 Sze Wing Cherelle Ho1*
Sze Wing Cherelle Ho1* Yuen Lung WONG
Yuen Lung WONG- 1The Jockey Club School of Public Health and Primary Care, The Chinese University of Hong Kong, Shatin, Hong Kong SAR, China
- 2Faculty of Medicine, The Chinese University of Hong Kong, Shatin, Hong Kong SAR, China
- 3School of Public Health, The University of Hong Kong, Pokfulam, Hong Kong SAR, China
Cannabis is the most extensively abused drug, leading to multiple health burdens such as traffic accidents and psychosis. There is a global wave of legalization of recreational and medical cannabis. This study aimed to understand future healthcare workers' intention to use cannabis through extended Theory of Planned Behavior (TPB). An online cross-sectional survey on cannabis, including validated survey tools and questions on demographics, knowledge, and constructs of the TPB was designed, and distributed during virtual classes in late 2020. Responses were obtained from the Faculty of Medicine of a local university. Nine hundred ninety-six responses were collected, of which 629 were complete and analysed. Age was the only demographic variable associated with cannabis use intention (p = 0.029). Respondents with intention had better knowledge of cannabis. All TPB and additional constructs, including perceived behavioral control (COR = 3.44, 95% CI 2.72–4.35, p < 0.001), descriptive norm (COR = 2.24, 95% CI 1.81–2.77, p < 0.001), injunctive norm (COR = 0.51, 95% CI 0.42–0.61, p < 0.001), attitude (COR = 1.23, 95% CI 1.18–1.28, p < 0.001), knowledge (COR = 1.08, 95% CI 1.03–1.14), and perceived availability (COR = 2.75, 95% CI 2.22–3.40, p < 0.001) were individually associated with intention. In the final multiple logistic regression model adjusted for age, only attitude (AOR = 1.19, 95% CI 1.13–1.25, p < 0.001) and perceived availability (p = 0.004) showed statistically significant associations with intention. Descriptive norm (standardized coefficient = 0.570) had better explanatory power than the injunctive norm (standardized coefficient = −0.143) in the model. Perceived behavioral control was associated with intention among respondents with negative to neutral attitudes towards cannabis (AOR = 2.48, 95% CI 1.63–3.77, p < 0.001), but not among those with positive attitudes. All TPB constructs positively correlated with the intention to use cannabis. Changing the attitudes and perceived control on cannabis use may be useful in preventing cannabis use.
Introduction
Cannabis use refers to the consumption of cannabis plant products, typically for recreational or medical purposes. The main psychoactive substance in cannabis products is delta-9 tetrahydrocannabinol (THC), which gives users a sense of euphoria and “high.” Another active ingredient is cannabidiol (CBD), which is not psychoactive. Cannabis is the most extensively used illicit drug, and its market size is rapidly expanding (1). There were an estimated 200.4 million users in 2019, approximately accounting for 4.0% of the global population (2). Cannabis also accounts for half of all drug seizures (3). In the United States, 3.5 million people initiated cannabis use in 2019, among which 38.9 per cent are between the ages of 12 and 17 years (4). Sociodemographic analysis shows that young adults aged between 18 and 25, males over age 18, and college graduates have a greater past-year prevalence of cannabis use (4).
Cannabis use is associated with numerous adverse outcomes, notably a heightened risk of psychosis, mood disorders, and cognitive impairments (5–8). Associated systemic effects include respiratory symptoms, and cardiovascular events (9–12). 22.1 million people were diagnosed with cannabis use disorder (CUD) in 2016. The median age of onset for CUD was found to be 22 in a meta-analysis covering Australia, Europe, and the US (13). Other effects include injuries and deaths from motor vehicle accidents (7). Despite the health burden and young ages involved, a wave of cannabis legalization and decriminalisation is underway. It was accompanied by an 18 per cent increase in cannabis use over the past 10 years (14). As of mid-2021, six countries legally permit the possession and use of recreational cannabis. More than 30 nations have decriminalised it, and more than 60 have allowed medical cannabis. Sativex, a cannabis extract with THC and CBD, has been approved for medical use in 27 countries. Epidiolex, which only contains CBD, was also approved for intractable childhood epilepsy. The general perception of cannabis has become less negative. Perceived harmfulness was lowered among adolescents in the US and Europe (15).
In Hong Kong, all cannabis and its psychoactive derivatives, including THC, are illegal (16). Cannabis trafficking and possession/consumption in Hong Kong are criminal offences punishable by a fine of up to USD 636,949 and life imprisonment, and a fine of up to USD 127,388 and imprisonment for seven years, respectively (16). However, pure CBD is not restricted, and its oil products are available on the market (17). The culture seems to disfavour cannabis use, but cannabis is becoming more popular among young adults (18). In general, cannabis use has become more prevalent in Hong Kong, especially among adolescents aged below 21, which account for 49% of local illicit drug users. Those aged 21 or above only account for 9% of users (19, 20). Overall, the growing popularity of cannabis in Hong Kong resembles the global landscape.
Recent studies show that the theory of planned behavior (TPB) could be used to explain cannabis use in different populations (21–24). TPB provides a framework for explaining and predicting human decisions, such as the initiation and termination of addictive behaviors (25, 26). TPB suggested that behavioral intention is the most influential predictor of behavior. Behavioral intention is predicted using attitude (positive or negative evaluations of cannabis use), injunctive norm (perceptions about what significant others think about cannabis use) and perceived behavioral control (perceptions of the ease or difficulty of controlling cannabis use). Meta-analysis have established the model's efficacy in different health behaviors (27, 28). However, it is increasingly shown that the descriptive norm (perception of the extent to which others are engaging in the behavior) is particularly relevant to young adults transitioning to college, suggesting the possibility that the descriptive norm gives TPB a higher predictive power than the injunctive norm (23, 29). Our study assessed whether the TPB model, with the two types of norms included, could explain the intention to use cannabis in Hong Kong.
Ajzen suggests that TPB is open to further expansion and that the addition of potential predictors can enhance the model's explanatory power (26). Several studies on business and sports suggest that perceived availability might be associated with behavior, although they yield inconsistent results (30–34). Perceived availability represents the degree of accessibility to a particular entity, in our study context, cannabis, perceived by a person. We postulate that the factor can add to the explanatory power of our behavioral model in the context of cannabis use.
In Hong Kong, around 40% of the initiation of cannabis use happened at the age of 16–20 (35). Most students are admitted to college or university at the ages of 17 and 18. Studies show that living on campuses, attending university in urban geographic locations, and school climate are risk factors for cannabis initiation and use (36). Hence, students receiving tertiary education may have higher risks of cannabis use, warranting more public health investigation and interventions.
Epidemiological data in Hong Kong centre on the use of illicit drugs in general. To our knowledge, no local studies focus especially on cannabis and the factors associated with its use. We targeted undergraduates from the Faculty of Medicine of the Chinese University of Hong Kong (CUHK), the largest tertiary education institution in Hong Kong. The target population represents an age group prone to cannabis use. Understanding how future healthcare professionals conceptualise cannabis would be important because they may have discursive power on the image of cannabis, influencing public perceptions. However, literature in this regard is inadequate (37). Along this line of thought, we assess their knowledge of cannabis, in addition to TPB and potential constructs.
Overall, we aim to
(1) Explore the proportion and determinants of cannabis use intention among university students with a health-related major.
(2) Assess the explanatory power of TPB constructs regarding the intention to use cannabis in the sample as specified.
(3) Assess knowledge and perceived availability about cannabis use as additional factors for TPB and cannabis use intention.
Materials and methods
Participants and data collection
Our data were obtained from a cross-sectional survey. Due to the prolonged suspension of face-to-face classes amid COVID-19, we visited online classes for survey distribution and collection.
Prior to official data collection, a visit plan was devised to cover all students from the faculty. We chose one major-required course for each year of study and each major. Some batches of students did not have major-required courses. Multiple elective courses were visited. Exceptions were Bachelor of Nursing and Bachelor of Science in Biomedical Sciences, for which most of the class visits requests could not be entertained. For these two majors, mass mail was sent. Access to the survey was in the form of a link and QR code. Survey objectives and information for consent are shown adjacent to the link and verbally explained. The data collection period lasted from 28th August to 12th October. Completion of the survey took ~10 min. Survey responses were captured in Qualtrics, which prevented multiple participation by using cookies and converted responses into a dataset. All undergraduate students from the Faculty of Medicine of CUHK were eligible.
A sample size of 546 is estimated with the proportion of intention to be ~16.5% (38), where nine variables are to be included in the multiple logistic regression. A total of 996 respondents participated. Six hundred twenty-nine responses were complete and included for analysis. The response rate was 629/996 × 100% = 63.2%. The demographic and social backgrounds of respondents are summarised in Table 1. About 15% of respondents showed intention to use cannabis. 59.0% of respondents were female. The most frequently reported age group was 18 (22.6%), followed tightly by 21 (19.7%), 19 (18.4%), and 20 (17.5%). The age group was also the only demographic factor associated with intention (p < 0.05). Respondents pursuing a Bachelor of Medicine and Bachelor of Surgery made up the greatest proportion of all (44.4%), while Bachelor of Science in Biomedical Sciences made up the least (3.3%).
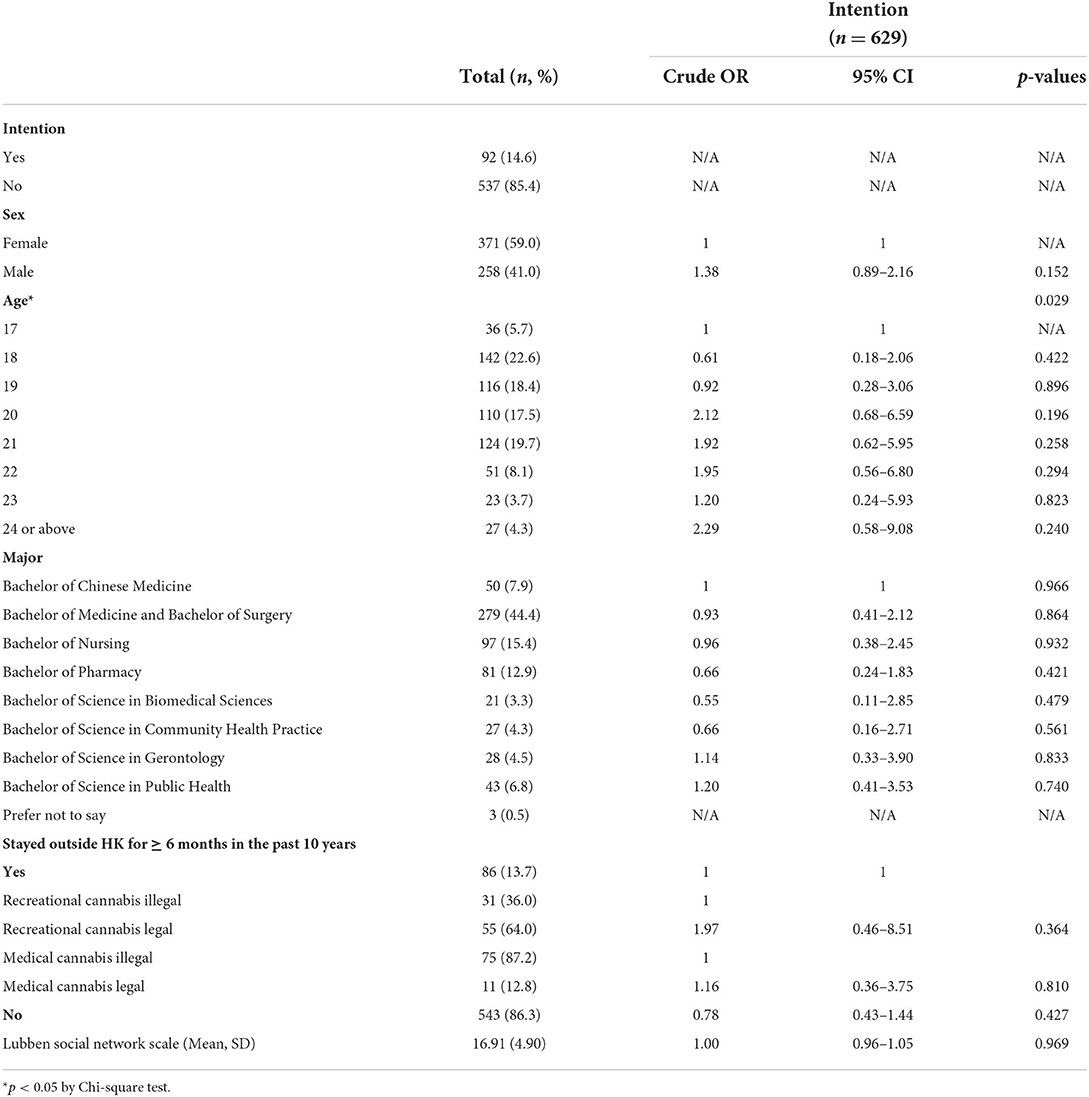
Table 1. Characteristics of respondents.
Instrument
To ensure the feasibility of the data collection method and face validity of the questionnaire, a pilot involving 48 subjects recruited by convenience sampling in the same population was done in April 2020. Face validity was established by assuring the clarity and meaning of the questions. Reliabilities of constructs composed of more than one item were estimated with Cronbach's alpha in the final sample, where the attitude construct has 0.95 and knowledge has 0.35. The domain knowledge of cannabis is a formative construct, where a change in one subscale does not imply the same directional change in other subscales. Therefore, a low Cronbach's alpha indicates that the questions within the knowledge construct are not redundant and not homogenous (39).
Extended theory of planned behavior
For knowledge, questions were designed to assess understanding of the properties, health effects, and legal statuses of cannabis. For properties, participants were asked to state whether “analgesics,” “hallucinogens,” “depressants,” “stimulants,” “tranquiliser,” and “others,” describe the type(s) of substance to which cannabis belong. Then, participants were to tell whether the following were active ingredients, namely “THB,” “CBD,” “CHB,” “THC,” and “TCD.” A maximum of 6 and 5 marks can be scored from the two parts respectively. For health effects, we asked if cannabis could lead to “anxiety,” “depression,” “increased risk of Parkinson's disease,” “euphoria,” “delusions,” “increased salivation,” “sleeplessness,” “dizziness,” “decreased heart rate,” “schizophrenia,” and “abnormally high body temperature.” A maximum of 11 marks can be earned. For legal statuses, we asked whether medical and recreational cannabis were respectively legal at the time of survey entry, in a range of states including Canada, Mainland China, United Kingdom, Japan, South Korea, Macau, Malaysia, South Africa, Hong Kong, Taiwan, and Singapore. A maximum of 11 marks can be earned, where each correct item accounts for 0.5 marks. The full marks for the total knowledge score are 33. Wrong responses, non-responses, and uncertainty would not result in mark deductions.
For attitude, we prepared sixteen questions listed in Table 2. Sixteen statements were rated by respondents. The questions were adapted from the Beliefs and Attitudes of Substance Abuse Inventory (BASAI), an instrument developed by Fok et al. to measure Chinese adolescent beliefs and attitudes towards substance abuse (40). Permission was granted by the authors. The items asked for the perceived effects of cannabis on mental, social, and general health. They also assessed the potential motivators of cannabis use, such as whether it helps “make friends,” “reduce anxiety,” “improve the quality of sleep,” and whether it is “fashionable” and “fun.” For each individual, scores from the sixteen items were added up to form the total attitude score.
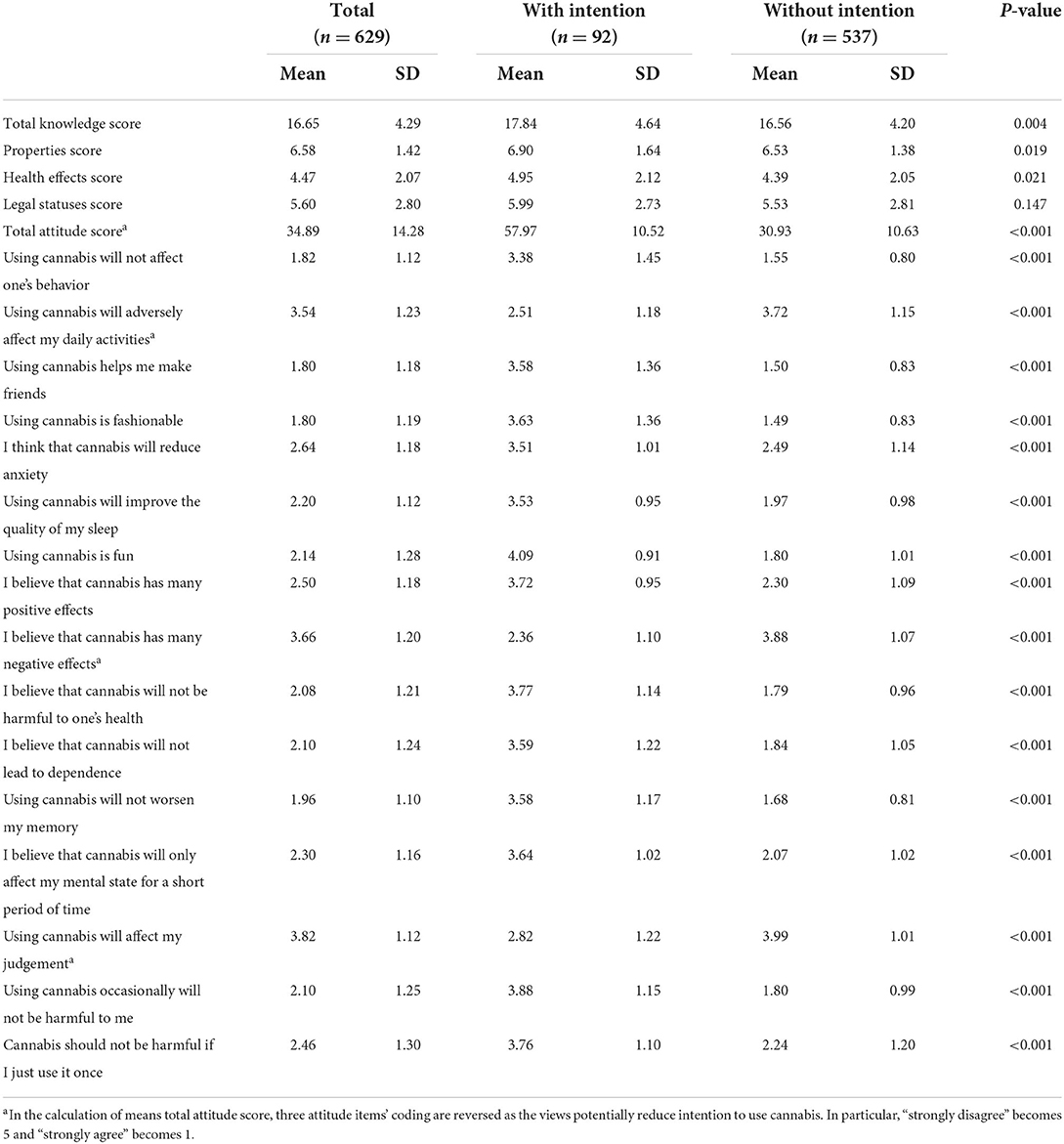
Table 2. Cannabis knowledge and attitude of respondents stratified by intention.
To assess the perceived behavioral control (PBC), the subjects were asked to rate the statement, “if I use cannabis, I will have the confidence to stop using them at any time.” Two kinds of norms were measured, including the descriptive norm among young people (“I think that cannabis use is common among young people”) and the injunctive norm from the society (“I think Hong Kong society is against the use of cannabis”).
For perceived availability, respondents were asked to rate “I think cannabis is readily available in my community.”
The core outcome of this study, the intention to use cannabis, was measured by asking respondents to rate the extent to which they agree with “I plan to use cannabis in the future.”
All items above were assessed with a Likert scale from 1 to 5, with 1 being “strongly disagree,” 3 being “neutral,” and 5 being “strongly agree.” Most attitude statements favoured cannabis, while some items disfavoured. The latter were reversely coded for the calculation of the total attitude score, where “strongly disagree” became “5” and “strongly agree” became “1.”
Demographics
Basic information, including subjects' sex, age, and major, was obtained. We collected geographical data, including whether the subjects had stayed outside Hong Kong for at least 6 months, the legal statuses of cannabis in the places they stayed, and that of cannabis for the nationality they identified with. In addition, we measured their social network with Lubben Social Network Scale-6 (final sample Cronbach's alpha: 0.798) (41), a validated tool that indicates social ties, with kind permission from the authors. The total scale, ranging from 0 to 30, is compiled by 6 items with equal weighting. A higher score indicates a better social network. These are potential confounders to be controlled.
Statistical analysis
Demographic variables were respectively tested for their association with intention with logistic regression, except for Lubben Social Network Scale-6 compiled with a T-test. Variables with statistical significance indicated an association with intention and are potential confounders. They were controlled in our model.
Participants rating 4–5 for intention statement were categorised as the “with intention” group, whereas those rating 1–3 as the “without intention” group.
Finally, the associations between interested independent variables and the intention were assessed. Crude odds ratios for each variable were computed by logistic regressions. To compile adjusted odds ratios, statistically significant demographic variables were assessed as covariates for each independent variable. A TPB-driven instead of a data-driven approach was used when building the two logistic regression models, i.e., the core model and the extended model. Several critical assumptions underlying multiple logistic regression were tested. Box-Tidwell Test was utilised to confirm linearity in the logit for continuous variables. All continuous independent variables (knowledge, PBC, norms, and attitudes) have a linear relationship with the logit of intention. Hence, the assumption was not violated. When using a variance inflation factor (VIF) threshold of 2.5, there was no multicollinearity between independent variables in the models. No outliers have a z-score larger than 3. All other assumptions were met.
To understand whether attitude moderates the relationship between PBC and intention, we did an exploratory post-hoc analysis by stratifying the samples into two groups, one with a positive attitude and the other with a negative or neutral attitude. A positive attitude was defined as having a total attitude score of 1 SD above the mean. We then see if PBC and intention were associated in each of the two groups.
A p-value smaller than 0.05 was taken as the level for statistical significance.
IBM SPSS Statistics Desktop 26.0 (IBM Corp., Armonk, N.Y., the U.S.) and Statgraphics Centurion 19 (Statgraphics Technologies, Inc., The Plains, Virginia, the U.S.) were used for data analysis.
Ethical statement
Ethics approval was obtained from The Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (CRE2019.496). Research reporting was on overall data at an aggregate level. No personally identifiable information was collected. The data was saved in a password-protected online account and computer.
Results
The knowledge and attitude of respondents regarding cannabis and its use are presented in Table 2. The mean Total Knowledge Score was 16.65 (SD = 4.29). Respondents showing intention to use cannabis had a slightly higher mean Total Knowledge Score (17.84, SD = 4.64) than those without intention (16.56, SD = 4.20, p < 0.01). Respondents with intention consistently showed higher means in all knowledge components, including Properties Score (6.90, SD = 1.64 vs. 6.53, SD = 1.38, p < 0.05), Health Effects Score (4.95, SD = 2.12 vs. 4.39, SD = 2.05, p < 0.05), and Legal Statuses Score (5.99, SD = 2.73 vs. 5.53, SD = 2.81, p = 0.147), although the last of which lacked statistical significance.
The mean Total Attitude Score was 34.89 (SD = 2.80). Respondents with an intention to use cannabis (57.97, SD = 10.52) had almost double the mean Total Attitude Score of those without intention (30.93, SD = 10.63, p < 0.001). The three attitude items disfavouring cannabis all showed lower means among respondents with an intention to use cannabis, whereas the rest of the items consistently showed higher means (p < 0.001).
Univariate analyses of each key construct are listed in Table 3. Of note, perceived behavioral control gave the highest magnitude of association (COR = 3.44, 95% CI 2.72–4.35, p < 0.001). A higher Total Attitude Score increased the odds of intention (COR = 1.23, 95% CI 1.18–1.28, p < 0.001). Both injunctive norm (COR = 0.51, 95% CI 0.42–0.61, p < 0.001) and descriptive norm (COR = 2.24, 95% CI 1.81–2.77, p < 0.001) were significant. Perceived Availability also carried a significant association with intention (COR = 2.75, 95% CI 2.22–3.40, p < 0.001). An increase in one mark in Total Knowledge Score increased the odds of intention by 1.08 (COR = 1.08, 95% CI 1.03–1.14, p < 0.01). All TPB and additional constructs were individually associated with the intention to use cannabis.
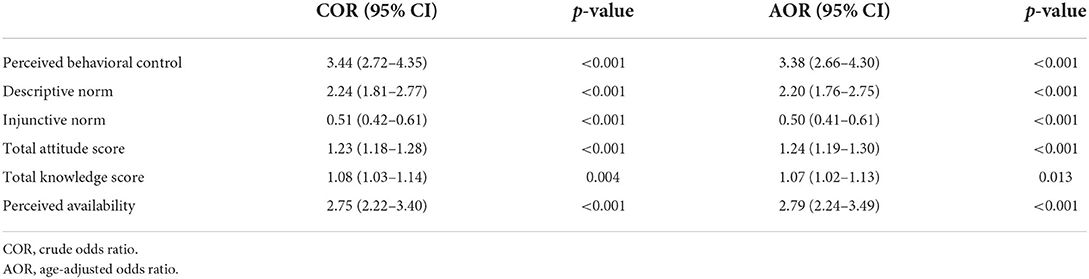
Table 3. Univariate analysis of key constructs with cannabis use intention.
Table 4 puts together the core TPB model (Nagelkerke R2 = 0.706) and its extended version (Nagelkerke R2 = 0.736) for cannabis use intention, where both models indicate good fits. In the core model, only descriptive norm (AOR = 1.59, 95% CI 1.12–2.27, p < 0.05) and attitude (AOR = 1.19, 95% CI 1.14-1.25. p < 0.001) demonstrate statistically significant correlation with intention. With the addition of knowledge and perceived availability, the descriptive norm loses its statistical significance, but still carries a higher explanatory power than the injunctive norm (standardized coefficients: 0.324 vs. −0.143). Attitude (AOR = 1.19, 95% CI 1.13–1.25, p < 0.001) becomes the only core TPB construct showing association with intention. Among the supplemented variables, perceived availability (p < 0.005) has a considerable association with intention. Treating the highest rating to perceived availability as the reference group, those who disagreed that cannabis was readily available had a much lower chance of having intention (AOR = 0.16, 95% CI 0.03–0.80, p < 0.05). Moreover, perceived availability carries a particularly high explanatory power in the model (standardized coefficient = 0.570), only second to attitude (standardized coefficient = 2.433). Finally, knowledge (AOR = 1.07, 95% CI 0.98–1.18, p = 0.152) is not shown to be associated with intention.
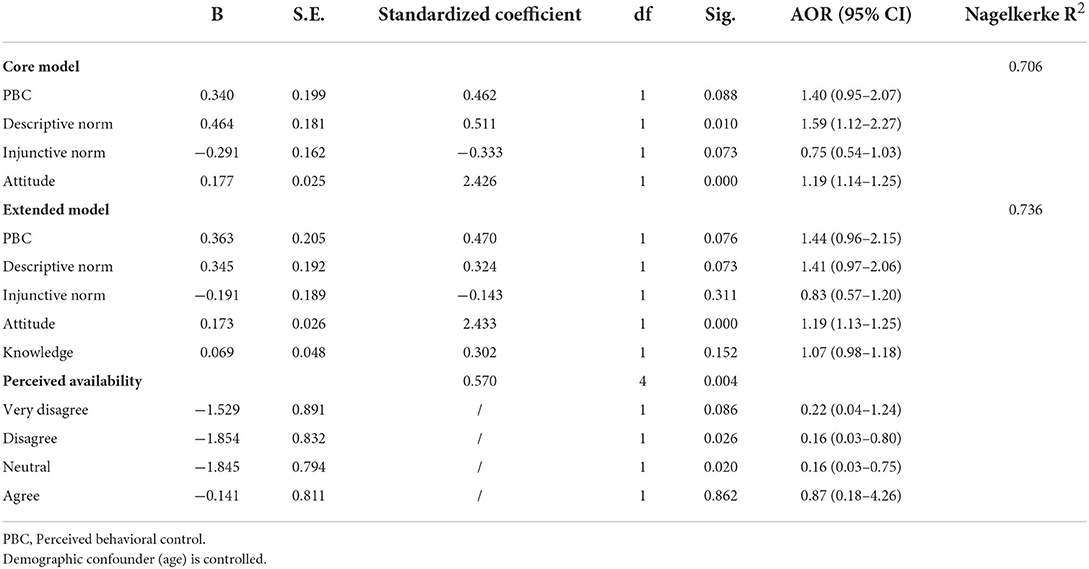
Table 4. Expanded theory of planned behavior model for cannabis use intention.
Further examination of PBC stratified by respondents' total attitude score is summarised in Table 5. PBC showed a significant association with intention among respondents with negative to neutral attitudes towards cannabis (COR = 2.67, 95% CI 1.76–4.04, p < 0.001), but not so among those with a positive attitude.

Table 5. Association between perceived behavioral control an intention stratified by total attitude score.
Discussion
Against the backdrop of cannabis legalization and popularization, we have conducted a cross-sectional study in Hong Kong, aiming to explore the determinants of cannabis use intention, with a particular focus on the theory of planned behavior. Our sample consists of a population rarely seen in cannabis studies, which was predominantly students of different allied health professionals. In our sample, each TPB variable alone significantly correlated to the intention to use cannabis. When placed in the extended regression model, all variables except attitude and perceived availability were no longer significant in the presence of other covariates. Comparing the two norms, the descriptive norm was consistently more influential than the injunctive norm, although both have not demonstrated statistical significance in our final model. Intention and knowledge were individually correlated but were not so in the final model. Overall, our study indicates patterns of cannabis use intention among young future healthcare workers, who are potential influencers of public health practice. It added to the small body of cannabis literature in cannabis-illegal regions and was the first study in Hong Kong investigating cannabis use intention and its determinants.
Previous research found that freshmen were the most prominent high-risk group for drug abuse, probably due to the “college effect” under which they have higher stress and responsibility, life transition, and a higher degree of freedom in a new community (42, 43). Contrary to this finding, we identified a peak of cannabis use intention among those aged 20–21, as freshmen in Hong Kong universities are typically aged 17–18. The development of social networks in college could increase the risk of cannabis use intention as this may expose students to resources of cannabis. Therefore, the authors speculate that a combination of the college effect and the aforementioned effect account for the peak in this age group. Moreover, some of those aged 20–21 could have been admitted from a previous higher diploma or associate degree, and the transition to a new institution may have put them at risk. Other underlying possibilities include larger stress due to seniority and cultural differences between Hong Kong and the West.
Knowledge of respondents was assessed according to the best available evidence we had at the time of data analysis. Nevertheless, cannabis research is rapidly evolving, and the knowledge encompassing it is subjected to change.
Subjects with an intention to use cannabis were more knowledgeable about cannabis. However, the score differences between subjects with and without intention were small, and the association between knowledge and intention was weak. The small score difference detected by our relatively large sample size could imply that it is only of statistical but not practical importance. However, it does challenge the a priori presumption, namely, that a higher intention to use a substance should be associated with a relative lack of knowledge. Moreover, the mean difference in the Legal Statuses score is not even statistically significant. These show the limited interaction between knowledge and cannabis use intention.
Few studies have investigated the relationship between knowledge of cannabis and intention to use. Among these limited studies, a Thai study has identified knowledge as a protective factor for the intention to take medical cannabis, running contrary to our results (44). We hypothesize that contextual differences may explain the discrepancy. At the time of their study, Thailand had just legalized medical cannabis. Before the commencement of this present study, Hong Kong has yet to legalize medical and recreational cannabis, and public health advocacy is generally unfavourable of cannabis use. Besides, the two studies have distinct study populations. In Rakpanich et al.'s study, respondents were rural Thais who were married and had low education levels (44). In our study, most participants were young and so were unlikely to be married, given the average ages of marriage in Hong Kong were 29.4 and 31.4 for females and males, respectively (45). Our participants also had higher education levels and lived in urban areas.
Interestingly, knowledge as one of the conventional triads (knowledge, attitude, and practice) for devising public health interventions is not necessarily reflective of intention, as shown in our study. This phenomenon could be unique to cannabis, where the same pieces of knowledge can be differentially interpreted. For example, there are both objective and subjective components in the evaluation of harm. Being more knowledgeable can both encourage or discourage cannabis use when there is controversy over how evidence is understood. Public health interventions shall consider the exact role of knowledge when it is targeted for behavioral modifications.
Similar to other studies (21, 23, 46, 47) and as expected, the total attitude score was positively associated with intention. Directions of association were consistent in all attitude items, and their aggregate attitude towards cannabis correlates with intention. Most importantly, attitude is the only core TPB construct retaining the significant association with intention upon the addition of potential covariates.
All the other TPB constructs correlated individually with intention. In both the core and extended models, the descriptive norm was consistently more influential than the injunctive norm based on the standardized coefficients. The descriptive norm has more explanatory power (higher Odds Ratio or explains more variance) than the injunctive norm, as shown in previous studies on the descriptive norm (23) and meta-analysis (48). In this meta-analysis (48), the descriptive norm has a particularly closer relationship with the behavior of adolescents and school-aged compared to adults (descriptive norm is better correlated with behavior in younger population). Such findings are different from that of Ito et al., who showed that only the injunctive norm, but not the descriptive norm, was a correlate. It could be explained by the differences in study populations. Ito et al. sampled students from the University of Colorado, where the baseline cannabis use rate (38.2%) was high, and the community was pro-marijuana. Our target population, however, has a low baseline cannabis use rate (6.4%). Hence, the effect of the descriptive norm may be less significant in their study.
Upon post-hoc analysis, PBC correlated well with intention univariately. However, when put alongside other variables in the model, it became insignificant. Therefore, we further investigated the moderation effect of attitude on PBC and intention, as suggested by Conner and McMillan. Previous studies (23, 49) showed a negative association between PBC and intention for those having a negative or neutral attitude towards cannabis. For those with a positive attitude, no association was observed. Our results resemble part of those studies. There was indeed no association between PBC and intention when focusing on those with a positive attitude. However, there was a positive association between those having a negative or neutral attitude. It should be unrelated to social desirability because, as Conner and McMillan suggested (23), if social desirability is involved, there should be a positive correlation between PBC and intention among those with a positive attitude, while no correlations between the variables would be observed for those having a neutral or negative attitude. Hence, similar to what Umeh and Patel suggested, we proposed that the discrepancy could be due to differences in intention measurement (50). Conner and McMillan measured the intention not to use cannabis while we measured the intention to use cannabis.
Perceived availability was found to carry a potent influence on intention to use cannabis, only second to attitude. It differs from other studies, where the exact influences of perceived availability are either not reported or contradictory (32–34). The relationship between perceived availability and drug use was explored in Hong Kong 20 years ago and was found to be closely related to cannabis use (51). The study sample (N = 969) consisted of 59.8% secondary school students and 40.2% incarcerated delinquents.
Ajzen (26) suggested that the availability of time is a control belief, a sub-construct of PBC. Analogous to his line of thoughts, we postulate that perceived availability is also a control belief closely related to PBC, hence explaining its strong effect on intention. Another possibility is that perceived availability could be related to the descriptive norm. If cannabis consumption is perceived to be prevalent among peers, the participant may also perceive cannabis as readily available in the participant's community. Our third postulation is that perceived availability was indicative of cannabis use. Those who use cannabis know where to obtain cannabis, so they likely have more access to it. In addition, the intention is very indicative of use [meta-analysis shows that 43–62% of intention will be translated into behavior (27)], so it is reasonable to assume a correlation between perceived availability and intention.
In this study, Nagelkerke R2 was used to describe the model fit. However, one should be aware that R2 gain might be due to the addition of new variables per se, not necessarily a better explanatory power.
Limitations
Our study was designed before the outbreak of COVID-19 and therefore does not consider the potential effects of the pandemic. Some studies showed that confinement in this period might raise the intention to use cannabis (52, 53). The results may differ considerably from a normal scenario. We suggest that readers interpret the results with scrutiny.
A small, convenient, and non-random sample was used for this study, undermining its representativeness to future health care workers. Also, there could be some mismatch between sample makeup and the target population. Only a small portion of participants was nursing students in our sample, but the proportion should be much larger in the Faculty of Medicine. Moreover, it is not generalisable to other educational institutions in Hong Kong. It also limits the generalisability to the future healthcare workforce in Hong Kong, as more than half of the workforce are nurses (54).
We might have underreported the prevalence of intention and use, as those who use or intend to use cannabis may miss out on class (55, 56). Bias may arise from self-report, social desirability, and memory inaccuracies.
It has been argued that cannabis use starts to develop at a much younger age (15–16 years), then increases with age, and finally tapers off (57, 58). Also noteworthy is that the younger is particularly prone to risky behaviors. In light of this, our sample may not be able to capture the initial phase of cannabis use and the characteristics of younger populations.
As an inherent limitation of a cross-sectional survey, we cannot establish any temporal relations, not to mention causal relations between variables. Further studies may work on these limitations, along with the moral norm, societal descriptive norm, and peer injunctive norm, which we have not but are worth exploring in the Asian population.
Implications
Overall, our findings both question and support the applicability of the TPB model for cannabis use and potentially other substance use contexts. On the positive side, the attitude has an immutable strength of association with intention. It shall continue to inform public health practices of the factors leading to cannabis use and targets of interventions. It would be beneficial to break down the processes whereby sociocultural contexts shape a population's perceptions and preferences of cannabis. For example, policymakers may identify the major sources of cannabis information, their contents, modes of delivery, and influences on different population groups. This is essential when cannabis and its culture become ever more globalized and that channels of information are unprecedentedly diverse. Unlike many other illicit drugs, cannabis is often commercialized as a recreational product with certain pharmaceutical effects, such as helping with sleep and anxiety. Even in Hong Kong, where THC is generally banned, there have been CBD products claiming the aforementioned effects. Therefore, how the population comes to interpret the functional aspects of cannabis and the underlying factors should be noteworthy for policymakers. This certainly does not mean that the psychosocial aspects of cannabis can be neglected. It is essential to keep inquiring into the role of cannabis in self-identity and relationships. While our study has not indicated an association between social networks and cannabis use intention, cannabis can still be perceived to play some role in social networks, especially among peers. In addition, our results encourage experimentation on attitude-modifying interventions, to which more resources can be directed. Equally important is to review current health promotion and education programs with regard to their relative position and effects among all other determinants of attitude. Policymakers should keep programs up to date in terms of their substances and modalities, especially in response to cultural influences and shifts among younger generations.
On the sceptical side, however, our findings imply uncertainties over the value of other TPB constructs. Many of the constructs have not shown significant associations with intention, and the types of norms included produce different results. Adding to the complexity is the potential of perceived availability and its effects on the TPB constructs. The implications are twofold. First, researchers shall continue to explore the application of various behavioral health models in a specific context and population. In addition to TPB, other health psychology models, such as the health belief model and social cognitive theory are also potential candidates when it comes to understanding health behaviors. Second, public health campaigns targeting cannabis norms have to distinguish the types of norms involved in light of their heterogeneous explanatory powers for intention. Third, a more in-depth delineation of perceived availability and its relations to TPB constructs is warranted.
Conclusion
This study demonstrates that TPB has limited explanatory power for cannabis use intention among a group of Hong Kong university students. Further research efforts may explore whether an extension of the model is appropriate for the context of cannabis. Comparisons can be made between various behavioral health models for the same population as well.
Author's note
The data collection and analysis was done during PC is employment under The Chinese University of Hong Kong.
Data availability statement
The original contributions presented in the study are included in the article/supplementary files, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
SH and YW: conceptualisation, data curation, formal analysis, methodology, project administration, writing—original draft, and writing—review and editing. PC: participant recruitment and writing—review and editing. All authors contributed to the article and approved the submitted version.
Acknowledgments
We genuinely thank Mr Kiang Ping Fai for awarding us the Pure Heart Academic Exchange Scholarship (2021–22) to support this publication. A notable expression of gratitude is due to Professor Zixin Wang (the Chinese University of Hong Kong) for his expertise, assistance, and substantial guidance on data analysis procedures. Our sincere thanks also go to Professor Marc Chong (the Chinese University of Hong Kong) for the advice on regression modeling. We are grateful for the valuable comments offered by Dr Crystal Chan (the Chinese University of Hong Kong) on questionnaire design. Also, we appreciate the effort of Dr Paul Chan (the Chinese University of Hong Kong) in reviewing our manuscript. Finally, we would like to thank the participated students and staff of the Faculty of Medicine at the Chinese University of Hong Kong for their time and support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Statista. Legal Cannabis Spending Worldwide From 2014 to 2024. (2020). Available online at: https://www.statista.com/statistics/1005176/global-legal-cannabis-market-size/ (accessed October 14, 2021).
2. United Nations. World Drug Report 2021. United Nations (2021). Available online at: https://www.unodc.org/unodc/en/data-and-analysis/wdr2021.html
3. United Nations Alcohol Drugs Addictive Behaviours Unit. Cannabis. (2021). Available online at: https://www.who.int/teams/mental-health-and-substance-use/alcohol-drugs-and-addictive-behaviours/drugs-psychoactive/cannabis (accessed October 14, 2021).
4. Centre for Behavioural Health Statistics Quality Substance Abuse Mental Health Services Administration. Results from the 2019 National Survey on Drug Use and Health: Detailed Tables. (2020). Available online at: https://www.samhsa.gov/data/sites/default/files/reports/rpt29394/NSDUHDetailedTabs2019/NSDUHDetailedTabs2019.htm
5. Hasan A, von Keller R, Friemel CM, Hall W, Schneider M, Koethe D, et al. Cannabis use and psychosis: a review of reviews. Eur Arch Psychiatry Clin Neurosci. (2020) 270:403–12. doi: 10.1007/s00406-019-01068-z
6. Gobbi G, Atkin T, Zytynski T, Wang S, Askari S, Boruff J, et al. Association of cannabis use in adolescence and risk of depression, anxiety, and suicidality in young adulthood: a systematic review and meta-analysis. JAMA Psychiatry. (2019) 76:426–34. doi: 10.1001/jamapsychiatry.2018.4500
7. McCartney D, Arkell TR, Irwin C, McGregor IS. Determining the magnitude and duration of acute Δ(9)-tetrahydrocannabinol (Δ(9)-THC)-induced driving and cognitive impairment: a systematic and meta-analytic review. Neurosci Biobehav Rev. (2021) 126:175–93. doi: 10.1016/j.neubiorev.2021.01.003
8. Ramaekers JG, Mason NL, Kloft L, Theunissen EL. The why behind the high: determinants of neurocognition during acute cannabis exposure. Nat Rev Neurosci. (2021) 22:439–54. doi: 10.1038/s41583-021-00466-4
9. Yang PK, Odom EC, Patel R, Loustalot F, Coleman King S. Nonmedical marijuana use and cardiovascular events: a systematic review. Public Health Rep. (2022) 137:62–71. doi: 10.1177/0033354920988285
10. Latif Z, Garg N. The impact of marijuana on the cardiovascular system: a review of the most common cardiovascular events associated with marijuana use. J Clin Med. (2020) 9:1925. doi: 10.3390/jcm9061925
11. Ghasemiesfe M, Barrow B, Leonard S, Keyhani S, Korenstein D. Association between marijuana use and risk of cancer: a systematic review and meta-analysis. JAMA Netw Open. (2019) 2:e1916318. doi: 10.1001/jamanetworkopen.2019.16318
12. Meehan-Atrash J, Korzun T, Ziegler A. Cannabis inhalation and voice disorders: a systematic review. JAMA Otolaryngol Head Neck Surg. (2019) 145:956–64. doi: 10.1001/jamaoto.2019.1986
13. Solmi M, Radua J, Olivola M, Croce E, Soardo L, Salazar de Pablo G, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. (2022) 27:281–95. doi: 10.1038/s41380-021-01161-7
14. Roth C. Global Marijuana Use Rose by 60 Percent Over the Past Decade. (2019). Available online at: https://www.dw.com/en/global-marijuana-use-rose-by-60-percent-over-the-past-decade/a-49358921 (accessed October 13, 2021).
15. United Nations Office on Drug Crime Division. Chapter 3 - Drug Market Trends: Cannabis Opioids. Austria: United Nation. (2021). Available online at: https://www.unodc.org/res/wdr2021/field/WDR21_Booklet_3.pdf (accessed November 28, 2021).
16. Hong Kong e-Legislation. Cap. 134 Dangerous Drugs Ordinance. (2019). Available online at: https://www.elegislation.gov.hk/hk/cap134?xpid=ID_1438402701417_001 (accessed October 14, 2021).
17. Narcotics Division Security Bureau Hong Kong Department Department of Health. Information on Cannabidiol (CBD) Products. (2021). Available online at: https://www.nd.gov.hk/pdf/CBD_Information_Note_English.pdf (accessed November 28, 2021).
18. The GrowthOp. Hong Kong Teens are Importing Cannabis Products at Alarming Rates. (2020). Available online at: https://www.thegrowthop.com/cannabis-news/hong-kong-teens-are-importing-cannabis-products-at-alarming-rates (accessed October 14, 2021).
19. Narcotics Division Security Bureau Hong Kong. Central Registry of Drug Abuse: Sixty-ninth Report. (2020). Available online at: https://www.nd.gov.hk/pdf/report/crda_69th/CRDA%2069th%20Report%20-%20(Full%20Version).pdf (accessed October 14, 2021).
21. Korn L, Haynie DL, Luk JW, Sita K, Simons-Morton BG. Attitudes, subjective norms, and perceived behavioral control associated with age of first use of cannabis among adolescents. J Sch Health. (2021) 91:50–8. doi: 10.1111/josh.12977
22. Hames A, Evangeli M, Harrop C, di Forti M. Understanding cannabis use in first-episode psychosis: an application of the Theory of Planned Behaviour. Early Interv Psychiatry. (2012) 6:38–44. doi: 10.1111/j.1751-7893.2011.00316.x
23. Conner M, McMillan B. Interaction effects in the theory of planned behaviour: studying cannabis use. Br J Soc Psychol. (1999) 38 (Pt 2):195–222. doi: 10.1348/014466699164121
24. Gagnon H, Côté J, April N, Julien AS, Tessier S. Predictors of intention not to use cannabis among young adults who attend adult education centers. Addict Res Theory. (2012) 21:123–31. doi: 10.3109/16066359.2012.703265
25. Bashirian S, Hidarnia A, Allahverdipour H, Hajizadeh E. Application of the theory of planned behavior to predict drug abuse related behaviors among adolescents. J Res Health Sci. (2012) 12:54–60.
26. Ajzen I. The theory of planned behavior: Frequently asked questions. Hum Behav Emerg Technol. (2020) 2:314–24. doi: 10.1002/hbe2.195
27. McEachan RRC, Conner M, Taylor NJ, Lawton RJ. Prospective prediction of health-related behaviours with the Theory of Planned Behaviour: a meta-analysis. Health Psychol Rev. (2011) 5:97–144. doi: 10.1080/17437199.2010.521684
28. Armitage CJ, Conner M. Efficacy of the Theory of Planned Behaviour: a meta-analytic review. Br J Soc Psychol. (2001) 40(Pt 4):471–99. doi: 10.1348/014466601164939
29. McEachan R, Taylor N, Harrison R, Lawton R, Gardner P, Conner M. Meta-Analysis of the Reasoned Action Approach (RAA) to Understanding Health Behaviors. Ann Behav Med. (2016) 50:592–612. doi: 10.1007/s12160-016-9798-4
30. Vermeir I, Verbeke W. Sustainable food consumption: exploring the consumer “Attitude – Behavioral Intention” Gap. J Agric Environ Ethics. (2006) 19:169–94. doi: 10.1007/s10806-005-5485-3
31. Brandão A, Costa AGd. Extending the theory of planned behaviour to understand the effects of barriers towards sustainable fashion consumption. Eur Bus Rev. (2021) 33:742–74. doi: 10.1108/EBR-11-2020-0306
32. Vermeir I, Verbeke W. Sustainable food consumption among young adults in Belgium: Theory of planned behaviour and the role of confidence and values. Ecol Econ. (2008) 64:542–53. doi: 10.1016/j.ecolecon.2007.03.007
33. Tarkiainen A, Sundqvist S. Subjective norms, attitudes and intentions of Finnish consumers in buying organic food. Br Food J. (2005) 107:808–22. doi: 10.1108/00070700510629760
34. Prins RG, van Empelen P, Te Velde SJ, Timperio A, van Lenthe FJ, Tak NI, et al. Availability of sports facilities as moderator of the intention-sports participation relationship among adolescents. Health Educ Res. (2010) 25:489–97. doi: 10.1093/her/cyq024
35. Narcotics Division Security Bureau Hong Kong. Table 19 Newly/Previously Reported Drug Abusers by age of First Abuse. (2021). Available online at: https://www.nd.gov.hk/statistics_list/doc/en/t19.pdf (accessed October 14, 2021).
36. Substance Abuse Mental Health Services Administration's Center. Preventing Youth Marijuana Use: Factors Associated With Use. (2017). Available online at: https://preventionsolutions.edc.org/sites/default/files/attachments/Preventing-Youth-Marijuana-use-Factors-Associated-with-Use_0.pdf (accessed October 15, 2021).
37. Gardiner KM, Singleton JA, Sheridan J, Kyle GJ, Nissen LM. Health professional beliefs, knowledge, and concerns surrounding medicinal cannabis – a systematic review. PLoS ONE. (2019) 14:e0216556. doi: 10.1371/journal.pone.0216556
38. Lau JTF. Study on Drug Abuse Situation and Service Needs of Non-engaged Youths in Hong Kong. Hong Kong: Security Bureau, Narcotics Division. (2013).
39. Stadler M, Sailer M, Fischer F. Knowledge as a formative construct: a good alpha is not always better. New Ideas Psychol. (2021) 60:100832. doi: 10.1016/j.newideapsych.2020.100832
40. Fok MS, Tsang WY. Development of an instrument measuring Chinese adolescent beliefs and attitudes towards substance abuse. J Clin Nurs. (2005) 14:986–94. doi: 10.1111/j.1365-2702.2005.01202.x
41. Lubben J, Blozik E, Gillmann G, Iliffe S, von Renteln Kruse W, Beck JC, et al. Performance of an abbreviated version of the Lubben Social Network Scale among three European community-dwelling older adult populations. Gerontologist. (2006) 46:503–13. doi: 10.1093/geront/46.4.503
42. Ross V, DeJong W. The Higher Education Center for Alcohol and Other Drug Abuse and Violence Prevention. Alcohol and Other Drug Abuse Among First-Year College Students. (2008). Available online at: https://safesupportivelearning.ed.gov/sites/default/files/hec/product/first-year.pdf
43. Derefinko KJ, Charnigo RJ, Peters JR, Adams ZW, Milich R, Lynam DR. Substance use trajectories from early adolescence through the transition to college. J Stud Alcohol Drugs. (2016) 77:924–35. doi: 10.15288/jsad.2016.77.924
44. Rakpanich W, Panomai N, Laohasiriwong W. Determinants of Intention to Use Medical Cannabis among People in the Northeast of Thailand. Indian J Public Health Res Dev. (2020) 11:1475–81. doi: 10.37506/ijphrd.v11i7.10304
45. Information Service Department Hong Kong. HK People Delaying Marriage. (2017). Available online at: https://www.news.gov.hk/en/categories/finance/html/2017/07/20170727_160533.shtml (accessed October 15, 2021).
46. Earle AM, Napper LE, LaBrie JW, Brooks-Russell A, Smith DJ, de Rutte J. Examining interactions within the theory of planned behavior in the prediction of intentions to engage in cannabis-related driving behaviors. J Am Coll Health. (2020) 68:374–80. doi: 10.1080/07448481.2018.1557197
47. Huansuriya T, Siegel JT, Crano WD. Parent-child drug communication: pathway from parents' ad exposure to youth's marijuana use intention. J Health Commun. (2014) 19:244–59. doi: 10.1080/10810730.2013.811326
48. Rivis A, Sheeran P. Descriptive norms as an additional predictor in the theory of planned behaviour: a meta-analysis. Curr Psychol. (2003) 22:218–33. doi: 10.1007/s12144-003-1018-2
49. McMillan B, Conner M. Applying an extended version of the theory of planned behavior to illicit drug use among students. J Appl Soc Psychol. (2003) 33:1662–83. doi: 10.1111/j.1559-1816.2003.tb01968.x
50. Umeh K, Patel R. Theory of planned behaviour and ecstasy use: an analysis of moderator-interactions. Br J Health Psychol. (2004) 9(Pt 1):25–38. doi: 10.1348/135910704322778704
51. Wong CSY, Tang CSK, Schwarzer R. Psychosocial correlates of substance use: Comparing high school students with incarcerated offenders in Hong Kong. J Drug Educ. (1997) 27:147–72. doi: 10.2190/5X79-QGJA-ADPJ-HFFU
52. Liebana-Presa C, Martinez-Fernandez MC, Benitez-Andrades JA, Fernandez-Martinez E, Marques-Sanchez P, Garcia-Rodriguez I. Stress, emotional intelligence and the intention to use cannabis in spanish adolescents: influence of COVID-19 confinement. Front Psychol. (2020) 11:582578. doi: 10.3389/fpsyg.2020.582578
53. van Laar MW, Oomen PE, van Miltenburg CJA, Vercoulen E, Freeman TP, Hall WD. Cannabis and COVID-19: Reasons for Concern. Front Psychiatry. (2020) 11:601653. doi: 10.3389/fpsyt.2020.601653
54. Hong Kong Food Health Bureau. Chapter 1 - Hong Kong Healthcare System and Healthcare Professionals. (2019). Available online at: https://www.fhb.gov.hk/download/press_and_publications/otherinfo/180500_sr/e_ch1.pdf (accessed March 28, 2022).
55. Lynskey M, Hall W. The effects of adolescent cannabis use on educational attainment: a review. Addiction. (2000) 95:1621–30. doi: 10.1046/j.1360-0443.2000.951116213.x
56. O'Callaghan FV, Joyce J. Cannabis: what makes university students more or less likely to use it? J Appl Biobehav Res. (2007) 11:105–13. doi: 10.1111/j.1751-9861.2006.tb00022.x
57. Guxens M, Nebot M, Ariza C, Ochoa D. Factors associated with the onset of cannabis use: a systematic review of cohort studies. Gac Sanit. (2007) 21:252–60. doi: 10.1157/13106812
Keywords: cannabis, theory of planned behavior, university students, future allied health workers, prevalence, questionnaire, young adult, adolescent
Citation: Ho SWC, WONG YL and Chung PH (2022) A cross-sectional survey: Exploring future healthcare workers' intention to use cannabis through extended theory of planned behavior. Front. Public Health 10:929016. doi: 10.3389/fpubh.2022.929016
Received: 26 April 2022; Accepted: 15 July 2022;
Published: 22 August 2022.
Edited by:
Michael A. Beazely, University of Waterloo, CanadaReviewed by:
Katerina Naumova, Ss. Cyril and Methodius University in Skopje, North MacedoniaYuen Onn Choong, Tunku Abdul Rahman University, Malaysia
Copyright © 2022 Ho, WONG and Chung. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sze Wing Cherelle Ho, Y2hlcmVsbGUuaG9AbGluay5jdWhrLmVkdS5oaw==