border Vaccination Plan With U.S.-Donated Shots Starts in Baja California. The San Diego Union-Tribune. (2021). Available online at: https://www.sandiegouniontribune.com/news/border-baja-california/story/2021-06-18/border-vaccination-plan-with-u-s-donated-shots-starts-in-baja-california (accessed April 21, 2022).
15. Morán Breña C,. Baja California Tendrá A Toda su población mayor de 18 Años Vacunada en 10 días El País. (2021). Available online at: https://elpais.com/mexico/2021-06-17/baja-california-tendra-a-toda-su-poblacion-mayor-de-18-anos-vacunada-en-10-dias.html (accessed April 20, 2022).
16. ‘Misión Cumplida': Baja California, Primer Estado En Vacunar a más del 90% de adultos: El, Financiero (2021). Available online at: https://www.elfinanciero.com.mx/nacional/2021/06/25/mision-cumplida-baja-california-primer-estado-en-vacunar-a-mas-del-90-de-adultos/ (accessed April 21, 2022).
17. Strathdee SA, Abramovitz D, Harvey-Vera A, Vera CF, Rangel G, Artamonova I, et al. Correlates of coronavirus disease 2019 (COVID-19) vaccine hesitancy among people who inject drugs in the San Diego-Tijuana border region. Clin Infect Dis. (2021). doi: 10.1093/cid/ciab975. [Epub ahead of print].
18. Secretaría, de Salud,. Cómo Registrarse Para ser Vacunado Contra el Covid-19 Available online at: https://mivacuna.salud.gob.mx/pdf/registro_vacuna_imgns_c6.pdf (accessed April 21, 2022).
19. Sanders C, Burnett K, Lam S, Hassan M, Skinner K. “You need ID to get ID”: a scoping review of personal identification as a barrier to and facilitator of the social determinants of health in North America. Int J Environ Res Public Health. (2020) 17:4227. doi: 10.3390/ijerph17124227
20. Swire-Thompson B, Lazer D. Public health and online misinformation: challenges and recommendations. Annu Rev Public Health. (2020) 41:433–51. doi: 10.1146/annurev-publhealth-040119-094127
21. U.S. Department of Agriculture. Food Security in the U.S. - Measurement 2021. (2021). Available online at: https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/measurement/#measurement (accessed April 21, 2022).
22. Gorbach PM, Siminski S, Ragsdale A, Investigators CP. Cohort profile: the collaborating consortium of cohorts producing NIDA opportunities (C3PNO). Int J Epidemiol. (2021) 50:31–40. doi: 10.1093/ije/dyaa163
23. Strathdee SA, Abramovitz D, Harvey-Vera AY, Vera CF, Rangel G, Artamonova I, et al. Correlates of COVID-19 vaccine hesitancy among people who inject drugs in the San Diego-Tijuana border region. Clin Infect Dis. (2021) ciab975. doi: 10.1101/2021.10.29.21265669. [Epub ahead of print].
24. Romer D. Jamieson KH. Conspiracy theories as barriers to controlling the spread of COVID-19 in the US. Soc Sci Med. (2020) 263:113356. doi: 10.1016/j.socscimed.2020.113356
25. Briggs SR, Cheek JM. The role of factor analysis in the development and evaluation of personality scales. J Pers. (1986) 54:106–48. doi: 10.1111/j.1467-6494.1986.tb00391.x
26. Food Drug Administration (FDA). Maverick™ SARS-CoV-2 Multi-Antigen Serology Panel v2 01030ART-01. Available online at: https://www.fda.gov/media/142915/download (accessed April 20, 2022).
27. VanderWeele TJ. Principles of confounder selection. Eur J Epidemiol. (2019) 34:211–9. doi: 10.1007/s10654-019-00494-6
28. Zou G A. modified poisson regression approach to prospective studies with binary data. Am J Epidemiol. (2004) 159:702–6. doi: 10.1093/aje/kwh090
29. Lee J, Tan CS, Chia KS A. practical guide for multivariate analysis of dichotomous outcomes. Ann Acad Med Singap. (2009) 38:714–9. doi: 10.47102/annals-acadmedsg.V38N8p714
30. Lemeshow S, May S, Hosmer Jr DW. Applied Survival Analysis: Regression Modeling of Time-to-Event Data. Hoboken, NJ: John Wiley & Sons. (2011).
31. Hosmer Jr DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression. Hoboken, NJ: John Wiley & Sons. (2013).
32. Cioffi CC, Kosty D, Nachbar S, Capron CG, Mauricio AM, Tavalire HF. COVID-19 vaccine deliberation among people who inject drugs. Drug Alcohol Depend Rep. (2022) 3:100046. doi: 10.1016/j.dadr.2022.100046
33. Westreich D, Greenland S. The table 2 fallacy: presenting and interpreting confounder and modifier coefficients. Am J Epidemiol. (2013) 177:292–8. doi: 10.1093/aje/kws412
34. Higgins ST, Klemperer EM, Coleman SRM. Looking to the empirical literature on the potential for financial incentives to enhance adherence with COVID-19 vaccination. Prev Med. (2021) 145:106421. doi: 10.1016/j.ypmed.2021.106421
35. Cioffi CC, Kosty D, Capron CG, Tavalire HF, Barnes RC, Mauricio AM. Contingency management and SARS-CoV-2 testing among people who inject drugs. Public Health Rep. (2022) 137:573–9. doi: 10.1177/00333549221074385
36. Wong CA, Pilkington W, Doherty IA, Zhu Z, Gawande H, Kumar D, et al. Guaranteed financial incentives for COVID-19 vaccination: a pilot program in North Carolina. JAMA Intern Med. (2022) 182:78–80. doi: 10.1001/jamainternmed.2021.6170
37. Kreps S, Dasgupta N, Brownstein JS, Hswen Y, Kriner DL. Public attitudes toward COVID-19 vaccination: the role of vaccine attributes, incentives, and misinformation. NPJ Vaccines. (2021) 6:73. doi: 10.1038/s41541-021-00335-2
38. Serra-Garcia M, Szech N. Incentives and defaults can increase Covid-19 vaccine intentions and test demand. Manage Sci. (2021) pp. 1–13. doi: 10.2139/ssrn.3818182
Keywords: COVID-19, substance use, people who inject drugs, COVID-19 vaccines, sex work
Citation: Harvey-Vera A, Munoz S, Artamonova I, Abramovitz D, Mittal ML, Rosales C, Strathdee SA and Rangel MG (2022) COVID-19 vaccine uptake among people who inject drugs in Tijuana Mexico. Front. Public Health 10:931306. doi: 10.3389/fpubh.2022.931306
Received: 28 April 2022; Accepted: 18 July 2022;
Published: 06 September 2022.
Edited by:
Giovanni Rezza, Ministry of Health, Rome, ItalyReviewed by:
Isaac Núñez, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán (INCMNSZ), MexicoCopyright © 2022 Harvey-Vera, Munoz, Artamonova, Abramovitz, Mittal, Rosales, Strathdee and Rangel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Steffanie A. Strathdee, c3N0cmF0aGRlZUBoZWFsdGgudWNzZC5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.