 Thais Lopes do Amaral Uchôa1
Thais Lopes do Amaral Uchôa1 Eliete da Cunha Araújo1
Eliete da Cunha Araújo1 Richardson Augusto Rosendo da Silva2
Richardson Augusto Rosendo da Silva2 Rubenilson Valois3
Rubenilson Valois3 Wanderson Santiago de Azevedo Junior1
Wanderson Santiago de Azevedo Junior1 Valéria Gabriele Caldas Nascimento1
Valéria Gabriele Caldas Nascimento1 Cintia Yolette Urbano Pauxis Aben-Athar1
Cintia Yolette Urbano Pauxis Aben-Athar1 Andressa Tavares Parente1
Andressa Tavares Parente1 Eliã Pinheiro Botelho1
Eliã Pinheiro Botelho1 Glenda Roberta Oliveira Naiff Ferreira1*
Glenda Roberta Oliveira Naiff Ferreira1*- 1Program of Post-Graduation in Nursing, Federal University of Pará, Belém, Brazil
- 2Program of Post-Graduation in Collective Health, Federal University of Rio Grande do Norte, Rio Grande do Norte, Brazil
- 3Program of Post-Graduation in Nursing, State University of Pará, Belém, Brazil
Background: There was a high proportion of pregnant women who were attending prenatal care who were not tested for syphilis or tested but not treated, among priority countries. The coverage for prenatal care visits, syphilis screening, and treatment are priority indicators for monitoring of the elimination of syphilis. The aim was to determine the factors associated with gestational syphilis among postpartum women who were in a prenatal care program in the Brazilian Amazon.
Methods: An unmatched case–control study was conducted at the hospital in Brazil. Data collection was carried out from November 2020 to July 2021 during hospitalization using a pretested structured questionnaire. The criteria for selection of cases and control followed the guidelines established by the Ministry of Health of Brazil; postpartum women with a laboratory diagnosis based on treponemal and/or nontreponemal tests, symptoms of syphilis or asymptomatic, treatment or not treated, and in a prenatal care program. Gestational syphilis cases were identified as women who tested positive for syphilis, and those who tested negative were controls, at minimally one prenatal care visit, childbirth, and/or the puerperium. The sample size encompassed 59 cases and 118 controls (1: 2 ratio of cases to controls). Data were analyzed using Minitab 20® and BioEstat 5.3® software. The odds ratio was calculated by multiple logistic regression.
Results: One hundred and seventy-seven postpartum women were included in the study, 59 cases and 118 controls. Among all participants, 95.5% (169) were tested for syphilis in any trimester during pregnancy and at the delivery and 4.5% (8) were tested in the maternity only, at the time childbirth and/or puerperium. The final multiple logistic regression model evidenced that cases had higher odds compared to controls if they had past history of sexually transmitted infections (AOR: 55.4; p: 0.00), difficulty talking about condom use with their sexual partner (AOR: 4.92; p: 0.01), one to six prenatal care visits (AOR: 4.93; p: 0.01), had not received a sexually transmitted infections test result in the maternity hospital (AOR: 4.09; p: 0.04), lower monthly income (AOR: 4.32; p: 0.04), or one to three miscarriages (AOR: 4.34; p: 0.01).
Conclusion: The sociodemographic, programmatic, obstetric, and sexual factors are associated with gestational syphilis among postpartum women.
Introduction
The elimination of mother-to-child transmission (EMTCT) of Treponema pallidum is a public health priority (1, 2). It is estimated that congenital syphilis (CS) rates decreased globally between 2012 and 2016, from 539 to 473 per 100,000 live births (1) suggesting an expansion of prenatal healthcare (PNC) services. However, there are still regional disparities (1–3).
In Brazil, between 2012 and 2019, the congenital syphilis and gestational syphilis (GS) rates presented an increased trend by 112.5 and 282.46%, respectively (3). Gestational syphilis poses a burden particularly in populations affected by socioeconomic inequality, like in the Brazilian Amazon. In this region, the GS and CS rates per 1,000 live births were 17.5 and 7.1 in 2019, respectively (3, 4). Additionally, a recent study mentioned the existence of gaps mainly in the early diagnosis and adequate treatment of gestational syphilis (4).
The Brazilian government has allocated resources to the EMTCT through the expansion of coverage for primary healthcare, rapid tests, and treatment for syphilis with autonomy in prescribing benzathine penicillin by nurses (5–7). However, the data reported suggest that these efforts have not been sufficient (3, 4).
Previous studies have reported that risk factors for GS are: one to three PNC visits (8), less education, a history of abortion (9, 10), previous sexually transmitted infections (8, 10, 11), multiple sex partners (9–11), unmarried status, travel of sex partner in the past 12 months (10), substance use (11). However, only one case-control study has assessed programmatic (access and quality of prenatal care) factors (8).
There has been no study to identify programmatic factors, sociodemographic, obstetric, and behavioral factors associated with GS among postpartum women with access to PNC in areas affected by social inequality (8–11). Therefore, identifying whether the access to a PNC program and an adequate number of PNC visits are capable of mitigating these factors is important for preventing mother-to-child transmission of syphilis (12–14).
This study aimed to determine the factors associated with GS among postpartum women who were part of PNC programs in the Brazilian Amazon.
Materials and methods
Study design
This observational, unmatched case-control study design was conducted at a referral hospital in Belém city, the capital of Pará state in northern Brazil. Among Brazilian states and capitals, Pará and Belém are the sixth and third lowest on the municipal Human Development Index (Pará = 0.746; Belém = 0.698), respectively. In addition, both this state and capital have low family health strategy coverage rates of 57.6 and 23.1%, respectively (15, 16). The study hospital was chosen because it is a public referral hospital in Belém, which provides the highest level of childbirth and PNC high risk for pregnant women in the state. Data collection was conducted from November 2020 to July 2021.
All participants of this study were postpartum women who had delivered at the study hospital and received PNC exclusively by the primary care. All women who were unable to answer the questionnaire were excluded.
The results of both the rapid test for syphilis (treponemal test) and Venereal Disease Research Laboratory (VDRL) nontreponemal test, as well as syphilis treatment data, were collected directly from the patients' medical records and the prenatal card. In this study, we followed the Brazilian Ministry of Health criteria for GS (17) which are defined as a case meeting the following conditions: (a) asymptomatic for syphilis, who during prenatal care, childbirth, and/or puerperium presents with at least one reagent test (treponemal or nontreponemal with any titration) and without any record of previous treatment; (b) symptomatic for syphilis, who during PNC, childbirth, and/or puerperium presents with at least one reactive test (treponemal or nontreponemal with any titration); or (c) during PNC, childbirth, and/or the puerperium, presents with a reactive nontreponemal test with any titration and reactive treponemal test, regardless of syphilis symptoms and prior treatment.
As a control population, we included postpartum women with nonreactive treponemal or nontreponemal tests during PNC, childbirth, and/or puerperium. In addition, women were excluded if the newborn's syphilis test (VDRL) was positive or clinical signs were exhibited.
The sample size was calculated using Epi Info™ version 7.2.2.16, StatCalc – Sample size and power function for unmatched case-control. The parameters used were: 95% Confidence Interval, 80% power, 13.7% the proportion of control exposed (less than three prenatal care visits) (8), and an odds ratio of 3.6. The final sample size was 47 cases and 94 controls (1:2 ratio of case to control) after subtracting the 25% non-response rate from the original 59 cases and 118 controls.
Data sources
Data were collected by trained nurses during the hospitalization in face-to-face interviews using a pretested, structured questionnaire, based on the medical records, the prenatal cards, and previous studies (8, 18–20).
The following variables were collected from the prenatal cards, medical records and interviews: (a) Sociodemographic factors — date of birth (current age - years), education level, marital status, monthly income, occupation, access to the internet; (b) Programmatic factors — number of visits for prenatal care, gestational age, syphilis screening, difficulty performing rapid tests for syphilis, difficulty talking about condom use with sexual partner, received prenatal card in the first visit for prenatal care, prenatal card in the maternity hospital, sexually transmitted infections test result in the maternity hospital; (c) Obstetrics and sexual factors — condom use, past history of sexually transmitted infections, age at first sexual intercourse (years), number of miscarriages, gravidity, and parity. A draft instrument was sent to the nurse researchers to check the content for clarity and adequacy. After these revisions, a pretest was conducted at the hospital using a 5% random sample of the total sample size. Women included in the pretest did not participate in the final sample. After the pretest, there were further questionnaire modifications, but no tests were performed to assess the reliability and validity of the questionnaire.
Variables
The principal outcome variable was the syphilis status of the women during prenatal care, childbirth, and/or puerperium. Participants were divided into two groups: reactive treponemal or nontreponemal test results (case) and not reactive (control). This variable was treated as a binary dependent variable. The response event selected was a case (reactive results). The independent variables were sociodemographic factors and programmatic, obstetric, and sexual aspects.
Statistical analysis
Data were analyzed using Minitab 20® and Biostat 5.3® software. Categorical variables were expressed as percentages, and numerical variables were expressed as the mean and standard deviation (SD). An odds ratio (OR), calculated by multiple logistic regression, was used to determine the factors associated with GS among postpartum women who attended a PNC program.
A bivariate regression analysis was used to assess the association between each independent variable and the dependent variable. All variables with a p < 0.20 were entered into a multiple logistic regression equation using a stepwise approach. Multicollinearity was verified using the variance inflation factor (VIF); the correlations were tolerable with a VIF < 5. A crude OR and adjusted odds ratio (AOR) with their respective 95% CIs were used to evaluate the effect. All p-values < 0.05 were considered statistically significant. To interpret the results, quality tests, the coefficient value of the independent variable, Z-value, and 95% CI and OR were considered in the regression.
Results
A total of 177 postpartum women (59 cases and 118 controls) comprised the sample of the study. Of the 177 women, only 31.5% were tested for syphilis during the first or third trimesters, or at childbirth, as recommended by the Brazilian Ministry of Health. Among the two groups, 20.3% of the case group and 36.4% of the controls received this test as recommended (Table 1).
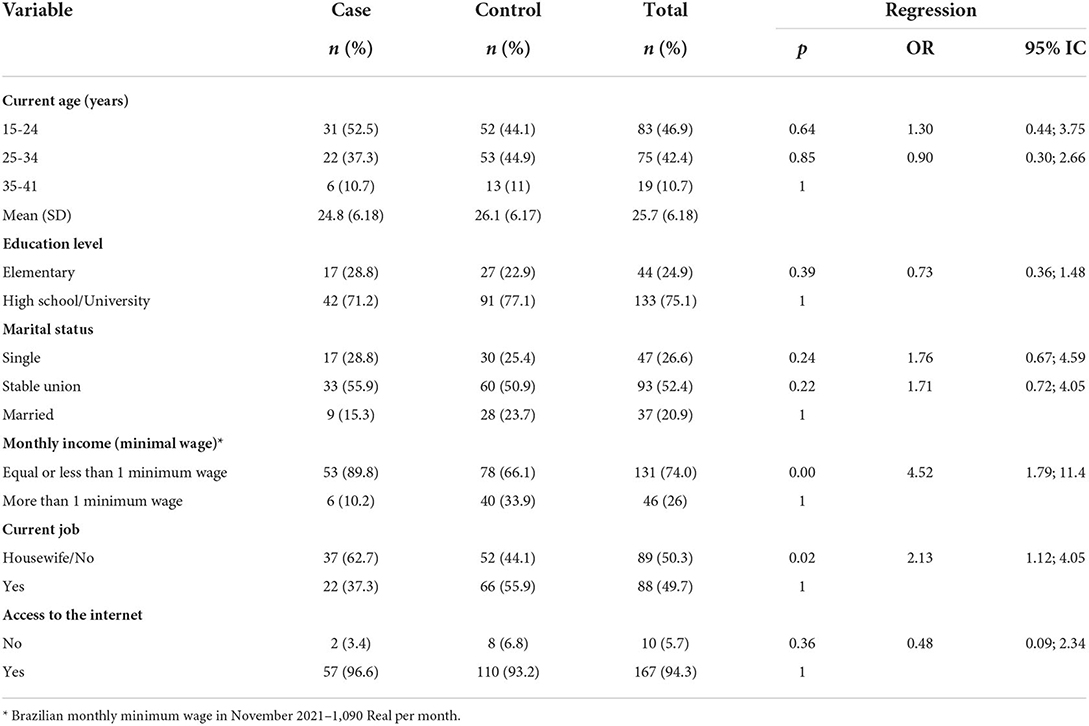
Table 1. Sociodemographic factors associated with gestational syphilis, in the Brazilian Amazon, 2020–2021.
All women in the case group were treated during pregnancy, childbirth, or puerperium. The therapeutic schemes are described below: 78% (46) benzathine benzylpenicillin 2.4 million international units administered in three-doses; 1.7% (01) benzathine benzylpenicillin 2.4 million international units administered as a single-dose; 3.4% (02) doxycycline 100 mg in postpartum women due to penicillin allergy (reactive result occurred at delivery or puerperium) and 18.6% (11) had no details of the therapeutic scheme or number of doses. In the case group, 84.7% (n = 50) had newborns diagnosed with CS. Among all participants, 95.5% (169) were tested for syphilis in any trimester during pregnancy and at the delivery and 4.5% (8) were tested in the maternity only, at the time childbirth, and/or puerperium (data not shown in tables).
Table 1 shows the sociodemographic characteristics of the two groups. Among all women, the mean age was 25.7, SD: ±6.18 years (95% CI: 24.7; 26.6; age range: 15 to 41 years). The age distributions were similar among cases (Mean: 24.8, SD: 6.18) and controls (Mean: 26.1, SD: 6.17). The odds of having a lower income are 5 times greater in the case group (OR = 4.52; 95% CI: 1.79–11.4; p = 0.00). In addition, the odds of being unemployed were two times greater in the case group than in the control group (OR: 2.13; 95% CI: 1.12; 4.05 p = 0.02). There were no statistically significant differences in education level, marital status, or internet access between the case and control groups (Table 1).
The programmatic aspects (access, offer, and use of healthcare services) for the control and case groups are shown in Table 2. The number of PNC visits was higher for the controls (Mean: 7.1; SD: 2.7) than for the case group (Mean: 5.8; SD: 2.7). The following factors were significantly more likely for cases than for controls: (a) one to six prenatal care visits (OR: 2.2; 95% CI: 1.16; 4.19; p = 0.01); (b) tested for syphilis (not as recommended) only in the second, third trimester, and when hospitalized for giving birth or only one test during pregnancy (OR: 2.24; 95% CI: 1.07; 4.69; p = 0.03); and (c) difficulty talking about condom use with their sexual partner (OR: 3.02; 95% CI: 1.27; 7.17; p = 0.01).
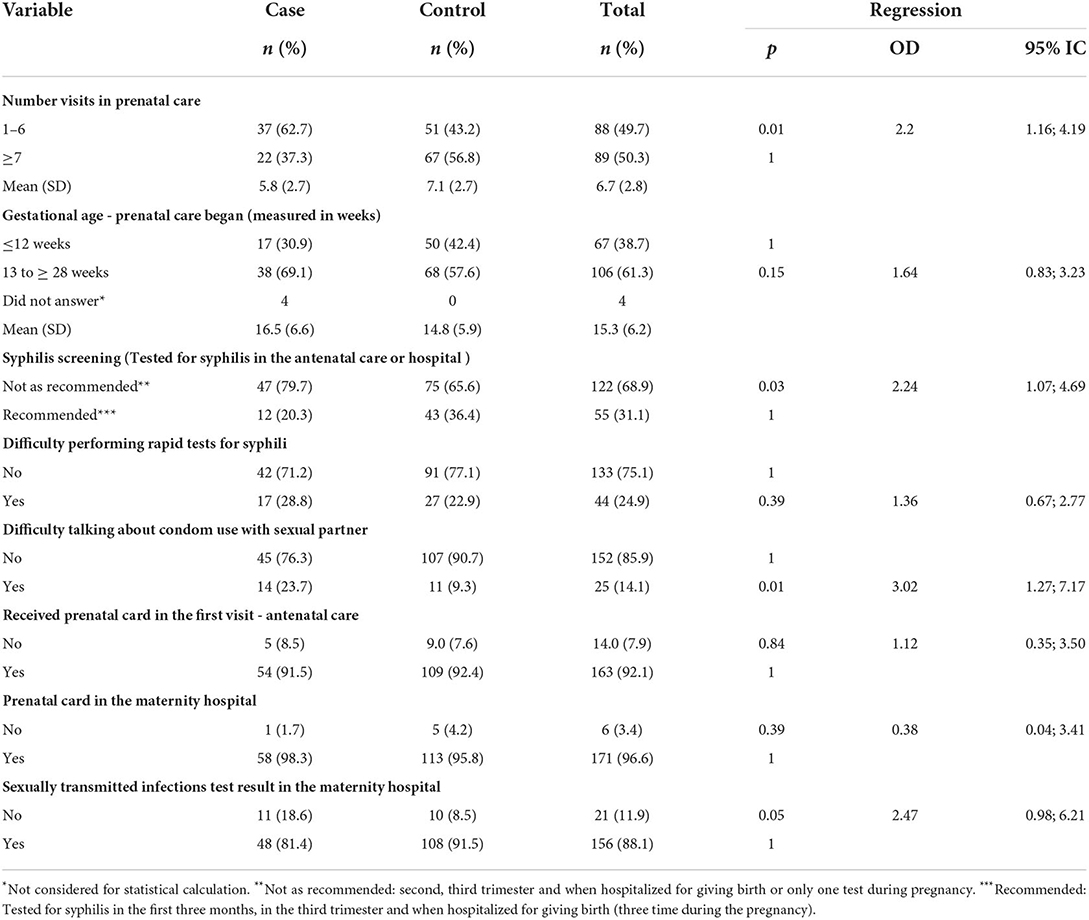
Table 2. Programmatic factors associated with gestational syphilis, in the Brazilian Amazon, 2020–2021.
The obstetric and sexual aspect data for the two groups are shown in Table 3. The age at first sexual intercourse was similar among cases (Mean: 16; SD: 2.3) and controls (Mean: 16.5, SD: 2.8). However, gravidity was higher in cases (Mean: 2.5; SD: 1.7) than in controls (Mean: 1.9; SD: 1.3). In regression, a past history of sexually transmitted infections (STI) was approximately 23 times more likely to occur in the case group than in the control group (OR: 22.9; 95% CI: 9.4; 55.8; p = 0.00). The cases were more likely to have one to three miscarriages (OR: 4.3; 95% CI: 2.08; 9.16; p = 0.00), and multigravida (OR: 2.56; 95% CI: 1.93; 4.90; p = 0.00).
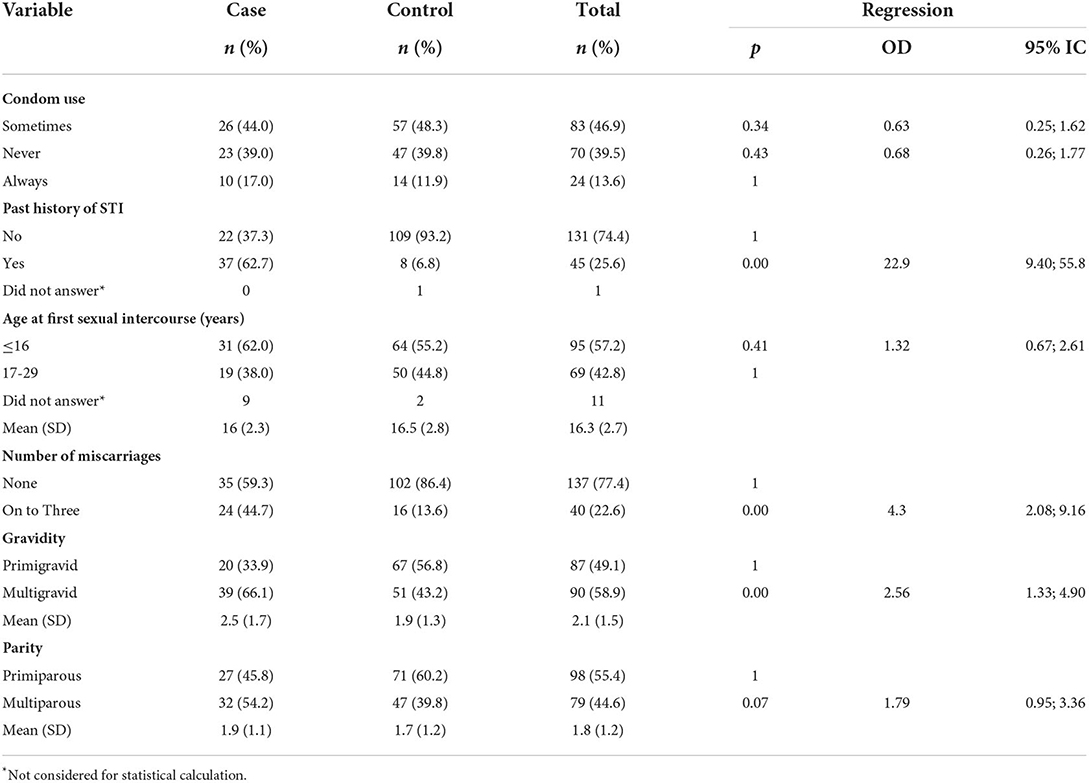
Table 3. Obstetrics and sexual factors associated with gestational syphilis, in the Brazilian Amazon, 2020–2021.
All variables in the binary regressions with p < 0.20 were then included in the final multiple logistic regression model (Table 4). The results showed that the case group, compared with the control group, had a lower monthly income, a past history of STI, one to three miscarriages, one to six prenatal care visits, difficulty talking about condom use with their sexual partner, and not receiving a STI test result in the maternity hospital.
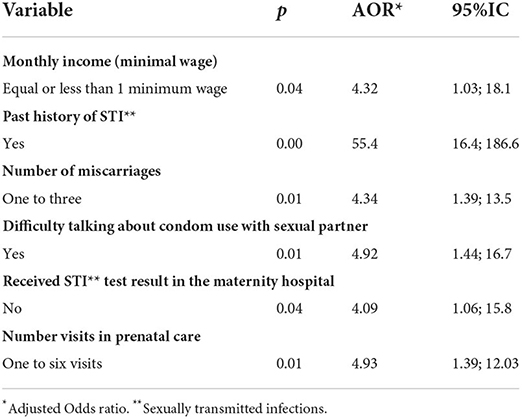
Table 4. Results of the multiple logistic regression analysis between factors and gestational syphilis, in the Brazilian Amazon, 2020–2021.
Discussion
This case-control study determined the factors associated with GS among postpartum women who were attending PNC programs in the Brazilian Amazon. In present study, the determinants of GS were lower monthly income, a past history of STI, one to three miscarriages, one to six prenatal care visits, difficulty talking about condom use with their sexual partner, and not receiving an STI test result in the maternity hospital.
Brazil has one of the world's largest universal healthcare systems, providing coverage and comprehensive healthcare for women and children in more than 5,500 municipalities (21, 22). The Brazilian Ministry of Health recommends seven or more prenatal care visits during pregnancy and the use of the reverse sequence algorithm for diagnostic syphilis for primary care services of the Unified Health System (22, 23). In 2019, the detection rates of gestational syphilis were 16.5 per 1,000 live births in Pará, a rate below that recorded in the North region (03).
In the present study, all participants used PNC services. However, more than half of the case group reported having only one to six prenatal visits during pregnancy. These women, 69.1% had their first prenatal care visit during the second or third trimester. Consequently, syphilis screening was performed later. The frequency of prenatal care visits was lower than that recommended by the Brazilian Ministry of Health, an important component of quality for PNC (2, 23, 24).
A late first visit is related to the quality of access to PNC (2, 25), including rapid syphilis testing. Early diagnosis makes possible the immediate treatment of pregnant women and their sexual partner (2, 26–28). This result is consistent with the findings of a similar case-control study from Northeast Brazil (8). Another study from Brazil showed that among women attending a prenatal program, one to three PNC visits were associated with nonperformance tests for syphilis (29). Studies conducted in China showed an association between the timing of first treatment for syphilis to adverse pregnancy outcomes and CS (30, 31), evidencing the importance of timing of the first PNC visit. In Brazil, after a positive syphilis reagent test (rapid syphilis test or VDRL), treatment can be provided during the same visit. But this does not exclude the need for a second test for a better diagnostic analysis (12).
The present study showed it was difficult for women to talk to their sexual partners about condom use, as demonstrated in other studies. In PNC visits, health professionals need to involve partners and provide the necessary support to pregnant women (32–34). Adequate treatment of the pregnant woman concomitantly with the treatment of the partner is a determining factor for preventing the vertical transmission of syphilis. To break the chain of transmission, all sexual partners must be educated and treated (4, 22). In Brazil, by the end of 2017, the treatment of the sex partners was taken out from the criteria defining adequate maternal treatment (12).
Studies conducted in Brazil have shown that regional and social inequities, including low income, are factors associated with GS (35, 36). In a population with precarious socioeconomic indicators, primary care professionals play a fundamental role in health education in all areas of care (37, 38). Our study location historically has the lowest percentage of primary care coverage of all the states in the northern region of the Brazilian Amazon (39). This low coverage directly impacts access to prenatal care, the follow-up for pregnant women, and the quality of PNC visits, especially for more vulnerable pregnant women. The CS rate is a consequence of these realities.
The findings of a past history of STI (8–10) and the number of miscarriages (9, 10) were consistent with previous case-control studies among GS cases in Brazil (8), Ethiopia (9) and China (10). Both factors should be investigated by healthcare professionals during prenatal care visits, especially if these diagnoses are associated with syphilis. The diagnosis of syphilis depends on a combination of the reactive test, as well as clinical and epidemiological history, independent of the adopted algorithm for syphilis testing (2, 22). Despite the improvement of public health policies that increase the coverage of primary care and are specific to syphilis, more needs to be done.
This study has some limitations. The GS cases in this study excluded postpartum women who did not attend the PNC program. The study was conducted in only the maternity hospital, and the syphilis status of the women was obtained from medical records, prenatal cards, and secondary data. Further studies in a larger number of maternity hospitals are needed. The findings of the present study include some flaws found in the recruitment of pregnant women, in the link in health responsibility, and in the attributes of the primary care based model. It is necessary to expand the studies to identify the structure and work process continuity in scenarios with a high incidence of gestational and congenital syphilis, as well as to understand the difficulties faced by pregnant women in accessing prenatal care, and to use mixed or qualitative methods to research this problem.
Conclusion
The study determined that sociodemographic, programmatic, obstetric, and sexual factors are associated with GS among postpartum women who were attending PNC programs in the Brazilian Amazon. The determinants were lower monthly income, a past history of STI, one to three miscarriages, one to six prenatal care visits, difficulty talking about condom use with their sexual partner, and not receiving a STI test result in the maternity hospital.
These results demonstrate that despite the advances in PNC to expand the availability of rapid tests for syphilis and an increase in penicillin prescriptions, there are still gaps in primary care in Pará such as late detected gestational syphilis and inadequate treatment in low-income populations that depend on the public health system. In this context, this study contributes to an analysis of the predictors of the high incidence rate of GS.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were reviewed and approved by the Research Ethics Committee of the Federal University of Pará under protocol n° 4.134.226. The patients/participants provided their written informed consent to participate in this study.
Author contributions
TU, EA, RS, EB, and GF conceived and designed the study. GF analyzed the data. TU collected the data. GF, VN, RV, and WA wrote the manuscript. CA-A, GF, and AP wrote the manuscript, provided critical comments, or revised the manuscript. All authors read and approved the final manuscript.
Funding
This study was supported by the Federal University of Pará (PAPQ-2022).
Acknowledgments
We thank all patients who agreed to participate in the study. Material from dissertation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer LM declared a shared affiliation with eight of the authors to the handling editor at the time of review.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.930150/full#supplementary-material
References
1. Korenromp EL, Rowley J, Alonso M, Mello MB, Wijesooriya NS, Mahiané SG, et al. Global burden of maternal and congenital syphilis and associated adverse birth outcomes-Estimates for 2016 and progress since 2012. PLoS One. (2019) 14:e0211720. doi: 10.1371/journal.pone.0211720
2. World Health Organization. Global guidance on criteria and processes for validation: elimination of mother-to-child transmission of HIV and syphilis, 2nd edition. Geneva (2017). Available online at: http://apps.who.int/iris/bitstream/handle/10665/259517/9789241513272-eng.pdf;jsessionid=6E8497E203EB1A272D44EEE0AE8F2028?sequence=1 (accessed April 10, 2022).
3. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Boletim epidemiológico: sífilis. Número Especial / Out. 2021. Ano V - n° 01 (2021). Available online at: http://www.aids.gov.br/pt-br/pub/2021/boletim-epidemiologico-de-sifilis-2021 (accessed April 10, 2022).
4. Carmo BAG, Santos DF, Hayase KAS, Santos MMQ, Naiff GRO, Botelho EP. Congenital syphilis in the Brazilian Amazon region: temporal and spatial analysis. Rev Eletr Enferm. (2020) 22:62349. doi: 10.5216/ree.v22.62349
5. Conselho Federal de Enfermagem (COFEN). Nota técnica 003/2017. Brasília-DF (2017). Available online at: http://www.cofen.gov.br/wp-content/uploads/2017/06/NOTA-T%C3%89CNICA-COFEN-CTLN-N%C2%B0-03-2017.pdf (accessed July 11, 2021).
6. Roncalli AG, Rosendo TMSS, Santos MMD, Lopes AKB, Lima KC. Effect of the coverage of rapid tests for syphilis in primary care on the syphilis in pregnancy in Brazil. Rev Saude Publica. (2021) 55:94. doi: 10.11606/s1518-8787.2021055003264
7. Figueiredo DCMM, Figueiredo AM, Souza TKB, Tavares G, Vianna RPT. Relationship between the supply of syphilis diagnosis and treatment in primary care and incidence of gestational and congenital syphilis. Cad Saude Publica. (2020) 36:e00074519. doi: 10.1590/0102-311x00074519
8. Macêdo VC, Lira PIC, Frias PG, Romaguera LMD, Caires SFF, Ximenes RAA. Risk factors for syphilis in women: case-control study. Rev Saude Publica. (2017) 51:78. doi: 10.11606/s1518-8787.2017051007066
9. Hailu K, Gebretsadik A. Determinants of gonorrhea and syphilis infections among pregnant women attending antenatal clinic at Dilla University Referral Hospital, Ethiopia: Unmatched case-control study. Womens Health. (2020) 16:1745506520940095. doi: 10.1177/1745506520940095
10. Zhou H, Chen XS, Hong FC, Pan P, Yang F, Cai YM, et al. Risk factors for syphilis infection among pregnant women: results of a case-control study in Shenzhen, China. Sex Transm Infect. (2007) 83:476–80. doi: 10.1136/sti.2007.026187
11. Lendado TA, Tekle T, Dawit D, Daga WB, Diro CW, Arba MA, Tekle T. Determinants of syphilis infection among pregnant women attending antenatal care in hospitals of Wolaita zone, Southern Ethiopia, 2020. PLoS One. (2022) 17:e0269473. doi: 10.1371/journal.pone.0269473
12. Domingues CSB, Duarte G, Passos MRL, Sztajnbok DCDN, Menezes MLB. Brazilian Protocol for Sexually Transmitted Infections, 2020: congenital syphilis and child exposed to syphilis. Rev Soc Bras Med Trop. (2021) 17:e2020597. doi: 10.1590/0037-8682-597-2020
13. Benzaken AS, Pereira GF, Cunha AR, Souza FM, Saraceni V. Adequacy of prenatal care, diagnosis and treatment of syphilis in pregnancy: a study with open data from Brazilian state capitals. Cadernos de Saúde Pública. (2020) 36:e00057219. doi: 10.1590/0102-311x00057219
14. Konje ET, Magoma MTN, Hatfield J, Kuhn S, Sauve RS, Dewey DM. Missed opportunities in antenatal care for improving the health of pregnant women and newborns in Geita district, Northwest Tanzania. BMC Preg Childbirth. (2018) 5:394. doi: 10.1186/s12884-018-2014-8
15. Instituto Brasileiro de Geografia e Estatística (IBGE). Dados demográficos- (2021). Available online at: https://www.ibge.gov.br/ (Accessed June 30, 2021).
16. Brasil. Ministério da Saúde. Secretaria de Atenção Primária à Saúde. Painel da atenção primária á saúde (2022). Available online at: https://aps.saude.gov.br/# (accessed March 5, 2022).
17. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Nota Informativa n° 2, de 19 de setembro de 2017. Altera os Critérios de Definição de Casos para notificação de Sífilis Adquirida, Sífilis em Gestantes e Sífilis Congênita do Guia de Vigilância da SVS/2017. IN. Boletim epidemiológico: sífilis. Número Especial. (2021). Available online at: http://www.aids.gov.br/pt-br/pub/2021/boletim-epidemiologico-de-sifilis-2021 (accessed April 10, 2022).
18. Teixeira LO, Figueiredo VLM, Mendoza-Sassi RA. Adaptação transcultural do Questionário sobre Conhecimento de Doenças Sexualmente Transmissíveis para o português brasileiro. J bras psiquiatr. (2015) 64:247–56. doi: 10.1590/0047-2085000000085
19. Bonnewell J, Magaziner S, Fava JL, Montgomery MC, Almonte A, Carey M, et al. Survey of syphilis knowledge among medical providers and students in Rhode Island. SAGE Open Med. (2020) 8:2050312120902591. doi: 10.1177/2050312120902591
20. Szwarcwald CL, De Almeida WDS, Damacena GN, De Souza-Júnior PRB, Ferreira-Júnior ODC, Guimarães MDC, et al. Changes in attitudes, risky practices, and HIV and syphilis prevalence among female sex workers in Brazil from 2009 to 2016. Medicine. (2018) 97: S46–53. doi: 10.1097/MD.0000000000009227
21. Giovanella L, Mendoza-Ruiz A, Pilar ACA, Rosa MCD, Martins GB, Santos IS, et al. Universal health system and universal health coverage: assumptions and strategies. Cien Saude Colet. (2018) 23:1763–76. doi: 10.1590/1413-81232018236.05562018
22. Freitas FLS, Benzaken AS, Passos MRL, Coelho ICB, Miranda AE. Brazilian Protocol for Sexually Transmitted Infections 2020: acquired syphilis. Rev Soc Bras Med Trop. (2021) 54:e2020616. doi: 10.1590/0037-8682-616-2020
23. WHO. WHO guideline on syphilis screening and treatment for pregnant women. Geneva: World Health Organization. Licence: CC BY-NC-SA 3.0 IGO. (2017). Available online at: https://apps.who.int/iris/handle/10665/259003 (accessed April 10, 2022).
24. BRASIL. Secretaria de Vigilância em Saúde. Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. Agenda Estratégica para redução da sífilis no Brasil 2020-2021. Brasília (2020). Available online at: http://www.aids.gov.br/pt-br/pub/2021/agenda-estrategica-de-sifilis-2020-2021 (accessed April 8, 2022).
25. Woldeamanuel BT, Belachew TA. Timing of first antenatal care visits and number of items of antenatal care contents received and associated factors in Ethiopia: multilevel mixed effects analysis. Reprod Health. (2021) 17:233. doi: 10.21203/rs.3.rs-110214/v1
26. Slutsker JS, Hennessy RR, Schillinger JA. Factors contributing to congenital syphilis cases - New York city, 2010-2016. MMWR Morb Mortal Wkly Rep. (2018) 67:1088–93. doi: 10.15585/mmwr.mm6739a3
27. Enkhbat E, Korenromp EL, Badrakh J, Zayasaikhan S, Baya P, Orgiokhuu E, et al. Adult female syphilis prevalence, congenital syphilis case incidence and adverse birth outcomes, Mongolia 2000-2016: Estimates using the Spectrum STI tool. Infect Dis Model. (2018) 3:13–22. doi: 10.1016/j.idm.2018.03.003
28. Kimball A, Torrone E, Miele K, Bachmann L, Thorpe P, Weinstock H, et al. Missed opportunities for prevention of congenital syphilis - United States, 2018. MMWR Morb Mortal Wkly Rep. (2020) 69:661–5. doi: 10.15585/mmwr.mm6922a1
29. Cesar JA, Camerini AV, Paulitsch RG, Terlan RJ. Non-performance of serological tests for syphilis during prenatal care: prevalence and associated factors. Rev Bras Epidemiol. (2020) 23:e200012. doi: 10.1590/1980-549720200012
30. Qin JB, Feng TJ, Yang TB, Hong FC, Lan LN, Zhang CL, et al. Risk factors for congenital syphilis and adverse pregnancy outcomes in offspring of women with syphilis in Shenzhen, China: a prospective nested case-control study. Sex Transm Dis. (2014) 41:13–23. doi: 10.1097/OLQ.0000000000000062
31. Wan Z, Zhang H, Xu H, Hu Y, Tan C, Tao Y. Maternal syphilis treatment and pregnancy outcomes: a retrospective study in Jiangxi Province, China. BMC Preg Childbirth. (2020) 20:648. doi: 10.1186/s12884-020-03314-y
32. Ali Abdulai M, Baiden F, Afari-Asiedu S, Gyabaa-Febir L, Adjei KK, Mahama E, et al. The risk of sexually transmitted infection and its influence on condom use among pregnant women in the kintampo north municipality of Ghana. J Sex Transm Dis. (2017) 26:8642685. doi: 10.1155/2017/8642685
33. Yan R, Deng B, Wen G, Huang L, Li L, Huang Z. Contact tracing of syphilis-seropositive pregnant women and syphilis-infection among their male partners in Bao'an district, Shenzhen, China. BMC Infect Dis. (2020) 20:684. doi: 10.1186/s12879-020-05403-x
34. Ngangue P, Fleurantin M, Adekpedjou R, Philibert L, Gagnon MP. Involvement of male partners of pregnant women in the prevention of mother-to-child transmission (PMTCT) of HIV in Haiti: a mixed-methods study. Am J Mens Health. (2021) 15:15579883211006003. doi: 10.1177/15579883211006003
35. Cardoso ARP, Araújo MAL, Cavalcante MDS, Frota MA, Melo SP. Analysis of cases of gestational and congenital syphilis between 2008 and 2010 in Fortaleza, State of Ceará, Brazil. Cien Saude Colet. (2018) 23:563–74. doi: 10.1590/1413-81232018232.01772016
36. Domingues RM, Viellas EF, Dias MA, Torres JA, Theme-Filha MM, Gama SG, et al. Adequação da assistência pré-natal segundo as características maternas no Brasil [Adequacy of prenatal care according to maternal characteristics in Brazil]. Rev Panam Salud Publica. (2015) 37:140–7.
37. Miltenburg AS, Lambermon F, Hamelink C, Meguid T. Maternity care and Human Rights: what do women think? BMC Int Health Hum Rights. (2016) 16:17. doi: 10.1186/s12914-016-0091-1
38. Kwame A, Petrucka PM. Universal healthcare coverage, patients' rights, and nurse-patient communication: a critical review of the evidence. BMC Nurs. (2022) 21:54. doi: 10.1186/s12912-022-00833-1
Keywords: congenital syphilis, case-control studies, pregnant women, syphilis, antenatal
Citation: Uchôa TLdA, Araújo EdC, da Silva RAR, Valois R, Azevedo Junior WSd, Nascimento VGC, Aben-Athar CYUP, Parente AT, Botelho EP and Ferreira GRON (2022) Determinants of gestational syphilis among women attending prenatal care programs in the Brazilian Amazon. Front. Public Health 10:930150. doi: 10.3389/fpubh.2022.930150
Received: 27 April 2022; Accepted: 04 October 2022;
Published: 09 November 2022.
Edited by:
Mathieu Nacher, INSERM CIC1424 Centre d'Investigation Clinique Antilles Guyane, French GuianaReviewed by:
Luiz Fernando Almeida Machado, Federal University of Pará, BrazilNajeh Hcini, INSERM CIC1424 Centre d'Investigation Clinique Antilles Guyane, French Guiana
Paul Le Turnier, Centre Hospitalier de Cayenne, French Guiana
Copyright © 2022 Uchôa, Araújo, da Silva, Valois, Azevedo Junior, Nascimento, Aben-Athar, Parente, Botelho and Ferreira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Glenda Roberta Oliveira Naiff Ferreira, Z2xlbmRhZkB1ZnBhLmJy